 Amalia Domingo-González1*
Amalia Domingo-González1* Rafael Alonso Fernández2
Rafael Alonso Fernández2 Ana Jiménez3
Ana Jiménez3 Teresa De Soto Álvarez4Ana Lerma-Verdejo5Virginia Pradillo6Gonzalo Benzo Callejo7Jose Sánchez-Pina2Elena Landete8Alberto Velasco-Valdazo9Marina Menéndez-Cuevas9Mónica María López Riñón10Andrés Ramírez-López11María-Jesús Blanchard3Elham Askari1
Teresa De Soto Álvarez4Ana Lerma-Verdejo5Virginia Pradillo6Gonzalo Benzo Callejo7Jose Sánchez-Pina2Elena Landete8Alberto Velasco-Valdazo9Marina Menéndez-Cuevas9Mónica María López Riñón10Andrés Ramírez-López11María-Jesús Blanchard3Elham Askari1- 1Hematology Department, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
- 2Hematology Department, Hospital Universitario 12 de Octubre, Madrid, Spain
- 3Hematology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 4Hematology Department, Hospital Universitario La Paz, Madrid, Spain
- 5Hematology Department, Hospital General Nuestra Señora del Prado, Toledo, Spain
- 6Hematology Department, Hospital Universitario Quirón Pozuelo, Madrid, Spain
- 7Hematology Department, Hospital Universitario La Princesa, Madrid, Spain
- 8Hematology Department, Hospital Universitario Infanta Leonor, Madrid, Spain
- 9Hematology Department, Hospital Rey Juan Carlos, Madrid, Spain
- 10Hematology Department, Hospital General de Tomelloso, Ciudad Real, Spain
- 11Hematology Department, Hospital General La Mancha Centro, Ciudad Real, Spain
Introduction: The regimen with daratumumab, bortezomib, melphalan, and prednisone (D-VMP) is one of the recommended treatments for newly diagnosed multiple myeloma (NDMM) non-transplant eligible due to the results described in the ALCYONE trial. However, real-life outcomes with this regimen are limited. This study assesses the real-life effectiveness and safety of this regimen.
Methods: We retrospectively analyzed the data on efficacy, safety, and survival parameters of D-VMP regimen in 112 patients with NDMM not eligible for autologous stem-cell transplantation with attention to the effect of age, R2-ISS, high-risk cytogenetic abnormalities (CA), and depth of response.
Results: Patients aged ≥75 years constituted 70% of our cohort. Fifty-two percent had R2-ISS 3-4, and 60% had high-risk CA. Twenty-three percent of patients would have been excluded from the ALCYONE trial. After a median follow-up of 31.4 months, all patients had completed induction, with a median number of cycles of 9 (IQR 6-9). The overall response rate was 95%, and 72% achieved very good partial response (VGPR) or better. The median progression-free survival (PFS) was 41.5 (95% CI, 34.3 to NE), and the median overall survival (OS) was not reached. The most frequent adverse event (AE) was neuropathy (27%), followed by gastrointestinal symptoms (13%) and hematological AE (10%). Age did not negatively impact survival outcomes. Patients with ≥2 high-risk CA or those who achieved <VGPR had a worse OS (p= 0.026 and p= 0.030). After performing multivariate analysis, we didn’t find statistically significant prognostic factors for PFS or OS.
Discussion: In real-life practice, the D-VMP combination showed a similar efficacy and safety profile to those reported in the ALCYONE and OCTANS trials.
Introduction
Multiple myeloma (MM) is a malignant hematological disease characterized by a clonal proliferation of plasma cells, causing bone lesions, renal failure, anemia, and hypercalcemia. MM accounts for ∼10% of all hematologic cancers and mainly affects elderly people (median age at diagnosis 70 years) (1). The treatment paradigm for MM has been considerably evolved over the last decades, and substantial improvement in outcomes has been reported (2). Although patients over 65-70 years old usually do not benefit from autologous stem-cell transplantation (ASCT) due to increased morbimortality (3, 4), the growing improvement in life expectancy and the amelioration in the fragility of older patients, has led to more and more of them benefiting from treatment (5, 6). However, the impact of therapy has been less notable in this group of patients, especially in those older than 75 years old (7). Currently, induction therapy with a multi-agents combination followed by continuous therapy has become a standard of care for newly diagnosed MM (NDMM), with several phase 3 trials showing superior survival benefits using triplet or quadruplet induction regimens (8, 9, 10, 11, 12). ALCYONE clinical trial demonstrated the benefit of adding daratumumab to the previous standard regimen of bortezomib, melphalan, and prednisone (VMP) and proved to be an effective and safe treatment for patients with NDMM ineligible for ASCT (13). These findings were later confirmed by the primary analysis of the phase 3 OCTANS trial (12). Currently, this regimen is one of the recommended treatments for NDMM non-transplant candidates along with others such as bortezomib, lenalidomide, dexamethasone (VRD) and daratumumab, lenalidomide, dexamethasone (DRD) (3, 14). However, effectiveness, tolerability, and adherence to novel regimens in day-to-day clinical practice often differ from the data described in clinical trials (15, 16, 17, 18). Herein, we report the real-world data of the effectiveness and safety profile of Daratumumab-VMP (DVMP) therapy in NDMM non-ASCT candidates from 11 centers in Spain, in hopes of providing additional data to help therapeutic decision-making. To the best of our knowledge, this is the first study addressing this regimen in real life.
Patients and methods
This is a multi-centric, retrospective, and observational study. It included 112 adults with NDMM ineligible for ASCT who received first-line treatment with D-VMP. They were identified through the hospital pharmacy registry. Patients were treated at 11 different medical centers from the Spanish Myeloma Group from June 2019 to February 2024. For inclusion in the study, patients had to be diagnosed with MM by the 2014 criteria of the International Myeloma Working Group (IMWG) (1) and to receive at least > 1 dose of treatment. The records including demographics, disease characteristics, treatment response, treatment duration, adverse events (AE), and survival outcome were retrieved and analyzed from each hospital’s medical records. High-risk cytogenetic abnormalities (CA) were detected locally by fluorescence in situ hybridization (FISH) or metaphase cytogenetics and included del(17p), t(4;14), t(14;16), gain/amp(1q), or del(1p). The minimum percentage of cells to count as high-risk cytogenetic was 20%. The primary endpoint was progression-free survival (PFS). The secondary endpoints were overall response rate (ORR), very good partial response (VGPR) rate, complete response (CR) rate, negative status for measurable residual disease (MRD), time to response, disease progression on next-line treatment (PFS2), overall survival (OS), and safety. PFS was defined as the time interval from the start of treatment to either disease progression or death. PFS2 was defined as the time interval from the start of treatment to disease progression on next-line treatment or death. OS was defined as the time from the start of treatment to the date of death, or to the date of censoring at the last time the subject was known to be alive. Response and progression were assessed by the investigators according to the 2016 consensus criteria of the International Myeloma Working Group (19), but due to the advanced age of our cohort and the retrospective nature of the study bone marrow aspiration was not required to confirm a CR. Complete response was considered when negative immunofixation on the serum and urine and the disappearance of any soft tissue plasmacytomas were obtained. The overall response rate included partial response or better. Disease assessments were done at the end of each cycle. Minimal residual disease (MRD) in bone marrow was assessed using flow cytometry at a minimum threshold of 1 tumor cell per 104 white cells. Minimal residual disease negativity by imaging was defined as the disappearance of every area of increased tracer uptake found at baseline or a preceding PET/CT or a decrease to less mediastinal blood pool SUV or a decrease to less than surrounding normal tissue (19). The severity of adverse events was evaluated according to version 5.0 of the National Cancer Institute’s (NCI) Common Terminology Criteria for Adverse Events (CTCAE) and dose adjustments were performed according to manufacturer’s guidelines. Dose adjustments consisted of dose reduction and temporary drug interruptions. The frailty status was defined by investigator criteria in each center.
Statistical analysis
Statistical analysis was conducted using R version 4.3.1 (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were used to describe baseline characteristics, response, and AE data. The Wilcoxon signed-rank test was used to compare median values with a reference value. The Z test for a proportion was used to compare a proportion with a reference value. The Chi-square test was used to compare two frequency distributions. Survival curves were estimated using the Kaplan-Meier method and were compared with the log-rank test. Regression models were carried out to estimate the hazard ratio and its 95% confidence interval. Significance was set at a two-sided value of P <0.05. The study was approved by the institutional ethics committee (CEIm-FJD) and conducted by the 1964 Helsinki Declaration and its later amendments (EO058-24_FJD).
Results
Patients
The analysis includes a total of 112 patients newly diagnosed with symptomatic MM who were not eligible for ASCT and were treated with D-VMP as first-line from 11 different sites. Only one patient was excluded due to < 2 doses of treatment. The patient had moderate chronic obstructive pulmonary disease (COPD) and suspended therapy due to a grade 3 infusion reaction to daratumumab. Table 1 shows the patients’ baseline demographic and clinical characteristics. The median age at diagnosis was 77 years old (range, 65-88). Seventy-eight patients (70%) were older than 74 years. Eighty-seven out of 112 (78%) patients had their fragility assessed before treatment. Sixty percent were considered fit according to the investigator assessment, 26% intermediate-fit, and 14% frail. Ninety-five percent of patients were not eligible for ASCT due to age ≥70 years, and 5% due to age ≥65 years and comorbidities. Eight patients (7%) had an Eastern Cooperative Oncology Group (ECOG) performance status of ≥3 at diagnosis, seven patients (6%) had anemia <7.5 g/dL, sixteen patients (14%) had a creatinine level >2 mg/dL, eight (7%) required in-hospital dialysis, and three (3%) had hypercalcemia >14 mg/dL. Regarding the type of imaging test at diagnosis, 62% of patients underwent PET-CT, 15% CT scan, 21% magnetic resonance, and 2% X-rays. In 69% of cases, the image test showed bone involvement. Sixty percent of patients had a high-risk CA, 13% had a high-risk CA included in R-ISS, and 12% had more than one high-risk CA. Seven percent of patients initiated treatment because of bone marrow plasma cells of ≥60% or serum-free light chain ratio of ≥100 without organ damage. Table 2 shows the prognosis index at diagnosis.
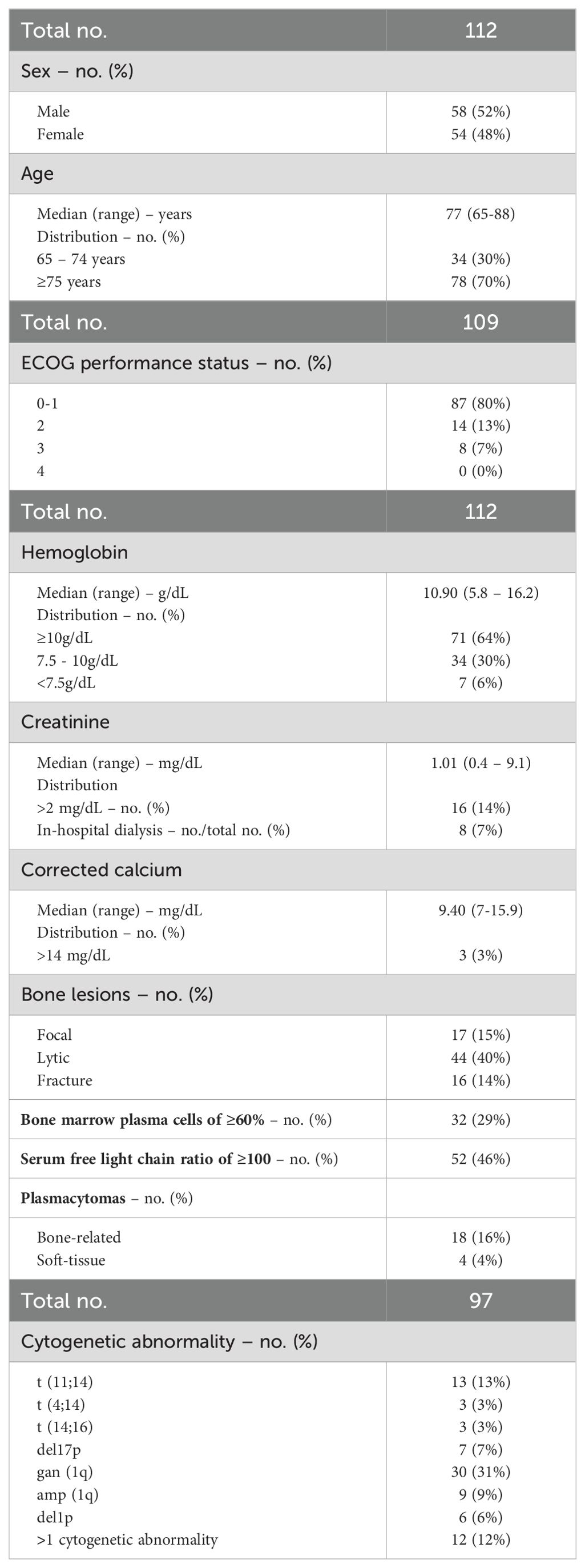
Table 1. Demographic and clinical characteristics at diagnosis.
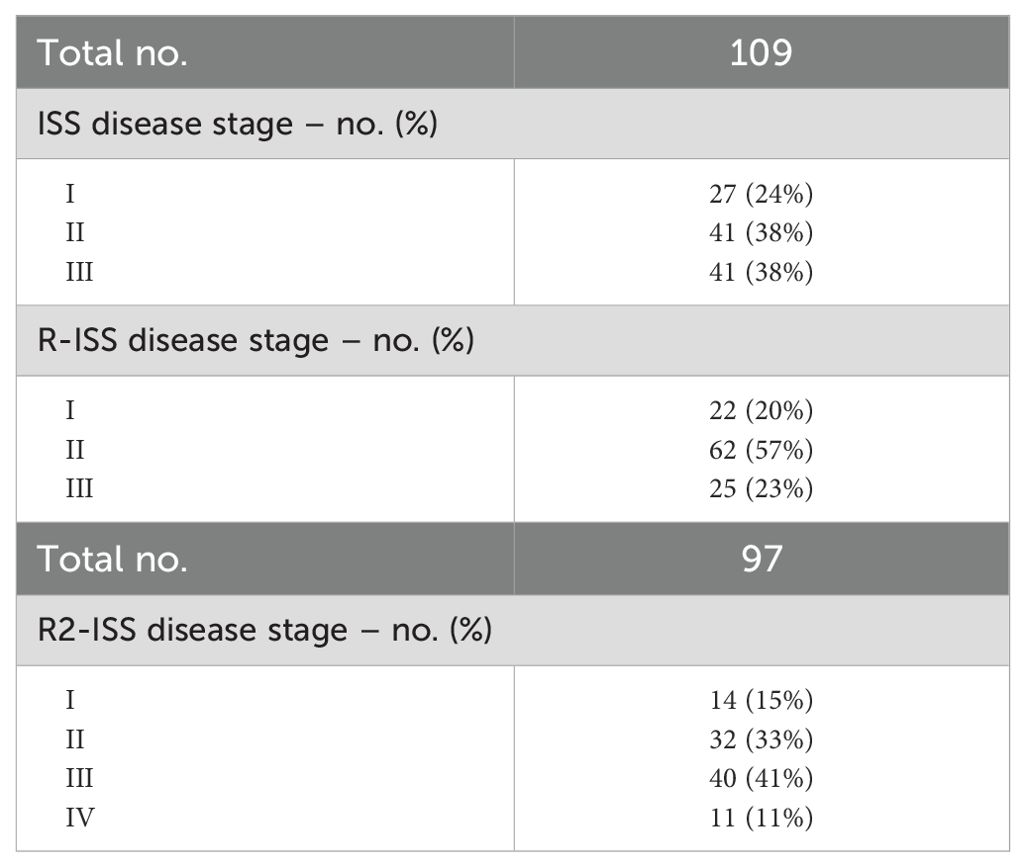
Table 2. Prognosis index at diagnosis.
Treatment exposure, response, and outcome
At a median follow-up of 31.4 months, all patients had completed induction, with a median number of cycles of 9 (IQR 6-9). Thirty-seven patients (33%) received continuous treatment with daratumumab and bortezomib to reach more sustained responses at the discretion of the treating physician. During the extended phase of treatment, bortezomib was administered biweekly throughout treatment until disease progression or intolerance. The ORR was 95% and 72% of patients achieved ≥ VGPR, 23% VGPR, and 49% CR. The median time to any type of response was 1.1 months (IQR 0.7-1.6) and the median time to best response was 7 months (IQR 3.2-14.9). Data about response to treatment including MRD is shown in Table 3. Among patients achieving ≥ VGPR, 50% had MRD assessment in bone marrow, while 58% underwent MRD evaluation by PET-CT. Of those patients with MRD assessment in bone marrow, 59% were MRD-negative. Among them, 13 patients (56%) were subsequently re-evaluated, and 7 sustained MRD negativity at 6 (1), 12 (3), 18 (2), and 30 (1) months. Twenty-eight out of 48 patients (58%) with MRD evaluation by PET-CT were MRD-negative. In the overall population, the median PFS was 41.5 (95% CI, 34.3 to NE) and the median OS was not reached (Figure 1). Those patients with ≥2 high-risk CA had a median PFS of 22.2 months (95% CI, 12.2 to NE) and a median OS of 43.3 months (95% CI, 24.5 to NE). Patients who achieved < VGPR had a median PFS of 42 months (95% CI, 21.6 - NE) and a median OS of 43.3 months (95% CI, 42.0 - NE). Age ≥ 75 did not negatively impact PFS, OS, or PFS2. Combined continuous therapy, ≤1 high-risk CA, and achieving ≥VGPR had a positive impact on OS, whereas R2-ISS 1-2 and achieving ≥VGPR had a positive impact on PFS2. Survival analysis is displayed in Figure 2. In a multivariate analysis including age, R2-ISS, high-risk CA, and depth of response the only statistically significant prognosis factor related to survival were the depth of response (≥VGPR) and R2-ISS (1-2), which were related to a better PFS2 (HR 5.44, CI 95% 2.0-14.9, p=0.001 and HR 4.06, CI 95% 1.29-12.8, p=0.017 respectively). A total of 35 patients (33%) experienced relapse. Nineteen patients (54%) had a clinical relapse and 16 (47%) had a biological one. Twenty-eight patients (80%) received subsequent therapy, 40% of them had a biochemical relapse, and 60% had a progression with end-organ damage. The most frequent subsequent therapy was carfilzomib-lenalidomide-dexamethasone (67%), followed by lenalidomide-dexamethasone (22%).
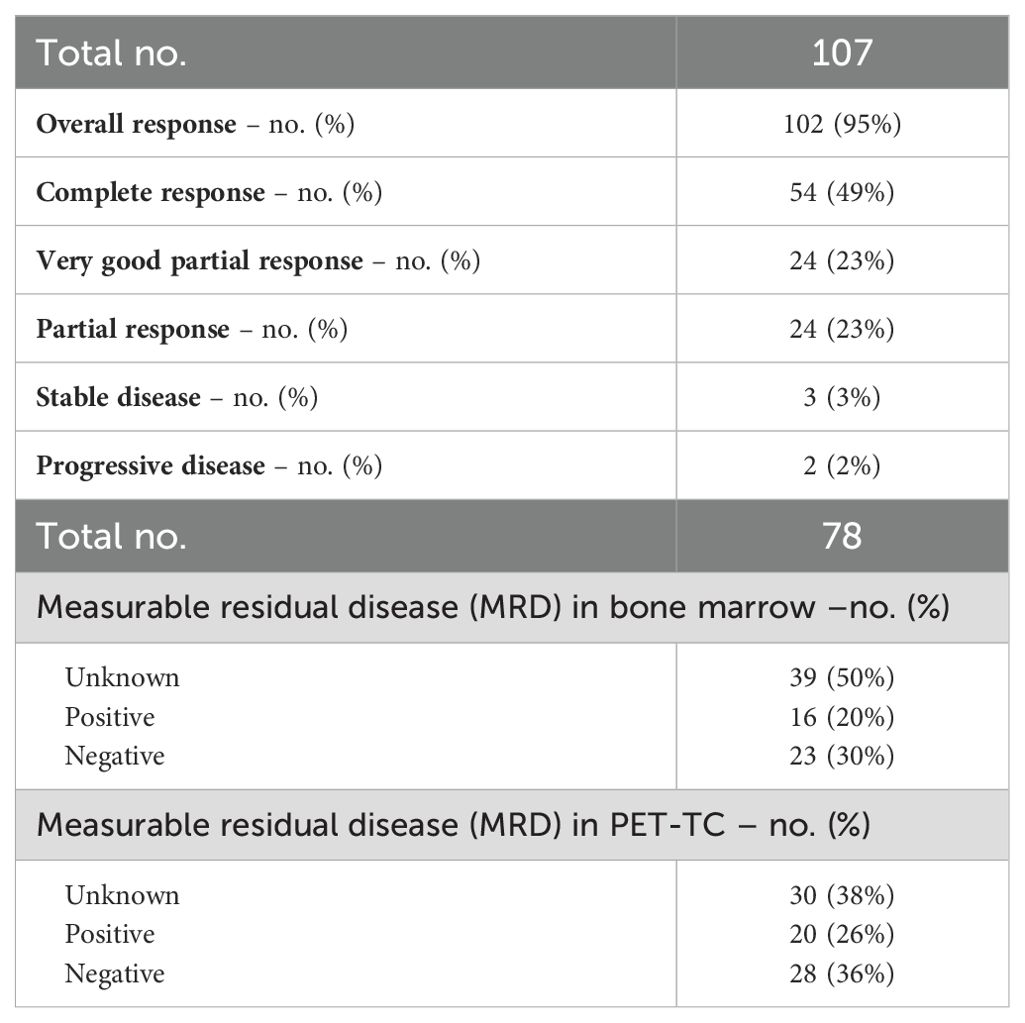
Table 3. Summary of best overall responses.
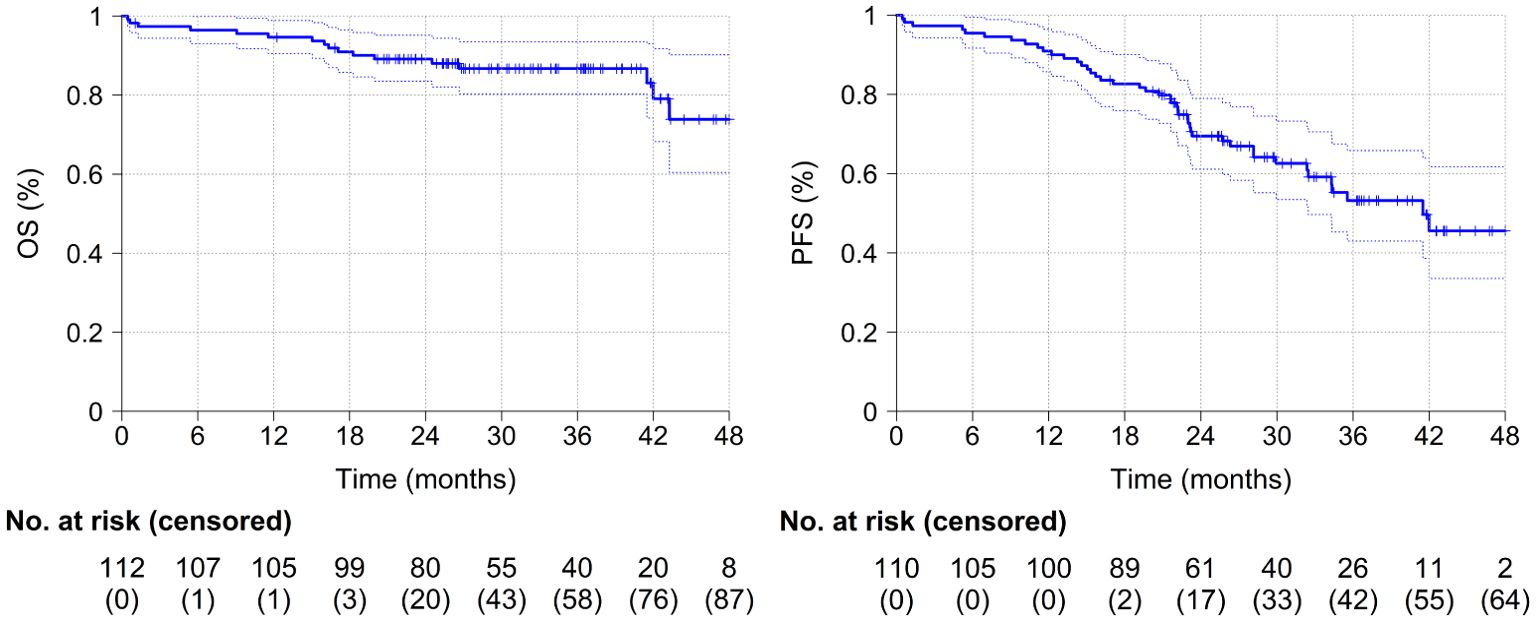
Figure 1. Survival analyses of the cohort.
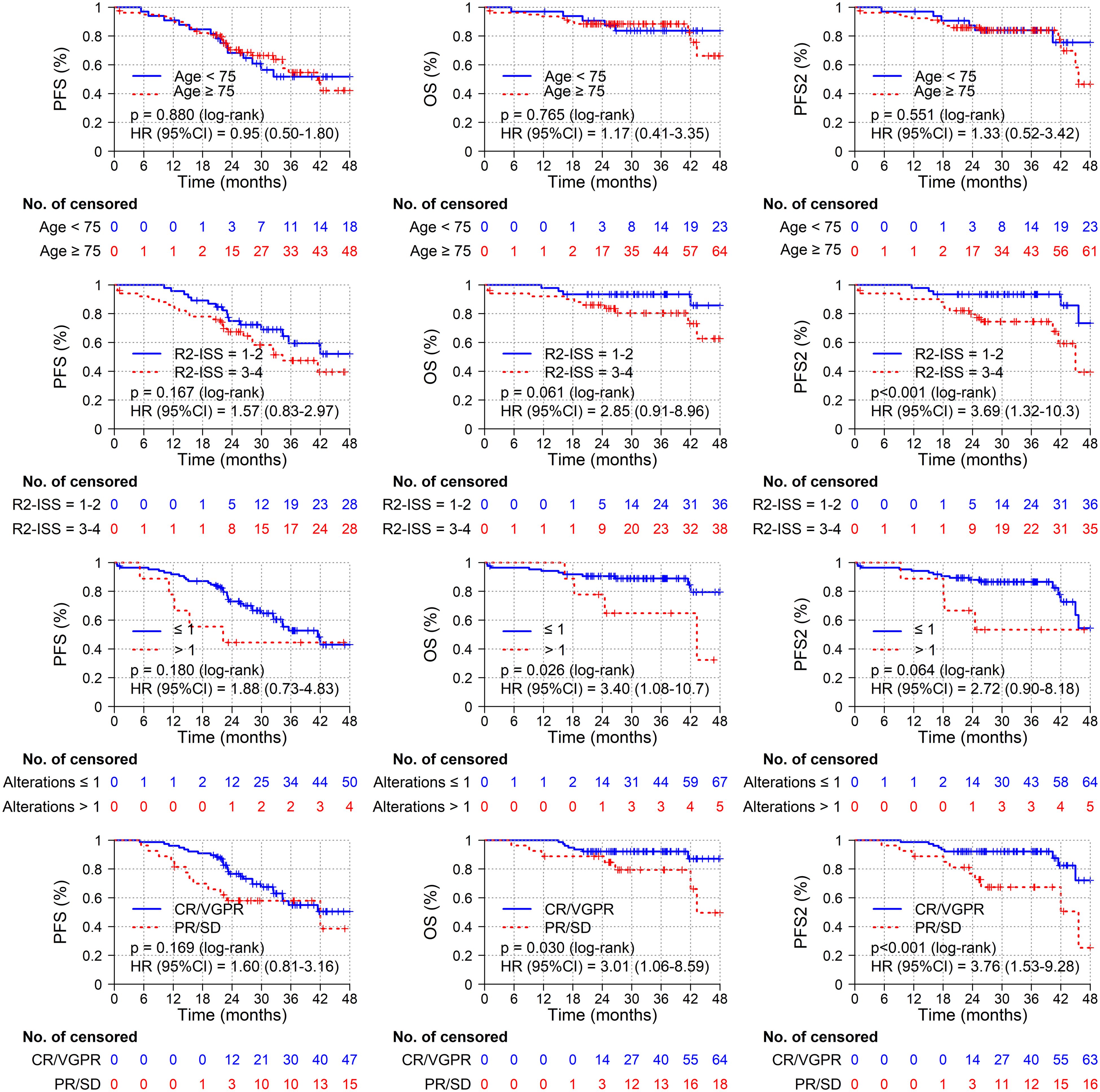
Figure 2. Survival analyses according to age (<75 years vs ≥75 years), R2-ISS (1-2 vs 3-4), number of high-risk cytogenetic abnormalities (0-1 vs >1) and depth of response (CR/VGPR vs PR/SD).
Safety profile
Sixty-three patients of our cohort (56%) received ≥ 9 cycles of induction. The causes for not completing induction therapy were toxicity (82%), disease progression (6%), death (6%), and other causes (6%). During the first 9 cycles of induction therapy, 67 patients (60%) had treatment adjusted due to treatment-emergent AE. Forty-five percent of patients had bortezomib dose adjusted, 28% melphalan, and 9% prednisone. Those who continued bortezomib during the extended phase needed adjustment in 8% of cases, all of them consisting of 1 dosage level reduction. Only 2% of patients required longer intervals between daratumumab doses, all during long-term treatment. Only 1 patient needed suspension. Two percent of patients needed to adjust prednisone during the long-term phase. Bortezomib dose reduction was mainly due to neuropathy (60%), followed by gastrointestinal toxicity (16%). Melphalan dose was decreased mostly due to myelotoxicity (34%), kidney failure (18%), and gastrointestinal toxicity (18%). The main reason to adjust steroids was glycemic decompensation (20%). The most frequent AE in our cohort was neuropathy (27%), followed by gastrointestinal symptoms (13%) and hematological AE (10%). There were 5 treatment-emergent AE grade 5 along induction, and in all cases, death was due to infection. There were 16 deaths (14%) along treatment, 6 due to progression, 5 due to treatment complications, and 5 due to causes unrelated to MM.
Discussion
Multiple myeloma is a malignant hematological disease that often affects the elderly population. Although the advent of immunotherapy, and the enhancement of regimens have increasingly improved outcomes, the impact of these new therapies has been less remarkable in the transplant non-eligible population, particularly those older than 75 years old (7). Triplet or quadruplet induction regimens followed by long-term therapy have been widely accepted in NDMM since they have demonstrated prolonged survival in numerous clinical trials (9, 10, 11, 12). On the other hand, it has also led to a substantial financial burden on patients, payers, and society in general (20, 21, 22). Since clinical trials include highly selected patients, observations from real-life studies may have relevant practical implications for the physicians, and may offer valuable information to healthcare systems. The quadruplet regimen of D-VMP exhibited favorable efficacy with an acceptable toxicity profile in NDMM non-eligible for ASCT, according to data from the ALCYONE and OCTANS trials (11, 12). In this study, we retrospectively analyzed the efficacy D-VMP regimen in 112 patients ineligible for ASCT in real life. Findings from our real-world study reflected the outcomes of a broader patient population, which was older than that included in ALCYONE (>74 years 70% vs 30%, p<0.001) and OCTANS (70% vs 16%, p<0.001), and showed signs of a more clinically advanced disease. Twenty-six (23%) patients of our cohort would have been excluded from the ALCYONE trial due to hemoglobin level <7.5 g (7%), creatinine clearance <40 ml per minute (14%), a corrected serum calcium level >14 mg (3%) or ECOG performance status of 3 (7%) at diagnosis. However, it should be noted that despite the advanced age of our cohort, only 14% of patients were considered fragile by the treating physician. On the other hand, the prevalence of ISS 3 and high-risk CA as t(4;14), t(14;16), and del17p were similar in our cohort compared to ALCYONE (high-risk CA 13% vs 17% p= 0.271, and ISS 3 38% vs 40% p= 0.673), and OCTANS (high-risk CA 13% vs 19.3% p=0.167, and ISS 3 38% vs 28% p=0.032). Although only 56% of patients received a complete induction in our cohort compared to 79% in ALCYONE (p<0.001), this data is similar to other real-life studies using bortezomib-based regimens in elderly patients (13, 18). This could be due to more flexible compliance with guidelines in a very elderly real-life cohort, since the rate of early suspension because of disease progression or death remains similar to ALCYONE (2.7% vs 6.6% p= 0.104, and 2.7% vs 3.2% p= 0.769 respectively). In terms of ORR and VGPR/CR rate, our results were similar to both ALCYONE (95% vs 91%, p= 0.070, and 77% vs 72% p= 0.360), and OCTANS clinical trials (95% vs 88.4%, p=0.032, and 77% vs 72% p=0.587). Regarding time to response, we found the time to best response was longer in our cohort compared to ALCYONE (7 vs 4.9 months respectively). This could be explained by a less close follow-up in routine clinical practice. At a median follow-up of 40.1 months (IQR 37,4–43,1), the Kaplan-Meier estimate of the 36-month rate of OS in ALCYONE was 78.0% (95% CI 73.2–82.0), whereas in our study the Kaplan-Meier estimate of the 36-month rate of OS was 86.2% (95% CI 79.7–93.3). However, when interpreting the survival analysis of our study, it must be taken into account that 33% of the patients included received combined continuous therapy with bortezomib and daratumumab. Although combined continuous treatment was not statistically significant in the multivariate analysis, it may have had a positive impact on survival outcomes. The clinical trial GEM-OPTIMAL (0064-2021-OBS) addresses this issue and is expected to clarify the role of combined continuous treatment in the D-VMP regimen. Despite the increasing age of our cohort, 80% received subsequent therapy. This data is similar to ALCYONE (76%, p=0.476), but it is superior to other real-life studies (14, 22). This may be related to a good performance status at relapse in our cohort. This assumption is supported by the choice of treatment at relapse since the majority of patients (67%) were considered fit for a triplet regimen. Among those patients who relapsed after D-VMP regimen, only 22% received a doublet regimen on next-line therapy vs ∼60% in ALCYONE (p< 0.001). Regarding the safety profile, we found some differences with the ALCYONE and OCTANS trial. Whereas in these trials, the most frequent AE was hematological (∼50% and 84% respectively), in our cohort hematological AE was reported in only 10% of patients (p< 0.001). This could be explained by the fact that 60% of our patients received a reduced dose during induction due to any type of toxicity, and we did not include hematological AE that did not involve treatment adjustments. On the other hand, the rate of peripheral neuropathy was similar in our study compared to ALCYONE (27% vs 28%, p=0.818), and OCTANS trial (27% vs 22%, p= 0.295), while the rate of gastrointestinal AE was lower in our cohort (13% vs 23%, p= 0.014 and 13% vs 28%, p==0.003 respectively). This last finding could be due to a less exhaustive search for toxicity outside of a clinical trial and a mostly mild symptomatology. Infection data in our study is scarce since it rarely caused dose adjustment or early suspension of treatment. This differs from what was published in the ALCYONE and OCTANS trials, where 23% and 42% of grade 3/4 infections were observed respectively. On the other side, the toxicity profile found in our study population is similar to that reported in other real-life studies with bortezomib-based regimens in elderly patients (14, 17). This study has potential limitations that warrant consideration, including its retrospective nature and the lack of a control arm to confirm the efficacy and safety of the regimen. Due to the heterogeneity among centers, we did not include a homogeneous geriatric assessment at baseline or during follow-up (23, 24). This has prevented us from reaching further conclusions regarding frailty and prognosis in our cohort. Additionally, the rate of CR may be overestimated, since a bone marrow study was not required to confirm it, and MRD data are limited since they were unknown in 64 patients (57%). Regarding the safety profile, we only reported AE that led the physician to adjust or suspend treatment. Therefore, we could not communicate AE which caused delays in treatment or mild AE that may have had a relevant impact on quality of life (QoL). Since just a few centers of our cohort use Patient-Reported Outcomes (PROs) (25), information about QoL is scarce, so we cannot add any information to that already communicated in ALCYONE (26) and OCTANS (12).
Conclusions
In this real-life analysis of newly diagnosed non-transplanted multiple myeloma patients who received D-VMP as first-line treatment, the rate and depth of responses were similar to that observed in the ALCYONE and OCTANS trials despite including an older and broader patient population. At a median follow-up of 31.4 months, the median PFS was 41.5 months, and age ≥ 75 did not adversely impact survival outcomes. This highlights the need for more formal frailty assessments in routine care.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité de Ética de la Investigación de la Fundación Jiménez Díaz. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because it was a retrospective observational study and many of the patients had already died.
Author contributions
AD-G: Writing – original draft, Writing – review & editing. RA: Writing – original draft, Writing – review & editing. AJ: Writing – original draft, Writing – review & editing. TS: Writing – original draft, Writing – review & editing. AL-V: Writing – original draft, Writing – review & editing. VP: Writing – original draft, Writing – review & editing. GB: Writing – original draft, Writing – review & editing. JS-P: Writing – original draft, Writing – review & editing. EL: Writing – original draft, Writing – review & editing. AV-V: Writing – original draft, Writing – review & editing. MM-C: Writing – original draft, Writing – review & editing. ML: Writing – original draft, Writing – review & editing. AR-L: Writing – original draft, Writing – review & editing. M-JB: Writing – original draft, Writing – review & editing. EA: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos M-V, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. (2014) 15:e538–48. doi: 10.1016/S1470-2045(14)70442-5
2. Lopez-Muñoz N, Hernández-Ibarburu G, Alonso R, Sanchez-Pina JM, Ayala R, Calbacho M, et al. Large-scale real-life analysis of survival and usage of therapies in multiple myeloma. J Hematol Oncol. (2023) 16:76. doi: 10.1186/s13045-023-01474-w
3. Dimopoulos MA, Moreau P, Terpos E, Mateos MV, Zweegman S, Cook G, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. (2021) 32:309–22. doi: 10.1016/j.annonc.2020.11.014
4. Rajkumar SV, Kumar S. Multiple myeloma current treatment algorithms. Blood Cancer J. (2020) 10:94. doi: 10.1038/s41408-020-00359-2
5. de la Rubia J, González B, Cruz-Jentoft AJ, Iglesias L, Jarque I, Persona EP, et al. Geriatric assessment in hematology scale predicts treatment tolerability in older patients diagnosed with hematological Malignancies: The RETROGAH study. J Geriatr Oncol. (2023) 14:101401. doi: 10.1016/j.jgo.2022.10.016
6. Facon T, Leleu X, Manier S. How I Treat Multiple myeloma in the geriatric patient. Blood. (2023). doi: 10.1182/blood.2022017635
7. Bringhen S, Mateos MV, Zweegman S, Larocca A, Falcone AP, Oriol A, et al. Age and organ damage correlate with poor survival in myeloma patients: meta-analysis of 1435 individual patient data from 4 randomized trials. Haematologica. (2013) 98:980–7. doi: 10.3324/haematol.2012.075051
8. Miguel JFS, Khuageva NK, Shpilberg O, Petrucci MT, Dmoszynska A, Schots R, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med. (2008) 359:906–917. doi: 10.1056/NEJMoa0801479
9. Mateos M-V, Cavo M, Blade J, Dimopoulos MA, Suzuki K, Jakubowiak A, et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet. (2020) 395:132–41. doi: 10.1016/S0140-6736(19)32956-3
10. Facon T, Kumar SK, Plesner T, Orlowski RZ, Moreau P, Bahlis N, et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. (2021) 22:1582–96. doi: 10.1016/S1470-2045(21)00466-6
11. Durie BGM, Hoering A, Abidi MH, Rajkumar SV, Epstein J, Kahanic SP, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. (2017) 389:519–27. doi: 10.1016/S0140-6736(16)31594-X
12. Fu W, Bang S-M, Huang H, Kim K, Li W, An G, et al. Bortezomib, melphalan, and prednisone with or without daratumumab in transplant-ineligible asian patients with newly diagnosed multiple myeloma: the phase 3 OCTANS study. Clin Lymphoma Myeloma Leuk. (2023) 23:446–455.e4. doi: 10.1016/j.clml.2023.02.009
13. Mateos M-V, Dimopoulos MA, Cavo M, Suzuki K, Jakubowiak A, Knop S, et al. Daratumumab plus bortezomib, melphalan, and prednisone for untreated myeloma. N Engl J Med. (2018) 378:518–28. doi: 10.1056/NEJMoa1714678
14. Kumar SK, Callander NS, Adekola K, Anderson LD, Baljevic M, Baz R, et al. Multiple myeloma, version 2.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2023) 21:1281–301. doi: 10.6004/jnccn.2023.0061
15. Buda G, Del Giudice ML, Antonioli E, Ghio F, Orciuolo E, Morganti R, et al. Real-life experience with first-line therapy bortezomib plus melphalan and prednisone in elderly patients with newly diagnosed multiple myeloma ineligible for high dose chemotherapy with autologous stem-cell transplantation. Front Med. (2021) 8:712070. doi: 10.3389/fmed.2021.712070
16. Del Fabro V, Di Giorgio MA, Leotta V, Duminuco A, Bellofiore C, Markovic U, et al. Lenalidomide plus dexamethasone combination as first-line oral therapy of multiple myeloma patients: A unicentric real-life study. Cancers. (2023) 15:4036. doi: 10.3390/cancers15164036
17. Trudel S, Tessoulin B, Jullien M, Blin N, Gastinne T, Mahé B, et al. Pomalidomide, cyclophosphamide, and dexamethasone for relapsed/refractory multiple myeloma patients in a real-life setting: a single-center retrospective study. Ann Hematol. (2019) 98:1441–7. doi: 10.1007/s00277-019-03649-3
18. Hus I, Walter A, Masternak A, Jurczyszyn A, Usnarska L, Bołkun Ł, et al. Real−life experience with bortezomib−based regimens in elderly patients with newly diagnosed multiple myeloma and comorbidities: a Polish retrospective multicenter study. Pol Arch Intern Med. (2017) 127(11):765–74. doi: 10.20452/pamw.4099
19. Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. (2016) 17:e328–46. doi: 10.1016/S1470-2045(16)30206-6
20. Bessou A, Colin X, De Nascimento J, Sopwith W, Ferrante S, Gorsh B, et al. Assessing the treatment pattern, health care resource utilisation, and economic burden of multiple myeloma in France using the Système National des Données de Santé (SNDS) database: a retrospective cohort study. Eur J Health Econ. (2023) 24:321–33. doi: 10.1007/s10198-022-01463-9
21. Bhattacharya K, Bentley JP, Ramachandran S, Chang Y, Banahan BF, Shah R, et al. Phase-specific and lifetime costs of multiple myeloma among older adults in the US. JAMA Netw Open. (2021) 4:e2116357. doi: 10.1001/jamanetworkopen.2021.16357
22. Neves M, Trigo F, Rui B, João C, Lúcio P, Mariana N, et al. Multiple myeloma in Portugal: burden of disease and cost of illness. PharmacoEconomics. (2021) 39:579–87. doi: 10.1007/s40273-020-00993-5
23. Cook G, Larocca A, Facon T, Zweegman S, Engelhardt M. Defining the vulnerable patient with myeloma—a frailty position paper of the European Myeloma Network. Leukemia. (2020) 34(9):2285–94.
24. Engelhardt M, Dold SM, Ihorst G, Zober A, Moller M, Reinhardt H, et al. Geriatric assessment in multiple myeloma patients: validation of the International Myeloma Working Group (IMWG) score and comparison with other common comorbidity scores. Haematologica. (2016) 101(9):1110–9.
25. Atkinson TM, Ryan SJ, Bennett AV, Stover AM, Saracino RM, Rogak LJ, et al. The association between clinician-based common terminology criteria for adverse events (CTCAE) and patient-reported outcomes (PRO): a systematic review. Support Care Cancer. (2016) 24(8):3669–76.
Keywords: newly diagnosed multiple myeloma, non-transplant candidates, daratumumab, bortezomib, melphalan and prednisone, real-life, DVMP, first-line treatment
Citation: Domingo-González A, Alonso Fernández R, Jiménez A, De Soto Álvarez T, Lerma-Verdejo A, Pradillo V, Benzo Callejo G, Sánchez-Pina J, Landete E, Velasco-Valdazo A, Menéndez-Cuevas M, López Riñón MM, Ramírez-López A, Blanchard M-J and Askari E (2024) Real-life experience with first-line treatment with daratumumab, bortezomib, melphalan, and prednisone in patients with newly diagnosed multiple myeloma ineligible for autologous stem-cell transplantation. Front. Hematol. 3:1438233. doi: 10.3389/frhem.2024.1438233
Received: 25 May 2024; Accepted: 23 August 2024;
Published: 11 September 2024.
Edited by:
Attaya Suvannasankha, Indiana University, United StatesReviewed by:
Francesca Fazio, Sapienza University of Rome, ItalySamo Zver, University Medical Centre Ljubljana, Slovenia
Christopher Strouse, The University of Iowa, United States
Copyright © 2024 Domingo-González, Alonso Fernández, Jiménez, De Soto Álvarez, Lerma-Verdejo, Pradillo, Benzo Callejo, Sánchez-Pina, Landete, Velasco-Valdazo, Menéndez-Cuevas, López Riñón, Ramírez-López, Blanchard and Askari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amalia Domingo-González, YW1hbGlhLmRvbWluZ29AcXVpcm9uc2FsdWQuZXM=