 Junying Li
Junying Li Lan Zhang1,†
Lan Zhang1,† Hui Jiang
Hui Jiang- 1Nursing Department, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai, China
- 2Outpatient Office, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai, China
Background: The promotion of breastfeeding is an important strategy to prevent neonatal death and improve maternal and infant health. But Chinese efforts to improve breastfeeding practices have not been particularly effective. There is still a long way to go to achieve the national health development goals. We aimed to explore the maternal demand for breastfeeding guarantee policy in China and to determine the impact of a range of socio-demographic and neonatal-related variables on breastfeeding guarantee policy demand.
Methods: The study was carried out in the Obstetrics and Gynecology hospital of Shanghai, one of China's earliest provincial and municipal maternal and child health care institutions. From June to November 2021, 1,292 women were recruited for the cross-sectional study in child health clinic. We collected relevant socio- demographic and neonatal-related data. Maternal breastfeeding needs were measured through a self-designed questionnaire on breastfeeding guarantee policy demands of mothers.
Results: The mean score of breastfeeding guarantee policy demand was 4.42 ± 0.51. There were statistically significant differences in the effects of maternal age, education level, family income per capita (Yuan), medical payment type, baby age, work status, and current feeding methods on the demand for breastfeeding guarantee policies (P < 0.05). Multiple linear regression analyses showed that higher education level (B = 4.437, P < 0.001), baby age (B = 2.150, P = 0.002), and current feeding methods (B = 2.754, P = 0.005) were significantly associated with a higher demand for a breastfeeding guarantee policy, the effect of medical payment type is the most influencing factor (B = −7.369, P < 0.001).
Conclusions: The maternal needs for breastfeeding guarantee policy are multi-faceted and urgent. In the process of improving and implementing policies, the government and relevant departments should take into account the actual needs of women who have different education levels, baby ages, family economics, and feeding methods.
1 Background
Breastfeeding is the gold standard for neonatal and infant feeding, and breastfeeding is the best form of nutritional supply early on in human life (1). The World Health Organization (WHO) and the United Nations International Children's Emergency Fund (UNICEF) recommend that children start breastfeeding within one hour of birth, and exclusively breastfeed for six months, and suggest sustainable breastfeeding until the child is two years old or older (2). Breastfeeding plays an important role in ensuring the health and survival of mothers and babies. However, global rates of breastfeeding and exclusive breastfeeding remain low. According to the UNICEF global database, as of 2020, only about 48% of infants worldwide are breastfed within one hour of birth, and the average rate of exclusive breastfeeding for infants aged 0–5 months is 44% (1). The rate of exclusive breastfeeding within the first six months is 28.6% in Mexico, 18.8%−55.0% in the United States and 29.0% in Australia, but only 21% in China (3–5).
In order to improve the national breastfeeding behavior in China, all parties have made a series of efforts, such as medical institutions providing professional breastfeeding knowledge (e.g., lack of lactation, engorgement), skills (e.g., breastfeeding position, latch) and personalized care (e.g., skin to skin, room-in, milk expression) (6, 7), and the community providing support through telephone follow-up, peer education, and family counseling (8, 9), as well as other support through mobile medical and psychological interventions (10, 11). The results were mixed. However, the research on maternal and infant rights and breastfeeding-related safeguarding policies is not widely used.
Breastfeeding is the biological natural ability of almost all mothers, but in real social life, breastfeeding behavior is often restricted by a variety of influencing factors, among which policy factors often play a guiding role (12). Research has shown that health worker counselling and guidance are the relatively most visible policy measures and guidelines affecting infant feeding (13).
Increased maternity leave is strongly associated with long-time breastfeeding (14), and ensuring no less than six months of paid maternity leave can increase breastfeeding rates by 8.9% (15). In addition, the continued breastfeeding rate among women after returning to work will also greatly increase when maternity leave is paid or child care and support are provided (16). Moreover, the workplace providing private breastfeeding spaces can also effectively reduce the breastfeeding barriers of working women (17). In Alabama, United States, the local Department of Public Health has created a number of “baby cafes” with the support of the Breastfeeding Council to provide a good social space for breastfeeding (18). The Brazilian government has initiated a breastfeeding promotion plan to publicize the importance of breastfeeding through the mass media, making the public aware of the urgency of increasing breastfeeding rates and controlling the promotion and marketing of breastmilk substitutes, such as formula milk. It has also achieved impressive results in promoting breastfeeding behavior (19).
In China, the government has gradually attached the importance of promoting and developing of breastfeeding since the 1980s. In 1990, the Ministry of Health clearly proposed to carry out extensive breastfeeding education and scientific research, and established 5.20 every year as the National breastfeeding promotion day (20). Since 1992, in response to the WHO's call, China has begun to promote the construction of baby-friendly hospitals and then actively formulated and implemented the “Measures for the Administration of Marketing of Breastmilk Substitutes” (1995) and the “Measures for the Implementation of the Maternal and Infant Health Law”. In the second revision of the “Maternal and Child Health Law of the People's Republic of China” in 2017, the maternal and child health care part includes: maternal and child health guidance; pregnant women care (provide pregnant women with health/nutrition/psychological consultation or guidance as well as regular prenatal examination); fetal health care and newborn health care (21).
In June 2021, the State Council officially issued a decision on optimizing childbirth policies to promote long-term balanced population development, and the three-child policy was proposed. And in the “Outline for Women's Development in China (2021–2030)” and “Outline on the Development of Chinese Children (2021–2030)”, they are proposed that employers should strengthen the protection of breastfeeding support for female employees, such as strengthening the protection of breastfeeding, providing time and space for breastfeeding, and ensuring maternity leave according to law; in terms of children's health care, it is proposed to encourage and promote medical institutions to set up “pregnant women schools”, parent classes and other popular science education activities; emphasizing the management of baby-friendly hospitals, expanding the number and coverage of maternal and infant facilities, and striving to achieve the target of 50% exclusive breastfeeding of infants within 6 months (22). In November of the same year, the state released for the first time a plan aimed only at promoting breastfeeding actions-“Notice on Printing and Distributing the Breastfeeding Promotion Action Plan (2021–2025)”, which started from building a social breastfeeding promotion network; focusing on breastfeeding consultation and guidance during pregnancy, childbirth, and breastfeeding; exploring the unique advantages of traditional Chinese medicine in breastfeeding promotion (23).
In addition, in order to better protect the rights of women and children, according to the “Special Rules on the Labor Protection of Female Employees”, female employees can enjoy 98 days of paid maternity leave, including prenatal leave 15 days. And each local government has made different local provision on female workers maternity leave and related treatment though the local “population and family planning management regulations”, with an average maternity leave of 158 days and 15 days for male paternity leave (24). The promulgation and implementation of these policies aroused widespread repercussions in society at that time and played a significant role in increasing the breastfeeding rate in China.
Although the Chinese government has made decades of efforts to improve breastfeeding practices, the current breastfeeding guarantee policies do not match the needs of the masses, and the relevant implementation is not yet in place. In the real social environment, it is difficult to achieve qualitative changes to greatly increase the exclusive breastfeeding rate and achieve the goal of “Healthy China 2030”, which, in the absence of breastfeeding-related hardware security facilities, means creating documents and leading efficient publicity. Therefore, in view of the current situation of breastfeeding in China, it is of practical significance to carry out relevant research from the perspective of a breastfeeding security policy.
Therefore, this study focuses on the strong driving effect of policy factors on breastfeeding, also, explores the needs of mothers for a breastfeeding guarantee policy and examined other relevant factors through a literature review and preliminary qualitative research. The study further proposes corresponding countermeasures and suggestions according to the voices of maternity in order to provide a reference for breastfeeding-related clinical treatment, as well as nursing and social intervention strategies. Also, the results are useful in the promotion of maternal and infant health and in efforts aimed at increasing the breastfeeding rate.
2 Methods
2.1 Design
This was a quantitative analytic study using a cross-sectional survey.
2.2 Setting
The study was carried out in Shanghai, one of China's largest cities and economic centers. The subjects were recruited from one of the Third-A-Class obstetrics and gynecology hospitals, which is one of the earliest provincial and municipal maternal and child health care institutions in China. It has more than 800 beds and a maximum annual delivery capacity of 30,000 (Shanghai First Maternity and Infant Hospital, 2020, and is known as the cradle of the new life in Shanghai). The convenience sampling method was used to find potentially suitable participants. The potential subjects had the right to refuse or withdraw from their participation in the study at any time. Importantly, they did not face any reprisal for doing so.
2.3 Ethical considerations
The study received ethical approval from the hospital's Institutional Review Board (KS21217). After informed consent was obtained from the subjects, women filled in an anonymous electronic questionnaire using their smartphone under the guidance of researchers. And the research purpose, significance, potential impact, and confidentiality of personal information were communicated to subjects in the participant information interface. All methods were performed in accordance with the relevant guidelines and regulations including the Declaration of Helsinki.
2.4 Recruitment and sampling
From June to November 2021, maternity women were recruited for the study during routine clinical physical examinations of neonates in the postpartum period (usually 0–24 months postpartum). The convenience sampling method was used to find potentially suitable participants. The inclusion criteria for the sample were as follows: women were at least 20 years old; full-term; live birth (gestation ≥37 weeks); the babies were aged 0–24 months; and the women voluntarily agreed to participate in the study. The exclusion criteria were women who had a history of mental illness and breastfeeding contraindications; used drugs that affect lactation; or their babies had congenital malformations; or refused to participate to the study.
We calculated the sample size according to the sample size calculation formula of the descriptive study design cross-sectional survey (25), taking α = 0.05, the allowable error δ = 3%. The exclusive breastfeeding rate within 6 months was 21% in China, according to the literature review (π = 21%). The sample size was calculated to be 710 cases. Taking into account the loss and failure of samples, the sample size was increased by 15%, and the final sample size was 820 cases.
2.5 Study design and the survey
2.5.1 Research instrument
This study is guided by the theory of policy tools and based on the classification introduced by Rothwell and Zegveld, which divides policy tools into three types: supply type, demand type, and environmental type (26). The first two types of policy tools directly promote the development of breastfeeding, and environmental policy tools have an indirect guiding role. It simplifies the complex policy system, not deliberately emphasizing the coercion of the government but rather highlighting the leading environmental role of relevant departments in promoting the development of a certain field.
Based on the policy tool theory, our research group created the questionnaire to assess the need of policy support, and named it the “Breastfeeding Guarantee Policy Demands of Mothers questionnaire”. According to Chinese national conditions and the medical environment, the initial item pool of the questionnaire was determined based on a literature review and previous qualitative research, and adapted by senior obstetricians, neonatologists, international lactation consultants, and senior clinical nurses. Finally, all of the above agreed on the final version of the questionnaire in terms of its content and face validity. The Cronbach' s α was 0.968 overall.
2.5.2 The socio- demographic characteristics
When women took their babies to the child health care clinic for evaluation, the researchers collected the following mothers' and babies' data: age, education, work situation, family economy, baby age, current feeding method (exclusive breastfeeding, mixed feeding, formula feeding), maternity leave time, paternity leave time.
2.5.3 Breastfeeding guarantee policy demands of mothers questionnaire
The questionnaire includes three dimensions: supply-type policy need, demand-type policy need, and environmental policy need, involving medical institution support, the construction of baby care rooms, workplace support, government support, maternity leave support, cultural breastfeeding publicity, and management of breast milk substitutes. There were seven aspects of such requirements and a total of 45 items. We used a 5-point Likert scale (1 = “no need at all”, 2 = “not a very strong need”, 3 = “general need”, 4 = “moderate need”, 5 = “strong need”), with a total score of 0–225. The total score was obtained by summing the item scores, the higher the score, the higher the demand of the mother for breastfeeding protection policies, and the higher the possibility of further promotion of breastfeeding. The Cronbach' s α of each dimension was between 0.827–0.965, and the average content validity of the questionnaire was 0.98, revealing excellent internal reliability and validity.
2.6 Data analysis
Data were entered with Excel 2016 and analyzed with IBM SPSS Statistics 21.0. The general data of the research subjects are described by frequency, percentage, means (M) and standard deviation (SD). The maternal demand for breastfeeding guarantee policies is presented as the M and SD. The normality test of the data shows that the score distribution of maternal demand for breastfeeding guarantee policies is non-normal. Thus, this paper used the statistical analysis method of a non-parametric test to compare the difference of the maternal demand for breastfeeding guarantee policies. We used a multiple linear regression analysis to explore the relationship between influencing factors and demand. All statistics were performed using a two-sided test, the test level was α = 0.05, and the statistical significance was set a P-value <0.05.
3 Result
3.1 Sample characteristics
The characteristics of the participants are shown in Table 1. We contacted 1,503 participants, some of whom chose to drop out due to other reasons, such as time or health constraints, missing questionnaires, or a filing time that was too short. Finally, we collected 1,292 cases from whom questionnaires were recovered, with an effective recovery rate of 85.96%. The average maternal age was 30.76 ± 3.54. In total, 68.8% of participants had a bachelor's degree or higher, 78.8% were primiparas, 17.5% of babies were ≥4 months old, and the rate of those who exclusively breastfed was 45.9%. Also, 64.65% of the maternity were working (including freelancers), and most of them were still taking maternity leave. Full-time mothers accounted for 15.7%, but 16.1% of the participants said they didn't know whether they had maternity leave, 31.0% of the maternity didn't know whether they had breastfeeding leave, 11.4% said they did not have breastfeeding leave, 22.1% did not know whether their spouses had paternity leave, and 9.7% said that their spouses did not have paternity leave.
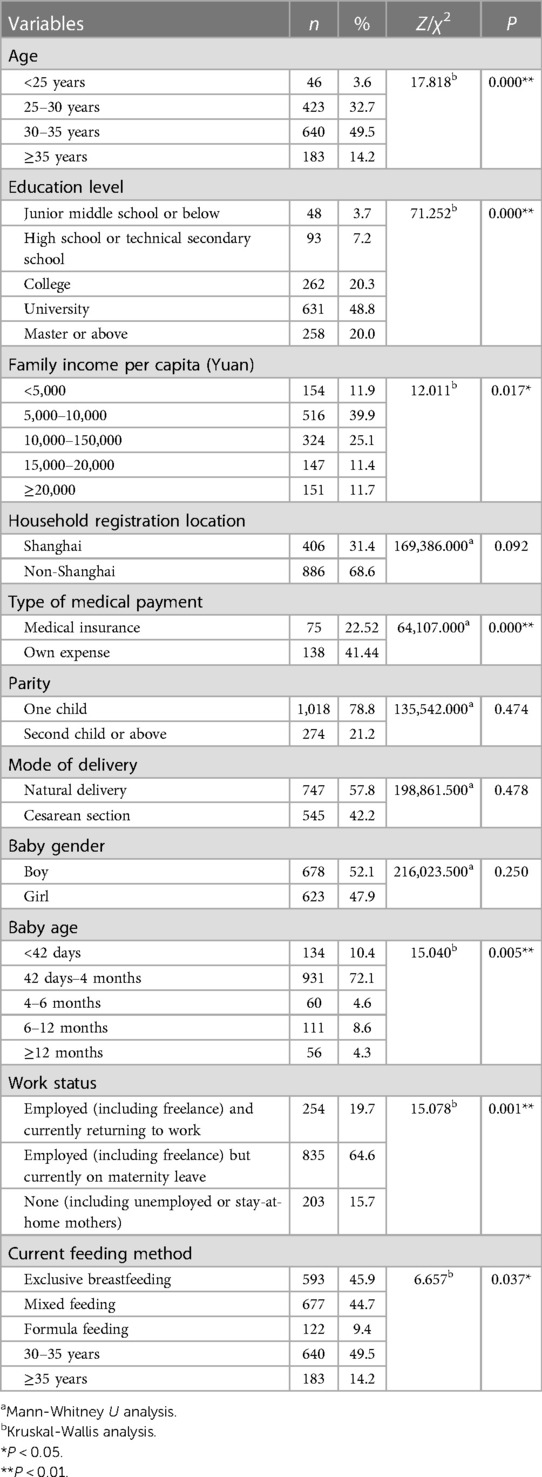
Table 1. Comparison of maternal demand for breastfeeding guarantee policies among different socio- demographic characteristics (n = 1,292).
The mean maternity leave was 130.31 ± 13.79 days, with a median of 128 days (four months); the actual breastfeeding leave was 1.6 ± 0.60 h per day, with a median of one hour per day, the expected duration of breastfeeding leave was 2.26 ± 0.94 per day, and the median time was two hours per day; the average length of paternity leave currently enjoyed by their spouses was 12.44 ± 9.03 days, with a median of ten days, and a median expected paternity leave duration of 30 days.
Table 1 shows the influencing factors of the maternal demand for a breastfeeding guarantee policy among different socio- demographic groups. There were seven variables that had an impact on breastfeeding guarantee policy scores, namely age, education, family income per capita (Yuan), type of medical payment, neonatal age in months, work status, and current feeding methods (P < 0.05, Table 1).
3.2 Maternal demand score for breastfeeding guarantee policy
Table 2 presents the scores of the maternal demand for a breastfeeding guarantee policy. The total score of all items was 198.70 ± 22.97, and the average score was 4.42 ± 0.51 between having a need and a strong need. The supply-type policy need had the highest score; the average score was 4.53 ± 0.51 and the lowest score was found for the environmental policy need, with an average score of 4.24 ± 0.58. In each sub-dimension score, the highest score was found for the demand for the Baby care rooms support (4.7 ± 0.53), followed by the demand for maternity leave support (4.59 ± 0.66), while the lowest score was found for the demand for breastmilk substitute management (4.09 ± 0.80), which showed a significant difference. Table 3 presents the five items with the highest and lowest scores in the questionnaire.

Table 2. The score of maternal demand for breastfeeding guarantee policy (n = 1,292).
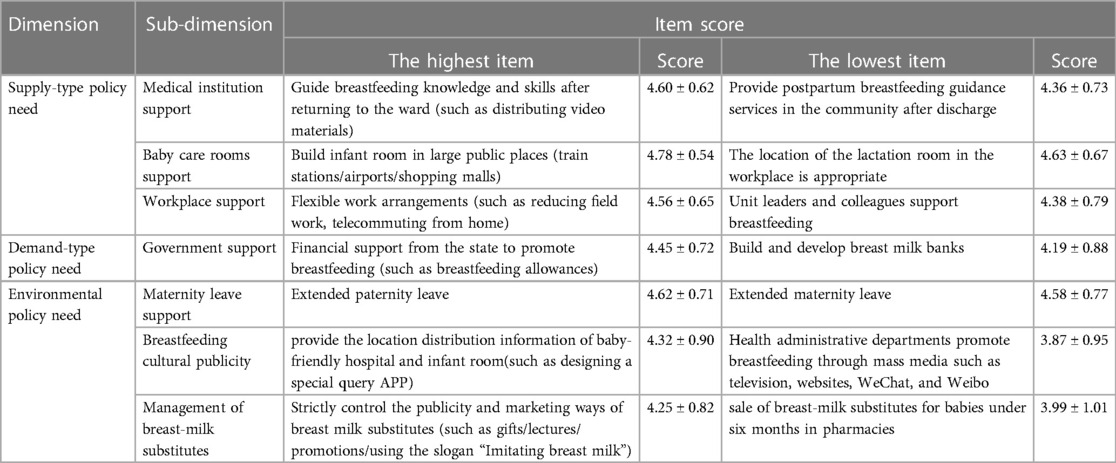
Table 3. The highest and lowest scores for each dimension of breastfeeding guarantee policy demands ().
3.3 Factors for maternal demand score for breastfeeding guarantee policy
For a better interpretation of the multiple linear regression analysis, the independent variable assignment method is shown in Table 4. Table 5 shows that a higher maternal demand for breastfeeding policy scores was significantly associated with education (B = 4.437, P < 0.001), neonatal age in months (B = 2.150, P = 0.002), and current feeding methods (B = 2.754, P = 0.005). The type of medical payment is the most influencing factor to the higher demand for breastfeeding guarantee policy (B = −7.369, P < 0.001).
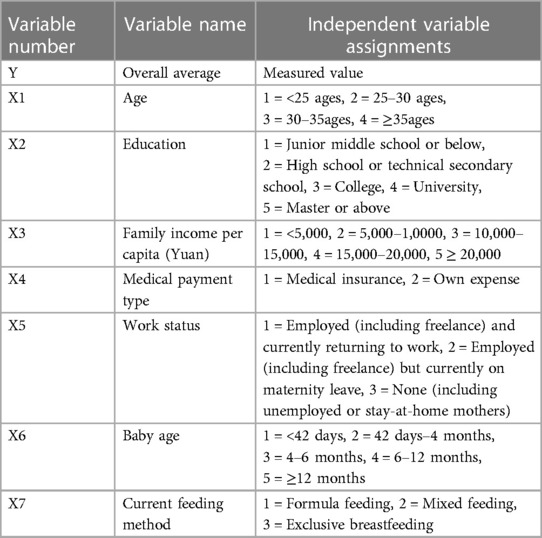
Table 4. Multiple linear regression analysis of independent variable assignments on maternal demand for breastfeeding guarantee policy.
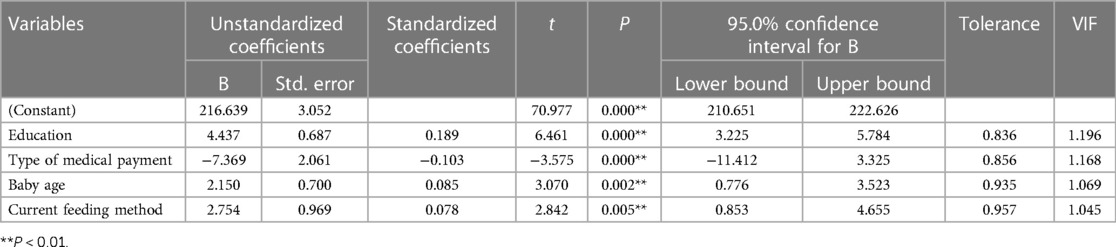
Table 5. Multiple linear regression analysis of factors associated with maternal demand for breastfeeding guarantee policy.
4 Discussion
4.1 High overall demand score
The implementation and development of breastfeeding guarantee policies are beneficial in promoting the growth and development of infants and improving immunity (27). In May 2021, after China's “Three-child Policy” was proposed, the “Decision of the Central Committee of the Communist Party of China and the State Council on Optimizing the Birth Policy to Promote Long-term Balanced Population Development” (hereafter referred to as the “Decision”) clearly mentioned the promotion of prenatal and postnatal care and the implementation of breastfeeding promotion (28). Maternal mothers have certain needs for breastfeeding knowledge, skills, duration of breastfeeding, and breastfeeding support at the social level (29, 30) similar to the results of this study. Breastfeeding policy could improve maternal women breastfeeding competency, which directly or indirectly affects breastfeeding behaviors. The Vietnamese government's integration of high-quality interpersonal counseling services into health system services has greatly improved the breastfeeding rate in the country (31). Alabama Breastfeeding Commission (ABC) developed breastfeeding services in the community. This service was developed in the form of lactation group during the perinatal period, aiming to solving feeding problems at the grassroots level and form a support network. It did a great job of improving breastfeeding practices in Alabama (32).
4.2 Urgent need for construction of baby care room
It is undeniable that constructing baby care rooms in public places is one of the important symbols of social civilization. Following the “Two-child Policy”, China has implemented the “Three-child Policy”, which will undoubtedly bring increased fertility, and the society's demand for childbearing support will also increase day by day. It has been documented that having a well-equipped nursing space and adequate nursing time increases the likelihood of breastfeeding by 2.3 times for working women (33). The results of our study showed that women have the highest scores for the item of “construct a baby care room in large public places (such as train stations/airports/shopping malls)” and “protect the privacy in breastfeeding spaces”, which indicated that women urgently need sufficient and quality-assured baby care rooms to support their breastfeeding. The findings of this study are similar to those of Ahmad et al., they found that women desired to continue breastfeeding after working if employers could provide facilities and flexible hours for expressing milk during working hours (34). The addition of the “Baby Cafe” in Alabama provides a good social space for the implementation and communication of breastfeeding (32). The Australian government's welcoming breastfeeding programme in public spaces has had a positive impact and increased public awareness of breastfeeding (35). However, compared with the mature and user-friendly standards for the equipment of baby care rooms in foreign countries (36), there are obvious deficiencies in the planning, equipment, and management of public facilities, such as baby care rooms in China.
4.3 Valuing the support needs of medical institutions
The postnatal breastfeeding experience during hospitalization is a key factor influencing lactation and the continuation of breastfeeding (37). Our study showed that breastfeeding is a behavior that requires study and support, especially for primiparas. Medical professionals are their most trusted group, and women are eager to acquire breastfeeding-related knowledge and skills from them. Nieuwoudt pointed out that consultation and guidance from health worker are the most obvious policies and guideline for infant feeding (13). Some studies have found that strengthening counseling and attention to maternal psychology at hospital level was important to promoting breastfeeding. It can help to learn their real need, also, avoid forced or mechanical feeding (38). Also, maternity trust that medical staff will pay close attention to their own emotional and psychological changes, rather than just paying attention to the newborn.
However, in the reality of busy clinical work, medical staff often neglect this. Therefore, medical staff should focus on communicating with maternity to understand their real needs using methods to encourage them to continue breastfeeding, such as sharing knowledge and imparting experience and skills (39). This should be done in an effort to improve the quality of nursing care for clinical breastfeeding.
Coincidentally, the study also found that most women had a low demand for prenatal education and community support for breastfeeding. Studies have also shown that maternal lack the prospective awareness of breastfeeding, mainly because of their lack of insight into breastfeeding (29). They are unprepared for the potential difficulties of breastfeeding, and cannot imagine the gap between breastfeeding ideal and reality.
Prenatal education and community-based health care services in China are still in the exploratory stage. Most women have insufficient awareness of prenatal education and community support, and some even think that it is unnecessary. The qualitative interview previously conducted also verified this result (40). However, national and international studies have proven that prenatal education has a significant effect on improving women's breastfeeding willingness, postpartum lactation initiation, and breastfeeding rate (41, 42). Developing community support for breastfeeding cannot only effectively relieve the pressure of medical treatment and follow-up in major hospitals but also systematically manage continuous maternal care services and save medical resources, thereby effectively protecting the rights and interests of mothers and babies (43, 44). Therefore, how to balance maternal breastfeeding demands and practical problems in work, and improve the ways to support education, are one of the directions of future research.
4.4 Emphasizing government support needs, but low demand for content beyond traditional concepts
Government support for breastfeeding significantly improves the initiation and continuation of breastfeeding. Study has shown that government financial support has had an important impact on the development of baby-friendly hospital initiatives and the promotion of breastfeeding (45). In Mexico, government leaders emphasized the need to increase the budget for the Integrated Nutritional Nursing Strategy health work, develop breastfeeding funds, and use maternity allowances (46). However, in China, financial support has not followed up and incentives have not been developed, while the government has chosen to make breastfeeding a priority for development, as this study also confirms.
Our study further finds the interesting result that the item of “build and develop breast milk banks” has the lowest score. Maybe other women's milk is often regarded as “unclean”, “carrying genetic disease”, or “dirty” in traditional Chinese concepts. It is difficult for most mothers to accept donated breast milk from the breast milk bank, both psychologically and physically. In 1980, both the WHO and UNICEF had proposed that the first choice for a baby's food source is donor milk when the mother cannot breastfeed herself (47). However, the first breast milk bank in China was built in 2013, and it is still in its infancy (48). It is undeniable that the development of breast milk banks plays a very important role in promoting breastfeeding, especially in improving breastfeeding and the prognosis of premature infants. Therefore, future research should vigorously develop and promote the use of breast milk banks on an evidence-based basis. This may lead more Chinese women to accept and be willing to use donor milk and ensure the proper nutrition of infants and young children.
4.5 Strong need for childbirth leave protection
In this study, mothers had a higher demand for extended maternity leave, breastfeeding leave, and paternity leave. For nearly half a century, growing academic research has focused on the important role of fathers in fertility and infant care (49, 50). The research of Petterson et al., show that both genders expressed interest in expanded paid maternity and paternity leave (51). Some organizations' leaders in the field have suggested that increasing paid childbirth leave could improve new parents experience and breastfeeding policies well (52, 53). Fathers' fulfillment of their roles and responsibilities has a positive predictive effect on the establishment and growth of children's positive parent-child relationships (54). The international community is also legally requiring and encouraging men to participate in family affairs, maternity care and childcare work, so as to promote the joint commitment of reproductive affairs (54). However, in real life, the phenomenon of a “lack of fatherhood” has become a common problem in society. Therefore, calls for an extension of paternity leave and an improvement fathers' awareness and quality of parenting deserve more extensive attention and support.
Furthermore, the vast majority of working women need to return to work within six months postpartum, which is the main obstacle for them to adhere to breastfeeding (55). In China, women are entitled to 98 days maternity leave, while the expected maternity leave was 233.87 ± 115.87 days, with a median of 180 days (six months) in the study. A study in the USA showed that the length of maternity leave was positively associated with duration of breastfeeding (56). Lactating women were less likely to continue breastfeeding when they return to a full-time job. Also, it has been reported that for each additional month of paid maternity leave, the prevalence of early initiation of breastfeeding increases by seven percentage points, the prevalence of exclusive breastfeeding for six months increases by approximately six percentage points, and the duration of breastfeeding increases by two months. Therefore, it is necessary for China to extend the three periods of leave for pregnancy, maternity, and breastfeeding, add parental leave, while also improving maternity leave and maternity insurance systems.
4.6 Low need for breastfeeding promotion and management of breastmilk substitutes
With the ongoing development of Internet, the information about breastfeeding that people have learned is mixed, and some induced consumption has seriously affected their choice of breastfeeding. Our results found that the maternal demand for cultural breastfeeding publicity was significantly lower. In their opinion, they have suffered substantial pressure to breastfeed, particularly in relation to the traditional parenting concepts of elders, physiological factors (such as nipple pain, fatigue, anxiety), and insufficient milk production have added pressure to their breastfeeding. If breastfeeding is promoted again, it will increase feeding anxiety and might be detrimental to mental health (57, 58). However, the vast majority of mothers lack scientific knowledge about breastfeeding, especially primiparas. Therefore, it is necessary to strengthen scientific publicity on breastfeeding to help women and their families fully understand breastfeeding (such as the benefits, difficulties, and methods) in order to help them to make the right feeding decision.
Many studies have pointed out that the promotion and marketing of breast milk substitutes is also a major reason for breastfeeding (59). This study found that women want tighter control of the marketing of breast milk substitutes, but the items “sale of breast milk substitutes for babies under six months in pharmacies” and “infants under six months of age require a pediatrician's permission to add formula” had lower scores. It is not difficult to see that mothers have a high demand for regulating the marking of breast milk substitutes, but they do not want to reduce their own right to choose breast milk substitutes. It is reported that at least 97% of women in China have been exposed to marketing of formula milk before their babies were born (60). In the face of such powerful marketing, the government should pay full attention to managing it. Adhering to the philosophy and practice that the interests of children and parents take precedence over commercial interests, the government should guide society to initiate and maintain breastfeeding.
4.7 Influencing factors of breastfeeding guarantee policy need
In traditional Chinese parenting concepts, the nutrient content of human milk becomes lower as the baby's age increases. Furthermore, with the addition of complementary food, parents gradually give up breastfeeding. Many mothers add food supplements too prematurely and think that it is sufficient to breastfeed their baby for 12 months, which our previous qualitative study has also verified. Naturally, their needs and expectations for breastfeeding safeguarding policies are ignored because of them prematurely ignoring breastfeeding.
Mothers' education levels have also been reported to be associated with breastfeeding. Less educated mothers are less likely to choose exclusive breastfeeding or even continue breastfeeding [World Health Organization and the United Nations Children's Fund (UNICEF)] (60). Especially in the most rural areas of China, women have many inappropriate feeding behaviors because of economic and knowledge limitations (23), so they cannot express their demand for breastfeeding guarantee policies. On the other hand, mothers with a higher level of education pay greater attention to the physical and mental health of their children. They will learn about more scientific and better feeding methods through various channels and pay greater attention to the needs of breastfeeding in terms of medical care, amenities, workplace support, and government subsidies (61).
The choice of different payment types by mothers also reflects a family's economic status. Women with higher family economic levels are often more likely to give up breastfeeding because they can afford it (62). They also tend to work and cannot bear the pain and fatigue of breastfeeding. Thus, they pay little attention and have a low demand for a series of policies and measures aimed at ensuring breastfeeding.
Consistent with previous studies, our study showed that the smooth initiation of breastfeeding facilitates the long-term adherence to subsequent breastfeeding recommendations (12). Mothers who choose exclusive breastfeeding will care more and pay greater attention to their baby's diets, also focus on a series of measures that are beneficial to breastfeeding, such as hospital and community support, convenience of breastfeeding in public places, and workplace support (such as flexible working conditions), long maternity leave, government maternity allowance, etc. Also, from promulgating the latest family planning policy (three-child policy) (28), women who want to insist on breastfeeding have more updated expectations and needs for the improvement and implementation of breastfeeding-related guarantee policies.
5 Conclusion
This study addressed some gaps in the quantitative research on breastfeeding policies in China and provided more intuitive data and a better understanding of this topic for the Chinese government to promote breastfeeding. In this study, the maternal demand for a breastfeeding guarantee policy is multifaceted and urgent. Maternal education, the baby's age, and current feeding method all have a positive predictive effect on the demand for breastfeeding policies. This also suggests that the government and relevant departments can promote and implement policies based on the relevant influencing factors in the process of improving and implementing policies.
5.1 Policy recommendation
Domestic and foreign research on the influencing factors and interventions for individuals, families, and hospitals regarding breastfeeding has been relatively detailed, but there are only a few studies on breastfeeding guarantee policies, especially in China. The formulation and improvement of such policies play a qualitative role in promoting breastfeeding (19). Considering the important leading role of policy, it is very important and necessary to understand the needs of women of childbearing age for breastfeeding guarantee policies. Moreover, according to the specific needs of mothers for relevant policies, the government and relevant departments can implement targeted breastfeeding promotion plans in medical institutions, construct public facilities, as well as ensure workplace support, government support, cultural breastfeeding publicity, and the effective management of breast milk substitutes. In order to further solve the bottleneck problem of persistently low breastfeeding rates, it is important to achieve greater breastfeeding satisfaction. Finally, guiding and controlling the implementation of the breastfeeding promotion plan at the policy level has important practical significance for safeguarding the basic health rights of mothers and infants, improving the quality of life of the population, and promoting coordinated social development, as well as social fairness and justice.
5.2 Limitations
Firstly, the convenience sampling and the voluntary nature of the study may lead to some selection bias. The study was conducted in the international city of Shanghai, China, and the sample population was mostly women with higher education and income. Therefore, our findings may not apply to people with lower education or from rural areas. Secondly, some characteristics of the women who refused to participate were not analyzed because of the online data collection method. Due to the limitations of time, manpower, material resources, and other conditions, only one tertiary first-class obstetrics and gynecology hospital in Shanghai was selected for data collection. There may further be some limitations in sample selection and coverage. Thus, the multi-center study will strive to conduct in-depth research in hospitals of different regions and levels. At the same time, the applicability and stability of this survey tool can be further verified. In addition, information on some important factors, such as marital problems and family support, was not collected in our study, which needs to be further confirmed by future studies.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Approval letter of Ethics Committee, Shanghai First Maternity and Infant Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JL: Data curation, Investigation, Methodology, Writing – original draft. LZ: Data curation, Investigation, Writing – review & editing. NG: Investigation, Methodology, Writing – review & editing. YL: Methodology, Project administration, Writing – review & editing. HJ: Funding acquisition, Resources, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study is supported by the Shanghai Science and Technology Innovation Research Foundation (No. 20Y11907100). The funder had no role in study design, data analysis, data interpretation, the decision to publish, or preparation of the manuscript.
Acknowledgments
We thank our study participants, research assistants, and staff without whom this work would not be possible. We also thank International Science Editing (http://www.internationalscienceediting.com) for editing this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. UNICEF. Infant and Young Child Feeding. (2021). Available online at: https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/
2. WHO. Breastfeeding. Available online at: https://www.who.int/health-topics/breastfeeding#tab=tab_1
3. UNICEF. Breastfeeding Practices Worldwide. (2020). Available online at: https://data.unicef.org/resources/world-breastfeeding-week-2020/ (accessed July 30, 2020).
4. Statistics Abo. Health Service Usage and Health Related Actions, Australia, 2017–18-Breastfeeding. (2018). Available online at: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/breastfeeding/latest-release (accessed December 12, 2018).
5. UNICEF. The State of the World's Children 2017: Children in a Digital World. https://www.unicef.org/reports/state-worlds-children-2017 (accessed December 2017).
6. Wenwen D, Minhui Z. Influence of mother-infant bedside intervention on mastery of breastfeeding knowledge and exclusive breastfeeding rate in Primiparas. J Clin Res. (2020) 37:340–2. doi: 10.3969/j.issn.1671-7171.2020.03.006
7. Tingting D, Biru L. Effect of individualized intervention on postpartum breast-feeding behavior after cesarean section. J Sichuan Univ. (2019) 50:609–14. doi: 10.13464/j.scuxbyxb.2019.04.030 [Chinese].
8. Mingzhu C, Jingxia F, Yang L. The role of father in breastfeeding and the status of related intervention research. Chin Nurs Manag. (2019) 19:1756–60. doi: 10.3969/j.issn.1672-1756.2019.11.034
9. Yingying L, Lu C, Mengxiao L. Effects of staged pregnancy health care intervention combined with third trimester fertility dance on maternal and infant outcomes and breastfeeding in Primiparas. Guangdong Med J. (2020) 41:425–9. doi: 10.13820/j.cnki.gdyx.20191809
10. Yan W, Ying Z, Yanfen Z. The effect of prenatal and postpartum nursing intervention on breastfeeding of mothers with nipple defects. Shanxi Med J. (2020) 49:1734–6. doi: 10.3969/j.issn.0253-9926.2020.13.041
11. Hui Y, Nafei G, Wei Z. Application and evaluation of mobile device-based continuous breastfeeding intervention program. Chin J Perinat Med. (2019) 22:467–71. doi: 10.3760/cma.j.issn.1007-9408.2019.07.008
12. Rollins NC, Bhandari N, Hajeebhoy N, Horton S, Lutter CK, Martines JC, et al. Why invest, and what it will take to improve breastfeeding practices? Lancet. (2016) 387:491–504. doi: 10.1016/S0140-6736(15)01044-2
13. Nieuwoudt SJ, Ngandu CB, Manderson L, Norris SA. Exclusive breastfeeding policy, practice and influences in South Africa, 1980–2018: a mixed-methods systematic review. PLoS One. (2019) 14:e0224029. doi: 10.1371/journal.pone.0224029
14. Kosmala-Anderson J, Wallace LM. Breastfeeding works: the role of employers in supporting women who wish to breastfeed and work in four organizations in England. J Public Health (Bangkok). (2006) 28:183–91. doi: 10.1093/pubmed/fdl012
15. Heymann J, Raub A, Earle A. Breastfeeding policy: a globally comparative analysis. Bull World Health Organ. (2013) 91(6):398–406. doi: 10.2471/BLT.12.109363
16. Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. (2016) 387:475–90. doi: 10.1016/S0140-6736(15)01024-7
17. Livingston-Rosanoff D, Shubeck SP, Kanters AE, Dossett LA, Minter RM, Wilke LG. Got milk? Design and implementation of a lactation support program for surgeons. Ann Surg. (2019) 270:31–2. doi: 10.1097/SLA.0000000000003269
18. Centers for Disease Control. Breastfeeding Report Card. United States (2016). Available online at: https://www.cdc.gov/breastfeeding/pdf/2016breastfeedingreportcard.pdf (accessed August, 2016).
19. Jinlu Z, Jiaqi H. Comparative study on the Status, causes and policies of child nutrition in China and developing countries. Food Nutr China. (2021) 27:5–11. doi: 10.3969/j.issn.1006-9577.2021.03.002
20. The Ministry of Health. Notice of the Ministry of Health on Further Strengthening Children’s Health Care Work. Beijing: Ministry of Health (1990). Available online at: https://www.pkulaw.com/chl/cd2fe62bde52ec2fbdfb.html
21. The National People’s Congress Standing Committee of the People’s Republic of China. Maternal and Child Health Law of the People’s Republic of China. (2017). Available online at: http://www.gov.cn/guoqing/2021-10/29/content_5647619.htm (accessed November 04, 2017).
22. The State Council. Notice of the State Council on Printing and Distributing the Outline for Women’s Development in China and the Outline on the Development of Chinese Children. Beijing: The State Council (2021). Available online at: http://www.gov.cn/zhengce/2020-12/26/content_5574502.htm
23. Department of Maternal and Child Health. Notice on Printing and Distributing the Breastfeeding Promotion Action Plan (2021–2025). Beijing: Department of Maternal and Child Health (2021). Available online at: http://www.gov.cn/zhengce/zhengceku/2021-11/24/content_5653169.htm
24. Zhen H, Xu D. List of Maternity Leave Policies in 31 Provinces, Autonomous Regions and Municipalities. Beijing: People. cn (2022). Available online at: http://leaders.people.com.cn/n1/2022/0214/c58278-32351813.html
25. Rothwell R, Zegveld W. Industrial Innovation and Public Policy: Preparing for the 1980s and 1990s. London: Frances Printer (1981) 2(1). p. 61. doi: 10.1016/0166-4972(83)90008-1
26. Li Z, Liu Y. Nursing Research Method. 2nd ed. Beijing: People′ s Medical Publishing Press (2018).
27. LiYan D, SuFen Q, YingKui Z, LiHong Z. Analysis of the status, problems and countermeasures of China’s breastfeeding protection policy. Chin J Women Child Health. (2019) 10:79–81. doi: 10.19757/j.cnki.issn1674-7763.2019.04.021
28. The State Council the People’s Republic of China. The Central Committee of C.P.C Decision of the State Council on Optimizing the Fertility Policy and Promoting the Long-term Balanced Development of the Population. (2021). Available online at: http://www.gov.cn/zhengce/2021-07/20/content_5626190.htm (accessed June 26, 2021).
29. Zhang Y, Jin Y, Vereijken C, Stahl B, Jiang H. Breastfeeding experience, challenges and service demands among Chinese mothers: a qualitative study in two cities. Appetite. (2018) 128:263–70. doi: 10.1016/j.appet.2018.06.027
30. Wu Y, Liu W, Liu X, Li Y, Wang Y, Chu Y, et al. Breastfeeding competency and its influencing factors among pregnant women in third trimester pregnancy: a cross-sectional study. Sci Rep. (2023) 13(1):1240. doi: 10.1038/s41598-023-28477-4
31. Dewey KG, Adu-Afarwuah S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr. (2008) 4 Suppl 1(Suppl 1):24–85. doi: 10.1111/j.1740-8709.2007.00124.x
33. Kozhimannil KB, Jou J, Gjerdingen DK, McGovern PM. Access to workplace accommodations to support breastfeeding after passage of the affordable care act. Women’s Health Issues. (2016) 26(1):6–13. doi: 10.1016/j.whi.2015.08.002
34. Ahmad RS, Sulaiman Z, Nik Hussain NH, Mohd Noor N. Working mothers’ breastfeeding experience: a phenomenology qualitative approach. BMC Pregnancy Childbirth. (2022) 22(1):85. doi: 10.1186/s12884-021-04304-4
35. Brown A. Breastfeeding as a public health responsibility: a review of the evidence. J Hum Nutr Diet. (2017) 30(6):759–70. doi: 10.1111/jhn.12496
36. Zhang L. Research on the Current Situation, Existing Problems and Countermeasures of the Implementation of Breast-Feeding Security Policy in China. Suzhou: Suzhou University (2016). doi: 10.7666/d.D01007589
37. Arrera CM, Beauregard JL, Nelson JM, Perrine CG. Association of maternity care practices and policies with in-hospital exclusive breastfeeding in the United States. Breastfeed Med. (2019) 14(4):243–8. doi: 10.1089/bfm.2018.0196
38. Marinelli A, Del Prete V, Finale E, Guala A, Pelullo CP, Attena F. Breastfeeding with and without the WHO/UNICEF babyfriendly hospital initiative: a cross-sectional survey. Medicine (Baltimore). (2019) 98(44):e17737. doi: 10.1097/MD.0000000000017737
39. Schmied V, Beake S, Sheehan A, McCourt C, Dykes F. Women’s perceptions and experiences of breastfeeding support: a meta synthesis. Birth. (2011) 38(1):49–60. doi: 10.1111/j.1523-536X.2010.00446.x
40. Junying L, Ying L, Lan Z, Hui J. Qualitative study of maternal perinatal breastfeeding needs: analysis of cognitive differences between healthcare professionals and parturients. Chin J Prac Nurs. (2022) 38(11):857–62. doi: 10.3760/cma.j.cn211501-20210911-02577
41. Chen J, Strodl E, Huang LH, Chen JY, Liu XC, Yang JH, et al. Associations between prenatal education, breastfeeding and autistic-like behaviors in Pre-schoolers. Children (Basel). (2021) 8(2):124. doi: 10.3390/children8020124
42. Colbourne G, Crane J, Murphy P, O'Brien D. The rates of any breastfeeding at the time of postpartum hospital discharge for early term (370–386 weeks) versus full term (390–416 weeks) infants. J Obstet Gynaecol Can. (2020) 42(4):453–61. doi: 10.1016/j.jogc.2019.09.021
43. Ara G, Khanam M, Papri N, Nahar B, Haque MA, Kabir I, et al. Peer counselling improves breastfeeding practices: a cluster randomized controlled trial in urban Bangladesh. Matern Child Nutr. (2018) 14(3):e12605. doi: 10.1111/mcn.12605
44. Shakya P, Kunieda MK, Koyama M, Rai SS, Miyaguchi M, Dhakal S, et al. Effectiveness of community-based peer support for mothers to improve their breastfeeding practices: a systematic review and meta-analysis. PLoS One. (2017) 12(5):e0177434. doi: 10.1371/journal.pone.0177434
45. Akik C, Ghattas H, Filteau S, Knai C. Barriers to breastfeeding in Lebanon: a policy analysis. J Public Health Policy. (2017) 38(3):314–26. doi: 10.1057/s41271-017-0077-9
46. González de Cosío T, Ferré I, Mazariegos M, Pérez-Escamilla R, BBF Mexico Committee. Scaling up breastfeeding programs in Mexico: lessons learned from the becoming breastfeeding friendly initiative. Curr Dev Nutr. (2018) 2(6): nzy018. doi: 10.1093/cdn/nzy018
47. WHO, UNICEF. The WHO/UNICEF international code of marketing of breast milk substitutes: principal provisions. Indian J Pediatr. (1981) 48:563–4. doi: 10.1007/BF02821571
48. Breast Milk Banking Group, Child Health Professional Committee of Chinese Medical Doctor Association. Analysis of the current situation of human milk bank operation in mainland China. Chin J Pediatr. (2017) 55(08):597–601. doi: 10.3760/cma.j.issn.0578-1310.2017.08.010
49. Edelblute HB, Altman CE. The interaction and impact of social support and father absence on breastfeeding. Breastfeed Med. (2021) 16(8):629–34. doi: 10.1089/bfm.2020.0202
50. Rempel LA, Rempel JK, Moore KCJ. Relationships between types of father breastfeeding support and breastfeeding outcomes. Matern Child Nutr. (2017) 13(3):e12337. doi: 10.1111/mcn.12337
51. Petterson T, Wolanskyj-Spinner A. Parental health in fellowship trainees: fellows’ satisfaction with current policies and interest in innovation. Womens Health (Lond). (2020) 16:1–8. doi: 10.1177/1745506520949417
52. Canon CL, Enzmann DR, Grist TM, Meltzer CC, Norbash A, Omary RA, et al. Society of chairs of academic radiology departments statement of support for paid parental leave. J Am Coll Radiol. (2019) 16(3):271–2. doi: 10.1016/j.jacr.2018.12.029
53. Englander MJ, Ghatan CE, Hamilton BN, Josephs SC, Nelson KJ, Traube LE. Society of interventional radiology position statement on parental leave. J Vasc Interv Radiol. (2017) 28(7):993–4. doi: 10.1016/j.jvir.2017.04.006
54. Jia L. On the Perfection of Maternity Leave[D]. Zhejiang: Zhejiang University of Finance and Economics (2014).
55. Chai Y, Nandi A, Heymann J. Does extending the duration of legislated paid maternity leave improve breastfeeding practices? Evidence from 38 low-income and middle-income countries. BMJ Glob Health. (2018) 3(5):e001032. doi: 10.1136/bmjgh-2018-001032
56. Ogbuanu C, Glover S, Probst J, Hussey J, Liu J. Balancing work and family: effect of employment characteristics on breastfeeding. J Hum Lact. (2011) 27(3):225–38. doi: 10.1177/0890334410394860
57. Lindsay AC, Wallington SF, Greaney ML, Hasselman MH, Tavares Machado MM, Mezzavilla RS. Brazilian immigrant mothers’ beliefs and practices related to infant feeding: a qualitative study. J Hum Lact. (2017) 33(3):595–605. doi: 10.1177/0890334416676267
58. McKenzie SA, Rasmussen KM, Garner CD. Experiences and perspectives about breastfeeding in “public”: a qualitative exploration among normal-weight and obese mothers. J Hum Lact. (2018) 34(4):760–7. doi: 10.1177/0890334417751881
59. Piwoz EG, Huffman SL. The impact of marketing of breast-milk substitutes on WHO-recommended breastfeeding practices. Food Nutr Bull. (2015) 36(4):373–86. doi: 10.1177/0379572115602174
60. Maternal, Newborn, Child & Adolescent Health & Ageing (MCA), Nutrition and Food Safety (NFS). How the Marketing of Formula Milk Influences our Decisions on Infant Feeding. Geneva: WHO, UNICEF (2022). Available online at: https://www.who.int/publications/i/item/9789240044609
61. Cohen SS, Alexander DD, Krebs NF, Young BE, Cabana MD, Erdmann P, et al. Factors associated with breastfeeding initiation and continuation: a meta-analysis. J Pediatr. (2018) 203:190–6.e121. doi: 10.1016/j.jpeds.2018.08.008
Keywords: breastfeeding, policy protection, maternal and infant rights, policy needs, China background
Citation: Li J, Zhang L, Guo N, Liu Y and Jiang H (2024) Investigation of maternal breastfeeding guarantee policy needs and influencing factors: a cross-sectional study in China. Front. Health Serv. 4:1348888. doi: 10.3389/frhs.2024.1348888
Received: 3 December 2023; Accepted: 27 February 2024;
Published: 7 March 2024.
Edited by:
Andrea Cioffi, University of Foggia, ItalyReviewed by:
Setyowati Setyowati, University of Indonesia, IndonesiaErmel Ameswué Kpogbé Johnson, Yackoley Institute, Burkina Faso
© 2024 Li, Zhang, Guo, Liu and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Jiang amlhbmdodWl0ZXN0QDE2My5jb20=
†These authors have contributed equally to this work and share first authorship