 Dahna Choi
Dahna Choi Katharina Förster
Katharina Förster Nina Alexander2,3
Nina Alexander2,3 Philipp Kanske
Philipp Kanske- 1Clinical Psychology and Behavioral Neuroscience, Department of Psychology, Institute of Clinical Psychology and Psychotherapy, Technische Universität Dresden, Dresden, Germany
- 2Department of Psychiatry and Psychotherapy, University of Marburg, Marburg, Germany
- 3Center for Mind, Brain and Behavior, University of Marburg, Marburg, Germany
Empathy as one of the basic prerequisites for successful social interactions seems to be aberrant in individuals with major depressive disorder (MDD). Although understanding empathic impairments in MDD is crucial considering the frequently reported social skill deficits in patients, the current state of research is still inconclusive, pointing to both elevated and impaired levels of empathy. In this review, we extend previous reports of MDD-related aberrations in self-reported and behavioral empathy by shedding light on the neural correlates of empathy in MDD. Study findings indicate a complex and potentially state-dependent association, comprising both elevated and lower neural activity in empathy-related brain regions such as the inferior frontal gyri, bilateral anterior insulae, and cingulate areas. Predominantly, lower activity in these areas seems to be induced by antidepressant treatment or remission, with accompanying behavioral results indicating a reduced negativity-bias in empathic processing compared to acute states of MDD. We propose a preliminary model of empathy development throughout the course of the disorder, comprising initially elevated levels of empathy and a somewhat detached and lower empathic responding during the further progression of the disorder or post-treatment. The seemingly multifaceted nature of the association between empathy and MDD requires further exploration in future multimodal and longitudinal studies. The study of neural correlates of empathy in MDD should prospectively be enlarged by including further socio-affective and -cognitive capacities in MDD and related mental disorders.
1 Introduction
Being empathic toward other people is one of the basic prerequisites for successful social interactions. This is reflected in various empirical findings on empathy being linked to positive intra- and interpersonal outcomes such as relationship satisfaction and prosocial behavior (Bailey et al., 2008; Chow et al., 2013; Lehmann et al., 2022). Accordingly, lower levels of empathy show associations with psychopathological conditions, for example schizophrenia or autism spectrum disorders (Bonfils et al., 2016; Harmsen, 2019).
Emerging evidence however also points to high levels of empathy not being unconditionally adaptive: Elevated empathy at the other end of the spectrum has also been suggested to be associated with negative mental health outcomes, potentially entailing a heightened sensitivity toward negative emotions (Chikovani et al., 2015; Green et al., 2018) and an exaggerated feeling of responsibility for another's suffering (Eisenberg et al., 2024). Although withdrawing from social situations as a coping strategy might alleviate one's discomfort in a particular moment, it yields the risk of social isolation in the long run (Buruck et al., 2014; Kim and Han, 2018).
In line with these assumptions, major depressive disorder (MDD) has been discussed to be associated with and triggered by an accumulation of negative affect resulting from empathizing with others' negative emotions (Ding et al., 2023). On the contrary, other researchers suggest that patients with MDD show reduced empathy compared to healthy control participants (HCs), supposedly due to a limited affective range and affective responsiveness (Field et al., 2009).
Either way, in line with the notion of empathy to be a “double-edged sword” (Russell and Brickell, 2015) or a “risky strength” (Tone and Tully, 2014), aberrations in the sense of either an elevation or reduction of empathy yield the potential of being a relevant mechanism underlying MDD-related difficulties in social interactions (Kupferberg et al., 2016). While MDD could result from elevated empathy—mediated by heightened distress by other's negative emotions—, it could also be triggered by reduced empathy that might interfere with an individual's social functioning and maintenance of social relationships. Understanding the relevance of empathic impairments in MDD is crucial when considering that social skill deficits are thought to contribute to the chronification of the disorder due to a loss of positive social reinforcement (Libet and Lewinsohn, 1973).
In contrast to previous studies having predominantly considered self-report measures of empathy that are prone to be affected by MDD-related cognitive biases (Schreiter et al., 2013; Kupferberg et al., 2016; Yan et al., 2021), we review studies on the neural correlates of empathy in association with MDD. We thereby focus on affective empathy, which we define as the sharing of another person's emotions, yielding an isomorphic affective state in the observer (De Vignemont and Singer, 2006). Such empathic affect sharing paves the way for differential functional outcomes: While it can result in adaptive, caring responses toward another person—also termed compassion—, it can also trigger empathic distress as a more self-oriented and aversive reaction (Singer and Klimecki, 2014). Affective empathy is to be distinguished from more cognitive aspects of empathy or Theory of Mind, comprising the ability to infer and reason about others' beliefs, thoughts, or emotions (Frith and Frith, 2005). Although affective and cognitive processes are likely to co-occur in naturalistic social situations, considering affective or cognitive empathy separately is required as a first step toward understanding their interplay with MDD. The differentiability between affective and cognitive routes of understanding others additionally shows in their neural distinctiveness: The bilateral anterior insulae (AI), inferior frontal gyri (IFG), and cingulate areas show associations with affective empathy, whilst brain areas related to cognitive empathy comprise the medial prefrontal cortex, middle temporal gyrus, and precuneus (Lamm et al., 2011; Kanske, 2018; Schurz et al., 2021).
Here, we summarize findings on aberrant empathy-related neural correlates in MDD patients at different disorder states and review changes after remission and treatment. Based on these findings, we propose a preliminary model of a state-dependent associational shift between empathy and MDD, which describes elevated levels of empathy before and during acute MDD and reduced empathy after remission and antidepressant treatment. Since socio-affective and -cognitive processes might not be readily tangible to the social agents, by elucidating the underlying neural mechanisms, we aim to provide new insights into the complex interplay between empathy and MDD.
2 Neural correlates of aberrant empathy at different states of MDD
Two studies on empathy for pain provided first indications on aberrations in empathy-related neural activity at different states of MDD. In Fujino et al.'s (2014) study, individuals with acute MDD and HCs were presented with videos showing painful and non-painful situations and were subsequently instructed to rate the pain intensity of the videos. Analyses revealed individuals with MDD to show less task-related neural activity in the left middle cingulate cortex (MCC) and somatosensory-related cortices—namely, the supramarginal gyrus and postcentral gyrus—, but elevated activity in the left IFG. On a self-report level, MDD patients indicated lower subjective pain ratings compared to HCs.
Based on prior studies on the MCC's and somatosensory-related cortices' functional implications and in accordance with lower self-reported pain ratings, the authors suggested inhibited activity in those brain regions to reflect reduced empathic processing in patients with MDD (Jackson et al., 2005). In contrast, considering the IFG's association with the regulation of negative emotions (Johnstone et al., 2007) and self-reported empathic distress (Saarela et al., 2006), elevated IFG activity might add to previous indications on higher empathic distress in MDD (Schneider et al., 2012).
While in Fujino et al.'s (2014) study, no inferences can be made on the associations between these neural aberrations and participants' disorder state, insights into the latter are provided in Rütgen et al.'s study from 2021: In an fMRI task, patients with acute MDD, remitted MDD patients, and HCs watched videos showing targets, alleged tinnitus patients, undergoing a painful noise treatment. Participants were then asked to rate the degree of unpleasantness that they thought the target person would feel (target unpleasantness rating), and the degree of unpleasantness for themselves when empathizing (self-experienced unpleasantness rating). fMRI analyses revealed that remitted MDD patients showed elevated activity in the right temporoparietal junction (TPJ) compared to patients with acute MDD and HCs. In the same group contrasts, remitted patients showed lower activity in areas associated with the processing of emotions and emotional facial expressions, such as the left visual association cortex, bilateral amygdalae, and the left AI. On a self-report level, remitted patients indicated higher ratings of target unpleasantness ratings compared to patients with acute MDD and HCs, while self-unpleasantness ratings were similar across all groups.
The authors interpret their findings as reflecting remitted MDD patients to cognitively anticipate more pain for the other and to show a higher self-other distinction reflected in elevated TPJ activity (Quesque and Brass, 2019; Borja Jimenez et al., 2020). Importantly, not only the stratification of the investigated sample based on disorder state but also the simultaneous assessment of the affective and cognitive processing of another's pain—measured in self-experienced and target unpleasantness ratings, respectively—provide a differential view on the association between empathy and MDD.
Although interpretations are preliminary, these studies indicate fluctuations in the association between empathy and MDD depending on the current disorder state. Elevated TPJ activity in remitted MDD might be reflective of elevated self-other distinction and higher cognitive empathic processing, which has meta-analytically shown to be one of the TPJ's major functional associations (Krall et al., 2015). Potentially, this might pose a learned compensatory mechanism counteracting elevated empathic distress at acute states of MDD. The generalizability of these findings on empathy for mere pain exposure to natural empathy-evoking situations as well as their longer-term implications require further investigation in future studies.
3 Treatment effects on neural correlates of empathy in MDD
Further studies on neural correlates of empathy in MDD provide important indications of a mediating role of empathy in mechanisms underlying symptom improvement after antidepressant treatment. In a study on empathy for pain from Rütgen et al. (2019) in which the same empathy for pain task was conducted as described above (Rütgen et al., 2021), HCs and patients with acute MDD performed the fMRI task before and 3 months after patients underwent antidepressant treatment.
Whilst no pre-treatment behavioral nor neural group differences were evident, after antidepressant treatment, MDD patients showed decreased neural activity in bilateral AI and the anterior MCC, as well as reduced self-experienced unpleasantness ratings compared to their pre-treatment responses and compared to HCs. Lower self-reported unpleasantness ratings in MDD patients moreover correlated with symptom improvement after treatment. These findings provide important indications of reduced affective processing of negative social information induced by antidepressant treatment, which is reflected in lower activity in empathy-related brain regions (Rütgen et al., 2019).
Although these interpretations are preliminary due to the data being correlational, further support is provided in two deep-brain stimulation (DBS) studies on patients with treatment-resistant MDD. In Merkl et al.'s (2016) study, oscillatory response patterns during the presentation of an empathy task (Dziobek et al., 2011) and the modulation of behavioral responses after 6 months of DBS were investigated. Patients underwent DBS in the subgenual anterior cingulate cortex (sgACC), as the sgACC has been shown to be a promising target for DBS in treatment-resistant MDD (Mayberg et al., 2005). Before DBS, patients compared to HCs showed higher negative versus positive affective sharing which was associated with enhanced beta-band desynchronization in the sgACC. This desynchronization correlated with self-reported severity of depressive symptoms. After 6 months of DBS, patients showed normalized empathic responses in the sense of no differences between empathic involvement ratings for persons who depicted negative emotions versus for those who depicted positive emotions. As neural oscillations are a crucial mechanism for coordinated neural functioning (Buzsáki and Draguhn, 2004) and as DBS has been shown to successfully suppress disruptive pathological oscillatory activity (Eusebio et al., 2011), these findings might be reflective of sgACC DBS improving clinical symptoms in MDD. Considering that the reduction of empathic affect sharing with negative stimuli showed a tendency to correlate with symptom improvement, these findings further support the notion of a mental-health-promoting effect of reduced empathic involvement with negative emotions in MDD.
In a similar vein, Kilian et al. (2024) applied DBS to the supero-lateral medial forebrain bundle (slMFB) in patients with treatment-resistant MDD and HCs. As the slMFB shows overlaps with neural correlates of socio-affective and -cognitive capacities and, as a connecting structure of the mesolimbic pathway, induces brain metabolism changes not only in the stimulated area but also distal to it, authors have pointed out the plausibility of slMFB DBS to modulate social affect. Before and 3 months after DBS, participants performed a task in which they were presented with naturalistic video stimuli of narrators presenting allegedly autobiographic stories that were either emotional or neutral in valence. Based on subjective ratings of affective valence, compassion, and answers to a multiple-choice question on the content of the video, not only affective empathy, but also related constructs of cognitive empathy and compassion were enquired (Kanske et al., 2015, 2016). While before DBS, affective empathy significantly differed between HCs and patients with MDD, these differences were not evident after 3 months of DBS. This effect was driven by changes from baseline to follow-up in the MDD group: Specifically, a reduced negativity bias in their affect ratings after watching neutrally valenced stimuli was observed. The supposedly normalized affective responsiveness in patients was accompanied by lower levels of self-reported depressive symptoms. No treatment effects occurred regarding persistingly lower levels of compassion and intact socio-cognitive skills in patients versus HCs both pre- and post-DBS.
Pointing out the anatomical and functional coupling between the slMFB and the sgACC, the authors suggest their findings together with Merkl et al.'s (2016) findings to show a network-specific effect of DBS in MDD. The suggested relevance of DBS-induced normalized affective responsiveness for long-term antidepressant effects is to be further investigated, as well as preliminary indications in Kilian et al.'s (2024) study on the specific malleability of affective empathy compared to other socio-affective and -cognitive functions. Importantly, these DBS studies do not only support the notion of reduced empathic responding to contribute to symptom improvement in MDD but moreover allow for a more detailed insight into the specific nature of aberrations revealing MDD-related negativity biases in empathic responding (see Figure 1 for overview of reviewed findings).
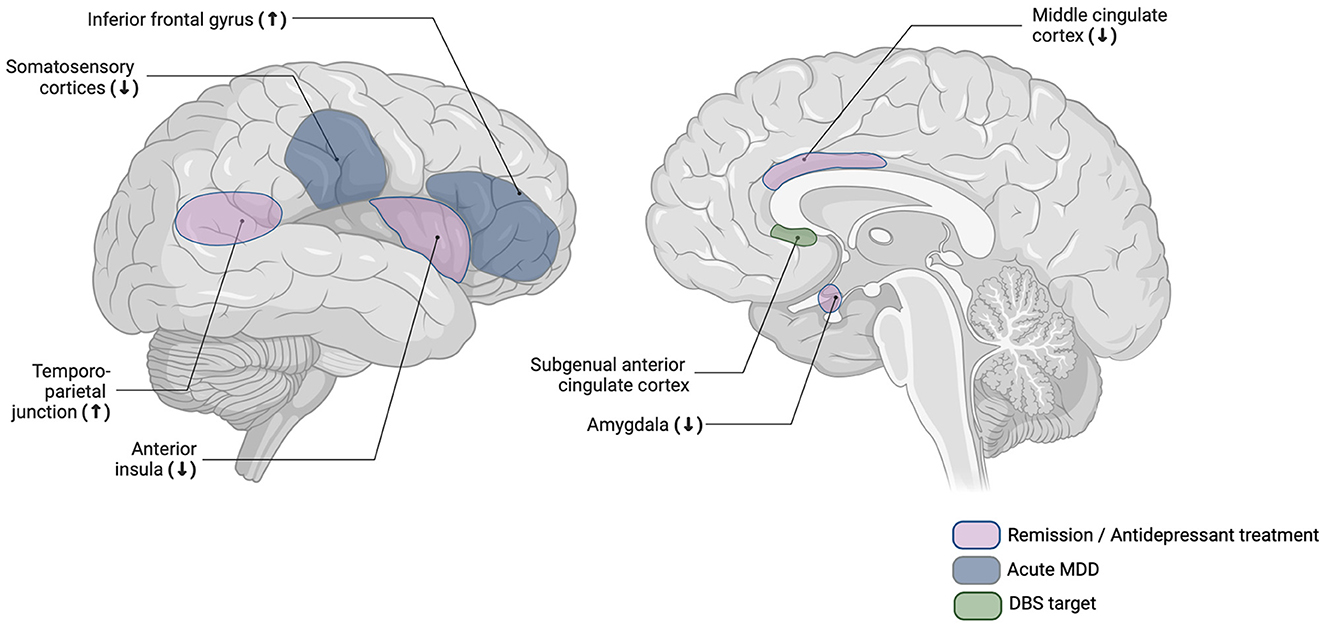
Figure 1. Schematic overview of brain regions that have been reported to show aberrant activity in acute MDD or after remission or antidepressant treatment. DBS, deep brain stimulation; MDD, major depressive disorder.
4 A proposed model of associational shifts between empathy and MDD throughout the course of the disorder
While the studies' heterogeneity renders the aggregation of findings challenging, it also provides important insights insights into a complex and potentially state-dependent association between MDD and empathy. Although preliminary, we suggest the neural activity findings to reflect a differential association between empathy and MDD depending on the state of the disorder and treatment effects. While elevated neural activity in empathy-related brain areas during acute symptomatology might reflect elevated empathic distress (Fujino et al., 2014)—also in accordance with findings on elevated self-reported empathy in MDD (Schreiter et al., 2013)—antidepressant treatment or remission might dampen empathic reactions toward negative stimuli. This notion is reflected in lower activity in empathy-related brain areas such as the AI and MCC after remission or antidepressant treatment compared to pretreatment or acute episodes, and is further supported in lower self-reports of affective empathy (Merkl et al., 2016; Rütgen et al., 2019; Kilian et al., 2024).
Conceivably, this associational shift might reflect a coping mechanism in the aftermath of elevated empathy in MDD, fostering compensatory, more detached empathic responding. The finding of elevated TPJ activity in patients with remitted compared to acute MDD and HCs could potentially indicate a mechanism enabling this dampened empathy: As the TPJ has been associated with higher self-other distinction and more cognitive aspects of empathy (Schurz et al., 2021), an elevated cognitive processing of others' negative emotions might enable individuals to be less overwhelmed by another's negative emotion and thereby counteract the MDD-related proneness to show empathic distress. It, thus, acts as a possible way to regulate difficult emotions, which bears importance given the described emotion regulation deficits in MDD (Kanske et al., 2012; Joormann and Quinn, 2014).
This suggested associational shift however requires further investigation in future longitudinal studies. Moreover, longer term implications of dampened empathic responding should be investigated, potentially yielding the risk of lower opportunities for rewarding social interactions in the long run (Trew, 2011; see Figure 2 for schematic depiction of proposed model).
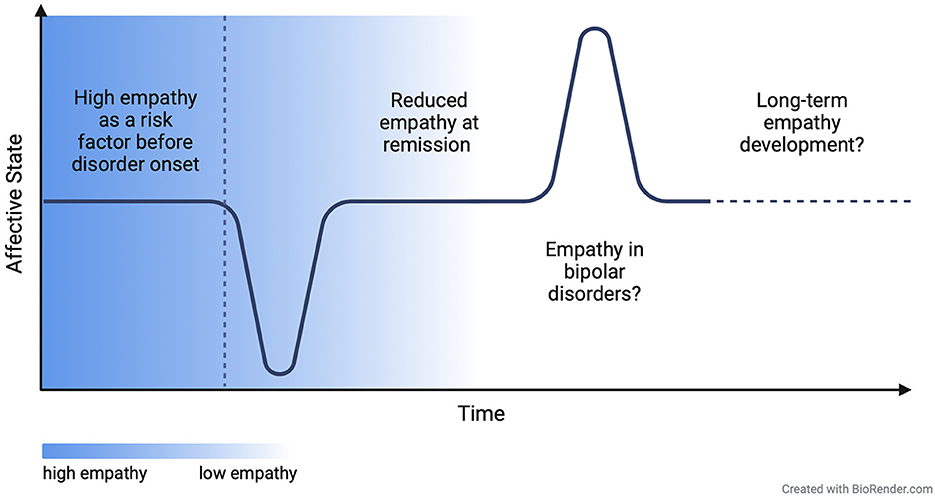
Figure 2. Proposed model of associational shift between empathy and affective symptoms throughout the course of the disorder.
5 Outlook
Since empathic responding does not evolve in a vacuum but is most probably significantly influenced in its emergence and outcomes depending on a specific composition of various moderators, future studies should take those moderators into consideration. Further affective and cognitive mechanisms that might come into play in real life social interactions and should be amongst others comprise cognitive empathy, emotion regulation (Tully et al., 2016; Guendelman et al., 2022), or executive functioning (Thoma et al., 2011).
Particularly neural correlates of cognitive empathy should be integrated in future studies due to their potentially interacting effects with affective empathy on the emergence of MDD. Importantly, a well-regulated interplay between cognitive and affective mechanisms has been suggested to show the most adaptive outcomes by allowing for understanding another's emotions and being affectively involved without becoming overwhelmed (Tully et al., 2016; Calandri et al., 2019). Since empathy can be constrained by information-processing biases channeling certain environmental input, cognitive empathy could be crucial to reduce these biases (Decety, 2021). Building upon previous findings on cross-network interactions during socio-affective and -cognitive processing (Schurz et al., 2020), research on potential changes in these interactions throughout the course of MDD could be of particular relevance.
Lastly, in order to elucidate the time-wise dynamics in the association between empathy and MDD, future studies should apply longitudinal approaches, that furthermore not only include patients with acute MDD and remitted MDD but also at-risk individuals before disorder onset. Based on this study design, it is to be investigated whether altered empathy is the antecedent or the consequence of MDD: While aberrations in empathy might be a vulnerability factor before the onset of MDD, depressive symptoms may heighten the emotional sensitivity toward others' emotions and alter an individual's empathic responding even after remission (Schreiter et al., 2013). Interestingly, Ding et al. (2023) have provided first longitudinal evidence on bidirectional positive associations between of empathy and depressive symptoms. Since their analyses were based on self-reports of empathy only, further research including neural activity data might yield relevant insights into the underlying mechanisms. Taken together, we suggest future studies to provide multimodal, longitudinal designs on stratified samples, ideally comprising affective as well as cognitive measures of empathy.
6 Clinical implications
From a clinical point of view, our findings add to previous indications of the efficacy of reversing the negativity bias in antidepressant treatment (Harmer et al., 2009; Rottenberg and Hindash, 2015) and extend its relevance to respective biases in affective empathy. It is still to be investigated whether this bias can be replicated for MDD specifically, or whether it might show the potential as a transdiagnostic marker of aberrant social affect for various mental disorders. Considering previously reported mood-congruent processing biases (Leppänen, 2006; Sterzer et al., 2011), extending investigations to potentially diverging biases in bipolar disorders might contribute to our clinical understanding of those mental disorders.
On a more general note, the consistency in results on elevated empathy to be associated with depressive symptoms highlight the relevance of adopting a critical perspective on the mental health impacts of fostering socio-affective and -cognitive capacities. Emerging indications of moderate levels of empathy to show the most adaptive outcomes (Tully et al., 2016) should find consideration in our notion of desirable social affect and cognition in social interactions and accordingly adjusted psychoeducation in clinical settings.
7 Conclusion
In this review, we have shed light on the complex relationship between MDD and neural correlates of affective empathy. Patients with MDD compared to HCs show seemingly state-dependent neural aberrations during empathic processing. Predominately post-treatment or after remission, lower empathy-related activity has been found in brain regions such as the AI, IFG, and cingulate areas, partly accompanied by reductions in subjective negative empathic affect sharing. Further longitudinal and multimodal research is required to test the suggested state-dependent associational shift between empathy and MDD. Prospectively, this might provide a more informative basis for psychotherapeutical interventions targeting aberrant social affect in various psychopathological conditions.
Author contributions
DC: Conceptualization, Writing – original draft. KF: Writing – review & editing. NA: Writing – review & editing. PK: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported in part by the SFB/TRR 393 consortium from the German Research Foundation (DFG), projects B05, C01 and C03. DC has received funding from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) grant number: GRK2773/1-454245598.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bailey, P. E., Henry, J. D., and Von Hippel, W. (2008). Empathy and social functioning in late adulthood. Aging Mental Health 12, 499–503. doi: 10.1080/13607860802224243
Bonfils, K. A., Lysaker, P. H., Minor, K. S., and Salyers, M. P. (2016). Affective empathy in schizophrenia: a meta-analysis. Schizophr. Res. 175, 109–117. doi: 10.1016/j.schres.2016.03.037
Borja Jimenez, K. C., Abdelgabar, A. R., De Angelis, L., McKay, L. S., Keysers, C., and Gazzola, V. (2020). Changes in brain activity following the voluntary control of empathy. NeuroImage 216:116529. doi: 10.1016/j.neuroimage.2020.116529
Buruck, G., Wendsche, J., Melzer, M., Strobel, A., and Dörfel, D. (2014). Acute psychosocial stress and emotion regulation skills modulate empathic reactions to pain in others. Front. Psychol. 5:517. doi: 10.3389/fpsyg.2014.00517
Buzsáki, G., and Draguhn, A. (2004). Neuronal oscillations in cortical networks. Science 304, 1926–1929. doi: 10.1126/science.1099745
Calandri, E., Graziano, F., Testa, S., Cattelino, E., and Begotti, T. (2019). Empathy and depression among early adolescents: the moderating role of parental support. Front. Psychol. 10:1447. doi: 10.3389/fpsyg.2019.01447
Chikovani, G., Babuadze, L., Iashvili, N., Gvalia, T., and Surguladze, S. (2015). Empathy costs: negative emotional bias in high empathisers. Psychiat. Res. 229, 340–346. doi: 10.1016/j.psychres.2015.07.001
Chow, C. M., Ruhl, H., and Buhrmester, D. (2013). The mediating role of interpersonal competence between adolescents' empathy and friendship quality: a dyadic approach. J. Adolesc. 36, 191–200. doi: 10.1016/j.adolescence.2012.10.004
De Vignemont, F., and Singer, T. (2006). The empathic brain: how, when and why? Trends Cogn. Sci. 10, 435–441. doi: 10.1016/j.tics.2006.08.008
Decety, J. (2021). Why empathy is not a reliable source of information in moral decision making. Curr. Dir. Psychol. Sci. 30, 425–430. doi: 10.1177/09637214211031943
Ding, D., Tan, X., Sun, L., Zeng, X., and Yan, Z. (2023). Does empathy lead to depression? A three-wave random intercept cross-lagged panel analysis in emerging adults. Curr. Psychol. 23:6. doi: 10.1007/s12144-023-05224-6
Dziobek, I., Preißler, S., Grozdanovic, Z., Heuser, I., Heekeren, H. R., and Roepke, S. (2011). Neuronal correlates of altered empathy and social cognition in borderline personality disorder. NeuroImage 57, 539–548. doi: 10.1016/j.neuroimage.2011.05.005
Eisenberg, N., Zuffian,ò, A., and Spinrad, T. L. (2024). Are prosocial tendencies relevant for developmental psychopathology? The relations of prosocial behavior and empathy-related responding to externalizing problems, internalizing problems, and autism spectrum disorder. Dev. Psychopathol. 63, 1–11. doi: 10.1017/S0954579424000063
Eusebio, A., Thevathasan, W., Doyle Gaynor, L., Pogosyan, A., Bye, E., Foltynie, T., et al. (2011). Deep brain stimulation can suppress pathological synchronisation in parkinsonian patients. J. Neurol. Neurosurg. Psychiat. 82, 569–573. doi: 10.1136/jnnp.2010.217489
Field, T., Diego, M., and Hernandez-Reif, M. (2009). Depressed mothers' infants are less responsive to faces and voices. Infant Behav. Dev. 32, 239–244. doi: 10.1016/j.infbeh.2009.03.005
Frith, C., and Frith, U. (2005). Theory of mind. Curr. Biol. 17, R644–R646. doi: 10.1016/j.cub.2005.08.041
Fujino, J., Yamasaki, N., Miyata, J., Kawada, R., Sasaki, H., Matsukawa, N., et al. (2014). Altered brain response to others? pain in major depressive disorder. J. Affect. Disord. 165, 170–175. doi: 10.1016/j.jad.2014.04.058
Green, L. M., Missotten, L., Tone, E. B., and Luyckx, K. (2018). Empathy, depressive symptoms, and self-esteem in adolescence: the moderating role of the mother-adolescent relationship. J. Child Fam. Stud. 27, 3964–3974. doi: 10.1007/s10826-018-1216-z
Guendelman, S., Bayer, M., Prehn, K., and Dziobek, I. (2022). Regulating negative emotions of others reduces own stress: neurobiological correlates and the role of individual differences in empathy. NeuroImage 254:119134. doi: 10.1016/j.neuroimage.2022.119134
Harmer, C. J., O'Sullivan, U., Favaron, E., Massey-Chase, R., Ayres, R., Reinecke, A., et al. (2009). Effect of acute antidepressant administration on negative affective bias in depressed patients. AJP 166, 1178–1184. doi: 10.1176/appi.ajp.2009.09020149
Harmsen, I. E. (2019). Empathy in autism spectrum disorder. J. Autism Dev. Disord. 49, 3939–3955. doi: 10.1007/s10803-019-04087-w
Jackson, P. L., Meltzoff, A. N., and Decety, J. (2005). How do we perceive the pain of others? A window into the neural processes involved in empathy. NeuroImage 24, 771–779. doi: 10.1016/j.neuroimage.2004.09.006
Johnstone, T., Van Reekum, C. M., Urry, H. L., Kalin, N. H., and Davidson, R. J. (2007). Failure to regulate: counterproductive recruitment of top-down prefrontal-subcortical circuitry in major depression. J. Neurosci. 27, 8877–8884. doi: 10.1523/JNEUROSCI.2063-07.2007
Joormann, J., and Quinn, M. E. (2014). Cognitive processes and emotion regulation in depression: review: cognitive processes in depression. Depr. Anxiety 31, 308–315. doi: 10.1002/da.22264
Kanske, P. (2018). The social mind: disentangling affective and cognitive routes to understanding others. Interdiscipl. Sci. Rev. 43, 115–124. doi: 10.1080/03080188.2018.1453243
Kanske, P., Böckler, A., Trautwein, F.-M., Parianen Lesemann, F. H., and Singer, T. (2016). Are strong empathizers better mentalizers? Evidence for independence and interaction between the routes of social cognition. Soc. Cogn. Affect. Neurosci. 11, 1383–1392. doi: 10.1093/scan/nsw052
Kanske, P., Böckler, A., Trautwein, F. M., and Singer, T. (2015). Dissecting the social brain: introducing the EmpaToM to reveal distinct neural networks and brain-behavior relations for empathy and Theory of Mind. NeuroImage 122, 6–19. doi: 10.1016/j.neuroimage.2015.07.082
Kanske, P., Heissler, J., Schönfelder, S., and Wessa, M. (2012). Neural correlates of emotion regulation deficits in remitted depression: the influence of regulation strategy, habitual regulation use, and emotional valence. NeuroImage 61, 686–693. doi: 10.1016/j.neuroimage.2012.03.089
Kilian, H. M., Schiller, B., Meyer-Doll, D. M., Heinrichs, M., and Schläpfer, T. E. (2024). Normalized affective responsiveness following deep brain stimulation of the medial forebrain bundle in depression. Transl. Psychiatry 14:6. doi: 10.1038/s41398-023-02712-y
Kim, H., and Han, S. (2018). Does personal distress enhance empathic interaction or block it? Personal. Individ. Differ. 124, 77–83. doi: 10.1016/j.paid.2017.12.005
Krall, S. C., Rottschy, C., Oberwelland, E., Bzdok, D., Fox, P. T., Eickhoff, S. B., et al. (2015). The role of the right temporoparietal junction in attention and social interaction as revealed by ALE meta-analysis. Brain Struct. Funct. 220, 587–604. doi: 10.1007/s00429-014-0803-z
Kupferberg, A., Bicks, L., and Hasler, G. (2016). Social functioning in major depressive disorder. Neurosci. Biobehav. Rev. 69, 313–332. doi: 10.1016/j.neubiorev.2016.07.002
Lamm, C., Decety, J., and Singer, T. (2011). Meta-analytic evidence for common and distinct neural networks associated with directly experienced pain and empathy for pain. NeuroImage 54, 2492–2502. doi: 10.1016/j.neuroimage.2010.10.014
Lehmann, K., Böckler, A., Klimecki, O., Müller-Liebmann, C., and Kanske, P. (2022). Empathy and correct mental state inferences both promote prosociality. Sci. Rep. 12:16979. doi: 10.1038/s41598-022-20855-8
Leppänen, J. M. (2006). Emotional information processing in mood disorders: a review of behavioral and neuroimaging findings. Curr. Opin. Psychiat. 19, 34–39. doi: 10.1097/01.yco.0000191500.46411.00
Libet, J., and Lewinsohn, P. (1973). Concept of social skill with special reference to the behavior of depressed persons. J. Consult. Clin. Psychol. 40, 304–312. doi: 10.1037/h0034530
Mayberg, H. S., Lozano, A. M., Voon, V., McNeely, H. E., Seminowicz, D., Hamani, C., et al. (2005). Deep brain stimulation for treatment-resistant depression. Neuron 45, 651–660. doi: 10.1016/j.neuron.2005.02.014
Merkl, A., Neumann, W.-J., Huebl, J., Aust, S., Horn, A., Krauss, J. K., et al. (2016). Modulation of beta-band activity in the subgenual anterior cingulate cortex during emotional empathy in treatment-resistant depression. Cereb. Cortex 26, 2626–2638. doi: 10.1093/cercor/bhv100
Quesque, F., and Brass, M. (2019). The role of the temporoparietal junction in self-other distinction. Brain Topogr. 32, 943–955. doi: 10.1007/s10548-019-00737-5
Rottenberg, J., and Hindash, A. C. (2015). Emerging evidence for emotion context insensitivity in depression. Curr. Opin. Psychol. 4, 1–5. doi: 10.1016/j.copsyc.2014.12.025
Russell, M., and Brickell, M. (2015). The “double-edge sword” of human empathy: a unifying neurobehavioral theory of compassion stress injury. Soc. Sci. 4, 1087–1117. doi: 10.3390/socsci4041087
Rütgen, M., Pfabigan, D. M., Tik, M., Kraus, C., Pletti, C., Sladky, R., et al. (2021). Detached empathic experience of others' pain in remitted states of depression—an fMRI study. NeuroImage 31:102699. doi: 10.1016/j.nicl.2021.102699
Rütgen, M., Pletti, C., Tik, M., Kraus, C., Pfabigan, D. M., Sladky, R., et al. (2019). Antidepressant treatment, not depression, leads to reductions in behavioral and neural responses to pain empathy. Transl. Psychiatry 9:164. doi: 10.1038/s41398-019-0496-4
Saarela, M. V., Hlushchuk, Y., Williams, A. C. D. C., Schurmann, M., Kalso, E., and Hari, R. (2006). The compassionate brain: humans detect intensity of pain from another's face. Cerebr. Cortex 17, 230–237. doi: 10.1093/cercor/bhj141
Schneider, D., Regenbogen, C., Kellermann, T., Finkelmeyer, A., Kohn, N., Derntl, B., et al. (2012). Empathic behavioral and physiological responses to dynamic stimuli in depression. Psychiat. Res. 200, 294–305. doi: 10.1016/j.psychres.2012.03.054
Schreiter, S., Pijnenborg, G. H. M., and Aan Het Rot, M. (2013). Empathy in adults with clinical or subclinical depressive symptoms. J. Affect. Disord. 150, 1–16. doi: 10.1016/j.jad.2013.03.009
Schurz, M., Maliske, L., and Kanske, P. (2020). Cross-network interactions in social cognition: a review of findings on task related brain activation and connectivity. Cortex 130, 142–157. doi: 10.1016/j.cortex.2020.05.006
Schurz, M., Radua, J., Tholen, M. G., Maliske, L., Margulies, D. S., Mars, R. B., et al. (2021). Toward a hierarchical model of social cognition: a neuroimaging meta-analysis and integrative review of empathy and theory of mind. Psychol. Bullet. 147, 293–327. doi: 10.1037/bul0000303
Singer, T., and Klimecki, O. M. (2014). Empathy and compassion. Curr. Biol. 24, R875–R878. doi: 10.1016/j.cub.2014.06.054
Sterzer, P., Hilgenfeldt, T., Freudenberg, P., Bermpohl, F., and Adli, M. (2011). Access of emotional information to visual awareness in patients with major depressive disorder. Psychol. Med. 41, 1615–1624. doi: 10.1017/S0033291710002540
Thoma, P., Zalewski, I., Von Reventlow, H. G., Norra, C., Juckel, G., and Daum, I. (2011). Cognitive and affective empathy in depression linked to executive control. Psychiat. Res. 189, 373–378. doi: 10.1016/j.psychres.2011.07.030
Tone, E. B., and Tully, E. C. (2014). Empathy as a “risky strength”: a multilevel examination of empathy and risk for internalizing disorders. Dev. Psychopathol. 26, 1547–1565. doi: 10.1017/S0954579414001199
Trew, J. L. (2011). Exploring the roles of approach and avoidance in depression: an integrative model. Clin. Psychol. Rev. 31, 1156–1168. doi: 10.1016/j.cpr.2011.07.007
Tully, E. C., Ames, A. M., Garcia, S. E., and Donohue, M. R. (2016). Quadratic associations between empathy and depression as moderated by emotion dysregulation. J. Psychol. 150, 15–35. doi: 10.1080/00223980.2014.992382
Keywords: major depressive disorder, social cognition, empathy, neural correlates, fMRI
Citation: Choi D, Förster K, Alexander N and Kanske P (2024) Downsides to the empathic brain? A review of neural correlates of empathy in major depressive disorder. Front. Hum. Neurosci. 18:1456570. doi: 10.3389/fnhum.2024.1456570
Received: 28 June 2024; Accepted: 26 July 2024;
Published: 15 August 2024.
Edited by:
Khatereh Borhani, Shahid Beheshti University, IranReviewed by:
Raluca Petrican, University of Liverpool, United KingdomCopyright © 2024 Choi, Förster, Alexander and Kanske. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dahna Choi, ZGFobmEuY2hvaUB0dS1kcmVzZGVuLmRl