 Miklos Egyed
Miklos Egyed Bela Kajtar2
Bela Kajtar2 Vibe Skov
Vibe Skov Lasse Kjær
Lasse Kjær Hans Carl Hasselbalch
Hans Carl Hasselbalch- 1Department of Hematology, Somogy County Moritz Kaposi General Hospital, Kaposvar, Hungary
- 2Pathology Institution, Medical University of Pécs, Pécs, Hungary
- 3Department of Cardiology, Gottsegen National Cardiovascular Center, Budapest, Hungary
- 4Department of Hematology, Zealand University Hospital, Roskilde, Denmark
The JAK2V617F mutation is an acquired somatic mutation, which is prevalent in patients with the Philadelphia-chromosome negative myeloproliferative neoplasms (MPNs). In these diseases the mutation gives rise to constitutive JAK-STAT signaling with increased blood cell counts and in vivo activation of neutrophils and platelets as well, which altogether contribute to a chronic inflammatory and thrombogenic state with a 12-fold increased risk of coronary disease. Treatment with recombinant interferon-alpha2 (rIFN) reduces the JAK2V617F allelic burden in a large number of MPN-patients. Long-term treatment with rIFN associates with low-burden JAK2V617F in a subset of patients and a decreased thrombosis risk as well. In the general population the JAK2V617F mutation has been shown to associate with ischemic heart disease and thrombosis. Based upon the above observations we herein report the first patient with CHIP-JAK2V617F, in whom treatment with rIFN resolved severe angina pectoris. During a short period off rIFN the symptoms reappeared to resolve in concert with reduction of JAK2V617F allele burden, when rIFN was reinstituted. The JAK2V617F mutation may be a novel therapeutic target to prohibit the development of cardiovascular diseases using rIFN either as monotherapy or in combination with potent anti-inflammatory agents.
Highlights
● Complete resolution of angina pectoris and major molecular remission in a CHIP-JAK2V617F patient with severe ischemic heart disease.
● In cardiovascular disease CHIP-JAK2V617F positive patients, the mutation may be a novel molecular target for rIFN to be investigated in future trials.
Introduction
The JAK2V617F mutation is prevalent in the Philadelphia-chromosome negative myeloproliferative neoplasms (MPNs) (1) and associates with a 12-fold increased risk of coronary disease (2, 3), which may be explained by its potential to induce a chronic inflammatory state by generating reactive oxygen species (4). Furthermore, this mutation also induces increased Peptidyl Arginine Deiminase Type 4 (PAD4), which is required for the formation of JAK2V617F-driven Neutrophil Extracellular Traps (NETs) and thrombosis (5). Other thrombosis- promoting mechanisms are elevated blood cell counts and their constitutive in vivo activation with formation of circulating microaggregates and impaired microcirculation (2). The above thrombogenic factors contribute significantly to morbidity and mortality in MPNs (2, 3). Taking into account the detrimental effects of the JAK2V617F mutation (2, 3, 6, 7), it is a great advantage that treatment with pegylated interferon alpha2 (rIFN) is able to reduce the JAK2V617F allelic burden (8–17) and in a subset of patients even to very low levels (< 1%), inducing minimal residual disease (MRD) (13–15). Thus, last year ropegInterferon (ropegIFN) was launched for the treatment of patients with PV (16, 17).
The development of MPNs is for decades preceded by Clonal Hematopoiesis of Indeterminate Potential (CHIP) which increases with ageing and associates with an increased risk of cardiovascular disease (CVD) (18). The JAK2V617F mutation is far more prevalent in the general population than previously anticipated with a prevalence of approximately 5% in individuals above 60 years (19). Importantly, JAK2V617F-positive clonal hematopoiesis associates with an increased incidence of thrombosis in the general population without a known myeloid disorder (5, 19).
Mathematical modelling studies have shown that the earlier treatment with rIFN is instituted in MPNs the better, since the JAK2V617F mutation will then more rapidly decline during treatment (20). Importantly, the JAK2V617F mutation might actually be a novel therapeutic target in the CHIP-stage, thereby potentially eradicating the malignant clone and prohibiting development of MPNs and associated comorbidities, including CVD (13, 21). Herein, we for the first time report the complete resolution of angina pectoris in a male patient with CHIP-JAK2V617F during treatment with rIFN.
Case story
A 50-year-old male patient was admitted with attacks of angina pectoris. His history included hypertension, type 2 diabetes mellitus, hypercholesterolemia and coronary sclerosis. In June 2019 the patient suffered myocardial infarction. In December 2019, an angiography displayed in-stent re-stenosis of previously applied stents and de-novo stenosis of other coronary segments. Three new stent implantations were performed. However, heart complaints persisted with daily, frequent angina pectoris, despite optimal medication for CVD, including aspirin and atorvastatin.
In January 2021 frequent attacks of angina appeared. A coronary angiography necessitated new stent implantation and a drug eluting balloon angioplasty. Despite these procedures, daily cardiac angina complaints persisted from March of 2021.
From January 2021 blood cell counts were repeatedly within the normal range. In January 2021 the JAK2V617F allele burden was 0,018% (22). A panel NGS of 59 genes relevant in myeloid malignancies was performed on the Illumina Novaseq 6000 platform. No pathogenic mutations were detected.
Treatment with ropeg-IFN was fueled by a report, proposing JAK2V617F as a new therapeutical target in CVD (21). Accordingly, treatment with ropeg-IFN 125 ug every other week was initiated on April 1 2021. Two weeks later the complaints significantly eased and later completely disappeared (Figure 1). From April 1 to November 1, 2021 the patient received a total of 14 injections every second week. In this period of time the patient was completely free of cardiac symptoms and was well. On November 1, the JAK2V617F mutation was no longer detectable and treatment with ropeg-IFN was accordingly paused. By Christmas evening 2021, serious angina reappeared and persisted despite medication as outlined above. A cardiac-CT scan was performed on December 27 which showed slight regression of the coronary artery disease (no in-stent or de-novo stenoses) but because of the symptoms treatment with ropeg-IFN was reinstituted (125 ug x 1 sc every second week) in February and the angina attacks disappeared within 2 weeks. On March 4, 2022, a JAK2V617F analysis was done, showing an allele burden of 0.012%, which declined to a level of 0.007% on June 16th, when the patient was still feeling well without any cardiac complaints (Figure 1).
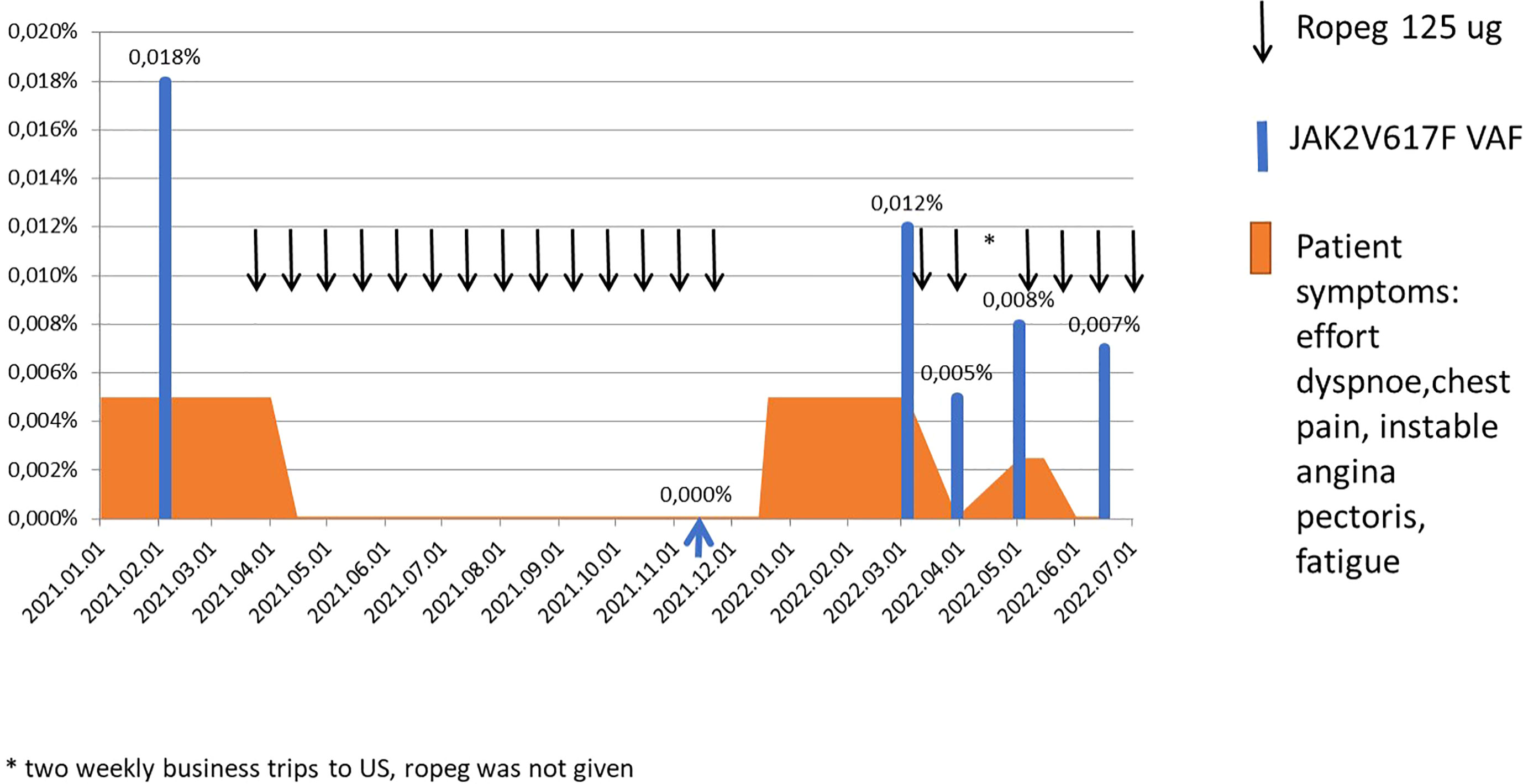
Figure 1 Treatment, symptoms and molecular answers.
Discussion
Chronic inflammation is considered an important pathogenetic mechanism for MPN-disease development and disease progression (2, 6, 7, 15). Several thrombo-inflammatory genes have been found to be upregulated, likely contributing to the increased risk of thrombosis (2, 23). In addition, long-term treatment with rIFN normalizes elevated cell counts in concert with induction of a remarkable decrease in the JAK2V617F allele burden and accordingly impacting important thrombosis promoting factors in MPNs (2, 8–17). Treatment with rIFN is also able to normo- or significantly downregulate upregulated thrombo-inflammatory genes in patients with MPNs, including PAD4 (23), which strongly induces NETosis and accordingly thrombosis (5). In addition, rIFN downregulates upregulated oxidative stress genes in MPNs (24).
Since CHIP in the general population associates with an increased risk of thrombosis and accordingly CVD it is pertinent to consider if the thrombosis-promoting JAK2V617F mutation might be a therapeutic target in the CHIP-stage (13, 21). In this report we have convincingly shown that rIFN rapidly induced resolution of angina pectoris together with a decline in the JAK2V617F mutation. Although only a singular observation we believe it to be unique and potentially of utmost importance, hopefully opening the avenue for pilot studies of the impact of rIFN in CHIP-JAK2V617F positive individuals with CVD (13, 19, 23). Such studies are even more pertinent, when considering that the JAK2V617F mutation associates with thrombosis and ischemic heart disease in the general population (5, 19). These studies should include serial transcriptomic and proteomic studies together with detailed thrombophilia studies in order to elucidate in depth the mechanisms behind the potentially beneficial effects of rIFN upon symptom burden and cardiovascular disease burden in terms of improvement of cardiac function and perhaps also regression of aortic valve calcification, which most recently has been reported to be prominent in patients with MPNs (25) and likely associated with the JAK2V617F mutation.
The future treatment of MPNs may imply both stem-cell targeting treatment with rIFN and treatment which targets the chronic inflammatory state, driving clonal expansion in the precursor stage of MPN - CHIP - towards overt MPNs (2, 6, 7, 10, 11, 13, 15). Taking into account the important role of chronic inflammation for clonal expansion both in the CHIP stage and in MPNs, there is an urgent need to investigate, whether stem-cell targeting therapy with rIFN in the CHIP-stage might induce MRD in concert with a reduction in inflammatory biomarkers.
In conclusion, we have for the first time shown rIFN treatment of a JAK2V617F positive CHIP patient to induce complete remission of repeated attacks of angina pectoris. We suggest, that the beneficial effects of rIFN might be related to the anti-inflammatory and anti-thrombotic potentials of rIFN, including normalization of elevated blood cell counts, reduction in the JAK2V617F allelic burden, dampening of oxidative stress and decrease in ROS together with downregulation of thromboinflammatory genes, such as the thrombosis-promoting PAD4 and accordingly NETosis activity. Our report calls for clinical studies of the impact of rIFN – either as monotherapy or in combination with potent anti-inflammatory agents upon the cardiovascular disease burden both in the CHIP-stage and in patients with MPNs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ME designed research, performed research, analyzed data, wrote the paper. BK and CF performed research. HH,VS, and LK wrote the paper. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Spivak JL. Myeloproliferative neoplasms. N Engl. J. Med. (2017) 376(22):2168–81. doi: 10.1056/NEJMra1406186
2. Hasselbalch HC, Elvers M, Schafer AI. The pathobiology of thrombosis, microvascular disease, and hemorrhage in the myeloproliferative neoplasms. Blood (2021) 137(16):2152–60. doi: 10.1182/blood.2020008109
3. Moliterno AR, Ginzburg YZ, Hoffman R. Clinical insights into the origins of thrombosis in myeloproliferative neoplasms. Blood (2021) 137(9):1145–53. doi: 10.1182/blood.2020008043
4. Marty C, Lacout C, Droin N, Le Couédic JP, Ribrag V, Solary E, et al. A role for reactive oxygen species in JAK2 V617F myeloproliferative neoplasm progression. Leukemia (2013) 27(11):2187–95. doi: 10.1038/leu.2013.102
5. Wolach O, Sellar RS, Martinod K, Cherpokova D, McConkey M, Chappell RJ, et al. Increased neutrophil extracellular trap formation promotes thrombosis in myeloproliferative neoplasms. Sci. Transl. Med. (2018) 10, 82–92. doi: 10.1126/scitranslmed.aan8292
6. Hasselbalch HC. Perspectives on chronic inflammation in essential thrombocythemia, polycythemia vera, and myelofibrosis: Is chronic inflammation a trigger and driver of clonal evolution and development of accelerated atherosclerosis and second cancer? Blood (2012) 119:3219–25. doi: 10.1182/blood-2011-11-394775
7. Hasselbalch HC. Chronic inflammation as a promotor of mutagenesis in essential thrombocythemia, polycythemia vera and myelofibrosis. A human inflammation model for cancer development? Leuk Res (2013) 37(2):214–20. doi: 10.1016/j.leukres.2012.10.020
8. Kiladjian JJ, Cassinat B, Chevret S, Fenaux P, Chomienne C, Rain JD. Pegylated interferon-alfa-2a induces complete haematological and molecular responses with low toxicity in polycythemia vera. Blood (2008) 112(11):1746. doi: 10.1182/blood-2008-03-143537
9. Silver RT, Kiladjian JJ, Hasselbalch HC. Interferon and the treatment of polycythemia vera, essential thrombocythemia and myelofibrosis. Expert Rev. Hematol. (2013) 6(1):49–58. doi: 10.1586/ehm.12.69
10. Kiladjian JJ, Giraudier S, Cassinat B. Interferon-alpha for the therapy of myeloproliferative neoplasms: Targeting the malignant clone. Leukemia (2016) 30(4):776–81. doi: 10.1038/leu.2015.326
11. Hasselbalch HC, Holmström MO. Perspectives on interferon-alpha in the treatment of polycythemia vera and related myeloproliferative neoplasms: Minimal residual disease and cure? Semin Immunopathol. (2018) 41(1):5–19. doi: 10.1007/s00281-018-0700-2
12. How J, Hobbs G. Use of interferon Alfa in the treatment of myeloproliferative neoplasms: Perspectives and review of the literature. Cancers (2020) 12:1954. doi: 10.3390/cancers12071954
13. Hasselbalch HC, Silver RT. New perspectives of interferon-alpha2 and inflammation in treating Philadelphia-negative chronic myeloproliferative neoplasms. HemaSphere (2021) 5(12):e645. doi: 10.1097/HS9.0000000000000645
14. Utke Rank C, Weis Bjerrum O, Larsen TS, Kjær L, de Stricker K, Riley CH, et al. Minimal residual disease after long-term interferon-alpha2 treatment: A report on hematological, molecular and histomorphological response patterns in 10 patients with essential thrombocythemia and polycythemia vera. Leuk Lymphoma. (2016) 57:348–54. doi: 10.3109/10428194.2015.1049171
15. Bjørn ME, Hasselbalch HC. Minimal residual disease or cure in MPNs? rationales and perspectives on combination therapy with interferon-alpha2 and ruxolitinib. Expert Rev. Hematol. (2017) 10(5):393–404. doi: 10.1080/17474086.2017.1284583
16. Gisslinger H, Klade C, Georgiev P, Krochmalczyk D, Gercheva-Kyuchukova L, Egyed M, et al. Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): A randomised, non-inferiority, phase 3 trial and its extension study. Lancet Haematol. (2020) 7:e196–208. doi: 10.1016/S2352-3026(19)30236-4
17. Barbui T, Vannucchi AM, De Stefano V, Masciulli A, Carobbio A, Ferrari A, et al. Ropeginterferon alfa-2b versus phlebotomy in low-risk patients with polycythaemia vera (Low-PV study): a multicentre, randomised phase 2 trial. Lancet Haematol (2021) 8:e175–84. doi: 10.1016/S2352-3026(20)30373-2
18. Jaiswal S, Fontanillas P, Flannick J, Manning A, Grauman PV, Mar BG, et al. Age- related clonal hematopoiesis associated with adverse outcomes. N Engl J Med (2014) 371:2488–98. doi: 10.1056/NEJMoa1408617
19. Cordua S, Kjaer L, Skov V, Pallisgaard N, Hasselbalch HC, Ellervik C. Prevalence and phenotypes of jak2 v617f and calreticulin mutations in a Danish general population. Blood (2019) 134:469–79. doi: 10.1182/blood.2019001113
20. Pedersen RK, Andersen M, Knudsen TA, Sajid Z, Gudmand-Hoeyer J, Dam MJB, et al. Data-driven analysis of JAK2V617F kinetics during interferon-alpha2 treatment of patients with polycythemia vera and related neoplasms. Cancer Med. (2020) 9(6):2039–51. doi: 10.1002/cam4.2741
21. Misaka T, Kimishima Y, Tokokawa T, Ikeda K, Takeishi Y. Clonal hematopoiesis and cardiovascular disease : role of JAK2V617F. J Cardiol (2022) 79:S0914–5087(22)00024-7. doi: 10.1016/j.jjcc.2022.02.001
22. Larsen TS, Christensen JH, Hasselbalch HC, Pallisgaard N. The JAK2 V617F mutation involves b- and T-lymphocyte lineages in a subgroup of patients with Philadelphia-chromosome negative chronic myeloproliferative disorders. Br. J. Haematol. (2007) 136(5):745–51. doi: 10.1111/j.1365-2141.2007.06497.x
23. Skov V, Riley CH, Thomassen M, KJær L, Larsen TS, Kruse TA, et al. Significantly upregulated thrombo-inflammatory genes are normoregulated or significantly downregulated during treatment with interferon-Alpha2 in patients with Philadelphia-negative chronic myeloproliferative neoplasms. Blood (2019) 134 (Supplement_1):2978. doi: 10.1182/blood-2019-131698
24. Skov V, Thomassen M, Kjær L, Ellervik C, Larsen MK, Knudsen TA, et al. Interferon-alpha2 treatment of patients with polycythemia vera and related neoplasms favourably impacts deregulation of oxidative stress genes and antioxidative defence mechanisms. PloS One (2022) 17(6):e0270669. doi: 10.1371/journal.pone.0270669
Keywords: JAK2V617F mutation, clonal hematopoiesis of indeterminate potential (CHIP), angina pectoris, recombinant interferon-alpha2, myeloproliferative neoplasms
Citation: Egyed M, Kajtar B, Foldesi C, Skov V, Kjær L and Hasselbalch HC (2022) Ropeginterferon-alfa2b resolves angina pectoris and reduces JAK2V617F in a patient with clonal hematopoiesis of indeterminate potential: A case report. Front. Hematol. 1:1005666. doi: 10.3389/frhem.2022.1005666
Received: 28 July 2022; Accepted: 29 August 2022;
Published: 26 October 2022.
Edited by:
Isabel Beerman, National Institutes of Health (NIH), United StatesReviewed by:
Reza Nejati, Fox Chase Cancer Center, United StatesMary Frances McMullin, Queen’s University Belfast, United Kingdom
Copyright © 2022 Egyed, Kajtar, Foldesi, Skov, Kjær and Hasselbalch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miklos Egyed, ZHJlZ3llZG1pa2xvc0B5YWhvby5jb20=