
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Hum. Neurosci., 24 August 2022
Sec. Brain Imaging and Stimulation
Volume 16 - 2022 | https://doi.org/10.3389/fnhum.2022.958247
This article is part of the Research TopicDeep Brain Stimulation Think Tank: Updates in Neurotechnology and Neuromodulation, Volume IIIView all 15 articles
 Petra Heiden1,2
Petra Heiden1,2 Daniel Tim Weigel1
Daniel Tim Weigel1 Ricardo Loução1,2
Ricardo Loução1,2 Christina Hamisch2Enes M. Gündüz1Maximilian I. Ruge1
Christina Hamisch2Enes M. Gündüz1Maximilian I. Ruge1 Jens Kuhn3,4
Jens Kuhn3,4 Veerle Visser-Vandewalle1Pablo Andrade1*
Veerle Visser-Vandewalle1Pablo Andrade1*Self-injurious behavior (SIB) is associated with diverse psychiatric conditions. Sometimes (e.g., in patients with autism spectrum disorder or acquired brain injuries), SIB is the most dominant symptom, severely restricting the psychosocial functioning and quality of life of the patients and inhibiting appropriate patient care. In severe cases, it can lead to permanent physical injuries or even death. Primary therapy consists of medical treatment and if implementable, behavioral therapy. For patients with severe SIB refractory to conventional therapy, neuromodulation can be considered as a last recourse. In scientific literature, several successful lesioning and deep brain stimulation targets have been described that can indicate a common underlying neuronal pathway. The objectives of this study were to evaluate the short- and long-term clinical outcome of patients with severe, therapy refractory SIB who underwent DBS with diverse underlying psychiatric disorders and to correlate these outcomes with the activated connectivity networks. We retrospectively analyzed 10 patients with SIB who underwent DBS surgery with diverse psychiatric conditions including autism spectrum disorder, organic personality disorder after hypoxic or traumatic brain injury or Tourette syndrome. DBS targets were chosen according to the underlying disorder, patients were either stimulated in the nucleus accumbens, amygdala, posterior hypothalamus, medial thalamus or ventrolateral thalamus. Clinical outcome was measured 6 months after surgery and at long-term follow-up after 10 or more years using the Early Rehabilitation Barthel index (ERBI) and time of restraint. Connectivity patterns were analyzed using normative connectome. Based on previous literature the orbitofrontal cortex, superior frontal gyrus, the anterior cingulate cortex, the amygdala and the hippocampus were chosen as regions of interest. This analysis showed a significant improvement in the functionality of the patients with DBS in the short- and long-term follow-up. Good clinical outcome correlated with higher connectivity to the amygdala and hippocampus. These findings may suggest a common pathway, which can be relevant when planning a surgical procedure in patients with SIB.
Self-injurious behavior (SIB) is defined as a behavior where the affected individual inflicts physical injury upon him/herself (Minshawi et al., 2014). SIB is associated with diverse psychiatric disorders. In most cases it is part of the clinical appearance of the disease. In rare cases SIB is the most dominant symptom, almost solely limiting the patients’ psychosociological functioning, reducing quality of life severely and inhibiting appropriate patient care. This mostly occurs in patients with advanced autism spectrum disorder, severe Tourette syndrome or in case of acquired brain injuries (Huisman et al., 2018). It is essential to differentiate SIB of these patients from non-suicidal self-injury in patients with borderline personality disorder or psychological distress (Brickman et al., 2014). Epidemiological studies have shown that about 4% to 9% of people with intellectual or developmental disabilities exhibit SIB; within the population of autism spectrum disorder this rate is 33% to 71% (Bradley et al., 2018) and within patients with Tourette syndrome 35% (Stafford and Cavanna, 2020). In severe cases, SIB can lead to serious permanent physical damages or even death and is frequently associated with social isolation and institutionalization. Further, it can entail a high psychological and financial burden for the social environment of the affected patient (Bradley et al., 2018).
Treatment should be focused on the underlying psychiatric diagnosis if a specific disorder is diagnosed (Antonacci et al., 2008). First-line treatment for SIB consists of pharmacological therapy. Mood stabilizers like valproate or carbamazepine have shown to be efficient in the treatment of aggression (Golden et al., 2006). Atypical antipsychotics are also used off-label, most frequently risperidone, aripiprazole or olanzapine. Behavioral therapies have been proven to be effective, however, severe symptoms may prohibit appropriate psychotherapeutic methods and only few have access to specialized centers (Antonacci et al., 2008). Also, several studies report a transient improvement of the symptoms after electroconvulsive therapy (Consoli et al., 2013).
Several stereotactic techniques have been introduced in the last decades with the aspiration to help patients with severe, otherwise therapy refractory SIB as a last resort. During the 1960s posteromedial hypothalamotomy and amygdalotomy emerged as treatment options for therapy refractory pathological aggressiveness (Narabayashi and Uno, 1966; Sano et al., 1966). Both procedures showed a significant improvement of the symptoms in more than half of the patients in the short- and long-term follow-up. However severe side effects were reported in studies with amygdalotomies, including Klüver-Bucy syndrome, seizures and hemiparesis (Narabayashi and Uno, 1966; Kiloh et al., 1974). Studies with hypothalamotomies only reported mild side effects (Sano et al., 1966). Further possible lesion targets described in subsequent literature are the anterior cingulate cortex (CC) and the anterior limb of the internal capsule (Jiménez et al., 2012). With the development of deep brain stimulation (DBS) it was reasonable to apply this possibly reversable method also for patients with severe pathological aggressiveness. The knowledge gained from studies using stereotactic lesioning was applied for the selection of possible target structures. The first DBS for pathological aggressiveness targeting the posteromedial hypothalamus was described by Franzini et al. (2005) in 2005. After that, Sturm et al. (2013) published the first case describing the efficacy of DBS of the amygdala for the treatment of pathological aggressiveness. Direct comparison of the reported cases is challenging due to the different clinical outcome measurements used, nonetheless most studies report satisfying results in most of the patients (Jiménez et al., 2012; Zhang et al., 2017; Torres et al., 2021; Yan et al., 2022). In summary, there are several possible target structures along the limbic system described in scientific literature for the treatment of pathological aggressiveness. It is believed that the neuronal circuits connecting the amygdala, the hippocampus and the periaqueductal gray, control reactive aggressiveness, moderated by the ventromedial frontal cortex, including the anterior CC (Rossel and Siever, 2015; Blair, 2016). Based on the functional and structural connections between the different stereotactic target regions and the observed beneficial outcome, this might indicate a common underlying neuronal network responsible for aggressive behavior.
The first objective of this study was to report the efficacy and safety of DBS in SIB patients treated at our clinic and their long-term clinical outcome. Our second objective was to analyze the connectivity patterns and the potentially identify common networks based on their clinical outcome.
We retrospectively analyzed the data of 10 patients with SIB who underwent surgery for chronic DBS at the University Hospital Cologne between 2003 and 2009. All patients suffered from severe, continuous, therapy resistant SIB for a long time period, which was the dominant symptom of their disorder. All patients were evaluated by psychiatric experts from our hospital. Surgery was offered to these patients and their families or caregivers after individual evaluation by experienced neurosurgical and psychiatric specialists of the University Hospital Cologne. The performance of stereotactic surgery followed the premise of an individual attempt of healing in otherwise treatment refractory patients. The University Hospital of Cologne Medical Ethical Committee was informed and ethical approval was obtained before each intervention.
Five patients were diagnosed with therapy refractory Tourette syndrome, three patients developed SIB after hypoxic or traumatic brain injury and two patients suffered from SIB since childhood as part of their severe autism spectrum disorder. The target for DBS surgery was chosen according to the underlying psychiatric disorder, in all cases bilaterally. In three patients with Tourette syndrome the nucleus accumbens was targeted, in one patient the ventrolateral thalamus and in one further patient the posterolateral hypothalamus. In two patients with SIB after brain injury the posterolateral hypothalamus was targeted, in the third patient the medial thalamus. One patient with autism spectrum disorder received DBS in the nucleus accumbens, the second patient in the amygdala. Targets were identified using the Atlas of the Human Brain (Schaltenbrand and Wahren, 1977) and a preoperative MRI-scan. Stereotactic planning was performed using the STP 3.5 software (Howmedica Leibinger, Freiburg, Germany). Quadripolar electrodes (Medtronic 3389 or 3387, Medtronic Plc, Minneapolis, Minnesota, USA) were implanted stereotactically-guided, the accurate location of the electrodes was confirmed using intraoperative x-rays. Stimulation parameters were gradually adjusted individually during the follow-up visits.
Clinical outcome was measured using the Early Rehabilitation Barthel Index (ERBI) and percentage of time patients stay restrained, which was assessed prior to surgery, 6 months after the procedure and at the last follow-up appointment. On the ERBI each item measures the independency of the patient in daily activities. The final score ranges from −325 to +100 points, more positive values indicating higher independency (Rollnik, 2011). Patients were classified as responders with an improvement over 20 points on the ERBI (Quinn et al., 2011) 6 months after the surgery. Low-responders were defined as patients with an improvement between 20 and 100 points, patients were classified as good-responders with an improvement over 100 points.
In order to analyze the connectivity patterns, we estimated the volume of activated tissue using the following method. The preoperative T1 sequence of each patient was co-registered and normalized to ICBM 152 MNI 2009b space (Fonov et al., 2009) through a combination of linear and non-linear transformations, using Advanced Normalization Tools (ANTs1, Avants et al., 2008; Tustison et al., 2019). The stereotactic AC/PC coordinates of the electrodes documented during surgery were transferred to MNI space and were projected using the open-source software Lead-DBS2 (Horn and Kühn, 2015). Using the model described by Horn et al. (2017a), we estimated the volume stimulated by the active contacts (VTA, Volume of Tissue Activated) based on the stimulation parameters documented at the follow-up appointment 6 months past the surgery, with a general heuristic electrical field threshold of 0.2 V/mm.
Based on previous studies (Rossel and Siever, 2015; Blair, 2016; Rizzi et al., 2017) the medial and lateral orbitofrontal cortex (OFC), the superior frontal gyrus, the anterior CC, the amygdala, and the hippocampus were defined as regions of interest (ROIs). Subcortical nuclei were identified using the MNI PD25 (Xiao et al., 2017) atlas and cortical regions using the Desikan-Killiany atlas (Desikan et al., 2006). The connectivity of the VTAs to the ROIs was analyzed in a structural group connectome based on the diffusion spectrum imaging of 32 healthy adult subjects (Human Connectome Project, HCP; Setsomop et al., 2013; Horn et al., 2017b). Using TrackVis imaging software (Wang et al., 2007), we quantified the number of tracts passing through the VTAs and connecting each of them to each ROI. The VTAs for the left and right hemisphere were analyzed separately and only the connectivity to the ROI to the ipsilateral hemisphere was included in the analysis.
In a further analysis, we performed a whole-brain analysis identifying fibers associated with better clinical outcome. First, the tracts in the normative connectome which were hit by any VTA of the whole patient cohort were isolated. Then, for each tract of this subset, two groups of patients were defined: patients whose VTAs hit the tract in question, and patients whose VTAs did not hit the tract. The clinical outcomes of these two groups were then compared using Mann-Whitney-U test and an approximate z-value was calculated and attributed to the tract in question. Negative z-scores are associated with clinical worsening, while positive ones to clinical improvement. This analysis was performed iteratively on all tracts of the subset using custom-built MATLAB routines (version 2020b, The Mathworks Inc., Natick, Massachusetts, USA).
All data were analyzed using SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Macintosh, Version 28.0. Armonk, New York, USA). Each brain hemisphere was analyzed separately. In the absence of normal distribution determined using the Kolmogorov–Smirnov test, the Spearman rank’s correlation was conducted between the connectivity parameters of each VTA with the individual ROIs and the clinical outcome. To compare clinical outcome at different time points the Wilcoxon test was conducted. p-values under 0.05 were considered significant. The data supporting the findings of this study, such as the DBS MRI datasets, are not publicly available due to data privacy regulations, but are available from the corresponding author upon reasonable request.
Demographic and clinical data of the patients prior to surgery is summarized in Table 1. The mean age at the date of the surgery was 30.9 years (SD ± 11 years), ranging from 13 to 45 years. On average SIB persisted for 17.1 years prior to surgery (SD ± 14.7 years). Seven patients were males and three females. The mean ERBI at the time of the surgery was −54.5 points (SD ± 74.1). In all patients, there was a significant improvement 6 months after the surgery, with a mean ERBI of 38.5 points (SD ± 72.62; z = −3.75, p < 0.001). One patient was classified as a non-responder, four patients as low-responders and five as good-responders. There was also a significant reduction of the mean duration of restraint from 65% prior to surgery (SD ± 46.2%) to 11.5% (SD ± 15.9%) of the day 6 months after the intervention (z = −3.09, p < 0.001). The individual clinical course of each patient is displayed in Table 2.
Table 1. Demographic table of the patients including stimulation parameters associated with the best clinical results 6 months past the surgery.
Table 2. Summary of the clinical outcome and complications of each patient.
Long-term follow-up after more than 10 years could be conducted in six patients. From the four patient who did not complete the long-term follow-up, two patients initially participated in follow-up appointments, however eventually did not visit our clinic anymore and could not be contacted via telephone or email. Two patients were excluded due to termination of the stimulation after several years because they did not benefit from the stimulation anymore. On average the last follow-up appointment was 14.7 years after the initial surgery (SD ± 2.3 years). The mean ERBI at the long-term follow-up was slightly lower than 6 months after the intervention, however the difference was not statistically significant (mean ERBI at long-term follow-up: 36.7, SD ± 74, z = −1.86, p = 0.063). Nonetheless, there was still a significant improvement when compared to the preoperative ERBI (z = −2.87, p = 0.002). The average time of restraint also increased in the long-term follow-up to 16.67% (SD ± 24.61%) of the day, however, there was still a significant difference to the pre-operative parameters (z = −2.59, p = 0.01).
Three patients had an infection of the DBS system, in one patient it occurred after 1 month, in the second patient after 3 months and in the third patient 5 years after the initial surgery. In all three cases a complete removal of the DBS system was performed. All three patients underwent additional surgery to reimplant the system at a later stage. Leads were placed at the same location in patients where the electrodes were removed after 1 and 3 months. For the third patient the target was changed from nucleus accumbens to the thalamus (centromedian nucleus/ventroralis internus). No further complications or permanent side effects were reported.
In both patients who underwent revision surgery within the first year, 6 months follow up data was collected 6 months after the reimplantation of the system.
The proportion of tracts connecting the VTA to each ROI in all tracts activated by the VTA was calculated in the HCP normative connectome. There was a moderate correlation between the mean percentage of tracts connecting the VTAs to the medial OFC and the clinical improvement measured with the ERBI 6 months after the surgery (mean 5.21%, SD ± 8.72%, rs = 0.37, p = 0.109; Figure 1A), however it was not statistically significant.
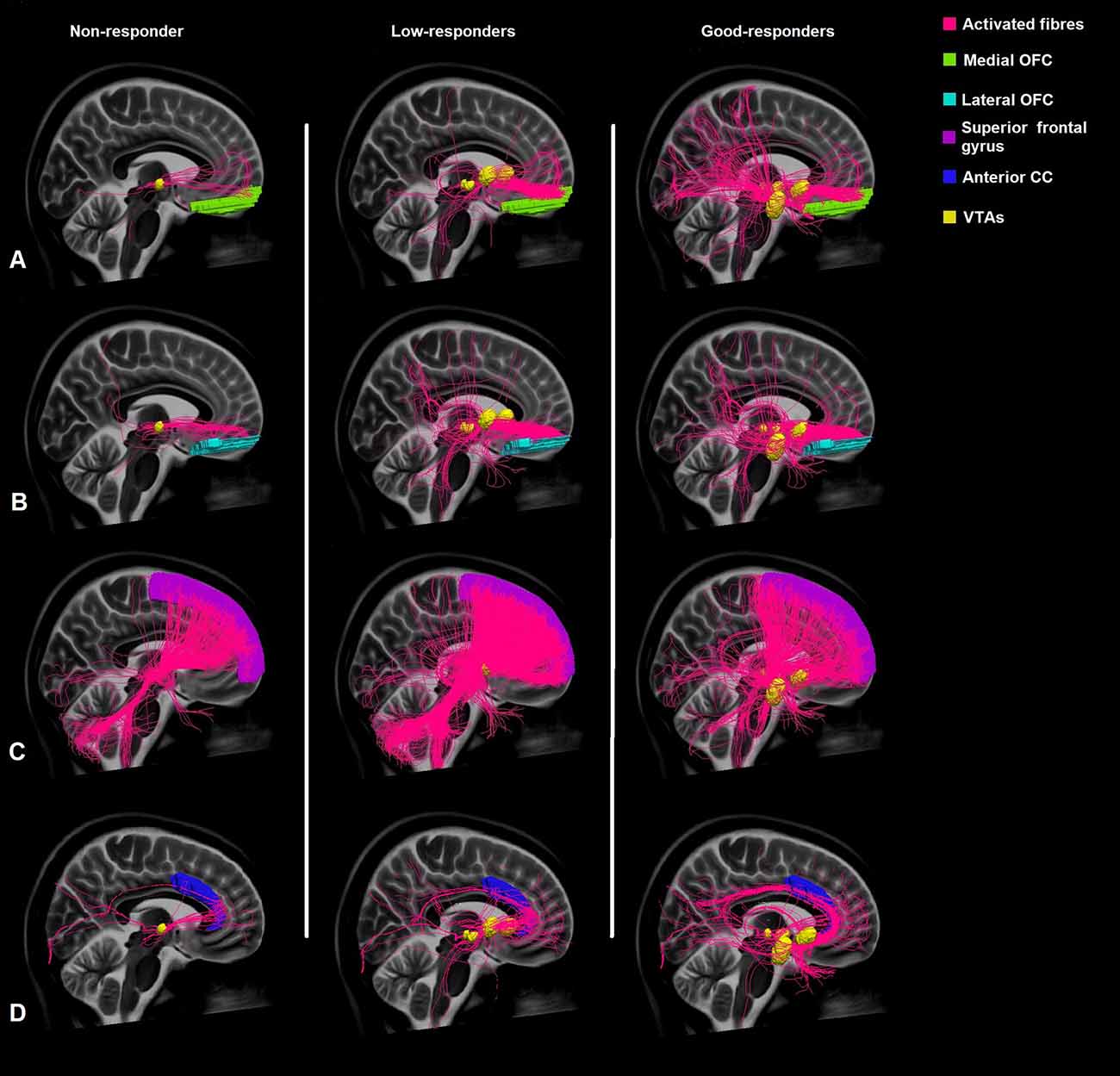
Figure 1. Comparison of the connectivity of the VTAs of non-responders, low-responders, and good-responders to the medial orbitofrontal cortex (medial OFC) (A), lateral orbitofrontal cortex (lateral OFC) (B), superior frontal gyrus (C), and the anterior cingulate cortex (anterior CC) (D) based on normative connectome.
There was also no significant correlation between the proportion of tracts connecting to the lateral OFC (mean 3.89%, SD ± 4.91%, rs = 0.26, p = 0.26; Figure 1B) or the superior frontal gyrus (mean 18.87%, SD ± 15.97, rs = −0.416, p = 0.068; Figure 1C) and the clinical outcome.
The portion of tracts connecting the VTAs to the anterior CC moderately correlated with the clinical outcome, however this correlation was not statistically significant (mean 2.41%, SD ± 3.93%, rs = 0.383, p = 0.96; Figure 1D).
Our data could show a significant moderate correlation between the clinical improvement measured on the ERBI and the percentage of tracts connecting to the amygdala (mean 12.04%, SD ± 14.19, rs = 0.478, p = 0.033; Figure 2).
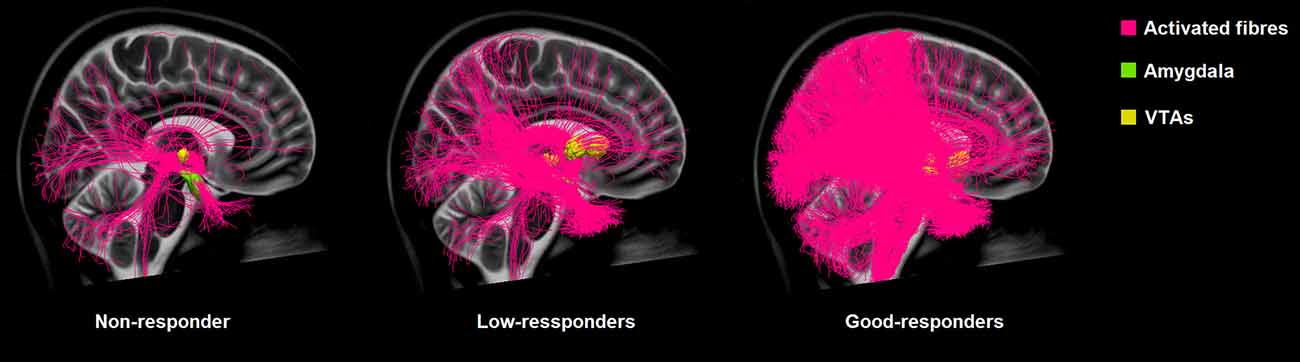
Figure 2. Comparison of the connectivity of the VTAs of non-responders, low-responders, and good-responders to the amygdala based on normative connectome.
There was a stronger, also significant correlation between the clinical outcome and the proportion of tracts connecting to the hippocampus (mean 2.35%, SD ± 4.75, rs = 0.574, p = 0.008; Figure 3).
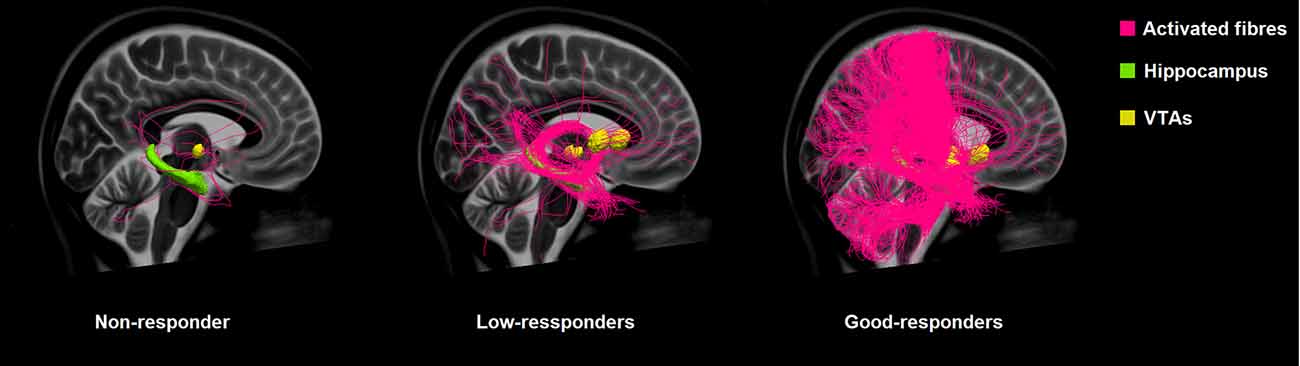
Figure 3. Comparison of the connectivity of the VTAs of non-responders, low-responders, and good-responders to the hippocampus based on normative connectome.
Connectivity patterns of the VTAs to the whole brain weighted by clinical improvement of the patients are displayed in Figures 4 and 5. Tracts associated with better clinical improvement connected the VTAs to the amygdala, hippocampus and to the CC on both sides. Tracts associated with worse clinical outcome showed stronger connectivity to the superior frontal gyrus. In the OFC, activated fibers connecting to the medial part were associated with a greater clinical improvement, while fibers connecting to the lateral OFC were associated with less improvement measured on the ERBI.
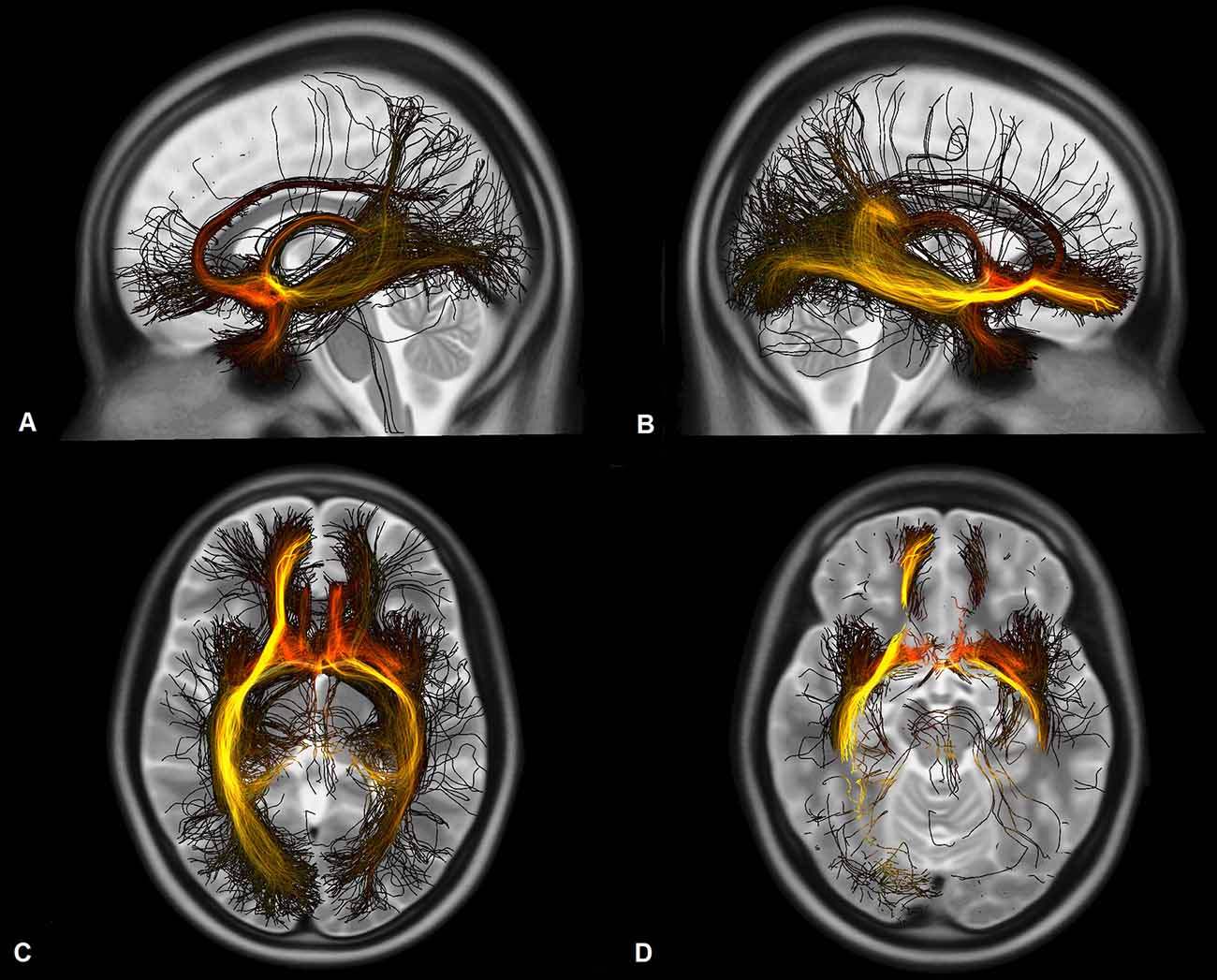
Figure 4. Fibers activated by the VTAs and associated with a better functional outcome of the patients measured on the ERBI in sagittal view from the left (A), from the right (B), in axial view on the level of the thalami (C), and on the level of the hippocampus and the amygdala (D). Darker colors represent a stronger correlation to the clinical outcome.
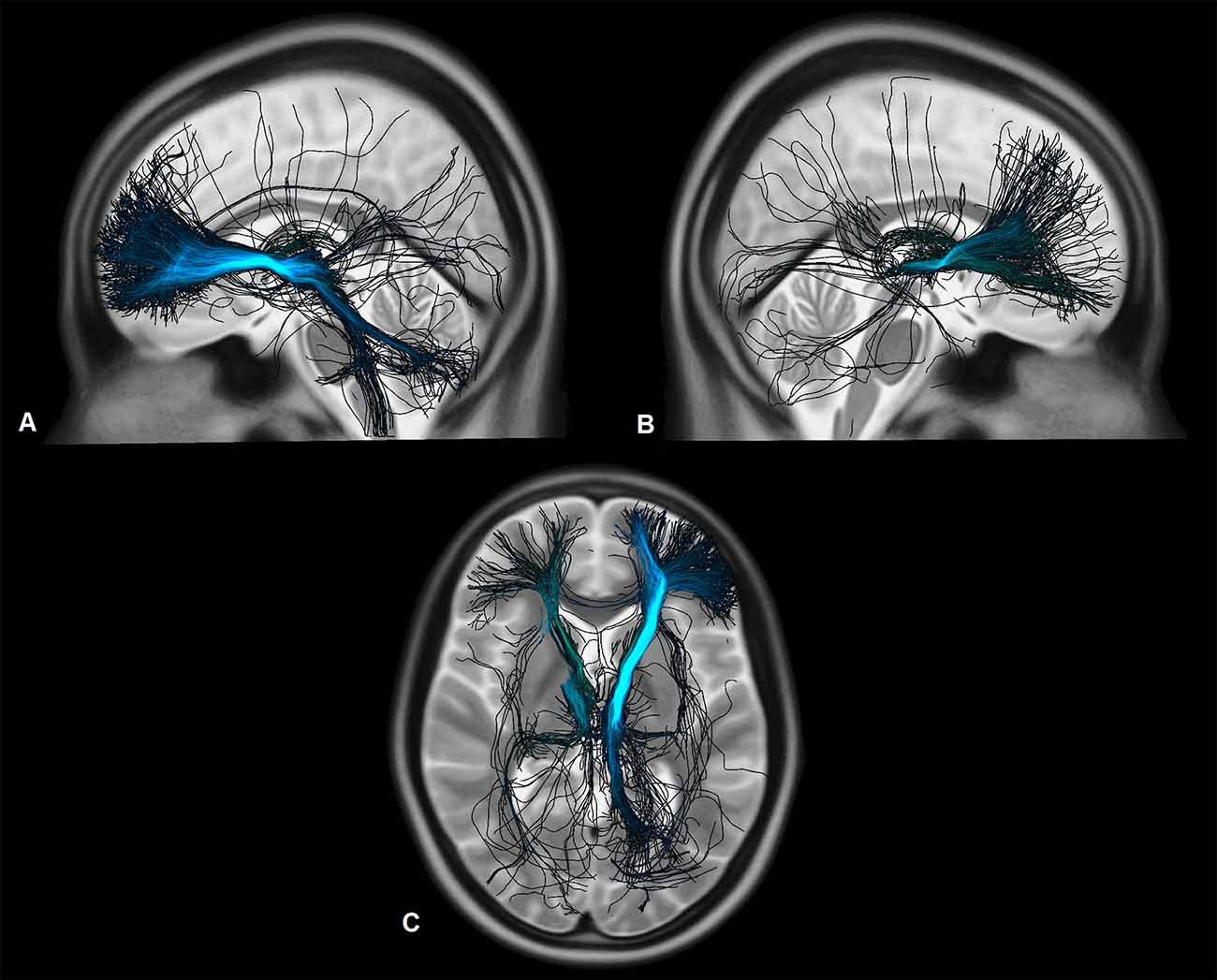
Figure 5. Fibers activated by the VTAs and associated with a worse functional outcome of the patients measured on the ERBI in sagittal view from the left (A), from the right (B), and in axial view on the level of the thalami (C). Darker colors represent a stronger correlation to the clinical outcome.
In this retrospective study we analyzed the clinical course of 10 patients with diverse psychiatric disorders under DBS, which all suffered from severe, chronic, therapy refractory SIB. Primary outcome was the improvement of functionality measured on the ERBI. As a further representative measurement for the psychosocial functionality of the patients we compared their time of restraint.
Our study showed a significant improvement in the functionality and time of restraint in SIB patients treated with DBS after 6 months as well as in a long-term follow-up with over 10 years of stimulation. In this retrospective analysis, 9 out of 10 patients reached satisfactory results with DBS, whereas one patient was a clear non-responder. A further patient was explanted due to loss of effect of the stimulation after several years of profiting from DBS. These results fall in line with the clinical outcome reported in the literature (Torres et al., 2021; Yan et al., 2022), however direct comparison is not possible due to different outcome measures. In our patient group, there was no further improvement in the long-term follow-up, rather a slight deterioration compared to the follow-up 6 months after the intervention. There was still a significant improvement of the clinical status in the long-term follow-up in comparison to the baseline. Three out of 10 cases needed additional surgery because of an infection of the DBS-system were reported, which resulted in additional surgeries for the patients. All patients did well after re-implantation and suffered no permanent complications. This infection-rate is higher than in other DBS-studies, reporting a risk of infection of 5% (Kantzanou et al., 2021), probably due to the complex care and specific clinical status on account of skin wounds of patients suffering from SIB.
Analysis of the connectivity patterns using normative connectome showed a significant positive correlation between clinical improvement and the strength of connectivity to the hippocampus and the amygdala. Further, fibers associated with better clinical outcome were shown to be connected to the amygdala and hippocampus and to the CC as well. Activated fibers projecting to the prefrontal cortex overlap the medial forebrain bundle as described by Coenen et al. (2018), these fibers are mostly associated with reward-associated behavior and motivation. Interestingly fibers associated with less improvement in the ERBI after 6 months organize in a more dorsal pathway which also overlaps the common pathway for deep-brain-stimulation in obsessive-compulsive disorder, as described by Li et al. (2020). Fibers which were associated with a better clinical outcome organize in a more ventral circuit and project more to the medial OFC.
Our results suggest a common underlying neuronal network which is stimulated at different areas in these patients, resulting in reduction of SIB. Whole-brain analysis also indicates a clear differentiation of this network from the common pathway previously identified for the treatment of obsessive-compulsive disorder. Identification of a common pathway would be especially helpful in these patients as they suffer from different underlying disorders, which should be also considered during the planning of a DBS procedure. For example, in patients with Tourette syndrome and SIB it might be beneficial to consider underlying pathways both in regard to the underlying neuropsychiatric condition and the auto-mutilative behavior. Previous studies showed that stronger connectivity to the supplementary motor area (SMA) and preSMA correlate with better tic-reduction (Andrade et al., 2020), thus a target affecting the motoric pathways and also with strong connectivity to the amygdala and hippocampus might be most beneficial for Tourette patients suffering from SIB.
Activated fibers associated with a worse clinical outcome projected to the superior frontal gyrus and the lateral OFC. However, it is important to note, that these fibers were not correlating with an increase of SIB, as none of the patients had a worse clinical outcome in compare to the baseline parameters at the follow-ups. Thus, these fibers probably have no association with the modulation of SIB.
An important limitation of this study is, that it analyses a symptom in a diversity of underlying psychiatric conditions, which makes the comparison and unification of these patients difficult.
Regarding the method of neuroimage analysis, it is important to remark, that traumatic and hypoxic brain injuries are associated with altered structural and functional connectivity (Hayes et al., 2016; Smyser et al., 2019), therefore using a normative connectome when analyzing these patients might be misleading. Structural abnormalities have been also reported in the socio-emotional circuits of patients with autism spectrum disorder (Ameis et al., 2011) and studies also show an altered functional and structural connectivity in Tourette syndrome (Worbe et al., 2012; Cheng et al., 2014; Heiden et al., 2021). Analysis based on patient specific diffusion imaging data would be more suitable considering this patient collective. A further limitation is the low number of subjects in this study, which has a considerable effect on the interpretation of the clinical and neuroimaging results. A multi-center study involving larger patient groups would be necessary to further isolate neuronal networks which contribute to the reduction of SIB. However, the diversity of underlying psychiatric conditions and comorbidities of patients with SIB might complicate such an analysis. Randomized-controlled studies, although potentially of a high scientific value, are less likely to be successful in this particular patient group because of the complicated care, ethical issues related to informed consent, and lacking compliance of this patient population.
In this study, we reported an improvement of the psychosocial functionality in patients with diverse psychiatric conditions with severe SIB using DBS in diverse anatomical targets. We showed a significant correlation between the clinical improvement and connectivity patterns with higher number of activated tracts to the amygdala and the hippocampus bilaterally. These findings suggest the presence of a common underlying neuronal network for SIB between these targets, which can eventually assist when considering a surgical procedure for treatment refractory patients with diverse underlying conditions and comorbidities.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
PH, VV-V, and PA: conceptualization. PH, DW, RL, CH, EG, MR, JK, and PA: investigation. PH, DW, RL, and PA: methods. PH and PA: writing—original draft. PH, DW, RL, CH, EG, MR, JK, VV-V, and PA: writing—review and editing. All authors contributed to the article and approved the submitted version.
We acknowledge support for the Article Processing Charge from the DFG (German Research Foundation, 491454339).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ameis, S. H., Fan, J., Rockel, C., Voineskos, A. N., Lobaugh, N. J., Soorya, L., et al. (2011). Impaired structural connectivity of socio-emotional circuits in autism spectrum disorders: a diffusion tensor imaging study. PLoS One 6:e28044. doi: 10.1371/journal.pone.0028044
Andrade, P., Heiden, P., Hoevels, M., Schlaman, M., Baldermann, J. C., Huys, D., et al. (2020). Modulation of fibers to motor cortex during thalamic DBS in Tourette patients correlates with tic reduction. Brain Sci. 10:302. doi: 10.3390/brainsci10050302
Antonacci, D. J., Manuel, C., and Davis, E. (2008). Diagnosis and treatment of aggression in individuals with developmental disabilities. Psychiatr. Q. 79, 225–247. doi: 10.1007/s11126-008-9080-4
Avants, B. B., Epstein, C. L., Grossmann, M., and Gee, J. C. (2008). Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Med. Image Anal. 12, 26–41. doi: 10.1016/j.media.2007.06.004
Blair, J. R. (2016). The neurobiology of impulsive aggression. J. Child Adolesc. Psychopharmacol. 26, 4–9. doi: 10.1089/cap.2015.0088
Bradley, V., Hiersteiner, D., Rotholz, D., Maloney, J., Li, H., Bonardi, A., et al. (2018). Personal characteristics and outcomes of individuals with developmental disabilities who need support for self-injurious behavior. J. Intellect. Disabil. Res. 62, 1043–1057. doi: 10.1111/jir.12518
Brickman, L. J., Ammerman, B. A., Look, A. E., Berman, M. E., and McCloskey, M. S. (2014). The relationship between non-suicidal self-injury and borderline personality disorder symptoms in a college sample. Borderline Pers. Disord. Emot. Dysregul. 1:14. doi: 10.1186/2051-6673-1-14
Cheng, B., Braas, H., Ganos, C., Treszl, A., Biermann-Ruben, K., Hummel, F. C., et al. (2014). Altered intrahemispheric structural connectivity in Gilles de la Tourette syndrome. Neuroimage Clin. 4, 174–181. doi: 10.1016/j.nicl.2013.11.011
Coenen, V. A., Schuhmacher, L. V., Kaller, C., Schlaepfer, T. E., Reinacher, P. C., Egger, K., et al. (2018). The anatomy of the human medial forebrain bundle: ventral tegmental area connections to reward-associated subcortical and frontal lobe regions. Neuroimage Clin. 18, 770–783. doi: 10.1016/j.nicl.2018.03.019
Consoli, A., Cohen, J., Bodeau, N., Guinchat, V., Wachtel, L., and Cohen, D. (2013). Electroconvulsive therapy in adolescents with intellectual disability and severe self-injurious behavior and aggression: a retrospective study. Eur. Child Adolesc. Psychiatry 22, 55–62. doi: 10.1007/s00787-012-0320-7
Desikan, R. S., Ségonne, F., Fischl, B., Quinn, B. T., Dickerson, B. C., Blacker, D., et al. (2006). An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 31, 968–980. doi: 10.1016/j.neuroimage.2006.01.021
Fonov, V. S., Evans, A. C., McKinstry, R. C., Almli, C. R., and Collins, D. L. (2009). Unbiased nonlinear average age-appropiate brain templates from birth to adulthood. Neuroimage 47:S102. doi: 10.1016/S1053-8119(09)70884-5
Franzini, A., Marras, C., Ferroli, P., Bugiani, O., and Broggi, G. (2005). Stimulation of the posterior hypothalamus for medically intractable impulsive and violent behavior. Stereotact. Funct. Neurosurg. 83, 63–66. doi: 10.1159/000086675
Golden, A. S., Haut, S. R., and Moshé, S. L. (2006). Nonepileptic uses of antiepileptic drugs in children and adolescents. Pediatr. Neurol. 34, 421–432. doi: 10.1016/j.pediatrneurol.2005.08.017
Hayes, J. P., Bigler, E. D., and Verfaellie, M. (2016). Traumatic brain injury as a disorder of brain connectivity. J. Int. Neuropsychol. Soc. 22, 120–137. doi: 10.1017/S1355617715000740
Heiden, P., Hoevels, M., Bayram, D., Baldermann, J. C., Schüller, T., Huys, D., et al. (2021). Connectivity patterns of deep brain stimulation targets in patients with Gilles de la Tourette syndrome. Brain Sci. 11:87. doi: 10.3390/brainsci11010087
Horn, A., and Kühn, A. A. (2015). Lead-DBS: a toolbox for deep brain stimulation electrode localizations and visualizations. Neuroimage 107, 127–135. doi: 10.1016/j.neuroimage.2014.12.002
Horn, A., Kühn, A. A., Merkl, A., Shih, L., Alterman, R., and Fox, M. (2017a). Probabilistic conversion of neurosurgical DBS electrode coordinates into MNI space. Neuroimage 150, 395–404. doi: 10.1016/j.neuroimage.2017.02.004
Horn, A., Reich, M., Vorwerk, J., Li, N., Wenzel, G., Fang, Q., et al. (2017b). Connectivity Predicts deep brain stimulation outcome in Parkinson disease. Ann. Neurol. 82, 67–78. doi: 10.1002/ana.24974
Huisman, S., Mulder, P., Kuijk, J., Kerstholt, M., van Eeghen, A., Leenders, A., et al. (2018). Self-injurious behavior. Neurosci. Biobehav. Rev. 84, 483–491. doi: 10.1016/j.neubiorev.2017.02.027
Jiménez, F., Soto, J. E., Velasco, F., Andrade, P., Bustamante, J. J., Gómez, P., et al. (2012). Bilateral cingulotomy and anterior capsulotomy applied to patients with aggressiveness. Stereotact. Funct. Neurosurg. 90, 151–160. doi: 10.1159/000336746
Kantzanou, M., Korfias, S., Panourias, I., Sakas, E. D., and Karalexi, M. A. (2021). Deep brain stimulation-related surgical site infections: a systematic review and meta-analysis. Neuromodulation 24, 197–211. doi: 10.1111/ner.13354
Kiloh, L. G., Gye, R. S., Rusworth, R. G., Bell, D. S., and White, R. T. (1974). Stereotactic amygdalotomy for aggressive behavior. J. Neurol. Neursurg. Psychiatry 37, 437–444. doi: 10.1136/jnnp.37.4.437
Li, N., Baldermann, J. C., Kibleur, A., Treu, S., Akram, H., Elias, G. J. B., et al. (2020). A unified connectomic target for deep brain stimulation in obsessive-compulsive disorder. Nat. Commun. 11:3364. doi: 10.1038/s41467-020-16734-3
Minshawi, N. F., Hurwitz, S., Fodstad, J. C., Biebl, S., Morriss, D. H., and McDougle, C. J. (2014). The association between self-injurious behavior and autism spectrum disorders. Psychol. Res. Behav. Manage. 7, 125–136. doi: 10.2147/PRBM.S44635
Narabayashi, H., and Uno, M. J. S. (1966). Long range results of stereotaxic amygdalotomy for behavior disorders. Confin. Neurol. 27, 168–171. doi: 10.1159/000103950
Quinn, T. J., Langhorne, P., and Stott, D. J. (2011). Barthel Index for stroke trials: development, properties, and application. Stroke 42, 1146–1151. doi: 10.1161/STROKEAHA.110.598540
Rizzi, M., Trezza, A., Messina, G., De Benedictis, A., Franzini, A., and Marras, C. E. (2017). Exploring the brain through posterior hypothalamus surgery for aggressive behavior. Neurosurg. Focus 43:E14. doi: 10.3171/2017.6.FOCUS17231
Rollnik, J. D. (2011). The early rehabilitation barthel index. Rehabilitation (Stuttg) 50, 408–411. doi: 10.1055/s-0031-1273728
Rossel, D. R., and Siever, L. J. (2015). The neurobiology of aggression and violence. CNS Spectr. 20, 254–279. doi: 10.1017/S109285291500019X
Sano, K., Yoshioka, M., Ogashiwa, M., Ishijima, B., and Ohye, C. J. S. (1966). Postero-medial hypothalamotomy in the treatment of aggressive behaviors. Confin. Neurol. 27, 164–167. doi: 10.1159/000103949
Schaltenbrand, G., and Wahren, W. (1977). Atlas for Stereotaxy of the Human Brain. 2nd edn. Stuttgart: Thieme.
Setsomop, K., Kimmlingen, R., Eberlein, E., Witzel, T., Cohen-Adad, J., McNab, J. A., et al. (2013). Pushing the limits of in vivo diffusion MRI for the Human Connectome Project. Neuroimage 80, 220–233. doi: 10.1016/j.neuroimage.2013.05.078
Smyser, C. D., Wheelock, M. D., Limbrick, D. D., Jr., and Neil, J. J. (2019). Neonatal brain injury and aberrant connectivity. Neuroimage 185, 609–623. doi: 10.1016/j.neuroimage.2018.07.057
Stafford, M., and Cavanna, A. E. (2020). Prevalence and clinical correlates of self-injurious behavior in Tourette syndrome. Neurosci. Biobehav. Rev. 113, 299–307. doi: 10.1016/j.neubiorev.2020.03.022
Sturm, V., Fricke, O., Bührle, C. P., Lenartz, D., Maarouf, M., Treuer, H., et al. (2013). DBS in the basolateral amygdala improves symptoms of autism and related self-injurious behavior: a case report and hypothesis on the pathogenesis of the disorder. Front. Hum. Neurosci. 6:341. doi: 10.3389/fnhum.2012.00341
Torres, C. V., Blasco, G., Navas García, M., Ezquiaga, E., Pastor, J., Vega-Zelaya, L., et al. (2021). Deep brain stimulation for aggressiveness: long-term follow-up and tractography study of the stimulated brain areas. J. Neurosurg. 134, 366–375. doi: 10.3171/2019.11.JNS192608
Tustison, N. J., Avants, B. B., and Gee, J. C. (2019). Learning image-based spatial transformation via convolutional neural networks: a review. Magn. Reson. Imaging 64, 142–153. doi: 10.1016/j.mri.2019.05.037
Wang, R., Benner, T., Sorensen, A. G., and Wedeen, V. J. (2007). Diffusion toolkit: a software package for diffusion imaging data processing and tractography. Proc. Int. Soc. Mag. Reson. Med. 15:3720. Available online at: http://www.trackvis.org/faq/2007_ISMRM_diffusion_toolkit.pdf.
Worbe, Y., Malherbe, C., Hartmann, A., Pélégrini-Issac, M., Messé, A., Vidailhet, M., et al. (2012). Functional immaturity of cortico-basal ganglia networks in Gilles de la Tourette syndrome. Brain 135, 1937–1946. doi: 10.1093/brain/aws056
Xiao, Y., Fonov, V., Chakravarty, M. M., Bériault, S., Al-Subaie, F., Sadikot, A., et al. (2017). A dataset of multi-contrast population-averaged brain MRI atlases of a Parkinson’s disease cohort. Data Brief 12, 370–379. doi: 10.1016/j.dib.2017.04.013
Yan, H., Elkaim, L. M., Venetucci Gouveia, F., Huber, J. F., Germann, J., Loh, A., et al. (2022). Deep brain stimulation for extreme behaviors associated with autism spectrum disorder converges on a common pathway: a systematic review and connectomic analysis. J. Neurosurg. . [Online ahead of print]. doi: 10.3171/2021.11.JNS21928
Keywords: self-injurious behavior, aggressiveness, deep brain stimulation, connectivity, psychosurgery
Citation: Heiden P, Weigel DT, Loução R, Hamisch C, Gündüz EM, Ruge MI, Kuhn J, Visser-Vandewalle V and Andrade P (2022) Connectivity in deep brain stimulation for self-injurious behavior: multiple targets for a common network? Front. Hum. Neurosci. 16:958247. doi: 10.3389/fnhum.2022.958247
Received: 31 May 2022; Accepted: 01 August 2022;
Published: 24 August 2022.
Edited by:
Michael S. Okun, University of Florida, United StatesReviewed by:
Takashi Morishita, Fukuoka University, JapanCopyright © 2022 Heiden, Weigel, Loução, Hamisch, Gündüz, Ruge, Kuhn, Visser-Vandewalle and Andrade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Andrade, cGFibG8uYW5kcmFkZS1tb250ZW1heW9yQHVrLWtvZWxuLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.