
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Health Serv. , 27 June 2022
Sec. Cost and Resource Allocation
Volume 2 - 2022 | https://doi.org/10.3389/frhs.2022.886513
 Métogara Mohamed Traore1*
Métogara Mohamed Traore1* Kéba Badiane2*
Kéba Badiane2* Anthony Vautier2
Anthony Vautier2 Arlette Simo Fotso3
Arlette Simo Fotso3 Odé Kanku Kabemba4
Odé Kanku Kabemba4 Nicolas Rouveau3
Nicolas Rouveau3 Mathieu Maheu-Giroux5
Mathieu Maheu-Giroux5 Marie-Claude Boily6
Marie-Claude Boily6 Joseph Larmarange3Fern Terris-Prestholt7
Joseph Larmarange3Fern Terris-Prestholt7 Marc d'Elbée8 for the ATLAS Team
Marc d'Elbée8 for the ATLAS TeamAchieving the first 95 of the UNAIDS targets requires the implementation of innovative approaches to knowing one's HIV status. Among these innovations is the provision of HIV self-testing (HIVST) kits in west Africa by the international partner organization Solthis (IPO). In order to provide guidance for the optimal use of financial resources, this study aims to estimate the program and site level costs of dispensing HIVST as well as HIV testing services (HTS)-excluding HIVST-in health facilities in Côte d'Ivoire, Mali and Senegal as part of the ATLAS project. We estimated from the provider's perspective, HIVST and HTS incremental costs using top-down and bottom-up costing approaches and conducted a time and motion study. We identified costs at the program level for HIVST (including IPO central costs) and at the site level for HIVST and HTS. The economic costs of distributing HIVST kits were assessed in 37 health facilities between July 2019 and March 2021 (21 months). Sensitivity analyses were also performed on unit costs to examine the robustness of our estimates related to key assumptions. In total, 16,001 HIVST kits were dispensed for 32,194 HTS sessions carried out. Program level HIVST average costs ranged $12–286, whereas site level costs ranged $4–26 across distribution channels and countries. Site level HTS costs ranged $7–8 per testing session, and ranged $72–705 per HIV diagnosis. Across countries and channels, HIVST costs were driven by personnel (27–68%) and HIVST kits (32–73%) costs. The drivers of HTS costs were personnel costs ranging between 65 and 71% of total costs across distribution channels and countries, followed by supplies costs between 21 and 30%. While program level HIVST average costs were high, site level HIVST average costs remained comparable to HTS costs in all countries. Health facility-based distribution channels operating at low volume exhibit high proportion of central costs which should be considered carefully for financial planning when run alongside high volumes mobile outreach distribution channels. HIVST can diversify the HIV testing offer at health facilities, thus improving access to screening for target populations not reached by HTS services.
The ambitious 95-95-95 strategy was announced by UNAIDS in 2020 aiming to end the AIDS epidemic by 2030 (1) by achieving 95% diagnosed among all people living with HIV (PLHIV), 95% on antiretroviral therapy (ART) among diagnosed, and 95% virally suppressed among treated (2). It is the result of the programmatic efforts of the actors who have thus made it possible to double in more ten years the annual volume of HIV tests carried out in sub-Saharan Africa (3, 4). In 2021, key populations and their sexual partners accounted for 72% of new adult HIV infections, and women and girls (aged 15 to 49 years) represented 65% in west and central Africa (5). The prevalence in the general population (15–49) was ranging from 0.6 to 3.8 (Côte d'Ivoire = 3.8; Mali = 1.3; Senegal = 0.6) (5). In west and central Africa, the coverage of HIV testing and antiretroviral therapy has grown at a quicker pace in recent years (81% people living with HIV who know their status), with nearly 77% of people living with HIV receiving antiretroviral therapy and 62% virally suppressed (5). In 2020, key populations (sex workers and their clients, gay men and other men who have sex with men, people who inject drugs, transgender people) and their sexual partners accounted for 65% of HIV infections globally whose 39% of new HIV infections in sub-Saharan Africa. Also, the risk of contracting HIV is, respectively, 35, 26, and 25 times higher among people who inject drugs, for sex workers and among gay men and other men who have sex with men (6).
In order to reach the first 95 in west Africa, it is necessary to implement approaches that reach those in need of HIV testing and who are being missed (4). One of the means used for this strategy is the provision of HIV self-testing (HIVST) kits to populations at risk. HIVST is an innovative method where a person collects his/her own specimen (oral fluid or blood), performs a rapid HIV test, and interprets the result, often in a private environment (7). It is a complementary testing approach, often seen as convenient and is highly accurate (8–10). Recent studies evaluated opportunities for implementing HIVST among key populations in Ghana (11). The authors found that a conducive and private environment was a factor facilitating the learning and practice of HIVST. It reduced stigma, and guaranteed the safety of vulnerable people by contributing to high rates of HIVST use. Other studies suggested that the ability of primary contacts to distribute HIVST kits to their contacts could be limited due to specific barriers such as acts of violence against FSW by their clients (12, 13).
The ATLAS project, implemented by the international partner organization (IPO) Solthis (Solidarité thérapeutique et initiative pour la santé) in Côte d'Ivoire, Mali and Senegal, promotes the distribution of HIVST to hard-to-reach/hidden populations as a complementary approach to traditional HIV testing services (HTS). In the context of this study, HTS definition excludes HIVST kits provision. Two main strategies are adopted: a large-scale strategy using mobile outreaches (mobile strategy) and a small-scale strategy in health facilities. The health facilities strategy aims to reach female sex workers (FSW), men who have sex with men (MSM), people who use drugs (PWUD), partners of sexually transmitted infections patients (STI) and sexual partners of PLHIV (Index Testing) in health facilities (Appendix 1). Regarding the introduction of HIVST in health facilities (fixed strategies), HTS is preferred (except PLHIV) for the patient coming in the health facility and HIVST is only offered for patients refusing HTS. In a primary distribution strategy, the HIVST kit is distributed directly to the intended user whereas for the secondary distribution, the kit is offered to a primary contact who will redistribute it to a secondary recipient. Secondary distribution strategies is preferred with the ATLAS project, allowing to reach hidden key populations, such as clients of FSW, partners of MSM, or index partners of pregnant women who are not routinely tested (12–15). Large scale programs being expanded nationally often benefit from economy of scale, even when incurring high initial fixed costs during the pilot phases as observed with ATLAS mobile strategies presented elsewhere (16, 17). On the other hand, low-volume interventions such as ATLAS health facilities strategies often pose challenges to estimating average costs (=total program costs/number of HIVST kits distributed) for informing analyses of cost-effectiveness and national program budgets. These observed average costs tend to be very high due to low output volumes and need to be considered carefully if to be used by program planners and researchers.
To establish the merits of the use of HIVST and therefore the adaptation of programmatic strategies and optimal financing in the fight against HIV in health facilities, data on costs at the level of programs and intervention sites prove necessary (18). Therefore, there is an urgent need to fill this knowledge gap regarding the costs of integrating HIVST into low-volume structures in West Africa.
The objective of this study is to estimate and analyse the program and site level costs of dispensing HIVST and providing HTS in health facilities using real-word data collected in Côte d'Ivoire, Senegal and Mali as part of the ATLAS project. The results of this study will inform HIV funding programs while providing key information for guiding actions tailored to low-volume health facilities.
This study focused on HIVST distribution channels implemented in health facilities and targeting, FSW, MSM, PWUD, partners of STI patients and partners of PLHIV (Table 1). There were no MSM distribution channel in Senegal, and no PWUD channel in Mali.
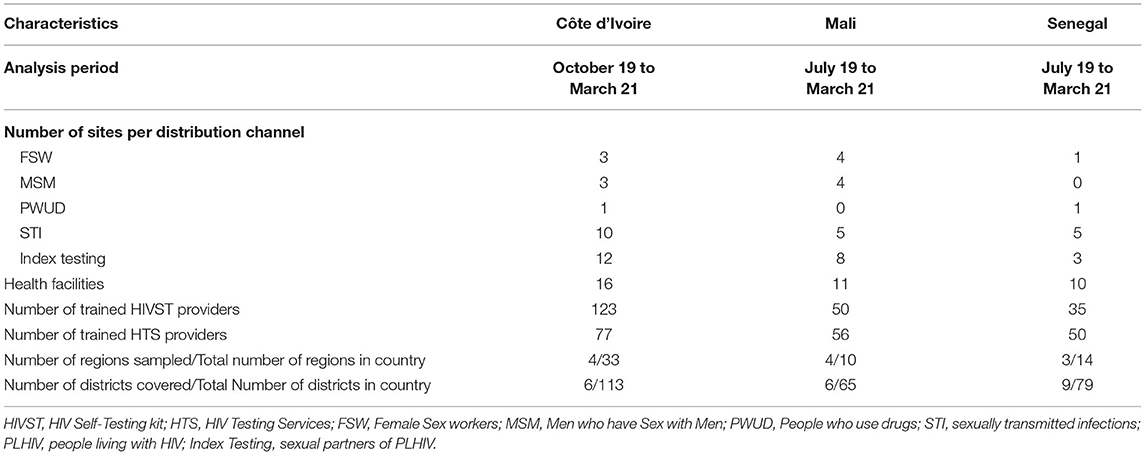
Table 1. Overview of the ATLAS project's implementing health facilities by country.
For HIVST cost data collection in the real-word, we used a top-down costing approach to collate the IPO's financial expenditures and categorize each cost item by input type and distribution channel (19). Also, on site observations were conducted to estimate donated goods/services such as personnel in the field or some equipment costs (bottom-up costing) to estimate economic costs (Appendix 2). Finally, a time and motion study was conducted to allocate field-based personnel costs based on the proportion of time spent on HIVST distribution and HTS, respectively (18, 20). HIVST program data were obtained from the IPO. HTS cost and program data were collected through bottom-up costing only.
We conducted convenience sampling of sites, based on the type of distribution channel, the cohort size estimated of each distribution channel, and contextual factors such as accessibility to the HIV testing site. Because HIVST implementation was progressive over time, the analysis period was 21 months in Senegal and Mali, and 18 months in Côte d'Ivoire. Some sites having opened in 2021, only health facilities where the distribution of HIVST was effective throughout the implementation phase were taken into account and started in 2019 were retained. There were 16 distribution sites in Côte d'Ivoire, 10 in Mali, and 11 in Senegal. The majority of these sites were public facilities (78%). A site is defined either as a primary health care facility for general population and/or key populations, a sexual health clinic, or a community health centre recognized by government authorities. Overall, HIVST kits were distributed by 208 agents (Côte d'Ivoire = 123; Mali = 50; Senegal = 35) of whom 183 were counselors (Côte d'Ivoire = 77; Mali = 56; Senegal = 50) also providing HTS. The study distinguishes providers that are the health care workers paid by the state budget (doctors, nurses, midwives, laboratory technicians or social workers) and financial and technical partners that are peer educators involved in project activities.
Data were analyzed among the sample sites according to the distribution channels FSW (Côte d'Ivoire = 3; Mali = 4; Senegal = 1), MSM (Côte d'Ivoire = 3; Mali = 4), PWUD (Côte d'Ivoire = 1; Senegal = 1), STI (Côte d'Ivoire = 10; Mali = 5; Senegal = 5) and Index Testing (Côte d'Ivoire = 12; Mali = 8; Senegal = 3) and we used standardized costing guidelines and analyzed data, ensuring consistency of methods across countries (16, 21). We conducted two economic cost analyses from the provider's perspective: HIVST and HTS. We distinguished between program and site level costs (Appendix 2).
Program costs were estimated for HIVST only, and include all costs incurred during the project phases and at all intervention levels (central, implementing partners headquarters, and delivery site levels) and provide costs of the entire program. These costs are distributed according to the three intervention phases of the project (Development, Start-up (start-up and other costs), Implementation) (Figure 1). The development phase (June 2018-March 2019) identified sustainable distribution models in each country; the start-up phase [April 2019-July 2019 (Senegal/Mali), October 2019 (Côte d'Ivoire)] consisted of the validation, adaptation and implementation of the training strategy for HIVST providers; and the implementation phase (until March 2021) corresponded to the effective distribution of HIVST kits, supervision and data validation activities. For HIVST, we also estimated site level costs at health facilities, therefore excluding central costs (IPO costs). For HTS, above site-level costs were not estimated because we did not have data access, therefore, only site level costs were estimated.
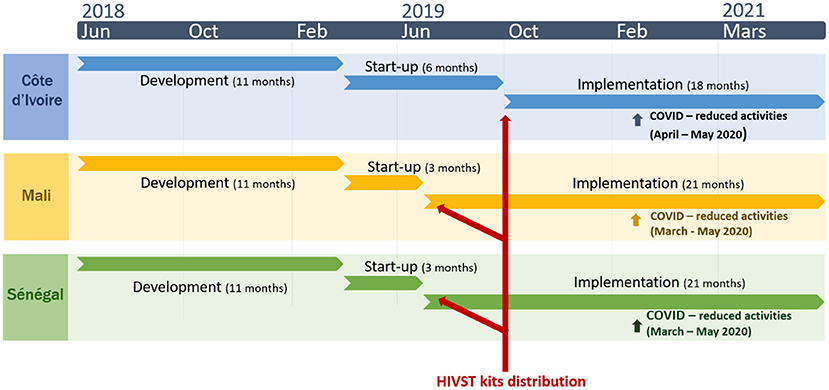
Figure 1. Description of the ATLAS project's three HIV self-testing (HIVST) deployment phases in Côte d'Ivoire, Senegal, and Mali over 2018–2021 [Source: (16)].
The HIVST kit purchase cost was provided by the IPO at $2.63 for Côte d'Ivoire and $3.08 for Senegal and Mali. Start-up, training, and all other capital costs were annualized using a 3% discount rate. All costs were estimated in 2021 US dollars (US$) using annual exchange rates (22). Inputs were categorized into capital and recurrent costs. We evaluated total costs, average and median costs per HIVST kit distributed, per HTS patient tested, and per HIV diagnosis.
Financial costs were allocated to sites based on allocation factors presented in Appendix 3. These factors included the percentage of HIVST distributors in each site, the estimated cohort size estimated of each distribution channel, the percentage of HIVST kits distributed, and the percentage of expenditure. The percentage of expenditure was an average obtained by weighting the total expenditures after all other allocation factors had been applied to relevant cost inputs. For the estimation of the HIVST delivery costs, we conducted an incremental cost analysis, where only additional resources needed to add HIVST onto existing service provision were considered. The values of the “average costs” in the tables are based on an average of unit costs (total costs/output) from each site per channel for each country.
Finally, we conducted a series of one-way sensitivity analyses to examine the robustness of the results to different assumptions used in the cost analysis as follows (23, 24). We assessed the influence of (1) the allocation factors by mutually inverting the number of distributors by patient cohort for each distribution channel; (2) the duration of the project by varying the number of year used to annualise of the life of the development phases (5 and 15 years, base of 10 years), the duration of start-ups (2.5 and 7.5 years, base of 5 years) and training and awareness costs (1 and 3 years, base of 2 years); (3) the discount rate by the varying the annualization rate for all costs combined from 0 to 16% (compared to base case: 3%) (21).
Figure 2 presents the average cost per HIVST kit distributed vs. the volume of kits distributed for each site. The greater the volume of kits distributed, the lower is the average cost of the HIVST kit and vice versa, in all three countries.
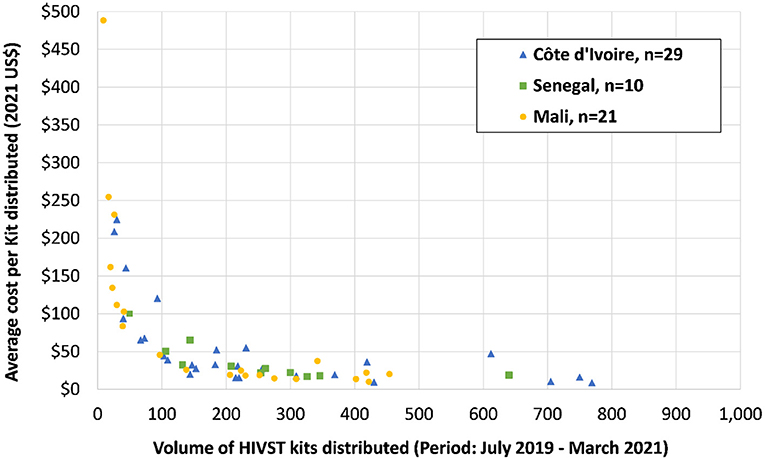
Figure 2. Average costs in health facilities by volume of HIVST Kits distributed by country (in 2021 US$).
Table 2 shows that in Côte d'Ivoire, the average costs in health facilities per HIVST kit distributed varied between distribution channels from $15 to 93 (FSW: $15; MSM: $15; PWUD: $12; STI: $31; Index Testing: $91), average costs per distributed kit ranged from $20 to 286 (FSW: $19; MSM: $90; STI: $145; Index: $286) in Mali, and ranged between $19 and 38 (FSW: $22; PWUD: $19; STI: $30; Index Testing: $38) in Senegal.
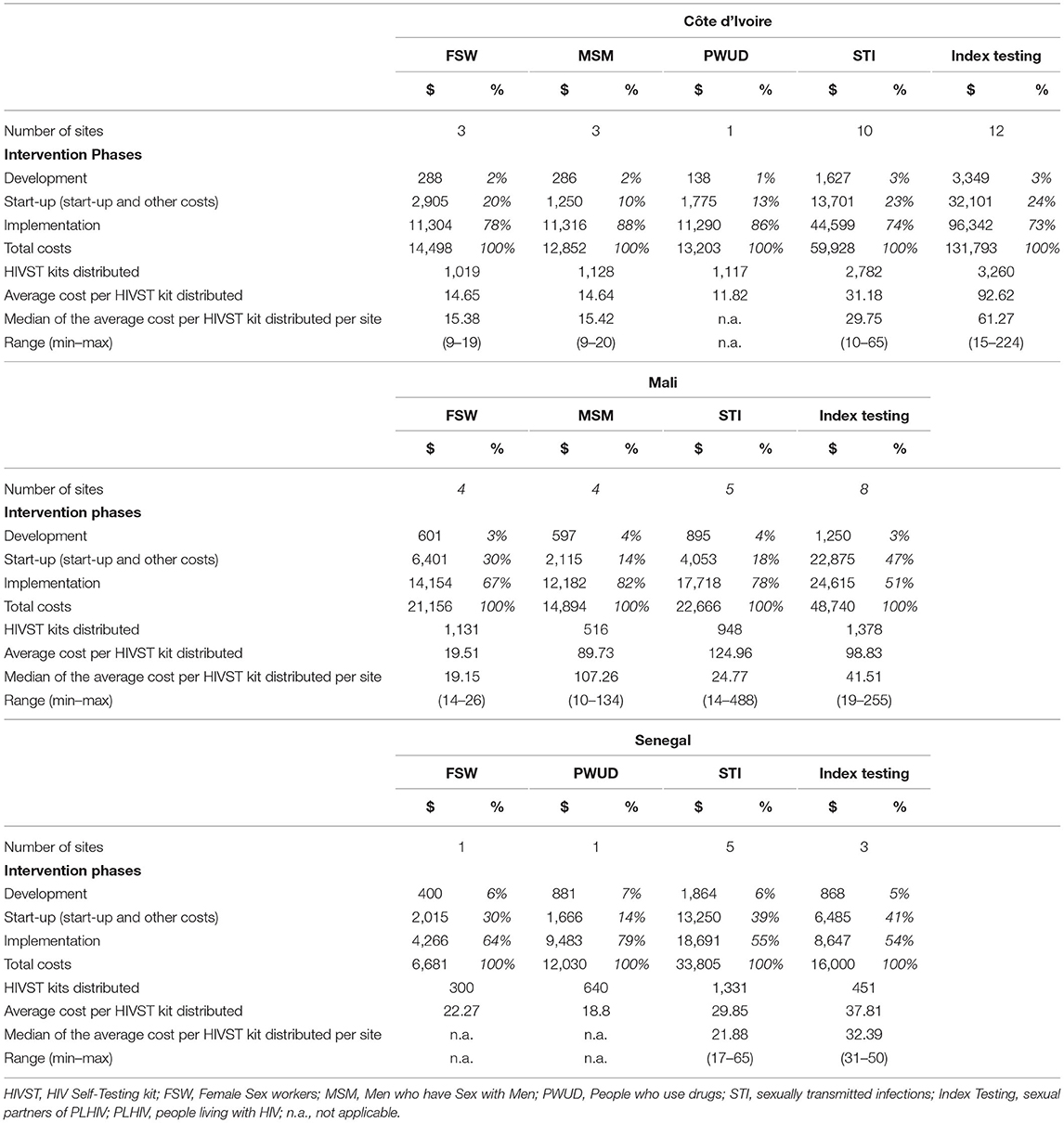
Table 2. Total, average, median and range of program level HIV self-testing costs, by country, by distribution channel, and by intervention phase in health facilities (in 2021 US$).
Figures 3A,B present HIVST average costs health facilities at program level by countries and distribution channel. They also highlight the proportion of site level costs ranging from 15 to 59%. In all countries, site level HIVST average costs range between $4 and 26 depending on the distribution channel and country (Table 3). Between 14 and 54% of these costs are induced by staff–Administration / management costs, 7–23% by staff-HIV testing providers, and 32–73% by HIVST kits costs. Average costs ranged from $4 to 8 in Côte d'Ivoire, $7 to 26 in Mali, and $4 to 5 in Senegal.
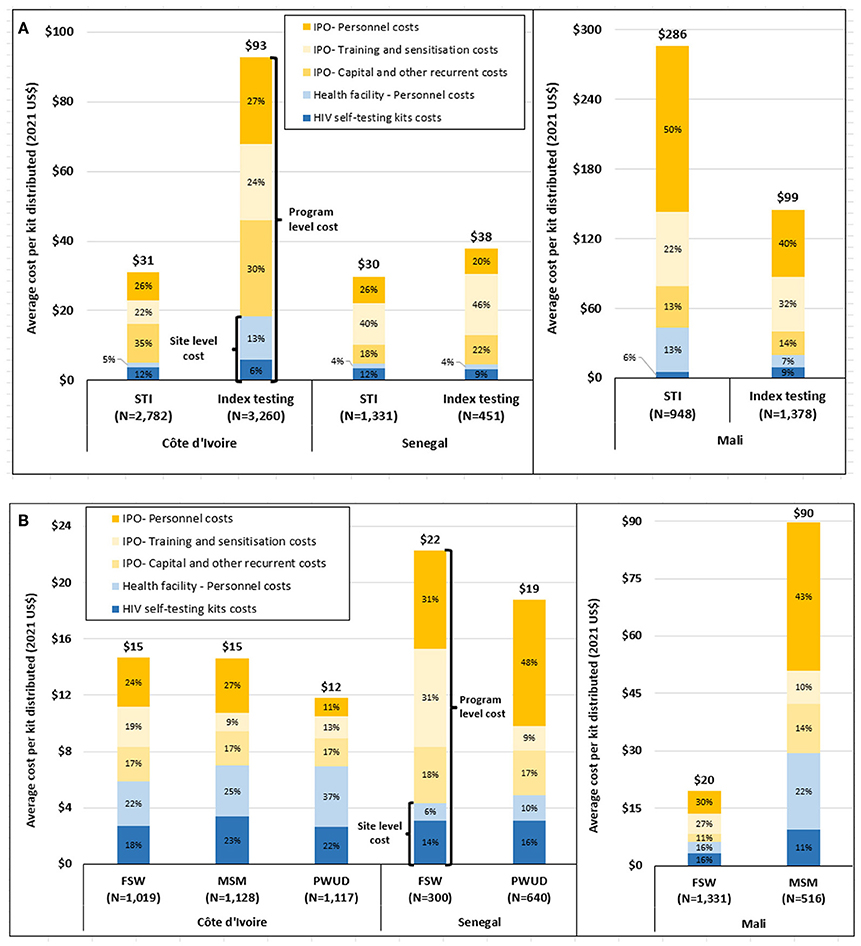
Figure 3. (A) Program and site level HIVST average costs in health facilities for the STI and Index testing distribution channels by country (in 2021 US$). (B) Program and site level HIVST average costs health facilities for the FSW, MSM and PWUD distribution channels by country (in 2021 US$). HIVST, HIV Self-Testing kit; FSW, Female Sex workers; MSM, Men who have Sex with Men; PWUD, People who use drugs; STI, sexually transmitted infections; Index, sexual partners of PLHIV; PLHIV people living with HIV.
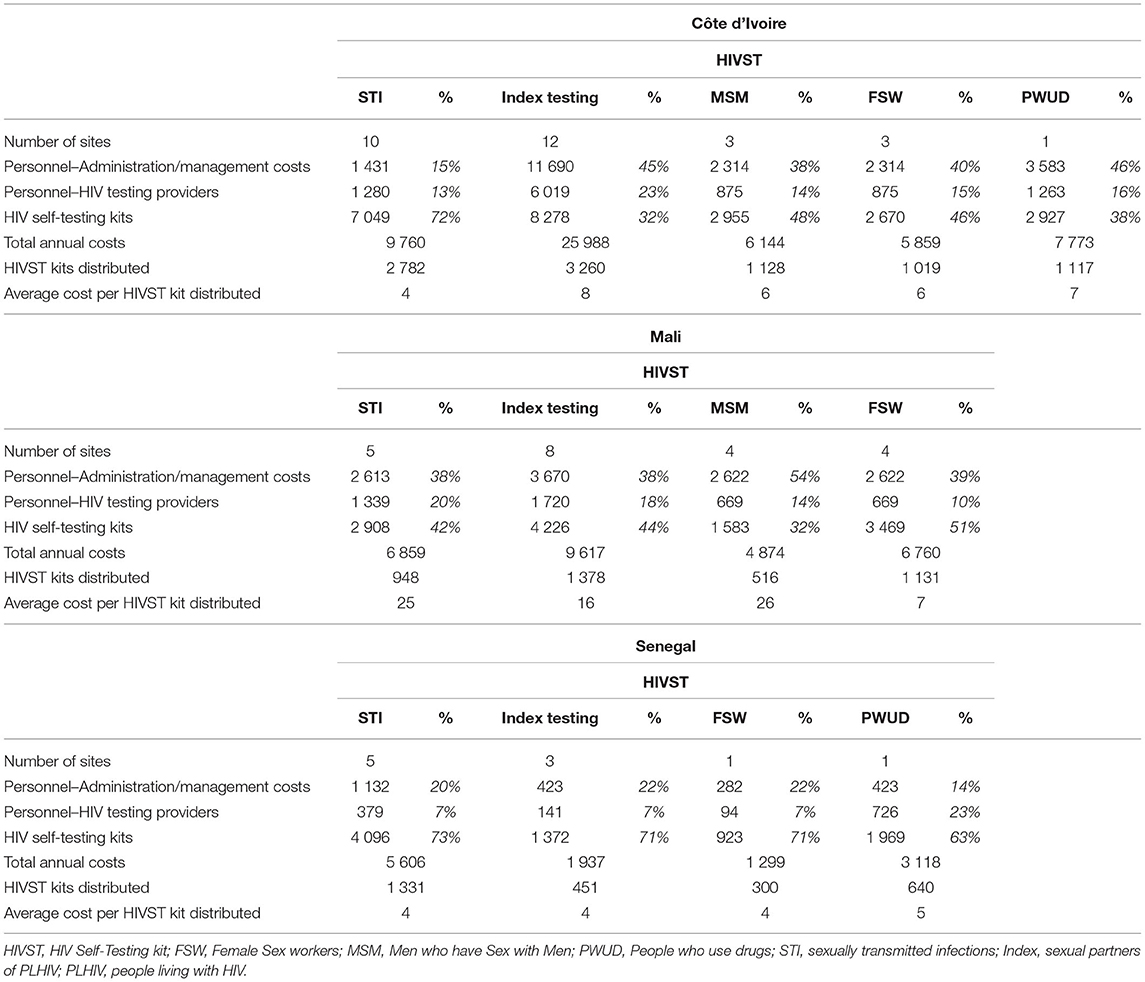
Table 3. Total and average site level HIV self-testing costs, by country, by distribution channel, and by expense item in health facilities (in 2021 US$).
Site level HTS average costs per person tested are comparable between STI and Index Testing services and range from $7 to 8 (Appendix 4). The average costs per HIV diagnosis range from $72 to 705. The cost drivers are personnel costs representing between 65 and 71% of total costs across distribution channels and countries, followed by costs of supplies between 21 and 30% and all other costs between 2 and 13%.
Average observed costs per HIVST kit distributed remain robust when key cost parameters are varied (Appendix Figures 5A–C). In Côte d'Ivoire, varying life of start-up sensitization and training between 1 and 3 years has the strongest effect on costs ranging between $14–16, $14–15, $11–13, $29–31, $92–94 for FSW, MSM, PWUD, STI, and Index Testing respectively. The variation of the assumed length of life for the development and start-up phases, and the variation of the discount rate have a moderate effect with less than a dollar variation. Switching trained distributors with the size of PLHIV cohorts in sites has a small effect with <$2 variation of average costs in all countries. In Mali, the discount rate has the strongest effect for the Index Testing ($98–100), STIs ($124–126) and MSM ($89–91), but only varies by <$2 for other parameters.
In this study, based on routine and observed data from public health service providers and administrative partners, we estimated at program and site level the average costs of low-volume delivery models for implementing HIVST and HTS strategies in health facilities in three west African countries. To our knowledge, this is the first multi-country cost analysis of the integration of HIVST into health facilities with small dispensing volumes in west Africa.
HIVST average cost showed some variability between countries ranging from $12 to 93 in Côte d'Ivoire, $20 to 286 in Mali and $19 to 38 in Senegal. Site level HIVST average costs ranged $4–26 across distribution channels and countries. Site level HTS costs ranged $7–8 per testing session, and ranged $72–705 per HIV diagnosis. Across countries, average costs per HIVST were lowest for FSW, MSM and PWUD distribution channels followed by STI, then Index Testing distribution channel. These differences were mostly explained by the HIVST number of kits distributed between sites, so variation was observed between and within countries. Distribution channels with a lower volume of distribution had higher observed costs. Mali was marked by a very low dispensing volume for small sample health facilities with a total of dispensed 2326 kits for all distribution channels taken together but in Côte d'Ivoire, 2782 kits were distributed in STI services and 3260 kits for Index Testing over the same period of 18 months. Other factors also explained this. HIVST distribution for the Index Testing distribution channel is dependent on the PLHIV patients and sharing of their HIV status with their partner, a slow process that may require sensitization over several weeks/months of follow-up (25). It is also important to note that the different facility-based distribution channels could sometimes overlap as many individuals going to key population dedicated clinics are also STI patients and/or PLHIV.
HIVST small-scale health facility distribution channels are part of a national HIVST implementation program with large scale distribution channels for outreach HIVST generating high central costs (16, 26), so central costs are likely negligible for these low-scale distribution channels, when run alongside larger-scale models. In addition, central costs are also particularly high with the ATLAS integrated approach that entailed a lengthy implementation process with partners (16, 17), so even if our cost allocation method of central costs was based on volumes, these central costs would still remain high–as shown by our sensitivity analysis.
Such information is essential in designing sustainable and cost-effective models of HIVST as countries approach the UNAIDS 95-95-95 targets (21). In southern Africa, HIVST costing studies were conducted focusing either on outreach or on health facilities distribution of HIVST between 2017 and 2020. These studies reported average costs per kit distributed of $9.66 for Malawi, $17.70 for Zambia, and $14.91 for Zimbabwe and incremental average costs of $15.40 and 14.00 in early and later phases of an outreach HIVST distribution program in Lesotho (27, 28). Another health facility based HIVST distribution study was done in Malawi and reported average costs of $4.99 (21).
The average costs of the HIVST dispensation of the STI and Index Testing distribution channels, excluding central costs, are on the same scales or even lower than those of the HTS. However, cost comparison between HIVST and HTS should be cautious. In the case of Index Testing, HIVST provision is conducted through secondary distribution whereas HTS requires the partner to come to the health facility. When comparing with recent similar studies at health facilities in southern Africa, HIVST average cost through the primary distribution approach given by Sande and al. are $4.27 in Zambia and $9.24 in Zimbabwe (21), while Mwenge et al. found that the cost per individual person tested using HTS is $5.03 in Malawi, $4.24 in Zambia, and $8.79 in Zimbabwe (27).
A study was conducted by Ahmed et al. in low HIVST volume health facilities in Malawi, Zambia and Zimbabwe where costs ranged from US$5.20 to 58.92 per kit distributed. Higher costs were associated with low scale of activity and poor integration of HIVST distribution into existing health services (29). During the ATLAS project, it is likely that other factors played a role on the estimation of costs. For instance, In Mali, there were safety concerns due to the country's rebellion in August 2020 and ongoing armed conflict with an intermittent suspension of fieldwork activities. Finally, the COVID-19 pandemic also led to reduced activities during 2–3 months because of lockdown's restrictions in Côte d'Ivoire, Mali, and Senegal (30), leading to high observed costs, although self-testing was shown to be a timely alternative to provider-delivered HIV testing during periods of lockdown and reduced social interactions.
Across countries, the site level average cost of integrating HIVST into health facilities ranged from $4 to 26 per kit distributed. Site level costs would be considered closer to those used for financial planning than program level average costs. Those per HTS carried out varied between $7–8. Personnel and HIVST kits were the major cost drivers. So, the average costs of introducing HIVST in fixed low-volume strategies were slightly higher than those of HTS. These costs being comparable, there is an opportunity to diversify the offer of HIV testing at health facilities and potentially improve access to screening for target populations not reached by HTS. Consideration of task shifting for the HIVST distribution through Index testing distribution channels from medical team to non-medical could also be cost saving as it was suggested with a case study in Mali in 2020 (17).
This study has some limitations. First, our outcome metric “per HIVST kit distributed” does not fully capture the HIVST cascade and additional costs would be incurred for linkage to confirmatory testing and HIV care services. For example, there remain uncertainties related to the true percentage of kits used in the secondary distribution model. Second, total and average costs are estimated across a diverse range of fixed health facilities for each country leading to inevitable cost variation by distribution channel. Third, reduced sample sizes from original targets were due to COVID restrictions for data collection and challenging partnerships with public sites, particularly in Mali. Therefore, results for this country should be interpreted with caution. Finally, cost analyses of small-scale interventions often generate extreme average costs per output without much application for program planning. Our suggestion to consider site level costs for financial planning in this specific study assumes that HIVST programs in these countries would always have larger-scale mobile HIVST distribution strategies in place where central costs would be accounted for, which is the case of the ATLAS project. However, the risk of underbudgeting such small-scale fixed strategies by cutting off too much central costs still remain and requires careful financial planning.
Ultimately, economic valuation of real-world costs from small-volume health facilities can offer valuable information to improve future program operations and should therefore be included as an important element in overall program planning (31). Although the average costs of HIVST at the program level were high, the average costs of HIVST at the site level remained comparable to the costs of HTS in all countries. Low-volume, facility-based distribution channels have high core costs that need to be carefully considered for budgeting of small volume health interventions. HIVST can diversify the offer of HIV testing in health facilities and would allow to expand the range of screening services to target populations difficult to reach with HTS services while identifying “best practices” that can inform the successful implementation of programs on a global scale.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the London School of Hygiene and Tropical Medicine Research Committee (n° 17141/RR/13198, 31st March 2019) WHO Ethic Research Committee (n°ERC0003181, 7th August 2019), and by three national ethic committees: Comité National d'Ethique des Sciences de la vie et de la Santé de Côte d'Ivoire (n°049-19/MSHP/CNESVS-kp, 28th May 2019), ComitéNational d'Ethique pour la Recherche en santé du Sénégal (n°SEN19/32, 26th July 2019), and Comité d'Ethique de la Faculté de Médecine de Pharmacie et d'Odonto-Stomatologie de l'Université des Sciences et des Techniques de Bamako au Mali (n°2019/88/CE/FMPOS, 14th August 2019). The patients/participants provided their written informed consent to participate in this study.
Md'E and FT-P designed the study. Md'E coordinated the study. MT and KB conducted data collection and analysis and wrote the article. AV, AS, OK, NR, MM-G, M-CB, and JL provided logistical support and intellectual inputs. All authors revised the manuscript and agreed for publication.
The study was funded by UNITAID through Solthis. This work was supported by UNITAID (Grant Number 2018-23-ATLAS) with additional funding from Agence Française pour le Développement (AFD). The funders played no role in study design, data collection and analysis, the decision to publish or preparation of the manuscript.
The content is solely the responsibility of the authors and does not necessarily represent the official views of UNITAID, Solthis, or UNAIDS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank all the participants, and the operational field workers in Côte d'Ivoire, Mali and Senegal.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2022.886513/full#supplementary-material
1. UNAIDS_FactSheet_en.pdf. Available online at: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed February 11, 2022).
2. CROI 2022 the Progress in HIV Research. Available online at: https://viivhealthcare.com/hiv-news-and-media/medical-conferences-and-events/croi-2022/ (accessed February 11, 2022).
4. Cambiano V, Johnson CC, Hatzold K, Terris-Prestholt F, Maheswaran H, Thirumurthy H, et al. The impact and cost-effectiveness of community-based HIV self-testing in sub-Saharan Africa: a health economic and modelling analysis. J Int AIDS Soc. (2019) 22:e25243. doi: 10.1002/jia2.25243
5. JC3032_AIDS_Data_book_2021_En.pdf. Available online at: https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf (accessed April 29, 2022).
6. Global, HIV & AIDS statistics — Fact sheet,. Available online at: https://www.unaids.org/en/resources/fact-sheet (accessed May 5, 2022).
7. Narasimhan M, Kapila M. Implications of self-care for health service provision. Bull World Health Organ. (2019) 97:76–76A. doi: 10.2471/BLT.18.228890
8. Figueroa C, Johnson C, Ford N, Sands A, Dalal S, Meurant R, et al. Reliability of HIV rapid diagnostic tests for self-testing compared with testing by health-care workers: a systematic review and meta-analysis. Lancet HIV. (2018) 5:e277–90. doi: 10.1016/S2352-3018(18)30044-4
9. Narasimhan M, Allotey P, Hardon A. Self care interventions to advance health and wellbeing: a conceptual framework to inform normative guidance. BMJ. (2019) 365:l688. doi: 10.1136/bmj.l688
10. Lyons CE, Coly K, Bowring AL, Liestman B, Diouf D, Wong VJ, et al. Use and acceptability of HIV self-testing among first-time testers at risk for HIV in senegal. AIDS Behav. (2019) 23:130–41. doi: 10.1007/s10461-019-02552-2
11. Abubakari GM, Turner D, Ni Z, Conserve DF, Dada D, Otchere A, et al. Community-based interventions as opportunities to increase hiv self-testing and linkage to care among men who have sex with men – lessons from Ghana, West Africa. Front Public Health. (2021) 9:660256. doi: 10.3389/fpubh.2021.660256
12. Oldenburg CE, Ortblad KF, Chanda MM, Mwale M, Chongo S, Kanchele C, et al. Brief report: intimate partner violence and antiretroviral therapy initiation among female sex workers newly diagnosed with HIV in Zambia: a prospective study. J Acquir Immune Defic Syndr 1999. (2018) 79:435–9. doi: 10.1097/QAI.0000000000001841
13. Thirumurthy H, Masters SH, Mavedzenge SN, Maman S, Omanga E, Agot K. Promoting male partner testing and safer sexual decision-making through secondary distribution of HIV self-tests by HIV-uninfected female sex workers and women receiving antenatal and postpartum care in Kenya: a cohort study. Lancet HIV. (2016) 3:e266–74. doi: 10.1016/S2352-3018(16)00041-2
14. Rouveau N, Ky-Zerbo O, Boye S, Fotso AS, d'Elbée M, Maheu-Giroux M, et al. Describing, analysing and understanding the effects of the introduction of HIV self-testing in West Africa through the ATLAS programme in Côte d'Ivoire, Mali and Senegal. BMC Public Health. (2021) 21:181. doi: 10.1186/s12889-021-10212-1
15. Lippman SA, Lane T, Rabede O, Gilmore H, Chen YH, Mlotshwa N, et al. High acceptability and increased HIV testing frequency following introduction of hiv self-testing and network distribution among south African MSM. J Acquir Immune Defic Syndr 1999. (2018) 77:279–87. doi: 10.1097/QAI.0000000000001601
16. d'Elbée M, Traore MM, Badiane K, Vautier A, Simo Fotso A, Kabemba OK, et al. Costs and scale-up costs of integrating hiv self-testing into civil society organisation-led programmes for key populations in cote d'ivoire, Senegal, and mali. Front Public Health. (2021) 9:653612. doi: 10.3389/fpubh.2021.653612
17. d'Elbée M, Badiane K, Ky-Zerbo O, Boye S, Kanku Kabemba O, Traore M. Can Task Shifting Improve Efficiency of HIV Self-Testing Kits Distribution? A Case Study in Mali. In online: poster (2020). Available online at: http://interestworkshop.org/ (accessed February 18, 2022).
18. Al Dallal SAM, Farghaly M, Ghorab A, Elaassar M, Haridy H, Awad N, et al. Real-world evaluation of costs of illness for pneumonia in adult patients in Dubai—A claims database study. PLoS ONE. (2021) 16:e0256856. doi: 10.1371/journal.pone.0256856
19. Cunnama L, Sinanovic E, Ramma L, Foster N, Berrie L, Stevens W, et al. Using top-down and bottom-up costing approaches in LMICs: the case for using both to assess the incremental costs of new technologies at scale. Health Econ. (2016) 25:53–66. doi: 10.1002/hec.3295
20. GHCC. Global Heath Cost Consortium. Available online at: https://ghcosting.org/pages/standards/reference_case (accessed February 11, 2022).
21. Sande LA, Matsimela K, Mwenge L, Mangenah C, Choko AT, d'Elbée M, et al. Costs of integrating HIV self-testing in public health facilities in Malawi, South Africa, Zambia and Zimbabwe. BMJ Glob Health. (2021) 6:e005191. doi: 10.1136/bmjgh-2021-005191
22. Countries Compared by Economy > Central Bank Discount Rate. International Statistics at NationMaster.com. Available online at: http://www.nationmaster.com/country-info/stats/Economy/Central-bank-discount-rate (accessed February 11, 2022).
23. Candio P, Violato M, Leal J, Luengo-Fernandez R. Cost-effectiveness of mechanical thrombectomy for treatment of nonminor ischemic stroke across Europe. Stroke. (2021) 52:664-73. doi: 10.1161/STROKEAHA.120.031027
24. Basics of Health Economics. CELforPharma. Available online at: https://www.celforpharma.com/course/basics-health-economics (accessed February 18, 2022).
25. Boye S, Bouaré S, Ky-Zerbo O, Rouveau N, Simo Fotso A, d'Elbée M, et al. Challenges of HIV self-test distribution for index testing when HIV status disclosure is low: preliminary results of a qualitative study in bamako (Mali) as part of the ATLAS project. Front Public Health. (2021) 9:653543. doi: 10.3389/fpubh.2021.653543
26. Maheu-Giroux M, Diabaté S, Boily MC, Jean-Paul N, Vesga JF, Baral S, et al. Cost-effectiveness of accelerated HIV response scenarios in CoĹte d'Ivoire. J Acquir Immune Defic Syndr. (2019) 80:10. doi: 10.1097/QAI.0000000000001956
27. Mwenge L, Sande L, Mangenah C, Ahmed N, Kanema S, d'Elbée M, et al. Costs of facility-based HIV testing in Malawi, Zambia and Zimbabwe. PLoS ONE. (2017) 12:e0185740. doi: 10.1371/journal.pone.0185740
28. Mangenah C, Mwenge L, Sande L, Ahmed N, d'Elbée M, Chiwawa P, et al. Economic cost analysis of door-to-door community-based distribution of HIV self-test kits in Malawi, Zambia and Zimbabwe. J Int AIDS Soc. (2019) 22:e25255. doi: 10.1002/jia2.25255
29. Ahmed N. Reaching the First 90%: Cost-Effectiveness of HIV Self Testing Services in Zambia. (2021). Available online at: https://researchonline.lshtm.ac.uk/id/eprint/4659290 (accessed February 13, 2022).
30. Kra AK, Colin G, Diop PM, Fotso AS, Rouveau N, Hervé KK, et al. Introducing and implementing HIV self-testing in côte d'ivoire, mali, and senegal: what can we learn from ATLAS project activity reports in the context of the COVID-19 crisis? Front Public Health. (2021) 9:653565. doi: 10.3389/fpubh.2021.653565
31. Subramanian S, Tangka FKL, Hoover S, Nadel M, Smith R, Atkin W, et al. Recommendations from the international colorectal cancer screening network on the evaluation of the cost of screening programs. J Public Health Manag Pract. (2016) 22:461–5. doi: 10.1097/PHH.0000000000000386
Keywords: real-world data, HIV self-testing, HIV testing services, health facilities, cost analysis, Côte d'Ivoire, Mali, Senegal
Citation: Traore MM, Badiane K, Vautier A, Simo Fotso A, Kanku Kabemba O, Rouveau N, Maheu-Giroux M, Boily M-C, Larmarange J, Terris-Prestholt F and d'Elbée M (2022) Economic Analysis of Low Volume Interventions Using Real-World Data: Costs of HIV Self-Testing Distribution and HIV Testing Services in West Africa From the ATLAS Project. Front. Health Serv. 2:886513. doi: 10.3389/frhs.2022.886513
Received: 28 February 2022; Accepted: 23 May 2022;
Published: 27 June 2022.
Edited by:
Jason Madan, University of Warwick, United KingdomReviewed by:
Firdaus Hafidz, Gadjah Mada University, IndonesiaCopyright © 2022 Traore, Badiane, Vautier, Simo Fotso, Kanku Kabemba, Rouveau, Maheu-Giroux, Boily, Larmarange, Terris-Prestholt and d'Elbée. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Métogara Mohamed Traore, dHJhb3JlbWV0b2dhcmFtb2hhbWVkQGdtYWlsLmZy; Kéba Badiane, a2ViYWRpYW5lQG91dGxvb2suZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.