 Tingting Sun
Tingting Sun Yake Lin
Yake Lin Yanan Huang
Yanan Huang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Hum. Neurosci. , 23 December 2024
Sec. Cognitive Neuroscience
Volume 18 - 2024 | https://doi.org/10.3389/fnhum.2024.1512291
Background and purpose: Vestibular migraine (VM) is a common clinical disorder with a genetic predisposition characterized by recurrent episodes of dizziness/vertigo. Patients often complain of the presence of cognitive dysfunction manifestations such as memory loss, which causes great distress in daily life. In this study, we will explore the characteristics and possible risk factors of VM-related cognitive dysfunction by observing the cognitive function and vestibular function status of VM patients, laying the foundation for further exploration of the mechanisms of VM-related cognitive dysfunction.
Methods: This study included 61 patients with VM and 30 healthy individuals matched for age, gender, and education level. All subjects underwent the Addenbrooke’s Cognitive Examination-Revised (ACE-R), Dizziness Handicap Inventory (DHI), Hospital Anxiety and Depression Scale (HADS), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) at the first time of enrollment. Based on the ACE-R scores, the VM group was divided into the VM with cognitive dysfunction (VM-CogD) group (ACE-R < 86) and the VM without cognitive dysfunction (VM-NoCogD) group (ACE-R ≥ 86). The VM-CogD group was further categorized based on DHI scores into mild, moderate, and severe dizziness/vertigo subgroups (DHI ≤ 30 for mild, 30 < DHI ≤ 60 as moderate, and DHI > 60 as severe). All subjects underwent the head-shaking test, head-impulse test, test of skew, Romberg test, Unterberger test, videonystagmography, and caloric test to evaluate their vestibular function including the semicircular canals, vestibulo-ocular reflex pathway, and vestibulo-spinal reflex pathway. Differential analysis, correlation analysis, and ROC curve analysis were used to analyze the characteristics and influencing factors of the above clinical indicators in VM patients. It was considered that p-value < 0.05 was statistically significant, and | r| > 0.3 indicated a good correlation.
Results: There were no significant differences between the VM group and healthy control (HC) group in sex, age and education level. The total ACE-R score of the VM group was [82 (68.5, 87)], and the total ACE-R score, memory, verbal fluency, language, and visuospatial function scores were significantly lower than those of the HC group (p-value < 0.05) The percentage of horizontal semicircular canal dysfunction in the VM group (82.0%), the percentage the ocular motor dysfunction (49.2%), the positive percentage of the head-shaking test (27.9%), head-impulse test (37.7%), Romberg’s sign (60.7%), and Unterberger’s sign (60.7%) were significantly higher than those in the HC group (p-value < 0.05). Comparing the VM-CogD group (ACE-R < 86) with the VM-NoCogD group (ACE-R ≥ 86), the differences in Canal Paresis (CP) value, age, years of education, and duration of the disease were statistically significant (p-value < 0.05). In the VM-CogD group, CP value was negatively correlated with the ACE-R total score (r = 0.571, p-value = 0.000), memory (r = 0.526, p-value = 0.000), verbal fluency (r = 0.345, p-value = 0.024), language (r = 0.524, p-value = 0.000), and visuospatial function (r = 0.340, p-value = 0.026) scores. Age was negatively correlated with language functioning scores (r = 0.384, p-value = 0.011), and years of education was positively correlated with ACE-R total score (r = 0.504, p-value = 0.001) and language functioning (r = 0.455, p-value = 0.002) scores. When the cutoff values for the CP value, age, years of education, and duration of disease were 25.5, 33, 15.5, and 6.5, the accuracy of predicting VM-related cognitive dysfunction was the highest. The differences in DHI, DHI-P, DHI-E, DHI-F, HADS, PHQ-9, and GAD-7 scores were statistically significant between the VM group and the HC group (p-value < 0.05). In VM-CogD patients presenting with moderate dizziness/vertigo, the DHI total score was negatively correlated with the ACE-R total score (r = 0.539, p-value = 0.008), the DHI-F score was negatively correlated with the language (r = 0.450, p-value = 0.031) and visuospatial functioning part (r = 0.415, p-value = 0.049) scores, and the HADS-D scores were negatively correlated with the ACE-R total score and the part of memory functioning score (r = 0.539, p-value = 0.008).
Conclusion: (1) VM Patients exhibit multifaceted vestibular dysfunction and varying degrees of cognitive dysfunction, and cognitive function is affected by age, duration of illness, years of education, and vestibular function; (2) VM is a functional disorder, and the function disturbance, in conjunction with anxiety and depression, may participate in the occurrence of development of cognitive dysfunction in VM.
VM is one of the most common disorders with episodic vestibular syndrome in clinical practice, predominantly affecting young to middle-aged women. It is primarily characterized by moderate to severe dizziness or vertigo, with or without unilateral pulsating headache, photophobia, phonophobia, and visual aura. Headache is not specific to VM, as patients may never experience it. However, when it does occur, it can be before, after, or even during the vestibular symptoms (Lampl et al., 2019). In addition to the typical dizziness and headache symptoms, there are some accompanying symptoms such as brain fog and difficulty finding words (Beh et al., 2019). In recent years, numerous studies have found that VM patients experience cognitive dysfunction, involving various aspects like attention, memory, visuospatial function, language function, etc (Balci et al., 2018; Preysner et al., 2022; Wang et al., 2016). It was also found that the cognitive dysfunction in VM patients are related to the duration of the disease and the frequency and the severity of symptom (Lu et al., 2024). But it was neglected because of the youthful onset and mild dysfunction of cognitive (Çelebisoy et al., 2022). The recurrent symptoms of dizziness and headache have already influenced the efficiency of work and daily life for the patients (Molnár et al., 2022). The appearance of cognitive dysfunction symptoms further exacerbates this suffering. Therefore we should pay attention to this issue, which is to identify VM-related cognitive dysfunction early and take appropriate measures.
There are many risk factors for the occurrence and progression of cognitive dysfunction, including age, level of education, psychological and emotional factors, traumatic brain injury, white matter lesions, and underlying conditions such as diabetes and coronary artery disease (Ding et al., 2019; Hugo and Ganguli, 2014). Olfactory dysfunction is also closely associated with cognitive dysfunction (Molnár et al., 2023b). Current studies have found that vestibular function is closely related to cognitive function, while it is particularly evident in vestibular diseases (Bigelow and Agrawal, 2015; Rizk et al., 2020). Patients with unilateral or bilateral vestibular dysfunction exhibit impairments in visuospatial function, memory, attention and executive function. The more severe the vestibular function damage, the more pronounced the cognitive impairment (Popp et al., 2017); Patients with vestibular neuritis also show varying degrees of impairment in executive function (Moser et al., 2017), visuospatial perception, and visuospatial memory function (Oh et al., 2023). Eraslan Boz et al. (2023) found that patients with Ménière’s disease experience widespread cognitive dysfunction, including in memory, attention, executive functioning, and visuospatial functioning. Many studies have identified varying degrees of vestibular dysfunction in VM patients (Yujie et al., 2018). However, whether vestibular dysfunction in VM patients is the cause of cognitive dysfunction and the specific interaction mechanism between the two is unclear. This study aims to investigate and analyze the vestibular and cognitive functions in VM patients to elucidate the correlation and the underlying mechanisms, providing new insights for the early identification and intervention of VM-related cognitive dysfunction.
This study was conducted from February 2023 to December 2023. The study was approved by the Ethics Committee of the First Affiliated Hospital of Harbin Medical University, and all participants voluntarily participated with signed informed consent forms. All 61 VM patients were recruited from the Dizziness and Vertigo Clinic of the Neurology Department at the First Affiliated Hospital of Harbin Medical University. Meanwhile the control group which include 30 participants, matched for age, gender and education years, required no history of headaches, dizziness/vertigo, or other serious illnesses and they mostly consisted of family members or friends accompanying the outpatients. The inclusion and exclusion criteria for VM patients are as follows. Upon enrollment, VM patients were assessed using the ACE-R, DHI, HADS, PHQ-9, and GAD-7 scales. Based on ACE-R scores, VM patients were divided into two groups: the VM-CogD group (ACE-R < 86) and the VM-NoCogD group (ACE-R ≥ 86). The VM-CogD group was further subdivided into 3 groups based on their total DHI score: mild, moderate, and severe dizziness/vertigo with cognitive dysfunction (DHI ≤ 30 for mild, 30 < DHI ≤ 60 for moderate, and DHI > 60 for severe). Bedside and laboratory vestibular function examinations, including the head-shaking test, head-impulse test, test of skew, Romberg test, Unterberger test, videonystagmography, and caloric test were performed on VM patients during the remission phase of episodes. All examinations were conducted by the same neurophysiologist.
(1) Meet the diagnostic criteria for VM according to the Bárány Society (Table 1) (Lempert et al., 2012); (2) Be able to read and complete questionnaires; (3) Be able to communicate properly; (4) Sign the informed consent form.
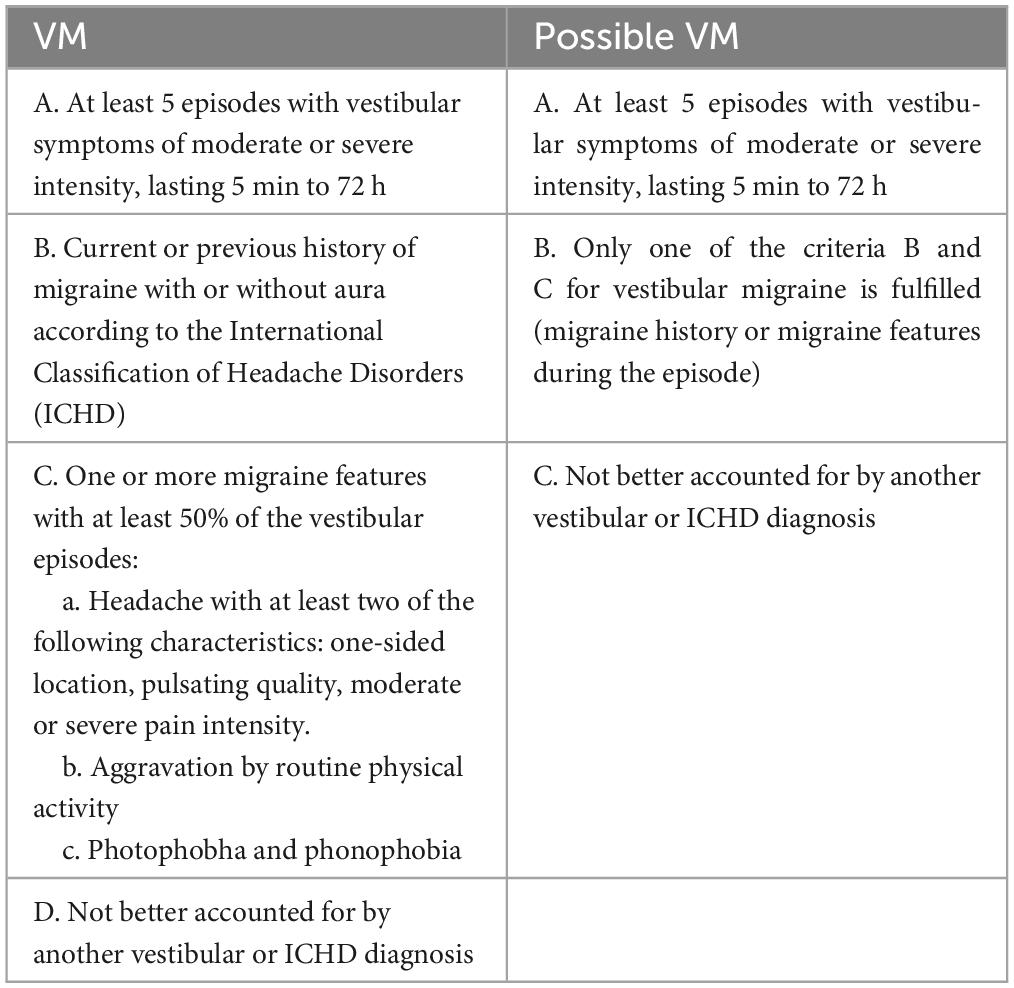
Table 1. Diagnostic criteria of VM.
(1) Inability to adequately expose the pupil or with blindness, strabismus and congenital spontaneous nystagmus; (2) Perforated eardrum, foreign body in the external auditory canal; (3) Other causes of cognitive dysfunction (such as Alzheimer’s disease, Lewy body dementia, vascular dementia, Parkinson’s disease, etc.); (4) Other vestibular disorders, such as benign paroxysmal positional vertigo (BPPV), vestibular neuritis, and Ménière’s disease (MD); (5) Individuals with severe physical illnesses, neuropsychiatric disorders and systemic diseases, such as stroke, coronary artery disease, schizophrenia; (6) Individuals with substance abusers; (7) Pregnant or breastfeeding women; (8) Individuals who refuse to sign the informed consent form.
(1) Demographic information: age, sex and years of education; (2) Clinical characteristics: duration of the disease and the frequency of episodes; (3) Vestibular function-related indicators: bedside and laboratory examinations (Tables 2, 3); (4) Scale scores of ACE-R, DHI, HADS, PHQ-9 and GAD-7 (Table 4).
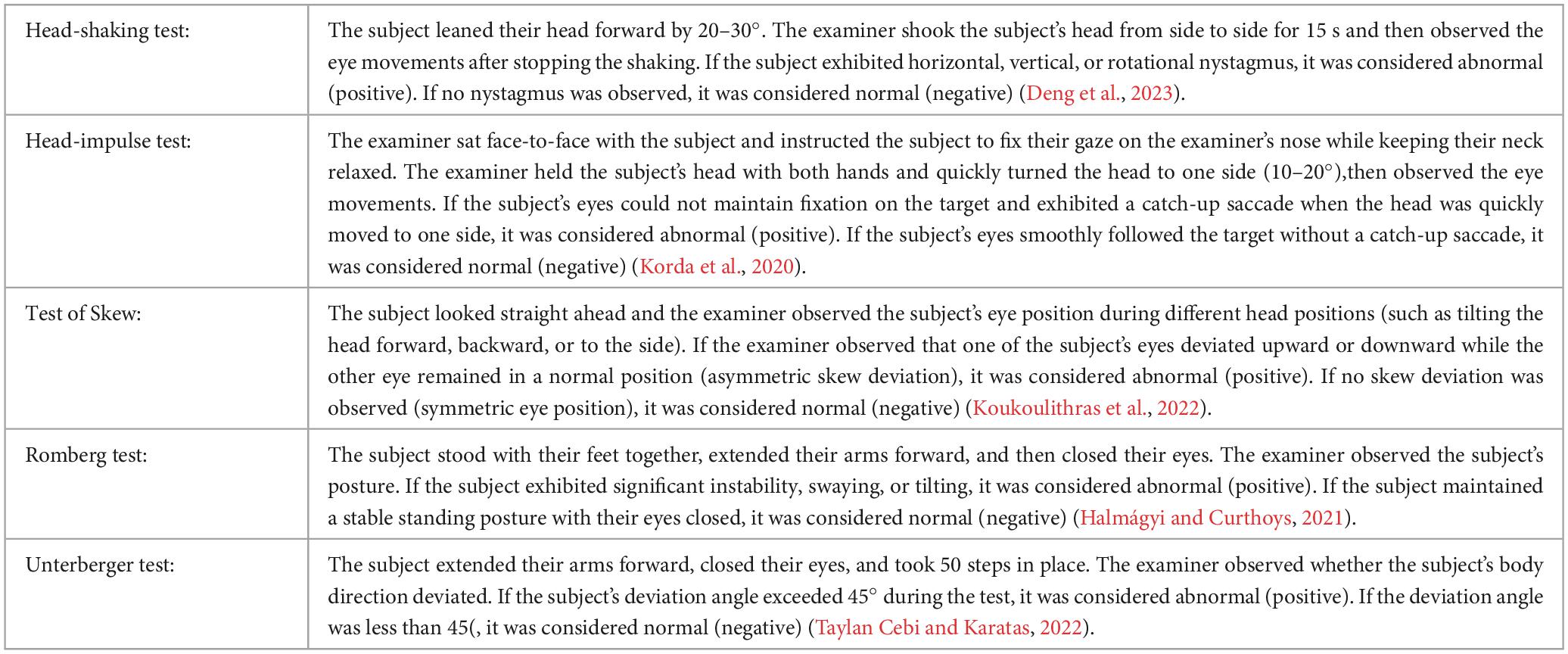
Table 2. Items of bedside examination for vestibular function.
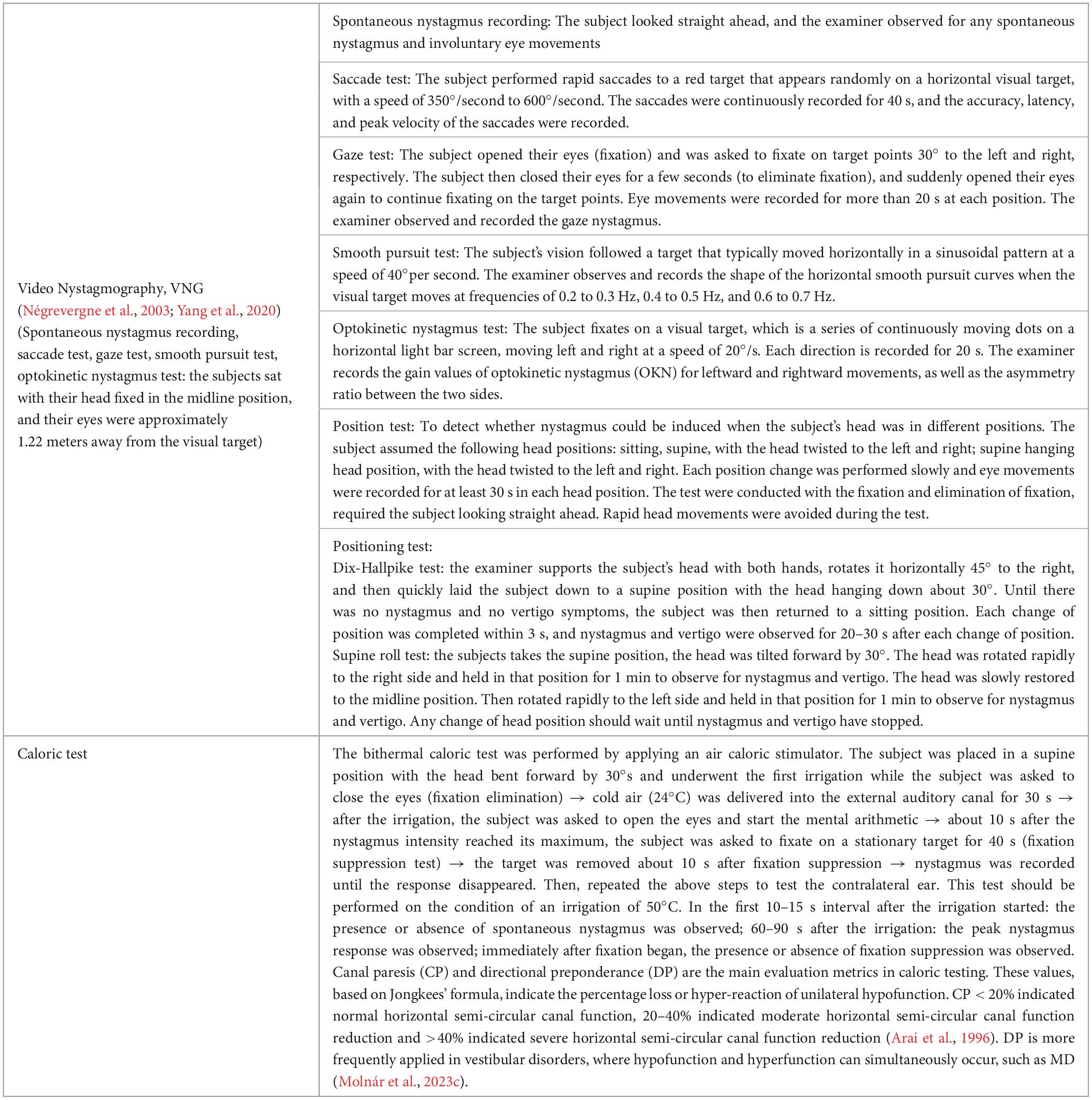
Table 3. Items of objective neurotological testing for vestibular function.
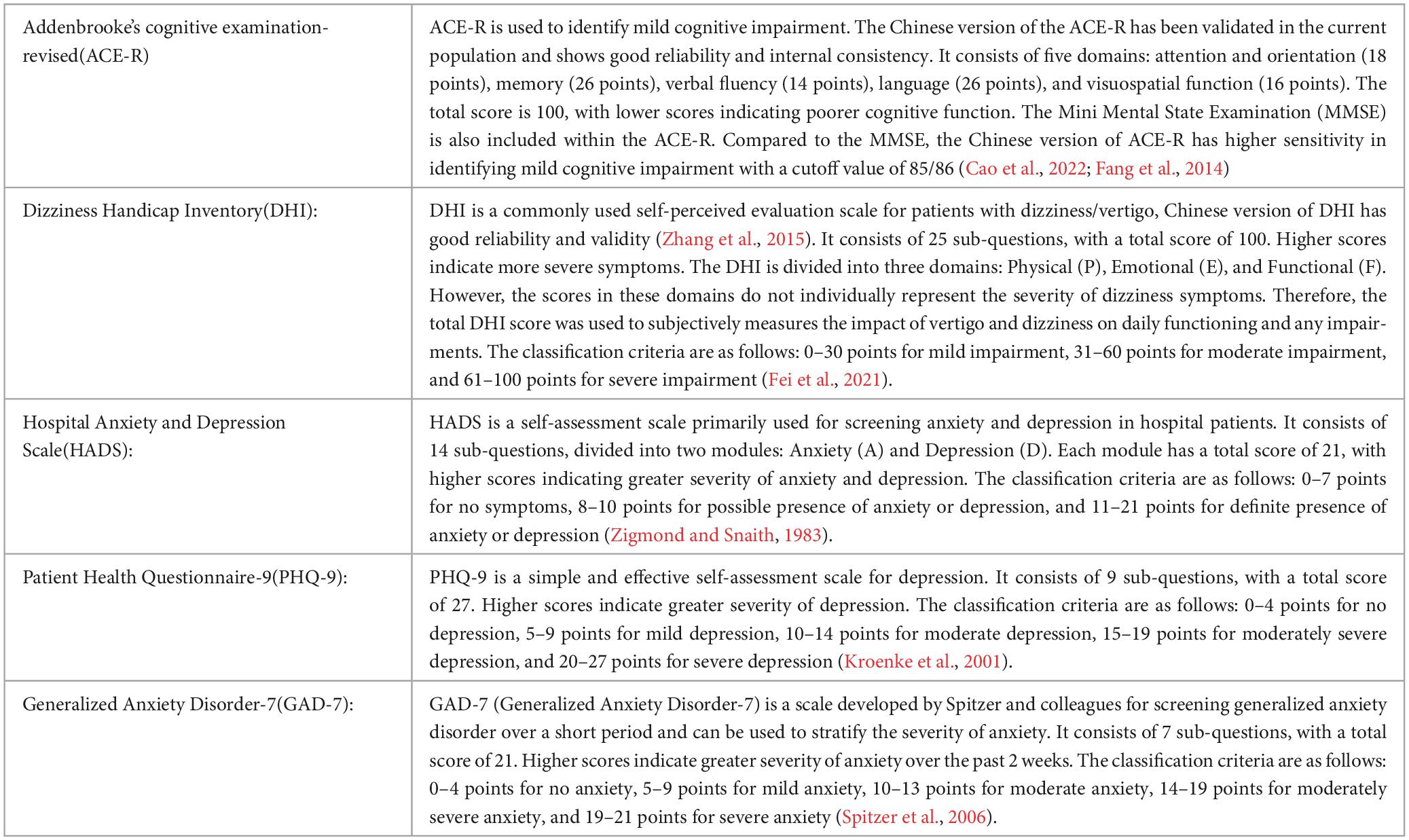
Table 4. Items of scales.
Statistical analysis was conducted using SPSS25.0. We used the Shapiro-Wilk test to perform normality testing on our data. Categorical data were presented as n (%), and intergroup comparisons were performed using the chi-square test or Fisher’s exact test. Continuous data that were normally distributed were presented as mean (SD), and intergroup comparisons were conducted using the independent samples t-test. Continuous data that were not normally distributed were presented as median (P25, P75), and the Mann-Whitney U test was used for intergroup comparisons. A p-value < 0.05 was considered statistically significant and | r| > 0.3 indicated a good correlation.
To assess the relationships between the variables, we conducted a correlation analysis. For normally distributed data, we used Pearson’s correlation coefficient, and for non-normally distributed data, we used Spearman’s rank correlation coefficient. To determine the statistical significance of the correlation coefficients, we used a two-tailed test with a significance level of α = 0.05. We also created scatter plots to visually represent the relationships between the variables.
To evaluate the performance of the diagnostic tests and determine the optimal cut-off values, we performed a Receiver Operating Characteristic (ROC) curve analysis. We calculated the True Positive Rate (TPR) and False Positive Rate (FPR) for each diagnostic metric at different cut-off values. We plotted the ROC curves with FPR on the x-axis and TPR on the y-axis. The Area Under the Curve (AUC) reflected the overall performance of the diagnostic tests, AUC > 0.5 indicates that the model has better predictive performance than random guessing. The ROC curves and AUC values were presented in both graphical and tabular forms. We reported the optimal cut-off values, sensitivity, specificity, and their corresponding 95% confidence intervals for each diagnostic metric.
A total of 61 patients were included in the VM group, with a median age of 47 years, consisting of 4 male and 57 female patients, and the median years of education for the VM group was 15 years. A total of 30 subjects were included in the HC group, with a median age of 45 years, consisting of 4 male and 26 female patients, and the median years of education was 13.5 years. There were no statistically significant differences in the general demographic data between the two groups (p-value > 0.05) (Table 5). Therefore, they were comparable in the subsequent studies.
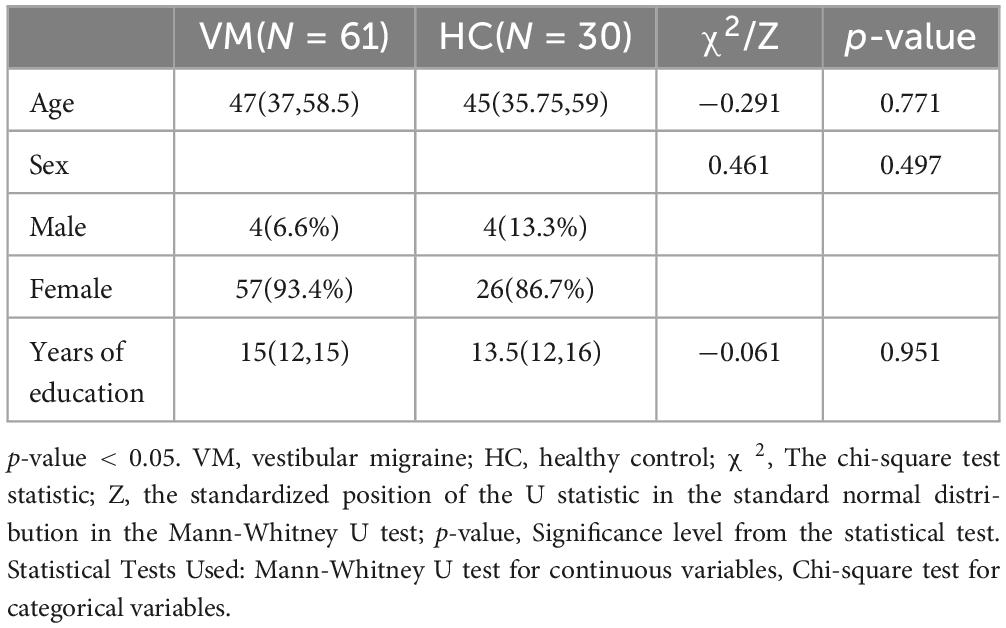
Table 5. Comparison of general demographic data between VM and HC groups.
There were statistically significant differences in the total DHI scores (p-value = 0.000), DHI-P (p-value = 0.000), DHI-E (p-value = 0.000), and DHI-F (p-value = 0.000) scores between the VM group and the HC group p-value (Figure 1 and Table 6). Specifically, the VM group had significantly higher DHI total score [46 (33, 63)], DHI-P [14 (10, 18)], DHI-E [12 (6, 20)], and DHI-F [20 (12, 27)] compare to the HC group, which had DHI total score [8 (4, 10.5)], DHI-P [2 (0, 6)], DHI-E [2 (0, 4)], and DHI-F [1 (0, 2.5)].
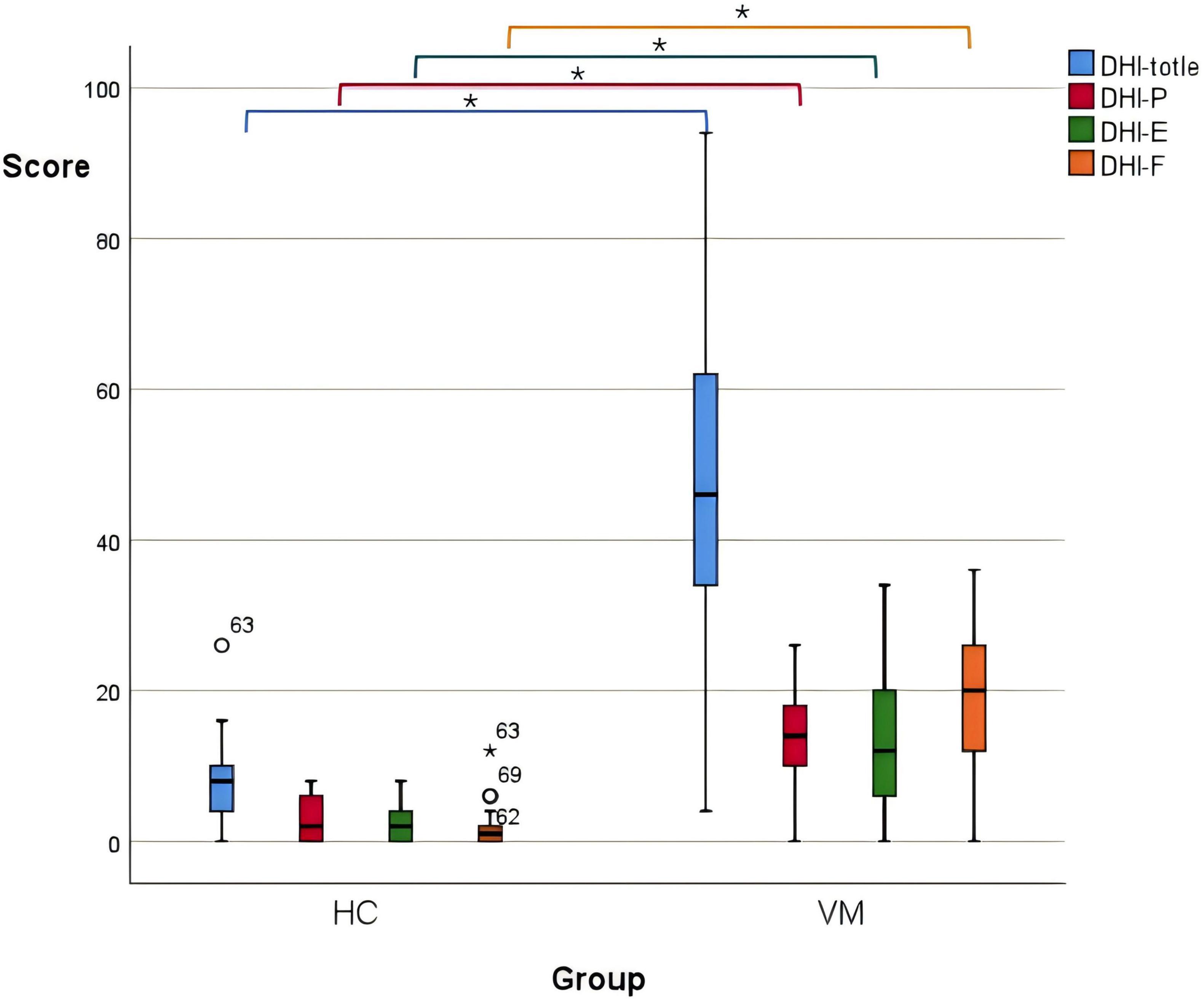
Figure 1. Boxplot comparing DHI scores between the VM and the HC groups. Black lines in the boxes: median values, box: the middle 50% of the data, whiskers: upper and lower 25%. * Represents extreme outliers.
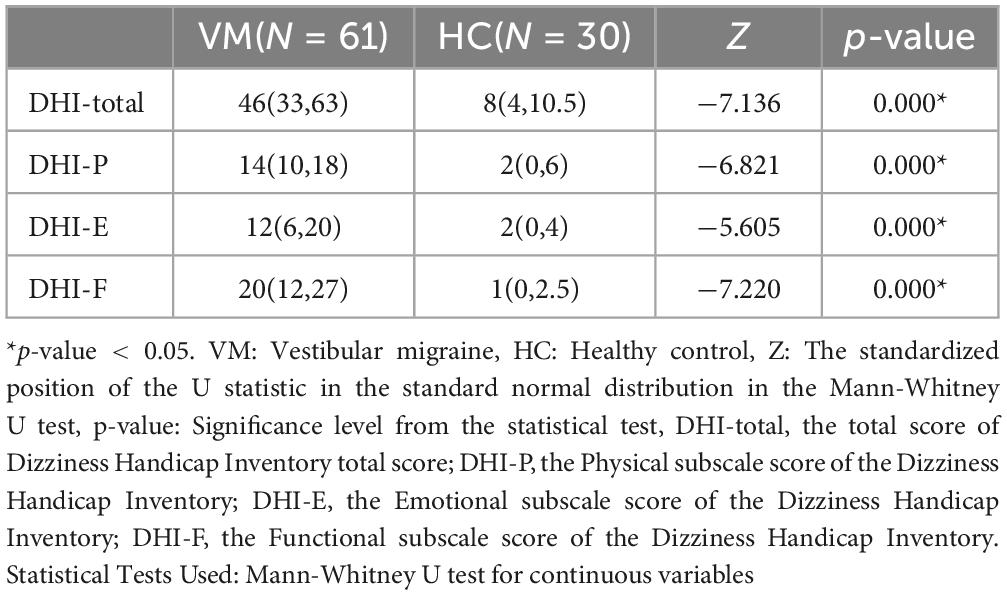
Table 6. Comparison of DHI scores between VM and HC groups.
Further, the ROC curve for the total DHI score in diagnosing VM was plotted. The AUC was 0.961 (95% CI: 0.922–1.000), with a corresponding p-value of 0.000, which is less than 0.05, indicating that the total DHI score has a high predictive value for VM. The cut-off value was 17, with a sensitivity of 0.951, and a specificity of 0.967, potentially serving as a predictive indicator (Figure 2 and Table 7).
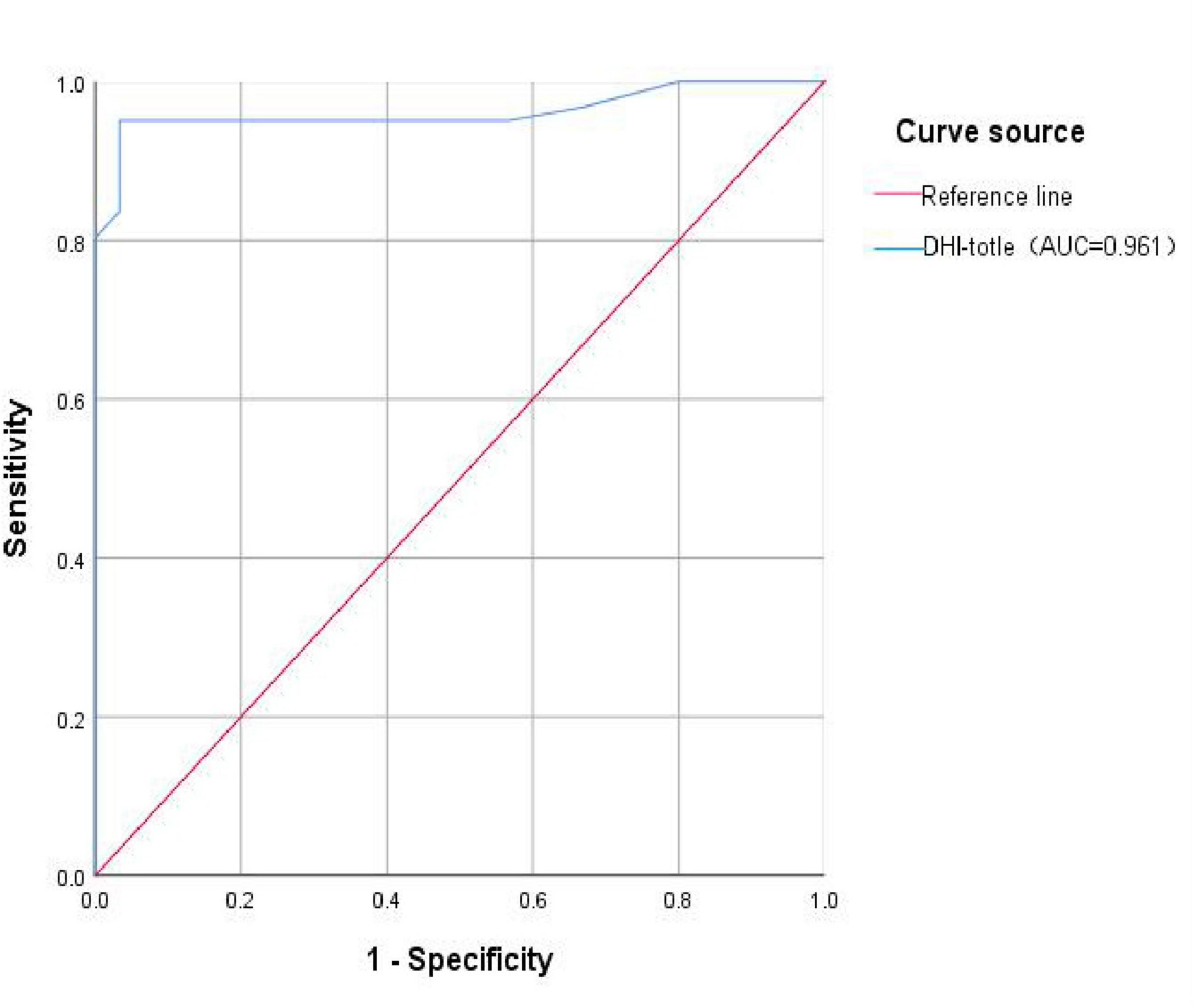
Figure 2. ROC curve of VM predicted by DHI total score. DHI-total, the total score of Dizziness Handicap Inventory total score; AUC, the Area Under the Curve.

Table 7. ROC curve for the total DHI score in diagnosing VM.
The emotional scales showed statistical differences between the VM group and the HC group (p-value = 0.000) (Figure 3 and Table 8). Specifically, the VM group had significantly higher HADS-A scores [7 (4, 11)], HADS-D scores [7 (4, 11)], PHQ-9 scores [8 (4, 13)], and GAD-7 scores [6 (2, 10)] compared to the HC group, which had HADS-A scores [2 (0, 4.25)], HADS-D scores [1 (0, 3)], PHQ-9 scores [1.5 (1, 2)], and GAD-7 scores [2 (1, 3.25)]. These results emphasized that the co-occurrence of psychiatric symptoms, particularly depression and anxiety, was significantly higher in VM patients.
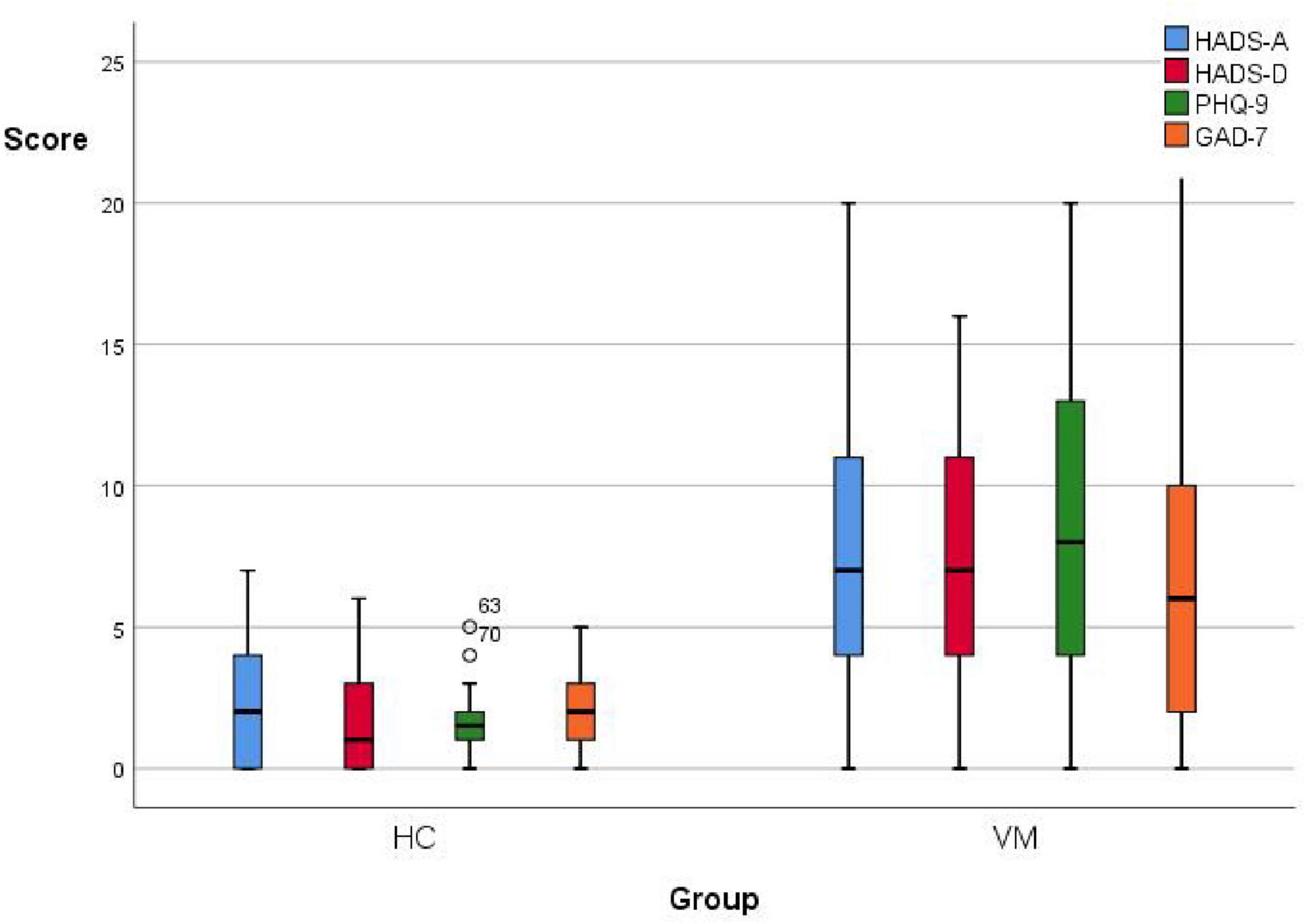
Figure 3. Boxplot comparing emotional scales scores between the VM and the HC groups. Black lines in the boxes: median values, box: the middle 50% of the data, whiskers: upper and lower 25%.
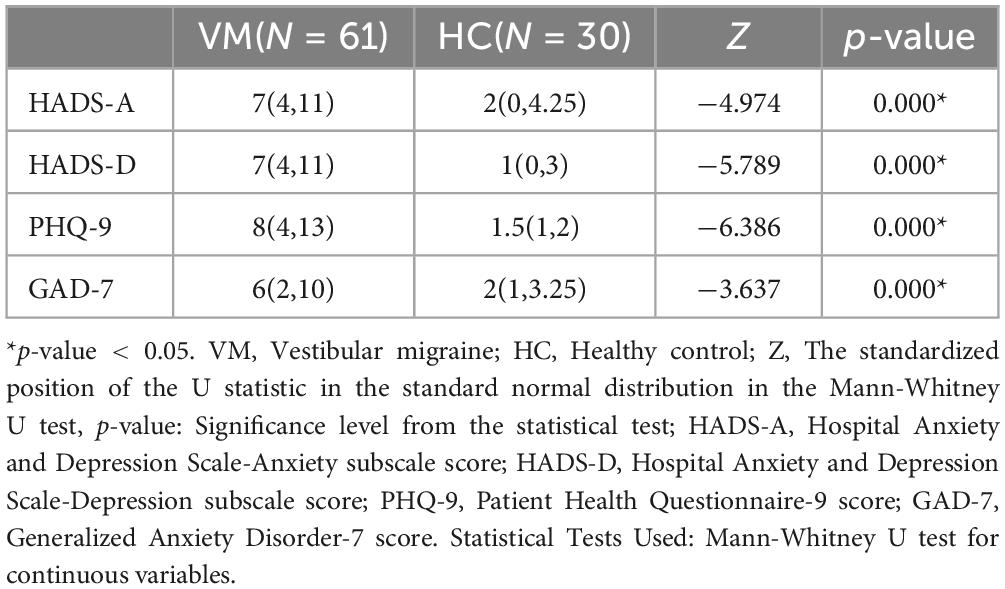
Table 8. Comparison of emotional scales between VM and HC groups.
It was statistically different in vestibular function indicators between the VM group and the HC group (p-value < 0.05) (Table 9). During the caloric test, we observed that VM patients exhibited reduced nystagmus intensity or even no nystagmus in response to cold/warm stimuli, as well as asymmetry in the intensity of nystagmus bilaterally. Additionally, some VM patients showed a change in the direction of nystagmus, such as nystagmus instead directed to the left when the right ear was stimulated with warm water. Specifically, the VM group had significantly higher percentages than the HC group for canal paresis (82.0% vs. 3.3%), oculor motor dysfunction (49.2% vs. 0.0%), positive head-shaking test (27.9% vs. 0.0%), positive head-impulse test (37.7% vs. 0.0%), positive Romberg’s sign (60.7% vs. 0.0%), and positive Unterberger’s sign (60.7% vs. 0.0%). Since the results of the test of skew were negative for all subjects in both groups, no statistical analysis was performed for this test.
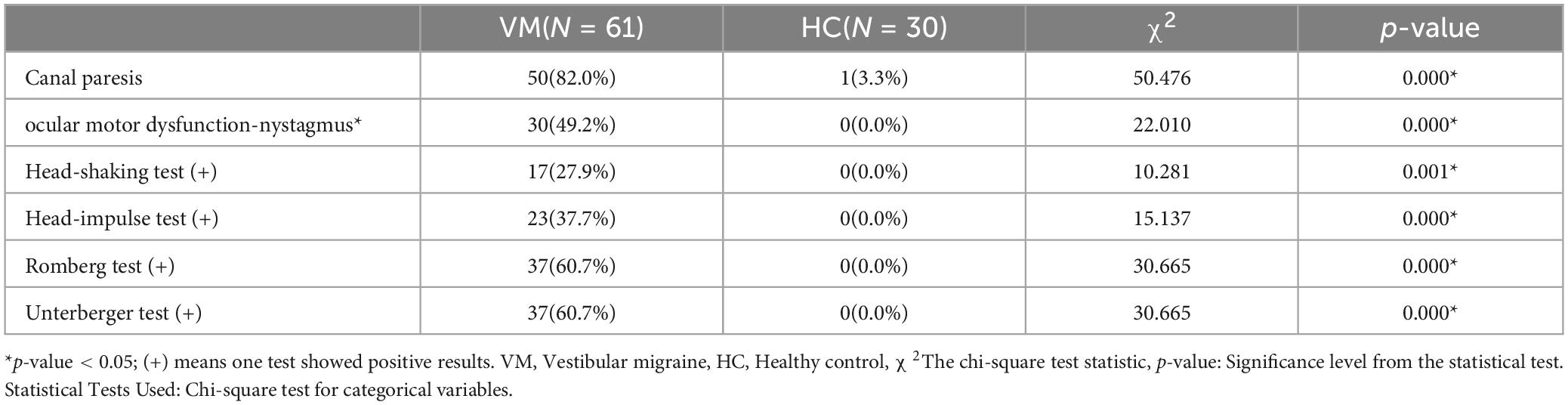
Table 9. Comparison of vestibular function between VM and HC groups.
The differences in the ACE-R total score, memory, verbal fluency, language, and visuospatial function scores between the VM group and the HC group were statistically significant (p-value < 0.05), while the differences in MMSE scores, attention, and orientation scores were not (p-value > 0.05) (Table 10). Specifically, the ACE-R total score [82 (68.5, 87)], memory score [18 (15, 24)], verbal fluency score [8 (6, 10)], language score [22 (19.5, 25)], and visuospatial functioning score [15 (12.5, 16)] in the VM group were significantly lower than those in the HC group, which had ACE-R total score [90.5 (86, 96)], memory score [24 (20, 25)], verbal fluency score [11 (9.75, 13)], language score [24 (23, 25)], and visuospatial function score [16 (14.75, 16)].
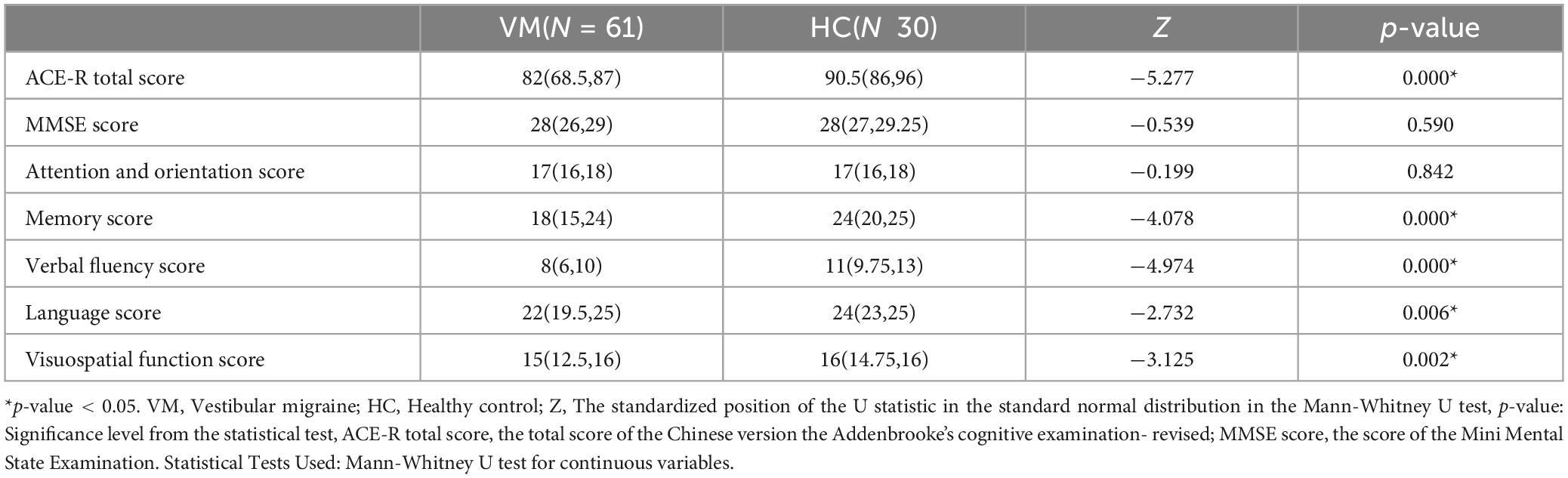
Table 10. Comparison of cognitive function between VM and HC groups.
It can be seen that only the differences in CP value (p-value = 0.000), age (p-value = 0.012), years of education (p-value = 0.016), and course of the disease (p-value = 0.045) were statistically different between the two groups, There were no statistical differences (p-value > 0.05) in sex, frequency of episodes, total DHI score, DHI-P, DHI-E, DHI-F, HADS-A, HADS-D, PHQ-9, GAD-7 scores, percentage of canal paresis and ocular motor dysfunctions, positive percentage of head-shaking test, head-impulse test, Romberg test, Unterberger test (Table 11). However, there was a significant unequal sex distribution in both groups, with a notably higher proportion of females than males. This seems to validate the observation mentioned in the introduction that VM is more common in females. Specifically, the VM-CogD group had significantly higher CP values (34.14 ± 18.051) and age [51 (40, 60)] compared to the VM-NoCogD group (CP: 12.28 ± 10.016, age: 36 (25, 57.5)). The years of education [12 (12, 15)] were significantly lower, and the disease duration [8 (5, 10)] was significantly longer in the VM-CogD group compared to the VM-NoCogD group (education: 15 (12, 16), disease duration: 5 (2, 8.5)).
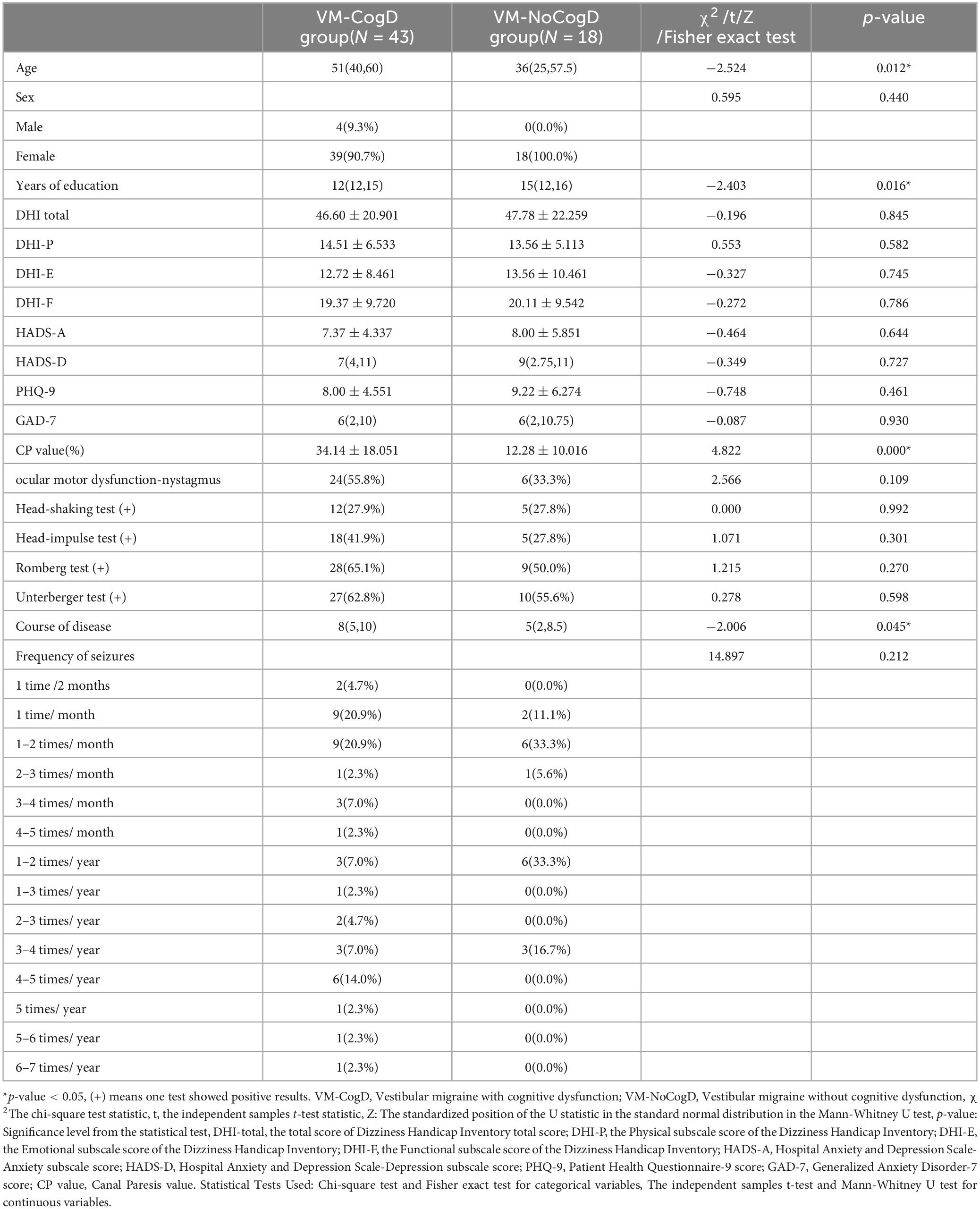
Table 11. Comparison of multiple factors between the VM-CogD and the VM-NoCogD groups.
There was a significant negative correlation between the ACE-R total score (r = −0.571, p-value = 0.000), memory (r = −0.526, p-value = 0.000), verbal fluency (r = −0.345, p-value = 0.024), language (r = −0.524, p-value = 0.000), visuospatial function (r = −0.340, p-value = 0.026) scores and the CP values (Table 12). A significant negative correlation was also observed between language (r = −0.384, p-value = 0.011) and age. Moreover, the ACE-R total score (r = 0.504, p-value = 0.001) and the language skill score (r = 0.455, p-value = 0.002) was positively correlated with years of education (Figure 4).
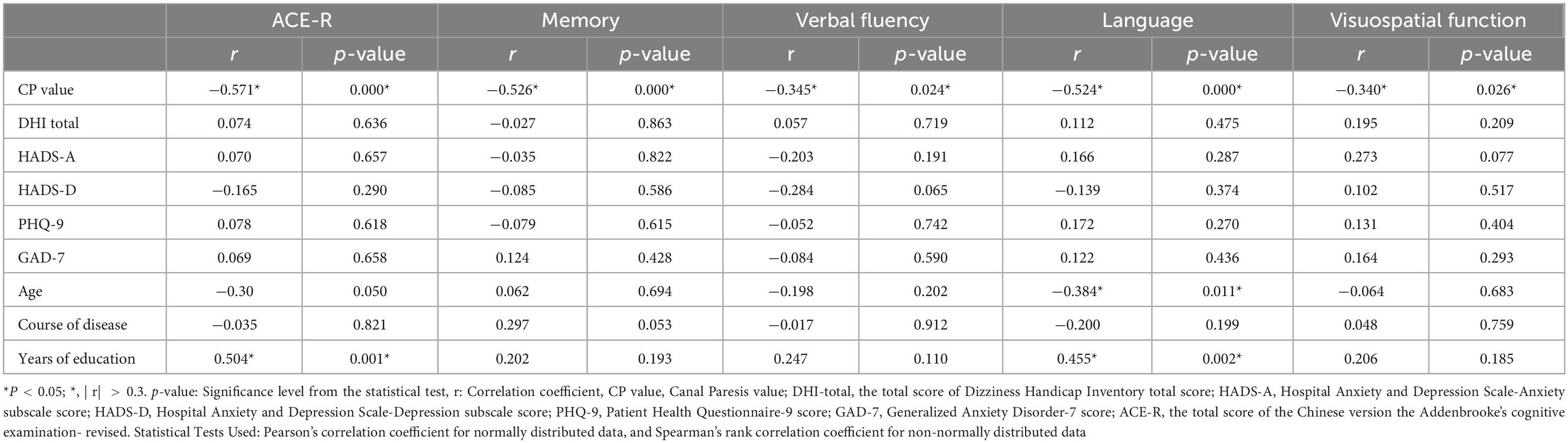
Table 12. Correlation analysis of cognitive dysfunction.
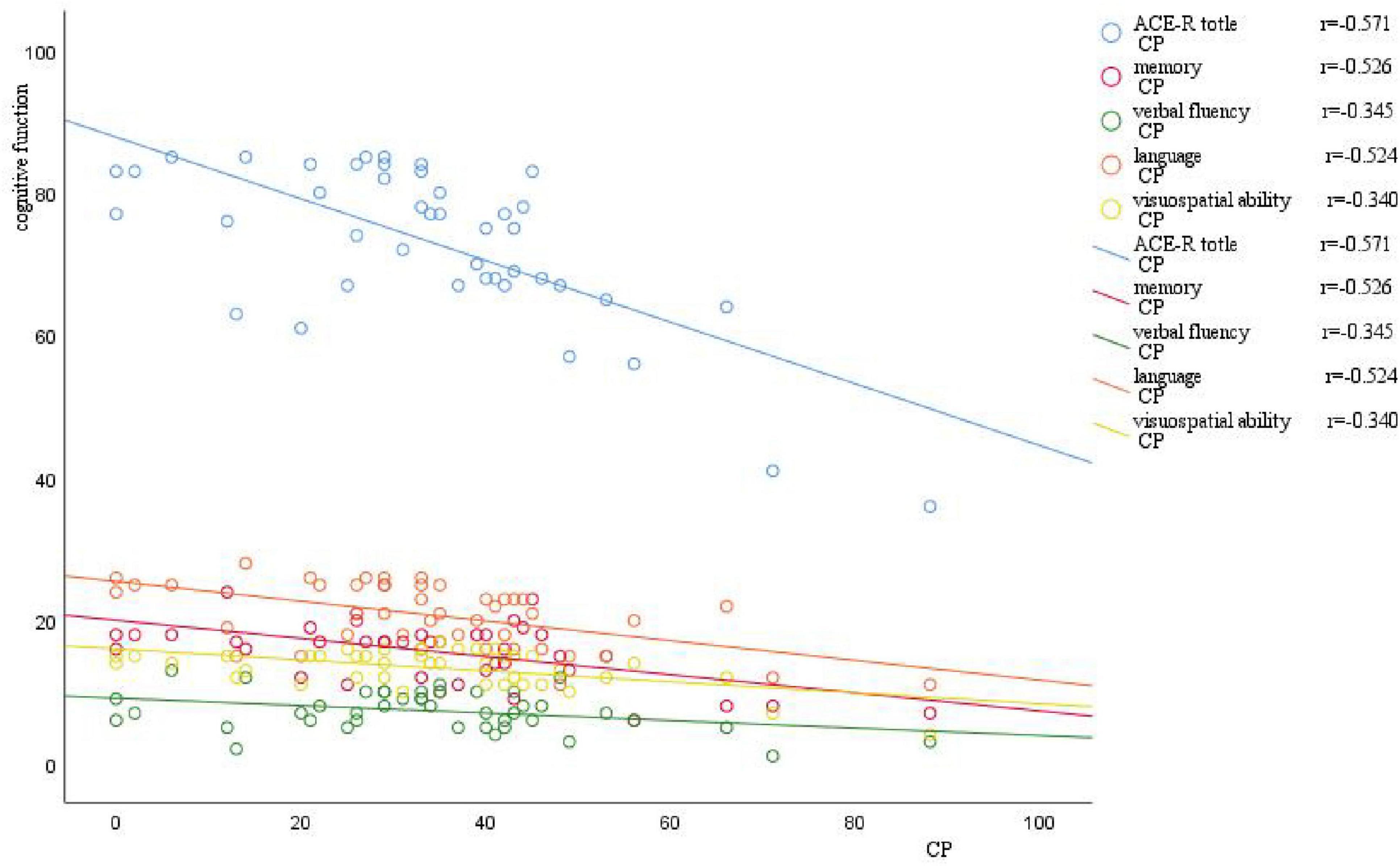
Figure 4. Scatter plot of correlation between CP value and cognitive function. The horizontal axis represents the CP value, and the vertical axis represents cognitive function. As the CP value increases, there is a varying degree of decrease in different domains of cognitive function.
We further drew ROC curves for VM-related cognitive dysfunction using CP value, age, years of education, and disease duration of VM (Figure 5) The AUC values were 0.860 (95% CI: 0.769–0.952), 0.706 (95% CI: 0.537–0.875), 0.311 (95% CI: 0.164–0.457), 0.663 (95% CI: 0.512–0.813), respectively. The corresponding p-values were 0.000, 0.012, 0.021, and 0.046. This indicated that the CP value, age, years of education, and duration of the VM disease had a certain predictive value for the cognitive dysfunction in VM, with cut-off values of 25.5, 33, 15.5, and 6.5, respectively (Table 13). Therefore, the diagnosis of VM-related cognitive dysfunction could be predicted when the CP value was greater than 25.5%, age was older than 33 years, years of education is less than 15.5 years, and disease duration of VM is longer than 6.5 years.
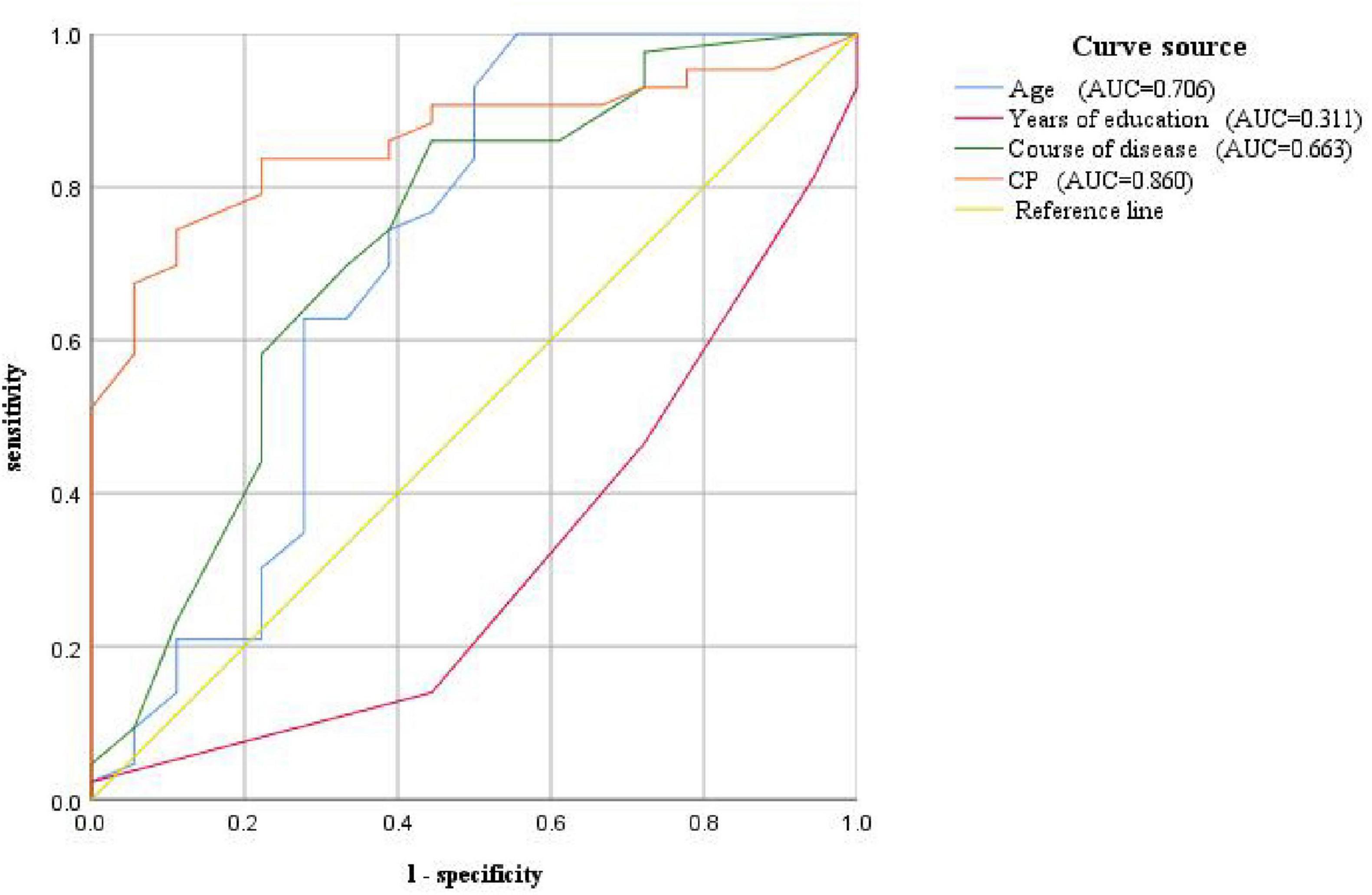
Figure 5. ROC curve for predicting VM-related cognitive impairment based on CP value, age, years of education, and disease course

Table 13. ROC curve of cognitive dysfunction related to VM diagnosis based on CP value, age, years of education, and disease course.
There was no statistically significant difference in the DHI scale and anxiety/depression scales between the VM-CogD group and the VM-NoCogD group. Further subgroup analysis based on the total DHI score in VM-CogD revealed that the majority (23) of the 43 patients with VM-CogD exhibited moderate dizziness/vertigo. Patients with moderate dizziness/vertigo showed a negative correlation between ACE-R total score and the HADS-D score (p-value = 0.047), between memory score and the DHI total score (p-value = 0.008), the DHI-E score (p-value = 0.016), the HADS-D (p-value = 0.023), between language score and the DHI-F score (p-value = 0.031), between visuospatial ability score and the DHI-F score (p-value = 0.049) (Table 14). VM patients’ cognitive function was significantly lower in those with concomitant depression, vestibular dysfunction, and more severe dizziness. The correlation between DHI, HADS, PHQ-9, and GAD-7 scores and cognitive dysfunction was lower in patients who exhibited mild and severe dizziness/vertigo (| r| < 0.3). In patients with VM-CogD, those who exhibited moderate dizziness/vertigo showed the strongest correlation between CP values and ACE-R total score. Furthermore, the CP values were negatively correlated with memory and language function in patients with moderate dizziness/vertigo and memory in patients with severe dizziness/vertigo (Tables 15, 16).
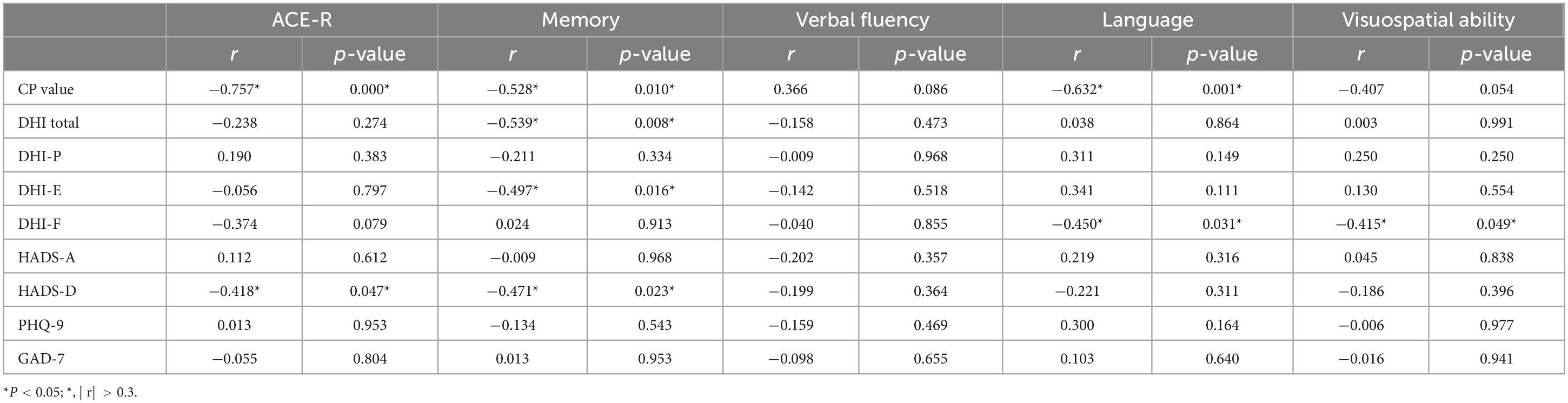
Table 14. Correlation analysis of VM-CogD presenting with moderate dizziness/vertigo.
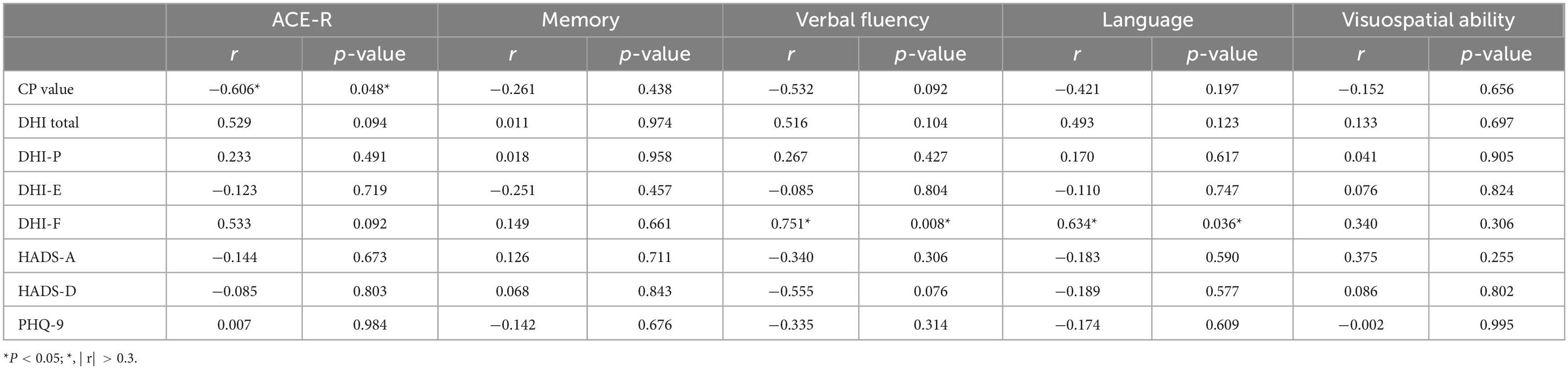
Table 15. Correlation analysis of VM-CogD presenting with mild dizziness/vertigo.
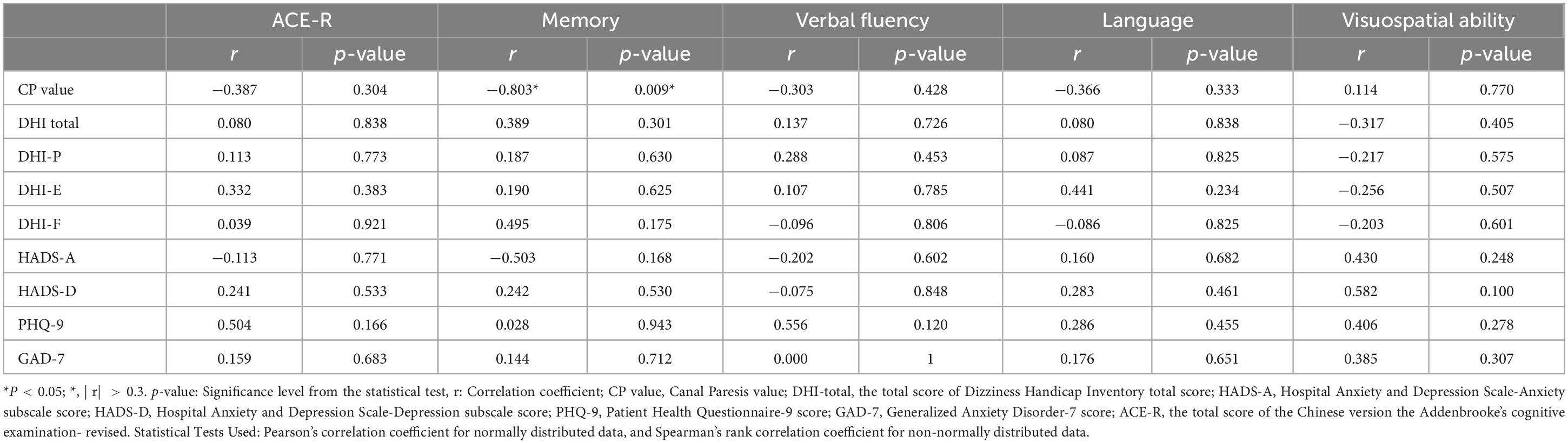
Table 16. Correlation analysis of VM-CogD presenting with severe dizziness/vertigo.
Our study found that VM, a paroxysmal vestibular disorder, involves both peripheral and central vestibular dysfunction, primarily manifesting as nystagmus and abnormalities in the caloric test, Romberg test, and Unterberger test. Although the median age of VM patients (47 years) is lower compared to Alzheimer’s Disease (AD), VM patients also exhibit cognitive dysfunction, mainly affecting visuospatial function, memory, verbal fluency, and language skill. However, the overall degree of cognitive dysfunction is relatively mild, with a median ACE-R total score of 82 out of 100(82/100). Further analysis of the factors related to VM-associated cognitive dysfunction revealed that the patient’s age, years of education, duration of VM disease, severity of vestibular dysfunction, and comorbid anxiety and depression can all influence the cognitive function of VM patients.
The caloric test is one of the main vestibular tests, alongside other important assessments. It assess the function of the bilateral horizontal semicircular canals with low-frequency stimulation, and is more sensitive to mild asymmetries in bilateral vestibular function (Mezzalira et al., 2017). CP value is a parameter generally considered for peripheral vestibular lesions, representing unilateral canal paresis (Molnár et al., 2023a). The DP value represents unilateral hyperresponse and is often used in patients with Meniere’s disease (MD), as both hypofunction and hyperfunction can occur simultaneously in this condition. Additionally, the DP value can show dynamic changes at different stages of vestibular disorders, even presenting opposite results. To ensure consistency in the results, this study only used the CP value (Lin et al., 2009). The head-shaking test is a medium-frequency stimulus, and the presence of characteristic unidirectional or bidirectional nystagmus suggests peripheral vestibular damage, and the intensity of the nystagmus can also determine the degree of vestibular compensation (Deng et al., 2023). The head-impulse test is a high-frequency stimulus. The presence of a significant catch-up saccade typically indicates an abnormality in the patient’s vestibular-ocular reflex (VOR) pathway, suggesting peripheral vestibular dysfunction (Korda et al., 2020). Romberg’s test and Unterberger’s test are based on the vestibulospinal reflex (VSR) pathway. When a patient has central vestibular lesions, these tests may reveal swaying with eyes closed and a tendency to fall or lean to one side (Halmágyi and Curthoys, 2021; Hemm et al., 2023). The combination of nystagmus test, head impulse test, and test of skew is known as the HINTS triad and is widely used to identify various acute vestibular syndromes (Kattah, 2018). Combining the HINTS triad with a bedside hearing test forms the HINTS+ test, which can effectively distinguish between acute central and peripheral vestibular lesions, particularly
in the context of posterior circulation strokes (Tarnutzer and Edlow, 2023). Alterations in the nystagmus system are numerous and complex. The advent of videonystagmography (VNG) has enabled the recording and study of subtle nystagmus that cannot be detected by the naked eye. VNG can record nystagmus caused by different lesions in the vestibular system, such as peripheral, central, or mixed (Skóra et al., 2018).
Vestibular function tests are often crucial and informative for definitive diagnosis, whether the vestibular disorder is central or peripheral. Recently, Meniere’s disease (MD) has been recognized as a cochleo-vestibular disorder rather than a mere cochlear disorder. In the early stages of MD, there is a decrease in amplitude of cervical vestibular evoked myogenic potentials (cVEMP), and in the later stages, there is a significant canal paresis in caloric testing and gain asymmetry in the video head impulse test (vHIT) (Sobhy et al., 2019). MD also presents with various ocular motor abnormalities, including spontaneous nystagmus, gaze test, saccade test, smooth pursuit, and optokinetic nystagmus in VNG. Positional nystagmus is crucial for the diagnosis of benign paroxysmal positional vertigo (BPPV), as the changes in nystagmus in different positions can identify the affected semicircular canal (Ziemska-Gorczyca et al., 2024). Additionally, patients with BPPV may exhibit abnormalities in smooth pursuit and optokinetic nystagmus. Patients with vestibular neuritis exhibit spontaneous nystagmus, which is generally horizontal-torsional, direction-fixed, and enhanced by removal of visual fixation. They also exhibit abnormal positional tests (Moideen et al., 2023) as well as lesions in the VOR and VSR pathways (Strupp et al., 2022).
Continuing research has found that vestibular disorders can manifest with cognitive impairments. The mobile tablet-based Vestibular Cognitive Assessment System (VCAS) is a system that use electronic devices to build a three-dimensional spatial structure based on cognitive questionnaires to assess visuospatial function in patients with vestibular disorders. Its tests have found that patients with vestibular dysfunction exhibit impaired spatial memory and spatial navigation function (Huang et al., 2023b). Among the above indicators reflecting vestibular function, CP value were correlated with the degree of cognitive dysfunction in VM patients. The more severe the semicircular canal damage, indicated by a higher CP value, the more severe the memory, verbal fluency, language, and visuospatial dysfunction in VM patients. Previous studies had reported a high prevalence of cognitive impairment in patients with VM and concomitant vestibular migraine and Menière’s disease (VMMD). These patients reported significantly higher frequencies of cognitive dysfunctional symptoms such as brain fog and chronic fatigue compared to those with MD alone (Chari et al., 2021). However, another study on cognitive function in VM patients reached the opposite conclusion, suggesting that the cognitive function of VM patients is normal. The latter study used the MMSE scale to assess cognitive function (Demirhan and Celebisoy, 2023). In our study, we used the ACE-R to evaluate cognitive function, which was more objective than self-reported symptoms and had higher sensitivity for mild cognitive impairment compared to the MMSE. This made our findings on cognitive impairment of VM more convincing. Other studies had evaluated immediate memory, delayed memory, language function, attention, executive function, and visuospatial abilities in VM patients and found dysfunction in all these areas. These cognitive dysfunction were also found to be correlated with latency and error frequency of anti-saccade. Our results were consistent with these findings, but our study included a more comprehensive assessment of the entire ocular motor system, recording spontaneous nystagmus, positional nystagmus, gaze-evoked nystagmus, and abnormalities in smooth pursuit (Lu et al., 2024). Liu et al. (2019) developed a new scale, the Neuro-Otologic Vestibular Instrument (NVI), to assess cognitive function in patients with vestibular disorders. They found that VM patients had cognitive dysfunction which was correlated with anxiety and depression scales. Our study also supports this finding. However, the NVI cannot be applied to healthy individuals, making it impossible to compare with them during the study. Therefore, the conclusions about the characteristics of cognitive dysfunction in VM were relatively unreliable. The experimental design of our study, which included inter-group comparisons, enhances the reliability of our conclusions (Liu et al., 2019).
How does canal paresis affect cognitive function? On one hand, it may be related to the transmission of neural pathways and the activity of brain regions. The vestibular system is a complex structure involving multiple components. The peripheral vestibular organs sense angular acceleration and linear acceleration and integrate this multisensory information, which is transmitted to the vestibular nucleus complex (VNC). The VNC integrates incoming information from vestibular, visual and proprioceptive senses, which are processed in the thalamus and cerebellum and reach the vestibular cortex, where the body responds to the information. In addition to the above structures, the VOR reflex and VSR reflex pathways are also essential for maintaining visual clarity and postural stability during movement (Aleman, 2022). The vestibular system overlaps with the cognitive system to some extent, where the vestibular cortex, thalamus, cerebellum, and basal ganglia are collectively involved in the influence of the vestibular system on cognitive functions (Hebert and Filley, 2022; Hitier et al., 2014). The vestibular cortex is a complex structure containing the cingulate gyrus, parietal cortex, hippocampus, and retrosplenial cortex. Among these, the parietal-insular vestibular cortex (PIVC) is the core structure of the vestibular cortex, which is activated to varying degrees when the vestibular system is stimulated. Various regions of the vestibular cortex have been consistently found to be involved in many processes of visuospatial function, such as the retrosplenial cortex in navigation and path integration, the anterior parietal cortex in integrating vestibular input to help distinguish self-motion from the motion of external objects, and the hippocampus in adjusting spatial orientation information in real-time via place cells, boundary cells, grid cells and head direction (HD) cells. The cerebellum and thalamus receive projections from the vestibular nerve or VNC, integration this information, and then project it to the vestibular cortex, forming a complex vestibular-cognitive network that modulates cognitive function. The basal ganglia area also receives vestibular input and participate in spatial cognitive processes. Galvanic vestibular stimulation (GVS) can affect subjects’ visuospatial function by modulating spatial representations in the hippocampus and striatum, but this modulation shows gender differences. It enhances spatial learning ability in females, and increase sensitivity to location and boundary information in males. Spatial boundary information is mostly associated with hippocampal activity, and location information is associated with striatal activity (Hilliard et al., 2019). An interesting study found that astronauts experience a diminished ability to perceive time and space, leading to incorrect estimation of time intervals and spatial distances. This spatiotemporal perception disorder is associated with the vestibular system. The vestibular system continuously integrates visual, proprioceptive, and vestibular input to accuracy of time and spatial position. The right parietal cortex, hippocampus, entorhinal cortex, which are part of the vestibular cortex are involved in the regulation of temporal and spatial cognition. In microgravity environments, the speed of the object movement decreases, and the interaction between the optokinetic stimuli and the vestibular system is reduced. In addition, microgravity reduces peripheral vestibular input, leading to functional changes in the right parietal cortex, ultimately resulting in spatiotemporal perception disorders (Navarro Morales et al., 2023).
On the other hand, it may be related to the allocation of cognitive resources. It has been proposed that the sum of an individual’s cognitive resources for vestibular and cognitive functioning is fixed. When vestibular function is impaired or the demands of vestibular tasks are increased, the body reduces its allocation of resources to cognitive functioning, resulting in varying degrees of cognitive dysfunction (Vermette et al., 2023). A recent dual-task study on patients with vestibular disorders found that when subjects were asked to complete a gait test while simultaneously executing cognitive tasks such as motor activities, calculations, and literacy, they performed poorly on the gait test. Furthermore, rapid visual information processing and paired-associate learning predicted the onset of gait deficits in subjects. Rapid visual information processing and paired-associate learning are important tests that reflect the cognitive function. The completion of vestibular task requires the coordinated use of cognitive resources, suggesting that vestibular function and cognitive processes are closely related. This relationship may be related to the fact that vestibular afferent stimuli affect the integration of information in the multisensory-motor integrating cortex of mesial temporal lobe, left posterior parietal lobe, and so on. Alzheimer’s disease (AD) is a neurodegenerative disorder characterized by progressive cognitive dysfunction. Numerous studies have found that vestibular dysfunction is more common in AD, and that loss of vestibular function increases the risk of dementia (Lim et al., 2023; Pavlou et al., 2023). The absence of bilateral cVEMPs and decreased cVEMP amplitudes are associated with an increased odds of AD (Harun et al., 2016). This may be related to the saccule mediating abnormal neuronal firing through neural pathways, leading to hippocampal atrophy, which is a pathological hallmark of AD. Based on the aforementioned findings, Huang et al. (2023a) proposed that cVEMPs may serve as a screening tool for AD. Appropriate vestibular rehabilitation exercises can improve balance and reduce fall risk in patients with cognitive impairment (Pavlou et al., 2023).
The severity of dizziness/vertigo in patients with vestibular disorders tends to correlate with the degree of cognitive dysfunction. Donaldson et al. (2021) found a negative correlation between DHI scores and scores on the Cognitive Fusion Questionnaire (CFQ) in patients with VM. Dornhoffer et al. (2021) concluded that changes in DHI scores in MD patients before and after treatment correlated with changes in CFQ scores. However, since the DHI cannot differentiate between different types of cognitive dysfunction associated with various vestibular disorders, its scores cannot currently be used as a screening tool for cognitive dysfunction (Liu et al., 2019). In our study, the average DHI score for VM patients was 46, indicating a moderate level of vertigo, which is significantly higher than that of the healthy individuals. However, we did not find a difference in DHI scores between VM-CogD group and VM-NoCogD group, which seems to indicate its limitations for the identification of cognitive dysfunction. To further investigate, we divided the VM-CogD into subgroups based on their DHI scores, categorizing them as having mild, moderate, or severe dizziness/vertigo. We then analyzed the correlation between DHI scores and cognitive dysfunction in these subgroups. We found that in the subgroup with moderate dizziness/vertigo subgroup, the functional disturbances in VM patients were associated with language and visuospatial dysfunction. This seems to suggest that VM is a functional disorder and there is potential to improve cognitive symptoms by addressing their functional abnormalities in VM patients.
The high comorbidity of affective disorders in patients with vestibular dysfunction may also contribute to the development of cognitive dysfunction. Xie et al. (2022) found that patients with dizziness/vertigo experienced more emotional problems and that anxiety and depression not only exacerbate the severity of the patient’s vertigo disorder (Feng and Zang, 2023), but also worsen the cognitive dysfunction caused by dizziness/vertigo. GAD-7 and PHQ-9 scores have been proposed as valid predictors of cognitive dysfunction in patients with vestibular dysfunction (Liu et al., 2019). In this study, among the VM patients, 35 had mild depressive disorders, 9 had moderate-to-severe depressive disorders, 25 had mild anxiety disorders, 10 had moderate-to-severe anxiety disorders. In the subgroup of VM-CogD who experience moderate dizziness/vertigo, the more depressed the patient was, the worse their memory was. Ma proposed that VM and anxiety / depression seem to be mutually influential. VM patients experience more severe anxiety and depression, and those with comorbid anxiety and depression have more severe dizziness. Anxiety and depression may contribute to the development of cognitive dysfunction in VM by affecting dizziness and sleep disorders (Ma et al., 2024). In this study, anxiety and depression were prevalent among VM patients. For example, 57% of VM patients had mild depressive disorder, 16% had moderate to severe depressive disorder, 41% had mild anxiety disorder, and 16% had moderate to severe anxiety disorder. We also found that the degree of depression was related to overall cognitive function and memory in VM-CogD with moderate dizziness/vertigo. The more severe the depression, the worse the cognitive function, particularly in memory. The correlation between emotional changes and cognitive function may be related to cognitive bias. Patients with anxiety and depression tend to focus on unpleasant or threatening information, leading to changes in the activity patterns of attention-related brain regions and a bias toward such information (Sass et al., 2014). Given the widespread comorbidity of vestibular dysfunction, cognitive impairment, and emotional abnormalities, Smith et al. (2019) proposed the concept of the “vestibular cognitive affective” syndrome, in which the vestibule is the foundation. Only by addressing the balance issues caused by vestibular dysfunction can the emotional and cognitive impairment be alleviated. The high correlation among vestibular, cognitive, and affective function may be related to a dominant hemisphere bias of the vestibular system. The greater the degree of the dominance bias, the lower the likelihood of cognitive and affective disorders (Bednarczuk et al., 2018). The molecular mechanisms may be the interactions between the vestibular system and regions involved in emotional regulation, such as the parabrachial nucleus, the locus coeruleus, and the insula, leading to changes in neurotransmitters such as 5-HT and norepinephrine (Balaban et al., 2011), ultimately leading to the comorbidity. In VM patients, venlafaxine, serotonin-norepinephrine reuptake inhibitor, significantly reduces the severity of dizziness disorders, the frequency of symptom episodes, and alleviate concomitant anxiety and depression in patients (Chen et al., 2023; Wang et al., 2020).
Our study emphasizes the following two points:
5.1 VM Patients exhibit multifaceted vestibular dysfunction and varying degrees of cognitive dysfunction, and cognitive function, is affected by age, duration of illness, years of education, and vestibular function
5.2 VM is a functional disorder, and this function disturbance in conjunction with anxiety and depression, may participate in the occurrence of the development of the cognitive dysfunction in VM.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of the First Affiliated Hospital of Harbin Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
TS: Data curation, Investigation, Writing – original draft, Writing – review and editing. YL: Data curation, Methodology, Writing – review and editing. YH: Investigation, Methodology, Writing – review and editing. YP: Funding acquisition, Project administration, Resources, Supervision, Writing – review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (Nos. 82071549 and 82371483) and the Key Research & Development Program of Heilongjiang (No. 2023ZX06C02).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aleman, M. (2022). Vestibular disease. Vet. Clin. North Am. Equine Pract. 38, 397–407. doi: 10.1016/j.cveq.2022.05.008
Arai, M., Tokumasu, K., Okamoto, M., Naganuma, H., and Hoshino, I. (1996). Optokinetic after-nystagmus in the human: A comparative study between normals and patients with peripheral vestibular and central disorders. Acta Otolaryngol. Suppl. 524, 27–32. doi: 10.3109/00016489609124344
Balaban, C. D., Jacob, R. G., and Furman, J. M. (2011). Neurologic bases for comorbidity of balance disorders, anxiety disorders and migraine: Neurotherapeutic implications. Expert Rev. Neurother. 11, 379–394. doi: 10.1586/ern.11.19
Balci, B., Şenyuva, N., and Akdal, G. (2018). Definition of balance and cognition related to disability levels in vestibular migraine patients. Noro. Psikiyatr. Ars. 55, 9–14. doi: 10.29399/npa.12617
Bednarczuk, N. F., Casanovas Ortega, M., Fluri, A. S., and Arshad, Q. (2018). Vestibulo-cortical hemispheric dominance: The link between anxiety and the vestibular system? Eur. J. Neurosci. 47, 1517–1524. doi: 10.1111/ejn.13948
Beh, S. C., Masrour, S., Smith, S. V., and Friedman, D. I. (2019). The spectrum of vestibular migraine: Clinical features, triggers, and examination findings. Headache 59, 727–740. doi: 10.1111/head.13484
Bigelow, R. T., and Agrawal, Y. (2015). Vestibular involvement in cognition: Visuospatial ability, attention, executive function, and memory. J. Vestib. Res. 25, 73–89. doi: 10.3233/VES-150544
Cao, L. X., Wang, G., Guo, Q. H., Zhang, W., Bak, T., and Huang, Y. (2022). Utility of Chinese versions of Addenbrooke’s cognitive examination: A narrative review. Healthcare 10:2052. doi: 10.3390/healthcare10102052
Çelebisoy, N., Kısabay, A. A., Özdemir, H. N., Gökçay, F., Durmaz, G. S., Kartı, D. T., et al. (2022). Vestibular migraine, demographic and clinical features of 415 patients: A multicenter study. Clin. Neurol. Neurosurg. 215:8. doi: 10.1016/j.clineuro.2022.107201
Chari, D. A., Liu, Y. H., Chung, J. J., and Rauch, S. D. (2021). Subjective cognitive symptoms and dizziness handicap inventory (DHI) performance in patients with vestibular migraine and Menière’s disease. Otol. Neurotol. 42, 883–889. doi: 10.1097/MAO.0000000000003081
Chen, J. J., Zeng, B. S., Su, K. P., Wu, Y. C., Tu, Y. K., Stubbs, B., et al. (2023). Network meta-analysis of different treatments for vestibular migraine. CNS Drugs 37, 837–847. doi: 10.1007/s40263-023-01037-0
Demirhan, M. A., and Celebisoy, N. (2023). Cognitive functions in episodic vestibular disorders: Meniere’s disease and vestibular migraine. J. Vestib. Res. 33, 63–70. doi: 10.3233/VES-220025
Deng, Q., Zhang, X., Wen, C., Liu, Q., Liu, Y., and Chen, T. (2023). [Further exploration of the classification and clinical value of head-shaking nystagmus]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 37, 473–477.
Ding, M. Y., Xu, Y., Wang, Y. Z., Li, P. X., Mao, Y. T., Yu, J. T., et al. (2019). Predictors of cognitive impairment after stroke: A prospective stroke cohort study. J. Alzheimers Dis. 71, 1139–1151. doi: 10.3233/JAD-190382
Donaldson, L. B., Yan, F., Liu, Y. F., Nguyen, S. A., and Rizk, H. G. (2021). Does cognitive dysfunction correlate with dizziness severity in patients with vestibular migraine? Am. J. Otolaryngol. 42:19. doi: 10.1016/j.amjoto.2021.103124
Dornhoffer, J. R., Liu, Y. F., Zhao, E. E., and Rizk, H. G. (2021). Does cognitive dysfunction correlate with dizziness severity in Meniére’s disease patients. Otol. Neurotol. 42, e323–e331. doi: 10.1097/MAO.0000000000002958
Eraslan Boz, H., Kırkım, G., Koçoğlu, K., Çakır Çetin, A., Akkoyun, M., Güneri, E. A., et al. (2023). Cognitive function in Meniere’s disease. Psychol. Health Med. 28, 1076–1086. doi: 10.1080/13548506.2022.2144637
Fang, R., Wang, G., Huang, Y., Zhuang, J. P., Tang, H. D., Wang, Y., et al. (2014). Validation of the Chinese version of Addenbrooke’s cognitive examination-revised for screening mild Alzheimer’s disease and mild cognitive impairment. Dement. Geriatr. Cogn. Disord. 37, 223–231. doi: 10.1159/000353541
Fei, Y., Zheng, Y., Meng, H., Li, G., Zhong, P., and Lu, J. (2021). Clinical practicality of the dizziness handicap inventory for evaluating dizziness in the Mandarin Chinese-speaking population: A prospective cross-sectional analysis. Int. J. Audiol. 60, 532–538. doi: 10.1080/14992027.2020.1839677
Feng, S., and Zang, J. (2023). The effect of accompanying anxiety and depression on patients with different vestibular syndromes. Front. Aging Neurosci. 15:1208392. doi: 10.3389/fnagi.2023.1208392
Halmágyi, G. M., and Curthoys, I. S. (2021). Vestibular contributions to the Romberg test: Testing semicircular canal and otolith function. Eur. J. Neurol. 28, 3211–3219. doi: 10.1111/ene.14942
Harun, A., Oh, E. S., Bigelow, R. T., Studenski, S., and Agrawal, Y. (2016). Vestibular impairment in dementia. Otol. Neurotol. 37, 1137–1142. doi: 10.1097/MAO.0000000000001157
Hebert, J. R., and Filley, C. M. (2022). Multisensory integration and white matter pathology: Contributions to cognitive dysfunction. Front. Neurol. 13:1051538. doi: 10.3389/fneur.2022.1051538
Hemm, S., Baumann, D., Duarte da Costa, V., and Tarnutzer, A. A. (2023). Test-re-test reliability and dynamics of the Fukuda-Unterberger stepping test. Front. Neurol. 14:1128760. doi: 10.3389/fneur.2023.1128760
Hilliard, D., Passow, S., Thurm, F., Schuck, N. W., Garthe, A., Kempermann, G., et al. (2019). Noisy galvanic vestibular stimulation modulates spatial memory in young healthy adults. Sci. Rep. 9:9310. doi: 10.1038/s41598-019-45757-0
Hitier, M., Besnard, S., and Smith, P. F. (2014). Vestibular pathways involved in cognition. Front. Integr. Neurosci. 8:59. doi: 10.3389/fnint.2014.00059
Huang, Y., Xu, J., Zhang, X., Liu, Y., and Yu, E. (2023a). Research progress on vestibular dysfunction and visual-spatial cognition in patients with Alzheimer’s disease. Front. Aging Neurosci. 15:1153918. doi: 10.3389/fnagi.2023.1153918
Huang, Y., Zhang, X., Tang, J., Xia, Y., Yang, X., Zhang, Y., et al. (2023b). Vestibular cognition assessment system: Tablet-based computerized visuospatial abilities test battery. Front. Psychol. 14:1095777. doi: 10.3389/fpsyg.2023.1095777
Hugo, J., and Ganguli, M. (2014). Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin. Geriatr. Med. 30, 421–442. doi: 10.1016/j.cger.2014.04.001
Kattah, J. C. (2018). Use of HINTS in the acute vestibular syndrome. An overview. Stroke Vasc. Neurol. 3, 190–196. doi: 10.1136/svn-2018-000160
Korda, A., Carey, J. P., Zamaro, E., Caversaccio, M. D., and Mantokoudis, G. (2020). How good are we in evaluating a bedside head impulse test? Ear. Hear. 41, 1747–1751. doi: 10.1097/AUD.0000000000000894
Koukoulithras, I., Drousia, G., Kolokotsios, S., Plexousakis, M., Stamouli, A., Roussos, C., et al. (2022). A holistic approach to a dizzy patient: A practical update. Cureus 14:e27681. doi: 10.7759/cureus.27681
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lampl, C., Rapoport, A., Levin, M., and Bräutigam, E. (2019). Migraine and episodic Vertigo: A cohort survey study of their relationship. J. Headache Pain 20:33. doi: 10.1186/s10194-019-0991-2
Lempert, T., Olesen, J., Furman, J., Waterston, J., Seemungal, B., Carey, J., et al. (2012). Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 22, 167–172. doi: 10.3233/VES-2012-0453
Lim, S. J., Son, S., Chung, Y., Kim, S. Y., Choi, H., and Choi, J. (2023). Relationship between vestibular loss and the risk of dementia using the 2002-2019 national insurance service survey in South Korea. Sci. Rep. 13:16746. doi: 10.1038/s41598-023-42598-w
Lin, P., Dong, H., Chen, T. S., Li, L., Lu, H. H., Song, W., et al. (2009). [Analysis of directional preponderance of caloric test in evaluation of vestibular dynamic compensation]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 44, 631–635.
Liu, Y. F., Locklear, T. D., Sharon, J. D., Lacroix, E., Nguyen, S. A., and Rizk, H. G. (2019). Quantification of cognitive dysfunction in dizzy patients using the neuropsychological vertigo inventory. Otol. Neurotol. 40, e723–e731. doi: 10.1097/MAO.0000000000002311
Lu, L., Ni, W., Liu, Y., Sun, L., and Li, F. (2024). Anti-saccade as a tool to evaluate cognitive impairment in vestibular migraine. Front. Neurol. 15:1419372. doi: 10.3389/fneur.2024.1419372
Ma, Y. M., Zhang, D. P., Zhang, H. L., Cao, F. Z., Zhou, Y., Wu, B., et al. (2024). Why is vestibular migraine associated with many comorbidities? J. Neurol. 20, 7422–7433. doi: 10.1007/s00415-024-12692-8
Mezzalira, R., Bittar, R. S. M., do Carmo Bilécki-Stipsky, M. M., Brugnera, C., and Grasel, S. S. (2017). Sensitivity of caloric test and video head impulse as screening test for chronic vestibular complaints. Clinics 72, 469–473. doi: 10.6061/clinics/2017(08)03
Moideen, A., Konkimalla, A., Tyagi, A. K., Varshney, S., Kumar, A., Jat, B., et al. (2023). Cross-sectional analysis of videonystagmography (VNG) findings in balance disorders. Cureus 15:e34795. doi: 10.7759/cureus.34795
Molnár, A., Jassoy, B. D., Maihoub, S., Mavrogeni, P., Tamás, L., and Szirmai, Á (2023a). Long-term follow-up of patients with vestibular neuritis by caloric testing and directional preponderance calculation. Eur. Arch. Otorhinolaryngol. 280, 1695–1701. doi: 10.1007/s00405-022-07660-9
Molnár, A., Maihoub, S., Mavrogeni, P., Krasznai, M., Tamás, L., and Kraxner, H. (2023b). The correlation between the results of the Sniffin’ sticks test, demographic data, and questionnaire of olfactory disorders in a Hungarian population after a SARS-CoV-2 infection. J. Clin. Med. 12:1041. doi: 10.3390/jcm12031041
Molnár, A., Maihoub, S., Mavrogeni, P., Tamás, L., and Szirmai, Á (2022). Depression scores and quality of life of vertiginous patients, suffering from different vestibular disorders. Eur. Arch. Otorhinolaryngol. 279, 5173–5179. doi: 10.1007/s00405-022-07366-y
Molnár, A., Maihoub, S., Tamás, L., and Szirmai, Á (2023c). Comparison between caloric and video-head impulse tests in Ménière’s disease and vestibular neuritis. Int. J. Audiol. 62, 393–399. doi: 10.1080/14992027.2022.2059711
Moser, I., Vibert, D., Caversaccio, M. D., and Mast, F. W. (2017). Acute peripheral vestibular deficit increases redundancy in random number generation. Exp. Brain Res. 235, 627–637. doi: 10.1007/s00221-016-4829-8
Navarro Morales, D. C., Kuldavletova, O., Quarck, G., Denise, P., and Clément, G. (2023). Time perception in astronauts on board the International Space Station. NPJ Micrograv. 9:6. doi: 10.1038/s41526-023-00250-x
Négrevergne, M., Ribeiro, S., Moraes, C. L., Maunsell, R., Morata, G. C., and Darrouzet, V. (2003). [Video-nystagmography and vibration test in the diagnosis of vestibular schwannoma. Review of 100 cases]. Rev. Laryngol. Otol. Rhinol. 124, 91–97.
Oh, S. Y., Nguyen, T. T., Kang, J. J., Kirsch, V., Boegle, R., Kim, J. S., et al. (2023). Visuospatial cognition in acute unilateral peripheral vestibulopathy. Front. Neurol. 14:1230495. doi: 10.3389/fneur.2023.1230495
Pavlou, M., Costafreda, S. G., Galsworthy, W., Korres, G., and Bamiou, D. E. (2023). The interplay between cognition, functional and dual-task gait in persons with a vestibular disorder versus healthy controls. Sci. Rep. 13:10130. doi: 10.1038/s41598-023-35904-z
Popp, P., Wulff, M., Finke, K., Rühl, M., Brandt, T., and Dieterich, M. (2017). Cognitive deficits in patients with a chronic vestibular failure. J. Neurol. 264, 554–563. doi: 10.1007/s00415-016-8386-7
Preysner, T. A., Gardi, A. Z., Ahmad, S., and Sharon, J. D. (2022). Vestibular migraine: Cognitive dysfunction, mobility, falls. Otol. Neurotol. 43, 1216–1221. doi: 10.1097/MAO.0000000000003700
Rizk, H. G., Sharon, J. D., Lee, J. A., Thomas, C., Nguyen, S. A., and Meyer, T. A. (2020). Cross-Sectional analysis of cognitive dysfunction in patients with vestibular disorders. Ear. Hear. 41, 1020–1027. doi: 10.1097/AUD.0000000000000825
Sass, S. M., Heller, W., Fisher, J. E., Silton, R. L., Stewart, J. L., Crocker, L. D., et al. (2014). Electrophysiological evidence of the time course of attentional bias in non-patients reporting symptoms of depression with and without co-occurring anxiety. Front. Psychol. 5:301. doi: 10.3389/fpsyg.2014.00301
Skóra, W., Stańczyk, R., Pajor, A., and Jozefowicz-Korczyńska, M. (2018). Vestibular system dysfunction in patients after mild traumatic brain injury. Ann. Agric. Environ. Med. 25, 665–668. doi: 10.26444/aaem/81138
Smith, L., Wilkinson, D., Bodani, M., Bicknell, R., and Surenthiran, S. S. (2019). Short-term memory impairment in vestibular patients can arise independently of psychiatric impairment, fatigue, and sleeplessness. J. Neuropsychol. 13, 417–431. doi: 10.1111/jnp.12157
Sobhy, O. A., Elmoazen, D. M., and Abd-Elbaky, F. A. (2019). Towards a new staging of Ménière’s disease: A vestibular approach. Acta Otorhinolaryngol. Ital. 39, 419–428. doi: 10.14639/0392-100X-2461
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Strupp, M., Bisdorff, A., Furman, J., Hornibrook, J., Jahn, K., Maire, R., et al. (2022). Acute unilateral vestibulopathy/vestibular neuritis: Diagnostic criteria. J. Vestib. Res. 32, 389–406. doi: 10.3233/VES-220201
Tarnutzer, A. A., and Edlow, J. A. (2023). Bedside testing in acute vestibular syndrome-evaluating HINTS plus and beyond-a critical review. Audiol. Res. 13, 670–685. doi: 10.3390/audiolres13050059
Taylan Cebi, I., and Karatas, A. (2022). The assessment of fukuda stepping test results in prognosis of benign paroxysmal postural vertigo. Braz. J. Otorhinolaryngol. 1(Suppl. 1), S142–S146. doi: 10.1016/j.bjorl.2021.05.005
Vermette, M. J., Prince, F., Bherer, L., and Messier, J. (2023). Concentrating to avoid falling: Interaction between peripheral sensory and central attentional demands during a postural stability limit task in sedentary seniors. Geroscience 24, 1181–1200. doi: 10.1007/s11357-023-00860-z
Wang, F., Wang, J., Cao, Y., and Xu, Z. (2020). Serotonin-norepinephrine reuptake inhibitors for the prevention of migraine and vestibular migraine: A systematic review and meta-analysis. Reg. Anesth. Pain Med. 45, 323–330. doi: 10.1136/rapm-2019-101207
Wang, N., Huang, H. L., Zhou, H., and Yu, C. Y. (2016). Cognitive impairment and quality of life in patients with migraine-associated vertigo. Eur. Rev. Med. Pharmacol. Sci. 20, 4913–4917.
Xie, D., Welgampola, M. S., Miller, L. A., Young, A. S., D’Souza, M., Breen, N., et al. (2022). Subjective cognitive dysfunction in patients with dizziness and vertigo. Audiol. Neurootol. 27, 122–132. doi: 10.1159/000518188
Yang, Y., Li, F., Pan, Y., Xie, F., Chen, J., Sun, Y., et al. (2020). [Abnormal eye movements in patients with idiopathic rapid eye movement sleep behavior disorder]. Zhejiang Da Xue Xue Bao Yi Xue Ban 49, 447–454.
Yujie, W., Bin, L., Weiqing, X., Jingwu, S., and Ruirui, G. (2018). Analysis of vestibular function in patients with vestibular migraine. J. Audiol. Speech Dis. 26, 387–391.
Zhang, Y., Liu, B., Wang, Y., Zhou, Y., Wang, R., Gong, J., et al. (2015). [Analysis of reliability and validity of the Chinese Version of Dizziness Handicap Inventory (DHI)]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 50, 738–743.
Ziemska-Gorczyca, M., Dżaman, K., Pavlovschi, D., Kantor, I., and Wojdas, A. (2024). Comparative study of clinical features of patients with different types of benign paroxysmal positional vertigo. J. Clin. Med. 13:4736. doi: 10.3390/jcm13164736
Keywords: vestibular migraine, cognitive dysfunction, vestibular function, canal paresis (CP) values, anxiety and depression
Citation: Sun T, Lin Y, Huang Y and Pan Y (2024) A preliminary clinical study related to vestibular migraine and cognitive dysfunction. Front. Hum. Neurosci. 18:1512291. doi: 10.3389/fnhum.2024.1512291
Received: 16 October 2024; Accepted: 04 December 2024;
Published: 23 December 2024.
Edited by:
Daniele Corbo, University of Brescia, ItalyReviewed by:
Jeyasakthy Saniasiaya, University of Malaya, MalaysiaCopyright © 2024 Sun, Lin, Huang and Pan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yonghui Pan, YWlndWkxOTkzQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.