 Theo Leitner1*
Theo Leitner1* Evgenii Shumilov2
Evgenii Shumilov2 Christina Schwitlick1Raphael Koch3Franziska Hamm1Marion Högner4Florian Bassermann4
Christina Schwitlick1Raphael Koch3Franziska Hamm1Marion Högner4Florian Bassermann4 Katja Weisel5
Katja Weisel5 Hermann Einsele6Martin Kortüm6
Hermann Einsele6Martin Kortüm6 Leo Rasche6Martin Görner7Kai Wegehenkel7Stefan Knop8
Leo Rasche6Martin Görner7Kai Wegehenkel7Stefan Knop8 Jan Krönke9Axel Nogai9
Jan Krönke9Axel Nogai9 Inke R. König10Maren Vens10Kay Horn11Nikolas von Bubnoff1
Inke R. König10Maren Vens10Kay Horn11Nikolas von Bubnoff1 Cyrus Khandanpour1*
Cyrus Khandanpour1*- 1Department of Hematology and Oncology, University Hospital of Schleswig-Holstein, University Cancer Center Schleswig-Holstein, University of Lübeck, Lübeck, Germany
- 2Department of Medicine A, Hematology, Oncology and Pneumology, University Hospital Münster, Münster, Germany
- 3Institute of Biostatistics and Clinical Research, University of Münster, Münster, Germany
- 4Department of Medicine III, Klinikum Rechts der Isar, Technical University of Munich, München, Germany
- 5University Medical Center Hamburg-Eppendorf, University of Hamburg, Hamburg, Germany
- 6Department of Internal Medicine II, University Hospital Würzburg, Würzburg, Germany
- 7Department of Hematology, Oncology and Palliative Care, Klinikum Bielefeld Mitte, Bielefeld, Germany
- 8Department Internal Medicine 5, Hematology and Oncology, Klinikum Nürnberg, Paracelsus Medical University, Nürnberg, Germany
- 9Department of Hematology, Oncology and Cancer Immunology, Charité-Universitätsmedizin Berlin, Berlin, Germany
- 10Institute of Medical Biometry and Statistics, University of Lübeck, Lübeck, Germany
- 11Center for Clinical Trials, University of Lübeck, Lübeck, Germany
Newly diagnosed multiple myeloma patients who are eligible for transplant usually receive several induction cycles of therapy, followed by one or two cycles of high-dose melphalan and autologous stem cell transfusion. In myeloma patients, high-dose melphalan improves overall survival and progression-free survival. However, melphalan exposure increases the risk of secondary malignancies and may lead to the transformation of residual myeloma cells into more aggressive clones, which may accelerate relapse. It remains to be determined whether low-risk patients also derive additional benefit from high-dose melphalan therapy compared with less toxic regimens. Here we publish the study protocol of a multicenter, interventional, controlled, randomized, prospective and open-label phase II trial to investigate whether patients with a low-risk profile (R-ISS stage I, characterized by a low tumor burden and the absence of negative cytogenetic findings or elevated LDH levels) and a standard-risk gene expression profile (using the SKY92 GEP assay) can be sufficiently treated with intensified consolidation regimens without prior high-dose melphalan chemotherapy. The primary objective is to assess whether three cycles of isatuximab, bortezomib, lenalidomide and dexamethasone (I-VRd) followed by stem cell apheresis and three additional cycles of I-VRd will result in a non-inferior rate of complete remission (CR) combined with MRD-negativity at week 40 after the start of induction therapy compared to three cycles of I-VRd followed by standard of care treatment (such as stem cell apheresis, high-dose melphalan, and autologous stem cell transplantation). We hypothesize that this approach could reduce toxicity, cost of treatment and the likelihood of the development of a more malignant plasma cell clone, while improving overall survival (OS) and progression-free survival (PFS) in newly diagnosed low risk myeloma patients.
EU Trial Number: 2022-500453-16-00, https://clinicaltrials.gov/study/NCT05665140, identifier NCT05665140. Registration Date: 21.07.2022.
1 Introduction
Multiple myeloma is a malignant disease of the bone marrow characterized by clonal expansion of plasma cells (1, 2). Current guidelines recommend that newly diagnosed, transplant-eligible patients with multiple myeloma (NDMMTE) undergo several cycles of induction, followed by one or two cycles high-dose melphalan (HDM) and autologous stem cell transfusion (ASCT) (3). With the introduction of novel agents in recent years, the prognosis for multiple myeloma patients has improved significantly. Modern induction therapy typically consists of quadruplet regimens with an immunomodulator (thalidomide or lenalidomide), a proteasome inhibitor, dexamethasone and most recently a CD38-targeting antibody. The addition of CD38-directed monoclonal antibodies has significantly improved outcome in myeloma patients (4). Isatuximab, the antibody used in this trial, has shown a progression-free survival benefit in both newly diagnosed and relapsed and refractory MM (5, 6).
Induction is followed by stem cell mobilization and either one or two cycles of high-dose melphalan chemotherapy. Current guidelines recommend a second cycle of high-dose melphalan followed by autologous stem cell transplantation in the presence of high-risk cytogenetic findings, an initial R-ISS stage III, or if the patient does not achieve at least a partial remission after the first cycle of high-dose melphalan according to the International Myeloma Working Group (IMWG) response criteria (7). Patients will then either receive 2-3 cycles of consolidation therapy followed by lenalidomide maintenance, or proceed directly to lenalidomide-based maintenance until disease progression or intolerable toxicity (3, 8). In conclusion, all NDMMTE patients receive at least one cycle of high-dose melphalan according to current guideline recommendations. However, HDM/ASCT is associated with a high rate of acute toxicities such as cytopenia, infections and gastrointestinal complications, as well as an increased risk of developing secondary malignancies (9). Preliminary data and published reports also suggest that exposure to high doses of the genotoxic drug melphalan may convert residual malignant myeloma cells into more aggressive clones and alter stromal tissue, potentially accelerating relapse (10–12). Across all risk groups high-dose melphalan therapy generally improves OS and PFS, despite a higher rate of toxicity.
However, given the favorable long-term prognosis of low-risk myeloma in the era of quadruplet therapy and the side effects of autologous stem cell transplantation, it is unclear whether HDM/ASCT remains the best treatment option for this subgroup. In this study low risk patients are defined by a R-ISS stage I (based on albumin, β2-microglobulin, lactate dehydrogenase, and high-risk cytogenetic aberrations) and a gene expression profile indicating a standard risk of relapse. Gene expression analysis of malignant bone marrow cells is performed using a standardized CE-certified gene expression array, the MMprofiler™. It enables risk prediction based on analyses of the expression pattern of 92 genes in CD138-positive plasma cells from fresh bone marrow aspirates. The results of the gene expression analysis are binary and distinguish between standard and high risk and its prognostic value has been demonstrated in several retrospective analyses involving more than 3,000 MM (13–15). Gene expression analysis is not yet part of routine clinical diagnostics, but could become a valuable tool for more personalized, risk-stratified myeloma therapy in the future.
The aim of this study is to determine whether patients with a low risk profile can be adequately treated with an intensified consolidation regimen consisting of isatuximab, bortezomib, lenalidomide and dexamethasone (I-VRd) followed by stem cell apheresis and three additional cycles of I-VRd in the absence of upfront high-dose melphalan chemotherapy. This will be compared to three cycles of I-VRd followed by standard of care treatment (such as stem cell apheresis, high-dose melphalan, and autologous stem cell transplantation) in the standard arm. The primary objective is to show non-inferiority of the experimental arm compared to the control arm regarding the rate of patients with MRD negativity combined with at least CR response according to IMWG criteria at week 40 after start of induction therapy.
We hypothesize that this approach could reduce toxicity, cost of treatment and the likelihood of the development of a more malignant plasma cell clone, while improving overall survival (OS) and progression-free survival (PFS) in newly diagnosed low risk myeloma patients.
2 Methods
2.1 Study design
This is a multi-center, interventional, controlled, randomized, prospective, open-label phase II trial with an adaptive statistical design. The target patient cohort consists of NDMMTE patients characterized by R-ISS stage I and a standard risk gene expression pattern of isolated plasma cells using the SKY92 GEP assay. The standardized CE-certified gene expression array, the MMprofiler™, allows accurate prediction of high-risk disease based on the SKY92 risk signature, which calculates a risk score based on the expression of 92 genes from malignant plasma cells.
The trial will measure the impact and calculate the risk-benefit ratio of three cycles of I-VRd, stem cell apheresis and high-dose melphalan followed by autologous stem cell transplantation and isatuximab and lenalidomide based maintenance therapy as a standard treatment group (with no trial-specific intervention regarding intensification of therapy) compared to the experimental group treated with three cycles of I-VRd, stem cell apheresis and three subsequent cycles of I-VRd followed by isatuximab and lenalidomide based maintenance therapy. Patients enrolled in this trial will undergo a screening visit to ensure that they meet all inclusion and no exclusion criteria. All eligible participants will start with I-VRd induction treatment and will undergo stem cell collection. This will allow patients in the experimental arm to receive subsequent high-dose melphalan treatment in the event of a relapse. After 3 cycles of I-VRd induction treatment, all patients who achieve at least partial remission according to the International Myeloma Working Group (IMWG) criteria will be randomized 1:1 to receive either standard treatment (high-dose melphalan followed by ASCT as suggested by local and national guidelines) or three further cycles of I-VRd. Randomization takes place on site at the respective trial site. A web-based randomization platform is used to ensure allocation concealment (www.randomizer.at). Block randomization with varying block length stratified by trial site will be applied. Only designated personnel at each trial site will have access to the randomization platform via a personalized, password-protected login.
The primary endpoint is minimal residual disease (MRD) negativity combined with a response of at least complete remission (≥CR) (MRDneg + ≥CR) at week 40 after the start of induction therapy (18 weeks after randomization either immediately following consolidation cycle 3 in the experimental arm or 112-126 days after the start of high-dose melphalan in the standard arm). MRD negativity is measured by flow cytometry and is defined as less than one malignant myeloma cell per 105 non-malignant cells. Response is assessed according to IMWG criteria. Patients who do not achieve at least VGPR will stop study treatment, enter the follow-up period and will be treated according to local standards, while all other patients will receive maintenance with isatuximab and lenalidomide. A schematic overview of the study design is shown in Figure 1.
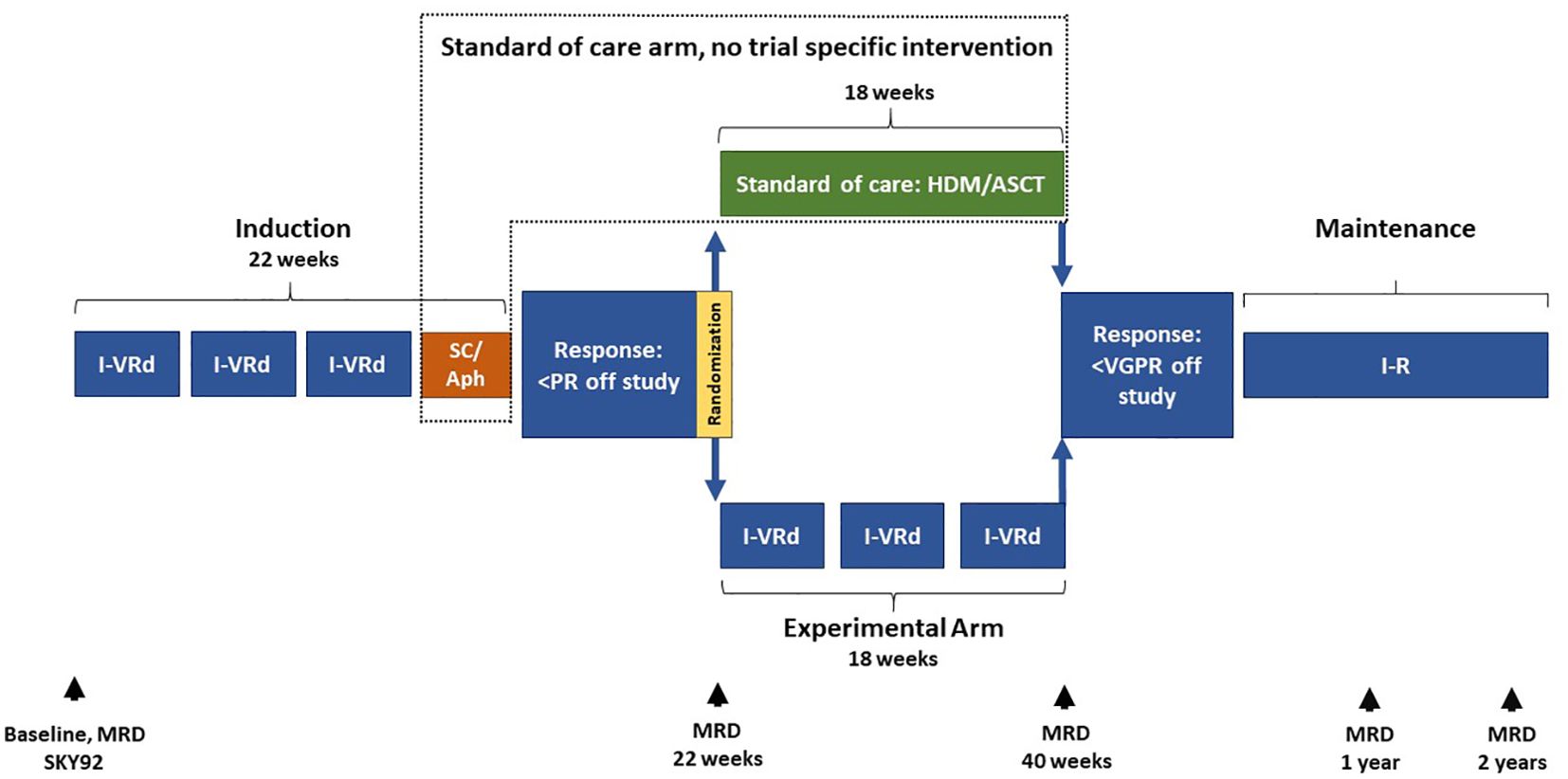
Figure 1. Concept of the ELIAS-study. Patients with R-ISS stage I will be asked if they are willing to undergo further evaluation by bone marrow sampling. Patients with R-ISS I and a standard plasma cell expression pattern as determined by the MMprofiler™ with SKY92 are eligible for the trial. All eligible patients who agree to participate in the trial will initially receive three cycles of I-VRd induction therapy. All patients will undergo stem cell mobilization and apheresis. Response will be assessed after stem cell apheresis. All patients who have achieved at least a partial remission (PR) according to the International Myeloma Working Group criteria will be randomized 1:1 to receive either standard of care (e.g. high-dose melphalan according to local and national guidelines) or three further cycles of I-VRd. The primary endpoint of MRD negativity combined with CR according to IMWG criteria will be assessed at week 40. All patients who have achieved at least a very good partial response (VGPR) will proceed to maintenance therapy. ASCT, Autologous stem cell transplantation; HDM, High-dose melphalan, I-VRd, Isatuximab, bortezomib, lenalidomide, dexamethasone; MRD, Minimal residual disease; PR, Partial response; SC/Aph, Stem cell mobilization and apheresis; VGPR, Very good partial response.
Secondary objectives are to detect possible differences in MRD negativity at week 40, year 1 and year 2 and to detect possible differences in MRD negativity combined with ≥CR rate at year 1 and year 2. Also, to characterize both arms in terms of overall survival (OS), progression-free survival (PFS), time to next treatment, overall response rate (ORR) and quality of life. Finally, the safety profile of both arms will be evaluated in terms of adverse events (AEs) and toxicities. An accompanying research project aims to investigate the molecular and phenotypic characteristics of myeloma cells and their microenvironment in the patient’s bone marrow during treatment. Specifically, this scientific program aims to measure differences in gene expression signatures, metabolic changes, and epigenetic patterns of myeloma cells in relapsed patients exposed to high-dose chemotherapy compared to relapsed patients not exposed to high-dose chemotherapy.
In summary, the aim of this trial is to achieve a more personalized treatment by combining the results of the gene expression array with the revised international staging system (R-ISS). For patients with R-ISS stage I and the absence of high-risk disease as determined by the SKY92 signature (GEP-SR), we propose a therapeutic approach that does not require high-dose chemotherapy as part of first-line therapy.
2.2 Study population
The target patient cohort consists of NDMMTE patients characterized by R-ISS stage I and a standard risk gene expression pattern of isolated plasma cells using the SKY92 GEP assay. We plan to enroll 100 patients to ensure a sufficient number of patients for evaluable MRD measurement and response assessment at week 40. R-ISS stage I patients represent approximately 25% of all NDMMTE patients. Therefore, approximately 400 patients need to be pre-screened to determine if they meet the criteria for R-ISS stage I. Patients who are eligible and willing to be enrolled in the trial will be further screened by obtaining bone marrow samples to determine gene expression patterns in myeloma cells. For the current clinical trial, we will enroll patients based on inclusion and exclusion criteria that are standard for NDMMTE patient study groups. The exact inclusion and exclusion criteria can be found in the Supplementary Appendix. Patients must have newly diagnosed, untreated, symptomatic, documented myeloma (according to the revised 2014 CRAB criteria, see Appendix 1) with clonal bone marrow (BM) plasma cells ≥10% or biopsy-proven osseous or extramedullary plasmacytoma. Additionally, one or more of the following myeloma defining events must be present: Hypercalcemia, renal insufficiency, anemia and bone lesions, a clonal bone marrow plasma cell percentage ≥60% and/or a involved: uninvolved serum free light chain ratio ≥100. With regards to risk stratification identification of a standard gene expression pattern of isolated plasma cell based on SKY92 GEP assay and proof of low-risk myeloma as defined by the revised International Staging System (R-ISS) by the International Myeloma Working Group (IMWG) is obligatory for this study. Exclusion criteria are detailed in the Supplementary Appendix, but include central nervous system (CNS) involvement, plasma cell leukemia, Waldenström’s macroglobulinemia, POEMS syndrome or clinically significant amyloidosis, non-secretory MM or active infection and evidence of another malignancy.
2.3 Study medication
All patients enrolled in this trial will receive I-VRd (isatuximab, bortezomib, lenalidomide and dexamethasone) as induction therapy. With all the limitations of comparing different trials, it appears that the combination of VRd (bortezomib, lenalidomide and dexamethasone) is superior to the current standard of care VTd (bortezomib, thalidomide and dexamethasone) in terms of better response rates and a lower rate of side effects such as polyneuropathy (16–18). Both bortezomib and lenalidomide have a well-defined safety profile in the treatment of multiple myeloma. The I-VRd induction regimen used in this trial has previously been evaluated in a phase III multiple myeloma trial (HD 7 trial), the final analysis of which is pending, but to date no excess lethal toxicity has been reported (19). In addition, there is strong evidence that bortezomib-based induction and lenalidomide-based maintenance regimens are associated with improved response rates (20).
2.3.1 Lenalidomide
Lenalidomide is a derivative of thalidomide and is commercially marketed as Lenalidomid® Hexal by Hexal AG. Lenalidomide has been extensively studied in clinical trials. As part of an induction regimen (VRd) and subsequent use of high-dose melphalan, autologous stem cell transfusion and maintenance lenalidomide has shown substantial anti-myeloma activity and good long-term disease control. Lenalidomide has been used in various studies as part of the first-line treatment of patients with NDMMTE, but is not yet approved in this indication (16, 17, 21).
2.3.2 Isatuximab
Isatuximab is an immunoglobulin (Ig) G1 monoclonal antibody (mAb) that binds selectively to the human cell surface antigen molecule classified as cluster of differentiation 38 (CD38) which is expressed on myeloma cells. Isatuximab is able to destroy CD38-expressing tumor cells through several mechanisms, including antibody-dependent cellular cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), complement-dependent cytotoxicity (CDC) and direct apoptosis. Binding of isatuximab to CD38 expressed on immune cells triggers immunomodulatory functions. Isatuximab can activate NK cells and increase their lytic activity (22, 23).
2.3.3 Dexamethasone
Dexamethasone is a potent synthetic member of the glucocorticoid class of steroids, with anti-allergic, anti-inflammatory, and immunosuppressive properties. Dexamethasone will be applied orally as tablets and i.v. as injection and has a marketing authorization under different trade names, e.g. Fortecortin® (24).
2.3.4 Bortezomib
Bortezomib is a proteasome inhibitor with anti-myeloma activity. Bortezomib is administered subcutaneous and is marketed under several trade names, including Velcade® (25).
2.3.5 Cyclophosphamide
Cyclophosphamide is approved in Germany for the treatment of multiple myeloma. It is often used as part of first-line treatment to facilitate stem cell apheresis (26). The use of cyclophosphamide followed by stem cell apheresis is not a study-specific therapeutic intervention and is not part of the trial.
2.3.6 Melphalan
High-dose melphalan (140-200mg/m² depending on renal function) followed by stem cell transfusion is the standard of care for NDMMTE. In this trial, patients who are randomized to the standard arm will receive melphalan according to local guidelines. This regimen of high-dose melphalan and stem cell rescue is the current standard of care and is not a trial-specific therapeutic intervention (3, 27).
2.4 Statistical analysis
The statistical analyses will be performed according to ICH E9 guideline (28). The primary objective of the study is the comparison of the proportion of patients showing MRD negativity and at least ≥CR at week 40 between the randomized groups in an adaptive two-stage non-inferiority design. Aim of the study is to show that the rate of MRDneg+≥CR in the group of patients with receiving three additional cycles of I-VRd consolidation is not relevantly worse than the MRDneg+≥CR rate in the group undergoing standard of care intensification therapy, i.e. treatment with three additional cycles of I-VRd is not inferior to standard of care regarding MRDneg+≥CR by more than a predefined margin (δ = 25%). The confirmatory hypotheses are: H0: πstand - πexp ≤ -δ vs. H1: πstand - πexp > -δ, with πexp and πstand denoting the proportion of patients with MRD negativity and ≥CR in the experimental and in the standard arm, and with denoting the non-inferiority margin for the MRDneg+≥CR rate. πstand -πexp represents the risk difference, which is used as summary statistic to estimate the treatment effect. The global significance level is α=5%. The confirmatory analysis of the primary endpoint will be conducted according to the per-protocol (PP) principle including all randomized patients with available MRD negativity and response evaluation at week 40. Progression or death before week 40 will be counted as failure for the binary endpoint (composite variable strategy). Further intercurrent events will be addressed using the treatment-policy strategy. An adaptive design with two stages, alpha-spending function (O’Brien & Fleming type) with preassigned weights (intended information rate 0.5 and 1) for the interim and final analysis, no futility stop, and inverse-normal combination function will be applied (29–31). At the interim analysis the null hypothesis is tested using the local significance level determined by the α-spending function at the respective information fraction for α=5%. If the null hypothesis is not rejected at the interim analysis, then it is tested using the critical value determined by the α-spending function at the final analysis. The stage-wise p-values will be calculated by applying Farrington and Manning’s likelihood score tests (32). After the first interim analysis, a data-dependent sample size recalculation may be performed. Then the accrual period, the observation time, and the schedule of the final analysis can be adapted.
Sensitivity analyses of the non-inferiority question are performed using several imputation strategies for potential missing data in MRDneg+≥CR. In supplementary analysis, multivariable logistic regression will be applied adjusting for covariates.
Analyses of secondary objectives will be performed following the intention-to-treat (ITT) principle using all available data of randomized patients, irrespective of protocol violations and therapy dropout, and are considered as exploratory analyses. Therefore, no significance level is fixed. Two-sided p-values are considered noticeable in the case of p ≤ 0.05, one-sided p-values are considered noticeable in the case of p ≤ 0.025. Statistical analyses of the secondary endpoints will be conducted with appropriate descriptive and frequentist statistical methods using summary statistics such as mean and standard deviation, median and quartiles, or frequency and percent. Continuous secondary endpoints are compared between randomized treatments groups using Welch’s t-test or Mann–Whitney U-tests and categorical variables via Fisher’s exact or chi-square tests. Time-to-event endpoints (PFS and OS) are analyzed using two-sided log-rank test. Multivariable analysis will be performed using Cox regressions. Analyses of specific failure risks are performed using a competing risk approach. Endpoints that are measured repeatedly over time and their changes are analyzed separately for each time point. In addition, (generalized) linear mixed models will be fitted. Safety data will be evaluated descriptively according to the as-treated principle in the safety population. Subgroup analyses will be conducted based on cytogenetics (hyperdiploidy (FISH), t (11, 14), all others), initial WHO Performance Status (ECOG 0 vs. 1 and 2), sex, age (18-55 years, 56-70 years), and response (response ≥VGPR, response <VGPR as well as response ≥PR, response <PR) and MRD (response ≥CR+ MRD negativity, response <CR and MRD negativity) status after induction therapy prior to randomization.
In general, number of patients with missing data and missingness patterns will be presented descriptively. In additional exploratory sensitivity analyses multiple imputation approaches or models applicable to longitudinal data with missing values (e.g. (generalized) linear mixed models) can be used. In case of the endpoint time-to-event endpoints, data will be treated as right-censored in case of no event before end of follow-up.
Data preparation and descriptive analysis will performed using SAS software, of the SAS System for Windows and adaptive analyses using ADDPLAN® and R software using the package “rpact” (33, 34).
2.5 Proposed sample size/power calculations
The sample size calculation is based on the primary binary endpoint MRDneg+≥CR at week 40 after the start of induction therapy. In the CASSIOPEIA trial which defined the current standard of care treatment for newly diagnosed multiple myeloma patients in Germany, the rate of MRDneg+≥CR was 20% for patients randomized to the standard arm (VTd without daratumumab) after completion of high-dose melphalan therapy (35). In the group of patients randomized to daratumumab VTd (experimental arm), the MRDneg+≥CR rate was 34% after completion of high-dose melphalan therapy. Based on the extrapolation of the results of the Griffin trial we assume that R-ISS I patients, who additionally have a standard risk gene expression pattern, will have an even higher MRDneg+≥CR rate of approximately 75% after completing standard care treatment such as high-dose chemotherapy (36). Using a non-inferiority margin of 25%, if the standard of care arm in our study meets the assumption of an MRDneg+≥CR rate of 75% and if the experimental arm has an MRDneg+≥CR rate of >50%, we propose that the experimental arm in our study is not-inferior to the conventional therapy used for patients. Under the specified two-stage adaptive non-inferiority design and the assumptions above (πstand = πexp = 75%, δ = 25%), a significance level of α=5%, an allocation ratio of 1:1, and an intended information rate of 0.5 and 1 for the interim and final analysis, 76 patients (38 experimental arm and 38 standard arm) with evaluable MRD measurement and response evaluation at week 40 are required to obtain an overall power ≥ 80% to show non-inferiority. The planned first interim analysis is intended to be performed after 38 evaluable patients. However, due to the alpha-spending approach, the timing can be chosen flexibly, so that the number of patients for the interim analysis can be smaller or larger. If the analysis is performed after 38 patients with an information rate of 0.5, the power in the interim analysis is 22% and the alpha spent is 0.0056. The sample size was calculated using the normal-approximation. Since MRD negativity and response (≥CR) are measured at week 40 after the start of treatment, we expected some missing values due to dropouts and technical difficulties. To account for dropouts, a total of 100 patients will be included.
3 Discussion
High-dose melphalan (HDM) followed by autologous stem cell transplantation (ASCT) is the current standard of care for transplant-eligible newly diagnosed multiple myeloma (NDMMTE). However, with the emergence of highly effective monoclonal antibody-based quadruplet induction regimens, it is not known whether HDM/ASCT remains the best choice for all transplant-eligible patients or whether a more tailored, risk-adapted therapeutic approach is needed. In particular, patients with low-risk myeloma may be sufficiently treated with a quadruplet substance therapy without HDM/ASCT in terms of PFS and OS. To the best of our knowledge, there is no clinical trial that systematically evaluates high-dose therapy versus quadruplet consolidation therapy specifically in low-risk myeloma. This study attempts to fill this gap: We hypothesize that low-risk patients do not benefit from high-dose chemotherapy upfront, as the disease may be sufficiently controlled by modern proteasome inhibitor and CD38-directed antibody combination therapies.
Across all risk groups, the addition of HDM/ASCT has repeatedly shown a benefit for progression-free survival in the context of three-drug therapies (16, 37–39). The IFM 2009 phase III trial, conducted by the French Intergroupe Francophone du Myélome (IFM), compared the efficacy of lenalidomide, bortezomib and dexamethasone (RVd) alone with that of RVd plus high-dose melphalan and ASCT. The addition of HDM/ASCT to RVd was associated with a significantly longer progression-free survival, but did not improve overall survival (16). These findings were confirmed in the DETERMINATION trial, which used a similar approach and also compared RVd plus high-dose melphalan and ASCT with RVd alone (39). An additional case in point is the FORTE trial, which demonstrated an improved progression-free survival with the addition of HDM/ASCT to carfilzomib, lenalidomide, dexamethasone (KRd) compared to KRd alone (38). Notably, these trials reported higher incidences of adverse events in patients receiving high-dose melphalan and ASCT.
For modern quadruplet therapy, randomized trials comparing HDM/ASCT with no HDM/ASCT are lacking. The MANHATTAN nonrandomized clinical trial assessed whether the addition of the anti-CD38 monoclonal antibody daratumumab to carfilzomib, lenalidomide, dexamethasone (Dara-KRd) was sufficient in achieving high rates of MRD-negativity in newly diagnosed multiple myeloma without high-dose melphalan chemotherapy and autologous hemopoietic cell transplantation. The study met its primary endpoint by demonstrating that 71% of patients achieved MRD-negativity without having undergone HDM/ASCT, proving the high efficiency of modern combinations regimens (40). However, in none of the trials mentioned above was the choice of treatment based on risk stratification.
Several findings suggest that particularly high-risk myeloma patients benefit from intensified therapy with autologous transplantation while low risk patients may not benefit equally. Bal et al. evaluated the impact of HDM/ASCT on minimal residual disease (MRD) in the context of quadruplet induction and were able to show that the greatest reduction in MRD burden was in the high-risk myeloma group (41, 42). The EMN-02/HOVON-95 trial studied NDMMTE patients who received bortezomib, cyclophosphamide and dexamethasone (VCD) and were then randomized to receive either high-dose chemotherapy followed by ASCT or a combination of bortezomib, melphalan and prednisone (VMP). Patients then received lenalidomide-based maintenance therapy (37). In a retrospective analysis of this trial, Hofste op Bruinink et al. demonstrated that a high-risk MM population benefits from an HDM-ASCT treatment over VMP it was shown that an extremely low-risk group of patients, defined as R-ISS stage I, absence of high-risk gene expression-based disease and absence of del17p, showed no OS benefit despite receiving high-dose chemotherapy and ASCT compared to patients treated with VMP alone (43). In conclusion, there is evidence that HDM may be an overtreatment for patients with low-risk myeloma in the era of novel therapies and that there may be no benefit in terms of PFS in this group when considering short and long-term toxicity. We believe that this trial will provide valuable insights into the role of HDM and ASCT in the context of low-risk multiple myeloma and modern quadruplet therapy as we move toward a more risk-stratified and personalized myeloma therapy.
4 Ethics and dissemination
The study will be conducted in compliance with the declaration of Helsinki (current version, October 2013, Fortaleza), the requirements of the clinical trials regulation (CTR) 536/2014 and the current German drug law (“Arzneimittelgesetz”), the current legal provisions regarding data protection, and the principles of Good Clinical Practice. The trial is registered under EU Trial Number: 2022-500453-16-00, Registration Date: 21.07.2022) and has been approved by the Medical Ethics Committee of Landesärztekammer Hessen on 03.11.2022. The results of this study will be widely disseminated through peer-reviewed publications and presentations at international conferences.
Ethics statement
The study will be conducted in compliance with the declaration of Helsinki (current version, October 2013, Fortaleza), the requirements of the clinical trials regulation (CTR) 536/2014 and the current German drug law (“Arzneimittelgesetz”), the current legal provisions regarding data protection, and the principles of Good Clinical Practice. The trial is registered under EU Trial Number: 2022-500453- 16-00, Registration Date: 21.07.2022) and has been approved by the Medical Ethics Committee of Landesärztekammer Hessen on 03.11.2022. The participants provided their written informed consent to participate in this study.
Author contributions
TL: Investigation, Writing – original draft, Writing – review & editing. ES: Writing – review & editing, Investigation. CS: Investigation, Writing – review & editing. RK: Investigation, Writing – review & editing. FH: Investigation, Writing – review & editing. MH: Investigation, Writing – review & editing. FB: Investigation, Writing – review & editing. KWei: Investigation, Writing – review & editing. HE: Writing – review & editing. MK: Methodology, Investigation, Resources, Writing – review & editing. LR: Investigation, Writing – review & editing. MG: Investigation, Writing – review & editing. KWeg: Investigation, Writing – review & editing. SK: Investigation, Writing – review & editing. JK: Investigation, Writing – review & editing. AN: Investigation, Writing – review & editing. IK: Writing – review & editing, Investigation. MV: Investigation, Writing – review & editing, Data curation, Writing – original draft. KH: Investigation, Writing – review & editing. NB: Investigation, Writing – review & editing. CK: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This trial is financially supported by Sanofi.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhem.2024.1436845/full#supplementary-material
References
1. Gerecke C, Fuhrmann S, Strifler S, Schmidt-Hieber M, Einsele H, Knop S. The diagnosis and treatment of multiple myeloma. Dtsch Arztebl Int. (2016) 113:470–6. doi: 10.3238/arztebl.2016.0470
2. Raab MS, Podar K, Breitkreutz I, Richardson PG, Anderson KC. Multiple myeloma. Lancet. (2009) 374:324–39. doi: 10.1016/S0140-6736(09)60221-X
3. Dimopoulos MA, Moreau P, Terpos E, Mateos MV, Zweegman S, Cook G, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. (2021) 32:309–22. doi: 10.1016/j.annonc.2020.11.014
4. Moreau P, Attal M, Hulin C, Arnulf B, Belhadj K, Benboubker L, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, phase 3 study. Lancet. (2019) 394:29–38. doi: 10.1016/S0140-6736(19)31240-1
5. Attal M, Richardson PG, Rajkumar SV, San-Miguel J, Beksac M, Spicka I, et al. Isatuximab plus pomalidomide and low-dose dexamethasone versus pomalidomide and low-dose dexamethasone in patients with relapsed and refractory multiple myeloma (ICARIA-MM): a randomised, multicentre, open-label, phase 3 study. Lancet. (2019) 394:2096–107. doi: 10.1016/S0140-6736(19)32556-5
6. Martin T, Dimopoulos MA, Mikhael J, Yong K, Capra M, Facon T, et al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized Phase 3 study. Blood Cancer J. (2023) 13:1–9. doi: 10.1038/s41408-023-00797-8
7. Durie BGM, Harousseau JL, Miguel JS, Bladé J, Barlogie B, Anderson K, et al. International uniform response criteria for multiple myeloma. Leukemia. (2006) 20:1467–73. doi: 10.1038/sj.leu.2404284
8. Mikhael J, Ismaila N, Cheung MC, Costello C, Dhodapkar MV, Kumar S, et al. Treatment of multiple myeloma: ASCO and CCO joint clinical practice guideline. JCO. (2019) 37:1228–63. doi: 10.1200/JCO.18.02096
9. Musto P, Anderson KC, Attal M, Richardson PG, Badros A, Hou J, et al. Second primary Malignancies in multiple myeloma: an overview and IMWG consensus. Ann Oncol. (2017) 28:228–45. doi: 10.1093/annonc/mdw606
10. Landau HJ, Yellapantula V, Diamond BT, Rustad EH, Maclachlan KH, Gundem G, et al. Accelerated single cell seeding in relapsed multiple myeloma. Nat Commun. (2020) 11:3617. doi: 10.1038/s41467-020-17459-z
11. Weinhold N, Ashby C, Rasche L, Chavan SS, Stein C, Stephens OW, et al. Clonal selection and double-hit events involving tumor suppressor genes underlie relapse in myeloma. Blood. (2016) 128:1735–44. doi: 10.1182/blood-2016-06-723007
12. Rellick SL, Piktel D, Walton C, Hall B, Petros W, Fortney JE, et al. Melphalan exposure induces an interleukin-6 deficit in bone marrow stromal cells and osteoblasts. Cytokine. (2012) 58:245–52. doi: 10.1016/j.cyto.2012.01.012
13. van Beers EH, van Vliet MH, Kuiper R, de Best L, Anderson KC, Chari A, et al. Prognostic validation of SKY92 and its combination with ISS in an independent cohort of patients with multiple myeloma. Clin Lymp Myeloma Leuk. (2017) 17:555–62. doi: 10.1016/j.clml.2017.06.020
14. Kuiper R, Broyl A, de Knegt Y, van Vliet MH, van Beers EH, van der Holt B, et al. A gene expression signature for high-risk multiple myeloma. Leukemia. (2012) 26:2406–13. doi: 10.1038/leu.2012.127
15. Kuiper R, van Duin M, van Vliet MH, Broijl A, van der Holt B, El Jarari L, et al. Prediction of high- and low-risk multiple myeloma based on gene expression and the International Staging System. Blood. (2015) 126:1996–2004. doi: 10.1182/blood-2015-05-644039
16. Attal M, Lauwers-Cances V, Hulin C, Leleu X, Caillot D, Escoffre M, et al. Lenalidomide, bortezomib, and dexamethasone with transplantation for myeloma. N Engl J Med. (2017) 376:1311–20. doi: 10.1056/NEJMoa1611750
17. Roussel M, Lauwers-Cances V, Robillard N, Hulin C, Leleu X, Benboubker L, et al. Front-line transplantation program with lenalidomide, bortezomib, and dexamethasone combination as induction and consolidation followed by lenalidomide maintenance in patients with multiple myeloma: a phase II study by the Intergroupe Francophone du Myélome. J Clin Oncol. (2014) 32:2712–7. doi: 10.1200/JCO.2013.54.8164
18. Moreau P, Hulin C, Macro M, Caillot D, Chaleteix C, Roussel M, et al. VTD is superior to VCD prior to intensive therapy in multiple myeloma: results of the prospective IFM2013-04 trial. Blood. (2016) 127:2569–74. doi: 10.1182/blood-2016-01-693580
19. Goldschmidt H, Mai EK, Bertsch U, Fenk R, Nievergall E, Tichy D, et al. Addition of isatuximab to lenalidomide, bortezomib, and dexamethasone as induction therapy for newly diagnosed, transplantation-eligible patients with multiple myeloma (GMMG-HD7): part 1 of an open-label, multicentre, randomised, active-controlled, phase 3 trial. Lancet Haematol. (2022) 9:e810–21. doi: 10.1016/S2352-3026(22)00263-0
20. McCaughan GJ, Gandolfi S, Moore JJ, Richardson PG. Lenalidomide, bortezomib and dexamethasone induction therapy for the treatment of newly diagnosed multiple myeloma: a practical review. Br J Haematol. (2022) 199:190–204. doi: 10.1111/bjh.18295
21. McCarthy PL, Holstein SA, Petrucci MT, Richardson PG, Hulin C, Tosi P, et al. Lenalidomide maintenance after autologous stem-cell transplantation in newly diagnosed multiple myeloma: A meta-analysis. J Clin Oncol. (2017) 35:3279–89. doi: 10.1200/JCO.2017.72.6679
22. Martin TG, Corzo K, Chiron M, van de Velde H, Abbadessa G, Campana F, et al. Therapeutic opportunities with pharmacological inhibition of CD38 with isatuximab. Cells. (2019) 8:1522. doi: 10.3390/cells8121522
23. Frampton JE. Isatuximab: A review of its use in multiple myeloma. Target Oncol. (2021) 16:675–86. doi: 10.1007/s11523-021-00827-0
24. Sinha S, Rajkumar SV, Lacy MQ, Hayman SR, Buadi FK, Dispenzieri A, et al. Impact of dexamethasone responsiveness on long term outcome in patients with newly diagnosed multiple myeloma. Br J Haematol. (2010) 148:853–8. doi: 10.1111/j.1365-2141.2009.08023.x
25. Kouroukis TC, Baldassarre FG, Haynes AE, Imrie K, Reece DE, Cheung MC. Bortezomib in multiple myeloma: systematic review and clinical considerations. Curr Oncol. (2014) 21:e573–603. doi: 10.3747/co.21.1798
26. Tuchman SA, Bacon WA, Huang LW, Long G, Rizzieri D, Horwitz M, et al. Cyclophosphamide-based hematopoietic stem cell mobilization before autologous stem cell transplantation in newly diagnosed multiple myeloma. J Clin Apher. (2015) 30:176–82. doi: 10.1002/jca.21360
27. Poczta A, Rogalska A, Marczak A. Treatment of multiple myeloma and the role of melphalan in the era of modern therapies—Current research and clinical approaches. J Clin Med. (2021) 10:1841. doi: 10.3390/jcm10091841
28. Westferry C, Canary WICH E9 statistical principles for clinical trials - Scientific guideline. London, UK: European Medicines Agency (2024). Available at: https://www.ema.europa.eu/en/ich-e9-statistical-principles-clinical-trials-scientific-guideline.
29. Kim K, Demets DL. Design and analysis of group sequential tests based on the type I error spending rate function. Biometrika. (1987) 74:149–54. doi: 10.1093/biomet/74.1.149
30. O’Brien PC, Fleming TR. A multiple testing procedure for clinical trials. Biometrics. (1979) 35:549–56. doi: 10.2307/2530245
31. Lehmacher W, Wassmer G. Adaptive sample size calculations in group sequential trials. Biomet Dezember. (1999) 55:1286–90. doi: 10.1111/j.0006-341X.1999.01286.x
32. Farrington CP, Manning G. Test statistics and sample size formulae for comparative binomial trials with null hypothesis of non-zero risk difference or non-unity relative risk. Stat Med Dezember. (1990) 9:1447–54. doi: 10.1002/sim.4780091208
33. Wassmer G, Pahlke F, Jensen T, Schueuerhuis S, Muetze T. rpact: Confirmatory Adaptive Clinical Trial Design and Analysis (2024). Available online at: https://cran.r-project.org/web/packages/rpact/index.html (Accessed September 2, 2024).
34. R: The R Project for Statistical Computing (2024). Available online at: https://www.r-project.org/ (Accessed September 2, 2024).
35. Moreau P, Hulin C, Perrot A, Arnulf B, Belhadj K, Benboubker L, et al. Maintenance with daratumumab or observation following treatment with bortezomib, thalidomide, and dexamethasone with or without daratumumab and autologous stem-cell transplant in patients with newly diagnosed multiple myeloma (CASSIOPEIA): an open-label, randomised, phase 3 trial. Lancet Oncol. (2021) 22:1378–90. doi: 10.1016/S1470-2045(21)00428-9
36. Voorhees PM, Sborov DW, Laubach J, Kaufman JL, Reeves B, Rodriguez C, et al. Addition of daratumumab to lenalidomide, bortezomib, and dexamethasone for transplantation-eligible patients with newly diagnosed multiple myeloma (GRIFFIN): final analysis of an open-label, randomised, phase 2 trial. Lancet Haematol. (2023) 10:e825–37. doi: 10.1016/S2352-3026(23)00217-X
37. Cavo M, Gay F, Beksac M, Pantani L, Petrucci MT, Dimopoulos MA, et al. Autologous haematopoietic stem-cell transplantation versus bortezomib-melphalan-prednisone, with or without bortezomib-lenalidomide-dexamethasone consolidation therapy, and lenalidomide maintenance for newly diagnosed multiple myeloma (EMN02/HO95): a multicentre, randomised, open-label, phase 3 study. Lancet Haematol. (2020) 7:e456–68. doi: 10.1016/S2352-3026(20)30099-5
38. Gay F, Musto P, Rota-Scalabrini D, Bertamini L, Belotti A, Galli M, et al. Carfilzomib with cyclophosphamide and dexamethasone or lenalidomide and dexamethasone plus autologous transplantation or carfilzomib plus lenalidomide and dexamethasone, followed by maintenance with carfilzomib plus lenalidomide or lenalidomide alone for patients with newly diagnosed multiple myeloma (FORTE): a randomised, open-label, phase 2 trial. Lancet Oncol. (2021) 22:1705–20. doi: 10.1016/S1470-2045(21)00535-0
39. Richardson PG, Jacobus SJ, Weller EA, Hassoun H, Lonial S, Raje NS, et al. Triplet therapy, transplantation, and maintenance until progression in myeloma. New Engl J Med. (2022) 387:132–47. doi: 10.1056/NEJMoa2204925
40. Landgren O, Hultcrantz M, Diamond B, Lesokhin AM, Mailankody S, Hassoun H, et al. Safety and effectiveness of weekly carfilzomib, lenalidomide, dexamethasone, and daratumumab combination therapy for patients with newly diagnosed multiple myeloma. JAMA Oncol. (2021) 7:862–8. doi: 10.1001/jamaoncol.2021.0611
41. Bal S, Dhakal B, Silbermann RW, Schmidt TM, Dholaria B, Giri S, et al. Impact of autologous hematopoietic cell transplantation on disease burden quantified by next-generation sequencing in multiple myeloma treated with quadruplet therapy. Am J Hematol. (2022) 97:1170–7. doi: 10.1002/ajh.26640
42. Crusoe E, Costa L. Repositioning autologous stem cell transplantation in the management of newly diagnosed multiple myeloma. Journal of Bone Marrow Transplantation and Cellular Therapy. (2023) 4(3):205.
43. Hofste op Bruinink D, van Duin M, Beksac M, Driessen C, Ludwig H, Vermeulen M, et al. Differential effect of upfront intensification treatment in genetically defined myeloma risk groups - a combined analysis of ISS, del17p and SKY92 scores in the EMN-02/HOVON-95 MM trial. Blood. (2018) 132:3186. doi: 10.1182/blood-2018-99-119873
Keywords: newly diagnosed multiple myeloma, clinical trial, high-dose melphalan, autologous stem cell transfusion, isatuximab, MRD, personalized therapy
Citation: Leitner T, Shumilov E, Schwitlick C, Koch R, Hamm F, Högner M, Bassermann F, Weisel K, Einsele H, Kortüm M, Rasche L, Görner M, Wegehenkel K, Knop S, Krönke J, Nogai A, König IR, Vens M, Horn K, von Bubnoff N and Khandanpour C (2024) Comparison of 6 cycles of isatuximab with lenalidomide, bortezomib and dexamethasone (I-VRd) versus 3 cycles of I-VRd followed by one cycle of high-dose melphalan in newly diagnosed low-risk multiple myeloma. Protocol for a multicenter, prospective, randomized, phase II clinical trial (ELIAS-Trial). Front. Hematol. 3:1436845. doi: 10.3389/frhem.2024.1436845
Received: 28 May 2024; Accepted: 20 August 2024;
Published: 06 December 2024.
Edited by:
Francesco Di Raimondo, University of Catania, ItalyReviewed by:
Francesca Cottini, The Ohio State University, United StatesVittorio Montefusco, Santi Paolo e Carlo Hospital, Italy
Giuseppe Mele, Antonio Perrino Hospital, Italy
Copyright © 2024 Leitner, Shumilov, Schwitlick, Koch, Hamm, Högner, Bassermann, Weisel, Einsele, Kortüm, Rasche, Görner, Wegehenkel, Knop, Krönke, Nogai, König, Vens, Horn, von Bubnoff and Khandanpour. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Theo Leitner, dGhlby5sZWl0bmVyQHVrc2guZGU=; Cyrus Khandanpour, Y3lydXMua2hhbmRhbnBvdXJAdWtzaC5kZQ==