
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Hum. Neurosci., 13 May 2022
Sec. Cognitive Neuroscience
Volume 16 - 2022 | https://doi.org/10.3389/fnhum.2022.867055
This article is part of the Research TopicRecording and Modulating Neural Activity in Neurodegenerative Diseases: Pathophysiological and Therapeutic ImplicationsView all 6 articles
 Valentino Rački1,2
Valentino Rački1,2 Mario Hero1,2
Mario Hero1,2 Gloria Rožmarić3
Gloria Rožmarić3 Eliša Papić1,2
Eliša Papić1,2 Marina Raguž4,5
Marina Raguž4,5 Darko Chudy4,6
Darko Chudy4,6 Vladimira Vuletić1,2*
Vladimira Vuletić1,2*Introduction: Parkinson’s disease (PD) patients have a significantly higher risk of developing dementia in later disease stages, leading to severe impairments in quality of life and self-functioning. Questions remain on how deep brain stimulation (DBS) affects cognition, and whether we can individualize therapy and reduce the risk for adverse cognitive effects. Our aim in this systematic review is to assess the current knowledge in the field and determine if the findings could influence clinical practice.
Methods: We have conducted a systematic review according to PRISMA guidelines through MEDLINE and Embase databases, with studies being selected for inclusion via a set inclusion and exclusion criteria.
Results: Sixty-seven studies were included in this systematic review according to the selected criteria. This includes 6 meta-analyses, 18 randomized controlled trials, 17 controlled clinical trials, and 26 observational studies with no control arms. The total number of PD patients encompassed in the studies cited in this review is 3677, not including the meta-analyses.
Conclusion: Cognitive function in PD patients can deteriorate, in most cases mildly, but still impactful to the quality of life. The strongest evidence is present for deterioration in verbal fluency, while inconclusive evidence is still present for executive function, memory, attention and processing speed. Global cognition does not appear to be significantly impacted by DBS, especially if cognitive screening is performed prior to the procedure, as lower baseline cognitive function is connected to poor outcomes. Further randomized controlled studies are required to increase the level of evidence, especially in the case of globus pallidus internus DBS, pedunculopontine nucleus DBS, and the ventral intermediate nucleus of thalamus DBS, and more long-term studies are required for all respective targets.
Parkinson’s disease (PD) is a widespread neurodegenerative disease that is most prevalent in individuals over the age of 65, posing a considerable burden on aging populations (Poewe et al., 2017). PD is a progressive disorder marked by motor symptoms like resting tremor, bradykinesia and rigidity, as well as non-motor symptoms such as sleep disorders autonomic dysfunction, behavioral changes and cognitive deficits (Vuletic et al., 2019). Additional research is elucidating the mechanisms underlying PD, which include the intracellular aggregation of α-synuclein, the formation of Lewy bodies (Bloem et al., 2021), and the loss of dopaminergic neurons. Damage of neurons starts in the olfactory bulb and locus caeruleus, but is most commonly followed in the substantia nigra dopaminergic neurons with further spreading throughout the brain as the disease progresses (Damier et al., 1999). This was postulated by Braak et al. (2003), who described a progressive escalation of pathology and symptom severity beginning in the lower brainstem and progressing to limbic and neocortical brain regions in the latter stages.
Research shows that PD patients have a significantly higher risk of developing dementia in later disease stages, leading to severe impairments in quality of life and self-functioning (Fang et al., 2020). Mild cognitive impairment is prevalent in PD patients, with a mean frequency of 27%, and many individuals develop to clinically severe dementia (Litvan et al., 2012). Additionally, the distribution of cognitive deficits in PD is centered on two distinct dopaminergic pathways in the frontal lobe and temporal lobes, with difficulties in planning, working memory, executive function, semantic verbal fluency and visual spatial ability (Fang et al., 2020).
The mainstay of treatment in early phases of the disease is focused on medicaments, although more invasive therapies may be employed in more advanced stages when medication alone cannot properly control symptoms (Armstrong and Okun, 2020). Deep brain stimulation (DBS) is a functional neurosurgical procedure that is used to treat movement, neurodegenerative and psychiatric disorders by modulating neuronal pathways (Lozano et al., 2019). It is typically used for treating motor symptoms in PD, while it is not as effective, or even aggravating, for gait, affective and cognitive symptoms (Mehanna et al., 2017). Common targets in PD include subthalamic nucleus (STN) and globus pallidus internus (GPi), while it is rarely used in ventral intermediate nucleus of thalamus (VIM) and pedunculopontine nucleus (PPN; Lozano et al., 2019). Current clinical practice of patient selection consists of patients with motor symptoms not controlled well with best medical therapy (BMT), while axial, speech, affective, and cognitive symptoms must be normal or minimally affected (Pollak, 2013). However, as the use of DBS broadens, a few questions remain. Mainly, what are the DBS effects on cognition, how to individualize therapy and reduce risk for adverse effects. The purpose of this systematic review is to review current knowledge in the field and to ascertain whether the findings have the potential to influence therapeutic practice.
We have conducted a systematic review according to PRISMA guidelines (Page et al., 2021). Our search was focused on the MEDLINE and Embase databases. The search was done on articles published up to December of 2021. We used the following keywords on all fields and MeSH terms: “deep brain stimulation,” “Parkinson’s disease,” “cognitive effects,” “cognitive impact,” “cognitive outcome,” “cognition,” “subthalamic nucleus,” “globus pallidus internus,” “pedunculopontine nucleus,” “ventral intermediate nucleus of thalamus,” along with Boolean terms “AND” and “OR.” The search rendered 590 records after we applied appropriate filters. The studies were then selected based upon the following inclusion and exclusion criteria (Figure 1). Articles were first screened by title and abstract, followed by full-text checking for their eligibility. The selection of articles was done independently by four authors (VR, EP, MH, and GR), and final inclusion was done by agreement.
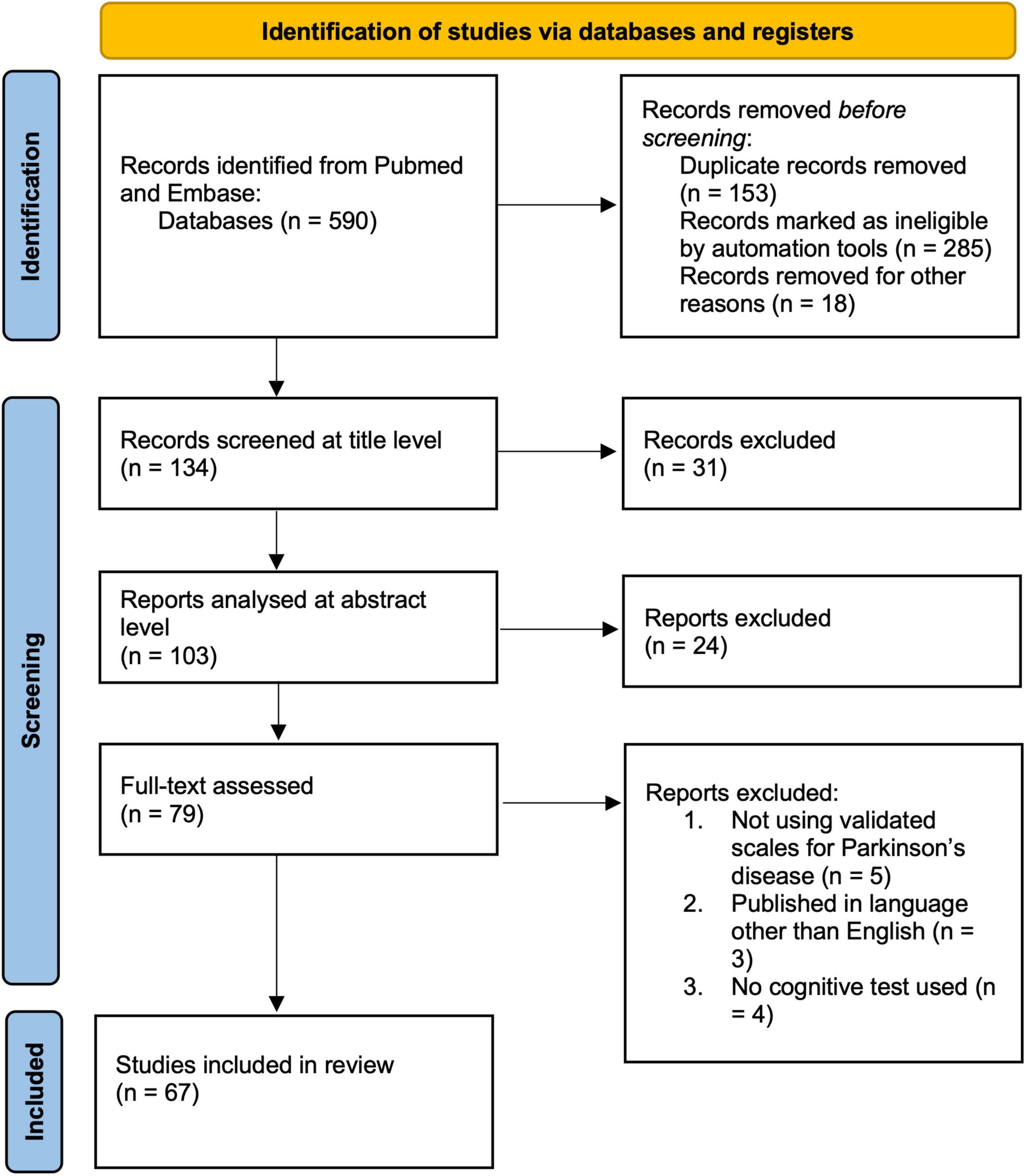
Figure 1. Prisma flow chart of the systematic review.
Studies accepted for inclusion were: (a) studies with patients diagnosed with PD; (b) studies published up to December of 2021; (c) published in the English language; (d) published in indexed and peer-reviewed journals; and (e) evaluated cognition using validated scales and scoring systems.
Exclusion criteria include: (a) studies published in regional languages other than English, (b) no clear cognitive methodology or testing parameters described. Studies were checked for quality and finally, 62 studies were included (Figure 1).
The primary search yielded a total of 590 studies using the described method and search parameters. 134 studies remained after excluding duplicate records and filtering them out with automation tools. These were screened on the title level and 31 studies were excluded, leaving 103 studies that were analyzed on the abstract level, where additional 24 studies were excluded. The full text was analyzed for 79 studies, and additional 12 studies were excluded (not using validated scales for PD, n = 5; published in a language other than English, n = 3; and no cognitive test used, n = 4). Therefore, 67 studies were included in this systematic review according to the selected criteria (Supplementary Table 1). The complete PRISM flow chart for this systematic review is given in Figure 1. When looking at study designs, the search yielded 6 meta-analyses, 18 randomized controlled trials, 17 controlled clinical trials, and 26 observational studies with no control arms. The total number of PD patients encompassed in the studies cited in this review is 3,194, not including the meta-analyses.
The impact of DBS on cognition can be viewed through changes in global cognitive functioning, as measured by scales such as the Mattis Dementia Rating Scale or the Mini-Mental State Examination, or specialized scales focusing on certain aspects of cognitive functioning. The reported studies on global functioning show somewhat opposing results. A meta-analysis by Combs et al. (2015) and Xie et al. (2016) revealed a statistically significant decrease in global cognition when comparing subthalamic nucleus DBS (STN-DBS) with BMT and globus pallidus internus DBS (GPi-DBS) patients, even though the overall change was not large. On the other hand, several randomized controlled clinical trials, controlled clinical trials, and observational studies found no changes in global cognitive functioning in their patients (Witt et al., 2004, 2008; Schüpbach et al., 2006; Smeding et al., 2006; Contarino et al., 2007; Klempírová et al., 2007; Heo et al., 2008; York et al., 2008; Okun et al., 2009; Weaver et al., 2009; Castelli et al., 2010; Daniels et al., 2010; Williams et al., 2011; Schuepbach et al., 2013; Asahi et al., 2014; Tang et al., 2015; Boel et al., 2016; Acera et al., 2019; Vats et al., 2019; You et al., 2020). When comparing targets, a meta-analysis by Wang et al. (2016) and a randomized controlled trial by Weaver et al. (2012) found that STN-DBS PD patients’ global cognition deteriorated more frequently than GPi-DBS patients, while several randomized controlled studies found no differences in global cognition or cognitive functional performance (Weaver et al., 2009; Odekerken et al., 2013, 2015, 2016). An observational study with the longest timeframe reported a decline in global functioning that was most pronounced up to the 9th year of treatment, and remained stable at the last tested period 14 years after surgery (Volonté et al., 2021). Researchers have also found that people who have lower global cognitive function scores before having STN-DBS are less likely to have good results after the procedure (Perriol et al., 2006; Tir et al., 2007; Tsai et al., 2009; Rinehardt et al., 2010; Witt et al., 2011; Fukaya et al., 2017; Acera et al., 2019).
Majority of the studies evaluated specific cognitive domains using specialized testing. The domains include language, executive function, attention, memory, and processing speed.
Changes in language were the most reported in numerous studies. Looking at meta-analyses, statistically significant decline in semantic and phonemic fluency was found in STN-DBS patients compared to BMT (Xie et al., 2016; Wang et al., 2021) patients and GPi-DBS patients (Combs et al., 2015; Tan et al., 2016; Wang et al., 2016), as well as a part of the natural disease progression with no control arms (Parsons et al., 2006). The decline of verbal fluency was detected in several randomized controlled trials in the STN-DBS groups (Wojtecki et al., 2006; Witt et al., 2008; Okun et al., 2009; Weaver et al., 2009; Zahodne et al., 2009b; Daniels et al., 2010; Phillips et al., 2012; Ehlen et al., 2014; Pinto et al., 2014; Tramontana et al., 2015), although this was not seen in all studies that compared STN-DBS to BMT or GPi-DBS (York et al., 2008; Daniels et al., 2010; Odekerken et al., 2013, 2015, 2016; Rothlind et al., 2015; Boel et al., 2016). One study assessed the differences between STN-DBS and pedunculopontine nucleus DBS (PPN-DBS) patients and found that PPN-DBS patients experienced greater language deterioration in a small sample size (Pinto et al., 2014). Similar was seen in a study comparing localizations closer to VIM rather than STN, with increased verbal fluency deterioration (Ehlen et al., 2014). Slight declines of fluency in STN-DBS patients compared to BMT control patients was seen in several controlled clinical trials (Gironell et al., 2003; Smeding et al., 2006; Zangaglia et al., 2009; Castelli et al., 2010; Merola et al., 2011, 2014; Williams et al., 2011; Sáez-Zea et al., 2012; Foki et al., 2017; Szlufik et al., 2020; You et al., 2020), with only one study reporting no changes (York et al., 2008). The same trend was seen in observational studies as well (Funkiewiez et al., 2004; Castelli et al., 2006; Contarino et al., 2007; Heo et al., 2008; Schoenberg et al., 2008; Higginson et al., 2009; Fasano et al., 2010; Houvenaghel et al., 2015; Tang et al., 2015; Acera et al., 2019; Leimbach et al., 2019). Several studies that looked at language processing other than verbal or phonemic fluency found no significant changes in GPi-DBS (Rothlind et al., 2015) and STN-DBS patients (Heo et al., 2008; Castelli et al., 2010; Asahi et al., 2014; Rothlind et al., 2015; Foki et al., 2017).
Executive function testing results published in the current meta-analysis reveal conflicting findings. Worsening of executive functions was seen in two studies, one comparing STN-DBS and GPi-DBS (Combs et al., 2015) and the other comparing STN-DBS to BMT control patients (Xie et al., 2016). On the other hand, two meta-analysis comparing STN-DBS and GPi-DBS (Tan et al., 2016; Wang et al., 2016), one that compared STN to BMT control patients (Wang et al., 2021), and lastly a single meta-analysis covering only STN-DBS patients found no significant alterations in executive function (Parsons et al., 2006). Four randomized clinical trials reported varying changes in executive functions, and interestingly, executive function was impaired in STN-DBS patients short-term (Daniels et al., 2010), but changes largely diminished in later time frames (Rothlind et al., 2015; Tramontana et al., 2015; Boel et al., 2016). Controlled clinical trials comparing STN-DBS to BMT control patients mostly reported no changes in executive function (Gironell et al., 2003; Smeding et al., 2006; York et al., 2008; Castelli et al., 2010; Foki et al., 2017), the exception was a two-part study with unilateral STN-DBS and GPi-DBS reporting decline in executive functioning compared to control patients (Zahodne et al., 2009a; Mikos et al., 2010). Similar findings were seen in a longer-term 3-year study comparing STN-DBS and BMT control patients (Zangaglia et al., 2009). Finally, non-consistent results can be seen in observational studies, with studies reporting either slight changes or no worsening in the clinical course of STN-DBS patients (Dujardin et al., 2001; Perozzo et al., 2001; Funkiewiez et al., 2004; Castelli et al., 2006; Klempírová et al., 2007; Ory-Magne et al., 2007; Fasano et al., 2010; Asahi et al., 2014; Rizzone et al., 2014; You et al., 2020).
Meta-analyses reveal inconsistent outcomes in terms of processing speed. A prior meta-analysis and an observational study involving solely STN-DBS patients reported no significant differences in processing speed (Castelli et al., 2006; Parsons et al., 2006), while one study found that STN-DBS improves reaction times (Temel et al., 2006). Similar results were found in two recent meta-analyses and a controlled clinical trial comparing STN-DBS and BMT control patients (Williams et al., 2011; Xie et al., 2016; Wang et al., 2021). Slightly worse performance on testing has been found in STN-DBS patients compared to GPi-DBS patients in several studies (Combs et al., 2015; Tan et al., 2016; Wang et al., 2016). This was also seen in randomized controlled trials by Weaver et al. (2009) and Rothlind et al. (2015). A decline in processing speed was also found in unilateral STN-DBS and GPi-DBS patients (Zahodne et al., 2009a; Mikos et al., 2010), as well as PPN-DBS patients (Leimbach et al., 2019).
Results of cognitive testing in the domain of attention are not frequently reported in studies. One meta-analysis comparing STN-DBS to BMT and one study with only STN-DBS patients found no significant change in DBS patients (Parsons et al., 2006; Xie et al., 2016; Wang et al., 2021). Some slight changes were observed comparing STN-DBS to GPi-DBS, with worse results in the STN-DBS groups (Combs et al., 2015; Wang et al., 2016). The vast majority of controlled clinical trials found no changes in STN-DBS patients compared to BMT PD patients (Gironell et al., 2003; Zangaglia et al., 2009; Castelli et al., 2010; Sáez-Zea et al., 2012; Merola et al., 2014; Foki et al., 2017; You et al., 2020), with the exception of single study finding worsening of symptoms (Smeding et al., 2006). A randomized controlled trial by Tramontana et al. (2015) revealed worsening at the first control visit 12 months after the procedure, that largely diminished 24 months after the procedure, while Dafsari et al. (2020) found improvement in attention after STN-DBS compared to BMT PD patients.
The cognitive domain of memory was assessed in numerous studies, with conflicting results. Meta-analyses generally point to a slight decline in working and general memory mostly in STN-DBS patients compared to GPi-DBS and BMT patients (Combs et al., 2015; Wang et al., 2016; Xie et al., 2016), with only a study by Wang et al. (2021) showing no significant changes, but a trend of worsening in STN-DBS patients compared with BMT. More conflicting findings are found in randomized controlled trials and controlled clinical trials, with slightly fewer studies finding worsening of memory and intact learning (Smeding et al., 2006; York et al., 2008; Weaver et al., 2009, 2012; Rothlind et al., 2015), and no changes compared to BMT controls or between STN-DBS and GPi-DBS patients (Gironell et al., 2003; Zangaglia et al., 2009; Castelli et al., 2010; Daniels et al., 2010; Merola et al., 2011, 2014; Sáez-Zea et al., 2012; Tramontana et al., 2015; Boel et al., 2016; Foki et al., 2017).
Visuospatial function testing reveals no change in STN-DBS vs BMT patients in all meta-analyses (Xie et al., 2016; Wang et al., 2021), as well as most randomized clinical trials (Weaver et al., 2009; Tramontana et al., 2015), and controlled clinical trials (Gironell et al., 2003; York et al., 2008; Merola et al., 2011; Acera et al., 2019). One randomized controlled trial reported a slight decline in STN-DBS patients compared to GPi-DBS patients (Weaver et al., 2012), that was not seen in a different trial during a similar time frame (Boel et al., 2016). Three controlled clinical trials and one observational study reported improvement in visuospatial function and visuoconstructional task (Schoenberg et al., 2008; Zahodne et al., 2009a; Mikos et al., 2010; You et al., 2020).
Quality of life is an important metric for measuring treatment benefits and the impact of possible adverse effects. DBS led to an increase in overall quality of life in both meta-analyses that reported results in this category, one of which reported a more significant improvement in GPi-DBS patients, and the other reported no changes between two targets (Tan et al., 2016; Wang et al., 2016). The same was found in two randomized controlled trials, one comparing STN-DBS and GPi-DBS, and another comparing STN-DBS with BMT patients (Smeding et al., 2006; Weaver et al., 2012). One randomized controlled trial focusing on early DBS intervention found significant improvement in quality of life in STN-DBS patients compared to BMT (Schuepbach et al., 2013). Quality of life appears to be connected to baseline cognitive functioning, as lower baseline functioning was related to worse outcomes in several studies (Zahodne et al., 2009b; Witt et al., 2011; Gruber et al., 2019). Furthermore, STN-DBS led to a reduction of quality of life when measuring communication, which was related to declines in fluency (Zahodne et al., 2009b). Importantly, this decline did not have a meaningful effect on daily activities in quality of life in the long term (Contarino et al., 2007).
Motor improvement post-DBS is well known and described in the literature (Bratsos et al., 2018). When looking at the effects of DBS on cognition, much is still uncertain due to some limitations in the field. It is clear that there is a profound difference in the number of patients when taking possible targets into account, with sparse studies of ventral intermediate nucleus of thalamus DBS (VIM-DBS) or PPN-DBS (Combs et al., 2015; Tan et al., 2016; Wang et al., 2016), which is a consequence of clinical practices and general preference for STN-DBS. Additional limitations in the field are a lack of long-term studies, as DBS can be used for more years by patients than present in the longest studies cited in this review (Hitti et al., 2019), and a small proportion of randomized controlled studies with large sample sizes. The primary questions addressed in this systematic review are how DBS affects cognition and whether this information can be utilized to guide individual therapy approaches, thereby avoiding potential detrimental effects.
With regard to global cognition, the studies with the strongest quality of evidence show that there is a slight decrease when comparing STN-DBS to BMT and GPi-DBS patients (Combs et al., 2015, 20; Xie et al., 2016). However, the majority of randomized controlled trials, controlled clinical trials and observational studies did not find any changes in global cognition, either when comparing STN-DBS and GPi-DBS, or STN-DBS to BMT, indicating that the overall effect is not large (Witt et al., 2004, 2008; Schüpbach et al., 2006; Smeding et al., 2006; Contarino et al., 2007; Klempírová et al., 2007; Heo et al., 2008; York et al., 2008; Okun et al., 2009; Weaver et al., 2009; Zahodne et al., 2009b; Castelli et al., 2010; Daniels et al., 2010; Williams et al., 2011; Asahi et al., 2014; Tang et al., 2015; Vats et al., 2019). This is further corroborated by studies that show no significant in the improvement of life quality, which is comparable in both targets (Smeding et al., 2006; Weaver et al., 2012; Tan et al., 2016; Wang et al., 2016). A long-term observational study covering patients up to 14 years after surgery reveled a decline in global functioning, however, the study was not controlled and overall declines in cognition are expected with aging (Volonté et al., 2021). Even so, it looks like both the STN DBS and the GPi DBS seem to be safe when it comes to cognitive function, with only small differences in performance that don’t have a big impact on quality of life.
Additionally, it is critical to emphasize the major findings on changes in specific cognitive functions. Most of the cited studies reported and assessed changes in fluency, with the vast majority of studies, including all meta-analyses, reporting a statistically significant decline in semantic or phonemic fluency in STN-DBS patients compared to both BMT and GPi-DBS patients (Gironell et al., 2003; Funkiewiez et al., 2004; Castelli et al., 2006, 2010; Smeding et al., 2006; Contarino et al., 2007; Heo et al., 2008; Schoenberg et al., 2008; Higginson et al., 2009; Zangaglia et al., 2009; Fasano et al., 2010; Merola et al., 2011, 2014; Williams et al., 2011; Sáez-Zea et al., 2012; Combs et al., 2015; Houvenaghel et al., 2015; Tang et al., 2015; Tan et al., 2016; Wang et al., 2016, 2021; Xie et al., 2016; Foki et al., 2017; Leimbach et al., 2019; Szlufik et al., 2020). Even greater deterioration of fluency has been described in VIM-DBS and PPN-DBS compared to STN-DBS, albeit in studies with a small sample, highlighting the need for further studies for these targets (Ehlen et al., 2014; Pinto et al., 2014). Importantly, there are indications that the deterioration in verbal fluency influences quality of life with regard to communication (Zahodne et al., 2009b), even though it did not have a meaningful effect on daily activities in a study by Contarino et al. (2007). These findings may have a significant impact on patient progression, and clinicians should be aware that DBS may result in fluency deficiencies when compared to BMT.
Findings for other specific cognitive functions are not as clear as fluency, with frequent contradictory findings. The deterioration reported in two meta-analyses that compared either STN-DBS and GPi-DBS, and STN-DBS to BMT patients, was slight, while five other meta-analyses did not show statistically significant changes in executive function (Parsons et al., 2006; Combs et al., 2015; Tan et al., 2016; Wang et al., 2016, 2021; Xie et al., 2016). Studies with longer-term follow-up had reported diminishing in executive function over time, even though this was also not consistent (Zangaglia et al., 2009; Rothlind et al., 2015; Tramontana et al., 2015). Comparing STN-DBS and BMT patients in processing speed and attention did not reveal significant changes (Williams et al., 2011; Xie et al., 2016; Wang et al., 2021), while slight deterioration is seen compared to GPi-DBS patients (Weaver et al., 2009; Combs et al., 2015; Rothlind et al., 2015; Tan et al., 2016; Wang et al., 2016). Similar is found in memory and learning, again a minor change in direct comparisons, but statistically significant for the majority of meta-analysis (Combs et al., 2015; Wang et al., 2016, 2021; Xie et al., 2016). On the other hand, randomized controlled trials and controlled clinical trials did have conflicting results, with the majority reporting no changes in memory (Gironell et al., 2003; Smeding et al., 2006; York et al., 2008; Weaver et al., 2009, 2012; Zangaglia et al., 2009; Castelli et al., 2010; Daniels et al., 2010; Merola et al., 2011, 2014; Sáez-Zea et al., 2012; Rothlind et al., 2015; Tramontana et al., 2015; Foki et al., 2017). Interestingly, studies that reported no changes had generally longer timeframes for endpoints, and the decline was more pronounced in STN-DBS rather than GPi-DBS. The effect of DBS on visuospatial functions seems to be more straightforward, as most of the studies revealed no changes in function when comparing STN-DBS and BMT patients (Gironell et al., 2003; York et al., 2008; Weaver et al., 2009; Merola et al., 2011; Tramontana et al., 2015; Xie et al., 2016; Wang et al., 2021), with slight differences in STN-DBS and GPi-DBS patients in one randomized controlled study (Weaver et al., 2012). Importantly, three studies highlighted improvements in visuospatial function and visuoconstructional task (Schoenberg et al., 2008; Zahodne et al., 2009a; Mikos et al., 2010). Taken together, these findings indicate that while the effects of DBS on specific cognitive functions are complex and variable, they almost always result in mild to moderate impairments in fluency, with conflicting findings for executive function, processing speed, attention, and memory, and no change or even slight improvement in visuospatial functions. The changes are less pronounced in GPi-DBS than in STN-DBS, PPN-DBS, or VIM-DBS, the latter two of which lack sufficient data to draw strong conclusions. Keeping this in mind can aid in patient selection for STN or GPi targets, even if the differences are minor.
Another key question is if we can lessen the likelihood of DBS having a detrimental effect on cognition. A randomized controlled trial by Witt et al. (2011) revealed that borderline global cognitive scores at baseline can lead to decreases in cognitive functioning after the procedure, significantly worsening the quality of life. The majority of patients repeatedly tested by the Repeatable Battery of Neuropsychological status remained stable, although patients who had difficulties in pre-surgical testing worsened after (Rinehardt et al., 2010). The importance of cognitive screening is also highlighted by several observational studies, as lower baseline global cognitive function was a predictor of worse outcomes in short and long term (Perriol et al., 2006; Tir et al., 2007; Tsai et al., 2009; Fukaya et al., 2017; Acera et al., 2019). All the studies mentioned in this paragraph are based on STN-DBS PD patients, and it would be interesting to see if GPi-DBS could be used to improve outcomes in patients who have slight cognitive impairment before the procedure.
It is relevant to highlight a potential limitation of our systematic review regarding the clinical applicability of the results, which is the potential relevance of genetic factors in cognitive outcomes of DBS therapy. Recent advances in the field of PD genetics highlight the potential importance of common risk and pathogenic variants such as GBA or LRRK2 on DBS outcomes, as unfavorable cognitive outcomes have been linked to GBA mutation carriers and certain LRRK2 phenotypes (Ligaard et al., 2019). This could allow for more personalized treatment based on a person’s genetics, and it should be looked into in both clinical trials and meta-analyses.
This review shows that cognitive performance can decline in PD patients, and that even small changes can have an effect on daily quality of life. Current research is significantly skewed toward the effects of STN-DBS, followed by studies on GPi-DBS. The evidence thus far indicates that the highest occurrence of impairment can be seen in verbal fluency, while inconclusive evidence is still present for executive function, memory, attention, and processing speed. Global cognition does not appear to be significantly impacted by DBS, especially if cognitive screening is performed prior to the procedure, as lower baseline cognition is associated with worse outcomes. As a result, risk can be mitigated by tailoring the approach to each patient and testing cognitive function prior to the treatment. Additional randomized controlled studies are required to increase the level of evidence, especially in the case of GPi-DBS, PPN-DBS, and VIM-DBS, and more long-term studies are required for all respective targets.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
VR, DC, and VV conceptualized the systematic review. VR, MH, GR, EP, MR, DC, and VV developed and consulted on the search strategy and methodology. VR, MH, GR, and EP assisted with screening articles. VR, MH, and GR abstracted data from the articles. VR drafted the manuscript. All authors reviewed, edited, assisted with writing subsequent drafts of the manuscript, and approved the final version of the manuscript.
This research was supported by the Croatian Science Foundation project CSF-IP-2020-02-4308.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnhum.2022.867055/full#supplementary-material
Acera, M., Molano, A., Tijero, B., Bilbao, G., Lambarri, I., Villoria, R., et al. (2019). Long-term impact of subthalamic stimulation on cognitive function in patients with advanced Parkinson’s disease. Neurología (Engl. Ed.) 34, 573–581. doi: 10.1016/j.nrleng.2017.05.008
Armstrong, M. J., and Okun, M. S. (2020). Diagnosis and treatment of Parkinson disease: a review. JAMA 323, 548–560. doi: 10.1001/jama.2019.22360
Asahi, T., Nakamichi, N., Takaiwa, A., Kashiwazaki, D., Koh, M., Dougu, N., et al. (2014). Impact of bilateral subthalamic stimulation on motor/cognitive functions in Parkinson’s disease. Neurol. Med. Chir. (Tokyo) 54, 529–536. doi: 10.2176/nmc.oa.2013-0364
Bloem, B. R., Okun, M. S., and Klein, C. (2021). Parkinson’s disease. Lancet 397, 2284–2303. doi: 10.1016/S0140-6736(21)00218-X
Boel, J. A., Odekerken, V. J. J., Schmand, B. A., Geurtsen, G. J., Cath, D. C., Figee, M., et al. (2016). Cognitive and psychiatric outcome 3 years after Globus pallidus pars Interna or subthalamic nucleus deep brain stimulation for Parkinson’s disease. Parkinsonism Relat. Disord. 33, 90–95. doi: 10.1016/j.parkreldis.2016.09.018
Braak, H., Tredici, K. D., Rüb, U., de Vos, R. A. I., Jansen Steur, E. N. H., and Braak, E. (2003). Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 24, 197–211. doi: 10.1016/S0197-4580(02)00065-9
Bratsos, S., Karponis, D., and Saleh, S. N. (2018). Efficacy and safety of deep brain stimulation in the treatment of Parkinson’s disease: a systematic review and meta-analysis of randomized controlled trials. Cureus 10:e3474. doi: 10.7759/cureus.3474
Castelli, L., Perozzo, P., Zibetti, M., Crivelli, B., Morabito, U., Lanotte, M., et al. (2006). Chronic deep brain stimulation of the subthalamic nucleus for Parkinson’s disease: effects on cognition, mood, anxiety and personality traits. Eur. Neurol. 55, 136–144. doi: 10.1159/000093213
Castelli, L., Rizzi, L., Zibetti, M., Angrisano, S., Lanotte, M., and Lopiano, L. (2010). Neuropsychological changes 1-year after subthalamic DBS in PD patients: a prospective controlled study. Parkinsonism Relat. Disord. 16, 115–118. doi: 10.1016/j.parkreldis.2009.08.010
Combs, H. L., Folley, B. S., Berry, D. T. R., Segerstrom, S. C., Han, D. Y., Anderson-Mooney, A. J., et al. (2015). Cognition and depression following deep brain stimulation of the subthalamic nucleus and Globus Pallidus Pars internus in Parkinson’s disease: a meta-analysis. Neuropsychol. Rev. 25, 439–454. doi: 10.1007/s11065-015-9302-0
Contarino, M. F., Daniele, A., Sibilia, A. H., Romito, L. M. A., Bentivoglio, A. R., Gainotti, G., et al. (2007). Cognitive outcome 5 years after bilateral chronic stimulation of subthalamic nucleus in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 78, 248–252. doi: 10.1136/jnnp.2005.086660
Dafsari, H. S., Dos Santos Ghilardi, M. G., Visser-Vandewalle, V., Rizos, A., Ashkan, K., Silverdale, M., et al. (2020). Beneficial nonmotor effects of subthalamic and pallidal neurostimulation in Parkinson’s disease. Brain Stimul. 13, 1697–1705. doi: 10.1016/j.brs.2020.09.019
Damier, P., Hirsch, E. C., Agid, Y., and Graybiel, A. M. (1999). The substantia nigra of the human brain: II. Patterns of loss of dopamine-containing neurons in Parkinson’s disease. Brain 122, 1437–1448. doi: 10.1093/brain/122.8.1437
Daniels, C., Krack, P., Volkmann, J., Pinsker, M. O., Krause, M., Tronnier, V., et al. (2010). Risk factors for executive dysfunction after subthalamic nucleus stimulation in Parkinson’s disease. Mov. Disord. 25, 1583–1589. doi: 10.1002/mds.23078
Dujardin, K., Defebvre, L., Krystkowiak, P., Blond, S., and Destée, A. (2001). Influence of chronic bilateral stimulation of the subthalamic nucleus on cognitive function in Parkinson’s disease. J. Neurol. 248, 603–611. doi: 10.1007/s004150170139
Ehlen, F., Schoenecker, T., Kühn, A. A., and Klostermann, F. (2014). Differential effects of deep brain stimulation on verbal fluency. Brain Lang. 134, 23–33. doi: 10.1016/j.bandl.2014.04.002
Fang, C., Lv, L., Mao, S., Dong, H., and Liu, B. (2020). Cognition deficits in Parkinson’s disease: mechanisms and treatment. Parkinsons Dis. 2020:2076942. doi: 10.1155/2020/2076942
Fasano, A., Romito, L. M., Daniele, A., Piano, C., Zinno, M., Bentivoglio, A. R., et al. (2010). Motor and cognitive outcome in patients with Parkinson’s disease 8 years after subthalamic implants. Brain 133, 2664–2676. doi: 10.1093/brain/awq221
Foki, T., Hitzl, D., Pirker, W., Novak, K., Pusswald, G., Auff, E., et al. (2017). Assessment of individual cognitive changes after deep brain stimulation surgery in Parkinson’s disease using the Neuropsychological Test Battery Vienna short version. Wien. Klin. Wochenschr. 129, 564–571. doi: 10.1007/s00508-017-1169-z
Fukaya, C., Watanabe, M., Kobayashi, K., Oshima, H., Yoshino, A., and Yamamoto, T. (2017). Predictive factors for long-term outcome of subthalamic nucleus deep brain stimulation for Parkinson’s disease. Neurol. Med. Chir. (Tokyo) 57, 166–171. doi: 10.2176/nmc.oa.2016-0114
Funkiewiez, A., Ardouin, C., Caputo, E., Krack, P., Fraix, V., Klinger, H., et al. (2004). Long term effects of bilateral subthalamic nucleus stimulation on cognitive function, mood, and behaviour in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 75, 834–839. doi: 10.1136/jnnp.2002.009803
Gironell, A., Kulisevsky, J., Rami, L., Fortuny, N., García-Sánchez, C., and Pascual-Sedano, B. (2003). Effects of pallidotomy and bilateral subthalamic stimulation on cognitive function in Parkinson disease. A controlled comparative study. J. Neurol. 250, 917–923. doi: 10.1007/s00415-003-1109-x
Gruber, D., Calmbach, L., Kühn, A. A., Krause, P., Kopp, U. A., Schneider, G.-H., et al. (2019). Longterm outcome of cognition, affective state, and quality of life following subthalamic deep brain stimulation in Parkinson’s disease. J. Neural Transm. (Vienna) 126, 309–318. doi: 10.1007/s00702-019-01972-7
Heo, J.-H., Lee, K.-M., Paek, S. H., Kim, M.-J., Lee, J.-Y., Kim, J.-Y., et al. (2008). The effects of bilateral subthalamic nucleus deep brain stimulation (STN DBS) on cognition in Parkinson disease. J. Neurol. Sci. 273, 19–24. doi: 10.1016/j.jns.2008.06.010
Higginson, C. I., Wheelock, V. L., Levine, D., King, D. S., Pappas, C. T. E., and Sigvardt, K. A. (2009). The clinical significance of neuropsychological changes following bilateral subthalamic nucleus deep brain stimulation for Parkinson’s disease. J. Clin. Exp. Neuropsychol. 31, 65–72. doi: 10.1080/13803390801982734
Hitti, F. L., Ramayya, A. G., McShane, B. J., Yang, A. I., Vaughan, K. A., and Baltuch, G. H. (2019). Long-term outcomes following deep brain stimulation for Parkinson’s disease. J. Neurosurg. 132, 205–210. doi: 10.3171/2018.8.JNS182081
Houvenaghel, J.-F., Le Jeune, F., Dondaine, T., Esquevin, A., Robert, G. H., Péron, J., et al. (2015). Reduced verbal fluency following subthalamic deep brain stimulation: a frontal-related cognitive deficit? PLoS One 10:e0140083. doi: 10.1371/journal.pone.0140083
Klempírová, O., Jech, R., Urgosík, D., Klempír, J., Spacková, N., Roth, J., et al. (2007). Deep brain stimulation of the subthalamic nucleus and cognitive functions in Parkinson’s disease. Prague Med. Rep. 108, 315–323.
Leimbach, F., Gratwicke, J., Foltynie, T., Limousin, P., Zrinzo, L., and Jahanshahi, M. (2019). The effects of deep brain stimulation of the pedunculopontine nucleus on cognition in Parkinson’s disease and Progressive Supranuclear Palsy. Clin. Park. Relat. Disord. 1, 48–51. doi: 10.1016/j.prdoa.2019.08.001
Ligaard, J., Sannæs, J., and Pihlstrøm, L. (2019). Deep brain stimulation and genetic variability in Parkinson’s disease: a review of the literature. NPJ Parkinsons Dis. 5, 1–10. doi: 10.1038/s41531-019-0091-7
Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., et al. (2012). Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: movement Disorder Society Task Force guidelines. Mov. Disord. 27, 349–356. doi: 10.1002/mds.24893
Lozano, A. M., Lipsman, N., Bergman, H., Brown, P., Chabardes, S., Chang, J. W., et al. (2019). Deep brain stimulation: current challenges and future directions. Nat. Rev. Neurol. 15, 148–160. doi: 10.1038/s41582-018-0128-2
Mehanna, R., Bajwa, J. A., Fernandez, H., and Wagle Shukla, A. A. (2017). Cognitive impact of deep brain stimulation on Parkinson’s disease patients. Parkinsons Dis. 2017:3085140. doi: 10.1155/2017/3085140
Merola, A., Rizzi, L., Zibetti, M., Artusi, C. A., Montanaro, E., Angrisano, S., et al. (2014). Medical therapy and subthalamic deep brain stimulation in advanced Parkinson’s disease: a different long-term outcome? J. Neurol. Neurosurg. Psychiatry 85, 552–559. doi: 10.1136/jnnp-2013-305271
Merola, A., Zibetti, M., Angrisano, S., Rizzi, L., Lanotte, M., and Lopiano, L. (2011). Comparison of subthalamic nucleus deep brain stimulation and Duodopa in the treatment of advanced Parkinson’s disease. Mov. Disord. 26, 664–670. doi: 10.1002/mds.23524
Mikos, A., Zahodne, L., Okun, M. S., Foote, K., and Bowers, D. (2010). Cognitive declines after unilateral deep brain stimulation surgery in Parkinson’s disease: a controlled study using Reliable Change, part II. Clin. Neuropsychol. 24, 235–245. doi: 10.1080/13854040903277297
Odekerken, V. J. J., Boel, J. A., Geurtsen, G. J., Schmand, B. A., Dekker, I. P., de Haan, R. J., et al. (2015). Neuropsychological outcome after deep brain stimulation for Parkinson disease. Neurology 84, 1355–1361. doi: 10.1212/WNL.0000000000001419
Odekerken, V. J. J., Boel, J. A., Schmand, B. A., de Haan, R. J., Figee, M., van den Munckhof, P., et al. (2016). GPi vs STN deep brain stimulation for Parkinson disease: three-year follow-up. Neurology 86, 755–761. doi: 10.1212/WNL.0000000000002401
Odekerken, V. J., van Laar, T., Staal, M. J., Mosch, A., Hoffmann, C. F., Nijssen, P. C., et al. (2013). Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): a randomised controlled trial. Lancet Neurol. 12, 37–44. doi: 10.1016/S1474-4422(12)70264-8
Okun, M. S., Fernandez, H. H., Wu, S. S., Kirsch-Darrow, L., Bowers, D., Bova, F., et al. (2009). Cognition and mood in Parkinson’s disease in subthalamic nucleus versus globus pallidus interna deep brain stimulation: the COMPARE trial. Ann. Neurol. 65, 586–595. doi: 10.1002/ana.21596
Ory-Magne, F., Brefel-Courbon, C., Simonetta-Moreau, M., Fabre, N., Lotterie, J. A., Chaynes, P., et al. (2007). Does ageing influence deep brain stimulation outcomes in Parkinson’s disease? Mov. Disord. 22, 1457–1463. doi: 10.1002/mds.21547
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. doi: 10.1136/bmj.n71
Parsons, T. D., Rogers, S. A., Braaten, A. J., Woods, S. P., and Tröster, A. I. (2006). Cognitive sequelae of subthalamic nucleus deep brain stimulation in Parkinson’s disease: a meta-analysis. Lancet Neurol. 5, 578–588. doi: 10.1016/S1474-4422(06)70475-6
Perozzo, P., Rizzone, M., Bergamasco, B., Castelli, L., Lanotte, M., Tavella, A., et al. (2001). Deep brain stimulation of the subthalamic nucleus in Parkinson’s disease: comparison of pre- and postoperative neuropsychological evaluation. J. Neurol. Sci. 192, 9–15. doi: 10.1016/s0022-510x(01)00575-5
Perriol, M.-P., Krystkowiak, P., Defebvre, L., Blond, S., Destée, A., and Dujardin, K. (2006). Stimulation of the subthalamic nucleus in Parkinson’s disease: cognitive and affective changes are not linked to the motor outcome. Parkinsonism Relat. Disord. 12, 205–210. doi: 10.1016/j.parkreldis.2005.11.009
Phillips, L., Litcofsky, K. A., Pelster, M., Gelfand, M., Ullman, M. T., and Charles, P. D. (2012). Subthalamic nucleus deep brain stimulation impacts language in early Parkinson’s disease. PLoS One 7:e42829. doi: 10.1371/journal.pone.0042829
Pinto, S., Ferraye, M., Espesser, R., Fraix, V., Maillet, A., Guirchoum, J., et al. (2014). Stimulation of the pedunculopontine nucleus area in Parkinson’s disease: effects on speech and intelligibility. Brain 137, 2759–2772. doi: 10.1093/brain/awu209
Poewe, W., Seppi, K., Tanner, C. M., Halliday, G. M., Brundin, P., Volkmann, J., et al. (2017). Parkinson disease. Nat. Rev. Dis. Primers 3, 1–21. doi: 10.1038/nrdp.2017.13
Pollak, P. (2013). Deep brain stimulation for Parkinson’s disease - patient selection. Handb. Clin. Neurol. 116, 97–105. doi: 10.1016/B978-0-444-53497-2.00009-7
Rinehardt, E., Duff, K., Schoenberg, M., Mattingly, M., Bharucha, K., and Scott, J. (2010). Cognitive change on the repeatable battery of neuropsychological status (RBANS) in Parkinson’s disease with and without bilateral subthalamic nucleus deep brain stimulation surgery. Clin. Neuropsychol. 24, 1339–1354. doi: 10.1080/13854046.2010.521770
Rizzone, M. G., Fasano, A., Daniele, A., Zibetti, M., Merola, A., Rizzi, L., et al. (2014). Long-term outcome of subthalamic nucleus DBS in Parkinson’s disease: from the advanced phase towards the late stage of the disease? Parkinsonism Relat. Disord. 20, 376–381. doi: 10.1016/j.parkreldis.2014.01.012
Rothlind, J. C., York, M. K., Carlson, K., Luo, P., Marks, W. J., Weaver, F. M., et al. (2015). Neuropsychological changes following deep brain stimulation surgery for Parkinson’s disease: comparisons of treatment at pallidal and subthalamic targets versus best medical therapy. J. Neurol. Neurosurg. Psychiatry 86, 622–629. doi: 10.1136/jnnp-2014-308119
Sáez-Zea, C., Escamilla-Sevilla, F., Katati, M. J., and Mínguez-Castellanos, A. (2012). Cognitive effects of subthalamic nucleus stimulation in Parkinson’s disease: a controlled study. Eur. Neurol. 68, 361–366. doi: 10.1159/000341380
Schoenberg, M. R., Mash, K. M., Bharucha, K. J., Francel, P. C., and Scott, J. G. (2008). Deep brain stimulation parameters associated with neuropsychological changes in subthalamic nucleus stimulation for refractory Parkinson’s disease. Stereotact. Funct. Neurosurg. 86, 337–344. doi: 10.1159/000163554
Schuepbach, W. m. m., Rau, J., Knudsen, K., Volkmann, J., Krack, P., Timmermann, L., et al. (2013). Neurostimulation for Parkinson’s disease with early motor complications. N. Engl. J. Med. 368, 610–622. doi: 10.1056/NEJMoa1205158
Schüpbach, M., Gargiulo, M., Welter, M. L., Mallet, L., Béhar, C., Houeto, J. L., et al. (2006). Neurosurgery in Parkinson disease: a distressed mind in a repaired body? Neurology 66, 1811–1816. doi: 10.1212/01.wnl.0000234880.51322.16
Smeding, H. M. M., Speelman, J. D., Koning-Haanstra, M., Schuurman, P. R., Nijssen, P., van Laar, T., et al. (2006). Neuropsychological effects of bilateral STN stimulation in Parkinson disease: a controlled study. Neurology 66, 1830–1836. doi: 10.1212/01.wnl.0000234881.77830.66
Szlufik, S., Duszynska-Lysak, K., Przybyszewski, A., Laskowska-Levy, I., Drzewinska, A., Dutkiewicz, J., et al. (2020). The potential neuromodulatory impact of subthalamic nucleus deep brain stimulation on Parkinson’s disease progression. J. Clin. Neurosci. 73, 150–154. doi: 10.1016/j.jocn.2019.12.059
Tan, Z.-G., Zhou, Q., Huang, T., and Jiang, Y. (2016). Efficacies of globus pallidus stimulation and subthalamic nucleus stimulation for advanced Parkinson’s disease: a meta-analysis of randomized controlled trials. Clin. Interv. Aging 11, 777–786. doi: 10.2147/CIA.S105505
Tang, V., Zhu, C. X. L., Chan, D., Lau, C., Chan, A., Mok, V., et al. (2015). Evidence of improved immediate verbal memory and diminished category fluency following STN-DBS in Chinese-Cantonese patients with idiopathic Parkinson’s disease. Neurol. Sci. 36, 1371–1377. doi: 10.1007/s10072-015-2117-1
Temel, Y., Blokland, A., Ackermans, L., Boon, P., van Kranen-Mastenbroek, V. H. J. M., Beuls, E. a. M., et al. (2006). Differential effects of subthalamic nucleus stimulation in advanced Parkinson disease on reaction time performance. Exp. Brain Res. 169, 389–399. doi: 10.1007/s00221-005-0151-6
Tir, M., Devos, D., Blond, S., Touzet, G., Reyns, N., Duhamel, A., et al. (2007). Exhaustive, one-year follow-up of subthalamic nucleus deep brain stimulation in a large, single-center cohort of parkinsonian patients. Neurosurgery 61, 297–304; discussion 304–305. doi: 10.1227/01.NEU.0000285347.50028.B9
Tramontana, M. G., Molinari, A. L., Konrad, P. E., Davis, T. L., Wylie, S. A., Neimat, J. S., et al. (2015). Neuropsychological effects of deep brain stimulation in subjects with early stage Parkinson’s disease in a randomized clinical trial. J. Parkinsons Dis. 5, 151–163. doi: 10.3233/JPD-140448
Tsai, S.-T., Lin, S.-H., Chou, Y.-C., Pan, Y.-H., Hung, H.-Y., Li, C.-W., et al. (2009). Prognostic factors of subthalamic stimulation in Parkinson’s disease: a comparative study between short- and long-term effects. Stereotact. Funct. Neurosurg. 87, 241–248. doi: 10.1159/000225977
Vats, A., Amit, A., and Doshi, P. (2019). A comparative study of bilateral subthalamic nucleus DBS in Parkinson’s disease in young versus old: a single institutional study. J. Clin. Neurosci. 70, 85–91. doi: 10.1016/j.jocn.2019.08.065
Volonté, M. A., Clarizio, G., Galantucci, S., Scamarcia, P. G., Cardamone, R., Barzaghi, L. R., et al. (2021). Long term follow-up in advanced Parkinson’s disease treated with DBS of the subthalamic nucleus. J. Neurol. 268, 2821–2830. doi: 10.1007/s00415-021-10430-y
Vuletic, V., Racki, V., Chudy, D., and Bogdanovic, N. (2019). Deep Brain Stimulation in Non-motor Symptoms of Neurodegenerative Diseases. London: IntechOpen. doi: 10.5772/intechopen.88430
Wang, J., Pan, R., Cui, Y., Wang, Z., and Li, Q. (2021). Effects of deep brain stimulation in the subthalamic nucleus on neurocognitive function in patients with Parkinson’s disease compared with medical therapy: a meta-analysis. Front. Neurol. 12:610840. doi: 10.3389/fneur.2021.610840
Wang, J.-W., Zhang, Y.-Q., Zhang, X.-H., Wang, Y.-P., Li, J.-P., and Li, Y.-J. (2016). Cognitive and psychiatric effects of STN versus GPi deep brain stimulation in Parkinson’s disease: a meta-analysis of randomized controlled trials. PLoS One 11:e0156721. doi: 10.1371/journal.pone.0156721
Weaver, F. M., Follett, K. A., Stern, M., Luo, P., Harris, C. L., Hur, K., et al. (2012). Randomized trial of deep brain stimulation for Parkinson disease: thirty-six-month outcomes. Neurology 79, 55–65. doi: 10.1212/WNL.0b013e31825dcdc1
Weaver, F. M., Follett, K., Stern, M., Hur, K., Harris, C., Marks, W. J., et al. (2009). Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: a randomized controlled trial. JAMA 301, 63–73. doi: 10.1001/jama.2008.929
Williams, A. E., Arzola, G. M., Strutt, A. M., Simpson, R., Jankovic, J., and York, M. K. (2011). Cognitive outcome and reliable change indices two years following bilateral subthalamic nucleus deep brain stimulation. Parkinsonism Relat. Disord. 17, 321–327. doi: 10.1016/j.parkreldis.2011.01.011
Witt, K., Daniels, C., Krack, P., Volkmann, J., Pinsker, M. O., Kloss, M., et al. (2011). Negative impact of borderline global cognitive scores on quality of life after subthalamic nucleus stimulation in Parkinson’s disease. J. Neurol. Sci. 310, 261–266. doi: 10.1016/j.jns.2011.06.028
Witt, K., Daniels, C., Reiff, J., Krack, P., Volkmann, J., Pinsker, M. O., et al. (2008). Neuropsychological and psychiatric changes after deep brain stimulation for Parkinson’s disease: a randomised, multicentre study. Lancet Neurol. 7, 605–614. doi: 10.1016/S1474-4422(08)70114-5
Witt, K., Pulkowski, U., Herzog, J., Lorenz, D., Hamel, W., Deuschl, G., et al. (2004). Deep brain stimulation of the subthalamic nucleus improves cognitive flexibility but impairs response inhibition in Parkinson disease. Arch Neurol. 61, 697–700. doi: 10.1001/archneur.61.5.697
Wojtecki, L., Timmermann, L., Jörgens, S., Südmeyer, M., Maarouf, M., Treuer, H., et al. (2006). Frequency-dependent reciprocal modulation of verbal fluency and motor functions in subthalamic deep brain stimulation. Arch. Neurol. 63, 1273–1276. doi: 10.1001/archneur.63.9.1273
Xie, Y., Meng, X., Xiao, J., Zhang, J., and Zhang, J. (2016). Cognitive changes following bilateral deep brain stimulation of subthalamic nucleus in Parkinson’s disease: a meta-analysis. Biomed Res. Int. 2016:3596415. doi: 10.1155/2016/3596415
York, M. K., Dulay, M., Macias, A., Levin, H. S., Grossman, R., Simpson, R., et al. (2008). Cognitive declines following bilateral subthalamic nucleus deep brain stimulation for the treatment of Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 79, 789–795. doi: 10.1136/jnnp.2007.118786
You, Z., Wu, Y.-Y., Wu, R., Xu, Z.-X., Wu, X., and Wang, X.-P. (2020). Efforts of subthalamic nucleus deep brain stimulation on cognitive spectrum: from explicit to implicit changes in the patients with Parkinson’s disease for 1 year. CNS Neurosci. Ther. 26, 972–980. doi: 10.1111/cns.13392
Zahodne, L. B., Okun, M. S., Foote, K. D., Fernandez, H. H., Rodriguez, R. L., Kirsch-Darrow, L., et al. (2009a). Cognitive declines one year after unilateral deep brain stimulation surgery in Parkinson’s disease: a controlled study using reliable change. Clin. Neuropsychol. 23, 385–405.
Zahodne, L. B., Okun, M. S., Foote, K. D., Fernandez, H. H., Rodriguez, R. L., Wu, S. S., et al. (2009b). Greater improvement in quality of life following unilateral deep brain stimulation surgery in the globus pallidus as compared to the subthalamic nucleus. J. Neurol. 256, 1321–1329. doi: 10.1007/s00415-009-5121-7
Keywords: deep brain stimulation, cognitive outcome, cognition, systematic review, Parkinson’s disease
Citation: Rački V, Hero M, Rožmarić G, Papić E, Raguž M, Chudy D and Vuletić V (2022) Cognitive Impact of Deep Brain Stimulation in Parkinson’s Disease Patients: A Systematic Review. Front. Hum. Neurosci. 16:867055. doi: 10.3389/fnhum.2022.867055
Received: 31 January 2022; Accepted: 06 April 2022;
Published: 13 May 2022.
Edited by:
Delin Sun, Duke University, United StatesReviewed by:
Carmen Terranova, University of Messina, ItalyCopyright © 2022 Rački, Hero, Rožmarić, Papić, Raguž, Chudy and Vuletić. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vladimira Vuletić, dmxhZGltaXJhLnZ1bGV0aWNAdW5pcmkuaHI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.