 Yafza Reyes Muñoz1*
Yafza Reyes Muñoz1* Vania Reyes Muñoz2*
Vania Reyes Muñoz2*- 1Escuela de Fonoaudiología, Universidad Santo Tomás, Sede Talca, Chile
- 2Programa de Doctorado en Arquitectura y Estudios Urbanos, Pontificia Universidad Católica de Chile, Santiago, Chile
Introduction: In the field of medical anthropology, particularly from the practices of medical care in a situated context, the text discusses how state care services under the “National Child Health Programme” implemented by nursing professionals in Chile transmit values and expectations that could be transformed into devices of acceptance to the social body for migrant mothers of African descent who come with their children to health centres.
Methods: The Methodology employed in this study was devised through a case study in the commune of Talca, within the Maule region, utilizing semi-structured interviews with nurses who work within the Programme, as well as open interviews and thematic workshops with migrant women users of the Programme.
Results: The results point to the valuation of the programme by the women, who identify it as an instance of providing and receiving care for their children; they also recognise that they are judged by their caregivers for not “correctly” following the instructions given to them with their children living in Chile or for exercising transnational maternity. On the other hand, nursing professionals revealed racial and class prejudices about women of African descent, especially Haitian women.
Discussion: It is suggested that this programme, recognized regionally as an effective assistance and care policy in the fight against infant mortality and morbidity, becomes an acculturation device for migrant mothers and their children born in Chile. It is expected that both mothers and children adhere to the program’s guidelines, resulting in similar behaviours and attitudes as those of Chilean mothers. This generates few instances of learning and appreciation of the native cultures of the new Chilean infants and reveals that categories of differences such as ethno-racial, gender, and migratory status are articulated in the nurses’ health practices, emphasising the mandate to follow the instructions of migrant mothers and their children.
1 Introduction
In Chile, the conceptualization of health within modern state development projects involved the transition from an activity carried out by religious entities and philanthropists to a public institutional framework aiming for uniformity and mass provision of healthcare services (Álvarez Díaz and Aguirre Munizaga, 2021). The significance of health and its access as a public policy materialized with the establishment of the National Health Service in 1952. In its early stages, the service operated through a national structure comprising Regional Health Zones, each overseen by a medical director, and an interconnected network of hospitals of varying complexity levels. Additionally, this structure included peripheral health centers (called consultorios) and rural health post1.
In the field of obstetrics, this meant shifting childbirth from home settings to hospitals and applying concepts and practices oriented toward the care of sick individuals, now directed toward birthing mothers and newborns (Castro, 2003). The social process of childbirth and postpartum, previously shared by family and close friends, came under the purview of medicine and its practitioners. Between 1962 and 1964, the National Fertility Regulation Policy was established, the Chilean Association for Family Protection (APROFA) was created, and the first Family Planning Policy focusing on women’s sexuality was enacted. (Álvarez Díaz and Aguirre Munizaga, 2021, p. 369) [Translate by authors].
In this context, various programs directed from the central level and implemented at the territorial level by the healthcare assistance network aimed to provide planned and coordinated health programs, specifically for population groups, such as: “healthy child check-ups, prenatal care, professional childbirth assistance, milk distribution and supplementary feeding programs for children, child and adult vaccination, rehabilitation, environmental sanitation” (Goic, 2015, p. 778) [Translate by authors].
Following the military dictatorship (1973–1989) and the return to democracy in 1990, the discourse of the state and public health professionals regarding health indicators emphasized the need to restore the image of a progressing state concerned about the well-being of children and committed to reducing the inequality exacerbated during the dictatorship. In this context, the “National Childhood Health Program” was established in 1991, which currently has the following general objectives:
Reduce mortality and morbidity among children younger than 10 years of age. Strengthen timely, efficient, continuous, decisive, and quality healthcare for boys and girls in the public health network. Contribute to improving the quality of life for the child population, regardless of their health and socioeconomic status. Promote healthy habits and reduce health risk factors in children younger than 10 years old, considering a life course approach. (Gobierno de Chile, 2013, p. 1) [Translate by authors].
After two decades of implementation, Chile exhibited unequivocal indicators of access to healthcare for the national population and its effectiveness, with the lowest rates of infant mortality (7.2 per 1,000 live births) and maternal mortality (18.5 per 100,000 live births) in Latin America. The public and private healthcare system achieves a 100% professional attendance rate for childbirth and high coverage of immunizations, outcomes attributed to the National Childhood Health Program, among other measures. “These indices reflect the strength of the public health sector, which serves 80% of the population, and the social significance of its healthcare concepts” (Goic, 2015, p. 771) [Translate by authors]. In other words, there is widespread recognition of the value of the program and the monitoring guidelines it incorporates for the care of children by the local population.
However, with the increase in international and cross-border migration in Chile over the last decade, new users have been incorporated into the public healthcare system, including migrant mothers and their Chilean-born children. The discourse of healthcare professionals has emphasized equality in the provision of healthcare services, including access and coverage of the Childhood Health Program, under the National Policy for the Health of International MINSAL, FONASA, and Superintendencia de Salud (2017).
Two important questions arise in this context. First, whether the State Childhood Health Program enjoys the same recognition among the migrant population. Second, whether the care practices toward children in Chile (regulated by the aforementioned state program) can unequivocally continue to be presented as the only valid way to manage the health of migrant mothers’ children, and, of course, the mothers themselves, particularly in terms of maternal processes, breastfeeding, and attachment practices.
In this regard, the text presents a critical approach from the perspectives of medical anthropology and acculturation, examining the normativity and homogenization of institutionalized care practices in maternal and child healthcare. It questions the imposition of a singular valid form of care (the Chilean way), which is not only controlled by healthcare personnel but must also be strictly adhered to “instructions” by migrant mothers. This adherence is observed as necessary for them to be considered valid and legitimate members of the destination society, i.e., to be recognized as valid and legitimate individuals within the context of the Chilean state and citizenship.
Text is structured into a section titled Background, where some reflections on medical anthropology, the objectives, and scope of the National Childhood Health Program are presented. Subsequently, it provides background information on Afro-Latin immigration in Chile, the violence experienced by pregnant migrant women, and the acculturation mechanisms. The Methodology section outlines the objectives of the research, the approach used, and certain characteristics of the participants. The Findings section describes the background information gathered through interviews with nurses and migrant women, organized according to the specific objectives of the research. In the Discussion section, the research findings are analyzed in light of the different specialized literature that underpins the theoretical framework of this investigation, namely, medical anthropology and acculturation. Finally, Conclusions propose some actions toward eradicating violence against migrant women in Chile, particularly in primary healthcare centers.
2 Background
2.1 Medical anthropology and critical reflexivity
The entry of social sciences into the realm of health and modern medicine is relatively recent. In its early stages in the mid-20th century, it primarily aimed to investigate how the social and environmental conditions in which a specific population lived influenced the emergence (or absence) of certain diseases. In other words, it sought explanations beyond the biological, taking into account the limitations of medical treatments offered at that time. Thus, “the recognition of social elements in the health-disease-care process has allowed understanding it as a historically, socially, and culturally determined process” (Díaz Bernal et al., 2015, p. 658) [Translation by authors], going beyond biological phenomena. It attempts to comprehend how beliefs, values, practices, and social structures influence the health and well-being of individuals and communities (Lock, 2000).
Therefore, medical anthropology complements perspectives from local cultures with studies in public health and epidemiology, aiming to comprehensively and diversely understand the health-disease process, as well as care and prevention. In this context, one of the main issues addressed by medical anthropology in the applied field is the existence of sociocultural differences or distances between those managing health-related activities and the health-disease-care process and those benefiting from them (Díaz Bernal et al., 2015). This includes actions that alter practices and cultural behaviors specific to certain communities, as well as differences and asymmetries in the interaction between healthcare personnel and the user population of various health centers. Therefore, applied medical anthropology critically focuses on challenging the universality and ahistoricity inherent in the biomedical model. This model homogenizes subjects (always referred to as “patients”), prioritizes biological determinism over social and structural factors, and offers unilinear explanations of disease and healing processes.
Medical anthropology places particular emphasis on the social determinants of health, recognizing that factors such as class, gender, ethnicity, and access to resources influence health and healthcare. Within this framework, the maternity of migrant women involves complexities related to access to reproductive healthcare (Inhorn, 2007), cultural and social pressures, and childbirth, motherhood, and breastfeeding practices in both the countries of origin and destination. Therefore, a critical approach from medical anthropology entails not forgetting women’s agency in the process (Van Hollen, 2003), recognizing the constraints they face in a medicalized and non-native context (Sadler Spencer, 2004, 2016), where dehumanizing, acculturating, and hegemonic power dynamics are formed.
In this context, a critical examination of the National Childhood Health Program is necessary based on two arguments. First, the program promotes a societal mandate of exclusive motherhood in women, viewing them as the sole responsible caregivers, lacking knowledge on the matter. As Caro (2009, p. 34) notes: “The type of woman produced by institutional discourse is the woman-mother, compelled to learn how to ‘properly’ raise her children (which hides the assumption that her prior knowledge is inadequate or non-existent) [Translation by authors].” Second, for migrant Afro-descendant women, this mandate and its underlying notions of inadequacy and responsibility become palpable in relation to the “instructions” for caregiving and judgments on their transnational motherhood. In other words, it also posits a standardization of the idea of a singular appropriate form of care: the national one, to which migrant mothers must adhere.
2.2 National Children’s Health Program: between protection and control
Since 1991, following the restoration of the democratic political system, Chile has progressed in global indicators across social, cultural, political, economic, and health domains. Changes in the population’s epidemiological profile over the past decades have necessitated adjustments in central-level public policies and their territorial deployment throughout the country. Health programs have incorporated modifications into how childhood is perceived and embraced within healthcare centers, yet they continue to operate under a unitary state logic that assumes population uniformity in demands and needs. Discursively, it is noted that:
Promoting optimal early childhood development has become a priority at both international and national levels, recognized as one of the most influential social determinants of health. Concurrently with advances in scientific knowledge, in 1990, Chile ratified the Convention on the Rights of the Child, adopted by the United Nations General Assembly in 1989. This convention promotes four fundamental principles: non-discrimination, the safeguarding of the child’s best interests, their survival and development, protection, and their participation in decisions that affect them. Since then, there has been progressive work to ensure these rights in the various spaces that children occupy in the community. However, despite the achievements, significant inequality persists, significantly impacting health indicators and the quality of life for children. [Translation by authors].
Moreover, it is acknowledged that there is a phenomenon of child poverty in the country, meaning that the child and adolescent population experiences higher levels of poverty compared with the general population. This is directly related to the family composition of these households, often led by a mother who serves as the head of the household and sole financial provider. This phenomenon is even more pronounced in the population younger than 4 years (EnfermeríaAPS, 2013).
In response to this, in 2008, the Comprehensive Early Childhood Protection System was implemented nationwide, better known as Chile Crece Contigo, which acquired the status of law in 2009 (Law 20.379). This system is a management model composed of various state agencies with the objective of providing differentiated conditions to socioeconomically deprived families, thereby reducing more complex inequalities during the critical period of development, specifically from gestation to 4 years of age. However, several authors have been critical in highlighting how the program was conceived and the implications of this for its development:
Chile Crece Contigo program originated from measures proposed by the Advisory Council for the Reform of Childhood Policies, which operated in 2006. This council was composed of representatives from the Catholic Church, the Ministry of Education, and the medical field. The council’s final report suggested establishing a system that contributes to ensuring all girls and boys undergo a full and balanced development process during their early years of life (Moreno, 2006). A consultation process took place involving representatives from more than twenty public institutions, civil society, and children and adolescents (Final Report Council, 2006). There was no requirement or indication of the involvement of women’s organizations in the consultation process, highlighting an initial separation in the treatment of policies directed toward children and gender and family policies. It is thus configured that addressing the needs of children is dissociated from the challenges faced by those responsible for their care: mothers and, to a lesser extent, fathers. (Caro, 2009, p. 27) [Translation by authors].
This is due to a technocratic, centralized, and normative idea of what would be the most appropriate ways to protect children and, at the same time, control the exercise of motherhood and, consequently, the sexuality of women. In this sense, Caro (2009) argues for the existence of a paradoxical logic in state protection discourses, as they go hand in hand with control in social interventions:
Protection, in most cases, implies control either of the person being intervened or of their environment. Being labeled as a subject “to be protected” places them in a position of vulnerability compared to others because they are assumed not to possess those standards considered normal at an individual or social level for the “normalized” development of that person. They are presumed to be a “not yet.” (Caro, 2009, p. 28) [Translation by authors].
It is worth noting that some actions have been adapted in pursuit of recognizing the autonomy of women and children. For example, the launch of the Biopsychosocial Development Support Program, which aims to “reinforce promotional and preventive actions with a view to protecting early childhood and achieving optimal development conditions, both at the primary care level and in motherhood” [Translate by authors]. Additionally, aspects that were previously not visualized or prioritized, such as the ethno-racial origin of children, the geographical areas where they live, and the socio-health conditions in which they develop, have been considered. These conditions manifest in unequal health outcomes in the child population aged 0 to 9 years.
While there is recognition of openness to other social categories and an intention to move toward a less centralized idea of the national territory, these advances still follow logics that position women from a material deprivation perspective. Equality is perceived primarily as an economic issue, “linked more to class than to other differences since the program is presented as a means to break the cycle of reproduction of inequality and poverty in families” (Caro, 2009, p.32) [Translate by authors]. In other words, there is a lack of an intersectional perspective (Fernández Labbé et al., 2020; Pinto Baleisan and Cisternas Collao, 2020; Reyes Muñoz and Reyes Muñoz, 2021) that considers other categories of difference that accentuate inequality in the national territory, such as migratory differences.
Similarly, the National Childhood Health Program includes various strategies for implementing, monitoring, and to a lesser extent, evaluating the general and specific objectives derived from its implementation. These strategies include targeting and annual supervision of the activities outlined in the program, which includes “skills leveling for professionals through a relevant and continuous training system for healthcare teams” [Translate by authors]. These strategies are administratively monitored in the Regional Ministerial Health Secretariats, Health Services, and Health Centers in the territory. The purpose is to:
Contribute to the health and integral development of children under 10 years of age, in their family and community context, through activities that promote, protect, prevent, recover health, and rehabilitate, encouraging the full expression of their biopsychosocial potential and a better quality of life2. [Translate by authors].
The National Childhood Health Program is presented as a public policy for the promotion of rights and protection of childhood, including the gestation and motherhood period. At the same time, it proposes strict control and monitoring in the execution of the activities it encompasses. This policy has as its basis and principle the same conditions for all participants of the program, however this assumption acts overlooking the differences of the population. What is expected is an acculturation of the other, a need to redirect the cultural forms, thoughts, and actions of diversity under the idea of equality policies that are absolutely exclusive of those who need to be addressed in diverse and intersectional ways.
2.3 Afro-Latino immigration in Chile, violence against pregnant women and acculturation
Migration in Chile has a long history and intersects, as in all Latin American countries, with a history of conquest, colonization, and slavery. In the country’s history, migrations of people from Peru, China, and Bolivia to the northern region during the saltpeter and mining boom in the late 19th and early 20th centuries are relevant. These migrations marked a social, demographic, and phenotypic identity in those territories. The migration of Yugoslav, German, and Polish people in the south and southern region of the country is also noteworthy, following the process of colonization and whitening of the Mapuche territory. This migration is characterized by a desired type of migrant compared with those who arrived in the northern region, primarily due to the European and white origin of the former (Cano and Soffia, 2009, Cátedra de Racismos y Migraciones Contemporáneas de la Vicerrectoría de Extensión y Comunicaciones de la Universidad de Chile, and Movimiento Acción Migrante, 2019).
However, despite a migratory history in Chile, the act of migrating is often put to the test, “both in a pragmatic sense, involving problem-solving practices in daily life, and in a societal, structural sense, linked to social mobility (…). At both levels, explicit and implicit forms of rejection and discrimination occur” (Sibrian, 2021, p. 2) [Translate by authors]. In this context, the challenges of any migration, according to Siberian, include obstacles in the new territory, such as job placement and access to health, as well as expectations of recognition and acceptance by the citizens of the destination country. It is at the intersection of obstacles and expectations that several complexities arise in the migratory experience of those who participated in this study.
Afro-Latin American immigration, particularly from the Afro-Caribbean regions of the Dominican Republic and Haiti, has received the least recognition and social acceptance in Chile, especially between 2010 and 2019, just before the arrival of people from Venezuela, who today also face such social stigma. Perceptions of the local Chilean population regarding foreign communities currently residing in the country have revealed a societal culture that is racist, classist, and increasingly xenophobic (Castillo et al., 2023). These ideologies, rooted in the modernization project of the state since the early 20th century, have constructed the imagery of a country that observes itself as white and Europeanized, despite its Amerindian, Afro-descendant, and mestizo origins (Reyes Muñoz et al., 2021).
Social stigmatization directed toward black populations, particularly Dominicans and Haitians, is based on their ethno-racial, class, and gender condition. In the case of Haitian women, this stigmatization is further compounded by their linguistic difference and their country of origin, classified as the poorest in Latin America and the Caribbean. Stigmatization is observed in the numerous biases expressed by health professionals and officials who, for instance, judge women for their attachment practices, parenting, breastfeeding, and motherhood, and for not conforming to presumed “national” and international standards of motherhood (Reyes Muñoz et al., 2021; Reyes Muñoz and Chatelier, 2023). They are also judged for supposedly “not planning their motherhood” due to their “high pregnancy rates compared with Chilean women” and for not controlling their gestation process from the 7th or 8th week, as is the trend among local citizens.
Regarding the State, the record from the year 2021 on an institutional page of the Health Service indicates:
Of the total foreign mothers, Haitian women contribute the highest percentage of births, accounting for 21.1%, followed by Peruvian women at 14.7%. Regarding regions, those with the highest percentage of births to foreign women are Tarapacá with 33.7%, Antofagasta with 28.5%, Arica and Parinacota with 22.8% (all in the northern zone of Chile), and the Metropolitan Region with 21.0%. However, according to the Ministry of Health (MINSAL), pregnancy check-ups have decreased, as the number of entries into the prenatal care program for pregnant women fell by 7%, reaching 162,542, the lowest figure in the last 5 years. (Migración en Chile, 2021, p. 1) [Translate by authors].
The data reveal that Chile has lowered its indicators regarding pregnancy, monitoring due to the arrival of foreign women. In this context, at the local level, Haitian women are often at the focus of the discussion. This is because in Haiti, women do not usually monitor their pregnancies as closely as in Chile, including cases where women are not monitored in their gestation until the day of delivery itself. This could be due to the existence of support networks among women in the family and friends of the expectant mother, who monitor the pregnancy and provide assistance to pregnant women during the process. Additionally, economic precarity, the costs of care, and the distance to some health centers may contribute to this situation (Reyes Muñoz et al., 2021). On the other hand, it is also essential to highlight that in Chile, pregnancy and childbirth are continuously monitored but also highly medicalized and pathologized (Sadler Spencer, 2004, 2016).
Research on the violence faced by racialized women who are mothers has been developed and expanded in recent years in Latin America. Examples include the studies by Lube Guizardi et al. (2019), León Gin (2014), Posso Quiceno (2010), Betancourt Burón and Gross Gutiérrez (2018), and Arias Hurtado and Carrillo Pineda (2019), among others. Social inequalities in child health have been predominantly studied in relation to the family’s socioeconomic status, class analysis, and the educational level of parents (González-Rábago and Martín, 2019). However, there has been less focus on inequalities associated with racism and the migratory status of these children and their parents. This has become an important category to analyze in the field of health inequalities and their social determinants in recent decades. González-Rábago and Martín (2019) point out that evidence of health inequalities among migrant and local adult populations is strong, but studies on the generations descended from immigrants are still scarce in Europe and Latin America.
In Chile, there have been some recent studies addressing the ethnic-racial category as a constitutive element of structural inequalities experienced by migrant women who are mothers in the health system (Reyes Muñoz et al., 2021). These studies also explore the conditions of access and use of the health system (Antilef Ojeda et al., 2020), discrimination and exclusion toward migrants in the health system (Liberona Concha and Mansilla, 2017; Zepeda Vega and González Campos, 2019), and maternity among Haitian women in Chile (Abarca Brown, 2018; Reyes Muñoz, 2023; Reyes Muñoz and Chatelier, 2023). These studies demonstrate that state and societal logics bring acculturation policies toward the Afro-descendant and migrant population.
In this regard, several studies in Chile have addressed how migrants, who assimilate into Chilean societal logics, are perceived as less threatening by locals compared with those who opt for biculturalism (maintaining their cultural identity while simultaneously adopting aspects of the dominant culture), as proposed by Berry (2003) in his theoretical model on acculturation. This theory establishes four types of acculturation, understanding that migrant individuals must make complex individual adjustments, as well as emotional and sociocognitive adjustments, to respond to the double dilemma of maintaining the cultural identity of origin or incorporating cultural characteristics of the host societies and thereby losing significant elements of their own culture.
These acculturation types are integration or biculturalism (maintaining one’s cultural identity while simultaneously adopting aspects of the dominant culture), assimilation (orientation toward the receiving culture and abandonment of one’s own cultural identity), separation (maintaining one’s cultural identity while simultaneously developing a negative attitude toward the culture of the receiving society), and marginalization or anomie (a negative attitude toward both cultural frameworks).
For example, in the research conducted by Mera et al. (2017) in the city of Concepción (in southern Chile), significant elements were found between perceived discrimination by migrants and their overall psychological well-being, which decreases when migrants choose the assimilation strategy. However, this has consequences for how they relate to their own communities in the destination countries. The study by Arenas and Urzúa (2016) on South–South migrants in northern Chile illustrates this. It indicates that migrants who chose loyalty to the in-group, i.e., a strategy of integration and separation from the host population, have a more positive orientation toward their ethnic group, unlike those who use an assimilation strategy.
3 Methodology
This research is part of a broader study framed within the doctoral research process of one of the authors, aiming to analyze the phenomenon of structural racism toward Haitian women—mothers and expectant mothers—living in Chile, from an intersectional approach. The study received approval from the Ethics Committee of her educational institution, the University Católica de Murcia, Spain, under the number CE0171925.
The presented text discusses how state care services under the National Childhood Health Program, implemented by nursing staff in Chile, can become a mechanism for the social acceptance of Afro-descendant migrant mothers who seek healthcare for their children in health centers across the country. To achieve this, five specific objectives were developed: two to understand the experiences of Afro-descendant women residing in Chile regarding access to healthcare for their children: (i) Describe the experiences of Afro-descendant migrant women in Chile regarding access to health; and (ii) Describe the experiences of migrant women bringing their children born in Chile to the check-ups of the National Childhood Health Program. Additionally, three objectives were designed to understand the implementation experiences of the program by nurses working directly with migrant mothers and children in primary healthcare. These were: (iii) Describe the experiences of nurses working with migrant mothers and their children in the National Childhood Health Program; (iv) Describe nurses’ perceptions of the motherhood of migrant women in general, particularly Afro-descendant women; and finally, (v) Describe the cultural adaptations made by nurses to the National Childhood Health Program when working with migrant children or mothers.
All participants in this research: migrant women and primary health care nurses, (see Tables 1, 2) were informed about the research objectives and provided informed consent by signing consent forms (Tables 1, 2).
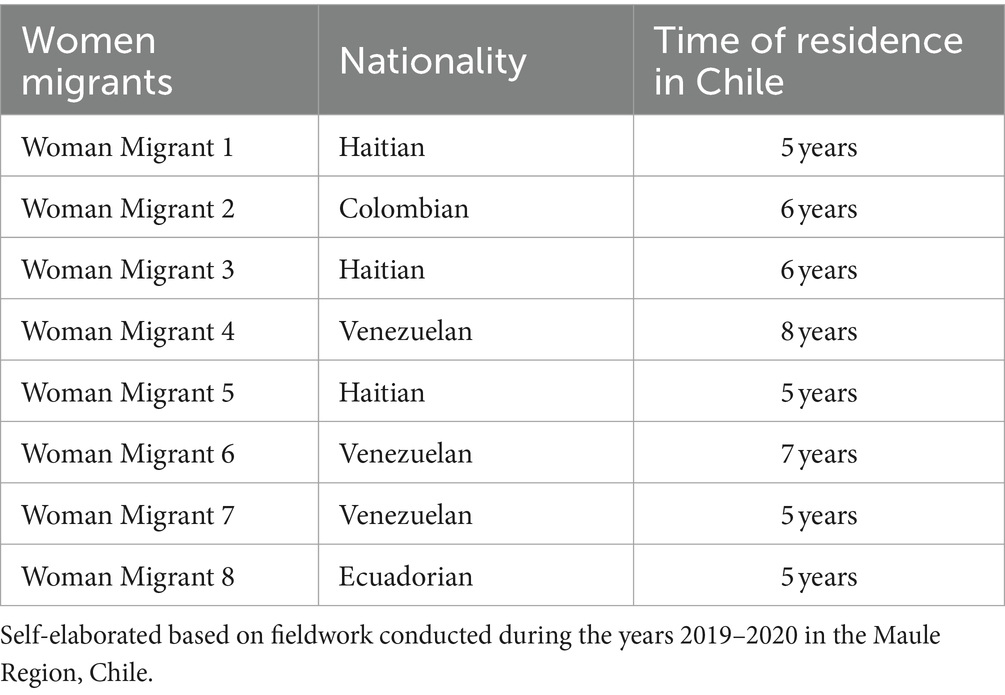
Table 1. Characterization of Afro-descendant migrant women participants.
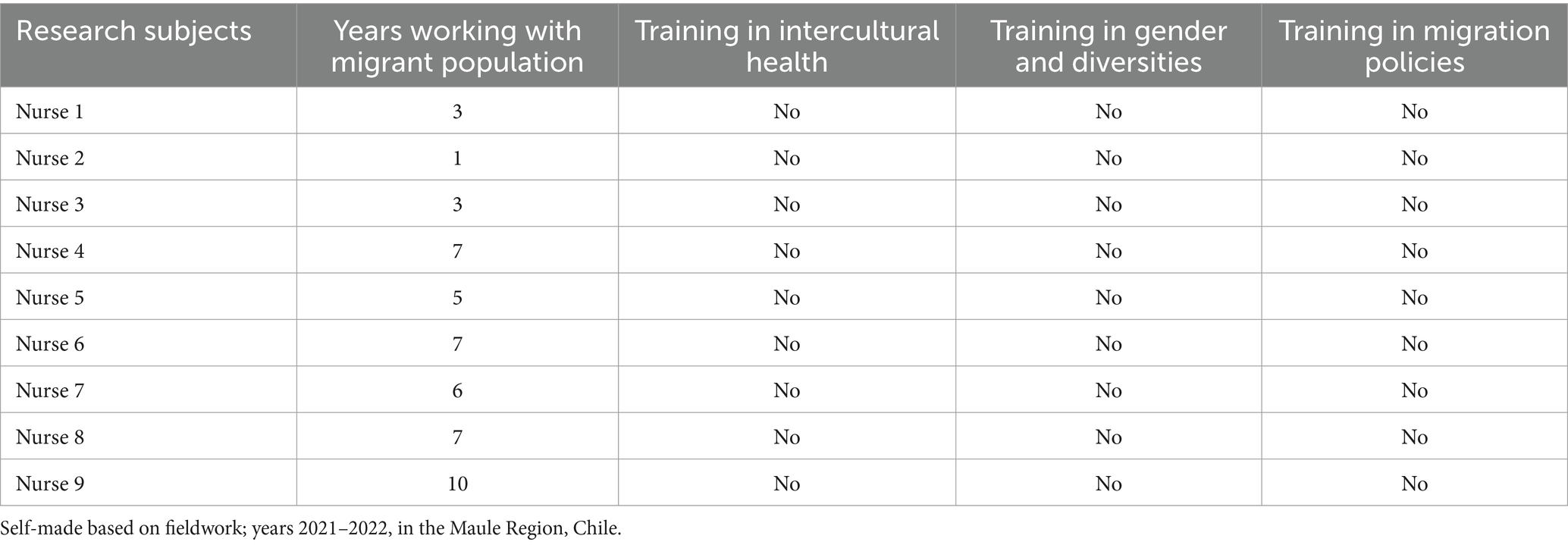
Table 2. Characterization of nurses participating in the study.
Narrative Productions were also conducted in six thematic workshops with migrant women to discuss their experiences in health centers in the Maule Region, city of Talca, Chile. Narrative Productions (Luxán Serrano and Azpiazu Carballo, 2017) stem from and build upon the work carried out in a conversation group or an individual interview, where people discuss a topic or a phenomenon, bringing forth relevant reflections about migrant motherhood.
4 Findings
4.1 Experiences in the access to healthcare for Afro-descendant migrant women in Chile
The experiences of migrant women when attending different healthcare centers are diverse. When broken down by nationality, the narratives are primarily shaped by the experiences of childbirth among Haitian women and their transnational motherhood, where it is highlighted:
One of the most notable differences is that in Haiti, there are more natural childbirths. There, what we do is natural childbirth because that’s how we want it. A cesarean section is only performed when the delivery is difficult… if there are complications. If there is a possibility of natural childbirth, a cesarean section is never done. Doctors do not perform a cesarean section just because a woman wants it; it is done only if the baby is in distress. Another very different thing is that in Haiti, the baby is not bathed when born, only cleaned. Because that will harm the baby later on. But here, the doctors do not understand and scold the women because they only want to clean with a cloth and be with the baby. And they take them away, they snatch them away, not letting the mother spend more time with the baby…” (Narrative Production) [Traslate by authors].
Haitian women also describe the misunderstanding they feel when healthcare professionals find out they have a son or daughter living in Haiti and therefore they prefer not to mention it. This reveals a ‘different’ way of thinking and understanding the exercise of motherhood by migrant women but also the fear of being judged as bad mothers, despite being aware of the difficulties of their experiences and that, many times, transnational motherhood is not the option they would have chosen. This makes them feel guilty in front of healthcare professionals, who, as Martínez Pereira (2021) points out, assign exclusive responsibility to women for their circumstances. As reflected in the narratives:
I think, I do not know… It’s better not to say that one has a child there (In Haiti). They look at you badly. (Migrant Woman 1).
I have a problem because my son lives in Haiti. They (healthcare professionals) thought, like, I’m crazy. They did not understand. I cried and cried, and they did not understand. (Migrant Woman 3).
I have my son in Haiti. I think that’s why they treat me poorly here. I believe they (healthcare professionals) think I’m bad because I’m not with my son. (Migrant Woman 5).
[Translate by authors].
The fear of rejection demonstrates an intention to do well, comply with what is requested, the effect of the normative mandate that must be fulfilled to participate in a healthcare system that does not feel like their own but in which they want and need to participate.
In the case of Venezuelan women, from another perspective, their stories reveal disparities between the healthcare received in their home country, where they paid for medical care, and Chile, where they are treated in the public service through the National Health Fund, which may involve co-payment or may be free depending on the income of the users. The interviewees point out that their experiences with healthcare in Chile are not as positive as in their home country, attributing this difference to the payment for private services in Venezuela versus the public healthcare they receive in Chile:
Healthcare in Venezuela is a bit more affordable than here, and generally, I used to go to private clinics. Also, the company I worked for covered health insurance; so, I preferred to attend private consultations, and I had no problem doing so. Because the public healthcare, like the CESFAM (Family Care Center) here, has a lot of people, and it would collapse, so I preferred to have a bit more money with insurance and have private consultations. (Migrant Woman 4).
I consider that the attention in my country is much better than here. Here they have 10 or 15 min to see the patient and that’s it. And sometimes they do not examine you as it should be. On the other hand, in my country (if I paid for a consultation, I did not go to the CESFAM like here where it is free) the attention can last an hour, they even do tests, and everything to say, to find out what you really have. But here (in Chile) I have taken my baby, who is 10 months old, to the hospital and I tell the doctor that he has a fever or vomiting and this and this, and they only give him medicine for the fever and I spent four or five hours there in observation and they do not do any tests, nothing… So that part is a little negative here, although as I said in my country I paid. So there they really try to see what the patient has, and in that case I say that I prefer the medical attention in my country as such. (Migrant Woman 6).
[Translate by authors].
In the narratives of Venezuelan women, there is criticism and objection to the normalized practices in Chilean healthcare, such as “sometimes they do not examine you as it should be,” while acknowledging that the condition of gratuity implies a tacit acceptance of the mistreatment being criticized, “although, as I tell you, in my country, I paid.”
The participants recognize the gratuity of public healthcare, regardless of nationality. However, as mentioned in the preceding paragraph, this condition seems to imply accepting all actions and behaviors, including mistreatment, as part of receiving a free service, which is often difficult for migrant women to challenge or criticize in the moment.
4.2 Experiences of migrant women with their children in the controls of the National Child Health Program
Regarding the specific experiences of migrant women in the check-ups for their children who attend the National Child Health Program, a very positive evaluation is noted. Mandatory check-ups and follow-up are appreciated as a genuine concern on the part of healthcare personnel. The centrality of gratuity persists, compared with the home country, seemingly also interpreted as a reward for completing the process:
In general, my experience here in Chile has been very good. Because back in my country, in Ecuador, they do not force you to go to the health center. For example, if you are pregnant, if you want to, you go to the health center, and if you do not want to, you just do not go to the health center and go when you are going to give birth. And when the baby is small, if you want to, you take it to the vaccinations and if you do not want to, you do not get any vaccinations and there is no problem, they do not say anything… they do not persecute you. On the other hand, here they force you to go to the check-ups, and if you do not go, they call you; they worry. And I feel that this is important because over there, for example, babies sometimes die, and mothers die too, especially in childbirth. In the hospitals the attention is very bad… so not here, here they care, they call you, the social worker asks you why you did not go to appointments, to check-ups. And that is important. Also, here they give the “Purita” milk to the mother and when the baby needs more milk they give another milk for free… so in my country they do not even give a diaper, here they gave me a crib, a complete set of baby things, clothes, diapers, games… In my country there is nothing like that, that’s why I never checked myself or anything, because they do not care if you go or not. (Migrant Woman 8) [Translate by authors].
Here, we observe how adapting to the requirements and practices of healthcare personnel is a way of demonstrating appreciation for the program. Therefore, while recognizing the shortcomings of the program, there is simultaneous gratitude for its existence and the care it provides during the gestation process for pregnant women and children. Gratuity remains a crucial element that motivates continued participation.
Everything is very good; the work, the health care… for example, now that I had my baby in the hospital, everything was very nice. Because in my country, for example, they do not take care of you with so much importance. For example, my baby was hospitalized for eleven days and every day the doctor came by and they explained to you what was wrong with your baby; the social worker was also looking after you, the nurses were looking after the baby… there was never something like saying it was bad… everything was excellent. And I was very happy because in reality the attention here is nothing compared to my country, in my country, first of all there is not even a pediatrician there, like here, specialties… if my baby had been sick maybe I would have spent a lot of money there, but instead here it was very free, it did not cost me a penny. Very nice attention, the doctors were excellent and I was very happy because my baby, thank God, is well and was able to come out well and it did not cost me anything, because the attention was free and very good. And then at the “Poli” (Family Health Center) at all the check-ups they have been very kind; I go with my baby to the appointments that are scheduled in advance and the nurse, the social worker, the whole team is there to attend us well; it is really a blessing. (Migrant Woman 2) [Translate by authors].
As it is evident, the interviewed women feel satisfied, especially regarding the check-up for their children. The follow-up is not considered an unnecessary or mechanical practice; on the contrary, it is a way in which they feel their presence, as well as the presence of their children is valued, and where they perceive a genuine concern for their well-being.
4.3 Experiences of nurses working with foreign mothers and their children in the care of the National Child Health Program
In this section, we will discuss the perspective that nurses have regarding the National Childhood Health Program and the care provided to migrant women and their motherhood practices.
The general knowledge that nurses have about this program would indicate that, with a greater number of years working in it, their knowledge becomes more specific, providing a theoretical background for the implementation of the policy. In contrast, the knowledge of nurses who have recently joined the program is more general and focuses on the practical aspects of care. For instance, a nurse with less than a year of experience in this area states:
Well, Chile Grows with You, which is more commonly known as the program, oversees the health care of children, specifically focusing on complementary feeding and also addressing children with food allergies. It also includes vaccinations, stimulation rooms with preschool educators, speech therapists, etc. However, sometimes parents do not take their children to these programs. Sets of games are also provided to encourage the cognitive development of children. (Nurse 2) [Translate by authors].
A nurse from a busier center, with 3 years of experience in the program, states:
The program looks for risk factors and potentialities, in addition to assessing tools for these children. Moreover, there is constant evaluation throughout the life cycle; from two months up to 9 years… well, 9 years, 11 months, and 30 days… because then children move on to another program. Also, it is a multidisciplinary program, with many professionals attending to them and providing what is necessary for their integral development. (Nurse 1) [Translate by authors].
Now, unlike the general view regarding the program and its ability to describe it, it seems that the time spent working on it does not imply mastery of other topics of interest for migrant women. However, unlike the general view about the program and their ability to describe it, the time working in this program does not imply knowledge of other topics of interest to migrant women, such as intercultural health, health and migration policies, or gender and sexual diversity, where the interviewees also demonstrate and recognize an important deficit in their training:
Regarding human rights, more than the program itself, there is the part of professional ethics that implies that we have to treat everyone equally. And from there, ethical values. Now, regarding a gender perspective, no, we do not have knowledge. And regarding health and international migrant policies, I know it exists, but not more than that. (Nurse 3).
On human rights, receiving timely health care. And yes, of course, their rights are respected. For example, there is the issue of immunization, vaccinations. The socioeconomic part of the children is also evaluated, social vulnerabilities; there is a social worker in charge of that, and we go to visit them at their homes, we do home visits when it is believed that children are exposed to situations of vulnerability. Nutrition is also considered, the food given to them depending on their nutritional condition. (Nurse 4).
Now, the gender and transgender aspects, that is not visible; I think it’s due to a lack of training. And health and international migrant policies, nothing. (Nurse 7).
[Translate by authors].
The absence of training processes is a critical element for the interviewed professionals; however, the recognition of the lack of tools does not justify judgments on the mothering or responsibility practices of migrant women. Furthermore, the social and political context in the country and the media portrayal of migration as a problem do not facilitate its approach from a rights perspective, which is reflected in healthcare practices. In this sense, the nurses’ perceptions of the migration phenomenon resonate with the scenario of restrictions on the entry of Haitian and Venezuelan populations into the country:
I feel that fewer people are entering now… My perception is that maybe, since there are people entering without papers or through unauthorized steps, maybe they do not come to the CESFAM. (Nurse 3).
Well, since they recently started reopening the borders after COVID-19, the migratory pattern has changed too. I would say that currently, we have one Haitian family, the rest are all Venezuelans. (Nurse 4).
There are conflicting opinions. Everything happening in the north, with people entering through unauthorized steps, living for months on the street, in tents, without basic services… and now we see that in the streets, here in the city, with Venezuelan children asking for money, and we did not see that before… I wonder, ‘Isn’t there an option for these children to go to kindergarten? Perhaps if they enter illegally, maybe they cannot, or they do not have the means… But when children ask for money, there is a violation of their rights. But I agree with migration. (Nurse 2) [Translate by authors].
The nurses’ narratives also show a lack of knowledge about the Policy on Health and International Migrants and the right to health care regardless of the migrant status of individuals.
4.4 Nurses’ perceptions of motherhood among migrant women, in general, and, particularly, Haitian and Afro-descendant women
Perceptions of the interviewed nurses regarding the motherhood of migrant women remain anchored in the idea of birth control as a measure to reduce poverty, which is inherent in the state’s modernization project (Álvarez Díaz and Aguirre Munizaga, 2021):
Mmm… Honestly, they do not take precautions. Look, they used herbs to avoid getting pregnant, and obviously, they got pregnant. The Venezuelans… oh, I’ve thought about it, but I do not want to think about it, but it’s true, I think about it… Well, they do not have jobs and get pregnant, they cannot support those children, and later they are out on the street asking for help… I do not know. I find it very irresponsible. (Nurse 5) [Translate by authors].
This occurs in a socioeconomic context which is perceived as critical for both locals and migrants. Despite Chile showing a significant decrease in local population birth rates, the notion of migrant-led fertility does not appear to be part of the predominant discourses, neither among healthcare professionals nor in the general society.
I feel that motherhood… that everything comes down to whether it is desired or not, in general terms… And that does not depend on whether they are Chilean or foreign, it depends on other things. Now, with the Haitian population, something particular happens to me; it happens with some mothers who do not have the same attachment. And talking to colleagues, this is related to the infant mortality rate in these countries. So, faced with these rates, it is linked to the lack of attachment. And I experience that with babies, but with older children, they do have a more affectionate relationship, they smile, they are happy. (Nurse 1) [Translate by authors].
In this scenario, the image constructed of Haitian motherhood demonstrates xenophobic, racist, and classist treatment. The socioeconomic context is used to justify the overemphasis on their healthcare and that of their children. This justifies control while disregarding the women’s own will regarding their maternal desires, parenting practices, and childcare (Álvarez Díaz and Aguirre Munizaga, 2021). This is under the unquestionable assumption that “migrant women are at risk if they do not adhere to the guidelines of the Chilean health system” (Martínez Pereira, 2021, p. 86) [Translate by authors], especially concerning their children who would not receive the “same attachment.”
For instance, if the mother does not speak, that is, if the mother only speaks Creole and does not speak Spanish, how can you educate her? If they do not speak, they do not speak. They are so shy that they barely greet. So, you cannot provide any education because if she does not speak Creole and does not understand Spanish, you limit yourself to conducting health checks, weighing the baby, anthropometric measurements, and referring if necessary. But what can you do if they have been living in Chile for four years and still cannot say hello? Or say any phrase like “my child is sick,” they communicate with signs. So, faced with that, what are you going to do? It’s challenging if we used to have a translator, so it was more straightforward because you would go get Agustin, for example, to translate the Edinburgh Postnatal Depression Scale, it was much easier, but now we do not have a translator. (Nurse 5) [Translate by authors].
This anchors the health professionals’ imaginings of “correct” ways to be mothers. In the following account, you can see how Haitian women are viewed when they follow the recommendations and instructions given in health centers:
Good, in general, it has been a good experience. Haitian moms are very humble; they are receptive to what you tell them, they always comply, as you told them; they are always concerned about the children and always seem happy, pleasant. It’s like they are always smiling, pleasant; I do not know what they see. But yes, the Spanish language is difficult for them. (…) for example, I do not know, the hip X-ray… but I think it’s more because, since they do not understand that they have to come to certain check-ups or go here or there, ultimately, they do not go. So sometimes, you tell them to go, and there they go. So I think they get a little confused, but in general, the experience is good. (Nurse 9) [Translate by authors].
Regarding differences between the health and psychomotor skills (or other skills) of Chilean mothers’ children and those of foreign mothers, nurses comment, continuing to construct an image of migrant mothers without knowledge or conditions to do what is supposed to be the right way to be/do:
Yes, a lot. I’ve had to go see what they have for dinner, for example, ask more in that sense about what they eat. I also see it a bit socially; for example, if they are arriving at the kindergarten, if the babies are well dressed, sometimes they put too much clothes on them, and then they arrive sick at the health center. (Nurse 2).
Honestly, I do not notice differences in health between Chilean and foreign mothers. Except in diet. Now, regarding psychomotor skills, yes, I have noticed that; all the referrals to stimulation rooms are children of foreign mothers. (Nurse 1).
[Translate by authors].
This is related to what Martínez Pereira (2021) points out about the Chile Grows with You program in family health centers, where there is an insistence and a mandate “to change habits and ways of life that are not considered normal for the local care culture” (2021, p. 85–86) [Translate by authors]. This adds to the idea that professionals must “convince migrant women” to adhere to the program because “she,” “the migrant,” does not see the benefits it offers, without considering underlying structural factors, such as absences from check-ups. The following narrative illustrates this very prominently:
…my experience was not very good in the sense that, well, there was the language barrier; she did not speak much Spanish. At one point, a six-month check-up came, and she was very emotionally labile. I had to apply the Edinburgh (test to assess postpartum depression), it came out altered, and well, to ensure that we have a good score, it was applied to her in Creole. The result came out altered, and we had to make a referral to a doctor; she went with the doctor, was referred to the psychosocial team, a social worker, a psychologist, but it was a completely ineffective intervention because, of course, she came, they did not understand her, like they could not achieve effective communication due to the scarcity of the language. So in the end, she did not want to come anymore, so she also stopped going to the psychologist, stopped going to the social worker. The child, also, being altered in Edinburgh, was referred to the stimulation room. He did not go to the stimulation room anymore, so he left all that aside. So when she later returned for a check-up, I had to apply the instrument again, also in Creole. There, a normal score came out, but even so, she tried to communicate with me and tell me that she had problems in Chile, family problems, everything that made her feel bad. Logical things. But it’s complex because you try to explain, you try to communicate with them anyway. And they say yes, yes, yes, yes. But in the end, you realize that they are not understanding you. So, it’s complex to address these check-ups. (Nurse 5) [Translate by authors].
4.5 Cultural adaptations made by nurses to the National Child Health Program when working with migrant children
As for the question of whether the Program influences the quality of life of the children of migrant mothers living in Chile, the professionals state:
I think in a very good way. The mothers leave very grateful. What has happened to me is that sometimes they do not go to the referrals; but in general they feel good, because there is also the delivery of food for the children, for them; so that is very important for the women and their babies and their older children. (Nurse 9).
The quality of life of children is related from before the child is born. And the National Child Health Program affects considerably; for example, the national complementary feeding program, which is now also considering poor nutrition due to deficit, because migrant children are underweight and before the nutritional problem of children in Chile was due to excess; but in the case of migrants, they are families who spend money here, who also send money to their relatives in their countries of origin. On the other hand, there are the vaccinations, the calendar is adapted to Creole; in addition, the test to evaluate postpartum depression is also adapted to Creole. (Nurse 1).
[Translate by authors].
As observed, the nurses, in general, have made adaptations more from their own initiative to better serve migrant children, especially those who are the offspring of Haitian women due to the language difference. However, they do not provide a critical assessment of the Program, let alone the normative, uniform, and overly vigilant behavior that it imposes on migrant motherhood, as illustrated in the following quote:
I do not really see any deficit in the program, but this center is such a small place, we do not have a large migrant population… besides, it is in a rather residential, old neighborhood, with a large retired population, so there are not many migrants. But there are, but I do not see any problems with them, so I have not had to make any adaptations. Everyone is treated the same here. (Nurse 2) [Translate by authors].
Nor do the nurses discuss the logic of equality that underlies their discourse and that of the State. Much less do they consider how “treating everyone equally” when providing differentiated care is also a form of violence and discrimination, given the real and structural differences in the ways the image of Chilean society and family has been constructed, with a single form of motherhood and attachment at its core.
Let us see if the wife does not speak Spanish, I give her everything in writing. She’ll have… she’ll have the job of telling the husband, some friend or some relative and have him translate it. (Nurse 5) [Translate by authors].
On the other hand, Program professionals state that it meets the needs of migrant communities and does not require adaptation or revision:
Here they are welcomed, visits are made to them, they are given the layette, the milk. Everything as it should be. (Nurse 5).
I believe that the care we provide to migrants is really good. (Nurse 9).
We provide equal care for all people who come here, we do not distinguish between Chileans and foreigners. (Nurse 3).
[Translate by authors].
Although there are professionals who recognize the need to change and evaluate the relevance of the Program in a dynamic social context, and who state that it is necessary to recognize the autonomy and agency of migrant and local women and mothers regarding care.
Yes, there are many things that I would modify, absolutely, starting with the facilitators; the training of professionals; the information available in Creole for children; training in language and also in culture, for example, learning about how health centers are in other countries, how the vaccine schedule is, etc., how families are there… And of course, understanding the appreciation that mothers have about the care we are providing them; what they specifically need. (Nurse 1) [Translate by authors].
5 Discussion
As observed in the findings, concerning the experiences of migrant mothers in the Chilean Health System (objective 1), they generally have a positive evaluation. However, variations arise due to the diverse maternal experiences in their respective home countries. For instance, Venezuelan women express that they used private healthcare in Venezuela, which they perceive as superior to the healthcare system in Chile. Nevertheless, they acknowledge seeking care in the Chilean public health service, which is either free or involves co-payment. On the other hand, Ecuadorian, Colombian, and Haitian women evaluate their healthcare experiences in Chile much more satisfactorily than in their countries of origin. They highlight the constant monitoring during pregnancy, regular check-ups, and the provision of essential items for child rearing in the early months, such as clothing, cribs, milk, among others. Moreover, ongoing check-ups for their growing children contribute to a positive perception.
Regarding the objective focusing on the experiences of migrant women in the Childhood Health Program (objective 2), there is a positive acknowledgment of the program and its associated practices. However, from a critical standpoint aligned with Martínez Pereira (2021), it is crucial to recognize that “women are within a constant logic of observation and monitoring by different health professionals” (p. 82) [Translate by authors]. This continuous scrutiny, combined with material incentives provided by the program, functions as a means to encourage adherence to local care practices. These normalized program practices limit the possibilities of complaints or questioning from users, establishing a power hierarchy between health professionals and women. It is noteworthy that women identify negative elements in healthcare, particularly during childbirth, where their cultural practices are overlooked, and they are not heard or informed about their experiences. Parallel to the experiences of indigenous women discussed by Caro (2009) and Smith-Oka (2009), the control and execution of non-consensual practices, as indicated in the narrative production: “they take them away, they take them away, they do not let the mother be with the baby anymore,” “they challenge women because they just want to wipe with a wipe and be with him” [Translate by authors], reveal an entrenched and normalized hierarchical operation within healthcare.
Addressing the incorporation of cultural knowledge and practices into the Childhood Health Program becomes imperative. The challenge is to avoid outright dismissal, infantilization, and violence against the knowledge and cultural practices of migrant women. They are not merely recipients of care but bearers of knowledge that can engage in meaningful dialogue with what Caro (2009) identifies as expert knowledge, in which women, and even more so if they are migrants or indigenous, are constructed as:
a needy other, who does not know, therefore, that it is necessary to “educate,” “inform” and “discipline.” How is this “expert knowledge” articulated with the knowledge possessed by families and especially by women on parenting issues that have been transmitted intergenerationally? We want to model in front of a field in which there is a popular knowledge, close or far from “scientific knowledge,” but which is necessary to recognize, contrast and dialogue with the expert knowledge. (Caro, 2009, p. 28) [Translate by authors].
Concerning the analysis of the experiences of nurses working in primary health care and specifically in the Childhood Health Program (objective 3), it is evident that these professionals do not perceive racialized migrant women as autonomous agents in their reproductive, nurturing, attachment, and motherhood processes. This aligns with Martínez Pereira (2021), highlighting an asymmetrical health professional-patient relationship where migrant women are not perceived as capable of understanding their health processes or conveying their needs. In this systemic logic, “women are continuously at risk if they fail to comply with the established guidelines in medical consultations and workshops” (Martínez Pereira, 2021, p. 87) [Translate by authors]. This is evident in various experiences described earlier, demonstrating how nursing professionals assume the responsibility to convince users to attend check-ups without considering the sociocultural, political, and economic context underlying the absence of migrant women from certain appointments. It emphasizes the necessity of analyzing the structures of inequality and power inherent in healthcare systems to comprehend the complexities faced by racialized migrant women. And while the possibility of risk is real, it is not due to complying or not with the Program’s contents; rather, it stems from the structural inequalities experienced by racialized migrant women in various state services, and, of course, in healthcare institutions.
In relation to objective 4, regarding the perception of nurses toward migrant women, it is indicated that there is a bias concerning their birth rates, arguing that they do not use contraceptive measures, do not control their pregnancies, and in the specific case of Haitian women, it is not possible to provide them with instructions on care for themselves and their children because they do not master Spanish. Thus, healthcare professionals naturally assert that their “ways” of care, motherhood, and attachment are the correct, only, and definitive ones for all users attending health centers. Moreover, it implies control and monitoring of migrant mothers, primarily racialized, as if they lacked autonomy and understanding to decide what is best for themselves and their children. In this regard, the work of Reyes Muñoz and Chatelier (2023) illustrates how Haitian women are constantly mistreated in Chilean health centers due to the ways in which they exercise care toward their children, breastfeeding practices, complementary feeding, and especially attachment.
Regarding objective 5, concerning the adaptations that nurses make to the National Childhood Health Program when working with migrant children, it should be noted that some professionals are critical of the program’s structure, perceiving it as stagnant. However, despite this reflection, they do not make relevant adjustments to the cultural reality of the users, repeatedly stating that they provide uniform care to all individuals who come to the health center. This is contradictory in a country that is becoming increasingly diverse and aspires paradoxically to less centralization, more diversity, and greater recognition. This may explain why autonomy and the inclusion of women, their knowledge, and experiences are not deemed relevant to the practices outlined in the program and by its implementers. In line with this, Martínez Pereira (2021) notes:
that the Chile Grows with You program (ChCC) has a local perspective on pregnancy care, using persuasion and guilt as a means to operationalize these guidelines and convince migrant women to adhere to the Chilean health system and prevailing care practices. (Martínez Pereira, 2021, p. 82) [Translate by authors].
Naturalizing many practices from the national discourse on care, attachment, breastfeeding, nutrition, etc., as universal and immutable issues, without reflecting on them as specific to the national context and without considering the real involvement of women in decisions about the care of their children; in other words, without recognizing them as subjects with agency. In this context, the work of Gideon and Ramm (2020) is interesting. They precisely point out that the State validates women as mothers, and therefore, its actions and discourses aim at the “protection” of motherhood. However, these political protection actions have the effect of confining women only to their role as mothers, excluding men, and denying the existence of women as citizens, thus establishing a maternal ideology that overlooks the cultural diversity of mother subjects and limiting women to their reproductive capacity. Therefore, if Chilean women do not comply with this imaginary associated with care, sacrifice, and submission, migrant women will be even more questioned and invalidated in what the State expects of them.
6 Conclusion
The experiences of Afro-descendant migrant women who have become mothers in Chile and who seek healthcare services through the National Childhood Health Program are diverse. They range from a majority expressing gratitude for the services provided by the State through healthcare professionals to criticisms of the system, where they sometimes feel ignored and mistreated.
The National Childhood Health Program needs to be evaluated not only based on outcome indicators but also in terms of the rationalities that shaped its design and how these are replicated in its implementation. It tends to disregard the knowledge and agency of women and their mothering practices, further overlooking the inequalities in their position in the host country. For example, there are significant differences in how pregnancies are carried out between Haitian and Chilean women. The former are accustomed to physiological births accompanied by dancing, prayers, and songs during labor itself, with pregnancies monitored by both healthcare professionals and traditional healers. They also follow breastfeeding practices supplemented with ground foods after the baby’s third month (Reyes Muñoz and Chatelier, 2023). This is viewed as incomprehensible by the Chilean healthcare system, where women are thoroughly controlled by biomedical professionals throughout the 9 months of pregnancy. There’s excessive medicalization and pathologization of childbirth, with cesarean section rates exceeding 55% (Sadler Spencer, 2004), and “mandatory” exclusive breastfeeding for the first 6 months (Reyes Muñoz, 2023).
Considering these findings, it can be argued that the Program operates uniformly in the discourses of nursing professionals without distinguishing between the local and migrant populations, ostensibly under the umbrella of human rights. However, two evident contradictions emerge from the narratives. First is that the evidence indicates there is a distinction from healthcare personnel toward Afro-descendant migrant women and their children. Second, the uniformity of the Program and the normativity underlying it imply a stance that does not promote human rights but rather controls and closely monitors women and their reproductive processes based on an idealized form of motherhood assumed to be the only correct way, without recognizing migrant women as autonomous beings capable of deciding on the exercise of their motherhood and their own agencies in these realms.
Therefore, the Program, which enjoys high prestige and recognition at the societal level, like any program, has a normative mandate. In this case, it is based on the control and close monitoring of women, and concerning migrant women, it tends toward assimilation in terms of Berry (2003), toward health practices in the destination country. In other words, it functions as a mechanism for acceptance into the social body, gradually compelling migrant women to abandon the cultural practices of their own identity. In this sense, women who comply with the Program and assimilate – as Berry (2003) would put it – into local forms, are valued, respected, and recognized, along with their children. Moreover, all women are perceived and positioned as the exclusive and sole caretakers, adhering to gender mandates, contracts, and roles naturally. Similarly, women who experience motherhood differently, exercise it in diverse ways, or conceptualize it from alternative logics of separation, are quickly labeled as “unfit,” “less affectionate,” “inexperienced,” and, therefore, subjects subjected to control and the reproduction of social norms.
In the same vein, it is argued that the monitoring of “instructions” and health control practices by the National Child Health Program on migrant mothers could influence expectations of inclusion and assimilation into the social body, both from the professionals who attend to them and the migrant women who visit healthcare centers. They are recognized as good mothers, as long as they behave like national women. However, this implies the acculturation of their forms of cultural identity, practices, actions, and desires.
Finally, this situated critical analysis cannot overlook the material conditions in which the National Child Health Program is implemented, as addressed in the findings, with few training opportunities for those providing care, but also with other deficiencies in terms of health coverage and suitable conditions for implementation. For example, the lack of intercultural facilitators, language mediators, experts in interculturality, gender diversity, human rights, among others.
In this context, medical anthropology and intercultural studies for addressing existing forms of acculturation could offer concrete actions to untangle critical knots involving the alteration of cultural practices and behaviors specific to certain communities. This includes addressing the differences and asymmetries that arise in the interaction between healthcare personnel and migrant women, along with their children, in various primary healthcare centers under the National Child Health Program.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by Comité de Ética de la Universidad Católica San Antonio de Murcia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YR: Writing – original draft, Investigation, Methodology, Writing – review & editing. VR: Writing – review & editing, Investigation.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors give thanks to Camila Faundez González, Alejandra Alegría Villenas, Carolina Pérez Vásquez and Karina Jara Olave.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^These ambulatory care facilities are situated in rural geographical areas, catering to populations of fewer than 20,000 residents. They are overseen by a health professional with technical expertise, supported by a team of professionals typically comprising individuals from the fields of medicine, nursing, dentistry, and obstetrics and childcare.
2. ^The overall objectives of the National Child Health Program with a Comprehensive Approach are four: (1) Reduce infant mortality and morbidity in the population under 10 years of age; (2) Strengthen timely, expeditious, continuous, decisive and quality health care for boys and girls in the public health network; (3) Contribute to the improvement in the quality of life in the child population, regardless of their health and socioeconomic condition; (4) Promote healthy habits and reduce health risk factors in children younger than 10 years of age, considering the life course approach.
References
Abarca Brown, G. (2018). “¡Promueva el apego!”: Sobre la maternidad de mujeres haitianas como objeto de Gobierno en Chile. Revista Bricolaje 3:3.
Álvarez Díaz, A., and Aguirre Munizaga, C. (2021). Desarrollismo Y Salud Reproductiva: La Intervención De Los Dispositivos Biomédicos En Los Cuerpos Femeninos Aymaras, En El Norte De Chile. Diálogo Andino 66, 365–376. doi: 10.4067/s0719-26812021000300365
Antilef Ojeda, M. A., Atherino dos Santos, E. K., and da Rosa Damiani, P. (2020). Experiencias de las mujeres inmigrantes en el acceso a la salud en Punta Arenas, Chile. Texto Contexto ENFERMAGEM 29:e20190276. doi: 10.1590/1980-265X-TCE-2019-0276
Arenas, P., and Urzúa, M. A. (2016). Estrategias de aculturación e identidad étnica: Un estudio en migrantes sur-sur en el norte de Chile. Univer. Psychol. 15, 15–25. doi: 10.11144/Javeriana.upsy15-1.eaie
Arias Hurtado, L., and Carrillo Pineda, M. (2019). Significados de la maternidad para un grupo de mujeres afrodescendientes. Index de Enfermería 28, 13–17.
Berry, J. W. (2003). “Acculturation: advances in theory, measurement, and applied research” in Conceptual approaches to acculturation. eds. K. M. Chun, P. Balls Organista, and M. Gerardo (Washington, DC: American Psychological Association), 17–37.
Betancourt Burón, D. D. L. C., and Gross Gutiérrez, A. G. (2018). Maternidades transnacionales. La reconfiguración de la parentalidad en familias cubanas protagonistas del proceso migratorio. Etnografías Contemporáneas 4, 159–184.
Cano, V., and Soffia, M. (2009). Los estudios sobre migración internacional en Chile: apuntes y comentarios para una agenda de investigación actualizada. Papeles de Poblacion 15, 129–167.
Caro, P. (2009). Análisis del programa Chile Crece Contigo desde los ideales normativos y la noción de prueba. Revista de Trabajo Social 77, 25–37. doi: 10.7764/rts.77.25-37
Castillo, J. C., Bonhomme, M., Miranda, D., and Iturra, J. (2023). Social cohesion and attitudinal changes toward migration: a longitudinal perspective amid the COVID-19 pandemic. Front. Sociol. 7:1009567. doi: 10.3389/fsoc.2022.1009567
Cátedra de Racismos y Migraciones Contemporáneas de la Vicerrectoría de Extensión y Comunicaciones de la Universidad de Chile, and Movimiento Acción Migrante. (2019). RACISMOS Y MIGRACIÓN CONTEMPORÁNEA EN CHILE (p. 60) [Informe alternativo para el Comité para la Eliminación de la Discriminación Racial]. Universidad de Chile.
Díaz Bernal, Z., Aguilar Guerra, T., and Linares Martín, X. (2015). La antropología médica aplicada a la salud pública. Revista Cubana de Salud Pública 41, 655–665.
EnfermeríaAPS (2013). Programa Nacional De Salud De La Infancia Con Enfoque Integral. Available at: https://www.enfermeriaaps.com/portal/norma-del-programa-nacional-de-salud-de-la-infancia-con-enfoque-integral-minsal-chile-2013
Fernández Labbé, J., Díaz Allendes, V., Aguirre Sanhueza, T., and Cortínez O’Ryan, V. (2020). Mujeres colombianas en Chile: Discursos y experiencia migratoria desde la interseccionalidad. Revista Colombiana de Sociología 43, 17–36. doi: 10.15446/rcs.v43n1.79075
Gideon, J., and Ramm, A. (2020). “Motherhood, social policies, and women’s activism in Latin America: an overview” in Motherhood, social policies and women’s activism in Latin America. eds. A. Ramm and J. Gideon (Cham: Springer International Publishing), 1–11.
Gobierno de Chile (2013). Programa Nacional de Salud de la Infancia con Enfoque Integral. Available at: https://extranet.who.int/nutrition/gina/es/node/39442
Goic, A. (2015). El Sistema de Salud de Chile: Una tarea pendiente. Rev. Med. Chile 143, 774–786. doi: 10.4067/S0034-98872015000600011
González-Rábago, Y., and Martín, U. (2019). Salud y determinantes sociales de la salud en hijos e hijas de personas inmigrantes internacionales: ¿desigualdades sociales en salud desde la infancia? Gac. Sanit. 33, 156–161. doi: 10.1016/j.gaceta.2017.10.007
Inhorn, M. C. (2007). Reproductive disruptions: gender, technology, and biopolitics in the new millennium, New York: Berghahn Books.
León Gin, C. (2014). La retradicionalización de los roles de género en la maternidad transnacional: El caso de mujeres peruanas en Santiago de Chile. Si Somos Americanos 14, 15–40. doi: 10.4067/S0719-09482014000100002
Liberona Concha, N. L., and Mansilla, M. Á. (2017). Pacientes ilegítimos: Acceso a la salud de los inmigrantes indocumentados en Chile. Salud Colectiva 13, 507–520. doi: 10.18294/sc.2017.1110
Lock, M. (2000). Encounters with Aging: mythologies of Menopause in Japan and North America. California: University of California Press.
Lube Guizardi, M., López Contreras, E., Valdebenito Tamborino, F., and Nazal Moreno, E. (2019). Dialécticas de la maternidad. Aportaciones al estudio de las desigualdades de género en territorios fronterizos. Estudios Atacameños 63, 81–104. doi: 10.22199/issn.0718-1043-2019-0021
Luxán Serrano, M., and Azpiazu Carballo, J. (2017). Módulo III: Metodología para la implementación de la igualdad. Tema 4: Metodologías de Investigación Feminista. Universidad del País Vasco/Euskal Herriko Unibertsitatea.
Martínez Pereira, M. M. A. (2021). Los cuidados en el embarazo y la lactancia de mujeres migrantes del programa Chile Crece Contigo. Santiago de Chile: Pontificia Universidad Católica De Chile.
Mera, M. J., Martínez-Zelayaa, G., Bilbao, M. Á., and Garrido, A. (2017). Chilenos ante la inmigración: Un estudio de las relaciones entre orientaciones de aculturación, percepción de amenaza y bienestar social en el Gran Concepción. Universitas Psychologica 16, 1–14. doi: 10.11144/Javeriana.upsy16-5.cier
Migración en Chile (2021). INE: 14% de los bebés en Chile nacen de madres extranjeras [Blog]. Available at: https://www.migracionenchile.cl/ine-14-de-los-bebes-en-chile-nacen-de-madres-extranjeras/
MINSAL, FONASA, and Superintendencia de Salud. (2017). Política de Salud y Migrantes Internacionales (T. Pizarro Quevedo, J. Iribarne Wiff, A. Fernández Benítez, V. Rojas Bagnara, C. Padilla Rubio, & J. Novoa Carrasco, Eds.). https://www.minsal.cl/wp-content/uploads/2015/09/2018.01.22.POLITICA-DE-SALUD-DE-MIGRANTES.pdf
Pinto Baleisan, C., and Cisternas Collao, N. (2020). Reflexiones sobre el uso de la interseccionalidad en los estudios migratorios en Chile. Revista Punto Género 14, 49–70. doi: 10.5354/0719-0417.2020.60866
Política de Salud de Migrantes Internacionales (2017). Available at: http://biblioteca.digital.gob.cl/handle/123456789/3633
Posso Quiceno, J. L. (2010). Las transformaciones del significado y la vivencia de la maternidad, en mujeres negras, indígenas y mestizas del suroccidente colombiano. Soc. Econ. 18, 59–84.
Reyes Muñoz, Y. (2023). Aportes de la antropología médica y la enfermería transcultural para el abordaje del fenómeno migratorio en Chile: El caso de enfermeras que trabajan con madres migrantes. Aiken. Revista de Ciencias Sociales y de la Salud 3:1
Reyes Muñoz, Y., and Chatelier, K. (2023). Maternidades haitianas: Diferencias en el proceso de maternaje entre Chile y Haití y la emergencia de la violencia interseccional cuando se omite el factor cultural en el ámbito de la salud. Narrativas Antropológicas 7:7
Reyes Muñoz, Y., Gambetta Tessini, K., Reyes Muñoz, V., and Muñoz-Sánchez, P. (2021). Maternidades negras en chile: Interseccionalidad y salud en mujeres haitianas. Revista Nuestra América 9, 1–13. doi: 10.5281/zenodo.5651360
Reyes Muñoz, V. L., and Reyes Muñoz, Y. T. (2021). Transnacionalidad e interseccionalidad para abordar la localización/posición de migrantes etnoracializados. ODISEA. Revista de. Estudios Migratorios 8:8
Sadler Spencer, M. (2004). “Así me nacieron a mi hija. Aportes antropológicos para el análisis de la atención biomédica del parto” in Nacer, Educar, Sanar: Miradas desde la Antropología del Género. eds. E. M. Sadler, M. E. Acuña, and A. Obach (Catalonia), 15–66.
Sadler Spencer, M. (2016). Etnografías del Control del Nacimiento en el Chile Contemporáneo. Revista Chilena de Antropología 33, 45–57. doi: 10.5354/rca.v0i33.43388
Sibrian, N. (2021). Ajustes emocionales de una gestante e inmigrante en Chile: Estrategias para atenuar el sufrimiento. Athenea Digital. Revista de Pensamiento e Investigación Social 21:2. doi: 10.5565/rev/athenea.2836
Smith-Oka, V. (2009). Unintended consequences: Exploring the tensions between development programs and indigenous women in Mexico in the context of reproductive health. Soc. Sci. Med. 68, 2069–2077.
Van Hollen, C. (2003). Birth on the threshold: childbirth and modernity in South India. California: University of California Press.
Keywords: migrant women, state care benefits, nurses, black motherhood, children’s health
Citation: Reyes Muñoz Y and Reyes Muñoz V (2024) State care services as devices of acceptance to the social body: the case of Afro-descendant migrant mothers in Chile, beneficiaries of the National Child Health Program. Front. Hum. Dyn. 6:1270601. doi: 10.3389/fhumd.2024.1270601
Edited by:
Arek Dakessian, Queen Margaret University, United KingdomReviewed by:
Jozelin María Soto-Alarcón, Autonomous University of the State of Hidalgo, MexicoNilesh Chandrakant Gawde, Tata Institute of Social Sciences, India
Lorena Núñez Carrasco, University of the Witwatersrand, South Africa
Copyright © 2024 Reyes Muñoz and Reyes Muñoz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yafza Reyes Muñoz, eWFmemF0YW1hcmFAZ21haWwuY29t; Vania Reyes Muñoz, dnlyZXllc0B1Yy5jbA==