 Kelsey E. Maslana
Kelsey E. Maslana Grace E. Skogerboe
Grace E. Skogerboe Douglas W. Sborov
Douglas W. Sborov Adriana M. Coletta
Adriana M. Coletta
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Hematol., 21 March 2025
Sec. Blood Cancer
Volume 4 - 2025 | https://doi.org/10.3389/frhem.2025.1550681
This article is part of the Research TopicElevating Supportive Care Measures for Multiple Myeloma in the Modern EraView all articles
Background: Multiple myeloma (MM) is the second most common blood cancer after leukemia in adults. Despite advancements in treatment that have extended survival, MM remains incurable and the cancer and its treatment result in adverse acute, long-term and latent side-effects, necessitating a focus on strategies to attenuate these side-effects and improve quality of life. This narrative review highlights MM patient preferences for exercise and/or diet interventions relative to complete and ongoing interventions to identify gaps and needs for future lifestyle interventions in MM patients aimed at improving MM survivorship care.
Methods: This updated review was completed using a comprehensive search that was conducted using PubMed and ClinicalTrials.gov databases using keywords related to MM, exercise, physical activity, diet, nutrition and patient preferences. Studies involving adults diagnosed with MM were included.
Results: Among published studies, there are five exercise interventions and four diet and nutrition observational studies. The importance of individualized exercise interventions tailored to MM patients’ needs was emphasized. Supervised exercise interventions showed higher adherence and engagement compared to unsupervised interventions. Observational diet/nutrition studies demonstrated that decreased gut microbiome diversity post-transplant is linked to poorer outcomes. Additionally, nutritional status and dietary patterns, such as high-carbohydrate and plant-based diets, can significantly impact clinical outcomes in MM patients, including sustained minimal residual disease negativity. Current clinical trials are primarily focused on feasibility and adherence, with a limited emphasis on long-term outcomes. In ClinicalTrials.gov, there are six ongoing exercise interventions, with an additional seven that are completed with no published results, one suspended trial and one active but not recruiting. Additionally, there are two combined diet and exercise interventions that are currently recruiting, with one active but no longer recruiting. Among diet and nutrition ongoing trials, there are currently two actively recruiting, two completed with no primary paper published and one study that was withdrawn.
Discussion: These findings underscore the need for more comprehensive, long-term and adequately powered studies on the impact of exercise and diet interventions in MM patients. Patient education and empowerment within these trials are crucial for enhancing engagement and adherence to these interventions.
Multiple Myeloma (MM) is categorized as a clonal plasma cell proliferative disorder that can significantly impact bones, kidneys and the body’s ability to produce healthy white blood cells, red blood cells, and platelets. It is the 14th most common cancer type in the United States and the second most prevalent blood cancer after leukemia (1). While the incidence of MM has increased over time (e.g., 5.5 per 100,000 persons in 1992 versus 6.8 in 2022), survival rates have increased an additional eight years due to improved treatment options (2, 3).
Patients with MM often experience adverse cancer- and treatment-related side effects, such as severe fatigue, poor appetite, reduced enjoyment of life, increased pain, and muscle weakness (4, 5). While engagement in regular exercise and physical activity (PA) have been widely recognized for numerous benefits in individuals living with varying cancer types and stages – such as reducing fatigue, anxiety, depression, and improving quality of life and physical function – there remains a gap in the evidence specifically addressing the impact of PA on those diagnosed with MM (6). The general PA guidelines for individuals living with cancer on active treatment or upon completion of treatment includes 90 or 150 minutes per week of moderate intensity aerobic activity, respectively, and two sessions per week of resistance training, targeting every major muscle group (6).
A recent literature review highlighted the potential benefits of using lifestyle modifications, such as regular exercise and healthful dietary strategies, to improve overall health in patients with MM, including enhancements in physical functioning, fatigue, quality of life, and long-term health outcomes (7). However, the review emphasized the need for further research to explore the associations between weight management, sleep, substance use, exercise, and nutrition on disease outcomes such as overall survival, progression-free survival, and non-relapse mortality. Similarly, a second review echoed these findings, noting that seven studies have investigated PA in MM patients, with five of those studies including PA interventions (8). These intervention studies often had small sample sizes (average n = 82) and short intervention durations (average length of 15 weeks). Despite these limitations, the studies consistently found that exercise is both feasible and safe for this population, including those undergoing active treatment such as autologous stem cell transplantation and maintenance therapy. Both reviews stressed the necessity for more comprehensive studies involving larger and more clinically diverse populations, such as those with bone and lytic lesions, to better understand the impact of PA on MM patients.
In addition to engagement in regular exercise, a healthy diet can play a crucial role in supporting cancer patients through treatment and recovery. It can help mitigate treatment side effects, maintain energy levels, and support immune function (9). The American Institute for Cancer Research (AICR) provides comprehensive guidelines for cancer prevention and survivorship, emphasizing the importance of a healthy diet, regular PA, and maintaining a healthy weight (10). There are currently no specific guidelines for MM patients; however, evidence supports that MM patients at higher risk of malnutrition, as measured by the Malnutrition Screening Tool, experience worse survival after stem cell transplant (11) and exacerbated effects of cytokine release syndrome in patients undergoing CAR-T cell therapy (12). Emerging research is also exploring the role of gut microbiome characteristics in MM patients. The gut microbiome, which can be influenced by exercise engagement and dietary intake, plays a significant role in immune function and inflammation (13, 14). Alterations in the gut microbiome, such as lower bacteria diversity compared to healthy controls pre- and post-treatment including transplant, have been linked to the progression of MM and the body’s response to treatment (15–17). Taken together, these findings highlight the importance of consuming a healthy diet during and after MM treatment, with further research evaluating the impact of diet quality and the gut microbiome in this patient population.
Considering this evidence supporting the roles of exercise and diet in MM survivorship care, the purpose of this literature review is to build upon previous reviews by providing an updated synthesis of the latest research on exercise and/or diet for individuals with MM. Additionally, this review will present patient preferences for these types of interventions to further guide future research.
To provide an update to the previous reviews (7, 8), we conducted a comprehensive search of the electronic database PubMed. The search terms used were a combination of keywords including, but not limited to “Multiple Myeloma”, “Myeloma”, “exercise”, “physical activity”, “Diet”, “Diet Therapy”, “Nutrition”, “Gut Microbiome”, “Patient Satisfaction”, “Patience Preference”, “Motivation”. The Medical Subject Headings (MeSH) terms and expansions were applied across the terms where applicable. Additionally, clinical trials registered with ClinicalTrials.gov were found using “Multiple Myeloma” as the disease type and search terms under keywords included “Exercise”, “Diet” and “Nutrition.”
Studies that involved human subjects who were diagnosed with MM that were over the age of 18 years old were considered. Exercise, diet and/or nutrition and a combination of exercise and diet interventional studies, including feasibility studies, and observational studies were included in the search. Dietary and nutrition studies assessing specific diets, nutrient modifications, nutrition timing, quality, dietary patterns, adherence and supplementation were considered. Studies that only included those diagnosed with monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma (SMM) were excluded. Interventional studies that have already been included in past systematic or meta-analysis reviews were not included in the effort to present the most up to date information. Clinical trials listed on ClinicalTrials.gov were reviewed with the same inclusion and exclusion criteria.
All search tasks were completed by a single researcher in October and November 2024 and all returned articles were entered in a shared online resource (University of Utah Box Cloud Storage) for screening and data extraction. Two reviewers independently screened the titles, abstracts and content according to the inclusion and exclusion criteria. The full-text articles were independently reviewed and synthesized by two reviewers within Microsoft Excel. As this is a narrative review, no statistical analyses were performed.
The initial search on PubMed retrieved 501 publications. Despite the structured query, a majority (n=492) of the extracted papers were not relevant to the topic of interest or did not meet the inclusion criteria. This review includes nine different studies for individuals living with MM, comprising of five exercise interventions and four observational studies on diet and/or nutrition (Table 1). Among the five exercise interventions, two were randomized controlled trials, two were single- arm trials, and one was a non-randomized, two-armed, prospective trial where participants were instructed to choose their study arm/intervention for the duration of the trial. Three of these studies implemented individual-based exercise interventions, while two incorporated both individual and group-based exercise, reflecting a mix of social and independent exercise approaches. Regarding diet, two were prospective observational studies, one was a retrospective cohort analysis, and one was a cross-sectional observational study. There were no published studies evaluating exercise and diet together. This review also includes 23 clinical trials registered on ClinicalTrials.gov focusing on exercise and/or diet interventions in individuals with MM, including 15 focused on exercise, five on diet, and three that combined exercise and diet (Table 2).
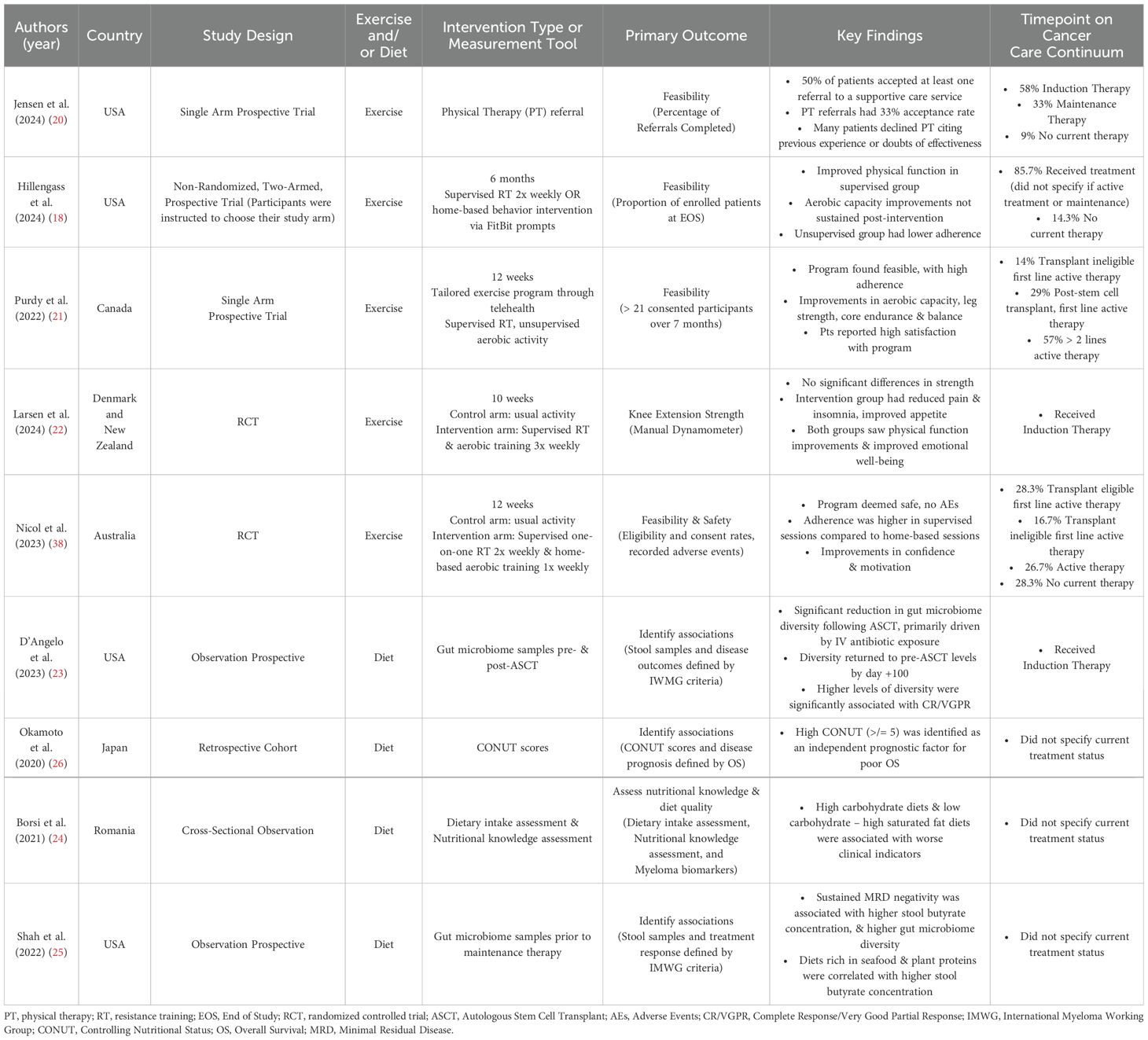
Table 1. Summary of studies examining Exercise/PA and Diet in MM.
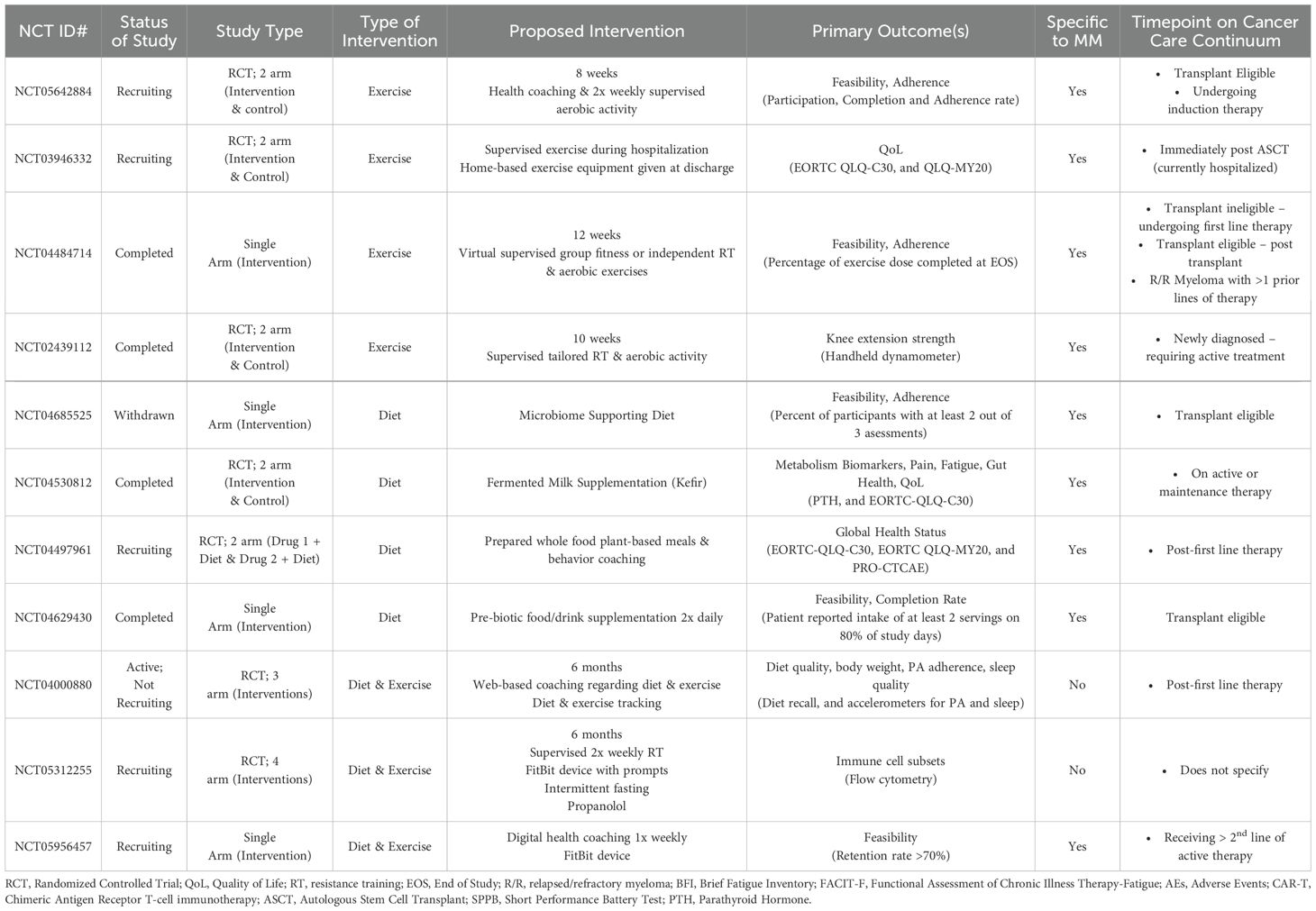
Table 2. Summary of studies registered in ClinicalTrials.Gov.
All interventions emphasize the importance of individualized exercise programs tailored to the needs of MM patients for safety and efficacy, patient engagement, and effectiveness (18–22) (Table 1). Additionally, interventions were implemented across the care continuum for all studies, including those who were newly diagnosed (22, 23), receiving first line or other active treatments (18–22), undergoing maintenance therapy (20), and those under active monitoring (18–20). There is noted variability in exercise adherence and patient engagement, with supervised programs showing higher adherence rates; for example, attendance in all supervised session was 88% whereas attendance at home-based, unsupervised sessions was 45.4% (19). The lack of reliable monitoring in unsupervised programs, such as technical issues with syncing devices or limited data collection, was a significant point of weakness where these challenges contributed to reduced adherence and engagement (18). Among individualized programs, various modalities, including telehealth with remote supervision, were found to be effective for both transplant-eligible and transplant-ineligible patients undergoing first line therapy. This includes patients either completing active therapy or under active surveillance (19). Of the five published exercise interventions, four focused on feasibility as the primary outcome (18–21). These trials demonstrated high feasibility and acceptability, however, Jensen et al. (20), had mixed results regarding acceptability. While 50% of patients accepted at least one referral to a supportive care service (e.g., physical therapy, mental health provider, etc.), only 33% accepted a physical therapy referral, while others shared negative experiences or doubts about effectiveness of this service. Hillengass et al. (18) noted that some benefits, particularly in aerobic endurance, were not sustained post-intervention, suggesting a need for follow-up programs or ongoing support for both patients undergoing treatment and those under active surveillance receiving no treatment. Among studies looking at outcomes beyond feasibility, exercise has been shown to significantly alleviate pain and improve symptoms like insomnia and appetite loss (19, 21, 22).
Findings related to diet and nutrition studies comprised only of observational studies (Table 1). These studies evaluated dietary patterns, gut microbiome, and nutritional status, in relation to important health outcomes in MM. Dietary patterns such as high-carbohydrate diets, including adequate fat and protein intake, or low-carbohydrate and high-saturated fat diets, with adequate protein intake, have been associated with poorer clinical indicators such as hemoglobin, uric acid, albumin, beta-2 microglobulin and percentage of bone marrow plasma cells, among others (24). Furthermore, gut microbiome diversity is significantly decreased following stem cell transplantation, primarily due to the use of intravenous antibiotics. The loss of diversity is primarily driven by the depletion of species from the Clostridia class, Lachnospiraceae family, and genera such as Blautia, Ruminococcus, and Faecalibacterium, all of which are independently linked to better outcomes after allogeneic stem cell transplants and CAR-T therapy (23). Notably, it was also found that the presence of butyrate-producing bacteria in MM patients, following plant-based diets, is linked to sustained minimal residual disease (MRD) negativity in those receiving lenalidomide maintenance therapy (25). Additionally, the Controlling Nutritional Status (CONUT) score, a tool used to assess malnutrition risk and predict adverse outcomes, has shown to be a significant prognostic factor in patients with MM, with lower scores indicating higher risk of malnutrition, poorer survival rates and increased complications, particularly among transplant-eligible patients (26).
Of the 23 clinical trials regarding exercise and/or diet for individuals diagnosed with MM, there are 15 that include exercise only interventions, five studies focused on diet, and three studies that include both an exercise and diet or nutrition component (Table 2). Nine of the listed trials have been marked “Completed”, 10 are categorized as “Recruiting”, while the remaining four are marked as “Withdrawn”, “Active; Not Recruiting”, or “Suspending – COVID-19.” All trials do not include posted results, do not overlap with previously presented material, and are exclusive to MM survivors with the exception of three trials that include other cancer types such as non-Hodgkin lymphoma, localized kidney or ovarian cancer and other hematological malignancies that are eligible for hematopoietic stem cell transplant. Primary study outcomes varied, but the majority of the trials (n=13) focused primarily on feasibility and/or adherence of the proposed intervention. Exercise interventions vary widely among those proposed, including both supervised and unsupervised individual and group exercise environments, as well as both resistance and/or aerobic training components. Diet and nutrition interventions include plant-based meal delivery services, pre-biotic food and drink supplements including fermented milk, as well as diet tracking and health coaching. Of the nutrition-based studies, nine reported that supervised training occurs one-on-one; however, only two studies indicated that the exercise would be individually tailored to the individual, with one study considering bone involvement in its programming.
Ten publications investigated patient preferences for exercise and diet interventions in MM, and of these, seven employed survey or questionnaire-based methodologies (27–33), providing quantitative insights into patient preferences. The remaining three utilized qualitative interview approaches (34–36), offering a deeper understanding of individual experiences and perspectives. This combination of methods allowed for a comprehensive examination of the current literature, highlighting both broad trends and personal insights into patient needs.
When interviewing patients with MM, Hodge et al. (28) found that only 17% of participants were aware of the American Cancer Society’s nutrition and PA guidelines. Furthermore, 56% of participants reported no direction from their oncology team regarding lifestyle recommendations. The review goes on to identify several unmet survivorship needs including access to dietitians for guidance on healthy eating as well as support and knowledge on safe PA and how to engage in PA while living with MM. An online survey of patients with plasma cell disorders, including MM, showed that the majority of respondents (90%) noted that they were interested in learning more about nutrition research and their diagnosis, with only 15% receiving detailed guidance from their oncology team (27). These themes are echoed in exercise and PA focused studies, including in a post exercise intervention qualitative study conducted by Purdy et al. (35) where participants felt safest and most confident when the exercise was tailored to their specific needs. The desire for patients to learn more about which exercises are safe to perform, how exercise can benefit their overall well-being, and accessibility concerns including conducting virtual exercise visits are all salient themes (29–34). Additionally, interest in a dual-component intervention combining both diet and exercise has been shown among those who are undergoing treatment for MM (28).
The purpose of this updated review was to highlight the current and ongoing research in exercise and diet interventions among those with MM and highlight the needs and desires of MM patients regarding these interventions. This review builds on previous work highlighting the potential benefits of individualized exercise programs, and potential dietary modifications. Out of the relevant studies found, common conclusions and limitations can be elicited. Previous reviews of the literature (7, 8, 37, 38) and most recent research regarding exercise and MM emphasized the importance of individualized exercise interventions, specific to the needs of MM patients (19, 20). Exercise programs tailored to the individual have been shown to lead to better adherence, improved safety, and improved patient confidence (18–20). Additionally, supervised exercise programs yield improved adherence compared to unsupervised home exercise programs (18). These outcomes align with patient preferences regarding interventions that will be most beneficial to them not only logistically, but also regarding their confidence in being able to perform PA safely (35).
The lack of available diet intervention research in the MM population speaks to the need of more nutrition-focused research. While current research suggests a promising relationship between diet, gut microbiome health, and MM outcomes, several significant gaps remain (39). There is limited understanding of how to actively modulate the microbiome in MM patients to support post-transplant recovery and disease control (24). Borsi et al. (24) also noted there was a return to pre-transplant microbiome diversity by 100 days post-transplant, which warrants further studies to explore targeted microbiome interventions (e.g., probiotics, dietary fiber, or prebiotics) to prevent diversity loss in the immediate post-transplant period. Although the potential benefits of plant-based diets on clinical outcomes were highlighted (25, 40), no standardized dietary guidelines exist for MM patients. Furthermore, findings on high carbohydrate intake’s adverse effects suggest a need for dietary counseling, especially for patients with advanced disease (24). The role of dietary changes and microbiome composition in enhancing drug efficacy, such as with lenalidomide maintenance, is still not well understood; it was found that butyrate-producing bacteria may support sustained MRD negativity (25), yet more research is needed to clarify these interactions to guide optimized dietary recommendations. Additionally, as noted by Borsi et al. (24), MM patients often lack adequate knowledge of their nutritional needs, emphasizing the need for comprehensive dietary education programs and/or counseling that deliver clear, evidence-based guidance on nutrition and microbiome health, both during and after treatment, to help patients make informed dietary choices that may improve treatment outcomes and quality of life. This lack of knowledge correlates with patients expressed desire to learn more about how to maximize their diet to help attenuate treatment side-effects and improve quality of life during their cancer journey (27, 28).
Patient preferences can play a crucial role in the success of PA and diet interventions for MM patients. As noted, studies have shown that MM patients often prefer individualized exercise programs that are tailored to their specific needs, including knowledge regarding safe exercises to complete with bone involvement. Despite this, many ongoing studies do not fully incorporate these preferences into their design. For instance, while supervised exercise programs have been shown to improve adherence, many studies are relying on unsupervised home-based programs that may not provide the necessary support or motivation for patients. Additionally, there is strong interest among patients in understanding how dietary modifications can support them during treatment, and as part of their overall health. The apparent disconnect between patient preferences and interventions highlights the need for more patient-centered research approaches that prioritize the specific desires and needs of MM patients to facilitate intervention adherence and sustained engagement in the promoted lifestyle behavior of the intervention.
One significant gap in the literature shared by both exercise and diet interventions, is the lack of trials with efficacy of the intervention or effectiveness of the program as the primary outcome. Most trials focused on feasibility of the diet and/or exercise intervention/program as the primary outcome. It is established that exercise and diet interventions and programs are feasible in multiple myeloma across the cancer care continuum, notably during induction and maintenance therapy. Moving forward, more work is needed evaluating the efficacy or effectiveness of such interventions and programs on relevant health outcomes for multiple myeloma patients. Moreover, longer-term interventions (i.e., > 12 weeks) are needed, especially those focusing on the impact of specific dietary patterns, such as plant-based or low-carbohydrate diets, are required to determine if these diets provide lasting benefits. Including studies exclusive to the post-HSCT peri-transplant recovery period, with interventions that explore this time in the cancer care continuum and beyond, is warranted. Additionally, there is a notable lack of studies that explore the associated physiological mechanisms that may be associated with the benefits of exercise and diet interventions on specific outcomes relevant to multiple myeloma patients.
This narrative review highlights the critical need for more comprehensive research on the impact of PA and diet interventions in patients with MM, as well as research that takes into consideration patient’s desires. The scarcity of research including diet and/or nutrition interventions, particularly regarding the relationship between the gut microbiome and health outcomes in MM patients, highlights the urgent need for future studies in this area.
Although this narrative review contributes to the field by synthesizing the most recent exercise and diet intervention studies published, as well as ongoing trials, including patient preferences, it is not without its limitations. First, the search was specific to only PubMed and ClinicalTrials.gov, potentially excluding relevant studies not indexed in the searched databases. Additionally, information regarding duration, frequency and mode of exercise was not consistently reported among studies registered in ClinicalTrials.gov.
In conclusion, significant gaps remain, including the lack of efficacy studies, dietary interventions to improve health outcomes, and interventions that consider the preferences of patients with MM. By developing integrated lifestyle interventions that align with patient preferences and needs, it is possible to improve adherence and engagement, as well as address underlying nutritional or physical function needs that could lead to improved quality of life and survival. Through a patient-centered approach, we can better support individuals with MM in managing their condition and improving their overall health.
KM: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. GS: Investigation, Methodology, Writing – original draft, Writing – review & editing. DS: Writing – review & editing. AC: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cancer stat facts: multiple myeloma . Available online at: https://seer.cancer.gov/statfacts/html/mulmy.html (Accessed September 23, 2024).
2. Puertas B, González-Calle V, Sobejano-Fuertes E, Escalante F, Queizán JA, Bárez A, et al. Novel agents as main drivers for continued improvement in survival in multiple myeloma. Cancers. (2023) 15:1558. doi: 10.3390/cancers15051558
3. Binder M, Nandakumar B, Rajkumar SV, Kapoor P, Buadi FK, Dingli D, et al. Mortality trends in multiple myeloma after the introduction of novel therapies in the United States. Leukemia. (2022) 36:801–8. doi: 10.1038/s41375-021-01453-5
4. Kamal M, Wang XS, Shi Q, Zyczynski TM, Davis C, Williams LA, et al. Symptom burden and its functional impact in patients with “symptomatic” relapsed or refractory multiple myeloma. Supportive Care Cancer. (2021) 29:467–75. doi: 10.1007/s00520-020-05493-y
5. Brazauskas R, Flynn K, Krishnan A, Landau H, Giralt S, Pasquini MC, et al. Symptom clusters and their impact on quality of life in multiple myeloma survivors: Secondary analysis of BMT CTN 0702 trial. Br J Hematol. (2024) 204:1429–38. doi: 10.1111/bjh.v204.4
6. Campbell KL, Winters-Stone K, Wiskemann J, May AM, Schwartz AL, Courneya KS, et al. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci sports exercise. (2019) 51:2375. doi: 10.1249/MSS.0000000000002116
7. Shapiro YN, Peppercorn JM, Yee AJ, Branagan AR, Raje NS, Donnell EKO. Lifestyle considerations in multiple myeloma. Blood Cancer J. (2021) 11:172. doi: 10.1038/s41408-021-00560-x
8. Hillengass M, Joseph J, Mccarthy J, Hillengass J. Physical activity in multiple myeloma: a review of the current literature. J Advanced Practitioner Oncol. (2023) 14:153. doi: 10.6004/jadpro.2023.14.2.5
9. Benefits of good nutrition during cancer treatment . Available online at: https://www.cancer.org/cancer/survivorship/coping/nutrition/benefits.html (Accessed October 9, 2024).
10. How to prevent cancer: 10 recommendations . Available online at: https://www.aicr.org/cancer-prevention/how-to-prevent-cancer/ (Accessed October 9, 2024).
11. Kuypers J, Simmance N, Quach H, Hastie K, Kiss N. Nutrition support use and clinical outcomes in patients with multiple myeloma undergoing autologous stem cell transplant. Supportive Care Cancer. (2022) 30:9341–50. doi: 10.1007/s00520-022-07358-y
12. Ding S, Cai L, Jin A, Zhou X, Yan J, Wang L, et al. Nutritional status alterations after chimeric antigen receptor T cell therapy in patients with hematological Malignancies: a retrospective study. Supportive Care Cancer. (2022) 30:3321–7. doi: 10.1007/s00520-021-06639-2
13. Dziewiecka H, Buttar HS, Kasperska A, Ostapiuk–Karolczuk J, Domagalska M, Cichoń J, et al. Physical activity induced alterations of gut microbiota in humans: a systematic review. BMC Sports Science Med Rehabil. (2022) 14:122. doi: 10.1186/s13102-022-00513-2
14. Ross FC, Patangia D, Grimaud G, Lavelle A, Dempsey EM, Ross RP, et al. The interplay between diet and the gut microbiome: implications for health and disease. Nat Rev Microbiol. (2024) 22:671–86. doi: 10.1038/s41579-024-01068-4
15. Jian X, Zhu Y, Ouyang J, Wang Y, Lei Q, Xia J, et al. Alterations of gut microbiome accelerate multiple myeloma progression by increasing the relative abundances of nitrogen-recycling bacteria. Microbiome. (2020) 8:74. doi: 10.1186/s40168-020-00854-5
16. Brevi A, Cogrossi LL, Lorenzoni M, Mattorre B, Bellone M. The insider: impact of the gut microbiota on cancer immunity and response to therapies in multiple myeloma. Front Immunol. (2022) 13. doi: 10.3389/fimmu.2022.845422
17. Kanellos PT, Baxevanis GK, Tentolouris A, Gavriatopoulou M, Ntanasis-Stathopoulos I. The role of nutrition and gut microbiome in the progression of multiple myeloma and its precursor disease. Front Oncol. (2024) 14. doi: 10.3389/fonc.2024.1461128
18. Hillengass J, Hillengass M, Joseph JM, Attwood K, Cannioto R, Jacobson H, et al. Effects on the physical functioning of two exercise interventions in patients with multiple myeloma: A pilot feasibility study. Cancers. (2024) 16:1774. doi: 10.3390/cancers16091774
19. Nicol JL, Cunningham BJ, Woodrow C, Adlard KN, Papinczak ZE, Spence RR, et al. Safety, feasibility, and acceptability of a multisite individualized exercise intervention for people with multiple myeloma. Med Sci Sports Exerc. (2023) 55:2214–27. doi: 10.1249/MSS.0000000000003267
20. Jensen CE, Deal AM, Nyrop KA, Logan M, Mangieri NJ, Strayhorn MD, et al. Geriatric assessment-guided interventions for older adults with multiple myeloma: A feasibility and acceptability study. J Geriatr Oncol. (2024) 15:101680. doi: 10.1016/j.jgo.2023.101680
21. Purdy GM, Venner CP, Tandon P, McNeely ML. Feasibility of a tailored and virtually supported home exercise program for people with multiple myeloma using a novel eHealth application. Digit Health. (2022) 8:20552076221129066. doi: 10.1177/20552076221129066
22. Larsen RF, Jarden M, Minet LR, Frølund UC, Hermann AP, Breum L, et al. Exercise in newly diagnosed patients with multiple myeloma: A randomized controlled trial of effects on physical function, physical activity, lean body mass, bone mineral density, pain, and quality of life. Eur J Hematology. (2024) 113:298–309. doi: 10.1111/ejh.v113.3
23. D’Angelo C, Sudakaran S, Asimakopoulos F, Hematti P, El-Gamal D, Safdar N, et al. Perturbation of the gut microbiome and association with outcomes following autologous stem cell transplantation in patients with multiple myeloma. Leukemia Lymphoma. (2023) 64:87–97. doi: 10.1080/10428194.2022.2131410
24. Borsi E, Serban CL, Potre C, Potre O, Putnoky S, Samfireag M, et al. High carbohydrate diet is associated with severe clinical indicators, but not with nutrition knowledge score in patients with multiple myeloma. Int J Environ Res Public Health. (2021) 18:5444. doi: 10.3390/ijerph18105444
25. Shah UA, Maclachlan KH, Derkach A, Salcedo M, Barnett K, Caple J, et al. Sustained minimal residual disease negativity in multiple myeloma is associated with stool butyrate and healthier plant-based diets. Clin Cancer Res. (2022) 28:5149–55. doi: 10.1158/1078-0432.CCR-22-0723
26. Okamoto S, Ureshino H, Kidoguchi K, Kusaba K, Kizuka-Sano H, Sano H, et al. Clinical impact of the CONUT score in patients with multiple myeloma. Ann Hematology. (2020) 99:113–9. doi: 10.1007/s00277-019-03844-2
27. Malik MA, Sweeney NW, Jafri M, Derkach A, Chmielewski C, Adintori PA, et al. Nutrition perceptions, needs and practices among patients with plasma cell disorders. Blood Cancer J. (2022) 12:70. doi: 10.1038/s41408-022-00666-w
28. Hodge A, Sheean P, O’Connor P, Tyler K, Kerschner A, Williams A, et al. Exploring health behaviors and the feasibility of a lifestyle intervention for patients with multiple myeloma. Supportive Care Cancer. (2022) 30:9771–9. doi: 10.1007/s00520-022-07385-9
29. Nicol JL, Woodrow C, Burton NW, Mollee P, Nicol AJ, Hill MM, et al. Physical activity in people with multiple myeloma: associated factors and exercise program preferences. J Clin Med. (2020) 9:3277. doi: 10.3390/jcm9103277
30. Rader J, Ihorst G, Moller MD, Pahl A, Greil C, Dreyling E, et al. Physical activity and exercise motivation of multiple myeloma patients: a prospective cross-sectional study. Oncologist. (2024) 29:e1336–e46. doi: 10.1093/oncolo/oyae111
31. Lecat CS, McCourt O, Land J, Yong K, Fisher A. Multiple myeloma and physical activity. BMC Res notes. (2021) 14:171. doi: 10.1186/s13104-021-05591-y
32. Kuehl R, Koeppel M, Goldschmidt H, Maatouk I, Rosenberger F, Wiskemann J. Physical activity-related health competence and symptom burden for exercise prescription in patients with multiple myeloma: a latent profile analysis. Ann Hematology. (2023) 102:3091–102. doi: 10.1007/s00277-023-05326-y
33. Purdy GM, Nanad R, Ternes L, Dolgoy ND, Sellar CM, Francis G, et al. Exercise preferences, barriers, and facilitators of individuals with cancer undergoing chemotherapy before stem cell transplantation: A mixed-methods study. Cancer Nursing. (2024) 47:E287–E97. doi: 10.1097/NCC.0000000000001240
34. Land J, Hackett J, Sidhu G, Heinrich M, McCourt O, Yong KL, et al. Myeloma patients’ experiences of a supervised physical activity program: a qualitative study. Supportive Care cancer. (2022) 30:6273–86. doi: 10.1007/s00520-022-07062-x
35. Purdy GM, Sobierajski FM, Al Onazi MM, Effa CJ, Venner CP, Tandon P, et al. Exploring participant perceptions of a virtually supported home exercise program for people with multiple myeloma using a novel eHealth application: a qualitative study. Supportive Care Cancer. (2023) 31:298. doi: 10.1007/s00520-023-07762-y
36. McCourt O, Fisher A, Land J, Ramdharry G, Roberts AL, Bekris G, et al. What I wanted to do was build myself back up and prepare”: qualitative findings from the PERCEPT trial of prehabilitation during autologous stem cell transplantation in myeloma. BMC Cancer. (2023) 23:348. doi: 10.1186/s12885-023-10799-1
37. Smith L, McCourt O, Henrich M, Paton B, Yong K, Wardle J, et al. Multiple myeloma and physical activity: a scoping review. BMJ Open. (2015) 5:e009576. doi: 10.1136/bmjopen-2015-009576
38. Nicol JL, Chong JE, McQuilten ZK, Mollee P, Hill MM, Skinner TL. Safety, feasibility, and efficacy of exercise interventions for people with multiple myeloma: A systematic review. Clin Lymphoma Myeloma Leukemia. (2023) 23:86–96. doi: 10.1016/j.clml.2022.10.003
39. Shah UA, Parikh R, Castro F, Bellone M, Lesokhin AM. Dietary and microbiome evidence in multiple myeloma and other plasma cell disorders. Leukemia. (2023) 37:964–80. doi: 10.1038/s41375-023-01874-4
Keywords: multiple myeloma, exercise, diet and nutrition, gut microbiome, patient preferences
Citation: Maslana KE, Skogerboe GE, Sborov DW and Coletta AM (2025) Exercise and diet studies among patients living with multiple myeloma: current evidence and considerations of patient preferences. Front. Hematol. 4:1550681. doi: 10.3389/frhem.2025.1550681
Received: 23 December 2024; Accepted: 06 March 2025;
Published: 21 March 2025.
Edited by:
Bhavana Bhatnagar, West Virginia University, United StatesReviewed by:
Natalia Neparidze, Yale University, United StatesCopyright © 2025 Maslana, Skogerboe, Sborov and Coletta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana M. Coletta, QWRyaWFuYS5jb2xldHRhQGhjaS51dGFoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.