 Malin Rosell Magerøy
Malin Rosell Magerøy Carl Macrae1,2
Carl Macrae1,2 Geir Sverre Braut
Geir Sverre Braut Siri Wiig
Siri Wiig- 1SHARE – Centre for Resilience in Healthcare, Faculty of Health Science, University of Stavanger, Stavanger, Norway
- 2Centre for Health, Innovation, Leadership and Learning, Nottingham University Business School, Nottingham, United Kingdom
- 3Department of Research, Stavanger University Hospital, Stavanger, Norway
- 4Department of Social Science, Western Norway University of Applied Sciences, Sogndal, Norway
Objective: Within healthcare, the role of leader is becoming more complex, and healthcare leaders carry an increasing responsibility for the performance of employees, the experience and safety of patients and the quality of care provision. This study aimed to explore how leaders of nursing homes manage the dual responsibility of both Health, Safety and Environment (HSE) and Quality and Patient Safety (QPS), focusing particularly on the approaches leaders take and the dilemmas they face. In addition, we wanted to examine how leaders experience and manage the challenges of HSE and QPS in a holistic way.
Design/setting: The study was designed as a case study. Data were collected through semi structured individual interviews with leaders of nursing homes in five Norwegian municipalities.
Participants: 13 leaders of nursing homes in urban and rural municipalities participated in this study.
Results: Data analysis resulted in four themes explaining how leaders of nursing homes manage the dual responsibility of HSE and QPS, and the approaches they take and the dilemmas they face:
1. Establishing good systems and building a culture for a work environment that promotes health and patient safety.
2. Establish channels for internal and external collaboration and communication.
3. Establish room for maneuver to exercise leadership.
4. Recognizing and having the mandate to handle possible tensions in the dual responsibility of HSE and QPS.
Conclusions: The study showed that leaders of nursing homes who are responsible for ensuring quality and safety for both patients and staff, experience tensions in handling this dual responsibility. They acknowledged the importance of having time to be present as a leader, to have robust systems to maintain HSE and QPS, and that conflicting aspects of legislation are an everyday challenge.
1 Introduction
Healthcare leaders have a complex role and face demands and responsibilities for maintaining the safety of both employees and patients and ensuring high quality care. In particular, healthcare leaders face an important task in managing and handling the dual responsibility of managing Health, Safety and Environment (HSE), and Quality and Patient Safety (QPS), within their healthcare organizations which encompasses both the safety of staff, and the safety and quality of care (1, 2). In Norway, for instance, different legislation regulates these dual responsibilities. Moreover, leaders face a range of practical challenges in the management of QPS including the need to ensure appropriate leaderships skills and system efficiency (3). In the context of nursing homes, there is a pressing need to increase and develop the knowledgebase for the management of QPS (2, 4). The systematic management of HSE and QPS is a leadership responsibility at all levels of the Norwegian healthcare system (5, 6). And, while HSE and QPS are often handled as separate management responsibilities, research shows that it is important to understand HSE and QPS in a holistic and integrated way (1, 7, 8). Managing the duality of safety and wellbeing for both patients and staff is increasingly important for healthcare leaders, and this depends on careful attention to the organizational, cultural, and psychosocial factors that enable safety, but limited attention has been paid to leaders’ understanding and perspectives of this dual responsibilities (1, 7, 9). Effective leadership can build organizational capacity to improve employee and patient outcome, but since leadership is contextual, there can be several ways to lead. Leadership level and organization could affect leadership approach and outcome for HSE and QPS (10, 11). There is some research in hospital settings on mid-level leaders and their role in QPS (12–14), but we know little about how mid-level leaders experience and approach the dilemmas of having the dual responsibility of HSE and QPS. There is limited research on leaders of nursing homes (which, for the purposes of this study, are considered mid-level leaders) experience on HSE and QPS, and this study will contribute to narrow the knowledge gap.
Systems Engineering Initiative for Patient Safety (SEIPS) offers one way of exploring the dual responsibility of QPS and HSE. SEIPS can be used as a theoretical framework that focuses on systems design, and its impact on safety processes and outcomes in healthcare (15). There are five components to a work system in the SEIPS model: person, task, tool/instrument, physical environment, and organizational conditions (15, 16). These components interact with and influence each other in ways that shape safety outcomes. Outcomes in the SEIPS model are divided into patient outcomes and employee and organizational outcomes. Patient outcomes in the SEIPS model are focused on issues related to patient safety or quality of care, while employee or organizational outcomes emphasizes job satisfaction, job stress and burnout, employee safety and health, turnover and profitability (15, 16). The SEIPS model shows how all parts of an organization affect and depend upon each other. By using the SEIPS model for mapping and understanding how nursing home leaders enact their leadership responsibility for HSE and QPS this article contributes to reduce the knowledge gap on how mid-level leaders handle the dual responsibility in their everyday work.
1.1 Aim and research question
The aim of this study was to explore how nursing homes leaders manage the dual responsibility of HSE and QPS, and the approaches they take and the dilemmas they face in this work. We wanted to examine how these leaders experience and manage HSE and QPS in a holistic way, and the support available or needed in the process of handling the dual responsibility.
The following research question guided the study:
How do nursing home leaders experience and manage HSE and QPS in a holistic way and what are the key challenges and enablers in this work?
2 Methods
2.1 Design
This study is a part of a single embedded case study. A case study is a method that investigates a contemporary phenomenon in depth in a real-world context, and the approach is suitable when wanting to understand a complex social phenomenon (17). In this study the case is defined in terms of the management of two versions of safety: HSE and QPS in Norwegian nursing home context; and how the management of these aspects of safety are organized, controlled, and overseen, particularly considering the possible tensions between them from a leadership perspective. The main overarching research of which this study is one part explores leadership at three levels of the healthcare system, which includes: politicians and top-level leaders in health and care services in the municipalities (municipal director, director of health and welfare, and head of health and care service), head of nursing homes (mid-level leaders), and department leaders in nursing homes (frontline leaders). This sub-study is exploring the experiences of head of nursing homes in five Norwegian municipalities (see Figure 1).
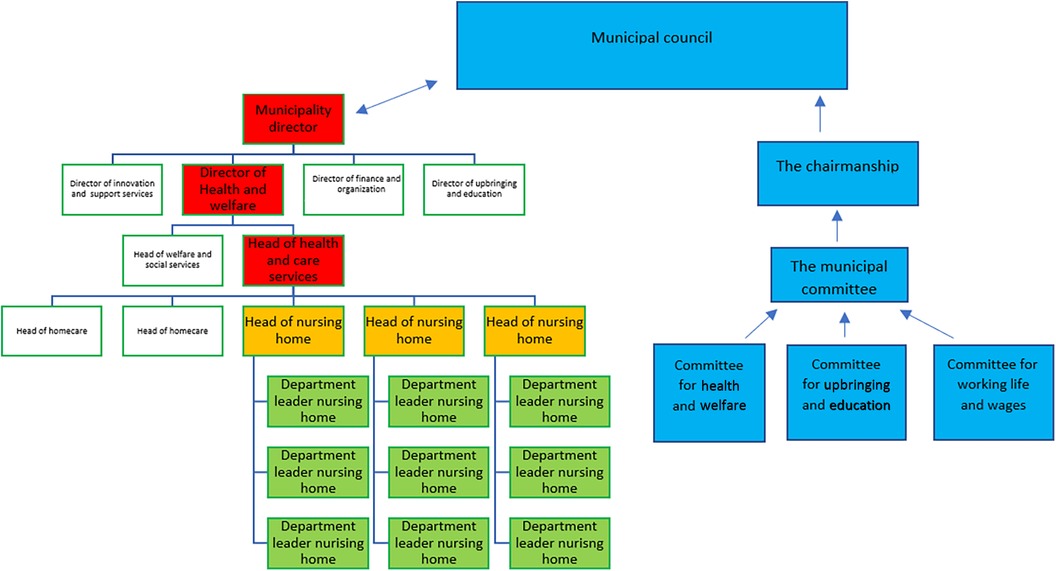
Figure 1. Organization of the municipality according to the chairmanship model. The political steering line is the blue part, while the rest of the organization chart represents the administration. The leadership level relevant in this study are the yellow.
We used the SEIPS model as a framework when formulating the research question and interview guide, and this provides a theoretical reference point throughout the discussion of the findings.
2.2 The Norwegian healthcare context; regulation and legislation
Responsibility for public health and care service in Norway is divided between municipalities and regional health care services. Municipalities are responsible for primary healthcare services, which includes home care services, nursing homes, emergency rooms and General practitioners (GP). The chairmanship model is the most common organization of Norwegian municipalities (see Figure 1). In the chairmanship model, political committees have the overall control and management of the municipality, and the municipal council is the highest political authority and makes decisions on behalf of the municipality. Within the legislative framework, the municipalities are free to prioritize and organize work, and develop plans and governing documents. According to the chairmanship model, healthcare leaders must follow the politicians' decisions regarding priorities and budget allocations. Municipalities are regulated by the “Act on Municipalities and County Municipality” (18). The management of QPS is regulated in the “Regulations on management and quality improvement in the health and care services act”, “Health and care services act” and “National action plan for patient safety and quality improvement” (6, 19–21). The management of HSE is regulated in “Regulations on systematic health, environment and safety work in companies” and “The working environment act” (6, 19).
2.3 Sample and recruitment
The municipalities were recruited through recommendations from the Norwegian Association of Local and Regional Authorities, of which all Norwegian municipalities and county councils are members. The recommended municipalities were contacted with an invitation to participate in the study, together with an information letter. The municipalities were selected based on size and location (urban/rural). When a municipality agreed to participate in this study, the head of health and care services or an HR-adviser identified and invited potential participating nursing homes with the accompanied information letter on the voluntary participation into the research (see Table 1 for the characteristics of the participating municipalities). Nursing home leaders in the urban municipalities were responsible for a larger number of employees and patients, while leaders of nursing homes rural municipalities were more often responsible for a wider professional field, e.g., nursing homes and home care.
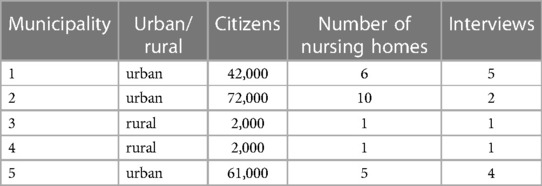
Table 1. Characteristics of municipalities and data collection.
2.4 Data collection
Data collection consisted of 13 individual semi-structured interviews with leaders of nursing homes (n = 13). All participants in this study had extensive leadership experience and formal leadership education. All interviews were conducted physically in the respective nursing home from March and June 2022. Semi-structured interviews were conducted by the first author and were based on an interview guide. Topics in the interview guide were inspired by SEIPS (15), organized in questions dealing with both system-level and individual-level issues, work system, tools, organization, tasks, environment and related to how leaders experience and manage HSE and QPS in a holistic way, what the key enablers and challenges are, and what kind of structure, system and tools they have in this work. The interviews lasted approximately one hour. All interviews were audio recorded and transcribed by the first author.
2.5 Data analysis
The transcribed data material was uploaded in NVivo and analyzed inductively using thematic analysis. The analysis process followed Braun and Clarkes 6-phase guide (22). See Table 2. Author MRM was responsible for the analysis with input from GSB and SW who red transcripts and discussed theme development throughout the analysis period. The interviews were coded, categorized, and sorted under four main themes on how nursing home leaders experience and manage HSE and QPS in a holistic way.
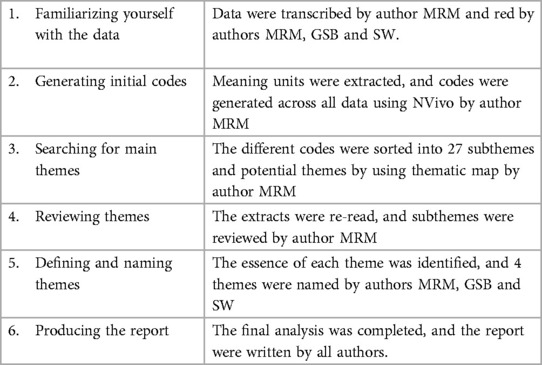
Table 2. Key stages in process of thematic analysis.
3 Results
Based on variation in size, organization and number of employees reporting to each leader in each nursing home, the analysis indicated that leaders experienced various challenges and enablers regarding the dual responsibility of handling HSE & QPS. Despite the structural differences in the municipalities and nursing homes, the four identified themes were recurring and common to all the participants. The results are presented theme-wise, with one table for each theme to illustrate initial quotations, sub-themes, and themes. See Tables 3–6.
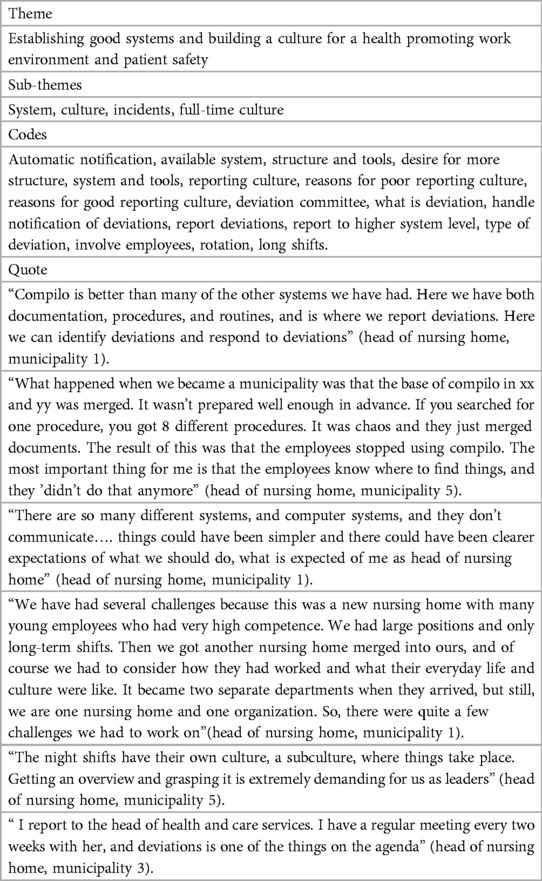
Table 3. Examples of the first theme.
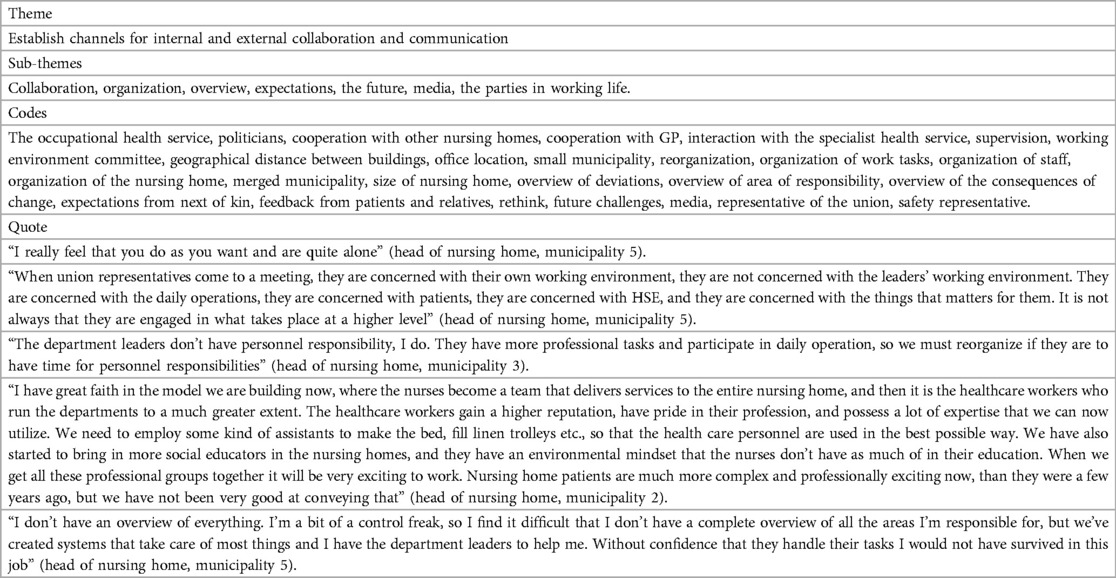
Table 4. Examples of the second theme.
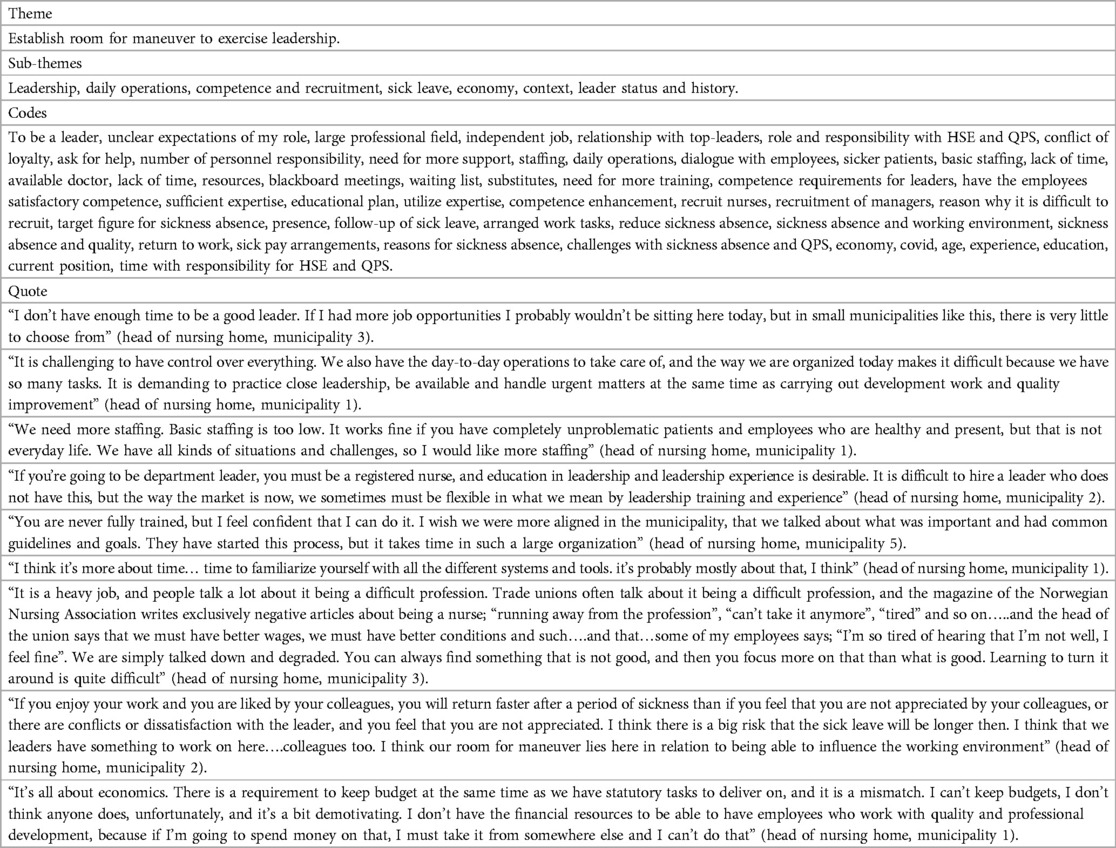
Table 5. Examples of the third theme.

Table 6. Examples of the fourth theme.
3.1 Establishing good systems and building a culture for a health promoting work environment and patient safety
For all leaders, having good and sufficient work systems was deemed necessary to have an overview and degree of control over HSE & QPS in the nursing home. They also indicated that having a culture for using the available systems and reporting adverse events was essential for a safe work environment for both patients and staff.
3.1.1 System
Leaders who were responsible for more than one nursing home had a greater need for management systems and structures than those who were responsible for one nursing home only. The size of the nursing home was also important, as participants who were responsible for large nursing homes with many departments needed more sophisticated management systems to maintain overview and control of safety. All nursing homes in the sample used Compilo as their quality system. Compilo is an electronic system where documents can be stored. It is moreover used to save updated regulations, guidelines, and procedures, and for reporting deviations, such as adverse events. There was great variation in the extent to which the participants used the various components of Compilo, but the majority were satisfied with the functionality the system provided. One of the participating municipalities was newly established, merged from two smaller neighboring municipalities. The two original municipalities were described as having had both different systems and a different culture around safety. The leaders experienced that the systems were not easily adapted to each other when the municipalities were merged, with the result that the employees stopped using it. The leaders subsequently spent a lot of time establishing a management system that works for everyone and encouraging a culture of engaging with the new system. The participants experienced that they had many and good systems, but the systems did not communicate with each other, and leadership expectations were unclear.
3.1.2 Culture
Cultural issues were often invoked to explain challenges and opportunities within both domains of HSE and QPS, and the nursing home leaders argued that culture influenced several areas. To build a culture for a health promoting working environment and patient safety, the nursing homes must build a common culture regarding how work is organized, the reporting of adverse events, the approach to working hours, as well as building a shared sense of coherence and community, the leaders said. Reorganizations and merger processes in recent years have led to several nursing homes being merged, rebuilt, or newly established. Leaders of merged or newly established nursing homes talked about the importance of working towards a common culture among their organizations and employees.
3.1.3 Incidents
Generally, the leaders believed they had been able to establish a good culture for reporting deviations and incidents. Incident reporting was a focus area, and leaders described that improvements in reporting culture required ongoing leadership emphasis on the importance of reporting. Some nursing homes and departments had a less effective reporting culture than others, and the leaders explained this was due to a historic lack of attention to developing reporting systems, staff being fearful of reporting incidents involving their colleagues, and a lack of training in how to use the reporting system. Leaders described how they encouraged the employees to report and subsequently used the incidents to support improvement work, however it was often deemed challenging to define what exactly constituted a reportable deviation in the context of nursing homes, and leaders suspected those uncertainties could lead to underreporting. The incidents reported mainly concerned events immediately related to patient care, such as medication errors and falls. Some were related to threats and violence from patients and next of kin, while there were almost no reports on more contextual or organizational issues such as the work environment. The incident reports were handled by the department leaders. To a varying degree, leaders in a higher hierarchical position were informed. Information about deviations was not requested by the top leaders in the large municipalities, while leaders across leadership levels in the small municipalities had regular meetings where deviations were on the agenda.
3.2 Establish channels for internal and external collaboration and communication
To meet the future needs and expectations from society in HSE and QPS, leaders of nursing homes saw the need for clear communication and cooperation with others. The degree of interaction varied in the different municipalities, but all had routinely collaborated with other stakeholders such as specialized healthcare services, the occupational health service, and GPs. Some leaders experienced effective collaboration with other leaders in the municipality, while others reported working more independently without the aid of common guidelines and close professional interaction. Collaboration with the governmental authorities through formal process of regulatory supervision was perceived by most leaders as constructive, and a way for the leaders of nursing homes to identify and focus attention on improvement activities. Politicians and media were seen as playing an important part in highlighting important safety issues, as well as communicating broader expectations, challenges, and opportunities according to the leaders.
3.2.1 Organization
The participating municipalities differed in size and organizational structure. In the larger municipalities there were several department leaders with personnel responsibility, while in the small municipalities, the department leaders did not always have personnel responsibility, and were more preoccupied with daily operations and rotation scheme. Employees within the nursing homes were organized in different ways. In some nursing homes they belonged to a specific department and were not flexible about changes, while in others, staff were used to work across departments to balance workload and resource. With greater flexibility in staffing, leaders found it easier to cover vacant shifts with equivalent staff and make less use of temporary staff. This was beneficial financially as it reduced costly reliance on temporary workers, and allowed leaders to ensure that teams with the appropriate skills and competence could be flexibly reorganized as necessary. The leaders who organized staff in this way initially experienced reluctance from some team members, but said that with guidance, support and a gradual cultural change, employees acknowledged the positive effect for both HSE and QPS. Leaders also indicated that they expected that the need to organize work in new ways, would only increase to meet future needs, such as the increasing number of elderly people in need of complex and advanced care.
3.2.2 Overview
The leaders of nursing homes reported that it could be challenging to maintain an overview of everything they were responsible for in relation to HSE and QPS, and described the need for effective systems, collaboration, and communication. Collaboration with representatives from the unions and safety representatives was seen as essential for leaders to have a clear view of health and safety issues in the work environment, to implement improvements and to create rotation schemes that consider both employees’ wishes, the need for competence and continuity in care, and laws and regulations on working hours. Although leaders valued this engagement, they also reported that union representatives did not always see the whole picture in the same way or were concerned with the leaders’ working conditions.
3.3 Establish room for maneuver to exercise leadership
All participants in this study had extensive leadership experience at different levels in the health care system. They agreed that it was challenging to find time and room to fully perform their leadership duties, as daily operations, financial limitations, and sick leave took considerable time and attention. They acknowledged the need to establish room for maneuver to ensure time and resources for practicing the leadership responsibilities.
3.3.1 Leadership
Being a leader was described as hard work. Leaders found it challenging to always be available to address challenges, and commonly reported that the distinction between work and leisure had been blurred, and that, particularly in the small municipalities, they could feel lonely in relations to their leadership and organizational responsibilities. Daily operations took time away from being physically present, and several of the participants found it challenging as they had responsibility for several nursing homes, and some employees worked nightshifts or weekends only. Participants highlighted the importance of practicing leadership by “being near” the employees. As leaders of nursing homes, they felt an enormous responsibility for both their patients’ and staff safety and wellbeing.
3.3.2 Daily operations
Daily operations took up much of the leader's time and availability, which resulted in more development-oriented work and long-term planning not being prioritized. Nursing home patients have become sicker and more demanding compared to a few years ago and leaders felt that the lack of resources available to them had not kept pace to handle this development. The staffing situation was described as similar, which could affect the management of both HSE and QPS in terms of not having enough qualified personnel. The leaders suggested implementing minimum staffing levels to maintain safe care.
3.3.3 Competence and recruitment
Staff competence was viewed as critical for the delivery of safe services and high quality care. Competence was also described as the foundation for meeting future needs and increasing patient demands and keeping health care personnel engaged and self-confident. Leaders reported that recruitment of nurses and department leaders had become more difficult and having substitutes in vacant positions affected daily operations and the overall competence. Heads of nursing homes in this study considered their department leaders to be appropriately qualified, but not all of them had formal leadership training or leadership experience. The leaders reported that they felt they had the competence needed for their own leadership position, but they also acknowledge that there was room for improvement in how the competence was used and maintained. To be a leader in a nursing home, there were no requirements other than a bachelor's degree in a health-related topic. In most municipalities it was required to be a registered nurse, while others also had physiotherapists and social workers as leaders. There were good opportunities for skills development internally in the municipalities through courses and further education regarding HSE and QPS. Despite these opportunities, many participants explained that the lack of time to get used to new systems and routines made everyday life demanding.
3.3.4 Sick leave
Sickness absence affected everyday life in nursing homes to a great extent and required a lot of attention and management by the leaders. Leaders argued that employee age, culture, and sick pay arrangements were factors they believed influenced the high rate of absence. Moreover, they believed that the reputation of working in nursing homes contributed to sick leave, as they experienced work being talked down and employees being told that it was a heavy and demanding profession. Since lack of visible and existing leadership can lead to increased sick leave, this became a negative spiral. Loosing continuity and valuable competence was the biggest consequence of the sick leave. Leaders often had to use unqualified substitutes during times with high sick leave, and several of the leaders tried to reorganize their nursing homes and how they used their staff so that they were not so vulnerable to absence. They all agreed that sick leave affected the working environment, and thus QPS, but also that a good work environment could contribute to employees returning to work earlier and maintaining effective work engagement. The leaders created some flexibility by changing work roles and adapting work demands so that employees could return faster after sick leave. But it was difficult when employee needs or necessary accommodations were long-term, or if there were several employees in need of easier work tasks or changed working hours. The leaders agreed that working with the rotation schemes, work environment, and increasing basic staffing levels would reduce sickness absence.
3.3.5 Economy
Economic considerations influenced several of the areas the leaders were responsible for and was decisive for whether they could hire additional personnel if needed. According to leaders, budgetary constraints affected most of their decisions, and they felt there was a gap between the financial resources they had available, and the tasks and quality of care they had to deliver.
3.4 Recognizing and having the mandate to handle possible tensions in the dual responsibility of HSE and QPS
The concept of dual responsibility for HSE and QPS was not a term that leaders were accustomed to. Several participants experienced that it could be difficult to separate the concepts of HSE and QPS. They argued it was holistic work that could not be divided. They acknowledged having an enormous responsibility, and that there were possible tensions within specific legislation and requirements. This affected their management of both HSE and QPS.
3.4.1 HSE and work environment
HSE was seen as a wide area that was difficult to define, but in addition to the physical work environment, the leaders highlighted the importance of the psychosocial work environment. They all agreed that internal control should be used as a tool in associated improvement activities, but not all nursing homes had a system to support this. Employee surveys were also used as a foundation to understand the working environment, and leaders had all put in place for this. Covid-19 contributed to a delay in following up employee surveys due to restrictions and meetings across cohorts.
3.4.2 Patient safety
Patient safety was seen as important and described as safe treatment and care, and the avoidance of injury and inconvenience for patients. Participants furthermore argued that patient safety also was related to more holistic care and dignity. Having routines and procedures was crucial for patient safety, leaders believed. The greatest enablers of patient safety in nursing homes were ensuring that staff follow routines, organizing everyday work effectively and recruiting qualified and appropriate personnel. One of the participating municipalities had participated in a patient safety program a few years ago, and as a result leaders in that location remained particularly focused on patient safety.
3.4.3 Quality
The concept of quality was difficult to define for the leaders. They all agreed that delivering services of high quality was important, but they had no clear definition of what high quality was. Quality was described as being about whether the services are performed in accordance with laws and requirements, but they also believed that quality was a subjective experience and talked about the importance of defining the “right” quality level. A key challenge related to the ability to provide the same level of quality of services throughout the nursing home, and that this could depend on which personnel were at work. Quality and safety influenced each other, participants said. High service quality was an overall objective for the leaders, however, they found it challenging to put this into practice when they did not have a clear definition of high quality and what is “good enough”. Having routines and procedures was viewed as important to maintain quality, but measuring quality was considered difficult across all municipalities, with most making use of user surveys, incident reports and risk analyses to understand quality of care.
3.4.4 Legislation
Legislation and requirements regulate the work related to HSE and QPS to a large extent. Leaders reported that it was difficult to find room to maneuver and make local decisions in relation to the various laws and regulations, especially when these were contradictory. They described an everyday balance between different legislation, ensuring both patient and staff safety and trying to get an overview. Especially the use of coercion on patients and maintaining safety for the healthcare personnel was highlighted as conflicting by the leaders.
3.4.5 The dual responsibility
HSE and QPS were according to the leaders a large field that could be challenging to maneuver in. They experienced this as concepts that influenced each other, and should be seen as one, but often had conflicting interests. To handle HSE and QPS and possible tensions between them participants needed to create good work systems and have confidence in the department leaders and staff that they are competent, uses the systems and report incidents when they occur. They all agreed that HSE and QPS was connected, and especially work engagement and a good working environment were seen as factors that influenced QPS. When changes were made, consequences in other areas were always considered. In events of conflicting interests e.g., use of coercion on patients and safety for staff, the participants had different points of view on what to prioritize. They had no instructions from the municipal management on how to prioritize HSE and QPS concerns in situations where these conflict, but they experienced having support and trust from the municipal management. The relationship with the politicians as decision makers and employer was more complicated as the informants experienced that they were not always supportive and lacked a comprehensive understanding.
4 Discussion
This study explored how nursing home leaders manage the dual responsibility of HSE and QPS, and four identified themes shed a light on how they experience this responsibility, their approaches, and the dilemmas they faced. Our findings show the complexity involved for leaders when enacting the dual responsibility of HSE and QPS, and culture, organization and leadership affect experience and outcome for patients and staff. We have discussed the results of this study considering the SEIPS model and have developed this further in Figure 2 (see Figure 2).
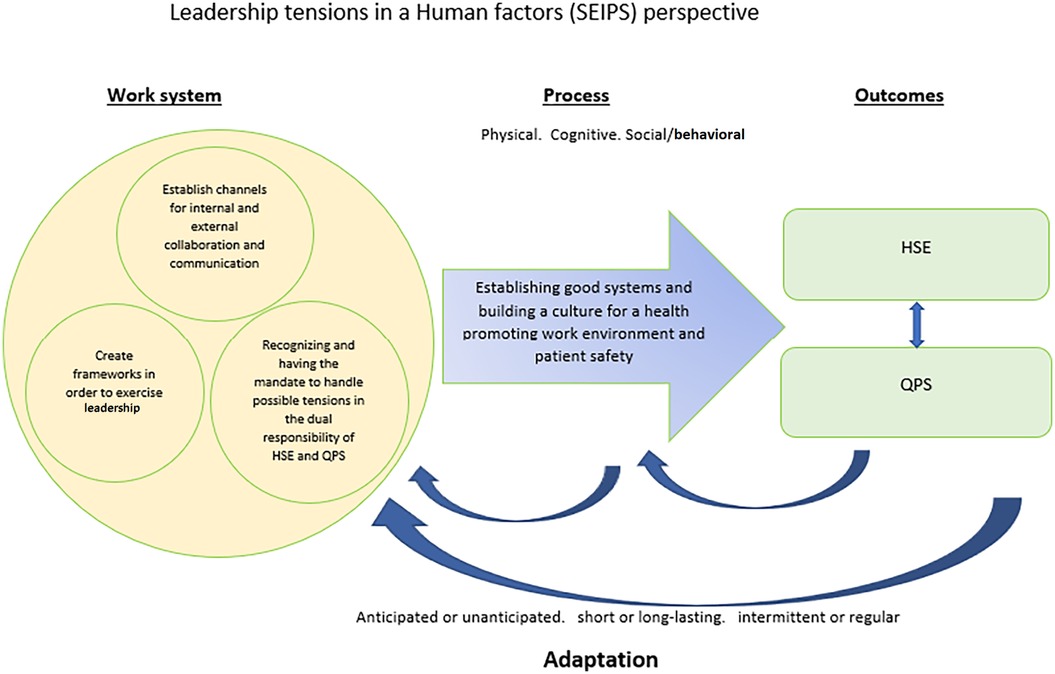
Figure 2. The four themes of how nursing home leaders manage the dual responsibility of HSE and QPS in a human factors’ perspective.
In a SEIPS and Human factors perspective these challenges can be systematically analyzed with a systems orientation to better understand the work system, processes, and outcomes by enacting their leadership roles in a nursing home context. This is discussed in the following along with future implications (23–25).
4.1 Leadership and organization
Mid-level leaders are defined as employees that are supervised by an organization's top-level leaders and who supervise frontline leaders and oversee a defined part of the organization (10, 26). Head of nursing homes holds a dual position both as mid-level leaders (within the overall care system) and as top-level leaders (within their specific organizations). As depicted in Figure 1 they enact the role as mid-level leaders because they are situated in the midlevel of stakeholders in the municipalities who are responsible for organizing the primary care services for all inhabitants (see Figure 1). At the same time, they are the top-level leaders within their specific care organization (nursing home) having the highest decision-making authority and responsibility, and employees at the nursing home could see them as their top-level leader. Healthcare mid-level leaders have an important role in translating top-level policies, strategies, and means into sustainable, high-quality healthcare (27, 28). For participants in this study, it was experienced as a challenge, having the highest management responsibility at the nursing home, being responsible for HSE and QPS, while being subject to instructions from the municipal management and politicians and at the same time handling the expectations from society and next of kin (see Figure 3). Mid-level leaders in healthcare are often professionals who have taken on a leadership role with limited leadership qualifications, and support (10, 27, 28). In our study, all participants had a health-related bachelor's degree, leadership education and leadership experience. This gave them a unique position as they know their organizational area well and can translate the strategy of top-level leaders (in the healthcare system) into everyday life (26, 29). Top-level leaders support have a significant effect on mid-level leaders commitment and effectiveness (29), and studies show that mid-level leaders are important for the organization as they can fill structural holes, motivate and engage employees in changes and improvement (10, 26, 30, 31). Our results indicate that leaders of nursing homes felt alone and had limited support from the municipalities’ top-level leaders. This could influence their engagement and ability to inspire employees in day-to-day operations and future research and practice should explore enablers of stronger support structures and processes within organizations, to avoid potential burnout and turnover of employees and its negative effects on QPS and HSE.
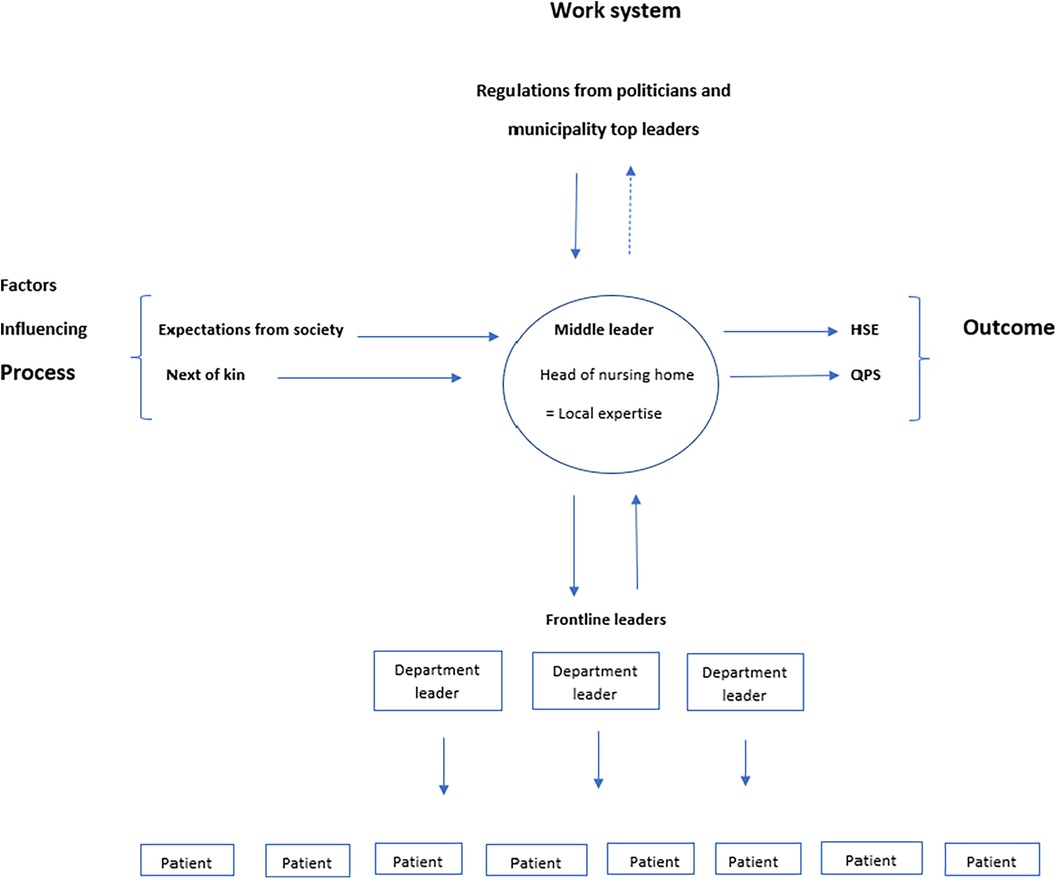
Figure 3. Mid-level leaders position in the municipalities, with responsibilities, considerations and influencing factors in a human factors perspective.
Leadership is associated with both employee and patient outcome (32–34), and different leadership approaches may enable different outcomes. Transformational leadership has significant impact on patient safety culture and work engagement (33), and Leader-Member exchange (LMX) theory suggests that leaders can develop high-quality relationships with employees and thus affect safety culture (35, 36). A fundamental managerial function is to ensure that the organization is adapted to its environment (37). Reform processes in Norway (regionalization and mergers) have resulted in frequent reorganizations, and together with future challenges and expectations this requires constant organizational adaptations and attention from the nursing home leaders. According to Carayon and Perry it is important to listen to and understand local expertise, since all work system have different barriers and facilitators (23). In this study, the nursing home leaders had local expertise regarding local opportunities and challenges, while politicians and municipal top-level management made decisions that applied to all nursing homes in the municipality regardless of local needs. In line with SEIPS this shows how both organizational factors within the nursing home, and factors in the external environment such as legislation, the economic situation and policy factors, can affect the work system that leaders are responsible for (i.e., the nursing home) and the people carrying out the tasks (i.e., the employees and leaders of nursing homes) (38–40). Handling the dual responsibility of HSE and QPS while complying with decisions from top-level leaders, cause continuous trade-offs for the leaders in this study. According to the Efficiency-Thoroughness Trade-Off principle (ETTO), there is a constant balancing act between demands and resources that affects efficiency and thoroughness, and an imbalance between these can lead to errors and adverse events (41). Achieving the right ETTO-balance is an important leadership responsibility within QPS and HSE (42, 43). In practice, this study indicates that it is the nursing home leaders who have the local expertise to make appropriate trade-offs to balance any tensions and manage HSE and QPS. However, our results indicate that there is a need for future studies investigating the role of local expertise when mid-level leaders maneuver in a landscape characterized by conflicting demands with the current local situation and policy and guidelines from the municipal management and politicians.
Changes and reorganizations may have negative effect on the working environment (44), and in our study we found that work environment, QPS and sick leave were closely connected. According to legislation, sick leave follow up is a leadership responsibility (6), and our results showed that leaders spent a lot of time on this task. Nursing home leaders experienced that, by investing a lot of time in employees on sick leave, they traded off other leadership tasks. Having time to fulfill all leadership duties was a constant challenge for nursing home leaders, and contributed to a “firefighting” approach, which other studies have shown is not in accordance with how healthcare professionals and leaders conceptualize providing high quality care (2).
4.2 Culture and QPS
Leaders in healthcare have a legal and professional obligation to improve and provide high quality care (12). Quality of care is a complex and multi-layered concept that is described in various ways including dimensions of clinical effectiveness, patient safety, patient experience as the most common elements in addition to equity, time, and coordination (45). The participants in this study experienced quality as difficult to define, and agreed that quality seemed to be situated, practical and linked to the actual work and care being done. They found quality to be subjective, and thus difficult to measure. Ensuring feedback loops from the organizational context and work system is important for learning, improvement and adaptation (16).
Organizational culture may affect how efficiency-thoroughness is negotiated and balanced, and thus affect QPS (43, 46). Leaders in this study were concerned that certain cultural characteristics might adversely influence multiple areas in the organization and affect work associated with HSE and QPS. Leadership is a key factor in creating, encouraging, and developing safety culture, and it is important that there is not too much pressure on mid-level leaders and that they have the right resources available (47, 48). In our study, nursing home leaders felt an enormous pressure from both policymakers, top-level leaders, frontline leaders, and society (see Figure 3), and they all described challenges related to a lack of resources (e.g., economy, qualified personnel, and support). As a way of utilizing resources, reducing sick leave and improve continuity and quality of care, the nursing homes had introduced full-time culture with long shifts. Studies show that long shifts could lead to unintended consequences such as burnout, reduced efficiency and effectiveness, and thus hinder QPS (49). SEIPS 2.0 states that changes in work system (e.g., long shifts), could have a delayed effect on outcomes (e.g., fatigue and turnover) and lead to a higher level of risk and more deviance (38).
In the event of conflicting interests between HSE and QPS, the leaders had different preferences on what should be prioritized, and there were no instructions from the top-level leaders. In line with other research (1, 12), leaders indicated that HSE and QPS were connected, and work engagement and a good working environment were considered as factors positively influencing QPS. Healthcare leaders possess an important role in QPS, and there is clear evidence that leaders have a great impact on workplace safety and organizational climate. This demonstrates how HSE and QPS should be understood in a holistic perspective (1, 7, 8). From a human factors and SEIPS perspective different priorities (process), will give different outcome for patients and staff and more research is needed to get in depth knowledge in this field.
4.3 Strengths and limitations
This study is the first to explore nursing home leaders’ experiences of the dual responsibility of HSE and QPS and associated key enablers and challenges. The strength of this study is that it contributes new insight regarding the challenges faced by nursing home leaders when handling this duality. The experience and challenges explored here are not exhaustive, but they provide insight that may be transferrable to other similar contexts (17). The study has some limitations. The participating leaders were recruited by the municipal top-level leaders, with some risk of selection bias or unintended pressure to participate in the study. Participants were informed both verbally and in writing that they could withdraw from the study at any time. When using a semi-structured interview guide, it is possible that participants may be prompted to answer in a certain way (50). To minimize that risk, we informed participants that we were interested in their experiences, and that no answer was right or wrong. This study consisted of 13 participants, and having a higher sample of leaders and municipalities could have provided other elements to the results.
5 Conclusions and implications
This study shows that both contextual factors and internal factors influence how nursing home leaders experience the dual responsibility of HSE and QPS. Nursing home leaders reported that time to exercise visible and present leadership, systems to maintain HSE and QPS work, and that conflicting legislation influenced their experience and ability to manage the dual responsibility of HSE and QPS. This study confirms that a change in one of the system components, e.g., organization of the employees (the work system), may affect how the work is carried out due to economic status, available and qualified personnel, etc. (outcome). We have theorized leadership tensions from a human factors perspective to develop a better understanding of nursing home leaders maneuver to handle the dual responsibility of HSE and QPS particularly in relation to the organization and context of Norwegian municipalities. Research on the dual responsibility of HSE and QPS is limited in a nursing home context, and more studies should be conducted to explore the middle leaders experience.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Sikt-Norwegian Agency for Shared Services in Education and Research [formerly known as the Norwegian Centre for Research Data (NSD)] ref.nr: 886397. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MM: Writing – original draft. CM: Writing – review & editing. GB: Writing – review & editing. SW: Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This project is funded by the University of Stavanger.
Acknowledgments
The authors wish to thank all participants for sharing their valuable knowledge and experience.
Conflict of interest
SW is member of Frontiers editorial board special topic; Occupational Health and Organizational Culture within a Healthcare Setting: Challenges, Complexities, and Dynamics. SW is associated editor in Frontiers in health services, special section on patient safety.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ose SO, Busch HJ. HMS I offentlig sektor: forebygging av sykefravær og tidlig avgang fra arbeidslivet. 1. utgave. ed. Oslo: Gyldendal (2020).
2. Aase I, Ree E, Johannessen T, Strømme T, Ullebust B, Holen-Rabbersvik E, et al. Talking about quality: how “quality” is conceptualized in nursing homes and homecare. BMC Health Serv Res. (2021) 21(1):104. doi: 10.1186/s12913-021-06104-0
3. Wiig S, Ree E, Johannessen T, Strømme T, Storm M, Aase I, et al. Improving quality and safety in nursing homes and home care: the study protocol of a mixed-methods research design to implement a leadership intervention. BMJ Open. (2018) 8(3):e020933. doi: 10.1136/bmjopen-2017-020933
4. Wiig S, Aase K, von Plessen C, Burnett S, Nunes F, Weggelaar AM, et al. Talking about quality: exploring how “quality” is conceptualized in European hospitals and healthcare systems. BMC Health Serv Res. (2014) 14(1):478. doi: 10.1186/1472-6963-14-478
5. Øyri SF, Braut GS, Macrae C, Wiig S. Hospital managers’ perspectives with implementing quality improvement measures and a new regulatory framework: a qualitative case study. BMJ Open. (2020) 10(12):e042847. doi: 10.1136/bmjopen-2020-042847
7. Eklof M, Torner M, Pousette A. Organizational and social-psychological conditions in healthcare and their importance for patient and staff safety. A critical incident study among doctors and nurses. Saf Sci. (2014) 70:211–21. doi: 10.1016/j.ssci.2014.06.007
8. Krause N, Dasinger LK, Deegan LJ, Rudolph L, Brand RJ. Psychosocial job factors and return-to-work after compensated low back injury: a disability phase-specific analysis. Am J Ind Med. (2001) 40(4):374–92. doi: 10.1002/ajim.1112
9. Aase K, Høyland S, Olsen E, Wiig S, Nilsen ST. Patient safety challenges in a case study hospital – of relevance for transfusion processes? Transfus Apher Sci. (2008) 39(2):167–72. doi: 10.1016/j.transci.2008.06.003
10. Birken S, Clary A, Tabriz AA, Turner K, Meza R, Zizzi A, et al. Middle managers’ role in implementing evidence-based practices in healthcare: a systematic review. Implement Sci. (2018) 13(1):149. doi: 10.1186/s13012-018-0843-5
11. Furunes T. Leadership in healthcare. In: Løvseth LT, de Lange AH, editors. Integrating the Organization of Health Services, Worker Wellbeing and Quality of Care. Cham: Springer (2020). p. 135–57.
12. Parand A, Dopson S, Renz A, Vincent C. The role of hospital managers in quality and patient safety: a systematic review. BMJ Open. (2014) 4(9):e005055. doi: 10.1136/bmjopen-2014-005055
13. Gutberg J, Berta W. Understanding middle managers’ influence in implementing patient safety culture. BMC Health Serv Res. (2017) 17(1):582. doi: 10.1186/s12913-017-2533-4
14. Burgess N, Strauss K, Currie G, Wood G. Organizational ambidexterity and the hybrid middle manager: the case of patient safety in UK hospitals. Hum Resour Manage. (2015) 54(S1):s87–109. doi: 10.1002/hrm.21725
15. Carayon P, Schoofs Hundt A, Karsh BT, Gurses AP, Alvarado CJ, Smith M, et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. (2006) 15(suppl 1):i50–8. doi: 10.1136/qshc.2005.015842
16. Carayon P, Wooldridge A, Hoonakker P, Hundt AS, Kelly MM. SEIPS 3.0: human-centered design of the patient journey for patient safety. Appl Ergon. (2020) 84:103033. doi: 10.1016/j.apergo.2019.103033
17. Yin RK. Case Study Research and Applications: Design and Methods. 6th edn ed. Los Angeles, California: SAGE (2018).
19. helsetjenesten Foloki. Forskrift om ledelse og kvalitetsforbedring i helse- og omsorgstjenesten. (2017).
20. Helsedirektoratet. Nasjonal handlingsplan for pasientsikkerhet og kvalitetsforbedring 2019–2023. (2019).
22. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3(2):77–101. doi: 10.1191/1478088706qp063oa
23. Carayon P, Perry S. Human factors and ergonomics systems approach to the COVID-19 healthcare crisis. Oxford. (2021) 33(Supplement_1):1–3. doi: 10.1093/intqhc/mzaa109
24. Carayon P, Wetterneck TB, Rivera-Rodriguez AJ, Hundt AS, Hoonakker P, Holden R, et al. Human factors systems approach to healthcare quality and patient safety: systems ergonomics/human factors. Appl Ergon. (2014) 45(1):14–25. doi: 10.1016/j.apergo.2013.04.023
25. Dul J, Bruder R, Buckle P, Carayon P, Falzon P, Marras WS, et al. A strategy for human factors/ergonomics: developing the discipline and profession. Ergonomics. (2012) 55(4):377–95. doi: 10.1080/00140139.2012.661087
26. Grinde E, Nilsen Y, Valebrokk K. Lederne. Balansekunstnerne: om Lederne og ledelse i 100 år. Lysaker: Dinamo (2010).
27. Hartviksen TA, Sjolie BM, Aspfors J, Uhrenfeldt L. Healthcare middle managers’ experiences developing leadership capacity and capability in a public funded learning network. BMC Health Serv Res. (2018) 18(1):433. doi: 10.1186/s12913-018-3259-7
28. Bradley EH, Taylor LA, Cuellar CJ. Management matters: a leverage point for health systems strengthening in global health. Int J Health Policy Manag. (2015) 4(7):411–5. doi: 10.15171/ijhpm.2015.101
29. Birken SA, Lee S-YD, Weiner BJ. Uncovering middle managers’ role in healthcare innovation implementation. Implement Sci. (2012) 7(1):28. doi: 10.1186/1748-5908-7-28
30. Birken SA, Lee S-YD, Weiner BJ, Chin MH, Chiu M, Schaefer CT. From strategy to action: how top managers’ support increases middle managers’ commitment to innovation implementation in health care organizations. Health Care Manage Rev. (2015) 40(2):159–68. doi: 10.1097/HMR.0000000000000018
32. Ree E, Wiig S. Employees’ perceptions of patient safety culture in Norwegian nursing homes and home care services. BMC Health Serv Res. (2019) 19(1):607. doi: 10.1186/s12913-019-4456-8
33. Ree E, Wiig S. Linking transformational leadership, patient safety culture and work engagement in home care services. Nurs Open. (2020) 7(1):256–64. doi: 10.1002/nop2.386
34. Sfantou DF, Laliotis A, Patelarou AE, Sifaki-Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. (2017) 5(4):73. doi: 10.3390/healthcare5040073
35. Trinchero E, Farr-Wharton B, Brunetto Y. A social exchange perspective for achieving safety culture in healthcare organizations. Int J Public Sect Manag. (2019) 32(2):142–56. doi: 10.1108/IJPSM-06-2017-0168
36. Graen GB, Uhl-Bien M. Relationship-based approach to leadership: development of leader-member exchange (LMX) theory of leadership over 25 years: applying a multi-level multi-domain perspective. Leadersh Q. (1995) 6(2):219–47. doi: 10.1016/1048-9843(95)90036-5
37. Hennestad BW, Revang Ø. Endringsledelse og ledelsesendring: fra plan til praksis. 3. utg. ed. Oslo: Universitetsforl (2017).
38. Holden RJ, Carayon P, Gurses AP, Hoonakker P, Hundt AS, Ozok AA, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. (2013) 56(11):1669–86. doi: 10.1080/00140139.2013.838643
39. Ree E, Johannessen T, Wiig S. How do contextual factors influence quality and safety work in the Norwegian home care and nursing home settings? A qualitative study about managers’ experiences. BMJ Open. (2019) 9(7):e025197. doi: 10.1136/bmjopen-2018-025197
40. Johannessen T, Ree E, Aase I, Bal R, Wiig S. Exploring managers’ response to a quality and safety leadership intervention: findings from a multiple case study in Norwegian nursing homes and homecare services. BMJ Open Qual. (2021) 10(3):e001494. doi: 10.1136/bmjoq-2021-001494
41. Hollnagel E. The ETTO Principle: Efficiency-Thoroughness Trade-Off: Why Things That Go Right Sometimes Go Wrong. 1st ed. London: CRC Press (2009).
42. Grant S, Guthrie B. Efficiency and thoroughness trade-offs in high-volume organisational routines: an ethnographic study of prescribing safety in primary care. BMJ Qual Saf. (2018) 27(3):199–206. doi: 10.1136/bmjqs-2017-006917
43. Glette MK, Wiig S. The role of organizational factors in how efficiency-thoroughness trade-offs potentially affect clinical quality dimensions – a review of the literature. Int J Health Gov. (2021) 26(3):250–65. doi: 10.1108/IJHG-12-2020-0134
44. Oreg S, Vakola M, Armenakis A. Change recipients’ reactions to organizational change:a 60-year review of quantitative studies. J Appl Behav Sci. (2011) 47(4):461–524. doi: 10.1177/0021886310396550
45. Løvseth LT. Quality of care. In: Løvseth LT, de Lange AH, editors. Integrating the Organization of Health Services, Worker Wellbeing and Quality of Care. Cham: Springer (2020). p. 15–47.
46. Davies HTO, Nutley SM, Mannion R. Organisational culture and quality of health care. Qual Health Care. (2000) 9(2):111–9. doi: 10.1136/qhc.9.2.111
47. Cappelen K. Pasientsikkerhetskultur i sykehjem. In: Aase K, editors. Pasientsikkerhet- teori og praksis. 3rd ed. Oslo: Universitetsforlaget (2018). p. 89–100.
48. Bergerød I, Wiig S. Ledelse og pasientsikkerhet. In: Aase K, editors. Pasientsikkerhet- teori og praksis. 3rd ed. Oslo: Universitetsforlaget (2018). p. 116–30.
49. Magerøy MR, Wiig S. The effect of full-time culture on quality and safety of care – a literature review. Int J Health Gov. (2023) 28(1):68–81. doi: 10.1108/IJHG-11-2022-0106
Keywords: leadership, patient safety, staff safety, quality, human factors
Citation: Magerøy MR, Macrae C, Braut GS and Wiig S (2024) Managing patient safety and staff safety in nursing homes: exploring how leaders of nursing homes negotiate their dual responsibilities—a case study. Front. Health Serv. 4:1275743. doi: 10.3389/frhs.2024.1275743
Received: 15 August 2023; Accepted: 19 January 2024;
Published: 29 January 2024.
Edited by:
Dirk De Korne, Erasmus University Rotterdam, NetherlandsReviewed by:
Brendan McCormack, The University of Sydney, AustraliaRené Schwendimann, University Hospital of Basel, Switzerland
© 2024 Magerøy, Macrae, Braut and Wiig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Malin Rosell Magerøy bWFsaW4uci5tYWdlcm95QHVpcy5ubw==
Abbreviations HSE, health, safety and environment; QPS, quality and patient safety; SEIPS, systems engineering initiative for patient safety.