
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Hum. Neurosci., 24 November 2022
Sec. Cognitive Neuroscience
Volume 16 - 2022 | https://doi.org/10.3389/fnhum.2022.991382
This article is part of the Research TopicStudy of COVID-19 Sequelae Using Non-Invasive Brain Imaging TechniquesView all 4 articles
 Zuhair Hawsawi1†
Zuhair Hawsawi1† Dilaware Khan2†
Dilaware Khan2† Igor Fischer2
Igor Fischer2 Jan Frederick Cornelius2Daniel Hänggi2
Jan Frederick Cornelius2Daniel Hänggi2 Sajjad Muhammad2,3*
Sajjad Muhammad2,3*Introduction: SARS-CoV-2 virus infection causes a dysbalanced and severe inflammatory response, including hypercytokinemia and immunodepression. Systemic inflammation triggered by a viral infection can potentially cause vascular damage, which may lead to cardiovascular and neurovascular events.
Research question: The aim was to investigate whether CNS complications are related to COVID-19.
Materials and methods: We examined 21 patients suffering from stroke and intracranial hemorrhage (ICH) and 9 (43%) of them were male. We compared relative frequencies using Fisher’s exact test. As we had few observations and many variables, we used principal component analysis (PCA) to reduce data dimensionality. We trained a linear support vector machine (SVM) on the first two PCs of the laboratory data to predict COVID-19.
Results: Patients suffering from stroke had either hypertension or SARS-CoV-2 infection, but seldom both (OR = 0.05, p = 0.0075). The presence of SARS-CoV-2 infection was strongly associated with the logarithm of CRP (p = 1.4e–07) and with D-DIMER (p = 1.6e–05) and moderately with PT (p = 0.0024). SARS-CoV-2 infection was not related to any other factor. CRP, D-DIMER, PT, and INR were all related to each other (R2 ranging from 0.19 to 0.52, p ranging from 0.012 to < 0.0001). The first two PCs covered 96% of the variance in the four variables. Using them, perfect linear discrimination between patients suffering from COVID-19 and other patients could be achieved.
Discussion and conclusion: SARS-CoV-2 infection causes systemic inflammation, which is suggested as a predictor of the severe course of ICH. SARS-CoV-2 infection is an additional risk factor for vascular complications.
The number of SARS-CoV-2 virus-infected patients is increasing rapidly. To this date, this virus has infected more than 100 million people leading to more than 2 million deaths (Johns Hopkins Coronavirus Resource Center). Preventive measures mainly vaccination is the main hope to overcome this pandemic. However, there is still uncertainty regarding the effectiveness of the currently available vaccination. Foremost, long-term outcomes after acute SARS-CoV-2 infection are unknown. In addition, more evidence regarding severe COVID-19 symptoms is not restricted to respiratory system failure, and also little is known about those “alongside” causalities. Our clinical correlative study provides new evidence for the association of COVID-19 to a hither comparatively unreported severe clinical complication, namely, bleeding of intracranial blood vessels. Our work further supports previous observations of others, such as endothelial cell infection and endotheliitis in COVID-19 patients (Varga et al., 2020), SARS-CoV-2 infected patients associated with stroke (Dhamoon et al., 2021), intracerebral hemorrhage (Cheruiyot et al., 2021), and CNS vasculitis, as well as our own previous experiences of coexisting SARS-CoV-2 infection and subarachnoid hemorrhage (Muhammad et al., 2020). This study further warns to monitor SARS-CoV-2 infected people for possibly the early onset of intracerebral bleeding and indicates the need to deeper investigate the interaction of the virus with the vascular system.
We performed a retrospective study on the patients admitted with neurological symptoms of a stroke. Clinical, radiological, and biochemical parameters and the SARS-CoV2 infection status (PCR-based) were documented. In addition to SARS-CoV2 infection status, hypertension was investigated as the probable cause of intracerebral hemorrhage. Other comorbidities and possible causes of cerebral hemorrhage, including diabetes, previous stroke, smoking, atrial fibrillation, and ischemic heart disease, were documented (Table 1). Clinical and on-admission laboratory data were collected retrospectively from a single center (Department of Neurosurgery, King Abdulaziz Hospital, Saudi Arabia) during April–June 2020. According to local law, no specific ethical approval to conduct this retrospective study was required. All required ethical and legal formalities according to the Saudi-Arabian national guidelines to conduct this retrospective study have been fulfilled for this work, and are in concordance with international standards such as the declaration of Helsinki.
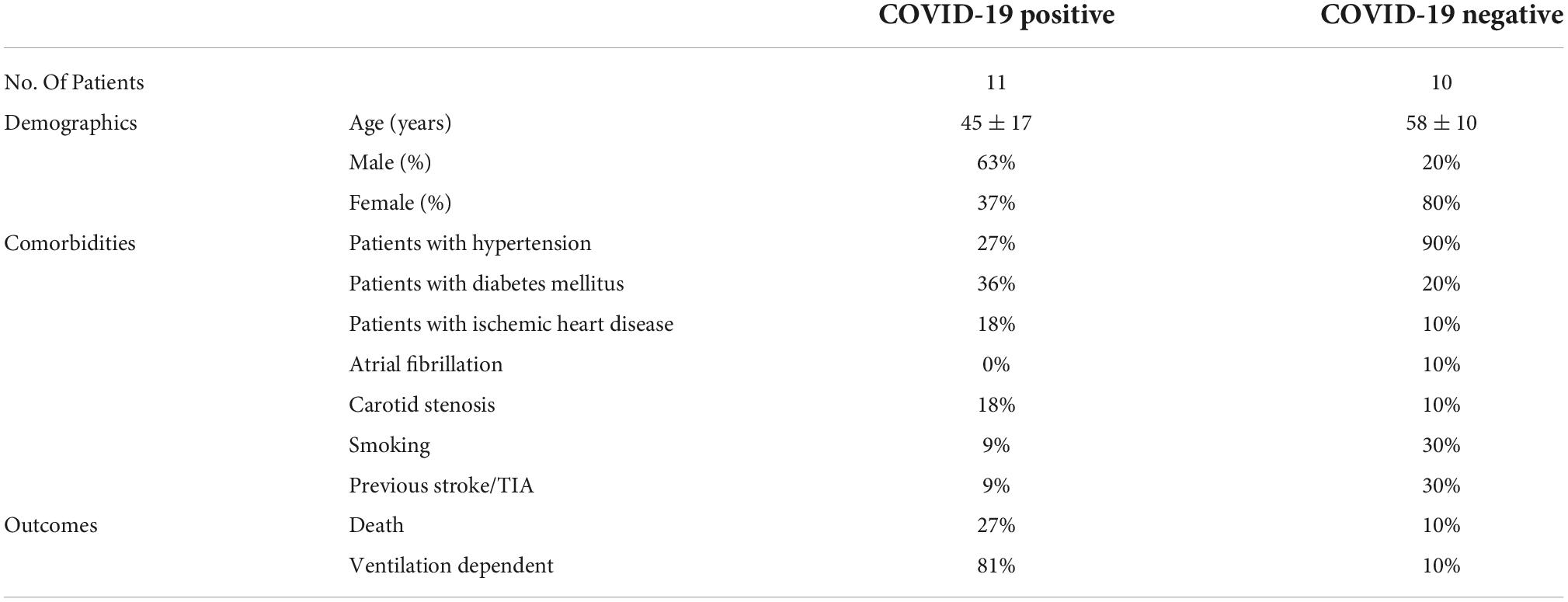
Table 1. Demographics, comorbidities, and outcomes.
Patients’ characteristics and clinical and laboratory data were analyzed using R, version 3.6.1 “Action of the Toes.” Collinearities were detected using linear regression. Odds ratios to count data were computed using Fisher’s exact test. Means between different groups were compared using Student’s t-test. When needed, variables were logarithmically transformed to more closely approximate normal distribution. The optimal classification boundary between COVID-positive and COVID-negative classes was obtained by training a linear support vector machine (SVM) from R’s e1071 library. A significance level of 0.05 was used.
Our study cohort presents the characteristics mentioned below.
Intracerebral hemorrhage in patients with COVID-19 infection showed an almost similar pattern of ICH location as in non-COVID-19 infected patients presented with hypertension (Figure 1). However, COVID-19 positive patients presenting with ICH were much younger than the patients with hypertensive bleeding without COVID-19 infection (Table 1). Interestingly, the frequency of male sex in COVID-19 patients with ICH was much higher (63%) than in uninfected patients with ICH (20%). The vascular risk factor, including smoking, arterial fibrillation, and previous TIA, was much less in COVID-19-positive patients with ICH in comparison to uninfected patients with ICH. Diabetes and ischemic heart disease were more frequent in COVID-19-infected patients with ICH. An expected combination of COVID-19 infection and ICH lead to a very high rate of intubation (81%) and mortality of around 27% (Table 1). The presence of COVID-19 infection was strongly associated with the logarithm of CRP (p = 1.4e–07), D-DIMER (p = 1.6e–05), and moderately with PT (p = 0.0024). COVID-19 infection was not related to monocytes, WBC count, neutrophil count, platelet count, blood urea nitrogen, creatinine, alanine transaminase, APTT, or PT. CRP, D-DIMER, PT, and INR were all related to each other, suggesting related pathophysiological mechanisms behind them (R2 ranging from 0.19 to 0.52, p ranging from 0.012 to < 0.0001) (Table 2).
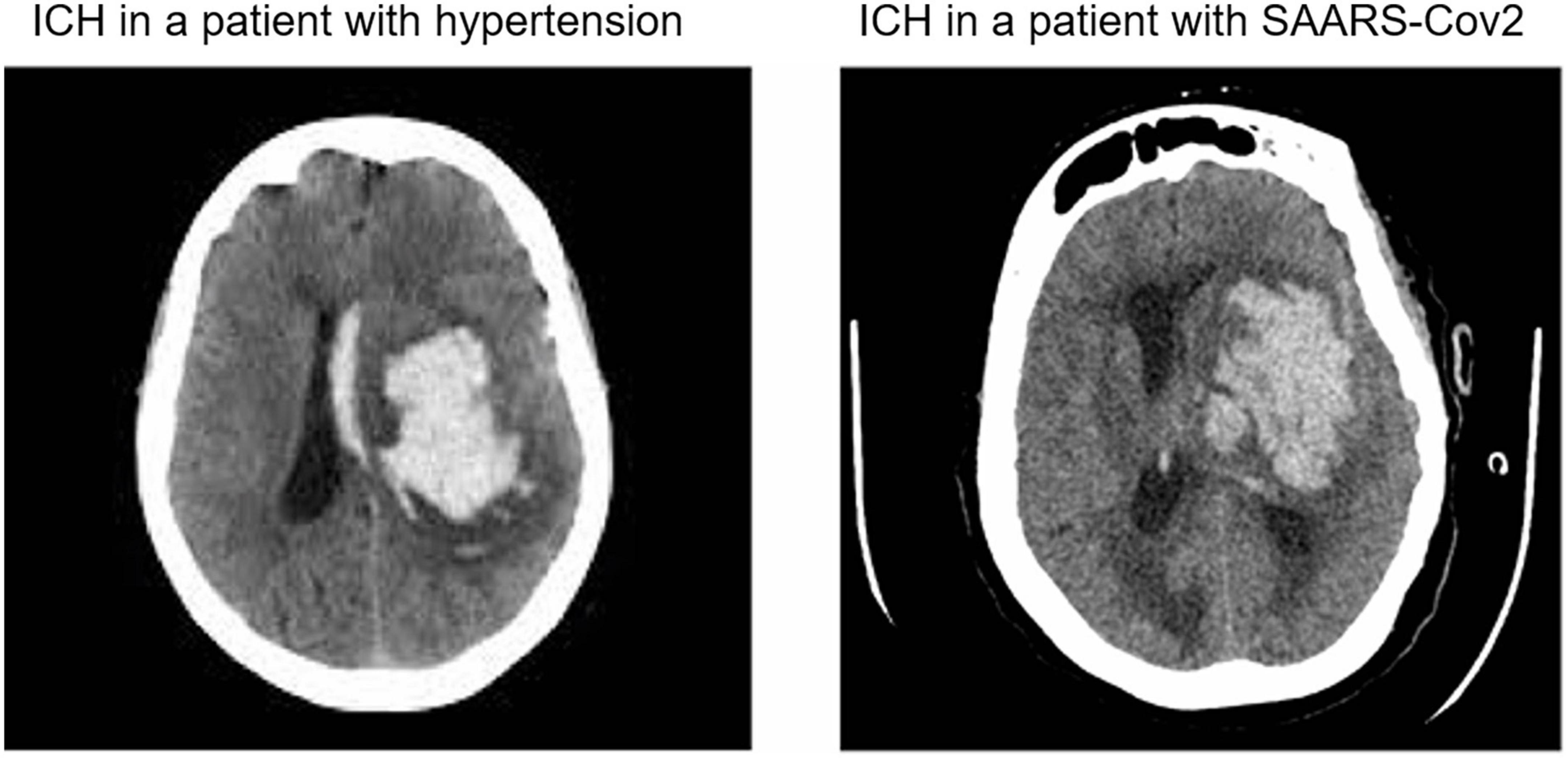
Figure 1. Representative computed tomography (CT) scans of patients with intracranial hemorrhage (ICH) suffering from hypertension or SARS-CoV2 infection/COVID-19.
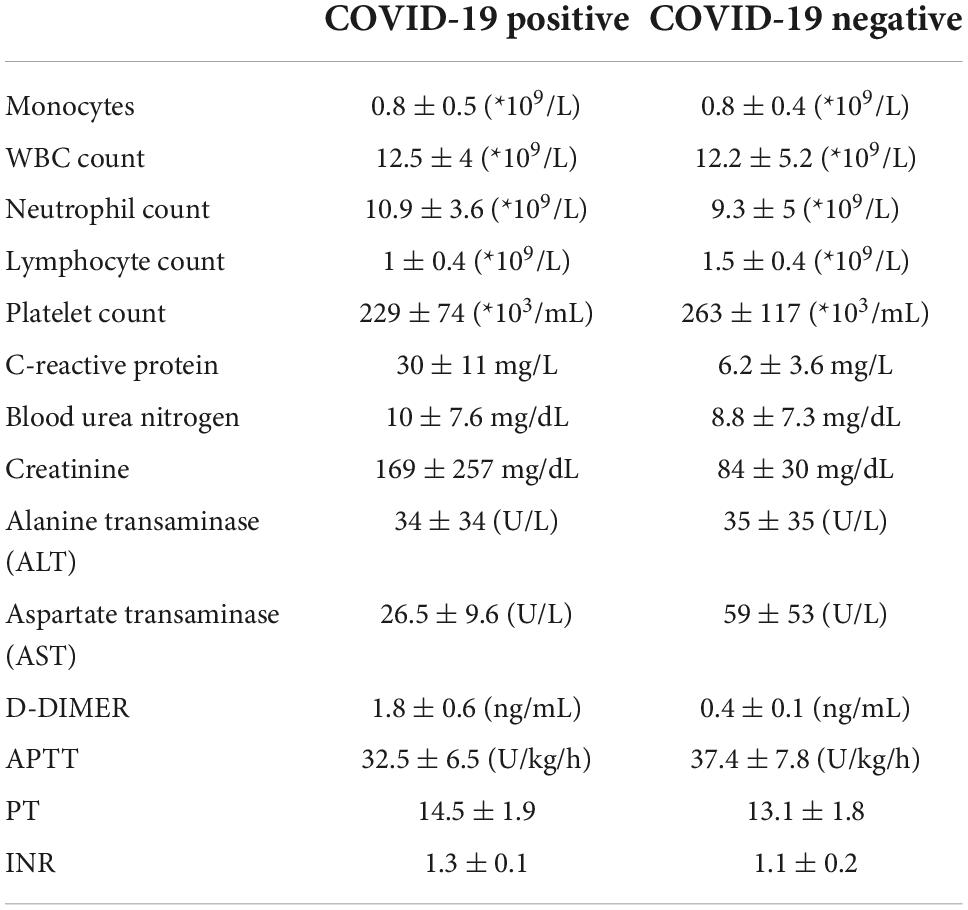
Table 2. Lab test values.
Around 90% of the non-COVID-19 patients with ICH had hypertension as a risk factor. However, COVID-19 positive cohort was mostly non-hypertensive (Table 1). Patients who suffered from a brain hemorrhage had either hypertension or COVID-19 and seldom both (OR = 0.05, p = 0.0075) (Figure 2). The first two PCs covered 96% of the variance in the four variables. Using them as predictors, perfect linear discrimination between patients suffering from COVID-19 and other patients could be achieved. Since hypertension is known to be a risk factor for ICH, we may conclude that COVID-19 is also an independent risk factor for ICH.
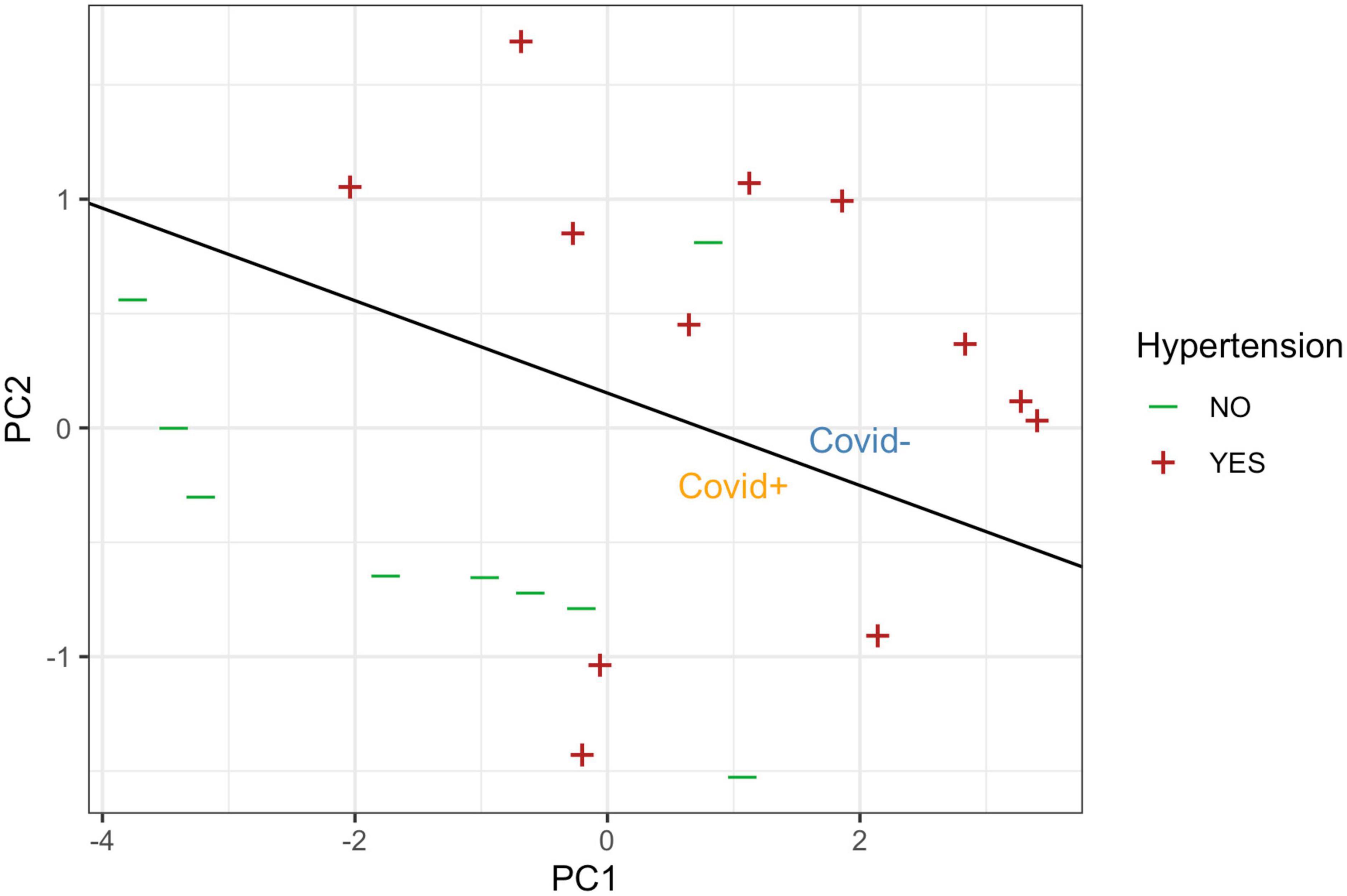
Figure 2. Presence of hypertension, plotted against the first two principal components of the four serum markers (log-CRP, D-DIMER, PT, and INR). The black line denotes the linear class boundary separating the SARS-CoV2/COVID-positive (orange, below) and SARS-CoV2/COVID-negative cases (blue area above the line).
The SARS-CoV-2 virus uses the angiotensin-converting enzyme 2 (ACE2) receptor, which is highly expressed in the epithelial cells of the lung. As the SARS-CoV-2 virus binds to the ACE2 receptor, the activity of the alternative anti-inflammatory RAS pathway resulting from ACE2-angiotensin interaction is diminished and the classical RAS pathway dominates leading to inflammation, vasoconstriction, water retention, and increased ROS, which consequently can increase the risk of aneurysm rupture due to the hypertensive and ischemic effects of COVID-19 (Panther and Lucke-Wold, 2022; Small et al., 2022). Moreover, three other mediators, including extracellular matrix metalloproteinase inducer (CD147) (Chen et al., 2005), sialic acid (Tortorici et al., 2019), and transmembrane serine protease 2 (Matsuyama et al., 2020), have been suggested to mediate the cellular entry of the virus. The above-mentioned three mediators as well as ACE2 are present in endothelial cells from small and larger arteries and veins, and arterial smooth muscle cells (Hamming et al., 2004). The presence of SARS-Cov-2 elements in endothelial cells and the accumulation of inflammatory cells accompanied by endothelial and inflammatory cell death has been reported (Varga et al., 2020). This damage to endothelial cells by increasing the expression of tissue factors can lead to clotting cascade activation resulting in clot formation, which can lead to stroke when lodged in brain vessels, and these clots via partially blocking vessels can cause turbulent flow that can subsequently lead to aneurysm rupture (Panther and Lucke-Wold, 2022; Small et al., 2022). It is already known that cytokine storm (hypercytokinemia) resulting in increased systemic inflammation with high levels of IL-6, IL-1β, and TNFα is induced by viral infections, including influenza A and COVID-19 (Muhammad et al., 2011; Qin et al., 2020). The elevated systemic inflammatory status in COVID-19 patients via increasing blood brain barrier permeability can increase MMP-9 and MMP-9 by the dysregulated breakdown of arterial collagen can lead to arterial instability and can consequently result in ICH and aneurysm aSAH (Panther and Lucke-Wold, 2022). All this basic science work clearly provides a mechanistic explanation for SARS-Cov-2 to possibly involve in stroke or stroke-like diseases.
Since the outbreak of the COVID-19 pandemic, some case reports have been published, which suggest the involvement of SARS-Cov-2 infection in hemorrhage and ICH disease course. As such, 0.25–0.7% incidence of ICH COVID-19 patients have been reported (Pavlov et al., 2020; Cheruiyot et al., 2021). In a meta-analysis, out of 108,571 COVID-19 infected patients, acute CVD occurred in 1.4% of patients with 87.4% ischemic stroke (87.4%) and 11.6% ICH cases (Nannoni et al., 2020). Extrapolating assumptions, with currently more than 100 million people infected by COVID-19, would add up to 1 million people, who are possibly at a higher risk for COVID-19-related ICH. In concordance, 105 (38%) stroke patients were SARS-Cov-2 positive out of 277 stroke patients (Dhamoon et al., 2021). The virus-infected stroke patients showed worse outcomes and had higher hospital death rates as compared to stroke patients that did not suffer from COVID-19 (Dhamoon et al., 2021). In support, the presented results—which to our knowledge is the first clinical cohort probing COVID-19 and its correlation to ICH/stroke insults—further evidence the new infectious disease to be an independent risk factor for the development of ICH.
We acknowledge that our study has several technical and experimental limitations. First, the data was collected at a single center. Multicenter studies, involving independent clinical units, are desirable to confirm our findings. Second, our results are based on an overall relatively low total number of patients and all of them are derived from the same ethnical background. We believe that the data are solid for drawing our conclusion in the view of the global state-of-the-art clinical research. Third, no information is available on the patient’s status regarding the risky lifestyle known to increase the risk of ICH development, such as alcohol abuse or smoking. It is possible that the COVID-19 patients are higher abusers as compared to the COVID-19-negative group.
Our study warns about the hitherto unrecognized association of COVID-19 neurovascular complications. Since COVID-19 is an emerging disease, our data suggest close monitoring of the patients for signs of developing neuronal bleeding. In consequence, timely preventive measures can be possibly taken to reduce the deadly secondary effects of the viral infection. Because the systemic inflammation index has been suggested as a predictor of the severity of the course of the disease (Muhammad et al., 2021), the correlation of the inflammatory index, radiology data, and COVID-19 symptoms will help to get more accurate and timely diagnosis. It will further establish the association of the viral infection with neurovascular rupture. In addition, post-mortem studies looking into the brain vasculature will provide more evidence in the support of SARS-Cov-2 to promote hemorrhage diseases.
Our correlative analysis indicates that SARS-Cov-2 infection increases the risk to develop ICH. Further studies with larger patients population derived from multi-center cohorts, ideally including ethnically diverse cases as well as the inclusion of more detailed patient history data, such as alcohol abuse or smoking habits, are required to validate our hypothesis.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
SM: conception of the work. ZH, DK, and IF: data collection, analysis, and interpretation. DK, JC, DH, and SM: drafting article and critically reviewing. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Chen, Z., Mi, L., Xu, J., Yu, J., Wang, X., Jiang, J., et al. (2005). Function of HAb18G/CD147 in invasion of host cells by severe acute respiratory syndrome coronavirus. J. Infect. Dis. 191, 755–760. doi: 10.1086/427811
Cheruiyot, I., Sehmi, P., Ominde, B., Bundi, P., Mislani, M., Ngure, B., et al. (2021). Intracranial hemorrhage in coronavirus disease 2019 (COVID-19) patients. Neurol. Sci. 42, 25–33. doi: 10.1007/s10072-020-04870-z
Dhamoon, M. S., Thaler, A., Gururangan, K., Kohli, A., Sisniega, D., Wheelwright, D., et al. (2021). Acute Cerebrovascular Events With COVID-19 Infection. Stroke 52, 48–56. doi: 10.1161/STROKEAHA.120.031668
Hamming, I., Timens, W., Bulthuis, M. L., Lely, A. T., Navis, G., and van Goor, H. (2004). Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 203, 631–637. doi: 10.1002/path.1570
Matsuyama, S., Nao, N., Shirato, K., Kawase, M., Saito, S., Takayama, I., et al. (2020). Enhanced isolation of SARS-CoV-2 by TMPRSS2-expressing cells. Proc. Natl. Acad. Sci. U S A. 117, 7001–7003. doi: 10.1073/pnas.2002589117
Muhammad, S., Fischer, I., Naderi, S., Faghih Jouibari, M., Abdolreza, S., Karimialavijeh, E., et al. (2021). Systemic Inflammatory Index Is a Novel Predictor of Intubation Requirement and Mortality after SARS-CoV-2 Infection. Pathogens 10:58. doi: 10.3390/pathogens10010058
Muhammad, S., Haasbach, E., Kotchourko, M., Strigli, A., Krenz, A., Ridder, D. A., et al. (2011). Influenza virus infection aggravates stroke outcome. Stroke 42, 783–791. doi: 10.1161/STROKEAHA.110.596783
Muhammad, S., Hafez, A., Karppinen, A., and Niemela, M. (2020). Surgical treatment of a rare rosette-forming glioneuronal tumor in the pineal region. Surg. Neurol. Int. 11:68. doi: 10.25259/SNI_294_2019
Nannoni, S., de Groot, R., Bell, S., and Markus, H. S. (2020). Stroke in COVID-19: A systematic review and meta-analysis. Int. J. Stroke 16, 137–149. doi: 10.1177/1747493020972922
Panther, E. J., and Lucke-Wold, B. (2022). Subarachnoid hemorrhage: Management considerations for COVID-19. Explor. Neuroprotective Ther. 2, 65–73. doi: 10.37349/ent.2022.00018
Pavlov, V., Beylerli, O., Gareev, I., Torres Solis, L. F., Solis Herrera, A., and Aliev, G. (2020). COVID-19-Related Intracerebral Hemorrhage. Front. Aging Neurosci. 12:600172. doi: 10.3389/fnagi.2020.600172
Qin, C., Zhou, L., Hu, Z., Zhang, S., Yang, S., Tao, Y., et al. (2020). Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 71, 762–768. doi: 10.1093/cid/ciaa248
Small, C., Mehkri, Y., Panther, E., Felisma, P., and Lucke-Wold, B. (2022). Coronavirus Disease-2019 and Stroke: Pathophysiology and Management. Can. J. Neurol. Sci. [Epub ahead of print]. doi: 10.1017/cjn.2022.267
Tortorici, M. A., Walls, A. C., Lang, Y., Wang, C., Li, Z., Koerhuis, D., et al. (2019). Structural basis for human coronavirus attachment to sialic acid receptors. Nat Struct Mol Biol 26, 481–489. doi: 10.1038/s41594-019-0233-y
Keywords: COVID-19, SARS-CoV-2, intracranial hemorrhage, stroke, clinical neurosurgery
Citation: Hawsawi Z, Khan D, Fischer I, Cornelius JF, Hänggi D and Muhammad S (2022) SARS-CoV-2 infection increases risk of intracranial hemorrhage. Front. Hum. Neurosci. 16:991382. doi: 10.3389/fnhum.2022.991382
Received: 11 July 2022; Accepted: 07 November 2022;
Published: 24 November 2022.
Edited by:
Sara Invitto, University of Salento, ItalyReviewed by:
Shambaditya Das, Bangur Institute of Neurosciences, IndiaCopyright © 2022 Hawsawi, Khan, Fischer, Cornelius, Hänggi and Muhammad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sajjad Muhammad, c2FqamFkLm11aGFtbWFkQG1lZC51bmktZHVlc3NlbGRvcmYuZGU=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.