 Muzee Kazamwali1
Muzee Kazamwali1 Arsène Kisanga2
Arsène Kisanga2 Juvenal B. Balegamire3
Juvenal B. Balegamire3 Euphrasie Kaningini2
Euphrasie Kaningini2 Jean-Benoît Falisse4Germaine Furaha2Denise M. Mapendo5
Jean-Benoît Falisse4Germaine Furaha2Denise M. Mapendo5 Clayton Boeyink4*
Clayton Boeyink4*- 1Faculté des Sciences Agronomiques et Environnement, Centre d’Excellence Denis Mukwege (CEDM-UEA), Bukavu, Democratic Republic of Congo
- 2Faculté des Sciences Economiques et de Gestion, Centre d’Excellence Denis Mukwege (CEDM-UEA), Bukavu, Democratic Republic of Congo
- 3Faculté des Sciences Sociales, Centre d’Excellence Denis Mukwege (CEDM-UEA), Bukavu, Democratic Republic of Congo
- 4Centre of African Studies, School of Social and Political Science, University of Edinburgh, Edinburgh, United Kingdom
- 5Fondation Panzi, Centre d’Excellence Denis Mukwege (CEDM-UEA), Bukavu, Democratic Republic of Congo
Introduction: Traditional, complementary and alternative medicine (TCAM) providers are central for many when seeking healthcare. Internally Displaced Persons (IDPs) are no exception. This paper seeks to better understand the use of TCAM by IDPs and its connection with the local integration of IDPs into the social fabric of the communities where they have taken refuge. We compare IDPs and non-IDPs access to TCAM providers and their level of confidence in having their healthcare needs met by these sources in Uvira and Kabare territories of South Kivu, Democratic Republic of Congo (DRC).
Methods: We draw from a mixed method, social connections design comprised of participatory workshops with 111 participants; a survey with 847 participants capturing exploring access and trust of TCAM and other wealth and demographic indicators; 24 interviews with traditional healthcare providers; and 56 in-depth life history interviews with IDPs. Collected data were analysed using both qualitative and quantitative approaches. Descriptive statistics (mean, percentage, and standard deviation) and statistical tests (proportions test and t test) were used as quantitative analysis tools whereas thematic content analysis was used for qualitative data.
Results: We show that IDPs use TCAM more than non IDPs. Access to and trust in traditional healers seems dependent on the exact nature of the services they offer, which varies across our sample. As such, processes of recognition and integration of both IDPs and TCAM providers into formal healthcare systems should be treated cautiously with an understanding of the socio-economic rationales that displaced people and TCAM providers operate under. While many of these TCAM providers are not highly trusted sources in South Kivu, their highly valued treatment of certain conditions such as what is locally known as “mulonge” (and bears similarities with the Buruli ulcer) suggest there may be potential specific areas where collaboration could be successful between biomedical health workers and TCAM providers.
Introduction
Since gaining independence in 1960, the Democratic Republic of Congo (DRC) has experienced several waves of armed conflicts in its eastern part among which the most recent can be traced back to the early 1990s. The two so-called liberation wars (1996 and 1998) and numerous rebellions and wars that followed had been responsible for massive population movements in this part of the country. Although various peace agreements repeatedly claimed to mark the end of war, and despite a series of elections organized in the country, violence remains widespread. Numerous small pockets of conflict, sometimes intercommunal or fanned by domestic and foreign armed groups, continue to feed this violence, increasing the number of displaced people in the country (Altare et al., 2020). In 2022, according to the Internal Displacement Monitoring Centre (IDMC) statistics, the DRC recorded 4 million displaced persons, most of them in the eastern provinces of the country (North Kivu, South Kivu and Ituri) following military operations carried out by the army against certain armed groups. For over a decade, the DRC has topped rankings of the countries hosting the highest number of Internally Displaced Persons (IDPs). Many IDPs, in general, and in South Kivu–the province our research focuses on–do not live in camp-type environments but are dispersed among host populations (Beyani, 2013; Jacobs et al., 2020).
IDPs typically find hosting arrangements with relatives, friends or through self-settlement for those with enough resources to rent a house. Those solutions are often unstable and return to places of origin often difficult before years or decades due to insecurity and damages. IDPs need, however, to be seen and understood as active agents within their host communities, looking for durable solutions for themselves and contributing to host communities’ economies through various income generating activities and services. In Bukavu for instance, making use of their social networks in their place of origin, IDPs have been described as enriching the city’s economy with honey, timber, palm oil, and charcoal (Jacobs et al., 2020).
Local integration is a long and gradual process. It goes smoothly for some and turns out to be challenging for others. It encompasses several dimensions that cannot been reduced to economic independence. Indeed, integration is also about being accepted by the host community, or trusted. Strong social connections and access to essential services are key to such integration and the well-being of IDPs. A key ‘domain of integration’, and the focus of the current study, is access to health-care (Ager and Strang, 2008).
Healthcare providers and IDPs in the DRC
The general situation with access to quality health is difficult in the DRC (Bapolisi et al., 2021), especially in rural areas (Ivlevs, 2019), for IDPs and non IDPs. The health system at both national and provincial levels faces major challenges. In a report published by the Ministère de la Santé, 2021, the analysis of health accounts showed that households remain the main contributors to current health expenditure in the Democratic Republic of Congo. Their financing of current expenditure increased by 29.3% (from USD 658,980,708 to 852,343,618, see Table 1) between 2016 and 2020. The government comes third after multilateral donors (Ministère de la Santé, 2021).

Table 1. Trend in the main aggregates of the health accounts from 2016 to 2020 in DRC.
At all levels, citizens, whether displaced or not, typically pay a substantial cost of healthcare out of their own pockets (Gerstl et al., 2013). Like other citizens, the IDPs find themselves exploring different options, both informal and formal, to find solutions to their health problems. Traditional, Complementary, and Alternative Medicine (TCAM)1 is one of the main, but also one of the least studied, options that displaced and non-displaced rely on when seeking healthcare. Most of Sub-Saharan Africa relies on TCAM to varying degrees, although a systematic review reveals that “there remains a dearth of research evidence […] on the drivers and facilitators of [TCAM] use, factors associated with TCAM use, and the impact of TCAM use on broader healthcare” (James et al., 2018, p. 1).
TCAM features prominently in the DRC, as with the rest of Sub-Saharan Africa. Over the past two decades, the World Health Organization (WHO) has recognized the important contributions of traditional and complementary medicines to healthcare worldwide and has developed a voluntary policy to engage member states in integrating locally important practices into their national health systems (WHO, 2013).2 As a WHO member country, the DRC is committed to promoting traditional medicine by integrating it into the official health system through laws and governmental censuses of TCAM (WHO, 2002), despite lacking the funding and capacity to comprehensively do so to this point (Mutombo et al., 2022). The Ministerial Order n°1,250/CAB/MIN/S/CJ/KIZ/32/2002 of 25 October 2002,3 identifies six different types of “traditional” healers: (1) phytotherapists are “recognized by their community as able to provide healthcare using plants, substances and other vegetal drugs”; (2) herbalists sell and utilize medicinal plants; (3) naturalists are “recognized by their community as able to provide healthcare using natural but non-vegetal substances”; (4) spiritualists are “recognized by their community as able to provide healthcare using religious or spiritual means”; (5) exorcists are “recognized by their community or religious hierarchy as able to provide mental or metaphysical healthcare by chasing away demons or evil spirits”; and (6) ritualists are “recognized by their community as being able to provide mental, metaphysical, or physical healthcare through incantations, dances, and other ritual practices.”
The reality regarding this classification is, however, much more complex as those categories often overlap. For instance, the boundary between a phytotherapist and a herbalist is blurry and other categories that are used by the population such as “fetishists” (féticheurs) and witch doctors do not necessarily fit neatly into one sub-category. The same applies to “exorcists” and “spiritualists” to whom we refer as exorcists in this paper. We also found the “ritualist” category rather broad and find it useful to divide it into sub-categories: catholic faith healers, protestant faith healers, religious leaders (pastors, priests or sheik) and other communities of faith. However, considering the use of some rituals in some of their practices, they will be considered here as ritualists. Religious leaders are differentiated from faith healers by the fact that they do not engage in direct, explicit, healing activities. They lead services and prayers but do not offer explicit healing services. In this paper, we will mostly uses the categories established by the Ministry –with the caveats we just mentioned– for the sake of convenience, but our argument is not about the different types of TCAM in the DRC and, ultimately, a different classification would probably have limited incidence on our findings.
Existing research
Research on TCAM in post-conflict settings in general remains limited, with some of the more recent studies in Burundi and Northern Uganda (Falisse et al., 2018; Mwaka et al., 2023). There are even fewer comprehensive studies on TCAM in refugee and internally displaced contexts (Ojeleke et al., 2022). Much of the work that exists in displacement contexts either touches briefly on TCAM as a small part of a general health inquiry (Roberts et al., 2022) or explores TCAM healers’ roles in combatting specific health crises, such as Ebola (Grant, 2018) and COVID-19 (Yesenia Olaya Requene, 2021). Roberts et al. (2022) focuses on differences between IDPs and refugees overseas development aid (ODA), stressing the relative lack of attention to IDPs. Possibly more directly relevant to our research and building on an anthropological perspective of spiritual beliefs around illness, death and health in South Sudan, Grant (2018) shows that traditional healers played an important role in the case of an Ebola outbreak in terms of surveillance and alerts within communities characterized by less trust toward the government system and where people use both traditional and biomedical health services. Traditional healers, although operating from an intricate and informal system, gained legitimacy within communities through demonstrated skills and compassion to the community. The present paper adopts yet another approach by directly engaging with displaced populations facing a wide range of medical issues.
The general reasons for using TCAM rather than biomedical health facilities (in non-conflict contexts) have generated an abundant literature [see for instance brief reviews in Uche (2017), Falisse et al. (2018), Mutombo et al. (2022)]. People consider TCAM less costly than biomedical health facilities (Uche, 2017) but trust, etiology (how people understand diseases), speed, and efficacy, among other factors, also matter (Mutombo et al., 2022). Overall, TCAM is likely to remain a key feature of African health-care for some time, with TCAM practitioners and biomedical health care providers existing and evolving in a parallel in a consumer-led delivery system (Boum et al., 2021). Indeed, even when in countries where major efforts for integrating TCAM into biomedical care have been made, such as Ghana (other examples include Nigeria, Mali, and Equatorial Guinea), a “power struggle” between traditional healers and biomedical health practitioners has been reported (Ampomah et al., 2020).
In the DRC, it has been found that recourse to traditional medicine is also shaped by limited access to the modern healthcare system (Shalukoma et al., 2016). In a study of Lubumbashi in the Haut-Katanga province of the DRC, nearly 80 per cent acknowledged having recently accessed TCAM, demonstrating the prominence of these healing practices (Mutombo et al., 2022). In South Kivu, however, another project reports much lower figures with only 5 % of respondents reporting TCAM as the first recourse of care (Bapolisi et al., 2021). Our main hypotheses is that it may be due to differences in the contexts –in particular, South Kivu had just seen a campaign against unregistered practitioners and side-effects of so-called “quacks” – but also in the exact question that was asked; the South Kivu project focused on “first recourse” (where do people go first), the Katanga one on “recourse at any point.” Interestingly, the Katanga research probed explanatory factors and reasons evoked for resorting to TCAM were much more efficacy, speed in healing and low cost. No significant relationship was found between religion, tribal affiliation, and recourse to TCAM, but the study emphasized the ability of the population to distinguish diseases for which TCAM constitutes the only possible care source.
Our paper builds on studies in the field of health in South Kivu that have already started addressing questions relating to health behavior in rural areas, including the factors affecting first recourse in seeking care (Bapolisi et al., 2021), or the routes taken to deal with sexual and gender-based violence (SGBV) using social connections (Boeyink et al., 2022; a paper which also provides more substantial background information on the population studied in the present paper). We focus on under-studied populations of IDPs. We do this bearing in mind Kadetz’s (2013) invitation to explore existing practices and preferences of patients in combination with a more thorough understanding of the characteristics of practitioners. Rather than focusing on levels of trust between TCAM and biomedical practitioners as in other studies (Akol et al., 2018; Krah et al., 2018), our point of departure is examining levels of trust and confidence patients have in TCAM practitioners.
The aim of this study is to document the use of non-biomedical healthcare by IDPs in South Kivu, and the extent to which the experience of displacement is affecting, or not, the use of such healthcare providers. Our study is guided by the following research questions, which will help us understand where care and access to social connections apply to integration processes: At what rates do IDPs and non-IDPs access TCAM? How much trust do IDPs and non-IDPs place in TCAM providers compared to formal healthcare providers? What are the types and characteristics of TCAM providers in South Kivu and what health services do they provide?
The rest of the paper is organized as follows. Firstly, we briefly review the literature on TCAM, identifying research on TCAM and trust between patients generally and among IDPs specifically. Secondly, we present our research methodology. The main discussion portion has two sections: The first section presents an overview of how our research participants access healthcare. This includes (a) the levels of access to traditional healthcare, (b) the demographic profiles of IDPs and non-IDPs who access TCAM; (c) the sources of health information people use to inform decisions; and (d) their level of trust and confidence they have in traditional healers. The second part of the results section (a) profiles the different characteristics of TCAM providers; (b) describes the services they provide and how they relate to IDPs’ concerns; and (c) outlines the economic dimension of TCAM services. The final section summarizes the findings and analyzes the policy implications.
Methodology
Study settings
Kabare and Uvira territories constitute the two selected sites for the current study. The Uvira site on the one hand, is composed of both rural and urban settings namely Katogota for war IDPs and Uvira town for floods IDPs. The Kabare site on the other hand comprises two rural sites namely Kavumu and Katana.
Katogota is a village located on the road between Bukavu and Uvira (town) on national road number 5. Victim of a massacre perpetrated by the Rassemblement Congolais pour la Démocratie (RCD-Goma) rebellion in 2000, Katogota subsequently experienced a massive influx of displaced people around 2009. Local authorities offered them a place to stay, and non-governmental organizations provided them with support. The space they were once given has now become a neighborhood in its own right. As for Uvira, it is an urban administration located 121.9 km south-east of Bukavu (capital of South Kivu province). In April 2020, the town was hit by torrential rain and flooding caused by the rising waters of the Mulongwe river. This led to the loss of several lives and the destruction of several houses. The victims were housed in several camps set up for them across the city. Only the Kasenga camp was given access by the local authorities.
Kavumu and Katana are two villages located more than 40 km north of Bukavu in the Bugorhe and Irhambi-Katana groupings, respectively. They are home to many war-displaced people from the surrounding villages (Karhanda, Mulangala, Kabulungu, Kabushwa etc.) who live among the rest of the population. The presence of a national airport in Kavumu and the FOMULAC (Fondation Médicale de l’Université de Louvain au Congo) hospital in Katana make these two villages two major hubs in Kabare territory.
Conceptual framework
Studying IDPs’ use of TCAM services within host communities as well as the role traditional healers play in the healthcare delivery system in South Kivu can be seen as studying the process of getting something valuable out of a society. It lays the foundations of IDPs’ integration in host communities through social connections. This study is therefore based on the Ager and Strang (2008) conceptual framework presented in Figure 1.
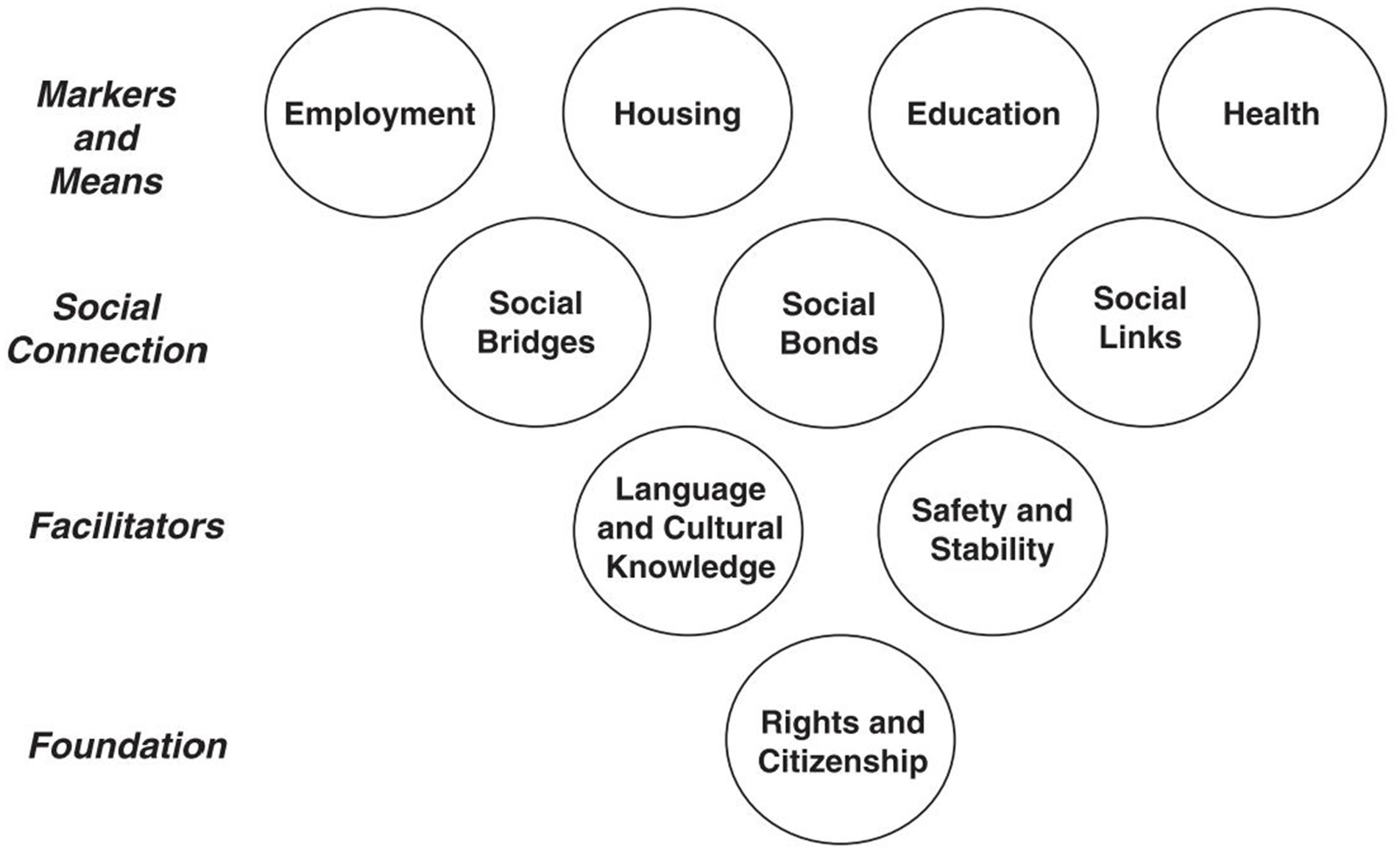
Figure 1. Ager and Strang’s conceptual framework of integration, from Ager and Strang (2008).
As depicted in Figure 1, integration is made of four main domains: markers and means; social connection; facilitators; and foundation (for more details about each domain of integration, see Ager and Strang (2008)). There has been a lot of debate regarding domains of integration and the concept itself. However, the most prominent argument against the afore-mentioned framework is its normative understanding of integration. It emphasizes more on how integration should look like, and not what it is in actual sense (Spencer and Charsley, 2021). Other scholars argue that more qualitative data are required to help capture interactions between indicators and the experiential side of integration (Phillimore and Goodson, 2008). Moreover, this conceptual framework, although designed for refugees, can also be adapted to suit IDPs’ context of integration (Bile et al., 2023). Thus, in the context of internal displacement, some domains of integration like foundation with citizenship and rights as main components are not usually considered since IDPs are in their own country. That is why the current study focuses on the use of traditional medicine among IDPs in their host communities by using the social connections tool.
Study design
A mixed research methodology was adopted for this study. The initial use of a quantitative approach aimed to identify the social connections to which displaced and non-displaced people often turn for help with their health problems. This methodology is based on the social-capital theory and was mainly developed to map and understand all kinds of social resources available to refugees or IDPs and how they are mobilized to protect and strengthen access to resources and their wellbeing (Strang and O’Brien, 2017; Strang and Quinn, 2021; Boeyink et al., 2022). These resources can be people or organizations IDPs go to in case of a problem or specific need, and which can play an important role for their integration in host communities. Based on real-life sample problems, this methodology can help generate a full list of potential social connections considered as relevant by IDPs and which can be considered as a proxy of their full range of connections.
It is worth mentioning that the “social connections” methodology does not impose any assumption regarding social connections or resources that would be considered as valuable in a particular context. Hence, information collected in this way would always be in relation to what is considered relevant by the collective participant group, and affected by cultural subgroups which different groups are made of (even within those living in close geographical areas) (Strang and O’Brien, 2017). The use of the social connections methodology in this study would not only provide general trends in this respect, but would also make it possible to quantify the relative importance of these connections and the level of trust placed in them. The same applies to non-displaced people. Incorporation of both displaced and non-displaced people would result from the fact that integration into a host environment is not a one-off process. On the contrary, it is seen as a two-way process that emphasizes mutual accommodation between displaced persons and members of their host community.
The use of qualitative methods, mostly interviews (including longer life histories) given the amount of time and resources available to us, enabled us to delve a little deeper into the lives of IDPs and the TCAM provider. It helped refine the explanations for the main trends identified with the quantitative approach and let emerge themes that were not integrated into the survey (because of our necessarily limited understanding of the topic prior to starting the research).
Sampling
As explained above, we started our research with a survey on a random sample of IDPs and non IDPs living in sites we knew hosted large IDP populations (see Study Settings above). The final sample size for the two target groups involved in this study is shown in the Table 2.
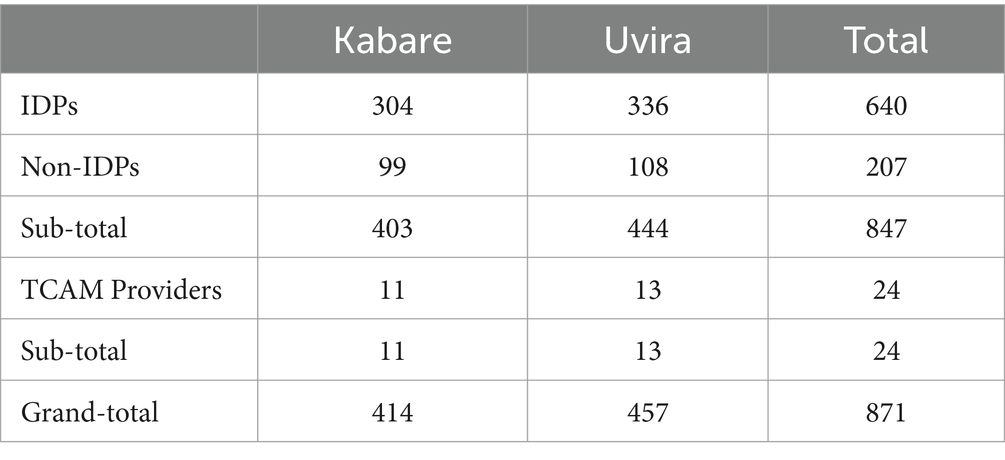
Table 2. Sample size distribution between Kabare and Uvira territories.
From the 640 IDPs sampled in this study, a total of 56 were selected from both areas (including 30 in Kabare and 26 in Uvira) for conducting in-depth interviews. They were purposefully selected based on their indicated willingness to talk more with us and their use of various health-care providers, including TCAM, and balancing gender, location, and age. As for TCAM practitioners, a total of 24 traditional healthcare providers were interviewed, including 13 in Uvira territory and 11 in Kabare territory. We started with a few contacts provided to us by the in-depth interview respondents and then used snowball sampling.
Data collection
Quantitative data
Implementation of the social connections methodology began with a series of participatory workshops of 8–12 people. Participants were both IDPs and non-IDPs but were grouped by gender (men and women separately). A series of three questions were discussed within each group regarding where somebody in their community would turn if suffering from “persistent physical pain” and “deep sadness” which impairs their daily functioning, as well as following incidences of SGBV. The responses given then created a list of social connections that the research team distilled to 30. This list of 30 social connections informed the quantitative survey made it possible to assess the extent and importance of the main channels used by IDPs to use the services of traditional care providers, as well as the quality of these links through the levels of trust they place in them. After giving basic demographic and economic information, the researcher went through each of the 30 social connections asking who they had contact with in the last 6 months when looking for help/support with their health or well-being (mental or physical). Another question on the questionnaire assessed through a scale of 1 to 5 (where 1 indicates no trust at all and 5 total trust) how much trust this person or organization was able to help with health-related issues.
The surveys covered the two territories in South Kivu, including Uvira and Kabare. Their implementation was facilitated by prior contacts with the respective administrative authorities of the different sites visited. These gatekeepers allowed us access to the sites inhabited by the IDPs. Local facilitators were used to ensure effective identification and contact. Surveys were generally carried out at the homes of respondents, depending on their availability. Thus, purposive sampling was used to select respondents.
Qualitative data
The individual interviews, drawing from previous survey participants who agreed to engage further in research, were semi-structured, using an interview guide. The interviews targeted IDPs and traditional healthcare providers. Three themes were discussed: health problems in the community (displaced and non-displaced people), the health behavior of displaced people, and the provision of and access to health services for internally displaced people. The interviews generally took place at the interviewees’ homes, and in some cases lasted more than an hour. Other individual interviews were conducted with IDPs in the form of life histories, gathering information on their origins, reasons for migration, migration route, living conditions and health problems encountered.
Data analysis
The qualitative data collected were subjected to thematic content analysis (TCA), which consists of “identifying in verbal or textual expressions recurring general themes which appear under various more concrete contents” (Mucchielli, 1996, p. 259). As for quantitative data, descriptive statistics were used mainly percentages and measures of central tendency. Comparisons of means and proportions have also been used to discriminate between IDPs and non-IDPs.
Ethics statement
The ethics committees of the School of Social and Political Science at the University of Edinburgh and the Université Evangélique en Afrique approved the project. Oral consent was deemed more appropriate and used for both the qualitative and the quantitative data collection. The research team was trained in ethics and safeguarding principles before the beginning of the research. The study was part of a larger UKRI-funded project ‘Improving healthcare at the intersection of gender and protracted displacement among Somali and Congolese refugees and IDPs’, which also considered displaced populations in Somalia, Kenya, and South Africa. More general cross-country findings that also pertain to TCAM will be published in subsequent publications.
Results and discussion
This section presents the results of the study. These can be divided into two main parts. The first focuses on the use of TCAM by IDPs. It presents data on IDPs’ access to traditional healthcare, their socio-economic profile, their main sources of health information and the level of confidence attached to the TCAM. The second part of the results then focuses on traditional healthcare providers. These include a description of their profile, the services they offer and finally the economics of traditional medicine.
Access to healthcare for IDPs vs. non-IDPs
The preliminary work on the social connections allowed us to identify a set of key actors that loosely fit the category of the “traditional” healthcare providers. They were then integrated into the survey, and we were able to analyze the responses to the question “Which people or organizations you have had contact with in the last six months when looking for help/support with your health or well-being (mental or physical)?” Across our four sites, we find that 64% of the IDPs cited at least one traditional healer or traditional healing practice as a way to access healthcare. Conversely, only 54% of the host community had recourse to TCAM in the considered period of time (p = 0.0095). On average, the IDPs cited 1.21 traditional providers, versus 0.87 for the host population (p = 0.0004). The main traditional care providers used by the two categories of respondents in the two settings are shown in Figure 2.

Figure 2. IDP/non-IDP access to traditional healers.
These include phytotherapists, herbalists, fetishists, various religious communities (Catholic, Protestant and Muslim) and religious leaders. Connections with different healthcare providers showed that IDPs were more likely than their non-displaced counterparts to use phytotherapists (15% versus 8%, p = 0.0323), herbalists (19% versus 8%, p = 0.0002), and religious leaders (21% versus 14%, p = 0.0167) for their mental and physical health and well-being problems. There was no significant difference between the two groups in their use of other providers such as exorcists or fetishists. Fetishists had very low rates of use compared with the rest of the providers for both IDPs and non-IDPs (2 and 1% respectively).
Generally speaking, displaced people are more likely than non-displaced people to seek healing services from specific TCAM providers such as exorcists, phytotherapists, herbalists, and ritualists. There are several possible reasons for this attitude. Lack of financial resources is primarily seen as the reason why IDPs turn to TCAM providers. Modern health facilities are considered too expensive for health care forcing IDPs to turn to traditional medicine, perceived to be cheaper.
One displaced woman in Uvira explained to us:
“My child has umbilical hernia. The disease started when he was 1 year old, and he is now 4. As far as I'm concerned, I think perhaps this illness is hereditary in our family because my biological brother suffers from this same illness… This illness has affected us a lot and we don't have sufficient funds to provide appropriate care for this child… I don't know the cause. It's not God's will, nor is it a supernatural illness… A friend of mine showed me a herbalist who tried using his amulets, but it didn't work. He had failed, moreover, he deceived us with his medicine. We went to another lady, also a traditional healer, who used her products to ease the pain. The child is sometimes relieved, but the illness remains. Relatives who came to see us advised to go to the hospital so that the child could undergo a surgery. That remains the only way of treating this illness. Due to a lack of funds, we stayed at home until then.”
TCAM providers are also seen as more flexible in terms of payment than biomedical healthcare providers –sometimes, as we explain below, their services can be free of charge. This is despite the proximity of biomedical health facilities. Often, and in line with the existing peer-reviewed research on the use of TCAM, people go to different types of healthcare providers depending on their issues (including social problems) (Tabi et al., 2006; Ndetei, 2007; Mutombo et al., 2022). TCAM providers are, for instance, seen as able to cast out all sorts of supernatural spells (some of which are associated with situations that affect displaced people). One of the displaced people from Kabare explained this arrangement:
“I was poisoned and have been suffering from stomach pains ever since (3 months ago). The pain is often excruciating but I can still walk. However, sometimes I can't get to work. Almost all my wages are spent on treating this illness. All my friends have abandoned me. Sometimes I think it's due to supernatural causes and other times I think it's God's will… At the hospital the treatment didn't work. I've never been satisfied because my illness remains the same. No change. I don't think they have the right medicines… I went to the pastors for prayers, but there too, there was no change. I thought it was witchcraft but there was no change. I went to the traditional healers, but again there was no change, and his medicine made the pain worse.”
Profiles of IDPs accessing TCAM
Traditional healers explained that their patients come from different ethnic groups, social classes, religious denominations and levels of education. A faith healer in Kabare explains:
“In the prayer rooms, we receive people of all religions, Catholics, Protestants and even Muslims. I recently had a young girl who had been a Muslim for 17 years. But she came to us, and we prayed for her. She even converted and married a Protestant boy. So we welcome everyone as they are. We have men who come to us, women and children so that we can pray for them… In my ministry, I also meet displaced people from places like Kahungu, Ziba and Bunyakiri who come here for various reasons such as security problems or other reasons.”
As for other TCAM providers, their patients include men and women of various levels of education and of all ages (children, young adults and the elderly). They are also of different professions (soldiers, footballers, aid workers), and originate from different tribes (Shi, Bembe, Fuliru, etc.) in South Kivu. Contrary to the way they are perceived by members of society, the clients or patients of the fetishists (and other non-Christian TCAM care providers) include people of different religious denominations, such as Catholics, Jehovah’s Witnesses and Protestants. According to the interviewees, however, Protestants hide when they go to the fetishists because of their religious convictions. This attitude is confirmed by studies by Koya (2016), which indicate that for many of the current generations in South Kivu or Bukavu, consulting a fetishist is going against their religion.
Our quantitative data also helps cast light on the socio-demographic characteristics associated with the use of traditional healers (see Table 3). Generally speaking, we find very few differences between users and non-users –be they IDP or not. Data in Table 3 below shows that women are slightly better represented among non-users in the IDP group. In terms of education, it can be observed that despite a significantly higher rate of illiteracy among non-users than among users of traditional medicine, the latter had relatively lower rates of school dropouts than TCAM non-users. This is consistent with the literature that finds that contrary to popular perceptions, the use of TCAM is widespread among all categories of the population (e.g., Falisse et al., 2018). The calculated wealth index (composed of the number of assets out of 20 items) shows that both groups of displaced people own fewer household assets, but again there are no differences between TCAM users and non-users. Information on maternal languages shows that IDPs speaking Swahili and Kifuliru as their mother tongues have a higher proportion of TCAM users. Although Swahili is a national language, and presumably second language for many, there are an increasing number of people who only speak Swahili without a good knowledge of other local languages (especially in urban areas). Catholic believers, as shown in the Table 3, are less represented among TCAM users.
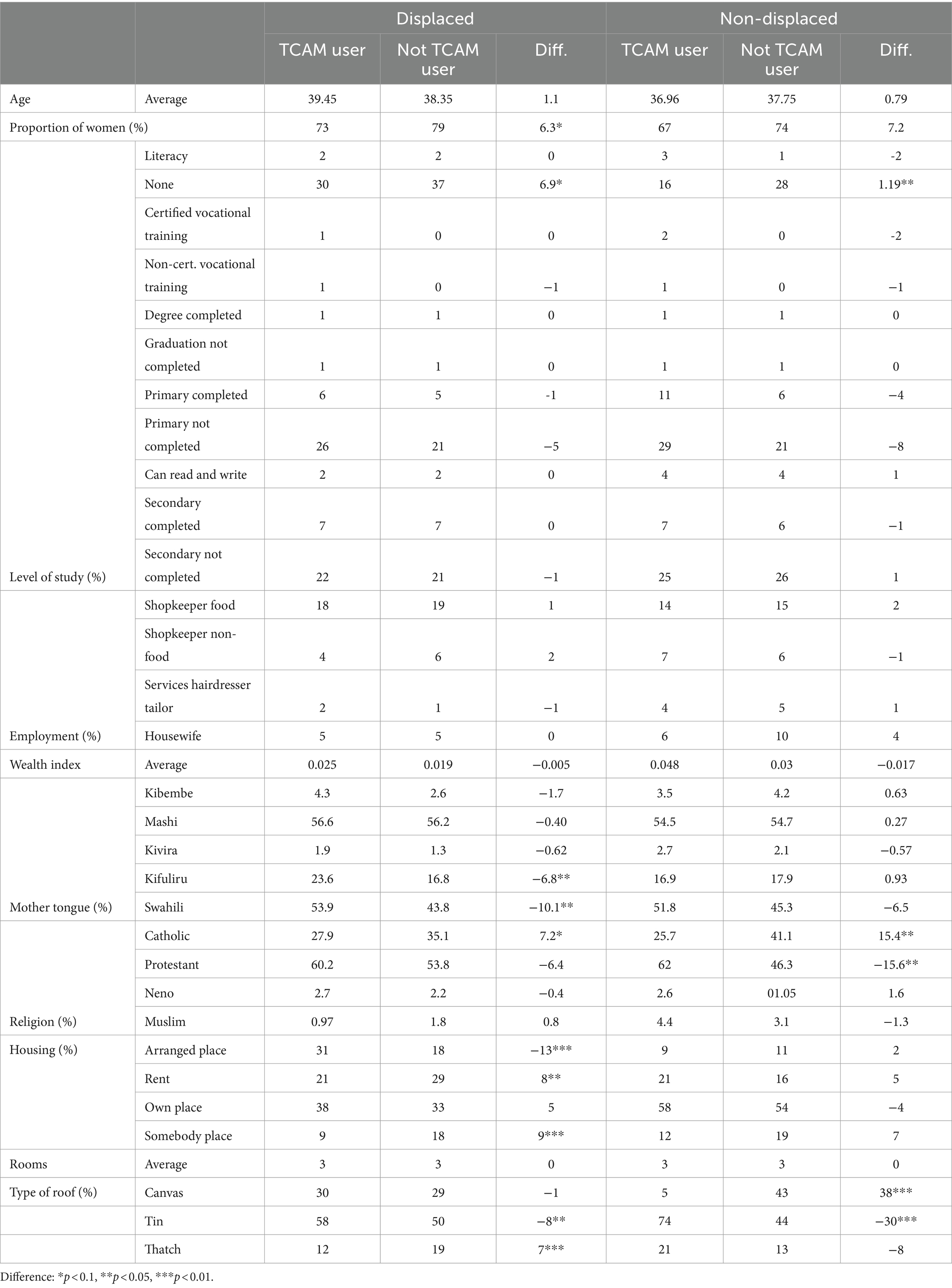
Table 3. Socio-demographic characteristics of IDPs and non-IDPSs.
Information on housing show that some IDPs have been able over time to own some plots within host communities. Statistics show that 38% of TCAM users (against 33% for non TCAM users) own places where they live. Others, on the other hand, either rent (21% of TCAM users compared with 29% of non-users) or live in places arranged for them by religious communities (31% of TCAM users compared with 18% of non-users). Another group live in places that do not belong to them but for which they pay nothing in return (9% of TCAM users compared with 18% of non-users). The relatively high proportions of displaced people living in places arranged by religious communities or charitable organizations can be explained by the presence of people displaced by disasters (especially in the territory of Uvira). The latter live in a camp, unlike the war-displaced, who live scattered in different communities.
Data on living conditions show that more than half of IDPs and many non-IDPs live in houses with tin roofs and composed of three rooms on average. Others live in houses with canvas roofs or made of thatch. This could be explained partly by the presence of people displaced by disasters living in Kasenga camp in Uvira and by the fact that data was also collected from rural areas. Although not included in Table 3, the data collected indicates that reasons for displacement remain numerous. However, the most dominant are war and intimidation for the most part (72%) and natural disasters (19%). Most war IDPs displaced from their place of origin came from neighboring villages to their current locations. In Kabare for instance, war IDPs came from Karhanda, Kabulungu, Cahoboka or Kabushwa, villages located a few kilometers away from Kavumu and Katana. The latter are two big cities in North Kabare where IDPs mostly relocated to. Many of them fled war, atrocities and lootings from the Forces Démocratiques pour la libération du Rwanda (FDLR). As for Uvira territory, Kamonyi was prominently the place of origin for many war IDPs in Katogota (village where IDPs relocated to).
Sources of health information
Displaced and non-displaced people have many sources of health information. The most common are friends and neighbors, the media (radio), and biomedical sources (nurses, doctors, health centers). These are followed by community meetings, family members, community relays and places of worship. Only a few sources of health information are significantly different between IDPs and non-IDPs (Figure 3). The non-displaced made greater use of community meetings (13% versus 7%, p = 0.0007) and places of worship (21% versus 15%, p = 0.0773) as sources of information about their health problems. Displaced people were more likely to obtain health information from family members and relatives (21% versus 13%, p = 0.0145), which may also be an explanation for why they would more easily orient themselves toward TCAM providers who are known within the community but rarely advertise publicly. The awareness-raising campaigns provided on the radio and television are, as the data shows, likely to be of limited efficiency among IDPs given their low usage of such media for health information purposes.
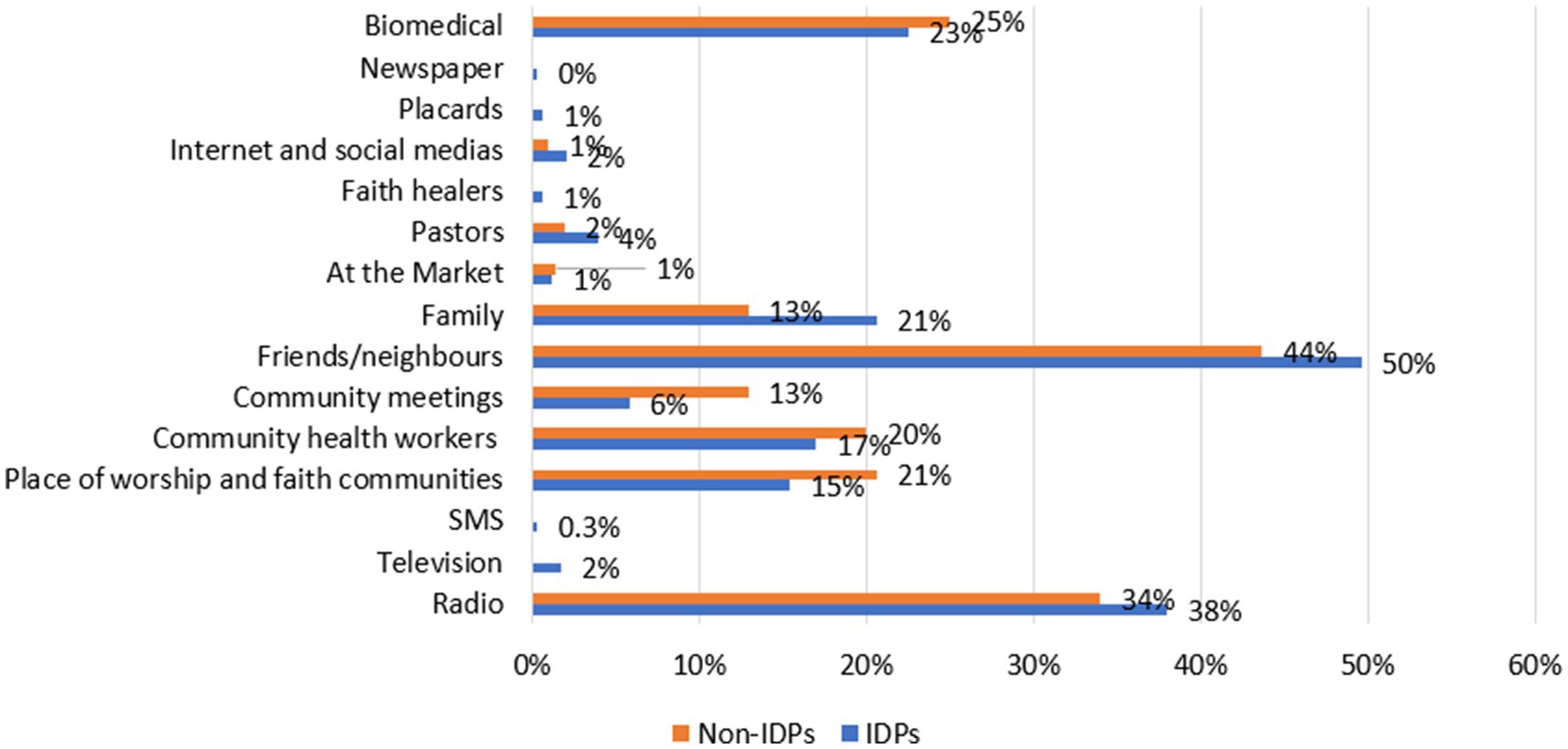
Figure 3. Sources of health information among IDPs and non IDPs.
Confidence level
In most cases, traditional healers, namely fetishists, phytotherapists, herbalists, and exorcists are reputed to have relatively cheaper services than modern health structures. Table 4 shows the levels of trust that IDPs and non-IDPs place in them to deal with their health problems in the territories of Kabare and Uvira.
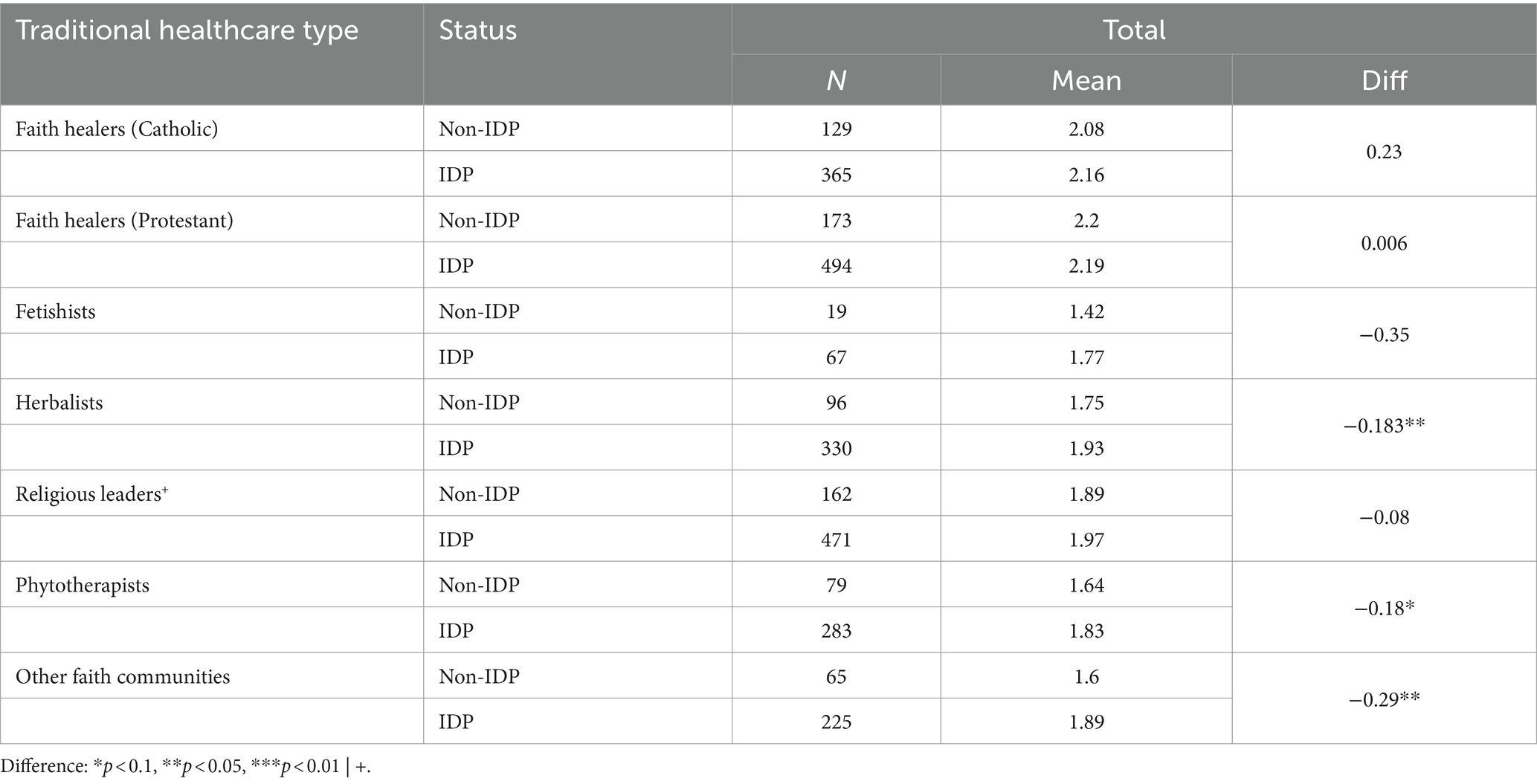
Table 4. Confidence level toward traditional healthcare providers (from 1 no trust at all, to 3 very high trust).
The Protestant and Catholic community organizations seem to be more trusted than the rest of the TCAM providers by both displaced and non-displaced people in finding solutions to their health problems. At the other extremity of the spectrum, the fetishists benefit from a low level of trust. These findings are, however, not different for IDPs and non-IDPs. The main difference, as the table shows is in the increased confidence IDPs have in herbalists, physiotherapists, and other faith communities outside the Catholic and Protestant communities.
Characterizing TCAM providers
We now turn to the data we collected among traditional healthcare providers to try to better understand how IDPs relate to traditional healers. We start by describing the profiles of the healers and their areas of activity. As the introduction sections of this paper pointed out already, TCAM providers refer to a wide range of practices. Categorizations are always hazardous, but in our 24 interviews, 17 people described their practice as close to what the official classification would call herbalists, 3 as ritualists, 3 as exorcists and 1 is best qualified as “mixed” –a category of TCAM providers who, by their practices, can be considered to be herbalists but who also engage in seances similar to those of the fetishists (ritualists) or faith healers (exorcists) found in religious communities (Protestants in particular). Men overwhelmingly dominate (18 of our respondents), and the average TCAM provider was aged 48 (standard deviation: 11.25) and had family responsibilities. On average, they have been in the profession for 22.5 years (standard deviation: 10.97), suggesting that TCAM providers start early.
TCAM services
TCAM providers (ritualists, herbalists, and exorcists) offer a range of services to those who consult them (whether displaced or not). From a simple abscess to conditions of so-called supernatural origin, the healing services offered by these care providers vary greatly depending on their specialty and the profile of the person seeking help.
Physical and mental healthcare
Services offered by TCAM providers include care for a wide range of physical and mental conditions, sometimes depending on the patient’s profile such as age, sex, or profession. For women, for example, there are a lot of services offered for gynecological conditions such as infertility, painful periods, or care for contraceptive measures. For children, the focus is typically on common ailments such as malaria, bronchitis, epilepsy (although also seen in adults), and certain pediatric illnesses. Men, on the other hand, seek treatment for sexual impotence, prostate problems, and tuberculosis. For most categories and different ages generally, we record healing services for mental health conditions. These include for instance psychopathology, mental disorders as well as nerve problems, and headaches. TCAM services are also requested for chronic illnesses (diabetes, high blood pressure, hemorrhoids, stomachache), toxicological complications (poison), orthopedic illnesses (fractures) and internal medicine conditions (rheumatism).
Exorcism
TCAM providers also offer exorcism services for victims of demonic possession –conditions that are more difficult to relate to those described and accepted by biomedicine. This is often the work of pastors, evangelists, servants of God, and even certain ritualists or fetishists. The latter practice exorcism, rituals or healing prayers for illnesses that they describe as having a supernatural origin. Exorcists from the Catholic and Protestant communities often work in prayer rooms or visit hospitals to pray for the sick. A pastor in Kavumu commented:
“…In terms of the illnesses we see most often, we have cases of demonic possession [with behavioral problems], people with problems linked to family curses [following magico-religious practices within their families]. In view of these problems, we hold deliverance sessions for them…".
Certain physical (such as premature death) and mental conditions are also associated with or interpreted as situations of demonic possession. In the absence of psychiatric facilities in the area, recourse is often made to traditional care providers, particularly ritualists (fetishists) or herbalists. This practice is very common in the area and is thought to be an integral part of a set of cultural practices with well-known social referents (Koya, 2016). A TCAM practitioner explains:
“Wars that make living conditions very difficult are at the root of many problems. Demons very well exist, and we see them. Some tribes, like the Bashi, have the Muhima [a spirit or demon] that never leaves them. We have a cultural practice whereby, to cure a person with this type of demon, the latter is given a girl from the same family to be his wife, and when the girl marries, another girl from the same family is sought to prevent premature death or illness among other family members. There are also hereditary diseases that need to be properly identified/diagnosed in the traditions. These diseases are transmitted from one generation to the next. Mulonge yenye ina ozesha ata ma moelle épinière (a disease that rots the spinal cord) comes from the bad faith of people with bad intentions. As fetishists, we break mizizi (amulets).”
Although culturally accepted, the role and use of traditional medicine also seem to be reinforced by the living conditions of the population, and those of displaced people in particular. The daily stress experienced by displaced people and the personality disorders they cause can be attributed to supernatural causes. In addition, diagnosis and treatment of hereditary and congenital diseases are sometimes beyond their means, given their poor living conditions, leading IDPs to turn to TCAM and its methods. Some of these illnesses are considered taboo and taken to fetishists. The latter is said to help counter the effects of certain enchantments or amulets, as well as curing certain supernatural ailments such as the “muhima” and “mulonge.” However, in the absence of suitable testing equipment, it is only the persistence of the disease that can enlighten healthcare providers as to the true origin of the disease and whether it requires biomedical monitoring. An exorcist explains:
“We see people coming here with cases of malaria and high blood pressure, but we deal much more with cases of demonic possession because these are the problems for which people seek us out. As for mental illness, we have three types of problems. There are those who are disappointed by life's problems (too much stress in life, either husband, wife or financial problems). Others are victims of demonic possession (paranormal activities). They may even undress in public. The third category is those with mental health problems linked to heredity (this third category often resists prayer).”
This explanation shows not only how difficult diagnosis of specific diseases can be in their early stages but also emphasizes the assumption that TCAM providers have earned a reputation of being “jack-of-all-trades.” Even for cases that would require biomedical treatment, some may retain patients in their prayer rooms or facilities. This usually ends up aggravating their situation or revealing their inability to help patients, particularly in the case of mental health conditions, malaria or anemia. Such an attitude has often tarnished the reputation of TCAM practitioners and aroused distrust among host communities, including IDPs. However, they are recognized as having a certain effectiveness in overcoming certain physical health conditions such as “mulonge,” which is widely recognized as being of supernatural origin in the area.
Illnesses of “supernatural” origin: Mulonge
Testimonies gathered from displaced people show that, although some traditional healers can offer healing services for illnesses that can easily be treated in a hospital, their specialty remains the treatment of poisons and Mulonge. Mulonge, or Buruli ulcer, is one of the neglected tropical diseases reported in certain countries in sub-Saharan Africa, South America and the Western Pacific. In the DRC, it was first reported in the 1950s and is known by different names depending on the region. In the west of the country, the disease is better known as “mbasu” or “plague due to a bad spell.” Mulonge or Mbasu is a disease characterized by skin lesions resembling a nodule, papule, plaque or oedema. These lesions can progress to ulcerations of various sizes and shapes, which can even reach the bone (Kibadi et al., 2009). If not treated effectively, the disease could lead to the death of the patient or the amputation of certain limbs.
The causes of Buruli ulcers are still the subject of much debate between the scientific community on the one hand and the lay community in South Kivu on the other hand. People do not understand why a person would be affected and not those around them, despite frequent contact (including the environment in which they live with their loved ones; Nendaz and Sordet, 2015). Scientific studies carried out on the disease show, however, that the main cause of the illness is linked to contact with the microbial agent transmitted by drinking or coming into contact with non-drinking water: Mycobacterium ulcerans (Kibadi et al., 2009; Ackumey et al., 2012).
The ineffectiveness of biomedical treatment in the advanced stages, caused by delayed care and negligence on the part of the patient (or those around them), as well as the mortality associated with this disease, reinforces its mystical nature. The literature therefore shows that many people with the disease in other African countries would be more inclined to resort to traditional treatment. Studies by Webb et al. (2009) showed that in Ghana, 71% of Buruli ulcer sufferers resorted to traditional treatment, but much more for reasons of proximity. Other factors could be a lack of empathy on the part of biomedical staff or delays in finding appropriate treatments (Ackumey et al., 2012).
Mulonge occupies a central part in narratives on accessing TCAM providers in South Kivu. It is also the preserve of certain fetishists. One of the internally displaced persons from Kabare explains:
“There are illnesses that require treatment by traditional healers, such as Mulonge, and even poisons can only be treated by herbalists. I remember once asking for water to drink. However, just as I felt the water was cold in my mouth, I felt it warm in my stomach. So I rushed to hospital. A friend had taken me to an herbalist who had given me some medicine that I used for six months. When I took these medicines from herbalists, I vomited if I took cold water and had diarrhea if I took hot water.”
Cases of poisoning and mulonge are very common in South Kivu, both in urban and rural areas. The suspected motives behind them are said to be varied. They may be economic (sudden retirement, dismissal at work followed by promotion in favor of someone else), land-related (land disputes), or motivated by pure jealousy (also known as the evil eye) of people who are not happy to see others prosper. There are many ways of poisoning people or throwing mulonge at them. In the case of poison, this can be done by the most mundane means possible, such as physical contact like shaking hands, drinking water, food or other beverages. As for mulonge, often-used means are contacts with clothes, locks, chairs or tables in offices on which its microbial agent had been deposited.
Amulets and protection
Finally, less related to the main healthcare topic of this article, those who are not ill also seek the services of TCMA providers. Some service providers such as fetishists would even offer amulets to improve their luck in their profession such as drivers or fishermen. As one fetishist in Uvira put it:
“I also give amulets to drivers and motorcyclists so that their work is too profitable. I also give them to fishermen so that they have lots of fish.”
It is important to point out that in the context of Bukavu and its outskirts, fetishists (who are included under the ritualist category) are perceived as multifaceted sorcerers whose remit go well beyond what is typically described as healthcare: the fetishes they use can also be used to protect against evil spells, to bring good luck, or even to punish or take the lives of certain people (criminals) (Koya, 2016).
TCAM healthcare access costs
The services offered by TCAM providers are not always free. There are different forms of remuneration, depending on whether the services are provided by fetishists, herbalists, or exorcists. We argue that while IDPs struggle to pay for biomedical as well as traditional healthcare. However, the more flexible modalities of payment that are found among traditional healers make them a potentially attractive option. IDPs are sometimes forced to work as farm laborers in the fields to earn 2,000 Congolese francs (less than USD $1 a day) a day to cater for their families and cover other expenditures.
When a person seeking care requests services from traditional healers or fetishists, they are usually first asked to offer either a goat, a chicken or a sum of money (ranging from USD $2.08 to USD $50) depending on the health condition they are experiencing. This process is known as “Kiingia pori” or “Kingiya pori.” According to the practice of traditional healers and fetishists in particular, this sum is a form of deposit that gives them the funds to go fetch in the forest (pori in Swahili) ingredients to be used in their treatment. It can also be used to pay those who will collect plant leaves on their behalf. In certain circumstances, the “Kiingia pori” can also be seen as a donation made by the patient or their relatives to appease the spirits and open the door to healing, blessings, or protection from the ancestors (Koya, 2016). In this case, the donation, either in kind or in cash, is the sole consideration for the services received. Providers may receive an envelope of money or a goat as a token of appreciation, or a thank you from the patient.
This type of payment is not the only approach found in our research. Some traditional healers charge (mostly) at the end of the treatment, and the bill can be as much as USD $100. Importantly, the bill depends on the illness treated, but also the patient’s socio-economic profile or the illness. Practices vary widely, but in some cases, in a fashion similar to biomedical healthcare, fees are clearly set in advance and publicly displayed. For instance, a traditional practitioner in Kabare had advertised:
• Migraine, chronic headache USD $10;
• Stomach: USD $15;
• Fractures: USD $30,
• External hemorrhoid: USD $30
• Mulonge: from USD $150 to USD $300
• Malaria: from USD $25 to USD $41.
We could not find any strong evidence that IDPs and non IDPs are treated differently, but the relative flexibility around payment suggests that specific vulnerabilities are taken into account when charging the patient.
Exorcists work with a different approach. Officially, their services are free as they act on “divine instructions.” In practice, though, “divine grace” seems to require a little nudge and a donation for exorcists to start working. Their attitude is one of “wait-and-see” what the patient actually has to offer (this is generally in keeping with the economic functioning of many churches in the DRC). This applies to all categories of the population, including IDPs. Among exorcists, some openly recognize that this approach to payment constitutes a barrier for IDPs to access their services. As one of them put it: “The problem I have with IDPs is their poverty. We can pray for them, but they do not have enough money to give us even a glass of milk.”
Other traditional healthcare providers share the same point of view. Interviews revealed that one of the major difficulties they face arises from IDP patients. Many of those who seek treatment from traditional healers find it difficult to pay their bills. The poverty in which many IDPs find themselves means that some ask to be treated free of charge. Others can start the treatment and then, once their condition begins to improve, disappear without paying their bills. We also have cases where IDP patients are fed by their TCAM providers in order to receive their treatment. An herbalist in Kabare explains:
“For IDPs, most of the time when they arrive, they don't even have the strength to stand up. What's more, they don't even have enough to eat. So there are medicines that we can't even give them in this state. So first we have to see how to find them something to eat and then treat them, or simply reduce the dose given to patients to prevent the treatment from causing harmful effects, which will also delay their recovery. Afterwards, as the treatment progresses, and especially when they notice that they are beginning to heal, they disappear before benefiting from the final dose. In particular, we have a case of a patient who was brought here on Tipoye after being poisoned. We took care of him. Now he's recovered, but he hasn't gone home yet. He now lives here with us. He leaves in the morning to go to work and comes back in the evening.”
The way TCAM providers offer their services to their patients, and IDPs in particular, appears somewhat unusual compared with current biomedical practice. While in modern health structures, patients benefit from regular follow-up in sanitary facilities, this is not often the case for some traditional healthcare providers. Because of the lack of adequate sanitary facilities, the patient becomes intertwined with the healthcare provider’s family. Some care providers even start to fetch food for patients to help them take their medication. We see patients who, once cured, enjoy the hospitality of their hosts, and become adopted by their families, using this environment to carry out their normal activities. The lack of financial resources is the most plausible cause of this situation (and explains why IDPs disappear before the end of treatment as they cannot afford it), but so is the lack of a purely professional framework on the part of TCAM providers.
On the supply side, TCAM providers report serious financial problems and tax red tape. Many of the treatments used by TCAM providers (herbalists, phytotherapists, but also ritualists and exorcists) come from plant extracts. Preserving and processing these extracts requires appropriate equipment, which they struggle to afford. This problem also affects their working conditions, such as the confinement of patients, who are sometimes obliged to live with their family carers. Another problem faced by TCAM providers is institutional: official and de facto taxes and tax harassment by government officials hamper their activities. As one of them put it: “We receive a lot of taxes and receipts from the state, and this is not proportional to our income. Just imagine, we can have a daily income of 5000FC [USD $2] but they will give you taxes of USD $250 per month.”
The main sources of income for TCAM providers are their clients, including displaced persons. Given the flexibility of their pricing system, the low level of income of their patients, and the de facto taxation, the income of traditional healthcare providers remains low. As the plant extracts they use become increasingly scarce due to population growth and deforestation, they are forced to turn to pygmies living in the vicinity of the Kahuzi Biega National Park or to other suppliers living in areas that regularly access the forest. Additional financial resources are then needed to pay their suppliers for the plant extracts to be used in their treatment. However, their patients, who sometimes lack the means, would not provide them with enough money to cover these expenses.
In the course of their work, many TCAM providers report being victims of jealousy on the part of their colleagues. Jealous of their performance, progress or clientele, rivals use amulets or other means to curse them. A traditional care provider in Uvira says:
“Some people even come and put charms on my house so that patients can no longer come to me for help. To do this, I also put grigris in my house to protect myself, because I remember one day, I was treating a patient and a snake appeared to intimidate me and interrupt me, fortunately, I caught it and cut off its head too.”
Some TCAM providers use negative criticism to try to destroy their rivals’ access to clientele and win the sympathy of customers. As for formal healthcare providers, they have little contact with traditional healers and other TCAM providers. In this separation, there is often enmity between them, seeing each other as “mbanda” or rivals. An exorcist from Kabare recalls:
“We are also victims of certain stereotypes on the part of people who are not in the same profession as us. This is particularly true of front-line healthcare providers. Often when we fall ill and go to the health facilities, they tend to tell us: “You are exorcists and intercessors. May the prayers that you are used to saying help you”.
This rivalry between traditional and modern medical care providers stems from several deaths that have already occurred either in prayer rooms or in their health facilities. Some illnesses that are not treated in time can get aggravated by treatments based on so-called “speculative” diagnoses by traditional medical care providers. Even among IDPs, recourse to traditional healthcare providers is not always unanimous, for various reasons mentioned above or simply because of a lack of trust.
Concluding remarks
This study addresses the role of traditional healthcare providers in the provision of health services to displaced and non-displaced people in Kabare and Uvira territories. In their search for healthcare, displaced and non-displaced people turn to TCMA providers for various healing services. This strengthens the emphasis on this category of healthcare providers whose services are reportedly cheap and recurrently requested. As part of the healthcare delivery system, traditional healers constitute an entry point for IPDs’ integration in host communities as social resources that can be mobilized in case of health problems. Thus, focusing only on the use of TCAM among IDPs would not tell the whole story about both supply and demand of traditional healthcare services in South Kivu. From this research, it is important to take away that TCAM providers are not monolithic but fall under multiple subcategories. Surveys carried out among this population in South Kivu reveal several types of traditional healthcare providers, including phytotherapists, herbalists, ritualists (including fetishists), and exorcists from different religious communities (Catholic, Protestant, Muslim, Church of the Faith, Neno, ministers of religion); including a mixed group of healthcare providers whose practices touch on all three of the above categories.
Furthermore, traditional healthcare providers are not universally turned to or trusted to adequately treat people in South Kivu’s needs. Therefore, before advocating for the integration of traditional healers into larger healthcare systems, it requires a comprehensive understanding of the role these actors play. In this sense, this article heeds Kadetz (2013) caution against the universal approach to healthcare integration of TCAM. He argues that the WHO’s valorization of Mao Zedong’s integration of traditional Chinese medicine into modern healthcare obscures the often violent politics of the Chinese integration process. Moreover, attempts in places such as the Philippines, where healthcare is decentralized and privatized as in DRC, the integration of TCAM has led to unintended consequences such as the increase of healthcare costs. Important lessons can be learned from this research:
There is a marked difference between the normative representation of integration as a purposeful intervention of the biomedical State apparatus and the practice of integration that occurs organically through practitioner application; through the natural syncretism of practices shaped by sociocultural factors over time; and most of all through the patient’s own plural and integrated use of their local practices and practitioners (Kadetz, 2013, p. 55).
Conflict and displacement complicate these processes further. As the results show, the use of these different care providers is much more pronounced among displaced people than among the non-displaced. More than 60 % of the displaced people questioned said that they had used at least one traditional healthcare provider. Analysis of the social connections established showed that phytotherapists, herbalists and exorcists were more frequented by IDPs than by non-displaced people. The main reason for using their services was the flexibility of their method of payment. Other reasons include where people turn to as sources of healthcare information and the level of trust some IDPs put in traditional healthcare providers, especially exorcists. Despite the presence of formal sources of health information, namely biomedical and radio, statistical test results showed that IDPs would more rely on family relatives for their health problems. Traditional medicine plays an important role in the treatment of certain illnesses in South Kivu. The government has made several efforts to integrate traditional medicine into the health system, but there is still a long way to go. This study highlights a variety of services provided by TCAM providers and how they are perceived. The services provided by traditional care providers are numerous and varied. There is also a high variance in trust people in the area have that they will receive the desired treatment through TCAM. The level of trust placed in certain traditional care providers remains relatively low, particularly for fetishists, except Uvira who have relatively high confidence in this group of care providers. Only phytotherapists, herbalists, and exorcists (including both religious leaders and religious communities) enjoy a relatively high level of trust among both displaced and non-displaced people. Despite these variances in trust and confidence in traditional treatment, certain conditions of Buruli ulcer, known in DRC as the supernaturally caused “mulonge,” are locally perceived to be effectively treated by TCAM.
Due to the high level of demand for traditional treatment for mulonge, this specific condition could form a bridge for collaboration between traditional and modern medicine in South Kivu, especially as many providers do not have adequate equipment for accurate and appropriate diagnoses. In the case of Buruli ulcer, it is recognized that once the causative agent has been eradicated, the wounds it leaves behind can easily be treated in modern medical facilities. As for poison, working together would make it possible to distinguish real cases of poisoning from cases of stomach ulcers. It is therefore in the interests of the government and political decision-makers to facilitate this collaboration by putting in place a rigorous system for monitoring and registering traditional medicine providers, to avoid cases of abuse. Secondly, the state and health systems should build on the trust that certain types of providers, such as phytotherapists, herbalists, and faith healers have to find additional potential convergences where partnerships can be built. Another example may be the prevention, treatment, and seeking of justice for SGBV that may be disclosed to these sources.
Structures for supervising and training traditional medicine providers in urban and rural areas would be the second step toward their integration into the national health system, where traditional and modern practitioners would work in close collaboration. These will be followed by the establishment of traditional medicine centers specializing in the treatment of supernatural diseases such as Buruli ulcers and cases of poisoning. However, understanding the economic incentives of TCAM providers and IDP/non-IDP patients is crucial. The formalization and institutionalization of traditional providers may push out those providers who do not have the means to be integrated and may change the flexible payment structures that have allowed TCAM to flourish in South Kivu. Any attempts to integrate traditional healthcare providers into the formal healthcare systems of IDP situations holistically and equitably must first consult a wide range of local stakeholders including TCAM providers, IDPs, and non-IDPs as we have done in this research.
Data availability statement
The raw data supporting the conclusions of this article will be made available without any reservation.
Ethics statement
The studies involving humans were approved by Ethics Committees of the School of Social and Political Science at the University of Edinburgh and the Université Evangélique en Afrique. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. AK: Conceptualization, Formal analysis, Investigation, Methodology, Writing – review & editing. JB: Conceptualization, Investigation, Methodology, Writing – review & editing. EK: Conceptualization, Data curation, Formal analysis, Investigation, Software, Writing – review & editing. J-BF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing. GF: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – review & editing. DM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – review & editing. CB: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was entirely funded by the Global Challenges Research Fund of the UKRI. The funder did not take any role in the design, analysis or writing of the paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^We recognize there is debate about what labels these healthcare providers should be referred to, including informal, indigenous, or traditional healers. In this article, we refer interchangeably to TCAM and traditional. We use TCAM because much of the academic literature is this or something similar. Traditional providers are also used because this was the language most commonly used by informants and the DRC government.
2. ^While this article addresses the integration and care of IDPs, there are separate debates in the global health field about the integration in the health system of actors considered outside of biomedical healthcare systems.
3. ^This ministerial decree concerns the organization of the practice of traditional medicine. It represents the Congolese government’s commitment to improving healthcare coverage through the development of traditional medicine and the harmonization of partnerships between the systems of modern conventional medicine and traditional medicine while guaranteeing intellectual property rights and the protection of indigenous knowledge.
References
Ackumey, M. M., Gyapong, M., Pappoe, M., Maclean, C. K., and Weiss, M. G. (2012). Socio- cultural determinants of timely and delayed treatment of Buruli ulcer: implications for disease control. Infect. Dis. Poverty 1, 1–13. doi: 10.1186/2049-9957-1-6
Ager, A., and Strang, A. (2008). Understanding integration: a conceptual framework. J. Refug. Stud. 21, 166–191. doi: 10.1093/jrs/fen016
Akol, A., Moland, K. M., Babirye, J. N., and Engebretsen, I. M. S. (2018). “We are like co-wives”: traditional healers’ views on collaborating with the formal child and adolescent mental health system in Uganda. BMC Health Serv. Res. 18:258. doi: 10.1186/s12913-018-3063-4
Altare, C., Malembaka, E. B., Tosha, M., Hook, C., Ba, H., Bikoro, S. M., et al. (2020). Health services for women, children and adolescents in conflict affected settings: experience from north and south Kivu, Democratic Republic of Congo. Confl. Heal. 14, 31–19. doi: 10.1186/s13031-020-00265-1
Ampomah, I. G., Malau-Aduli, B., Malaud-Aduli, A. E. O., and Emeto, T. I. (2020). Effectiveness of Integrated Health Systems in Africa: A Systematic Review. Medicina. 56:271. doi: 10.3390/medicina56060271
Bapolisi, W. A., Karemere, H., Ndogozi, F., Cikomola, A., Kasongo, G., Ntambwe, A., et al. (2021). First recourse for care-seeking and associated factors among rural populations in the eastern Democratic Republic of the Congo. BMC Public Health 21, 1367–1313. doi: 10.1186/s12889-021-11313-7
Beyani, C. (2013). Under the radar: internally displaced persons in non-camp settings. (issue October).
Bile, A. S., Boeyink, C., Ali-Salad, M. A., Lowe, L., Mohamoud, S. A., Jama Mahmud, A., et al. (2023). Rethinking (local) integration: domains of integration and their durability in Kismayo and Garowe, Somalia. Front. hum. dyn. 5:1283098. doi: 10.3389/fhumd.2023.1283098
Boeyink, C., Ali-Salad, M. A., Baruti, E. W., Bile, A. S., Falisse, J.-B., Kazamwali, L. M., et al. (2022). Pathways to care: IDPs seeking health support and justice for sexual and gender-based violence through social connections in Garowe and Kismayo, Somalia and south Kivu, DRC. J. Migrat. Health 6:100129. doi: 10.1016/j.jmh.2022.100129
Boum, Y., Kwedi-Nolna, S., Haberer, J. E., and Leke, R. R. G. (2021). Traditional healers to improve access to quality health care in Africa. Lancet Glob. Health 9, e1487–e1488. doi: 10.1016/S2214-109X(21)00438-1
Falisse, J.-B., Masino, S., and Ngenzebuhoro, R. (2018). Indigenous medicine and biomedical health care in fragile settings: insights from Burundi. Health Policy Plan. 33, 483–493. doi: 10.1093/heapol/czy002
Gerstl, S., Sauter, J., Kasanda, J., and Kinzelbach, A. (2013). Who can afford health care? Evaluating the socio-economic conditions and the ability to contribute to health Care in a Post-Conflict Area in DR Congo. PLoS One 8, e77382–e77389. doi: 10.1371/journal.pone.0077382
Grant, C. (2018). Ebola preparedness and traditional healers in South Sudan. K4D Helpdesk Report: UK Department for International Development.
Ivlevs, A. (2019). Are IDPs satisfied with the quality of public health and education services they receive? In Global Report on Internal Displacement.
Jacobs, C., Assumani, I., Katembera, R. S., Kubiha, S. L., Kyamusugulwa, P. M., and Mugenzi, J. R. (2020). Figurations of displacement in the DRC (TRAFIG Working Paper.
James, P. B., Wardle, J., Steel, A., and Adams, J. (2018). Traditional, complementary and alternative medicine use in sub-Saharan Africa: a systematic review. BMJ Glob. Health 3:e000895. doi: 10.1136/bmjgh-2018-000895
Kadetz, P. (2013). Challenging a universal approach to health care integration: China, Cuba, and the Philippines. Eur. J. Integr. Med. 5, 54–61. doi: 10.1016/j.eujim.2012.11.006
Kibadi, K., Boelaert, M., Kayinua, M., Minuku, J. B., Muyembe-Tamfum, J. J., Portaels, F., et al. (2009). Therapeutic itineraries of patients with ulcerated forms of Mycobacterium ulcerans (Buruli ulcer) disease in a rural health zone in the democratic republic of Congo. Trop. Med. Int. Health 14, 1110–1116. doi: 10.1111/j.1365-3156.2009.02324.x
Koya, P. M. N. (2016). Sociocultural aspects of mental disorders among Shi people past and present: what effective management? The Other 17, 110–118. doi: 10.3917/lautr.049.0110
Krah, E., De Kruijf, J., and Ragno, L. (2018). Integrating traditional healers into the health care system: challenges and opportunities in rural northern Ghana. J. Community Health 43, 157–163. doi: 10.1007/s10900-017-0398-4
Ministère de la Santé (2021). Rapport sur les comptes de la santé Available at: https://sante.gouv.cd/content/uploads/RAPPORT_CNS_2020_86e645c64a.pdf
Mucchielli, A. (1996). Dictionnaire des méthodes qualitatives en sciences humaines et sociales. Paris: éditions Armand Collin.
Mutombo, C. S., Bakari, S. A., Ntabaza, V. N., Nachtergael, A., Lumbu, J. B. S., Duez, P., et al. (2022). Perceptions and use of traditional African medicine in Lubumbashi, haut-Katanga province (DR Congo): a cross-sectional study. PLoS One 17:e0276325. doi: 10.1371/journal.pone.0276325
Mwaka, A. D., Achan, J., and Orach, C. G. (2023). Traditional health practices: a qualitative inquiry among traditional health practitioners in northern Uganda on becoming a healer, perceived causes of illnesses, and diagnostic approaches. PLoS One 18:e0282491. doi: 10.1371/journal.pone.0282491
Ndetei, D. M. (2007). Traditional healers in East Africa. Int. J. Psychiatry. 4, 85–86. doi: 10.1192/s1749367600005233
Nendaz, L., and Sordet, C. (2015). Buruli ulcer: Elements determining the therapeutic itinerary of affected persons in Africa. Haute Ecole de santé Genève.
Ojeleke, O., Groot, W., and Pavlova, M. (2022). Care delivery among refugees and internally displaced persons affected by complex emergencies: a systematic review of the literature. J. Public Health 30, 747–762. doi: 10.1007/s10389-020-01343-7
Phillimore, J., and Goodson, L. (2008). Making a place in the global city: The relevance of indicators of integration. J. Refug. Stud. 21, 305–325. doi: 10.1093/jrs/fen025
Roberts, B., Ekezie, W., Jobanputra, K., Smith, J., Ellithy, S., Cantor, D., et al. (2022). Analysis of health overseas development aid for internally displaced persons in low-and middle-income countries. J. Migrat. Health 5:100090. doi: 10.1016/j.jmh.2022.100090
Shalukoma, C., Duez, P., Bigirimana, J., Bogaert, J., Stévigny, C., Pongombo, C., et al. (2016). Characterization of traditional healers in the mountain forest region of Kahuzi-Biega, south-Kivu, DR Congo. Base 20, 25–41. doi: 10.25518/1780-4507.12616
Spencer, S., and Charsley, K. (2021). Reframing ‘integration’: acknowledging and addressing five core critiques. Comparative Migration Studies, 9. doi: 10.1186/s40878-021-00226-4
Strang, A. B., and O’Brien, O. (2017). Who Can I Turn To? Mapping social connections, trust and problem-solving among conflict-affected populations. Available at: https://jliflc.com/wp-content/uploads/2017/07/2017-QMU-Tearfund-Who-Can-I-Turn-To-En.pdf
Strang, A. B., and Quinn, N. (2021). Integration or Isolation? Refugees’ Social Connections and Wellbeing. J. Refug. Stud. 34, 328–353. doi: 10.1093/jrs/fez040
Tabi, M. M., Powell, M., and Hodnicki, D. (2006). Use of traditional healers and modern medicine in Ghana. Int. Nurs. Rev. 53, 52–58. doi: 10.1111/j.1466-7657.2006.00444.x
Uche, E. O. (2017). European journal of social sciences studies factors affecting health seeking behaviour among rural dwellers in Nigeria and its implication on. Euro. J. Soc. Sci. Stud. 2, 74–86. doi: 10.5281/zenodo.400695
Webb, B. J., Hauck, F. R., Houp, E., and Portaels, F. (2009). Buruli ulcer in West Africa: strategies for early detection and treatment in the antibiotic era. East African Journal of Public Health, 6, 144–147. doi: 10.4314/eajph.v6i2.51744
Keywords: social connections, integration, indigenous healers, spiritual healers, DRC, IDPs
Citation: Kazamwali M, Kisanga A, Balegamire JB, Kaningini E, Falisse J-B, Furaha G, Mapendo DM and Boeyink C (2024) Traditional, complementary, and alternative medicine and the provision of health care to internally displaced persons in South Kivu, Democratic Republic of the Congo. Front. Hum. Dyn. 6:1289169. doi: 10.3389/fhumd.2024.1289169
Edited by:
Jannie Hugo, University of Pretoria, South AfricaReviewed by:
Thierry Ngoyi, University of Pretoria, South AfricaProsper Lutala, Kamuzu University of Health Sciences, Malawi
Copyright © 2024 Kazamwali, Kisanga, Balegamire, Kaningini, Falisse, Furaha, Mapendo and Boeyink. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clayton Boeyink, Y2JvZXlpbmtAZWQuYWMudWs=