
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Health Serv., 20 December 2021
Sec. Health Policy and Management
Volume 1 - 2021 | https://doi.org/10.3389/frhs.2021.766677
This article is part of the Research TopicSelected Practical Perspectives in Health Policy and Management: 2022View all 6 articles
 Wenxing Wang1*
Wenxing Wang1* Jeroen van Wijngaarden1
Jeroen van Wijngaarden1 Hujie Wang1
Hujie Wang1 Martina Buljac-Samardzic1
Martina Buljac-Samardzic1 Shasha Yuan2
Shasha Yuan2 Joris van de Klundert1,3
Joris van de Klundert1,3Background: China has been encouraged to learn from international innovations in the organization and management of health service delivery to achieve the national health reform objectives. However, the success and effectiveness of implementing innovations is affected by the interactions of innovations with the Chinese context. Our aim is to synthesize evidence on factors influencing the implementation of non-Chinese innovations in organization and management of health service delivery in mainland China.
Methods: A systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We searched seven databases for peer-reviewed articles published between 2009 and 2020. Data were analyzed and combined to generate a list of factors influencing the implementation of foreign innovations in China. The factors were classified in the categories context, system, organization, innovation, users, resources, and implementation process.
Results: The 110 studies meeting the inclusion criteria revealed 33 factors. Most supported by evidence is the factor integration in organizational policies, followed by the factors motivation & incentives and human resources. Some factors (e.g., governmental policies & regulations) were mentioned in multiple studies with little or no evidence.
Conclusion: Evidence on factors influencing the implementation of foreign innovations in organization and management of health service delivery is scarce and of limited quality. Although many factors identified in this review have also been reported in reviews primarily considering Western literature, this review suggests that extrinsic motivation, financial incentives, governmental and organizational policies & regulations are more important while decentralization was found to be less important in China compare to Western countries. In addition, introducing innovations in rural China seems more challenging than in urban China, because of a lack of human resources and the more traditional rural culture.
The Chinese government has committed to establishing a health system that is accessible, equitable, affordable and efficient for all (1). Improving health service delivery forms a major challenge in achieving these objectives (2). Given the complexity and scale of this challenge, a sequence of incremental improvement steps is unlikely to suffice. Substantial innovations in the management and organization of service delivery are called for (3). Moreover, China has been encouraged to learn from “international best practices” in pursuit of service delivery innovation (4).
Innovation of the management and organization of service delivery has been broadly defined as: “A novel set of behaviors, routines, and ways of working, that are directed at improving health outcomes, administrative efficiency, cost effectiveness, or users experience and that are implemented by planned and coordinated actions” (5). China is actively adopting a wide variety of innovative international practices in the management and organization of health service delivery that are novel to China. For example, China is introducing “family doctors to rejuvenate the three-tier network” of the Chinese health system, integrating and strengthening primary care in analogy with health systems in Western countries (6, 7). However, the success of implementing such innovations, may depend on unpredictable interactions of the innovations in and with the context (5). For instance, differences in organizational cultures between countries may influence the effectiveness of an innovation (8, 9). Innovations which have been developed in Western healthcare systems may be challenging to implement in China, where the working culture is more collective and the power distance in organizations is much higher (10). At the least, the contextual differences typically imply that adaptation is needed.
Previous systematic reviews have identified factors that influence the spread and implementation of innovations in the management and organization of health service delivery, such as the characteristics of innovations and the system antecedents for innovations (5, 11). However, these reviews are primarily based on Western literature and lack evidence on the spread of innovations in management and organization of health service delivery in other context and from Western to non-Western healthcare systems, such as China.
Several studies on the implementation of innovations in the management and organization of health service delivery in the Chinese context have revealed factors influencing the success of implementation, such as knowledge & skills of those involved and their awareness of the innovation and their roles in the implementation (12–14). However, present knowledge and understanding are scarce and fragmentary. To gain a systematic understanding of factors that influence the successful implementation of such innovations from abroad in China, we conducted a systematic literature review. The main research question of the systematic review was: what factors influence the implementation of innovations in management and organization of health service delivery that are developed abroad and implemented in China?
The following seven databases (4 English and3 Chinese) were systematically searched for eligible studies: Embase, Medline ALL Ovid, Web of Science Core Collection, Cochrane CENTRAL register of trials, CNKI, VIP, and WANFANG. We restricted the year of publication to 2009 and later because in 2009 China initiated a new round of national health-care reform in which it explicitly intended to adopt international best practices (10, 15). The design of the English and Chinese literature searches was supported by a Dutch and a Chinese librarian respectively to promote equivalence of the search strategies. The search strategies are included in Supplementary Material 1.
Studies which met all criteria below were included:
• Address innovations related to the organization and management of health service delivery;
• The innovations originate from abroad;
• The innovations are implemented in mainland China;
• The studies present factors influencing the implementation;
• Presents original empirical research;
• Published in a peer-reviewed scientific journal;
• Published between 2009-2020, with all data collected in 2009 or later;
• Written in English or Chinese.
The screening process consisted of two steps. In the first step, three researchers (WW, JW, and WH) independently screened all English-written articles (WW and JW) and Chinese-written articles (WW and WH) by scanning the titles and abstracts. Articles were excluded if they did not meet all inclusion criteria. If disagreement existed, the articles were then screened by a third reviewer (JvdK: English and YS: Chinese) who had a decisive vote. The origin of the innovations was not always explicitly specified. In such cases, the first author performed an internet search for additional information. Based on this information, articles were excluded if there was consensus among three reviewers (WW, JW, JvdK) that the innovation was not from outside China. In the second step, three reviewers (WW, JW, and WH) independently screened the articles by closely reading the full texts. In case of disagreement, the same third reviewers (JvdK, YS) made the final decision.
Data were extracted using a form which summarized author(s), year of publication, innovation, study aims, context, innovation origin, study design, factors presented as study results, factors proposed otherwise (e.g., mentioned in the introduction or discussion), and conclusions. As the Chinese context and our cross-border innovation focus are essentially different from the Western contexts of the evidence considered in preceding reviews and on which existing frameworks are based, we adopted an inductive approach. This avoids limitations imposed by deductively following frameworks whose validity is not established for the Chinese context. Moreover, it naturally allows identifying factors and categories for which apparently no evidence has been identified in Western reviews but which are relevant in the Chinese context (5, 11, 16). Following the approach of other systematic reviews to identify factors from a heterogenous set of qualitative and quantitative studies, we conducted a narrative synthesis (17, 18). In our study, two authors (WW and JW) conducted inductive data analysis independently, in the form of close reading of all included studies to identify factors and categories of factors. The identified factors were categorized, synthesized and discussed in various inductive cycles until consensus was reached. Furthermore, the two other authors (MB, JvdK) were involved to assess the consistency and logic of these factors and categories, resulting in three more improvement iterations until final consensus among all authors.
The heterogeneity of the included studies brought along a wide variety in research design and quality (19). We assessed the level of the evidence presented using the classification of the Oxford Center for Evidence Based Medicine (OCEBM level) (20).
The search strategy resulted in 5499 articles after 3860 duplicate records were removed. Of these, 417 met all inclusion criteria in the first step and were included for full text screening. After the second round, 110 articles were included for the review. Figure 1 shows the PRISMA flow diagram. Before reporting on the findings, we present a synthesis of descriptives on the included studies.
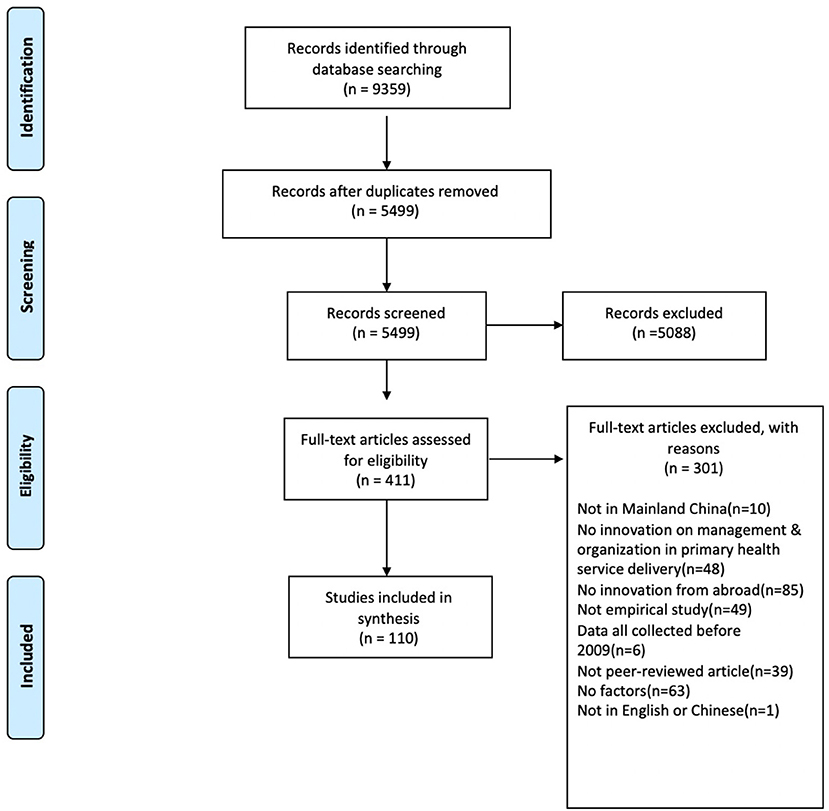
Figure 1. PRISMA 2009 flow diagram.
More than one-third of the studies (n = 43, 39%) presented evidence on factors influencing the implementation of the innovation in the study results (see Supplementary Material 2). Almost two-third of the studies (n = 67, 61%) discussed possible factors without presenting evidence (see Supplementary Material 3). The 43 studies with evidence mostly had quantitative designs (n = 27, 24.5%), while some had a qualitative design (n = 11, 10%) or used mixed methods (n = 5, 4.5%). Following the OCEBM evidence classification, most studies (n = 106, 97%) presented level 3, 4 or 5 evidence. The quantitative studies that used stronger designs (level 1 or 2) were not designed to identifying factors influencing the implementation of the innovation and discussed such factors rather than presenting evidence as a result of the research conducted.
The reader may also find the descriptive synthesis of the wide variety of innovations introduced in the included studies presented in Supplementary Material 4 helpful to develop an impression of the studies and evidence included. It categorizes each of the studies, where each study is categorized only once even it may fit in multiple categories. The main categories are evidence-based best practices (n = 42, 38%), integrated care approaches (n = 26, 24%) and management tools (e.g., balanced score card) (n = 26, 24%).
The majority of the included studies was conducted in Chinese public hospitals (n = 71, 65%). From the studies specifying the country from which the innovation originated (n = 41, 37%), most came from Australia (n = 16,15%) and the United States (n = 16, 15%), followed by Japan (n = 5, 5%). Most studies were conducted in the southeast of China (economically developed regions), e.g., in Shanghai (n = 29, 26%), Guangdong (n = 16, 15%), and Zhejiang (n = 13, 12%).
Turning from descriptives to the results, let it first be mentioned that the inductive analysis of the 110 included studies resulted in 33 factors and seven categories. Table 1 presents the factors per category, with a description of each factor. Below, we report on the findings of the most frequently mentioned factors per category and provide more details on findings which are specific for China. Table 2 summarizes the main findings with supporting evidence.
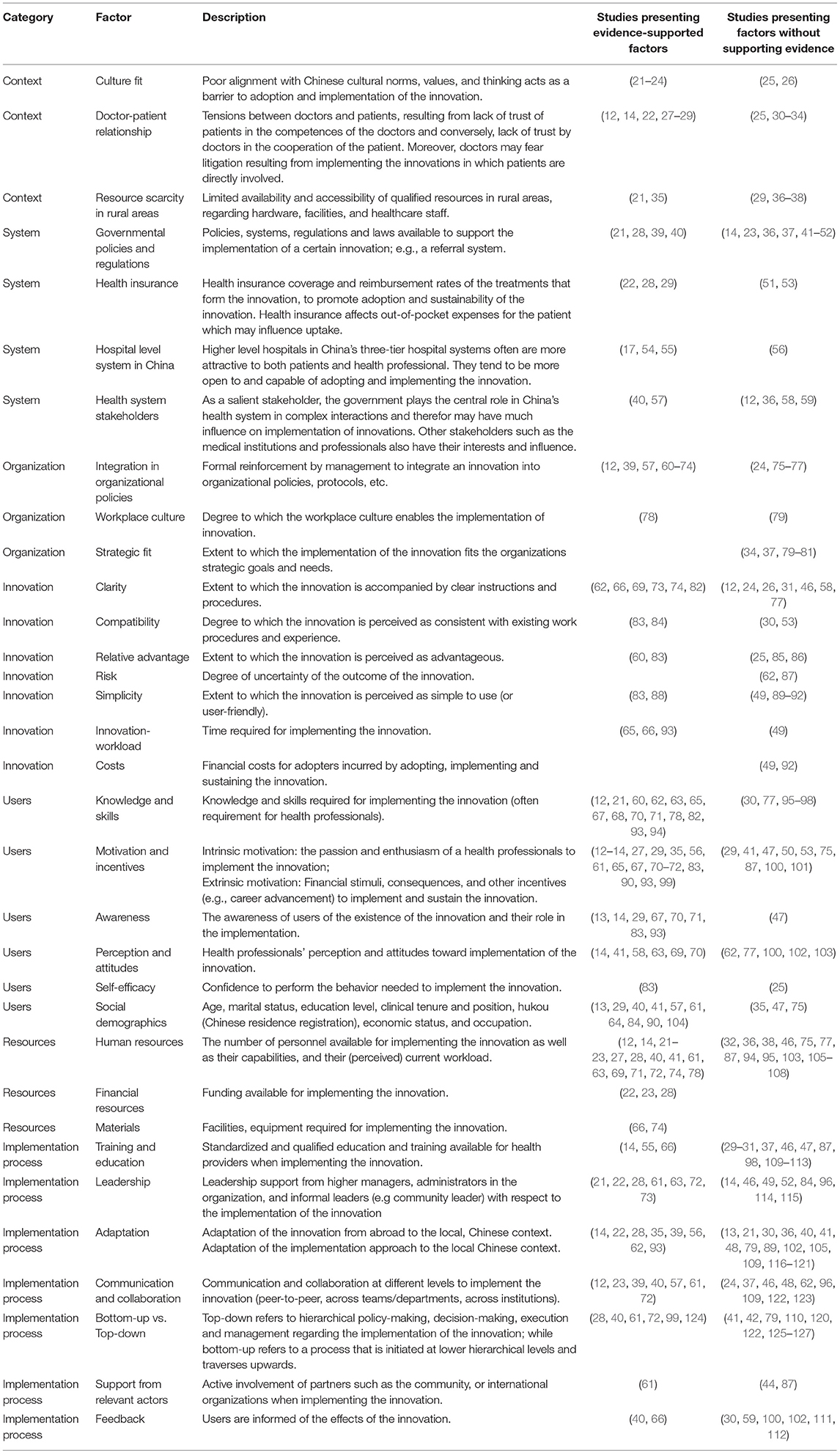
Table 1. The list of factors and descriptions.
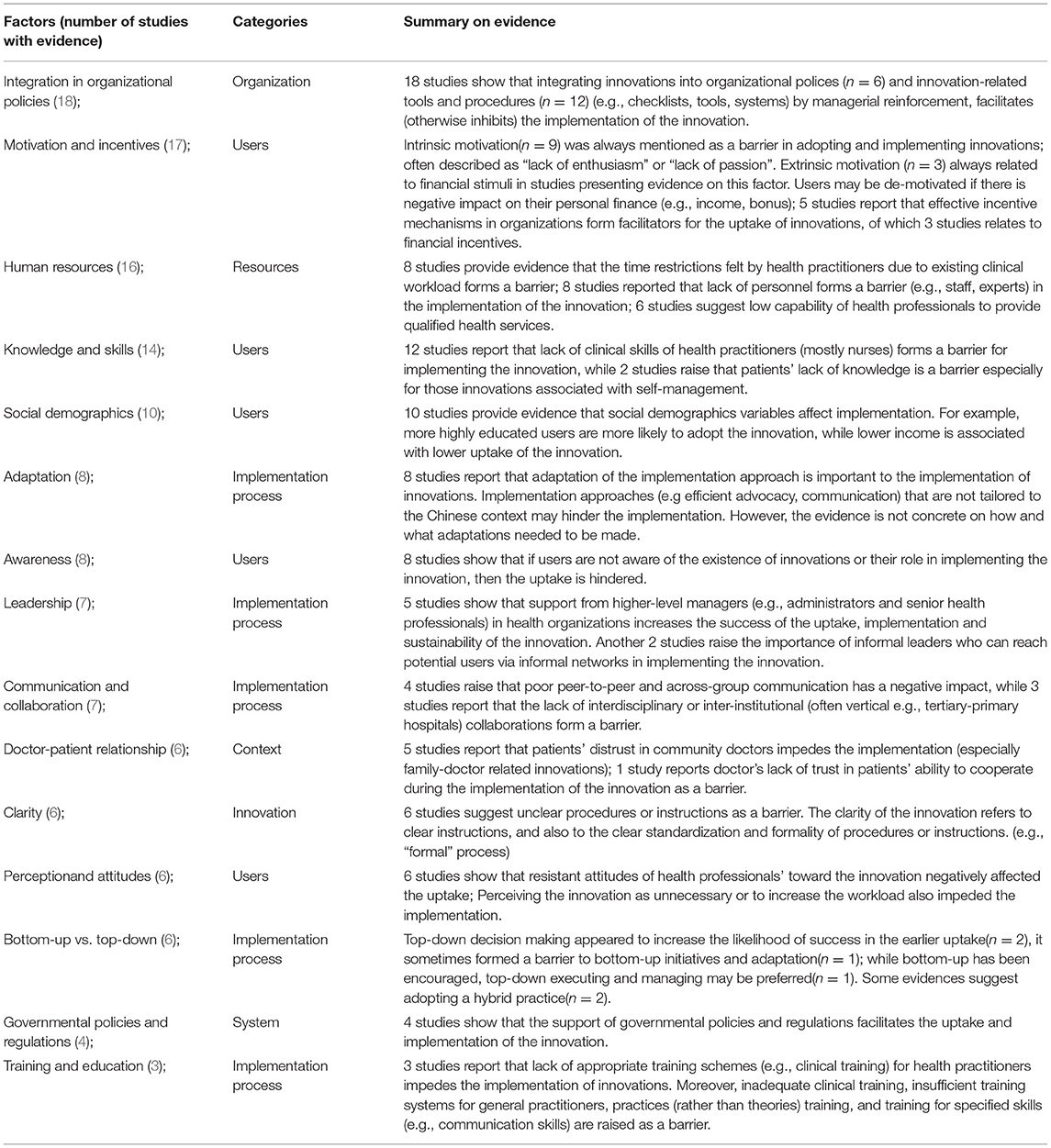
Table 2. Summary of main findings with supporting evidence.
This category contains the broad variety of social, cultural, economic, and other contextual factors. Twenty-one studies (19%) reported factors in the context category, identifying the factors cultural fit (n = 6, 5%), doctor-patient relationship (n = 12, 11%), and resource scarcity in rural areas (n = 6, 5%).
First, with respect to the factor of cultural fit, two studies (2%) focused on birth-related innovations in which psychological discomfort experienced by pregnant women concerning institution-based child delivery with the help of midwives found it to be barrier to the implementation of birth-related innovations. The psychological discomfort resulted from the mismatch with Chinese values, related to “accepting suffering” (25) and the tradition of “giving birth at home” in some rural areas (21). In addition, two studies mentioned that Chinese people, especially the elderly, rely on their family to decide about to adopting innovative approaches (22, 26).
Second, the distrust of patients in the skills of doctors and the service quality formed a barrier, especially for family- and community-based innovations (12, 14, 25, 27–33). For instance, in a survey to investigate the factors affecting mutual referral behavior, 69.9% of respondents mentioned the low quality of health service provided by doctors in community health service centers (12). Interestingly, the low trust of health professionals' in the ability of patients to cooperate during and after the innovation implementation also formed a barrier.
A third factor worth highlighting is the resource scarcity in China's rural areas. Compared to urban contexts, rural settings have less high-quality health resources such as facilities, equipment, and staff (21, 29, 35–38). One example was the shortage of skilled birth attendants in rural areas of the Guangxi Zhuang Autonomous Region. This shortage prevented the successful integration of traditional birth attendants into the health system in rural regions, when aiming to provide universal access to skilled birth attendance (35).
This category includes factors related to China' s health system. Combinedly, the 31 corresponding studies (28%) reported the factors governmental policies and regulations (n = 20, 18%), health insurance (n = 5, 5%), hospital level system (n = 4, 4%), and health system stakeholders (n = 6, 6%).
First, “policy push” (governmental policy initiatives to promote the innovation implementation) was reported as a supportive factor, especially for innovation involving institutions at multiple levels (37). The support can be achieved by instating specific new policies and regulations (23, 37, 41–44) or by building upon the existing ones (28, 39, 45–47).
China has a 3-tier hospital system, in which hospital levels are set based on their ability to provide medical care, medical education, and to conduct medical research. Higher-level hospitals are more likely to adopt innovations than their lower-level counterparts. For example, regarding implementation of the balanced score card; the differences in the adoption rates between all levels were (very) significant (54).
This category includes factors at an organizational level, such as organizational characteristics, cultures, and structures. The corresponding 28 studies (26%) mentioned the factors integration in organizational policies (n = 22, 20%), workplace culture (n = 2, 2%), and strategic fit (n = 5, 5%).
First, 22 studies (20%) reported that implementation was inhibited by the absence of formal reinforcement by management to integrate the innovation with organizational policy/protocols (57, 60–64), or with other innovation-related elements (15, 24, 39, 65–73, 75–77). Those elements include tools (e.g., communication tools to guide nursing handover) (65), checklists (e.g., Chinese HF discharge checklist) (65), indicators (e.g., referral indicators) (12), systems (e.g., information management system) (72), and forms (e.g., ETT: endotracheal tube assessment form) (66).
This category includes the characteristics of the innovation itself. 31 studies (28%) reported on the factors clarity (n = 13, 12%), compatibility (n = 4, 4%), relative advantage (n = 5, 5%), risk (n = 2, 2%), simplicity (n = 7, 6%), innovation-workload (n = 4, 4%), costs (n = 2, 2%).
In 13 studies (12%), unclear procedures or instructions related to the innovation were a barrier for implementing the innovation. This was not only related to the clarity of the content of these procedures (e.g., clear workflow on handover procedures) but also to the extent in which procedures were formalized and standardized.
This category includes factors related to the users (health providers and patients) that impact implementation of the innovation. 50 studies (46%) reported on the following factors in this category: knowledge and skills (n = 20, 18%), motivation & incentives (n = 20, 18%), awareness (n = 9, 8%), perception and attitudes (n = 11, 10%), self-efficacy (n = 2, 2%), and social demographics (n = 13, 12%).
Insufficient knowledge and skills regarding the innovation of health professionals (12, 60, 62, 63, 65, 67, 68, 70, 71, 78, 82, 93, 95–98) and patients (21, 30, 60, 77, 94) was raised as an inhibitor of implementing the innovation. For example, in one study (60) nurses' lack of knowledge and skills of stoma management was identified by the project team as one of the barriers. A bundle of interventions, including training, significantly improved compliance rates. Lack of patient knowledge and skills was especially reported for implementation of self-management approaches (21, 30, 77, 94).
Second, the factor motivation & incentives was mentioned in multiple studies both in terms of intrinsic (n = 15, 14%) and of extrinsic (n = 5, 5%) motivation. The former one relates to an individual's passion and enthusiasm to implement the innovation. For example, nurses' lack of enthusiasm to implement discharge education formed a barrier when implementing discharge planning for acute coronary syndrome patients (67). Extrinsic motivation mostly related to financial incentives in the included studies. For instance, frontline doctors were reluctant to adopt clinical pathways when their bonus incomes which are based on drugs and services prescribed were affected (99). Likewise, nurses would choose comprehensive hospitals (59.7%) and tertiary hospitals (51.9%) for dual practice (multiple job-holding) over working solely for primary health care centers (41) because of financial advantages. In addition, six studies (6%) reported that incentive mechanisms in organizations formed facilitators for the uptake of innovations, among which half could be characterized as financial incentives (27, 56, 72). For instance, 88 of 89 hospitals used the balanced score card for improving financial results by linking performance to the assignment of bonuses (56).
Finally, awareness of the innovation and of one's role in implementing the innovation was identified as a factor in nine studies (8%) (13, 14, 29, 47, 67, 70, 71, 83, 93). For example, awareness of the family doctor policy had significant effect on residents' decision to sign family doctor contracting services (29). Conversely, unawareness of caregivers regarding their role in helping patients adhere to fluid-intake restrictions was identified as a barrier to implementation (93).
This category includes various resources required to implement innovations. The 31 studies (28%) in this category reported the factors human resources (n = 30, 27%), financial resources (n = 3,3%), and materials (n = 2, 2%). Human resources were raised as a barrier in case of lack of personnel (n = 18, 16%), insufficient capability of health workers (n = 10, 9%), or heavy existing workload (n = 8, 7%).
First, the lack of personnel (e.g., health workers, experts, coordinators) was raised as a barrier in 18 studies (12, 14, 23, 27, 32, 36, 40, 46, 61, 72, 74, 87, 94, 95, 105–108). Second, existing workload was raised as a barrier for implementing innovations in 8 studies (7%) when the existing workload was perceived to leave no time for implementation of innovations (21, 41, 61, 63, 69, 71, 74, 78). A related barrier is when health professionals perceive that the innovation would result in an increase of workload (14, 41, 58, 62, 63, 69, 70, 77, 100, 102, 103). Finally, the lack of organizational capability; represented by the number of skilled health professionals (often skilled nurses) within health facilities and abilities of qualified health service provision (e.g., emergency departments' capacity to implement thrombolysis) formed a barrier for implementing the innovation in ten studies (9%) (12, 22, 23, 27, 28, 38, 61, 75, 77, 128).
This category includes factors that influence the process of turning implementation plans into actions and to succeed with the intended innovation. Factors in this category were reported in 70 studies (64%), including training & education (n = 16,15%), leadership supports (n = 20,18%), adaptation (n = 27, 25%), communication & collaboration (n = 16, 15%), bottom-up vs. top-down (n = 15, 14%), support from relevant actors (n = 3, 3%), and feedback (n = 8, 7%).
First, many of these studies identified adaptation as an important factor to facilitate implementation; both the adaptation of the innovation (n = 10, 9%) (41, 48, 79, 89, 102, 105, 109, 116–118) and that of the implementation approach. (n = 17, 15.5%) (13, 14, 21, 22, 28, 30, 35, 36, 39, 40, 56, 62, 79, 93, 119–121). Four studies (4%) (102, 105, 109, 117), for example focussed on Chinese adaptations of integrated care approaches (e.g., clinical pathways). Clinicians were often responsible for adapting innovations, as was the case when a working group comprising 22 cardiologists representing both level 2 and level 3 hospitals provided expert advice on how to tailor interventions to local circumstances (105). Many studies (16%) reported on the need to adapt the implementation process without further elaboration.
Second, 7 studies reported top-down policy-making and decision-making in China (n = 7, 6%) (40–42, 61, 99, 120, 125). While top-down decision making appeared to increase the likelihood of success in the earlier uptake, it sometimes formed a barrier to bottom-up initiatives and adaptation (40, 99, 120, 125). For example, in one study top-down policy goals were not seen as relevant and attainable due to the specific local context (40). Five studies (5%) mentioned bottom-up execution and management to be facilitating (79, 110, 122, 126, 127). While one study (72) reported a top-down approach as a facilitator. Finally, two studies (2%) (26, 124) pointed out that the best practice would utilize both top-down and bottom-up approaches.
Third, leadership was mentioned in 15 studies (14%) as an important facilitator, including high-level administrator support in hospitals (14, 22, 28, 46, 49, 61, 63, 72, 84, 111, 114, 115) and informal leader support (e.g., by community leaders) (21, 73, 96). For instance, many participants perceived making changes to hospital systems or processes based on data audit and feedback as too difficult in the absence of high-level administrative support (22).
Fourth, lack of training & education, especially lack of practical training for health professionals was identified as an inhibitor in 16 studies (15%) (14, 29–31, 37, 46, 47, 66, 87, 98, 104, 109–113). The studies which regarded training programs included both clinical and non-clinical training, such as communication skills training for health care practitioners (30).
Finally, poor peer-to-peer and across-group communication was a barrier (12, 24, 40, 61, 72, 96, 109) while multidisciplinary cooperation and inter-institutional collaborations were of great importance in implementing innovations (e.g., the referral system) (23, 37, 39, 46, 48, 57, 62, 122, 123). For example, close collaboration with other institutions benefited quality and safety improvement projects (46).
This review identified 33 factors in 7 categories that may influence implementation of foreign innovations in management and organization of health service delivery in China. Most supported by evidence were the factors human resources and users' knowledge & skills, hindering implementation because of shortages. Of the 33 factors identified, 28 also appear in the systematic review of Greenhalgh, which is mostly based on western literature (5). Compared to previous reviews which mostly rely on Western evidence (5, 11), new factors or new perspectives relate to motivation & incentives, governmental policies and regulations, integration into organizational policies, clarity of innovations and bottom-up & top-down management approaches.
It is worth noting that out of the 110 studies included only 43 present results with evidence on factors. Moreover, 29 of these 43 studies were not specifically designed to identify factors, but for example focused on the outcomes achieved. Nevertheless, many factors were mentioned in multiple studies, suggesting they are relevant. For example, governmental policies & regulations to support implementation were mentioned in 20 studies, four of which provided evidence. Likewise, the need to adapt the innovation and the implementation methods to the (Chinese) context was mentioned in many articles, mostly without supporting evidence or specifics.
Western evidence suggests that both intrinsic and extrinsic motivation can stimulate potential users of an innovation (5). It is important for the innovation to meet an identified need of the user (129) and costs and benefits of the innovation should be balanced (5). For instance, several theoretical frameworks indicate that user's may be willing to put in extra time and effort by utilizing an innovation, if it improves the quality of their work (130). However, our review only provided evidence for intrinsic motivation as a barrier (e.g., lack of enthusiasm) for implementation. Extrinsic motivation, especially based on financial incentives, was identified as both a barrier and facilitator; potential financial gains or losses were likely to motivate or de-motivate users. This confirms other Chinese studies that show how intrinsic rewards, compared to extrinsic and social rewards, have limited influence in public sectors in China compared to the West (131). Research also found that career development and financial benefits rank first and second in motivating health workers in China (132). This may be explained by the relatively low incomes and high work-pressure experienced by Chinese health workers (132, 133).
Western evidence furthermore shows that making adoption mandatory may promote the initial adoption of an innovation, yet may decrease the effectiveness and sustainability (5). In contrast, our review provides evidence that formalization (relating s to integration into organizational policies & clarity of innovations in our review) promotes not only the initial adoption, but also the effectiveness and sustainability of innovations. Likewise, both Greenhalgh and Chaudoir (5, 11) state that centralization (relating to top-down and governmental policies and regulations in this review) has a negative effect on innovativeness of organizations, while decentralization to front-line personal (relating to bottom-up approaches) positively affects the implementation of innovations. The evidence we found on decentralization is inconclusive. Some studies suggest that a combination or so called “hybrid” top-down/bottom-up' approach in which leaders initiate top-down procedures that enable and mandate bottom-up initiatives for adaptations are more effective in the Chinese context (10). These differences probably relate to power distance (the extent to which less powerful members of organizations and institutions accept and expect that power is distributed unequally) (134). With a power distance index of 80, China scores higher than most Western countries. Chinese are more likely to be influenced by formal authority and sanctions and are in general optimistic about people's capacity for leadership and initiative) (134). This may explain why formalization and organizational leadership (relating to top-down leadership) have been attached great importance in the uptake and implementation of innovations in China. Thus, although decentralization has increasingly been encouraged, both governmental guidance and hierarchical superior-subordinate relationship are the norm in China (40–42, 61, 99, 120, 125). The centralized leadership, power and responsibilities defined by authoritative regulations and rules appear to provide users with a sense of certainty and safety, thus facilitating the adoption, implementation and sustainability of innovations.
In addition to cultural differences, the review also revealed other novel, perhaps relatively Chinese contextual characteristics that influence the implementation of innovations. First, availability of skilled personal appears as a major challenge for innovation in China's healthcare system (135). Professionals either lack relevant skills, there is no appropriate training available, or there is a lack of personnel and therefore time. Most included studies are about innovations in tertiary hospitals which have more highly skilled staff. If human resource capacity is mentioned as a barrier in tertiary hospitals, it likely applies even more to primary care, for which the evidence however remains very scarce.
A second specifically Chinese contextual finding relates to the challenges encountered in rural areas. The few studies on innovation in rural China mention challenges faced in relation to the resource disparity compared to urban areas. With China's urbanization, about half a billion people moved from rural areas to urban areas over the past three decades (136). Corresponding reallocations of labor across space and sectors in some parts of China contributed to rapid economic growth but increased disparities between rural and urban areas (136). As many skilled health professionals have been attracted to big cities, availability of qualified health services in rural areas tends to be restricted (135). In addition, cultural norms in rural China are more traditional, which may form a general barrier for innovation (10). Such rural challenges underlie several of our findings, e.g., regarding innovations in maternal and child health services (21, 25).
As there is no universally adopted terminology or strong indexation in both Chinese and English databases for the concept of innovations in organization and management of health service delivery, it is possible that some published studies meeting the inclusion criteria were not identified through the search. In addition, although we designed the search in a librarian-mediated and a process-equivalent manner, some linguistic differences between Chinese and English may not have been addressed. We found that concepts (notably innovation itself) have no direct translation from English to Chinese. We therefore used an adapted combination of search terms in Chinese databases. Also, Chinese databases use different algorithms compared to English databases to facilitate searches, for example they often do not use mesh terms. The assistance of librarians helped us to navigate both Chinese and English database to try and find similar types of publications, but differences may have remained.
Our synthesis of the evidence is limited by the lack of studies with robust evidence and the large heterogeneity in methods used, innovations studied, and aims. Few studies explicitly focused on identifying factors that influence implementation of innovations in China. Furthermore, most studies were done in more affluent parts of China and primarily in tertiary hospitals with better skilled staff. As our analysis has not compared innovations from abroad with domestic innovations, caution is called for when attributing the results to the non-domestic origin of the innovations considered.
There is a general lack of studies on implementation processes of innovations in the Chinese health system. Most studies are quantitative in nature and report primarily on the relationship between an innovation and clinical outcomes, while the implementation process remains a black box. A better understanding of these processes not only requires studies with more robust designs, but also qualitative studies to identify why and how factors frequently mentioned in included studies affect the uptake and implementation of innovations. Furthermore, these studies should also include rural areas in China and primary care facilities.
By studying which factors influence the implementation of innovations from abroad in China we tried to better understand contextual influences. Many of the identified factors also surfaced in previously conducted reviews which are strongly biased toward affluent Western countries with individualistic working cultures and relatively low power distance. This review provides first evidence that such contextual differences between countries may have more influence on implementation of innovation processes than has been recognized. Previous reviews have largely disregarded such cultural and country-related differences.
Our review presents new factors and provides new perspectives on previously identified factors. This evidence base can serve to advance further research and better inform policy and practice to implement international best practices to achieve China's health reform objectives. First, it is of practical importance to bear previously identified factors in mind while implementing foreign innovations in organization and management of health service delivery, and additionally consider the factors especially important in China such as extrinsic motivation, financial incentives, governmental and organizational policies & regulations. Moreover, it is important to recognize that, somewhat in contrast with existing evidence from Western contexts, centralization and top down mechanisms promote implementation in the Chinese context with high power distance. Lastly, it is important to recognize that China is not a small monocultural context. Within the large country of China, considerable differences exist, for instance between rural and urban China. The local characteristics must be addressed when implementing innovations.
This review shows that China has specific cultural and contextual characteristics that need to be taken into account when implementing innovations in management and organization of health service delivery from abroad. Compared to many of the countries in which these innovations originate, China has a high-power distance. Formalization and organizational leadership are therefore more important for successful implementation. Furthermore, financial incentives are prime motivators in China. Also, China has major shortages in skilled health personal, on top of large disparities in development and capacity between primary and secondary care and between affluent and less affluent regions. Implementation of innovations is therefore much more challenging in primary care and developing areas in China. Although many factors identified in this review are not specific for innovations in China, our findings suggest that cultural and contextual differences have more impact than is currently recognized in literature.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
SY provided support in finalizing the Chinese search query. WW and JW screened the English titles and abstracts. WW and HW screened the Chinese titles and abstracts. WW, JW, and JK reviewed the English full texts. WW, HW, and SY reviewed the Chinese full texts. WW, JW, MB-S, and JK analyzed the data and categorized the results together. WW initiated the draft of the manuscript. All authors read and approved the final manuscript.
This work was supported by China Scholarship Council (CSC201908500106). This funder has no role in the study design, data collection and analysis, interpretation of data and writing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank Wichor Bramer (a Librarian at the Erasmus Medical Center, Rotterdam, The Netherlands) and Tingchao Xiao (a Librarian at Chongqing Medical University, Chongqing, China), for their vital contributions in executing search strategies.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2021.766677/full#supplementary-material
1. World Health Organization. Healthy China 2030 (from vision to action). (2016). Available online at: https://www.who.int/healthpromotion/conferences/9gchp/healthy-china/en/. (accessed January 22, 2021).
2. Meng Q, Mills A, Wang L, Han Q. What can we learn from China's health system reform? BMJ. (2019) 365:12349. doi: 10.1136/bmj.l2349
3. World Bank. Reform and Innovation for Better Rural Health Services in China (2015). Available online at: https://www.worldbank.org/en/results/2015/04/02/reform-innovation-for-better-rural-health-services-in-china. (accessed February 22, 2021).
4. World Bank. Will China become a global innovation champion? Keeping the global innovation system open will be key (2020). Available online at: https://blogs.worldbank.org/eastasiapacific/will-china-become-global-innovation-champion-keeping-global-innovation-system-open. (accessed February 22, 2021).
5. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. (2004) 82:581–629. doi: 10.1111/j.0887-378X.2004.00325.x
6. Eggleston K. (2012). Health Care for 1.3 Billion: An Overview of China's Health System. Stanford Asia Health Policy Program Working Paper No. 28, Available at SSRN: Available online at: https://ssrn.com/abstract=2029952 or http://dx.doi.org/10.2139/ssrn. (accessed January 9, 2012)
7. OECD. Organisation of health care delivery (2012). Available online at: https://www.oecd.org/els/health-systems/organisation-health-care-delivery.htm. (accessed February 22, 2021).
8. Hofstede G. Dimensionalizing cultures: the Hofstede model in context. Online Read Psychol Cult. (2011) 2:2307–0919. doi: 10.9707/2307-0919.1014
9. Meyer JU. Strengthening innovation capacity through different types of innovation cultures. In: This paper was presented at the. (2014). doi: 10.2139/ssrn.2506307
10. Klundert JVD, de Korne D, Yuan S, Wang F, Van Wijngaarden J. ‘Hybrid'top down bottom up health system innovation in rural China: a qualitative analysis. PLoS ONE. (2020) 15:e0239307. doi: 10.1371/journal.pone.0239307
11. Chaudoir SR, Dugan AG, Barr CH. Measuring factors affecting implementation of health innovations: a systematic review of structural, organizational, provider, patient, and innovation level measures. Implement Sci. (2013) 8:1–20. doi: 10.1186/1748-5908-8-22
12. Du J, Lu X, Wang Y, Cui S, Guo A, Coid D. Mutual referral: a survey of GPS in Beijing. Fam Pract. (2012) 29:441–7. doi: 10.1093/fampra/cmr122
13. Huang J, Liu S, He R, Fang S, Lu W, Wu J. Factors associated with residents' contract behavior with family doctors in community health service centers: a longitudinal survey from China. PLoS ONE. (2018) 13:11. doi: 10.1371/journal.pone.0208200
14. Penm J, Moles R, Wang H, Li Y, Chaar B. Factors affecting the implementation of clinical pharmacy services in China. Qual Health Res. (2014) 24:345–56. doi: 10.1177/1049732314523680
15. Chen Z. Launch of the health-care reform plan in China. Lancet. (2009) 373:1322–4. doi: 10.1016/S0140-6736(09)60753-4
16. Thomas DR. A general for analyzing qualitative evaluation data. Am J Eval. (2006) 27:237–46. doi: 10.1177/1098214005283748
17. CRD. Centre for reviews, dissemination (CRD). Systematic reviews: CRD's guidance for undertaking reviews in health care: Centre for Reviews and Dissemination. (2009)
18. Liu Y, Kong Q, Yuan S, van de Klundert J. Factors influencing choice of health system access level in China: a systematic review. PLoS ONE. (2018) 13:e0201887. doi: 10.1371/journal.pone.0201887
19. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. (2005) 52:546–53. doi: 10.1111/j.1365-2648.2005.03621.x
20. CEBM (2021) (2021) “The Oxford 2011 Levels of Evidence.” Oxford Centre for Evidence-Based Medicine. Available online at: http://www.cebmnet/indexaspx?o=56532011. (accessed Feb 22, 2021).
21. Ma W, Liu B, Nan L, Portela A, Yin B, Wei C. Clan-involved approaches to increasing antenatal care use in a rural minority area of China: implementation research. Acta Paediatr. (2018) 107:7–16. doi: 10.1111/apa.14357
22. Ranasinghe I, Rong Y, Du X, Wang Y, Gao R, Patel A. System barriers to the evidence-based care of acute coronary syndrome patients in China: qualitative analysis. Circ Cardiovasc Qual Outc. (2014) 7:209–16. doi: 10.1161/CIRCOUTCOMES.113.000527
23. Ma F, Lv F, Xu P, Zhang D, Meng S, Ju L. Task shifting of HIV/AIDS case management to Community Health Service Centers in urban China: a qualitative policy analysis. BMC Health Serv Res. (2015) 15:253. doi: 10.1186/s12913-015-0924-y
24. Cao Y, Jiang S, Zhou Q. Introducing evidence-based practice improvement in Chinese neonatal intensive care units. Transl Pediatr. (2019) 8:257–61. doi: 10.21037/tp.2019.07.07
25. Cheung N, Mander R, Wang X, Fu W, Zhou H, Zhang L. Clinical outcomes of the first midwife-led normal birth unit in China: a retrospective cohort study. Midwifery. (2010) 27:582–7. doi: 10.1016/j.midw.2010.05.012
26. Wen W, Zhang C, Huang Q, Yang P, Zhang Y, Xing P. Effects of quality supervision and continuous improvement on early management efficiency in patients with acute ischemic stroke. Chin J Cerebrovasc Dis. (2017) 14:169–74. doi: 10.3969/j.issn.1672-5921.2017.04.001
27. Xu J, Mills A. Challenges for gatekeeping: a qualitative systems analysis of a pilot in rural China. Intern J Equity Health. (2017) 16:106. doi: 10.1186/s12939-017-0593-z
28. Yuan S, Wang F, Li X, Jia M, Tian M. Facilitators and barriers to implement the family doctor contracting services in China: findings from a qualitative study. BMJ Open. (2019) 9:10. doi: 10.1136/bmjopen-2019-032444
29. Zhang X, Yang S, Wang Y. Factors influencing residents' decision to sign with family doctors under the new health care reform in China. Int J Health Plann Manage. (2019) 34:4.e1800–e09. doi: 10.1002/hpm.2896
30. Browning C, Yang H, Zhang T, Chapman A, Liu S, Enticott J. Implementing a chronic disease self-management program into china: the happy life club TM. Front Public Health. (2014) 2:181. doi: 10.3389/fpubh.2014.00181
31. Zhang J, Fu W, Qian L, Lu M, Zhang M. Evaluation of the effect of a clinical pathway on the quality of simulated pre-hospital cardiopulmonary resuscitation: primary experience from a Chinese pre-hospital care centre. Hong Kong J Emerg Med. (2015) 22:14–22. doi: 10.1177/102490791502200102
32. Long H. The practice and reflection on the implementation famil doctor system in Shanghai. Zhongguo Wei Sheng Zi Yuan. (2014) 17:225–26.
33. Li L. Improved implmenation of family doctor system in managing diabetes patients in communities. Zhong Yi Yao Guan Li Za Zhi. (2015) 19:144. doi: 10.16690/j.cnki.1007-9203.2015.19.144
34. Wu Y, Li S, Patel A, Li X, Du X, Wu T, et al. Effect of a quality of care improvement initiative in patients with acute coronary syndrome in resource-constrained hospitals in China: a randomized clinical trial. JAMA Cardiol. (2019) 4:418–27. doi: 10.1001/jamacardio.2019.0897
35. Jiang H, Qian X, Chen L, Li J, Escobar E, Story M, et al. Towards universal access to skilled birth attendance: The process of transforming the role of traditional birth attendants in Rural China. BMC Preg Childbirth. (2016) 16:1. doi: 10.1186/s12884-016-0854-7
36. Lei J, Wen D, Zhang X, Li J, Lan H, Meng Q, et al. Enabling health reform through regional health information exchange: a model study from China. J Healthc Eng. (2017) 1–9. doi: 10.1155/2017/1053403
37. Li L, Zhong C, Mei J, Liang Y, Li L, Luang L. Effect of family practice contract services on the quality of primary care in Guangzhou, China: a cross-sectional study using PCAT-AE. BMJ Open. (2018) 8:11. doi: 10.1136/bmjopen-2017-021317
38. Jin X, Zhang G, Xu G. Exploration and practice of responsibility holistic nursing based on individual case management model. Hu Li Xue Za Zhi. (2014) 29:24. doi: 10.3870/hlxz.2014.24.070
39. Yuan S, Wang F, Li C. The chronic disease management in community health service institutions based on Innovative Care for the Chronic Conditions Framework. Zhongguo Wei Sheng Zheng Cei Yan Jiu. (2015) 8:39–45. doi: 10.3969/j.issn.1674-2982.2015.06.007
40. Furtado K, Budd E, Ying X, deRuyter A, Armstrong R, Pettman T, et al. Exploring political influences on evidence-based non-communicable disease prevention across four countries. Health Educ Res. (2018) 33:89–103. doi: 10.1093/her/cyy005
41. Bai X, Wang A, Plummer V, Lam L, Cross W, Guan Z. Using the theory of planned behaviour to predict nurse's intention to undertake dual practice in China: a multicentre survey. J Clin Nurs. (2019) 28:2101–10. doi: 10.1111/jocn.14791
42. Chen J, Fang X, Fang Q, Fang Q, Cai H, Su Q, et al. The clinical application of remote critical care network. Chin Crit Care Med. (2009) 21:679–81. doi: 10.3760/cma.j.issn.1003-0603.2009.11.013
43. Fu W, Bao J, Meng J. Development of community nursing in Zhejiang Province, China: a report of the driving measures. Int Nurs Rev. (2010) 57:265–8. doi: 10.1111/j.1466-7657.2009.00787.x
44. Zhang Y, Liu S, Sheng X, Lou J, Fu H, Sun X. Evaluation of a community-based hypertension self-management model with general practitioners. Int J Health Plann Manage. (2019) 34:960–74. doi: 10.1002/hpm.2867
45. Chen L. The risk management of medical device-related pressure ulcers based on the Australian/New Zealand standard. J Int Med Res. (2018) 46:4129–39. doi: 10.1177/0300060518786902
46. Xu W, Huang Y, Bai J, Varughese A. A quality improvement project to reduce postoperative adverse respiratory events and increase safety in the postanesthesia care unit of a pediatric institution. Paediatr Anaesth. (2019) 29:200–10. doi: 10.1111/pan.13534
47. Lin K, Yang X, Wu Y, Chen S, Yin G, Zhan J. Impact of disease-management programs on metabolic control in patients with type 1 diabetes mellitus: a cohort study in Shantou, China. Medicine. (2016) 95:52.e5681. doi: 10.1097/MD.0000000000005681
48. Zhong X, Potemans B, Zhang L, Oldenburg B. Getting a Grip on NCDs in China: an Evaluation of the Implementation of the Dutch-China Cardiovascular Prevention Program. Int J Behav Med. (2015) 22:393–403. doi: 10.1007/s12529-014-9453-z
49. Huang Y, Lei Y, Wang Q, Li D, Ma L, Guo L, et al. Telepathology consultation for frozen section diagnosis in China. Diagn Pathol. (2018) 13:29. doi: 10.1186/s13000-018-0705-0
50. Huang J, Lu W, Wang L, Zhang T, Liu C, Liu S. A preliminary effect analysis of family doctor and medical insurance payment coordination reform in Changning District of Shanghai, China. BMC Fam Pract. (2019) 20:60. doi: 10.1186/s12875-019-0949-0
51. Shi L, Lee D, Liang H, Zhang L, Makinen M, Blanchet N. Community health centers and primary care access and quality for chronically-ill patients - a case-comparison study of urban Guangdong Province, China. Intern J Equity Health. (2015) 14:90. doi: 10.1186/s12939-015-0222-7
52. Peiris D, Sun L, Patel A, Tian M, Essue B, Jan S, et al. Systematic medical assessment, referral and treatment for diabetes care in China using lay family health promoters: protocol for the SMARTDiabetes cluster randomised controlled trial. Implement. Sci. 11:116 doi: 10.1186/s13012-016-0481-8
53. Liang C, Mei J, Liang Y, Hu R, Li L, Kuang L. The effects of gatekeeping on the quality of primary care in Guangdong Province, China: a cross-sectional study using primary care assessment tool-adult edition. BMC Fam Pract. (2019) 20:93. doi: 10.1186/s12875-019-0982-z
54. Zhijun LI, Zengbiao YU, Zhang L. outcomes of balanced scorecard application in hospital administration in China. China Econ Rev. (2014) 30:1–15. doi: 10.1016/j.chieco.2014.05.003
55. Su M, Zhou Y, Yu J. The level of evidence-based pain management practices among head nurses. Hu Li Xue Za Zhi. (2018) 33:62–5. doi: 10.3870/j.issn.1001-4152.2018.05.062
56. Gao T, Gurd B. Meeting the challenge in performance management: the diffusion and implementation of the balanced scorecard in Chinese hospitals. Health Policy Plan. (2015) 30:234–41. doi: 10.1093/heapol/czu008
57. Su D, Hu B, Rosenthal VD, Li R, Hao C, Pan W, et al. Impact of the International Nosocomial Infection Control Consortium (INICC) Multidimensional Hand Hygiene Approach in five intensive care units in three cities of China. Public Health. (2015) 129:979–88. doi: 10.1016/j.puhe.2015.02.023
58. Lei J, Sockolow P, Guan P, Meng Q, Zhang J. A comparison of electronic health records at two major Peking University Hospitals in China to United States meaningful use objectives. BMC Med Inf Decis Mak. (2013) 13:96. doi: 10.1186/1472-6947-13-96
59. Du Z, Liao Y, Chen C, Hao Y, Hu R. Usual source of care and the quality of primary care: a survey of patients in Guangdong province, China. Intern J Equity Health. (2015) 14:60. doi: 10.1186/s12939-015-0189-4
60. Cao X, Bo L, Zeng M. Management of stoma among colorectal cancer patients in a surgical ward: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2014) 12:533–47. doi: 10.11124/jbisrir-2014-1487
61. Budd E, de Ruyter A, Wang Z, Chan P, Ying X, Furtado K, et al. A qualitative exploration of contextual factors that influence dissemination and implementation of evidence-based chronic disease prevention across four countries. BMC Health Serv Res. (2018) 18:233. doi: 10.1186/s12913-018-3054-5
62. Wu P. Post-operative care of total laryngectomy patients in the ward: a best practice implementation project. JBI Libr Syst Rev. (2014) 12:413–23. doi: 10.11124/jbisrir-2014-1571
63. Wang N, Yang Z, Miao J, Mi X, Liu S, Stern C, et al. Clinical management of cancer-related fatigue in hospitalized adult patients: A best practice implementation project. JBI Database Syst Rev Implement Rep. (2018) 16:2038–49. doi: 10.11124/JBISRIR-2017-003769
64. Rosenthal VD, Pawar M, Leblebicioglu H, Navoa-Ng J, Villamil- Gómez W, Armas-Ruiz A, et al. Impact of the international Nosocomial infection control consortium (INICC) multidimensional hand hygiene approach over 13 years in 51 cities of 19 limited-resource countries from Latin America, Asia, the Middle East, and Europe. Infect Control Hosp Epidemiol. (2013) 34:415–23. doi: 10.1086/669860
65. Chen Y, Zhu L, Xu F, Chen J. Discharge planning for heart failure patients in a tertiary hospital in shanghai: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2016) 14:322–36. doi: 10.11124/jbisrir-2016-2510
66. Hu X, Zhang Y, Cao Y, Huang G, Hu Y, McArthur A. Prevention of neonatal unplanned extubations in the neonatal intensive care unit: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2017) 15:2789–98. doi: 10.11124/JBISRIR-2016-003249
67. Lu M, Tang J, Wu J, Yang J, Yu J. Discharge planning for acute coronary syndrome patients in a tertiary hospital: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2015) 13:318–34. doi: 10.11124/01938924-201513070-00019
68. Xiaoju Z, Xiaoju Z. The assessment and management of chemotherapy-induced peripheral neurotoxicity among adult patients receiving chemotherapy in a tertiary hospital: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2014) 12:484–500. doi: 10.11124/jbisrir-2014-1486
69. Yu Z, Zhang Y, Gu Y, Xu X, McArthur A. Pediatric clinical handover: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2017) 15:2585–96. doi: 10.11124/JBISRIR-2016-003296
70. Zhang Y, Huang L, Ding Y, Shi Y, Chen J, McArthur A. Management of perineal pain among postpartum women in an obstetric and gynecological hospital in China: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2017) 15:165–77. doi: 10.11124/JBISRIR-2016-003232
71. Zhu L, Xu J, Wang Q, Xu F, Chen J. Nursing care of transradial angiography and intervention in a tertiary hospital in shanghai: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2016) 14:286–94. doi: 10.11124/JBISRIR-2016-002509
72. Qian Y, Hou Z, Wang W, Zhang D, Yan F. Integrated care reform in urban China: a qualitative study on design, supporting environment and implementation. Intern J Equity Health. (2017) 16:185. doi: 10.1186/s12939-017-0686-8
73. Yang J, Zhang J. Improving the postoperative handover process in the intensive care unit of a tertiary teaching hospital. J Clin Nurs. (2016) 25:1062–72. doi: 10.1111/jocn.13115
74. Cai X, McArthur A. Discharge following sedation for endoscopic procedures: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2019) 18:348–56. doi: 10.11124/JBISRIR-D-19-00053
75. Gong Y, Peng P, Bao P, Zhong W, Shi Y, Gu K. The implementation and first-round results of a community-based colorectal cancer screening program in Shanghai, China. Oncologist. (2018) 23:928–35. doi: 10.1634/theoncologist.2017-0451
76. Hui L, Zhang Z, Wang Y, Che H. Comprehensive analysis on quality of clinical pathway for hospitalized patients with cataract. Intern Eye Sci. (2014) 14:1863–5. doi: 10.3980/j.issn.1672-5123.2014.10.35
77. Feng C. Modification of triage process for pediatric emergency. Hu Li Xue Za Zhi. (2013) 28:28–9. doi: 10.3870/hlxzz.2013.21.028
78. Wu Y, Stephenson LW, Cong M, Zhou WC. Pre-treatment assessment for patients with breast cancer undergoing chemotherapy: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2020) 18:212–23. doi: 10.11124/JBISRIR-D-19-00163
79. Dai Y. A Quasi-experimental Study of Improving Work Engagement of Nurses based on Applying the Magnet Hospital Model in Chinese Hospital. Invest Clin. (2018) 59:332–40.
80. Yi L, Hao A, Hu M, Huang P, Yuan H, Xing M. Construction and application of a refined hospital management chain. Cell Biochem Biophys. (2015) 72:19–22. doi: 10.1007/s12013-014-0395-5
81. Zhou C. Modified record sheet of transfer with the use of SBAR. Zhongguo Yi Yuan Tong Ji. (2017) 24:393–395. doi: 10.3969/j.issn.1006-5253.2017.05.026
82. Liu H, Shi Y, Hu R, Jiang H. Nursing management of post-stroke dysphagia in a tertiary hospital: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2016) 14:266–74. doi: 10.11124/JBISRIR-2016-002971
83. Zhang D. Empirical research on the influencing factors of the intention to use of mobile health management service:from the perspective of innovation diffusion. Qing Bao Za Zhi. (1965) 36:120–7.
84. Xu X, Ke D, Deng D, Houser S, Wang LX. An innovative medical consultation model in mainland China. Int. J. Health Care Qual. Assur. (2019) 32:1055–71. doi: 10.1108/IJHCQA-02-2017-0033
85. Fang J, Huang B, Xu D, Li J, Au WW. Innovative application of a home-based and remote sensing cardiac rehabilitation protocol in chinese patients after percutaneous coronary intervention. Telemed J E Health. (2019) 25:288–93. doi: 10.1089/tmj.2018.0064
86. Gu W, Wang Y, Feng Q, Bao X, Chen H. Practice and exploration of clinical virtual beds pre-hospitalization mode. J Shanghai Jiaotong Univ Med Sci. (2015) 35:1691–5. doi: 10.3969/j.issn.1674-8115.2015.11.019
87. Hu L, Flood P, Li Y, Tao W, Zhao P, Xia Y, et al. No pain labor and delivery: a global health initiative's impact on clinical outcomes in China. Anesth Analg. (2016) 122:1931–8. doi: 10.1213/ANE.0000000000001328
88. Li J, Zhang X, Chu J, Chu J, Suzuki M, Araki K. Design and development of EMR supporting medical process management. J Med Syst. (2012) 36:1193–203. doi: 10.1007/s10916-010-9581-1
89. Yang W, Wen X. Modified early warning score in pre-hospitalized emergency management. Dang Dai Hu Shi (Xia Xun Kan). (2016) 4:172–73.
90. Fang J, Li J, Li Z, Xu D, Chen C, Xie B, et al. Attitudes towards acceptance of an innovative home-based and remote sensing rehabilitation protocol among cardiovascular patients in Shantou, China. J Geriatr Cardiol. (2016) 13:326–32. doi: 10.11909/j.issn.1671-5411.2016.04.006
91. Guo Y, Sun H. Establishing quality control circle in innovative nursing quality management. Guo Ji Hu Li Xue Za Zhi. (2013) 009:2109–11. doi: 10.3760/cma.j.isn.1673–4351.2013.09.116
92. Zhu B, Jiang M, Wang Z. Modified early warning score in triage of cardiology clinic. Hu Li Jin Xiu Za Zhi. (2013) 28:22.
93. Jia S, Huang B, Chu Y, Lu Y. McArthur A. Management of non-adherence to fluid intake restrictions in hemodialysis patients in a tertiary hospital: a best practice implementation project. JBI Database Syst Rev Implement Rep. (2016) 14:309–22. doi: 10.11124/JBISRIR-2016-003046
94. Wang N, Zhang H, Zhou Y, Jiang H, Dai B, Sun M, et al. Using electronic medication monitoring to guide differential management of tuberculosis patients at the community level in China. BMC Infect Dis. (2019) 19:1. doi: 10.1186/s12879-019-4521-2
95. Zheng X, Zhong F, Zhang X. Doctors' compliance with national guidelines and clinical pathway on the treatment of tuberculosis inpatients in Hubei, China. J Eval Clin Pract. (2014) 20:288–93. doi: 10.1111/jep.12127
96. Liu D, Li X. The implementation of foreign nursing modes in Chinese communities. Qi Lu Hu Li Za Zhi. (2011) 17:21. doi: 10.3969/j.issn.1006-7256.2011.21.059
97. Wang P. The value of applying PDCA in quality managenment of operating rooms. Zhongguo Bao Jian Ying Yang. (2018) 28:183.
98. Zhu Y, Qian J. The application of modified SBAR communication mode in reversed nursing handover in the oncology clinic. Zhong Xi Yi Jie He Hu Li. (2018) 4:172.
99. He J, Yang W. Clinical pathways in China - an evaluation. Int J Health Care Qual Assur. (2015) 28:394–411. doi: 10.1108/IJHCQA-09-2014-0096
100. Cheng T. A pilot project using evidence-based clinical pathways and payment reform in China's rural hospitals shows early success. Health Aff. (2013) 32:963–73. doi: 10.1377/hlthaff.2012.0640
101. Yang F, He L. Application and promotion in nursing quality management quality control circle. Dang Dai Hu Shi (Xia Xun Kan). (2014) 12:181–2.
102. Bai J, Bai F, Zhu H, Xue D. The perceived and objectively measured effects of clinical pathways' implementation on medical care in China. PLoS ONE. (2018) 13:5. doi: 10.1371/journal.pone.0196776
103. Wang Y, Wang Y, Li Z, Zhao X, Wang C, Wang X, et al. Effect of a multifaceted quality improvement intervention on hospital personnel adherence to performance measures in patients with acute ischemic stroke in China: a randomized clinical trial. JAMA. (2018) 320:245–54. doi: 10.1001/jama.2018.8802
104. Luo Q, Wang P, Wang X. The implementation of innovative mode in managing outpatient clinic services. Jia Ting Yi Yao. (2017) 7:143.
105. Du X, Gao R, Turnbull F, Wu Y, Rong Y, Lo S. Hospital quality improvement initiative for patients with acute coronary syndromes in China a cluster randomized, controlled trial. Circ Cardiovasc Qual Outcome. (2014) 7:217–26. doi: 10.1161/CIRCOUTCOMES.113.000526
106. Zhou Q, Lee S, Jiang S, Chen C, Kamaluddeen M, Hu X. Efficacy of an infection control program in reducing ventilator-associated pneumonia in a Chinese neonatal intensive care unit. Am J Infect Control. (2013) 41:1059–64. doi: 10.1016/j.ajic.2013.06.007
107. Guo Q, Guo L, Yan H. Application of modified SBAR communication mode in nursing handover management of patients with severe hepatopathy. Zhong Xi Yi Jie He Hu Li. (2017) 3:134. doi: 10.11997/nitcwm.201706040
108. Shen H, Wang Y, Edwards H. Can a community-based peer-led diabetic self-management programme be effective: 12-week evaluation. J Clin Nurs. (2017) 26:1621–31. doi: 10.1111/jocn.13526
109. Ge Z, Xia Z, Ma K, Cao J, Mao S, Gong L. Clinical practice and evaluation of management of patients based on clinical pathway of emergency respiratory and cardiac arrest. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. (2019) 31:313–18. doi: 10.3760/cma.j.issn.2095-4352.2019.03.011
110. Huang Q, Wei G, Lu L. The effect of innovative thinking on nursing management. You Jiang Min Zu Yi Xue Yuan Xue Bao. (2016) 38:236–38. doi: 10.3969/j.issn.1001-5817.2016.02.040
111. Cong L, Yu J, Liu Y. Implementing a continuous quality improvement program for reducing pressure prevalence in a teaching hospital in China. J Wound Ostomy Contin Nurs. (2012) 39:509–13. doi: 10.1097/WON.0b013e318264c3a0
112. Hao Y, Liu J, Liu J, Smith S, Huo Y, Fonarow G, et al. Rationale and design of the Improving Care for Cardiovascular Disease in China (CCC) project: A national effort to prompt quality enhancement for acute coronary syndrome. Am Heart J. (2016) 179:107–15. doi: 10.1016/j.ahj.2016.06.005
113. Cai J, Huang X, Gu X. Application of graded partition nursing based on modified early warning score in management of orthopedic ward. Hu Li Shi Jian Yu Yan Jiu. (2020) 2020:6. doi: 10.3969/j.isn.1672-9676.2020.06.029
114. Gu C, Zhang Z, Ding Y. Chinese midwives' experience of providing continuity of care to labouring women. Midwifery. (2011) 27:243–9. doi: 10.1016/j.midw.2009.06.007
115. Li DC, Cheng HR, Zhang W, Chen L, Weng AW, Wu BQ. The experience of shortening average length of stay in china. Biomed Res. (2018) 29:3228–32. doi: 10.4066/biomedicalresearch.29-17-3984
116. Gao H, Chen H, Feng J, Qin X, Wang X, Liang S. Balanced scorecard-based performance evaluation of Chinese county hospitals in underdeveloped areas. J Int Med Res. (2018) 46:1947–62. doi: 10.1177/0300060518757606
117. Wang X, Yan S, Wang Y, Wu N. Surgical quality surveillance and sustaining improvement of lung cancer surgery based on Standard Operation Procedure (SOP): experience of single surgical team. Chin J Lung Cancer. (2017) 20:253–8. doi: 10.3779/j.issn.1009-3419.2017.04.05
118. Feng S, Lyu Y, Yang Y. Innovative practice and effect evaluation of refined nursing management in children's ENT ward. Shi Yong Lin Chuang Hu Li Xue Za Zhi. (2019) 8. Available online at: https://www.cnki.com.cn/Article/CJFDTotal-SLHL201908140.htm. (accessed February 8, 2020).
119. Chen C, Huang Y, Liu C, Xu Y, Zheng L, Li J. Effects of an Interdisciplinary Care Team on the Management of Alzheimer's Disease in China. J Gerontol Nurs. (2019) 45:39–45. doi: 10.3928/00989134-20190318-01
120. Ren J, Liu C, Gao Q, Yang L, Huang X, Guo Q. Use of appropriate healthcare technologies: a cross-sectional study in rural Zhejiang of China. BMC Health Serv Res. (2015) 15:295. doi: 10.1186/s12913-015-0947-4
121. Su C, Lu Z, Yi L. Application of meticulous management in the clinical nursing pathway. Zhonghua Xian Dai Hu Li Za Zhi. (2014) 017:2136–8. doi: 10.3760/cma.j.issn.1674–2907.2014.17.037
122. Wang X, Sun X, Gong F, Huang Y, Chen L, Zhang Y, et al. The Luohu model: a template for integrated urban healthcare systems in China. Int J Integr Care. (2018) 18:3. doi: 10.5334/ijic.3955
123. Li S, Fu X. Analysis on the clinical pathway for patients with cataract. Intern Eye Sci. (2014) 14:343–5. doi: 10.3980/j.issn.1672-5123.2014.02.42
124. Tang W, Wei L, Zhang L. Analysing a Chinese regional integrated healthcare organisation reform failure using a complex adaptive system approach. Int J Integr Care. (2017) 17. doi: 10.5334/ijic.2420
125. Zhang H, van Doorslaer E, Xu L, Zhang Y, van de Klundert J. Can a results-based bottom-up reform improve health system performance? Evidence from the rural health project in China. Health Econ. (2019) 28:1204–19. doi: 10.1002/hec.3935
126. Wang L, Wang Y, Lou Y, Li Y, Zhang X. The role of quality control circles in sustained improvement of medical quality. Springerplus. (2013) 2:141. doi: 10.1186/2193-1801-2-141
127. Ji J, Jin X, Chen Z. Improvement of nude scheduling based on six thinking hats thinking model. Hu Li Xue Za Zhi. (2018) 2018:15. doi: 10.3870/j.issn.1001-4152.2018.15.049
128. Qian G. The clinical effect of risk management on cardiology nursing. Shi Yong Lin Chuang Hu Li Dian Zi Za Zhi. (2016) 1. Available online at: https://www.cnki.com.cn/Article/CJFDTotal-SLHL201606022.htm. (accessed September 18, 2020).
130. Wisdom J, Chor KHB, Hoagwood K, Horwitz S. Innovation adoption: a review of theories and constructs. Admin Policy Mental Health. (2014) 41:480–502. doi: 10.1007/s10488-013-0486-4
131. Miao Q, Newman A, Sun Y, Xu L. What factors influence the organizational commitment of public sector employees in China? The role of extrinsic, intrinsic and social rewards. Int J Hum Resour Manage. (2013) 24:3262–80. doi: 10.1080/09585192.2013.770783
132. Li L, Hu H, Zhou H, He C, Fan L, Liu X. Work stress, work motivation and their effects on job satisfaction in community health workers: a cross-sectional survey in China. BMJ Open. (2014) 4:6.e004897. doi: 10.1136/bmjopen-2014-004897
133. Zhang C, Liu Y. The salary of physicians in Chinese public tertiary hospitals: a national cross-sectional and follow-up study. BMC Health Serv Res. (2018) 18:1–9. doi: 10.1186/s12913-018-3461-7
134. Hofstede G. (2021). COUNTRY COMPARISON. Available online at: https://www.hofstede-insights.com/country-comparison/china/. (accessed February 22, 2021).
135. Meng Q, Yuan J, Jing L. Mobility of primary health care workers in China. Hum Resour Health. (2009) 7:1–5. doi: 10.1186/1478-4491-7-24
136. World Bank Urban China (2014). Available online at: https://www.worldbank.org/content/dam/Worldbank/document/EAP/China/Urban-China-SRs1-3.pdf. (accessed February 16, 2021).
Keywords: innovation, implementation, health service, China, systematic review
Citation: Wang W, van Wijngaarden J, Wang H, Buljac-Samardzic M, Yuan S and van de Klundert J (2021) Factors Influencing the Implementation of Foreign Innovations in Organization and Management of Health Service Delivery in China: A Systematic Review. Front. Health Serv. 1:766677. doi: 10.3389/frhs.2021.766677
Received: 29 September 2021; Accepted: 02 December 2021;
Published: 20 December 2021.
Edited by:
Steven W. Howard, Saint Louis University, United StatesReviewed by:
Pedro Gallo, University of Barcelona, SpainCopyright © 2021 Wang, van Wijngaarden, Wang, Buljac-Samardzic, Yuan and van de Klundert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenxing Wang, dy53YW5nQGVzaHBtLmV1ci5ubA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.