
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Hum. Neurosci. , 04 August 2022
Sec. Brain Imaging and Stimulation
Volume 16 - 2022 | https://doi.org/10.3389/fnhum.2022.940759
This article is part of the Research Topic TMS application in both health and disease View all 13 articles
 Rebecca Strafella1,2
Rebecca Strafella1,2 Robert Chen1,3,4Tarek K. Rajji1,2,5,6Daniel M. Blumberger1,2,5
Robert Chen1,3,4Tarek K. Rajji1,2,5,6Daniel M. Blumberger1,2,5 Daphne Voineskos1,2,3,5*
Daphne Voineskos1,2,3,5*Electroencephalography (EEG) is a non-invasive method to identify markers of treatment response in major depressive disorder (MDD). In this review, existing literature was assessed to determine how EEG markers change with different modalities of MDD treatments, and to synthesize the breadth of EEG markers used in conjunction with MDD treatments. PubMed and EMBASE were searched from 2000 to 2021 for studies reporting resting EEG (rEEG) and transcranial magnetic stimulation combined with EEG (TMS-EEG) measures in patients undergoing MDD treatments. The search yielded 966 articles, 204 underwent full-text screening, and 51 studies were included for a narrative synthesis of findings along with confidence in the evidence. In rEEG studies, non-linear quantitative algorithms such as theta cordance and theta current density show higher predictive value than traditional linear metrics. Although less abundant, TMS-EEG measures show promise for predictive markers of brain stimulation treatment response. Future focus on TMS-EEG measures may prove fruitful, given its ability to target cortical regions of interest related to MDD.
Major depressive disorder (MDD) is a leading cause of disability worldwide and is increasing in prevalence (Friedrich, 2017). Unfortunately, little progress has been made in identifying biological indicators of treatment response, and much intervention is via trial-and-error. While some possible neurobiological indicators of response have been identified using genetic and imaging studies (reviewed Belmaker, 2008; Kupfer et al., 2012), a less-costly, non-invasive option is electroencephalography (EEG), which indexes neural activity with high temporal resolution (Berger, 1929). EEG has several investigational uses, characterizing cortical activity after perturbation, or reflecting frequency bands associated with specific cognitive patterns (Freeman and Quiroga, 2013). The combination of transcranial magnetic stimulation with EEG (TMS-EEG) has sparked interest as a way to record direct and downstream cortical responses to a targeted magnetic stimulus (Farzan et al., 2016).
EEG provides multiple avenues to identify putative markers differentiating treatment responders and non-responders in MDD. Common interventions for MDD include pharmacotherapy, psychotherapy, and brain stimulation (Voineskos et al., 2020). However, there is a lack of synthesis of evidence in the MDD literature regarding the utility of EEG indices as markers of treatment response. To date, one meta-analysis has focused solely on quantitative EEG to examine markers of treatment response (Widge et al., 2019), but did not find reliable indices or include other types of EEG investigations, such as TMS-EEG. Due to the breadth of EEG markers in the existing literature, there is a need to combine evidence to understand which markers consistently demonstrate the potential for clinical utility across therapeutic interventions for MDD. Identifying potential biological predictors of response will hopefully lead to a departure from the trial-and-error approach of MDD treatment, although several steps remain before declaring this achievement. Below, we will briefly define both resting EEG (rEEG) and TMS-EEG prior to presenting our systematic review of relevant findings.
Resting EEG (rEEG) indexes brain activity without stimulus presentation, typically via 64 electrodes distributed with the 10–20 system (Jasper, 1958). REEG frequency bands characterize the signal in delta to gamma domains (Niedermeyer, 1999). The low frequency delta band (<4 Hz) appears in stage 3 non-rapid eye movement sleep and is not typically seen in rEEG (Amzica and Steriade, 1998). Theta (4–8 Hz) is related to emotional processing and internal focus (Aftanas and Golocheikine, 2001; Aftanas et al., 2002). Frontal theta activity may reflect neurotransmission to and from the anterior cingulate cortex (ACC) (Asada et al., 1999), regions implicated in MDD (Spellman and Liston, 2020). The alpha (8–12 Hz) band appears during relaxation and is the most dominant band present in occipital or posterior regions (Niedermeyer, 1999). In MDD, the presence of alpha indicates brain regions with lower activity (Bruder et al., 1997). Beta (12–30 Hz) and gamma bands (>30 Hz) are considered “high-frequency”, reflecting alertness and concentration (Abhang et al., 2016) and attention and executive functioning (Freeman and Quiroga, 2013), respectively. Deciphering the relevance of frequency band activity may have potential for MDD response markers.
Transcranial magnetic stimulation (TMS) non-invasively stimulates the brain, inducing electric currents in neurons via electromagnetic induction (i.e., Faraday's law) (Barker et al., 1985). The TMS stimulus is thought to act on inhibitory interneurons and results in the depolarization of pyramidal cells (Kobayashi and Pascual-Leone, 2003), which can be captured via EEG. The combination of TMS-EEG then provides an accurate window into the direct localized and downstream cortical effects of the TMS pulse, and can provide measurable output for cortical regions outside of the motor and somatosensory cortices. Single-pulse TMS-EEG produces TMS evoked potentials (TEPs) reflecting excitatory and inhibitory neurotransmission (Farzan et al., 2016) and can index both inter and intra-regional connectivity between cortico-cortical and cortico-subcortical areas (Daskalakis et al., 2012). Unlike rEEG, TMS-EEG allows for both direct stimulation and recording of output from the cortical region of interest. Both cortical responses at the stimulated region, as well as downstream effects can then be interpreted. These measures have identified cortical abnormalities in MDD, that may be used as markers of treatment response.
We conducted a formal narrative synthesis of the included studies, which focused on rEEG and TMS-EEG indexing the effects of antidepressant interventions (pharmacotherapy, brain stimulation, other therapies) on resulting outcomes (response or remission from a major depressive episode). The objectives were to: report changes in EEG measures of treatment; compare changes in EEG measures following treatment in responders and non-responders; report whether EEG measures at baseline predicted response.
PubMed and EMBASE were searched between January 1st, 2000 and December 31st, 2021 for publications studying treatment effects (i.e., pharmacotherapies and non-pharmacotherapies) on EEG (rEEG and TMS-EEG) in patients with MDD. Search terms are detailed in the Appendix. Results were filtered to only include human studies reported in English.
Studies included examined subjects with unipolar MDD (DSM-IV and DSM-5 criteria) who underwent antidepressant treatment in conjunction with EEG measures. Studies must have reported rEEG or TMS-EEG measures before, during, or post-treatment.
Case studies, review articles, protocols, posters, and conference abstracts were excluded (i.e., incorrect design). Studies reporting on animal populations, healthy subjects, bipolar depression, or conditions other than unipolar MDD were excluded (i.e., incorrect patient population). Non-therapeutic interventions were also excluded (i.e., incorrect intervention). Studies reporting antidepressant effects using techniques other than EEG (i.e. magnetoencephalography and electromyography), were excluded (i.e., incorrect EEG type). Sleep EEG, ictal EEG, neurofeedback studies, resting connectivity EEG, event-related EEG, and machine learning studies were excluded for focus and brevity (i.e., incorrect outcome). For the purpose of this review, incorrect was used to denote criteria that deemed to be out of scope.
Two study authors (RS, DV) conducted an independent literature search using pre-defined inclusion and exclusion criteria following duplicate removal. Covidence (www.covidence.org), an internet-based software, facilitated screening and extraction. Following initial screening, eligible studies underwent full-text review. Conflicts between authors were resolved by discussion. Approved studies were then moved to data extraction.
Quality of evidence assessment was performed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group methodology (Schünemann et al., 2008). Quality was marked with four levels: high, moderate, low, very low. High studies were randomized, double-blinded, and placebo-controlled; moderate were randomized without blinding; low were non-randomized with a placebo or control group; very low were non-randomized without a placebo or control group. Studies marked Very low were excluded to focus on higher quality, and reliable designs.
Figure 1 provides full information on the study selection process, using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
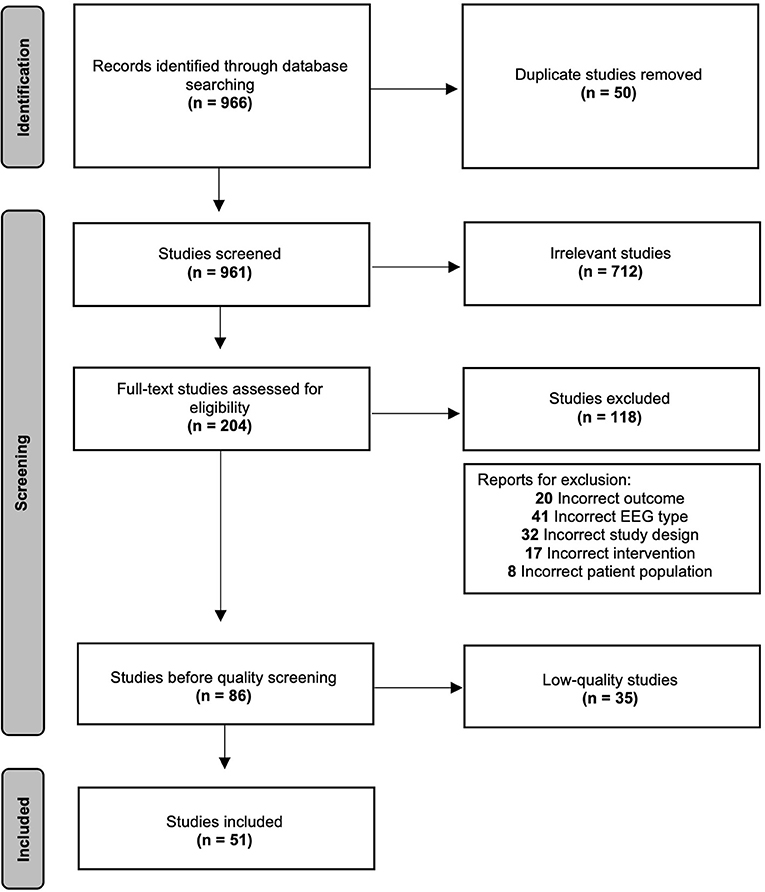
Figure 1. Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram.
Search terms yielded 966 studies after applying filters, 916 after removing duplicates. Primary screening excluded 712 for irrelevance based on the abstract. Two hundred and four underwent full-text review. One hundred and eighteen were excluded for incorrect design, outcomes, EEG type, patient population, or intervention. For more details on reasons for exclusion, see Section Exclusion criteria. Thirty-five studies had a Very low quality assessment and were removed for brevity. Overall, 51 studies underwent qualitative synthesis.
Quality ratings are included in Tables 1, 2. After exclusion of Very low quality studies, the vast majority of studies were marked as High, followed by Moderate and Low ratings. The following sections are presented in order of decreasing quality rating.
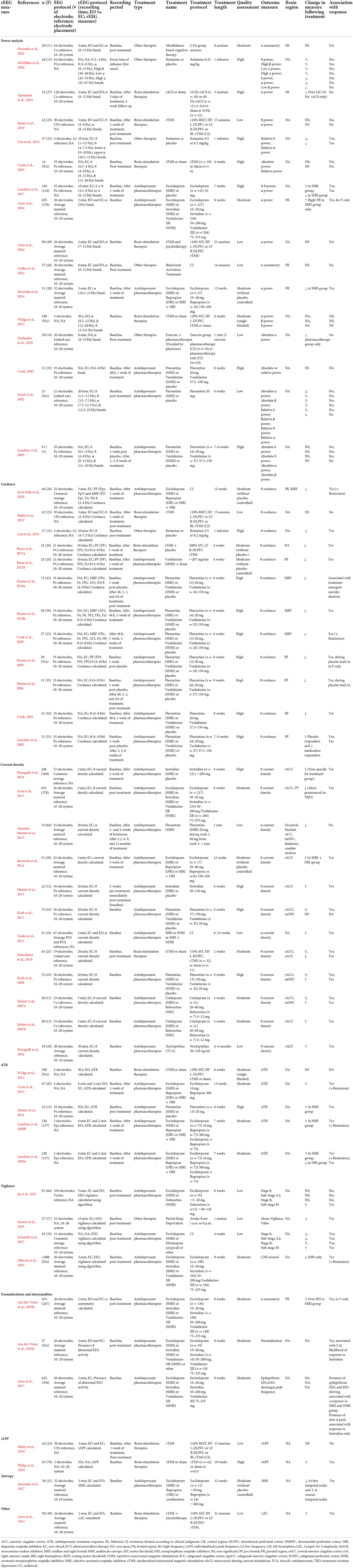
Table 1. Resting EEG outcomes for antidepressant, brain stimulation, and other studies.
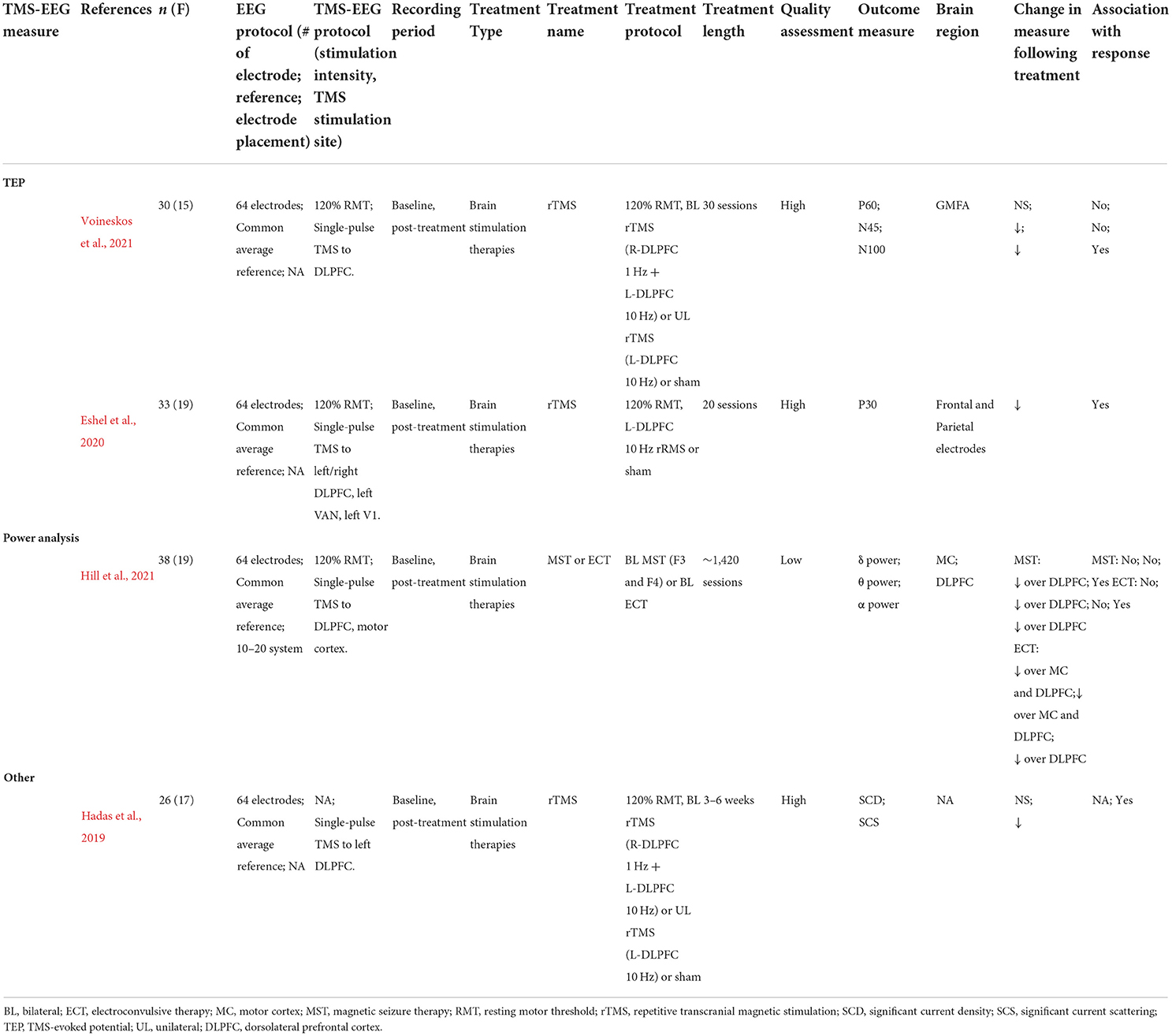
Table 2. TMS-EEG outcomes for brain stimulation studies.
Forty-seven studies examined rEEG markers of treatment response to pharmacotherapies, brain stimulation therapies, and other therapies (Table 1). These studies reported quantitative rEEG measures such as power analysis (Cook, 2002; Knott et al., 2002; Deslandes et al., 2010; Widge et al., 2013; Gollan et al., 2014; Jaworska et al., 2014, p. 201; Leuchter et al., 2002, 2017; Arns et al., 2014, 2016; Alexander et al., 2019; Bailey et al., 2019; Cao et al., 2019; Cook et al., 2019; McMillan et al., 2020; Szumska et al., 2021), cordance (Cook, 2002; Leuchter et al., 2002; Hunter et al., 2006, 2009, 2010a,b; Cook et al., 2009; Bares et al., 2015a; Bailey et al., 2019; Cao et al., 2019; de la Salle et al., 2020), current density (Pizzagalli et al., 2001, 2018; Mulert et al., 2007a,b; Korb et al., 2009, 2011; Narushima et al., 2010; Tenke et al., 2011; Hunter et al., 2013, p. 201; Jaworska et al., 2014; Almeida Montes et al., 2015; Arns et al., 2015), a weighted combination of alpha and theta power compared over time (termed: antidepressant treatment response (ATR) index) (Leuchter et al., 2009a,b; Hunter et al., 2011; Cook et al., 2013; Widge et al., 2013), vigilance (Olbrich et al., 2016; Schmidt et al., 2017; Sander et al., 2018; Ip et al., 2021), normalizations and abnormalities (Arns et al., 2017; van der Vinne et al., 2019a,b), individualized alpha-peak frequency (iAPF) (Bailey et al., 2019; Philip et al., 2019), entropy (Jaworska et al., 2017), and other algorithms (Arns et al., 2014).
rEEG studies included a variety of pharmacotherapies, brain stimulation therapies, and other therapies. Pharmacotherapy studies used various dosages, schedules, and antidepressant classes of medication [serotonin-reuptake inhibitors (SSRI), serotonin-norepinephrine reuptake inhibitors (SNRI), tricyclic antidepressants (TCA), dopamine reuptake inhibitors (DRI), mirtazapine, or combinations]. Some used fixed dosages and treatment lengths, others followed naturalistic designs. Brain stimulation interventions included repetitive transcranial magnetic stimulation (rTMS), synchronized transcranial magnetic stimulation (sTMS), and transcranial alternating current stimulation (tACS). Treatment parameters varied by stimulation target, intensity, and number of treatments. Other therapies included IV ketamine, psychotherapies (i.e., mindfulness-based cognitive therapy, behavioral activation treatment), aerobic training, and partial sleep deprivation. Across treatment types, rEEG protocols varied in recording length, electrode placement, number of electrodes of interest, eyes closed vs. open and outcome measures. The following section will focus on reported rEEG measures by treatment type.
Frequency bands are computed by absolute or relative band power. Absolute band power measures all activity within a specific range, whereas relative band power expresses band power as a percentage of total signal power.
Three high quality rated studies reported power analysis findings. One week of SSRI resulted in decreased relative alpha power and increased relative delta-theta (Leuchter et al., 2017). However, there were no significant results in patients randomized to SSRI, SNRI or placebo (Cook, 2002; Leuchter et al., 2002). One moderate quality rated study reported higher frontal alpha absolute power at baseline in SSRI, DRI or combination pharmacotherapy responders which decreased in the SSRI group after 1 week (Jaworska et al., 2014). Additionally, female SSRI responders and remitters showed greater baseline right-sided alpha power (Arns et al., 2016). In one low rated study in men only, both SSRI and placebo resulted in increased relative and absolute beta, but decreased alpha power after 6 weeks (Knott et al., 2002). Overall, alpha findings warrant more exploration, however, it remains unclear whether other frequency bands show promise due to the variability in these results.
Two high-quality studies reported power analysis outcomes. Patients randomized to receive 10 Hz tACS for 5 sessions showed decreased frontal alpha power over the left hemisphere, which was not noted in patients who received 40 Hz or sham tACS (Alexander et al., 2019). In contrast, there were no changes in absolute or relative power bands following 6 weeks of sTMS (Cook et al., 2019). One moderately rated HF L-DLPFC rTMS study (Widge et al., 2013) reported no absolute or relative power differences between responders and non-responders at baseline. In low quality rated studies, no differences in alpha power appeared between responders and non-responders to HF L-DLPFC or LF R-DLPFC rTMS combined with psychotherapy (Arns et al., 2014). Further, there were no changes in theta or alpha power following 3 weeks of HF L-DLPFC, LF R-DLPFC, or combination rTMS (Bailey et al., 2019). To conclude, most brain stimulation studies did not find significant power analysis findings.
Two high-quality studies reported IV ketamine effects on power analysis (Cao et al., 2019; McMillan et al., 2020). Post-infusion, theta, high-beta, and gamma power increased, whereas delta, alpha, and low-beta power decreased. However, no relationship was found between any bands and antidepressant response (McMillan et al., 2020). In contrast, in an earlier study, decreases in relative theta and alpha power following IV ketamine infusion were associated with treatment response (Cao et al., 2019). One moderate quality rated study following 8 sessions of mindfulness-based cognitive therapy showed no change in frontal alpha power over either cortical hemisphere (Szumska et al., 2021). Two low-rated studies reported conflicting results. Absolute alpha power decreased following 1-year of pharmacotherapy alone, but not in patients receiving pharmacotherapy plus aerobic training (Deslandes et al., 2010). In contrast, there was no change in frontal alpha power following 16 sessions of behavioral activation therapy (Gollan et al., 2014). As such, decreased alpha power appears to consistently be associated with treatment response across diverse modalities of antidepressant intervention.
Cordance is quantified by integrating absolute and relative EEG power measures, and is strongly associated with cerebral blood perfusion (Leuchter et al., 1994, 1999). Similar to functional neuroimaging, it is used to quantify abnormalities in brain activity, namely over dysregulated regions in MDD such as the frontal cortex (Hunter et al., 2007).
Seven high quality rated studies reported cordance. Treatment response was associated with decreased prefrontal (PF) theta cordance after 48 h and 1 week of SSRI or SNRI treatment (Cook, 2002). Similar results in midline and right frontal regions emerged after 8 weeks of SSRIs or SNRIs (Cook et al., 2009; Hunter et al., 2010b). Interestingly, decreases in midline and right frontal theta cordance were also associated with medication-induced suicidal ideation (Hunter et al., 2010a). PF theta cordance decrease during placebo lead-in was also associated with greater response (Hunter et al., 2006), especially in female participants (Hunter et al., 2009), but the opposite trend was found for placebo responders (Leuchter et al., 2002). Two moderately rated studies examined theta cordance. One week after SNRI initiation, decreased PF theta cordance predicted greater response (AUC = 0.89) (Bares et al., 2015b). This relationship also appeared 1 week after initiation of SSRI, DRI, or combination, in both PF and midline and right frontal regions (de la Salle et al., 2020). Taken together, the above evidence demonstrates that decreased theta cordance after 1 week of pharmacotherapy may be a reliable measure of forthcoming antidepressant response.
No high quality rated studies were found addressing cordance measures with regard to brain stimulation. One moderately rated study reported decreased PF theta cordance following high-frequency (HF) left dorsolateral prefrontal cortex (DLPFC) rTMS with placebo in treatment-resistant depression (TRD) (Bares et al., 2015b). Higher PF theta cordance at baseline was correlated with a greater reduction in symptoms following 4 weeks of rTMS, and PF theta cordance values decreased in responders 1 week post-treatment (Bares et al., 2015b). One low quality rated study following 3 weeks of HF L-DLPFC, LF R-DLPFC, or combination rTMS found no significant changes in theta cordance (Bailey et al., 2019). Despite this conflicting evidence, the moderately rated brain stimulation study is more in line with trends of decreased PF theta cordance that were noted with antidepressants.
Only one study met criteria for this section, a high quality rated investigation which reported decreased theta cordance in responders after IV ketamine infusion (Cao et al., 2019). While singular, these findings echo the trend from pharmacotherapy and brain stimulation studies.
Current density quantifies rEEG activity, and is positively correlated with glucose metabolism (Pizzagalli et al., 2001). In MDD, abnormal metabolism levels in the rostral anterior cingulate cortex (rACC) and frontal regions have been related to symptom presentation (Martinot et al., 2011), and may be studied using current density.
Four high quality rated studies reported theta current density. At baseline, responders showed higher rACC (SSRIs and SNRIs) and medial orbitofrontal cortex (mOFC) (SNRIs) (Korb et al., 2009; Hunter et al., 2013) theta current density, although another study did not replicate findings (Korb et al., 2011). Responders in both placebo and TCA groups showed elevated rACC at baseline and after 1 week of pharmacotherapy (Pizzagalli et al., 2018). Four moderate quality rated studies reported theta current density. In two, pharmacotherapy responders showed baseline elevated mOFC (NRIs and SSRIs) and rACC (NRIs) theta current density (Mulert et al., 2007a,b). DRI, but not SSRI responders, had higher baseline rACC theta current density. Responders showed increased rACC theta current density after 1 week of combination SSRI and DRI treatment (Jaworska et al., 2014). In contrast, at baseline and 8 weeks after SSRI or SNRI initiation, non-responders exhibited higher rACC and frontal theta current density, especially in non-responders with treatment resistant depression (Arns et al., 2015). Three low quality studies reported theta current density. One linked elevated baseline rACC theta current density with TCA response (Pizzagalli et al., 2001). Another, following 1 year of SSRIs, showed that patients exhibited lower alpha current density at each follow-up visit compared to healthy controls, despite some subjects reaching remission (Almeida Montes et al., 2015). In contrast, responders to SSRI, SNRI, or SSRI plus NDRI exhibited higher alpha current density at baseline compared to non-responders and healthy controls (Tenke et al., 2011). Given the above evidence, higher baseline theta current density shows clear promise in predicting pharmacotherapeutic response.
One moderately rated randomized, sham-controlled HF L-DLPFC rTMS trial in patients with vascular depression recorded theta current density in the subgenual anterior cingulate cortex (sACC) and rACC (Narushima et al., 2010). At baseline, responders showed higher theta current density in sACC than non-responders, but no significant rACC findings were reported. No high or low quality rated studies were found in the literature review, but the single brain stimulation study reported findings consistent with antidepressant studies.
No studies reported on current density measures.
The antidepressant treatment response (ATR) is a non-linear weighted combination of theta and alpha power, both relative and absolute, measured at baseline and 1 week after initiation (Leuchter et al., 2009a,b). However, it is unclear how the ATR directly reflects brain activity (Wade and Iosifescu, 2016).
One high quality rated study reported higher ATR predicted both response and remission after 8 weeks of SSRIs (Hunter et al., 2011). Three moderately rated studies reported ATR levels following SSRI, DRI, or combination (Leuchter et al., 2009a,b; Cook et al., 2013). SSRI responders who underwent 7 weeks (Leuchter et al., 2009a,b) and 13 weeks (Cook et al., 2013) of treatment showed higher ATR values than non-responders, but findings were inconsistent for DRIs. Overall, higher ATR may predict response to some antidepressant pharmacotherapies.
One moderately rated study reported no association between ATR and response following HF L-DLPFC rTMS (Widge et al., 2013).
No studies reported on the ATR measure.
EEG vigilance is a validated algorithm using rEEG frequency bands to quantify brain arousal into specific stages (Olbrich et al., 2009). Individuals with MDD typically show higher arousal patterns than healthy individuals (Hegerl et al., 2012).
No high-quality rated studies were present in the literature review. One moderately rated study recorded vigilance as an index of central-nervous system arousal, and found decreased arousal in patients following 8-weeks of SSRIs, but not SNRI (Olbrich et al., 2016). Two low quality rated studies recorded vigilance following SSRIs, mirtazapine, SNRIs, or other medications (Schmidt et al., 2017; Ip et al., 2021). At baseline, responders had high vigilance in relaxed wakeful states and low vigilance in drowsy states, trends which were reversed after 4 weeks (Schmidt et al., 2017) and 8 weeks of treatment (Ip et al., 2021). Taken together, vigilance measures indicate that responders to various pharmacotherapies show high arousal at baseline that may be reversed following treatment.
No studies reported on vigilance measures.
One low quality rated study which calculated mean vigilance values (MVV) as a measure of average brain arousal following partial sleep deprivation therapy showed that responders were characterized by lower MVV compared to non-responders (Sander et al., 2018).
Abnormal EEG activity is characterized by slowing, epileptiform or paroxysmal activity, and alpha peak frequencies (APF) (Noachtar et al., 1999; Niedermeyer, 2005). In contrast, normalization occurs when abnormalities disappear or return to stable recording.
Three moderately rated studies reported EEG normalization or abnormalities. Following SSRIs or SNRIs, epileptiform activity or slowing was negatively correlated with response (Arns et al., 2017). Slow APF was associated with SSRI response only (Arns et al., 2017). EEG normalization was noted in SSRI but not SNRI responders (van der Vinne et al., 2019a). Higher right-sided alpha power at baseline and after 8 weeks of SSRI was a stable marker associated with response in females, but not SNRI response (van der Vinne et al., 2019b). No high or low quality rated studies were present in the literature review. While there were inconsistencies, EEG abnormalities and normalization and stability may predict SSRI response.
No studies reported on EEG normalizations and abnormalities.
No studies reported on EEG normalizations and abnormalities.
Individualized alpha peak frequency (iAPF) is used to quantify the average alpha power across frontal electrodes in eyes open and eyes closed conditions (Doppelmayr et al., 1998). It has been used to capture inter- and intra-individual differences in alpha frequency (Haegens et al., 2014).
No studies reported on the iAPF measure.
One high quality study demonstrated that higher iAPF at baseline was associated with response to 10 weeks of sTMS, compared to sham (Philip et al., 2019). In contrast, iAPF did not appear to have association with response after multiple therapeutic rTMS paradigms (HF L-DLPFC, LF R-DLPFC rTMS or BL rTMS) in a low quality rated study (Bailey et al., 2019). Thus, the predictive value of iAPF may be different depending on the type of brain stimulation delivered.
No studies reported on the iAPF measure.
Multiscale entropy (MSE) quantifies brain signal variability over fine or coarse time scales (Costa et al., 2005), and may be used to study global and local connectivity disturbances in MDD (Jaworska et al., 2017).
Only one moderately rated study recorded MSE with SSRI, DRI or combination pharmacotherapy. Responders were characterized by decreased baseline MSE at fine and increased MSE at coarser temporal scales (Jaworska et al., 2017).
No studies reported on entropy measures.
No studies reported on entropy measures.
The Lempel-Ziv Complexity (LZC) value quantifies the complexity of the EEG signal (see Bravi et al., 2011), to understand whether non-linear measures can better characterize cortical temporal patterns in MDD.
No studies reported on the LCZ value.
Only one low quality rated study reported on this measure. In patients undergoing HF L-DLPFC or LF R-DLPFC rTMS combined with psychotherapy (Arns et al., 2014), LZC increased from minute 1 to 2 of the baseline EEG in responders and decreased in non-responders. Further examination of LZC may further clarify its value as an EEG marker of brain stimulation response.
No studies reported on the LCZ value.
No studies reported TMS-EEG outcome with antidepressant pharmacotherapies or other therapies. Four studies reported brain stimulation effects on TMS-EEG measures (Table 2). From the limited number of studies, TMS-EEG outcomes included TEP components (Eshel et al., 2020; Voineskos et al., 2021), power analysis (Hill et al., 2021), and other novel TMS-EEG algorithms (Hadas et al., 2019).
TMS-EEG studies mainly analyzed the effects of therapeutic rTMS, although the ECT and magnetic seizure therapy (MST) were also explored. Stimulation targets and duration/number of treatment sessions varied across studies. As well, diverse stimulation targets were applied in the investigatory TMS-EEG protocols. Due to the low number of studies, synthesis was limited.
TEPs over the motor cortex and DLPFC demonstrate replicable peaks (i.e., P30, N45, P60, N100) characterized by polarity and latency (Freeman and Quiroga, 2013). Several components have been linked to specific neurotransmitter receptor activity, including the P60 to glutamatergic receptor activity (Noda et al., 2017; Belardinelli et al., 2021), and N45 and N100 to gamma-aminobutyric acid (GABA) receptor activity (Farzan et al., 2013; Premoli et al., 2014; Rogasch et al., 2015).
Two high quality rated investigations reported on the effects of a therapeutic course of rTMS on TEP components. Following 20 sessions of HF L-DLPFC rTMS, P30 amplitude decreased over the left frontal and parietal electrodes and was correlated with better clinical outcomes (Eshel et al., 2020). Similarly, the N45 and N100 amplitude decreased following 30 sessions of HF L-DLPFC or sequential bilateral rTMS (LF R-DLPFC rTMS followed by HF L-DLPFC rTMS), but there was no change to P60 (Voineskos et al., 2021). As well, the N100 decrease was related to improved depression symptoms post-treatment (Voineskos et al., 2021). Given the different components reported, high-quality replication studies are needed to elucidate the predictive ability of the P30, N45, and N100.
TMS-EEG power analysis is very similar to resting EEG power analysis, with frequency bands defined from alpha to theta.
One low-quality rated study reported power analysis from TMS-EEG at baseline and after MST or ECT for TRD (Hill et al., 2021). Both treatments resulted in decreased delta and theta power over DLPFC (Hill et al., 2021). However, only ECT resulted in reduced alpha power over the DLPFC, and decreased delta and theta power over motor cortex (Hill et al., 2021). To this end, it is possible that MST effects were localized whereas ECT effects appear generalized over the cortex. As well, combined ECT and MST datasets showed a relationship between reduced alpha power and depression symptom improvements following treatment.
Significant current density (SCD) and significant current scatter (SCS) are measures of subgenual cingulate cortex (SGC) excitability, and DLPFC-SGC effective connectivity, respectively (Hadas et al., 2019). Hyperactivity of the SGC and DLPFC-SGC connectivity have repeatedly been implicated in the pathophysiology of MDD (Mayberg et al., 1999).
One high quality rated study examined SCS and SCD in patients with TRD. Here, the effects of HF L-DLPFC, sequential bilateral rTMS (LF R-DLPFC rTMS followed by HF L-DLPFC rTMS) or sham for 3–6 weeks were compared (Hadas et al., 2019). After active rTMS, SCS change and change in depression severity were positively correlated (Hadas et al., 2019). Further, after active rTMS, both P60 and P200 TEP component SCD decreased (Hadas et al., 2019). Given these results, TMS-EEG connectivity measures should be further explored in relation to treatment response.
We have presented a synthesis of existing literature focused on EEG markers of treatment response in MDD. In studies focused on rEEG markers, both theta cordance and theta current density consistently show potential as predictors of response for multiple modalities of MDD treatment. Decreased prefrontal theta cordance 1-week post-treatment was robust in predicting pharmacotherapy response, regardless of antidepressant medication class. The same trend was seen in higher quality brain stimulation and other therapy studies. Thus, theta cordance appears to be a reliable measure, especially for pharmacotherapies, perhaps in part due to the larger volume of studies focused on this intervention. Additionally, higher baseline theta current density may also have predictive value in pharmacotherapy response, with less existing evidence for brain stimulation interventions. In antidepressant studies, these findings were noted in rACC (Pizzagalli et al., 2001; Mulert et al., 2007b; Korb et al., 2009; Hunter et al., 2013; Jaworska et al., 2014) and mOFC (Mulert et al., 2007b; Korb et al., 2009). In contrast, alpha current density showed inconsistent value (Tenke et al., 2011; Almeida Montes et al., 2015). To this end, the replication of theta current density across higher-rated quality studies reinforces its potential as a predictive measure. These findings are encouraging given the biological implications of the theta band in MDD. Theta is usually most prominent in fronto-central regions, specifically the ACC and frontal cortex, both shown to be hypoactive in MDD (Asada et al., 1999). As theta is thought to represent drowsiness and low levels of cortical activation (Kropotov, 2016), it follows that this marker may hold high promise in our understanding of MDD. Thus, we encourage future biomarker guided clinical trials to verify theta markers of treatment response, specifically theta current density and theta cordance, as both show high potential to serve clinical utility in the treatment of MDD.
When examining power analysis, decreases in alpha power were the most consistently reported following treatment with SSRI (Knott et al., 2002; Jaworska et al., 2014; Leuchter et al., 2017), 10 Hz-tACS (Alexander et al., 2019), and IV Ketamine (Cao et al., 2019; McMillan et al., 2020). Thus, this measure may serve as a broad marker across treatment types, although further high-quality replication studies are needed. The remaining frequency bands (delta, theta, beta, and gamma) were reported in limited studies, with variable treatment types and inconsistent findings. Nevertheless, future focus on the alpha band is warranted given its ability to reflect inactivity of brain regions in MDD (Bruder et al., 1997). Previous research has linked the left frontal cortex to hypoactivity, reflected by high alpha power and reduced approach behavior (i.e., positive emotions) (Davidson, 1992). In contrast, the opposite trend is found over the right frontal cortex, reflected by low alpha power and increased withdrawal behavior (i.e., negative emotions). Taken together, the linkage between alpha power, cortical activity, and behavioral manifestations in MDD indicate the potential of this measure being extended to help guide treatment. Alpha band guided treatments have already proved useful in novel closed-loop neuromodulation techniques (Zrenner et al., 2016, 2020). Alpha oscillation-synchronized rTMS appears to improve treatment efficacy and may prove useful in personalizing therapeutic rTMS parameters (Zrenner et al., 2016, 2020). Phase synchronization has also been explored with the theta rhythm in healthy subjects, but requires replication in MDD populations undergoing therapeutic rTMS as a method for novel personalized treatments (Gordon et al., 2021). Additionally, sleep EEG power analysis may prove fruitful in identifying frequency band markers of MDD treatment response. Since the brain evidently behaves differently in wakeful and sleep states, especially for lower frequency bands, there is likely added value in exploring these markers in patients undergoing MDD interventions during sleep (Olbrich and Arns, 2013).
There were inconsistent findings across multiple treatment modalities with the remaining rEEG measures. First, higher ATR was replicated in responders or remitters to SSRIs (Leuchter et al., 2009a; Hunter et al., 2011), but was inconsistent for other medication classes such as DRIs (Leuchter et al., 2009b; Hunter et al., 2011), and in brain stimulation (Widge et al., 2013). Second, EEG abnormality measures were inconsistent, possibly due to high variability in selected outcome measures. SSRI response favored low EEG abnormalities and higher stability at baseline, but these were not predictive of SNRI response (Arns et al., 2017; van der Vinne et al., 2019a,b). Third, the different vigilance outcomes reported hindered the synthesis of results, but most studies reported that responders to various pharmacotherapies showed high brain arousal at baseline (Olbrich et al., 2016; Schmidt et al., 2017; Ip et al., 2021). Finally, very few studies reported iAPF (Bailey et al., 2019; Philip et al., 2019), entropy (Jaworska et al., 2017), and LCZ (Arns et al., 2014). While promise may remain within these measures, clear future directions cannot be gleaned from this synthesis of the literature.
In contrast, there were relatively few TMS-EEG studies to review, and all were focused on brain stimulation. Of the four studies included, three were high-quality, reflecting the high promise of TMS-EEG as a repository for neurophysiological biomarkers across brain stimulation modalities. rTMS appears to modulate DLPFC-SGC connectivity in parallel with improvements in MDD symptoms (Hadas et al., 2019). Additionally, better clinical outcomes were associated with decreased P30 amplitude (Eshel et al., 2020), and N100 amplitude (Voineskos et al., 2021) following active HF L-DLPFC and BL rTMS. While the biological association of the P30 is still unknown, the N100 seems to be linked to GABAergic receptor activity (Farzan et al., 2013; Premoli et al., 2014; Rogasch et al., 2015), a neurotransmitter highly implicated in the pathophysiology of MDD (Luscher et al., 2011). One low-quality study reported that decreased alpha power following MST or ECT was related to clinical response (Hill et al., 2021), adding to rEEG evidence of alpha band predictive power. There were three additional articles from our search that explored TMS-EEG effects following MST and ECT, however, they were deemed very Low quality and reported different outcomes, limiting synthesis (Casarotto et al., 2013; Miyauchi et al., 2019; Hadas et al., 2020). Overall, the high quality findings indicate that TMS-EEG measures may serve as MDD markers of response in the future.
There were some limitations to the literature reviewed. While non-linear rEEG quantitative algorithms (i.e., theta cordance, theta current density) show higher predictive value than traditional linear metrics, in part due to the non-linear behavior of brain function (Elbert et al., 1994), a recent meta-analysis calls the reliability of these indices into question, given the lack of direct replication studies and under-reporting of negative results (Widge et al., 2019). Further, evidence of biological linkages between rEEG measures and MDD symptomatology should also be verified using other modalities (i.e., imaging) or correlational studies before implementing these markers into clinical practice. A potential way of relieving these issues is by exploring novel computational and modeling approaches, which have gained traction. Cross-validated machine learning combining rEEG and mood measures show promise in distinguishing rTMS responders (Bailey et al., 2019). As well, a recent machine learning rEEG study differentially predicted response to SSRIs vs. low-frequency rTMS (Wu et al., 2020), which has generated much discussion on generalizability (Michel and Pascual-Leone, 2020; Nilsonne and Harrell, 2021; Wu et al., 2021). As such, while traditional rEEG measures are well documented, future studies may benefit from focusing on more complex indices.
A potential future direction of TMS-EEG markers may be in predicting specific MDD symptom improvements, as was shown by TMS-EEG indicators of suicidal ideation remission following MST (Sun et al., 2016). As well, combining TMS-EEG measures with other predictors of treatment response, such as rEEG outcomes or symptom presentation, using machine learning is another promising avenue that may serve clinical utility (Wu et al., 2020). Theta-burst stimulation (TBS), a novel rTMS therapy that produces significant antidepressant effects in patients with TRD (Blumberger et al., 2018), provides a further field for marker exploration with TMS-EEG. Notably, TBS builds on the concept of theta-gamma coupling, first proposed in animal models (Larson et al., 1986), a potential method of neural communication between brain regions thought to underly the basis of learning and memory (Lisman and Jensen, 2013). Taken together, TMS-EEG time-frequency analysis may be used to examine this theory by measuring changes in frequency power markers before and after TBS. Overall, TMS-EEG offers a novel area for discovery, offering replicable indices of cortical reactivity and connectivity that should be explored by future studies.
This review calls for more placebo-controlled, high-powered, replication studies to identify response markers for MDD treatments. Future EEG studies focusing on brain stimulation and novel therapeutics may lead to further understanding of neurophysiological treatment effects. We suggest a focus on TMS-EEG, given its potential to specifically target brain regions relevant to MDD. Specifically, emphasis on automation of TMS-EEG techniques and outcomes may eliminate variability in results, which can allow for more widespread clinical use in the future. In addition, rEEG has been more extensively studied than other methods, but further work is needed and the highest yield results are likely to emerge from the theta and alpha frequency markers defined above. Given the minimal cost associated with EEG, the potential for recordings to be distilled to a few electrodes and performed in community labs, it allows for far reaching real world clinical utility if such a treatment marker is identified. Importantly, improving predictions of treatment response, has the potential to spare patients and our healthcare system the burden of undergoing ineffective therapies, which would be of great clinical and scientific benefit.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
RS and DV conceived and designed the study, carried out the search, screening, data extraction, quality assessment, and drafted the manuscript. DV checked the inclusion/exclusion criteria. DMB, RC, and TKR critically revised the manuscript for intellectual content and reviewed the drafted manuscript. All authors contributed to critical revisions of the manuscript and gave final approval of the version to be published.
RS was supported by an Ontario Graduate Scholarship. This work was also supported in part by an Academic Scholars Award from the Department of Psychiatry, University of Toronto, awarded to DV.
TKR has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, Canadian Institutes of Health Research, Center for Aging and Brain Health Innovation, National Institutes of Health, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute. TKR also received for an investigator-initiated study in-kind equipment support from Newronika, and in-kind research online accounts from Scientific Brain Training Pro, and participated in 2021 in an advisory board for Biogen Canada Inc. DMB receives research support from CIHR, NIH, Brain Canada and the Temerty Family through the CAMH Foundation and the Campbell Research Institute. He received research support and in-kind equipment support for an investigator-initiated study from Brainsway Ltd., and he has been the site principal investigator for three sponsor-initiated studies for Brainsway Ltd. He also receives in-kind equipment support from Magventure for investigator-initiated studies. He received medication supplies for an investigator-initiated trial from Indivior. He has participated in Scientific Advisory Board for Welcony Inc. DV holds the Labatt Family Professorship in Depression Biology, a University Named Professorship at the University of Toronto. She receives research support from CIHR, the Center for Addiction and Mental Health (CAMH) and the Department of Psychiatry at the University of Toronto. DV declares no biomedical interests or conflicts.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abhang, P. A., Gawali, B. W., and Mehrotra, S. C. (2016). Introduction to EEG-and Speech-Based Emotion Recognition. Academic Press.
Aftanas, L. I., Varlamov, A. A., Pavlov, S. V., Makhnev, V. P., and Reva, N. V. (2002). Time-dependent cortical asymmetries induced by emotional arousal: EEG analysis of event-related synchronization and desynchronization in individually defined frequency bands. Int. J. Psychophysiol. 44, 67–82. doi: 10.1016/S0167-8760(01)00194-5
Aftanas, L. I., and Golocheikine, S. A. (2001). Human anterior and frontal midline theta and lower alpha reflect emotionally positive state and internalized attention: high-resolution EEG investigation of meditation. Neurosci. Lett. 310, 57–60. doi: 10.1016/S0304-3940(01)02094-8
Alexander, M. L., Alagapan, S., Lugo, C. E., Mellin, J. M., Lustenberger, C., Rubinow, D. R., et al. (2019). Double-blind, randomized pilot clinical trial targeting alpha oscillations with transcranial alternating current stimulation (tACS) for the treatment of major depressive disorder (MDD). Transl. Psychiatry 9, 1–12. doi: 10.1038/s41398-019-0439-0
Almeida Montes, L. G., Prado Alcántara, H., Portillo Cedeño, B. A., Hernández García, A. O., and Fuentes Rojas, P. E. (2015). Persistent decrease in alpha current density in fully remitted subjects with major depressive disorder treated with fluoxetine: a prospective electric tomography study. Int. J. Psychophysiol. 96, 191–200. doi: 10.1016/j.ijpsycho.2015.03.010
Amzica, F., and Steriade, M. (1998). Electrophysiological correlates of sleep delta waves. Electroencephalogr. Clin. Neurophysiol. 107, 69–83. doi: 10.1016/S0013-4694(98)00051-0
Arns, M., Bruder, G., Hegerl, U., Spooner, C., Palmer, D. M., Etkin, A., et al. (2016). EEG alpha asymmetry as a gender-specific predictor of outcome to acute treatment with different antidepressant medications in the randomized iSPOT-D study. Clin. Neurophysiol. 127, 509–519. doi: 10.1016/j.clinph.2015.05.032
Arns, M., Cerquera, A., Gutiérrez, R. M., Hasselman, F., and Freund, J. A. (2014). Non-linear EEG analyses predict non-response to rTMS treatment in major depressive disorder. Clin. Neurophysiol. 125, 1392–1399. doi: 10.1016/j.clinph.2013.11.022
Arns, M., Etkin, A., Hegerl, U., Williams, L. M., DeBattista, C., Palmer, D. M., et al. (2015). Frontal and rostral anterior cingulate (rACC) theta EEG in depression: implications for treatment outcome? Eur. Neuropsychopharmacol. 25, 1190–1200. doi: 10.1016/j.euroneuro.2015.03.007
Arns, M., Gordon, E., and Boutros, N. N. (2017). EEG abnormalities are associated with poorer depressive symptom outcomes with escitalopram and venlafaxine-XR, but not sertraline: results from the multicenter randomized iSPOT-D study. Clin. EEG Neurosci. 48, 33–40. doi: 10.1177/1550059415621435
Asada, H., Fukuda, Y., Tsunoda, S., Yamaguchi, M., and Tonoike, M. (1999). Frontal midline theta rhythms reflect alternative activation of prefrontal cortex and anterior cingulate cortex in humans. Neurosci. Lett. 4. doi: 10.1016/S0304-3940(99)00679-5
Bailey, N. W., Hoy, K. E., Rogasch, N. C., Thomson, R. H., McQueen, S., Elliot, D., et al. (2019). Differentiating responders and non-responders to rTMS treatment for depression after one week using resting EEG connectivity measures. J. Affect. Disord. 242, 68–79. doi: 10.1016/j.jad.2018.08.058
Bares, M., Brunovsky, M., Novak, T., Kopecek, M., Stopkova, P., Sos, P., et al. (2015a). QEEG Theta cordance in the prediction of treatment outcome to prefrontal repetitive transcranial magnetic stimulation or venlafaxine er in patients with major depressive disorder. Clin. EEG Neurosci. 46, 73–80. doi: 10.1177/1550059413520442
Bares, M., Novak, T., Kopecek, M., Brunovsky, M., Stopkova, P., and Höschl, C. (2015b). The effectiveness of prefrontal theta cordance and early reduction of depressive symptoms in the prediction of antidepressant treatment outcome in patients with resistant depression: analysis of naturalistic data. Eur. Arch. Psychiatry Clin. Neurosci. 265, 73–82. doi: 10.1007/s00406-014-0506-8
Barker, A. T., Jalinous, R., and Freeston, I. L. (1985). Non-invasive magnetic stimulation of human motor cortex. Lancet 325, 1106–1107. doi: 10.1016/S0140-6736(85)92413-4
Belardinelli, P., König, F., Liang, C., Premoli, I., Desideri, D., Müller-Dahlhaus, F., et al. (2021). TMS-EEG signatures of glutamatergic neurotransmission in human cortex. Sci. Rep. 11, 8159. doi: 10.1038/s41598-021-87533-z
Belmaker, R. H.. (2008). Major depressive disorder. New Engl. J. Med. 14, 96. doi: 10.1056/NEJMra073096
Berger, H.. (1929). On the EEG in humans. Arch. Psychiatr. Nervenkr 87, 527–570. doi: 10.1007/BF01797193
Blumberger, D. M., Vila-Rodriguez, F., Thorpe, K. E., Feffer, K., Noda, Y., Giacobbe, P., et al. (2018). Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet 391, 1683–1692. doi: 10.1016/S0140-6736(18)30295-2
Bravi, A., Longtin, A., and Seely, A. J. (2011). Review and classification of variability analysis techniques with clinical applications. Biomed. Eng. Online 10, 1–27. doi: 10.1186/1475-925X-10-90
Bruder, G. E., Fong, R., Tenke, C. E., Leite, P., Towey, J. P., Stewart, J. E., et al. (1997). Regional brain asymmetries in major depression with or without an anxiety disorder: a quantitative electroencephalographic study. Biol. Psychiatry 41, 939–948. doi: 10.1016/S0006-3223(96)00260-0
Cao, Z., Lin, C.-T., Ding, W., Chen, M.-H., Li, C.-T., and Su, T.-P. (2019). Identifying ketamine responses in treatment-resistant depression using a wearable forehead EEG. IEEE Trans. Biomed. Eng. 66, 1668–1679. doi: 10.1109/TBME.2018.2877651
Casarotto, S., Canali, P., Rosanova, M., Pigorini, A., Fecchio, M., Mariotti, M., et al. (2013). Assessing the effects of electroconvulsive therapy on cortical excitability by means of transcranial magnetic stimulation and electroencephalography. Brain Topogr. 26, 326–337. doi: 10.1007/s10548-012-0256-8
Cook, I.. (2002). Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 27, 120–131. doi: 10.1016/S0893-133X(02)00294-4
Cook, I. A., Hunter, A. M., Abrams, M., Siegman, B., and Leuchter, A. F. (2009). Midline and right frontal brain function as a physiologic biomarker of remission in major depression. Psychiatry Res. Neuroimaging 174, 152–157. doi: 10.1016/j.pscychresns.2009.04.011
Cook, I. A., Hunter, A. M., Gilmer, W. S., Iosifescu, D. V., Zisook, S., Burgoyne, K. S., et al. (2013). Quantitative electroencephalogram biomarkers for predicting likelihood and speed of achieving sustained remission in major depression: a report from the biomarkers for rapid identification of treatment effectiveness in major depression (BRITE-MD) trial. J. Clin. Psychiatry 74, 813. doi: 10.4088/JCP.10m06813
Cook, I. A., Wilson, A. C., Corlier, J., and Leuchter, A. F. (2019). Brain activity and clinical outcomes in adults with depression treated with synchronized transcranial magnetic stimulation: an exploratory study. Neuromodul. Technol. Neural Interface 22, 894–897. doi: 10.1111/ner.12914
Costa, M., Goldberger, A. L., and Peng, C.-K. (2005). Multiscale entropy analysis of biological signals. Phys. Rev. E 71, 021906. doi: 10.1103/PhysRevE.71.021906
Daskalakis, Z. J., Farzan, F., Radhu, N., and Fitzgerald, P. B. (2012). Combined transcranial magnetic stimulation and electroencephalography: its past, present and future. Brain Res. 1463, 93–107. doi: 10.1016/j.brainres.2012.04.045
Davidson, R. J.. (1992). Anterior cerebral asymmetry and the nature of emotion. Brain Cogn. 20, 125–151. doi: 10.1016/0278-2626(92)90065-T
de la Salle, S., Jaworska, N., Blier, P., Smith, D., and Knott, V. (2020). Using prefrontal and midline right frontal EEG-derived theta cordance and depressive symptoms to predict the differential response or remission to antidepressant treatment in major depressive disorder. Psychiatry Res. Neuroimag. 302, 111109. doi: 10.1016/j.pscychresns.2020.111109
Deslandes, A. C., Moraes, H., Alves, H., Pompeu, F. A., Silveira, H., Mouta, R., et al. (2010). Effect of aerobic training on EEG alpha asymmetry and depressive symptoms in the elderly: a 1-year follow-up study. Braz. J. Med. Biol. Res. 43, 585–592. doi: 10.1590/S0100-879X2010007500041
Doppelmayr, M., Klimesch, W., Pachinger, T., and Ripper, B. (1998). Individual differences in brain dynamics: important implications for the calculation of event-related band power. Biol. Cyber. 79, 49–57. doi: 10.1007/s004220050457
Elbert, T., Ray, W. J., Kowalik, Z. J., Skinner, J. E., Graf, K. E., and Birbaumer, N. (1994). Chaos and physiology: deterministic chaos in excitable cell assemblies. Physiol. Rev. 74, 1–47. doi: 10.1152/physrev.1994.74.1.1
Eshel, N., Keller, C. J., Wu, W., Jiang, J., Mills-Finnerty, C., Huemer, J., et al. (2020). Global connectivity and local excitability changes underlie antidepressant effects of repetitive transcranial magnetic stimulation. Neuropsychopharmacology 45, 1018–1025. doi: 10.1038/s41386-020-0633-z
Farzan, F., Barr, M. S., Hoppenbrouwers, S. S., Fitzgerald, P. B., Chen, R., Pascual-Leone, A., et al. (2013). The EEG correlates of the TMS induced EMG silent period in humans. Neuroimage 83, 120–134. doi: 10.1016/j.neuroimage.2013.06.059
Farzan, F., Vernet, M., Shafi, M. M. D., Rotenberg, A., Daskalakis, Z. J., and Pascual-Leone, A. (2016). Characterizing and modulating brain circuitry through transcranial magnetic stimulation combined with electroencephalography. Front. Neural Circuits 10, 73. doi: 10.3389/fncir.2016.00073
Freeman, W. J., and Quiroga, R. Q. (2013). Imaging Brain Function With EEG: Advanced Temporal and Spatial Analysis of Electroencephalographic Signals [WWW Document]. Available online at: https://books-scholarsportal-info.myaccess.library.utoronto.ca/en/read?id=/ebooks/ebooks3/springer/2016-05-20/1/9781461449843#page=18 (accessed November 15, 2020).
Friedrich, M. J.. (2017). Depression is the leading cause of disability around the world. JAMA 317, 1517–1517. doi: 10.1001/jama.2017.3826
Gollan, J. K., Hoxha, D., Chihade, D., Pflieger, M. E., Rosebrock, L., and Cacioppo, J. (2014). Frontal alpha EEG asymmetry before and after behavioral activation treatment for depression. Biol. Psychol. 99, 198–208. doi: 10.1016/j.biopsycho.2014.03.003
Gordon, P. C., Dörre, S., Belardinelli, P., Stenroos, M., Zrenner, B., Ziemann, U., et al. (2021). Prefrontal theta-phase synchronized brain stimulation with real-time EEG-triggered TMS. Front. Hum. Neurosci. 15, 1821. doi: 10.3389/fnhum.2021.691821
Hadas, I., Sun, Y., Lioumis, P., Zomorrodi, R., Jones, B., Voineskos, D., et al. (2019). Association of repetitive transcranial magnetic stimulation treatment with subgenual cingulate hyperactivity in patients with major depressive disorder. JAMA Netw Open. 2, 5578. doi: 10.1001/jamanetworkopen.2019.5578
Hadas, I., Zomorrodi, R., Hill, A. T., Sun, Y., Fitzgerald, P. B., Blumberger, D. M., et al. (2020). Subgenual cingulate connectivity and hippocampal activation are related to MST therapeutic and adverse effects. Transl. Psychiatry 10, 1–8. doi: 10.1038/s41398-020-01042-7
Haegens, S., Cousijn, H., Wallis, G., Harrison, P. J., and Nobre, A. C. (2014). Inter- and intra-individual variability in alpha peak frequency. Neuroimage 92, 46–55. doi: 10.1016/j.neuroimage.2014.01.049
Hegerl, U., Wilk, K., Olbrich, S., Schoenknecht, P., and Sander, C. (2012). Hyperstable regulation of vigilance in patients with major depressive disorder. World J. Biol. Psychiatry 13, 436–446. doi: 10.3109/15622975.2011.579164
Hill, A. T., Hadas, I., Zomorrodi, R., Voineskos, D., Fitzgerald, P. B., Blumberger, D. M., et al. (2021). Characterizing cortical oscillatory responses in major depressive disorder before and after convulsive therapy: a TMS-EEG study. J. Affect. Disord. 287, 78–88. doi: 10.1016/j.jad.2021.03.010
Hunter, A. M., Cook, I. A., Greenwald, S., Tran, M. L., Miyamoto, K. N., and Leuchter, A. F. (2011). The antidepressant treatment response (ATR) index and treatment outcomes in a placebo-controlled trial of fluoxetine. J. Clin. Neurophysiol. 28, 478–482. doi: 10.1097/WNP.0b013e318230da8a
Hunter, A. M., Cook, I. A., and Leuchter, A. F. (2007). The promise of the quantitative electroencephalogram as a predictor of antidepressant treatment outcomes in major depressive disorder. Psychiatr. Clin. North Am. 30, 105–124. doi: 10.1016/j.psc.2006.12.002
Hunter, A. M., Korb, A. S., Cook, I. A., and Leuchter, A. F. (2013). Rostral anterior cingulate activity in major depressive disorder: state or trait marker of responsiveness to medication? J, Neuropsychiatry Clin. Neurosci. 8, 330. doi: 10.1176/appi.neuropsych.11110330
Hunter, A. M., Leuchter, A. F., Cook, I. A., and Abrams, M. (2010a). Brain functional changes (QEEG cordance) and worsening suicidal ideation and mood symptoms during antidepressant treatment: QEEG cordance and worsening symptoms. Acta Psychiatr. Scand. 122, 461–469. doi: 10.1111/j.1600-0447.2010.01560.x
Hunter, A. M., Leuchter, A. F., Morgan, M. L., and Cook, I. A. (2006). Changes in brain function (quantitative EEG Cordance) during placebo lead-in and treatment outcomes in clinical trials for major depression. Am. J. Psychiatry 7, 1426. doi: 10.1176/ajp.2006.163.8.1426
Hunter, A. M., Muthén, B. O., Cook, I. A., and Leuchter, A. F. (2010b). Antidepressant response trajectories and quantitative electroencephalography (QEEG) biomarkers in major depressive disorder. J. Psychiatr. Res. 44, 90–98. doi: 10.1016/j.jpsychires.2009.06.006
Hunter, A. M., Ravikumar, S., Cook, I. A., and Leuchter, A. F. (2009). Brain functional changes during placebo lead-in and changes in specific symptoms during pharmacotherapy for major depression. Acta Psychiatr. Scand. 119, 266–273. doi: 10.1111/j.1600-0447.2008.01305.x
Ip, C.-T., Ganz, M., Dam, V. H., Ozenne, B., Rüesch, A., Köhler-Forsberg, K., et al. (2021). NeuroPharm study: EEG wakefulness regulation as a biomarker in MDD. J. Psychiatr. Res. 141, 57–65. doi: 10.1016/j.jpsychires.2021.06.021
Jasper, H. H.. (1958). The ten-twenty electrode system of the International Federation. Electroencephalogr. Clin. Neurophysiol. 10, 370–375.
Jaworska, N., Blondeau, C., Tessier, P., Norris, S., Fusee, W., Blier, P., et al. (2014). Examining relations between alpha power as well as anterior cingulate cortex-localized theta activity and response to single or dual antidepressant pharmacotherapies. J. Psychopharmacol. 28, 587–595. doi: 10.1177/0269881114523862
Jaworska, N., Wang, H., Smith, D. M., Blier, P., Knott, V., and Protzner, A. B. (2017). Pre-treatment EEG signal variability is associated with treatment success in depression. Neuroimage Clin. 17, 368–377. doi: 10.1016/j.nicl.2017.10.035
Knott, V., Mahoney, C., Kennedy, S., and Evans, K. (2002). EEG correlates of acute and chronic paroxetine treatment in depression. J. Affect. Disord. 69, 241–249. doi: 10.1016/S0165-0327(01)00308-1
Kobayashi, M., and Pascual-Leone, A. (2003). Transcranial magnetic stimulation in neurology. Lancet Neurol. 2, 145–156. doi: 10.1016/S1474-4422(03)00321-1
Korb, A. S., Hunter, A. M., Cook, I. A., and Leuchter, A. F. (2009). Rostral anterior cingulate cortex theta current density and response to antidepressants and placebo in major depression. Clin. Neurophysiol. 120, 1313–1319. doi: 10.1016/j.clinph.2009.05.008
Korb, A. S., Hunter, A. M., Cook, I. A., and Leuchter, A. F. (2011). Rostral anterior cingulate cortex activity and early symptom improvement during treatment for major depressive disorder. Psychiatry Res. 192, 188–194. doi: 10.1016/j.pscychresns.2010.12.007
Kropotov, J.. (2016). Functional Neuromarkers for Psychiatry: Applications for Diagnosis and Treatment. Academic Press.
Kupfer, D. J., Frank, E., and Phillips, M. L. (2012). Major depressive disorder: new clinical, neurobiological, and treatment perspectives. Lancet 379, 1045–1055. doi: 10.1016/S0140-6736(11)60602-8
Larson, J., Wong, D., and Lynch, G. (1986). Patterned stimulation at the theta frequency is optimal for the induction of hippocampal long-term potentiation. Brain Res. 368, 347–350. doi: 10.1016/0006-8993(86)90579-2
Leuchter, A. F., Cook, I. A., Gilmer, W. S., Marangell, L. B., Burgoyne, K. S., Howland, R. H., et al. (2009a). Effectiveness of a quantitative electroencephalographic biomarker for predicting differential response or remission with escitalopram and bupropion in major depressive disorder. Psychiatry Res. 169, 132–138. doi: 10.1016/j.psychres.2009.04.004
Leuchter, A. F., Cook, I. A., Lufkin, R. B., Dunkin, J., Newton, T. F., Cummings, J. L., et al. (1994). Cordance: a new method for assessment of cerebral perfusion and metabolism using quantitative electroencephalography. Neuroimage 1, 208–219. doi: 10.1006/nimg.1994.1006
Leuchter, A. F., Cook, I. A., Marangell, L. B., Gilmer, W. S., Burgoyne, K. S., Howland, R. H., et al. (2009b). Comparative effectiveness of biomarkers and clinical indicators for predicting outcomes of SSRI treatment in major depressive disorder: results of the BRITE-MD study. Psychiatry Res. 169, 124–131. doi: 10.1016/j.psychres.2009.06.004
Leuchter, A. F., Cook, I. A., Witte, E. A., Morgan, M., and Abrams, M. (2002). Changes in brain function of depressed subjects during treatment with placebo. Am. J. Psychiatry 159, 122–129. doi: 10.1176/appi.ajp.159.1.122
Leuchter, A. F., Hunter, A. M., Jain, F. A., Tartter, M., Crump, C., and Cook, I. A. (2017). Escitalopram but not placebo modulates brain rhythmic oscillatory activity in the first week of treatment of Major Depressive Disorder. J. Psychiatr. Res. 84, 174–183. doi: 10.1016/j.jpsychires.2016.10.002
Leuchter, A. F., Uijtdehaage, S. H., Cook, I. A., O'Hara, R., and Mandelkern, M. (1999). Relationship between brain electrical activity and cortical perfusion in normal subjects. Psychiatry Res. Neuroimag. 90, 125–140. doi: 10.1016/S0925-4927(99)00006-2
Lisman, J. E., and Jensen, O. (2013). The theta-gamma neural code. Neuron 77, 1002–1016. doi: 10.1016/j.neuron.2013.03.007
Luscher, B., Shen, Q., and Sahir, N. (2011). The GABAergic deficit hypothesis of major depressive disorder. Mol. Psychiatry 16, 383–406. doi: 10.1038/mp.2010.120
Martinot, M.-L. P., Martinot, J.-L., Ringuenet, D., Galinowski, A., Gallarda, T., Bellivier, F., et al. (2011). Baseline brain metabolism in resistant depression and response to transcranial magnetic stimulation. Neuropsychopharmacol 36, 2710–2719. doi: 10.1038/npp.2011.161
Mayberg, H. S., Liotti, M., Brannan, S. K., McGinnis, S., Mahurin, R. K., Jerabek, P. A., et al. (1999). Reciprocal limbic-cortical function and negative mood: converging pet findings in depression and normal sadness. AJP 156, 675–682.
McMillan, R., Sumner, R., Forsyth, A., Campbell, D., Malpas, G., Maxwell, E., et al. (2020). Simultaneous EEG/fMRI recorded during ketamine infusion in patients with major depressive disorder. Prog. Neuro Psychopharmacol. Biol. Psychiatry 99, 109838. doi: 10.1016/j.pnpbp.2019.109838
Michel, C. M., and Pascual-Leone, A. (2020). Predicting antidepressant response by electroencephalography. Nat. Biotechnol. 38, 417–419. doi: 10.1038/s41587-020-0476-5
Miyauchi, E., Ide, M., Tachikawa, H., Nemoto, K., Arai, T., and Kawasaki, M. (2019). A novel approach for assessing neuromodulation using phase-locked information measured with TMS-EEG. Sci. Rep. 9, 428. doi: 10.1038/s41598-018-36317-z
Mulert, C., Juckel, G., Brunnmeier, M., Karch, S., Leicht, G., Mergl, R., et al. (2007a). Prediction of treatment response in major depression: integration of concepts. J. Affect. Disord. 98, 215–225. doi: 10.1016/j.jad.2006.07.021
Mulert, C., Juckel, G., Brunnmeier, M., Karch, S., Leicht, G., Mergl, R., et al. (2007b). Rostral anterior cingulate cortex activity in the theta band predicts response to antidepressive medication. Clin. EEG Neurosci. 38, 78–81. doi: 10.1177/155005940703800209
Narushima, K., McCormick, L., Yamada, T., Thatcher, R., and Robinson, R. G. (2010). Subgenual cingulate theta activity predicts treatment response of repetitive transcranial magnetic stimulation in participants with vascular depression. J. Neuropsychiatry Clin. Neurosci. 22, 75–84. doi: 10.1176/jnp.2010.22.1.75
Niedermeyer, E.. (1999). The normal EEG of the waking adult. Electroencephalogr. Basic Princip. Clin. Appl. Relat. Fields 20, 149–173.
Niedermeyer, E.. (2005). Abnormal EEG patterns: Epileptic and paroxysmal. Electroencephalogr. Basic Princip. Clin. Appl. Related Fields. 5th edition. 255–280.
Nilsonne, G., and Harrell, F. E. (2021). EEG-based model and antidepressant response. Nat. Biotechnol. 39, 27–27. doi: 10.1038/s41587-020-00768-5
Noachtar, S., Binnie, C., Ebersole, J., Mauguière, F., Sakamoto, A., and Westmoreland, B. (1999). A glossary of terms most commonly used by clinical electroencephalographers and proposal for the report form for the eeg findings. The international federation of clinical neurophysiology, Electroencephalography and Clinical Neurophysiology. Supplement. 52, 21-U41.
Noda, Y., Zomorrodi, R., Cash, R. F. H., Barr, M. S., Farzan, F., Rajji, T. K., et al. (2017). Characterization of the influence of age on GABAA and glutamatergic mediated functions in the dorsolateral prefrontal cortex using paired-pulse TMS-EEG. Aging 9, 556–567. doi: 10.18632/aging.101178
Olbrich, S., and Arns, M. (2013). EEG biomarkers in major depressive disorder: Discriminative power and prediction of treatment response. Int. Rev. Psychiatry 25, 604–618. doi: 10.3109/09540261.2013.816269
Olbrich, S., Mulert, C., Karch, S., Trenner, M., Leicht, G., Pogarell, O., et al. (2009). EEG-vigilance and BOLD effect during simultaneous EEG/fMRI measurement. Neuroimage 45, 319–332. doi: 10.1016/j.neuroimage.2008.11.014
Olbrich, S., Tränkner, A., Surova, G., Gevirtz, R., Gordon, E., Hegerl, U., et al. (2016). CNS- and ANS-arousal predict response to antidepressant medication: findings from the randomized iSPOT-D study. J. Psychiatr. Res. 73, 108–115. doi: 10.1016/j.jpsychires.2015.12.001
Philip, N. S., Leuchter, A. F., Cook, I. A., Massaro, J., Goethe, J. W., and Carpenter, L. L. (2019). Predictors of response to synchronized transcranial magnetic stimulation for major depressive disorder. Depress Anxiety 36, 278–285. doi: 10.1002/da.22862
Pizzagalli, D., Pascual-Marqui, R. D., Nitschke, J. B., Oakes, T. R., Larson, C. L., Abercrombie, H. C., et al. (2001). Anterior cingulate activity as a predictor of degree of treatment response in major depression: evidence from brain electrical tomography analysis. AJP 158, 405–415. doi: 10.1176/appi.ajp.158.3.405
Pizzagalli, D. A., Webb, C. A., Dillon, D. G., Tenke, C. E., Kayser, J., Goer, F., et al. (2018). Pretreatment rostral anterior cingulate cortex theta activity in relation to symptom improvement in depression: a randomized clinical trial. JAMA Psychiatry 75, 547. doi: 10.1001/jamapsychiatry.2018.0252
Premoli, I., Castellanos, N., Rivolta, D., Belardinelli, P., Bajo, R., Zipser, C., et al. (2014). TMS-EEG signatures of GABAergic neurotransmission in the human cortex. J. Neurosci. 34, 5603–5612. doi: 10.1523/JNEUROSCI.5089-13.2014
Rogasch, N. C., Daskalakis, Z. J., and Fitzgerald, P. B. (2015). Cortical inhibition of distinct mechanisms in the dorsolateral prefrontal cortex is related to working memory performance: a TMS–EEG study. Cortex 64, 68–77. doi: 10.1016/j.cortex.2014.10.003
Sander, C., Schmidt, J. M., Mergl, R., Schmidt, F. M., and Hegerl, U. (2018). Changes in brain arousal (EEG-vigilance) after therapeutic sleep deprivation in depressive patients and healthy controls. Sci. Rep. 8, 15087. doi: 10.1038/s41598-018-33228-x
Schmidt, F. M., Sander, C., Dietz, M.-E., Nowak, C., Schröder, T., Mergl, R., et al. (2017). Brain arousal regulation as response predictor for antidepressant therapy in major depression. Sci. Rep. 7, 45187. doi: 10.1038/srep45187
Schünemann, H. J., Schünemann, A. H. J., Oxman, A. D., Brozek, J., Glasziou, P., Jaeschke, R., and Vist, G. E.. (2008). Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ 336, 1106–1110. doi: 10.1136/bmj.39500.677199.AE
Spellman, T., and Liston, C. (2020). Toward circuit mechanisms of pathophysiology in depression. Am. J. Psychiatry 177, 381–390. doi: 10.1176/appi.ajp.2020.20030280
Sun, Y., Farzan, F., Mulsant, B. H., Rajji, T. K., Fitzgerald, P. B., Barr, M. S., et al. (2016). Indicators for remission of suicidal ideation following magnetic seizure therapy in patients with treatment-resistant depression. JAMA Psychiatry 73, 337–345. doi: 10.1001/jamapsychiatry.2015.3097
Szumska, I., Gola, M., Rusanowska, M., Krajewska, M., Zygierewicz, J., Krejtz, I., et al. (2021). Mindfulness-based cognitive therapy reduces clinical symptoms, but do not change frontal alpha asymmetry in people with major depression disorder. Int. J. Neurosci. 131, 453–461. doi: 10.1080/00207454.2020.1748621
Tenke, C. E., Kayser, J., Manna, C. G., Fekri, S., Kroppmann, C. J., Schaller, J. D., et al. (2011). Current source density measures of EEG alpha predict antidepressant treatment response. Biol. Psychiatry 70, 388–394. doi: 10.1016/j.biopsych.2011.02.016
van der Vinne, N., Vollebregt, M. A., Boutros, N. N., Fallahpour, K., van Putten, M. J. A. M., and Arns, M. (2019a). Normalization of EEG in depression after antidepressant treatment with sertraline? A preliminary report. J. Affect. Disord. 259, 67–72. doi: 10.1016/j.jad.2019.08.016
van der Vinne, N., Vollebregt, M. A., van Putten, M. J. A. M., and Arns, M. (2019b). Stability of frontal alpha asymmetry in depressed patients during antidepressant treatment. Neuroimage Clin. 24, 2056. doi: 10.1016/j.nicl.2019.102056
Voineskos, D., Blumberger, D. M., Rogasch, N. C., Zomorrodi, R., Farzan, F., Foussias, G., et al. (2021). Neurophysiological effects of repetitive transcranial magnetic stimulation (rTMS) in treatment resistant depression. Clin. Neurophysiol. S1388245721005927. doi: 10.1016/j.clinph.2021.05.008
Voineskos, D., Daskalakis, Z. J., and Blumberger, D. M. (2020). Management of treatment-resistant depression: challenges and strategies. Neuropsychiatr. Dis. Treat. 16, 221–234. doi: 10.2147/NDT.S198774
Wade, E. C., and Iosifescu, D. V. (2016). Using electroencephalography for treatment guidance in major depressive disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 1, 411–422. doi: 10.1016/j.bpsc.2016.06.002
Widge, A. S., Avery, D. H., and Zarkowski, P. (2013). Baseline and treatment-emergent EEG biomarkers of antidepressant medication response do not predict response to repetitive transcranial magnetic stimulation. Brain Stimul. 6, 929–931. doi: 10.1016/j.brs.2013.05.001
Widge, A. S., Bilge, M. T., Montana, R., Chang, W., Rodriguez, C. I., Deckersbach, T., et al. (2019). Electroencephalographic biomarkers for treatment response prediction in major depressive illness: a meta-analysis. Am. J. Psychiatry 176, 44–56. doi: 10.1176/appi.ajp.2018.17121358
Wu, W., Pizzagall, D. A., Trivedi, M. H., and Etkin, A. (2021). Reply to: EEG-based model and antidepressant response. Nat. Biotechnol. 39, 28–29. doi: 10.1038/s41587-020-0738-2
Wu, W., Zhang, Y., Jiang, J., Lucas, M. V., Fonzo, G. A., Rolle, C. E., et al. (2020). An electroencephalographic signature predicts antidepressant response in major depression. Nat. Biotechnol. 38, 439–447. doi: 10.1038/s41587-019-0397-3
Zrenner, B., Zrenner, C., Gordon, P. C., Belardinelli, P., McDermott, E. J., Soekadar, S. R., et al. (2020). Brain oscillation-synchronized stimulation of the left dorsolateral prefrontal cortex in depression using real-time EEG-triggered TMS. Brain Stimul. 13, 197–205. doi: 10.1016/j.brs.2019.10.007
Zrenner, C., Belardinelli, P., Müller-Dahlhaus, F., and Ziemann, U. (2016). Closed-loop neuroscience and non-invasive brain stimulation: a tale of two loops. Front. Cell Neurosci. 10, 92. doi: 10.3389/fncel.2016.00092
Appendix 1. PubMed Search Strategy (“Depressive Disorder, Major/therapy”[Mesh]) OR (“Depression/therapy”[MAJR]) OR (“Antidepressive Agents/therapeutic use”[MAJR])) AND ((EEG) OR (electroencephalography) OR (TMS-EEG) OR (TMS)) Filters: English, Human Date range: 2000-2021.
Appendix 2. EMBASE Search Strategy (major depressive disorder) AND (antidepressant agent OR ECT OR transcranial magnetic stimulation OR repetitive transcranial magnetic stimulation) AND (electroencephalography) Filters: English, Human Date range: 2000-2021.
Keywords: major depressive disorder (MDD), electroencephalography (EEG), transcranial magnetic stimulation (TMS), TMS-EEG, biomarkers, repetitive transcranial magnetic stimulation (rTMS), antidepressant, treatment
Citation: Strafella R, Chen R, Rajji TK, Blumberger DM and Voineskos D (2022) Resting and TMS-EEG markers of treatment response in major depressive disorder: A systematic review. Front. Hum. Neurosci. 16:940759. doi: 10.3389/fnhum.2022.940759
Received: 11 May 2022; Accepted: 28 June 2022;
Published: 04 August 2022.
Edited by:
Joao Miguel Castelhano, University of Coimbra, PortugalReviewed by:
Alena Damborská, Masaryk University, CzechiaCopyright © 2022 Strafella, Chen, Rajji, Blumberger and Voineskos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daphne Voineskos, ZGFwaG5lLnZvaW5lc2tvc0BjYW1oLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.