 Ambareen Main Thompson
Ambareen Main Thompson Sheikh Mohd Saleem
Sheikh Mohd Saleem
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Health Serv., 05 February 2025
Sec. Mental Health Services
Volume 4 - 2024 | https://doi.org/10.3389/frhs.2024.1471528
Pakistan confronts a severe mental health crisis that compels urgent action. Mental disorders constitute a burgeoning global burden, with depression alone accounting for a staggering 4.4% of worldwide Disability-Adjusted Life Years (DALYs) (1). A stark inequity persists, with over 90% in low- and middle-income nations lacking access to mental health treatment, compared to over 50% receiving care in high-income countries (2). These disparities emanate from a chronic underinvestment, with low-income nations allocating a mere fraction, less than 1% of health budgets, to mental health (3).
Pakistan mirrors these global inequities. With a paucity of just 0.19 psychiatrists per 100,000 people (4), and an underwhelming allocation of only 0.4% of the health budget for mental health (5), Pakistan grapples to meet the needs of an estimated 24 million individuals requiring mental health services (6). Depressive, anxiety, and schizophrenia disorders are the most prevalent (7). Stigma surrounding mental illness remains an entrenched societal challenge (8).
Currently, Pakistan's mental health system operates primarily through tertiary care hospitals in major cities, with minimal integration into primary healthcare. Mental health services are largely concentrated in psychiatric departments of teaching hospitals, creating geographic and economic barriers for rural populations. The existing system relies heavily on psychiatrists and clinical psychologists, with limited involvement of general physicians, community health workers, or other non-specialist providers. Mental health education is notably absent from school curricula, and workplace mental health programs are virtually non-existent. Digital mental health solutions remain unexplored within the public sector, while community-based mental health services are severely limited. The proposed transformations would mark significant departures from this status quo through: task-sharing with non-specialist providers instead of exclusive specialist care; integration of services into primary healthcare facilities rather than tertiary hospitals alone; establishment of community clinics in place of centralized urban facilities; leveraging digital technology where traditional in-person care is the norm; and engaging community partners vs. the current isolated clinical approach.
To expand access, the WHO recommends strategies such as task-sharing care to non-specialist providers, integrating services into primary care and educational institutions, developing community clinics, leveraging digital technology, and engaging community partners (9). Pakistan could adapt approaches like training primary care workers in mental health protocols, building teacher capacity for school-based services, deploying lay counselors with specialist supervision, offering telemental health services, and engaging community health workers in outreach efforts (10) (Figure 1).
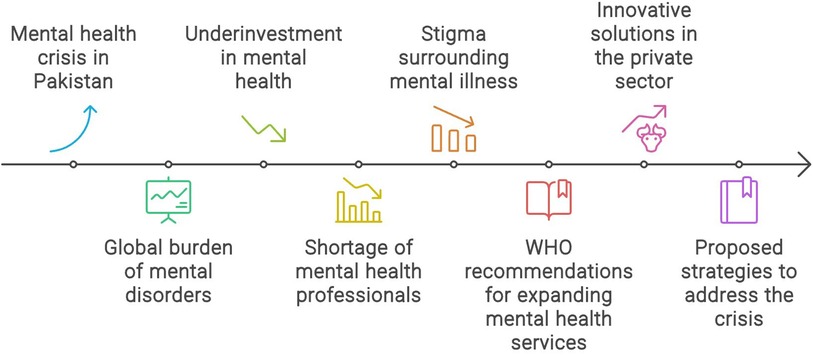
Figure 1. Factors accociated with mental health crisis in Pakistan.
Amidst public sector constraints, Pakistan's private sector pioneers innovative solutions. NGOs like SINA- Health Education and Welfare trust conduct grassroots awareness campaigns, integrate mental health into community clinics, utilize telepsychiatry and digital tools, and address social determinants through campaigns on gender equity (11). Organizations like Pakistan Institute of Living and Learning (PILL) advocate for policies, build workforce capacity, and scale up culturally-adapted interventions (12). Digital startups like Sehat Kahani use telepsychiatry and mobile applications to bridge the workforce gap (13).
A critical component in addressing Pakistan's mental health crisis is the implementation of comprehensive anti-stigma campaigns (14). These initiatives should operate at multiple levels based on established evidence (15) (Figure 2):
A. Community-level interventions (14, 15):
(a) Engaging religious leaders and community elders to challenge traditional misconceptions
(b) Training community health workers to provide accurate mental health information
(c) Organizing community dialogue sessions and support groups
(d) Using local media and art forms to share stories of recovery and hope
B. Educational initiatives (9, 16):
(a) Incorporating mental health literacy into school curricula
(b) Training teachers to recognize and respond to mental health concerns
(c) Creating safe spaces for students to discuss mental health
(d) Engaging parents through awareness programs
(a) Partnering with media outlets to promote responsible reporting on mental health
(b) Creating public service announcements featuring respected public figures
(c) Using social media platforms to reach younger populations
(d) Developing culturally sensitive content in local languages
D. Workplace programs (9, 16):
(a) Implementing mental health awareness training in organizations
(b) Establishing employee assistance programs
(c) Creating supportive workplace policies
(d) Reducing discrimination in employment practices
Research suggests such comprehensive anti-stigma campaigns can lead to (14, 15):
• Increased help-seeking behavior
• Earlier intervention and better outcomes
• Reduced discrimination
• Greater social support for individuals with mental health conditions
• Improved public understanding of mental health**
To comprehensively address the crisis, Pakistan must invest in scaling up its mental health workforce through training more specialists and task-sharing to non-specialists (3, 16). Integrating services into primary care and establishing community mental health centers is crucial for decentralizing access (9, 10). Increasing public mental health spending, developing sustainable financing mechanisms, and strengthening governance and policies are imperative (5, 16). Research on effective, contextually-appropriate interventions should guide investments (14). Developing quality monitoring mechanisms is key to ensuring standards of care (9).
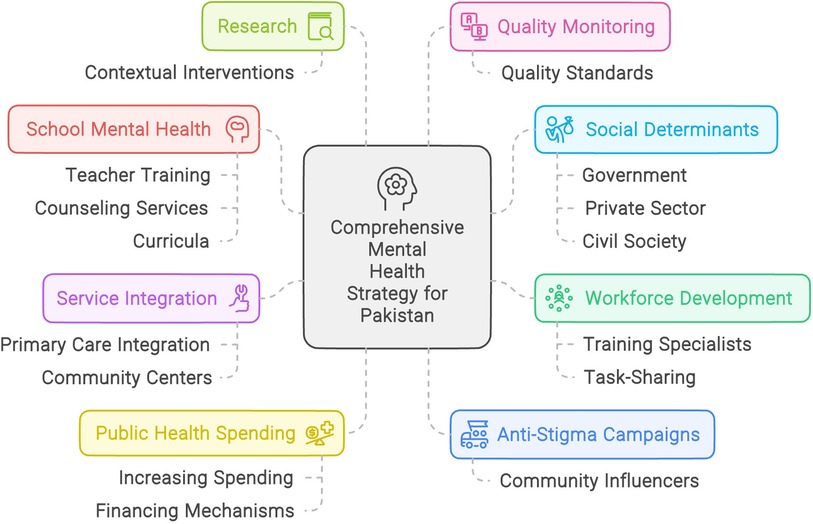
Figure 2. Mental health strategy for Pakistan.
Addressing social determinants through multi-sectoral coordination and whole-of-society approaches involving government, private sector, and civil society is vital (14). Sustained political commitment and strategic investments enabling universally accessible, community-based mental healthcare are crucial for realizing wellbeing for all Pakistanis (15, 16).
In essence, Pakistan confronts a formidable treatment gap with escalating rates of mental illness amid extreme limitations in mental health system capacity. Comprehensive strategies are necessitated, spanning workforce expansion, service integration into communities, increased financing, anti-stigma efforts, school interventions, research, quality assurance, and multi-sectoral coordination. While challenges are immense, prioritizing community-driven, decentralized mental health systems can ensure no individual is left behind on the path to greater wellbeing.
AT: Conceptualization, Funding acquisition, Investigation, Project administration, Writing – original draft. SS: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Collaborators GMD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. (2022) 9(2):137–50. doi: 10.1016/S2215-0366(21)00395-3
2. Kakuma R, Minas H, Van Ginneken N, Dal Poz MR, Desiraju K, Morris JE, et al. Human resources for mental health care: current situation and strategies for action. Lancet. (2011) 378(9803):1654–63. doi: 10.1016/S0140-6736(11)61093-3
3. World Health Organization. Mental Health Atlas 2017. Geneva: WHO (2018). Available online at: https://www.who.int/publications/i/item/mental-health-atlas-2017 (Accessed January 30, 2025).
5. Alvi MH, Ashraf T, Kiran T, Iqbal N, Gumber A, Patel A, et al. Economic burden of mental illness in Pakistan: an estimation for the year 2020 from existing evidence. BJPsych Int. (2023) 20(3):54–6. doi: 10.1192/bji.2023.4
6. Meghrajani VR, Marathe M, Sharma R, Potdukhe A, Wanjari MB, Taksande AB. A comprehensive analysis of mental health problems in India and the role of mental asylums. Cureus. (2023) 15(7):e42559. doi: 10.7759/cureus.42559
7. Alvi MH, Ashraf T, Naz F, Sardar A, Ullah A, Patel A, et al. Burden of mental disorders by gender in Pakistan: analysis of global burden of disease study data for 1990–2019. BJPsych Bull. (2023) 48(6):1–8. doi: 10.1192/bjb.2023.76
8. World Health Organization. WHO Pakistan celebrates World Mental Health Day. Cairo: WHO Regional Office for the Eastern Mediterranean (2023). Available online at: https://www.emro.who.int/pak/pakistan-news/who-pakistan-celebrates-world-mental-health-day.html (Accessed January 30, 2025).
9. World Health Organization. Mental Health, Human Rights and Legislation: Guidance and Practice. Geneva: WHO (2021). p. 58–63. Available online at: https://www.who.int/publications/i/item/9789240031029 (Accessed January 30, 2025).
10. Islam A. Health sector reform in Pakistan: future directions. J Pak Med Assoc. (2002) 52(4):174–82.12174483
14. Waqas A, Naveed S, Makhmoor A, Malik A, Hassan H, Aedma KK. Social stigma and mental health in Pakistan: a systematic review. Community Ment Health J. (2020) 56:65–74. doi: 10.1007/s10597-019-00459-9
15. Mehran N, Afzal S, Rafique I, Hussain S. A systematic review of mental health literacy interventions in Pakistan. Int J Ment Health Syst. (2022) 16(1):1–12. doi: 10.1186/s13033-021-00510-x
16. Sustainable Development Policy Institute. Analyzing Health Budget 2023 in Context of Wellbeing of People. Islamabad: SDPI (2023). Available online at: https://sdpi.org/analyzing-health-budget-2023-in-context-of-wellbeing-of-people/news_detail (Accessed January 30, 2025).
Keywords: mental health, mental health crisis, multifaceted approach, multisectorial collaboration, primary health care, treatment gaps
Citation: Main Thompson A and Saleem SM (2025) Closing the mental health gap: transforming Pakistan's mental health landscape. Front. Health Serv. 4:1471528. doi: 10.3389/frhs.2024.1471528
Received: 27 July 2024; Accepted: 30 December 2024;
Published: 5 February 2025.
Edited by:
Daniel John Alexander Devoe, Mount Royal University, CanadaReviewed by:
Samantha Brady, University of York, United KingdomCopyright: © 2025 Main Thompson and Saleem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheikh Mohd Saleem, c2FsZWVtLjkwMEBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.