 Noémie Roland
Noémie Roland Sébastien Froelich
Sébastien Froelich Alain Weill1*
Alain Weill1*
- 1EPI-PHARE Scientific Interest Group Department (French National Agency for the Safety of Medicines and Health Products, and French National Health Insurance), Saint-Denis, France
- 2Department of Neurosurgery, Lariboisière University Hospital, Paris-Cité University, Assistance Publique-Hôpitaux de Paris, Paris, France
1 Introduction
Depot medroxyprogesterone acetate (DMPA) is a widely-prescribed injectable progestogen contraceptive used by 74 million women each year around the world (1). DMPA is particularly popular for its high effectiveness and ease of administration (2). Indeed, this contraception consists of a medroxyprogesterone acetate 150 mg/ml intramuscular injection or a 104 mg/0.65 ml subcutaneous injection every 3 months (3). DMPA's usage varies greatly from one country to another: from 1.8% of women aged 15–49 in high-income countries to 8.7% in low-income countries (1). Inexpensive, DMPA is particularly widespread in countries with a strong family planning policy, like many countries in South-Eastern Asia (13% of women of Southeast Asia use DMPA, i.e., about 22 million women/year in 2019) (1, 4). In Indonesia, it is the contraception used by one quarter of women (17 million women, which makes this country the biggest user of this contraception), and by one woman out of five in Myanmar (2.5 million), one woman out of 10 to 20 in Thailand (1.5 to 2 million), Cambodia (0,3 million), Laos (0,2 million), and one woman out of 30 in the Philippines (0,9 million) and Malaysia (0,3 million) (1, 5, 6). In Africa, Malawi (33.6% of women, 1.1 million), Ethiopia (21% of women, 4.6 million) and South Africa (23.4% of women, 3.6 million) are the most concerned. Lastly, 1% of Australian women were concerned by this contraception in 2015, and in the USA, 25.4% of women aged 15–44 years have ever used DMPA in their life (2.6% of American women/year, 1.7 million) (7).
However, DMPA has significant and sometimes serious adverse side effects, such as weight gain, menstrual irregularities, changes in mood, osteoporosis, and arteriovenous thrombosis disorders. In addition to these known side effects, the risk of meningioma has been added by international scientific publications for DMPA, as added previously for other progesterone-derived drugs.
2 Risk of meningioma
2.1 Progressive evidence of a causal relationship between progestogens and meningioma
As early as 2007, two case reports (in Italy and France) reported the first cases of meningioma in women exposed to a progestogen with strong antiandrogen effects, cyproterone acetate, suggesting that this progestogen is a causal factor of a particular histopathological tumor entity (8, 9). The French team also noted stabilization of the tumor after the cessation of cyproterone acetate treatment (9).
In 2019, a nationwide pharmaco-epidemiological study conducted by the French National Health Insurance confirmed the strong dose-response relationship between the use of cyproterone acetate and meningiomas requiring surgery or radiotherapy (10). Indeed, the risk was multiplied by 20 for a cumulative dose over 60 g (i.e., 5 years of treatment). In the aftermath of this study, the European Medicines Agency (EMA) reassessed the benefit/risk ratio of cyproterone acetate and recommended restricting its prescription and regular MRI screening. Cyproterone acetate is marketed in high doses in Australia, Indonesia, Thailand and New Zealand but not currently marketed in the United States. This progestogen treatment is also widely used in many countries as antiandrogen cross-sex hormone treatment for transgender women with a well-identified risk of intracranial meningioma (11).
Then, in 2021, studies found a strong association between the risk of meningioma and the use of two other potent progestogens, nomegestrol and chlormadinone acetate, mainly prescribed for the hormonal treatment of menopause in Europe. In Asia and Oceania, nomegestrol acetate (2.5 mg in combination with estradiol 1.5 mg) is only marketed in Australia, Malaysia and New Zealand, whereas chlormadinone acetate is not marketed. These drugs have never been approved in the US. The magnitude of meningioma risk with nomegestrol and chlormadinone was less than that of cyproterone acetate, although still high (12–15). In July 2022, the EMA recommended that high-dose formulations of nomegestrol and chlormadinone acetate be used at the lowest possible dose over the shortest possible period.
For these three progestogens—cyproterone, chlormadinone and nomegestrol acetate -, European drug regulators have recognized the causal nature of the association between exposure and intracranial meningiomas.
2.2 About 6-fold increase in the risk of meningioma for DPMA
In a recent study in France (12), where DMPA is not frequently used, an excess risk of intracranial meningioma linked to its long-term use (≥1 year) has been found at the dose of 150 mg [OR = 5.6 (2.2–14.4)] (12), leading to fears of a significant prevalence of intracranial meningiomas where women are highly exposed to DMPA. If this result had been isolated internationally, it could have constituted a weak signal that would have to be further analyzed and, if necessary, confirmed by other studies. However, there is already a great deal of converging evidence in favor of a very strong association between DMPA contraception and meningiomas.
First, meningiomas that occur during DMPA exposure seem to share common characteristics with meningiomas associated with other progestogens [cyproterone, nomegestrol and chlormadinone acetates (10, 14)]: high progesterone- and low estrogen-receptors expressions, frequent existence of several meningiomas at the time of diagnosis (meningiomatosis), preferential location in the anterior and/or middle part of the base of the skull (10, 12–15), regression of volume on cessation of progestogen treatment (16–18), predominance of transitional sub-types, and a specific mutational landscape with a high rate of PIK3CA mutation and low rate of NF2 mutation (19). The characteristic location in the skull base makes surgery more difficult, with more frequent incomplete resections, leading to more sequelae, recurrences and re-operations.
Secondly, a first case-report in 2000 (20), a review of case reports in the USA published in 2023 (21), a large case-control in the USA published in September 2024 (22), and several studies carried out and Indonesia (seven studies, including only three medline-indexed), in which one quarter of women taking contraception use DMPA, have assessed a risk between this contraceptive exposure and intracranial meningiomas (6, 23–29). These studies have been somewhat overlooked, despite providing us with valuable epidemiological data Table 1.
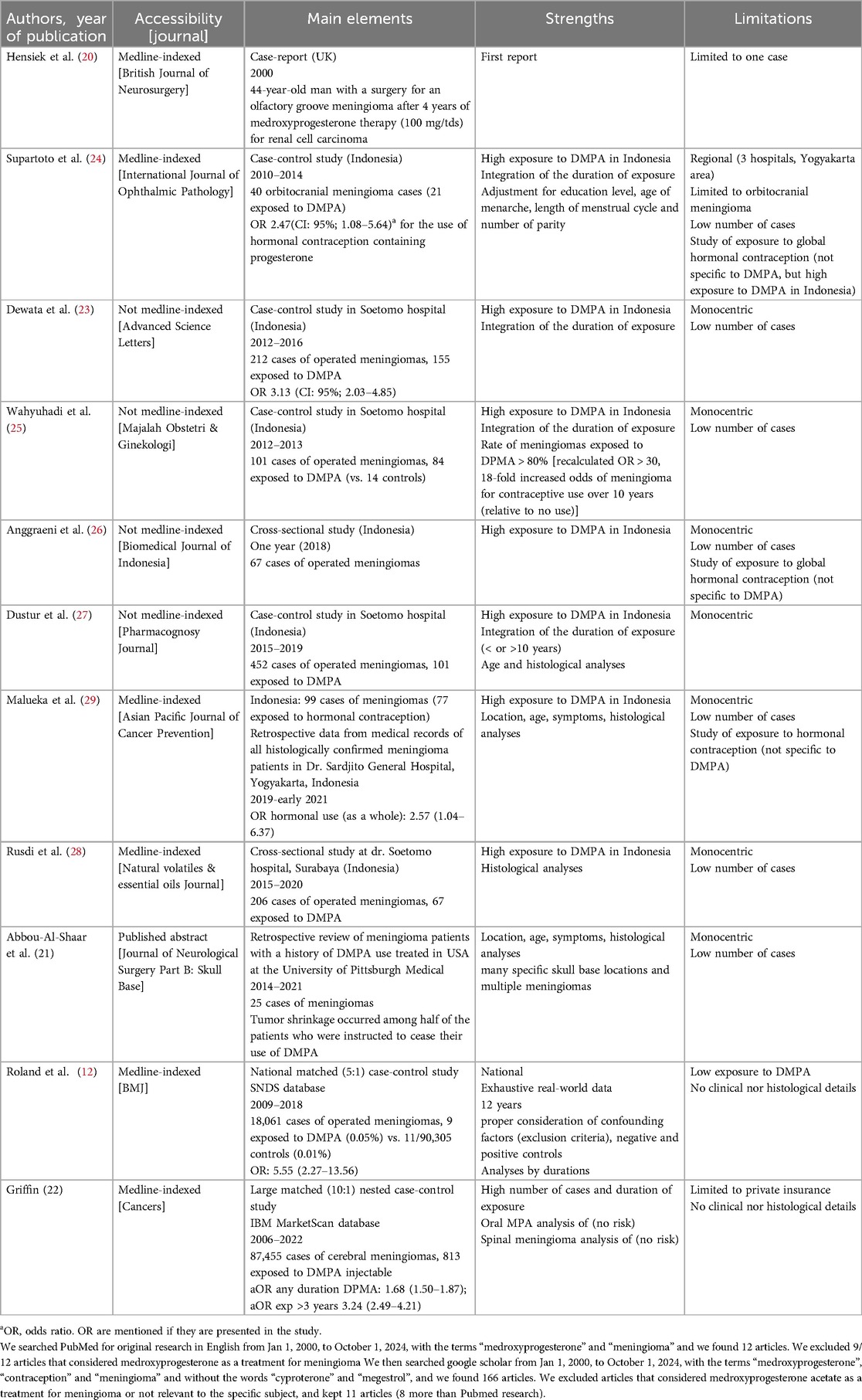
Table 1. Available observational studies on medroxyprogesterone acetate and risk of meningioma.
In the United-States, Abou-Al-Shar et al. first performed a retrospective review of meningioma patients with a history of DMPA use treated at the University of Pittsburgh Medical center between 2014 and 2021 (21). They included 25 women with a mean age of 46 years suffering from intracranial meningiomas [a total of 49 meningiomas (1 to 6 per woman)] and exposed to DMPA chronic use. The mean duration of use was 15 years [6 to 26 years] and more than two thirds of patients had at least one skull base meningioma located in the spheno-cavernous, spheno-orbital, or orbital region. Interestingly, five non-operated patients showed clear signs of tumour shrinkage after stopping DMPA injections. Moreover, recently, using US private insurance data, a large case-control study showed that DMPA exposure was associated with meningioma [480 cases of cerebral meningioma exposed to DMPA, OR: 1.68 (95% CI: 1.50–1.87)] (22). This association was dose-dependent (OR DPMA > 3 years: 3.24 (2.49–4.21). This association was not found with oral medroxyprogesterone [OR 0.99 (0.94–1.04)], nor with spinal meningiomas (22).
Then, some monocentric Indonesian studies have assessed hormonal contraceptive exposure in surgical records of meningiomas (from 47% for Anggraeni et al. in 2018 (26) to 96% for Dustur et al. in 2015–2019 (27). Some studies detailed the prior use of hormonal contraceptives et found specific history of DMPA exposure (from 36% of meningioma patients for Rusdi et al. (28) to 83% for Dustur et al. (27). Lastly, two case-controls studies assessed the dose-response association between meningioma risk and DMPA use. Wahyuhadi et al. found that DMPA has a higher risk rate of meningioma compared with other hormonal contraceptives (25): 84/101 (83.2%) cases were exposed among the cases group (i.e., operated on meningiomas), and 14/101 (13.9%) were exposed among the controls (non-meningioma patients who had undergone contrast head CT-scan). Even though cases and controls in this study were not completely similar in terms of age, these results are particularly concerning. Lastly, Dewata et al. found a specific risk of meningioma among women exposed to DMPA (155 DMPA users/212 cases) of 3.13 (CI: 95%; 2.03–4.85) with a dose-cumulative effect: the longer the duration of exposure to DMPA, the higher the risk for meningioma [duration of 10 to 15 years: OR 2.33 (CI: 95%; 1.31–4.15), and more than 15 years: OR 4.45 (CI: 95%; 2.35–8.35)] (23).
3 Discussion
3.1 A plea for a global awareness
Using the incidence of meningioma among women aged 35–44 year-old from Wiemels et al. (30), we can assess that a risk of meningioma multiplied by 1.68 [OR from Griffin, 2024 (22)] to 5.55 [Roland et al. (12)] would lead to a number of symptomatic and/or surgical meningiomas attributable to DMPA exposure of more than 2,800 to more than 18 000 worldwide each year.
The magnitude of the risk of meningioma between that associated with the use of cyproterone acetate and that associated with DMPA is, of course, not the same. Nevertheless, DMPA is much more widely prescribed than CPA, and the contraceptive can be used without interruption for periods of over 10 years. With the arrival of the subcutaneous form, we can expect to see even more prescriptions for DMPA worldwide than before, as it could be self-administrated, although with a smaller dose (31). As the subcutaneous form is not available in France, we have not been able to carry out meningioma risk studies with this specific dosage. Countries with access to these data should take up this subject to assess the associated risk of meningioma with 104 mg/0.65 ml form.
DMPA may influence the cellular proliferation of meningioma cell lines; however, the molecular mechanisms underlying this process fall beyond the scope of this viewpoint article. While a potential causal relationship between DMPA use and meningioma formation cannot be ruled out, definitive experimental evidence remains lacking. Notably, some studies on animal models of meningiomas have reported an overexpression of progesterone receptors in subjects that developed these tumors (32, 33). Given the potential clinical implications, specialized molecular research teams should further investigate this topic to clarify the underlying mechanisms.
While DMPA is presented as a lever for equitable access to contraception (34), particularly since the COVID crisis or in the post-Roe era (35), women and prescribers must be aware of the risk of meningioma in order to make an informed choice of contraception. In our experience, neurological monitoring should be the rule in the event of DMPA prolonged treatment (more than 10 years) and in patients over 40 years of age to detect a meningioma as early as possible. In case of meningioma discovery, DMPA must be discontinued, as this may lead to tumor regression and avoid the need for surgery.
Since these DPMA-exposed meningiomas occur in countries with a low socio-economic level where access to brain imaging for neurological symptoms could be very complicated and neurosurgery less accessible, it is likely that many diagnoses are ignored or that skull-base surgery is rejected because of its complexity, the vital risk and the neurological prognosis. Similarly, in high-income countries, DMPA particularly affects vulnerable populations or those suffering from known inequalities in access to healthcare (e.g., DMPA users are disproportionately non-White in the USA (34), and DMPA is also known to prescribed to migrants and people with mental conditions (36). Thus, even in countries with extensive healthcare networks, the utmost vigilance is also called for.
3.2 Conclusion
The meningioma risk arising from the prolonged and ongoing use of DMPA should be the subject of epidemiological studies in all the countries concerned, especially cohort or case-control studies using claims data, such as the one carried out recently in the USA (22). Priority should be given to targeting people with the least access to health care facilities: disadvantaged populations in developed countries, for whom DMPA is often prescribed (using public rather than private insurance databases, for example), or to larger-scale, better-conducted case-control studies in neurosurgical centers from disadvantaged countries than those carried out in Indonesia to date. Lastly, assessing the risk associated with the specific dose prescribed subcutaneously, and the risk associated after treatment discontinuation are also important issues. The benefit-risk balance and alternatives also need to be discussed.
We call on the international scientific community to mobilize in the face of this legitimate public health concern on the sensitive but essential subject of contraception. Assessing the risk of meningioma among DMPA users, especially in countries with low socio-economic levels, has become a global public health necessity.
Author contributions
NR: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. SF: Validation, Writing – original draft, Writing – review & editing. AW: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the French National Health Insurance Fund (CNAM) and the French National Agency for Medicines and Health Products Safety (ANSM) via the Health Product Epidemiology Scientific Interest Group EPI-PHARE.
Acknowledgments
We would like to thank Alex Edelman and Associates for English proofreading of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. United Nations. Contraceptive Use by Method 2019: Data Booklet. New York: UN (2019). doi: 10.18356/1bd58a10-en
2. Jacobstein R, Polis CB. Progestin-only contraception: injectables and implants. Best Pract Res Clin Obstet Gynaecol. (2014) 28:795–806. doi: 10.1016/j.bpobgyn.2014.05.003
3. Halpern V, Brache V, Taylor D, Lendvay A, Cochón L, Jensen JT, et al. Clinical trial to evaluate pharmacokinetics and pharmacodynamics of medroxyprogesterone acetate after subcutaneous administration of Depo-Provera. Fertil Steril. (2021) 115:1035–43. doi: 10.1016/j.fertnstert.2020.11.002
4. United Nations. World Contraceptive Use | Population Division. (2022). Available online at: https://www.un.org/development/desa/pd/data/world-contraceptive-use (accessed July 17, 2024).
5. United Nations. Family Planning and the 2030 Agenda for Sustainable Development (Data Booklet). New York: United Nations (2019). doi: 10.18356/e154e49d-en
6. Maharani A, Sujarwoto S, Ekoriano M. Health insurance and contraceptive use, Indonesian family planning census 2021. Bull World Health Organ. (2023) 101:513–21. doi: 10.2471/BLT.22.289438
7. Centers for Disease Control and Prevention. Key Statistics from the National Survey of Family Growth. (2019). http://www.cdc.gov/nchs/nsfg/key_statistics/i.htm (accessed April 28, 2024).
8. Gazzeri R, Galarza M, Gazzeri G. Growth of a meningioma in a transsexual patient after estrogen-progestin therapy. N Engl J Med. (2007) 357:2411–2. doi: 10.1056/NEJMc071938
9. Froelich S, Dali-Youcef N, Boyer P, Kehrli P, Maitrot D, Auwerx J, et al. L’acétate de cyprotérone (Androcur) favorise-t-il la méningiomatose? Rev Méd Int. (2007) 28S:S317–89.
10. Weill A, Nguyen P, Labidi M, Cadier B, Passeri T, Duranteau L, et al. Use of high dose cyproterone acetate and risk of intracranial meningioma in women: cohort study. Br Med J. (2021) 372:n37. doi: 10.1136/bmj.n37
11. Nota NM, Wiepjes CM, de Blok CJM, Gooren LJG, Peerdeman SM, Kreukels BPC, et al. The occurrence of benign brain tumours in transgender individuals during cross-sex hormone treatment. Brain J Neurol. (2018) 141:2047–54. doi: 10.1093/brain/awy108
12. Roland N, Neumann A, Hoisnard L, Duranteau L, Froelich S, Zureik M, et al. Use of progestogens and the risk of intracranial meningioma: national case-control study. Br Med J. (2024) 384:e078078. doi: 10.1136/bmj-2023-078078
13. Hoisnard L, Laanani M, Passeri T, Duranteau L, Coste J, Zureik M, et al. Risk of intracranial meningioma with three potent progestogens: a population-based case-control study. Eur J Neurol. (2022) 29(9):2801–9. doi: 10.1111/ene.15423
14. Nguyen P, Roland N, Neumann A, Hoisnard L, Passeri T, Duranteau L, et al. Prolonged use of nomegestrol acetate and risk of intracranial meningioma: a population-based cohort study. Lancet Reg Health Eur. (2024) 42:100928. doi: 10.1016/j.lanepe.2024.100928
15. Roland N, Nguyen P, Neumann A, Hoisnard L, Passeri T, Duranteau L, et al. Prolonged use of chlormadinone acetate and risk of intracranial meningioma: a population-based cohort study. Eur J Neurol. (2024) n/a:e16505. doi: 10.1111/ene.16505
16. Passeri T, Champagne P-O, Bernat A-L, Hanakita S, Salle H, Mandonnet E, et al. Spontaneous regression of meningiomas after interruption of nomegestrol acetate: a series of three patients. Acta Neurochir. (2019) 161:761–5. doi: 10.1007/s00701-019-03848-x
17. Voormolen EHJ, Champagne PO, Roca E, Giammattei L, Passeri T, di Russo P, et al. Intracranial meningiomas decrease in volume on magnetic resonance imaging after discontinuing progestin. Neurosurgery. (2021) 89:308–14. doi: 10.1093/neuros/nyab175
18. Passeri T, Giammattei L, Le Van T, Abbritti R, Perrier A, Wong J, et al. Atypical evolution of meningiomatosis after discontinuation of cyproterone acetate: clinical cases and histomolecular characterization. Acta Neurochir. (2022) 164:255–63. doi: 10.1007/s00701-021-05005-9
19. Peyre M, Gaillard S, de Marcellus C, Giry M, Bielle F, Villa C, et al. Progestin-associated shift of meningioma mutational landscape. Ann Oncol. (2018) 29:681–6. doi: 10.1093/annonc/mdx763
20. Hensiek AE, Kellerman AJ, Hill JT. Spontaneous regression of a solitary cerebral metastases in renal carcinoma followed by meningioma development under medroxyprogesterone acetate therapy. Br J Neurosurg. (2000) 14:354–6. doi: 10.1080/026886900417388
21. Abou-Al-Shaar H, Wrigley R, Patel A, Mallela AN, Zenonos GA, Gardner PA. Skull base meningiomas as part of a novel meningioma syndrome associated with chronic depot medroxyprogesterone acetate use. J Neurol Surg B Skull Base. (2023) 84:S1–S344. doi: 10.1055/s-0043-1762201
22. Griffin RL. The association between medroxyprogesterone acetate exposure and meningioma. Cancers (Basel). (2024) 16:3362. doi: 10.3390/cancers16193362
23. Dewata L, Prasetyo B, Yuliati A, Wahyuhadi J. Hormonal contraceptive exposure and risk factors for meningioma in Soetomo hospital 2012–2016. Adv Sci Lett. (2017) 23:3291–4. doi: 10.1166/asl.2017.9121
24. Supartoto A, Mahayana IT, Christine RN, Suhardjo Agni AN, Sasongko MB. Exposure to exogenous female sex hormones is associated with increased risk of orbito-cranial meningioma in females: a case-control study. Int J Ophthalmic Pathol. (2016) 5:3. doi: 10.4172/2324-8599.1000183
25. Wahyuhadi J, Heryani D, Basuki H. Risk of meningioma associated with exposure of hormonal contraception. A case control study. Maj Obstet Ginekol. (2018) 26:36. doi: 10.20473/mog.V26I12018.36-41
26. Anggraeni D, Diansari Y, Hafy Z. Demographic, clinical, and tumor profile of meningioma in mohammad hoesin hospital palembang, Indonesia. Biomed J Indones. (2022) 8(1):1–4. doi: 10.32539/BJI.v8i1.122
27. Dustur S, Wahyuhadi J, Utomo B, Parenrengi M, Bajamal A, Dwiningsih S. Relationship histopathology grading of meningioma with the use of medroxyprogesterone acetate (MPA) as a hormonal contraceptive. Pharmacogn J. (2022) 14:938–41. doi: 10.5530/pj.2022.14.193
28. Rusdi AFP. Association between hormonal contraception with histopathology grading of meningioma. Nat Vol Essent Oil. (2022) 9(1):1583–92.
29. Malueka RG, Hartanto RA, Setyawan NH, Fauzi DNF, Damarjati KR, Rismawan A, et al. Association of hormonal contraception with meningioma location in Indonesian patients. Asian Pac J Cancer Prev. (2022) 23:1047–51. doi: 10.31557/APJCP.2022.23.3.1047
30. Wiemels J, Wrensch M, Claus EB. Epidemiology and etiology of meningioma. J Neurooncol. (2010) 99:307–14. doi: 10.1007/s11060-010-0386-3
31. Aderoba AK, Steyn PS, Kiarie JN. Implementation strategies to scale up self-administered depot medroxyprogesterone acetate subcutaneous injectable contraception: a scoping review. Syst Rev. (2023) 12:114. doi: 10.1186/s13643-023-02216-2
32. Adamo PF, Cantile C, Steinberg H. Evaluation of progesterone and estrogen receptor expression in 15 meningiomas of dogs and cats. Am J Vet Res. (2003) 64:1310–8. doi: 10.2460/ajvr.2003.64.1310
33. Tomanelli M, Florio T, Vargas GC, Pagano A, Modesto P. Domestic animal models of central nervous system tumors: focus on meningiomas. Life Basel Switz. (2023) 13:2284. doi: 10.3390/life13122284
34. Burlando AM, Flynn AN, Gutman S, McAllister A, Roe AH, Schreiber CA, et al. The role of subcutaneous depot medroxyprogesterone acetate in equitable contraceptive care: a lesson from the coronavirus disease 2019 (COVID-19) pandemic. Obstet Gynecol. (2021) 138:574. doi: 10.1097/AOG.0000000000004524
35. Nakaishi L, Castelli G. Is self-administered DMPA an answer to contraception access in the post-roe era? J Fam Pract. (2023) 72:84–6. doi: 10.12788/jfp.0558
Keywords: depot medroxyprogesterone acetate, contraception, meningioma, progestogen, public health
Citation: Roland N, Froelich S and Weill A (2025) Medroxyprogesterone acetate and meningioma: a global issue. Front. Glob. Women's Health 6:1470539. doi: 10.3389/fgwh.2025.1470539
Received: 14 August 2024; Accepted: 17 March 2025;
Published: 26 March 2025.
Edited by:
Berna Dilbaz, University of Health Sciences, TürkiyeReviewed by:
Omkar Ijare, Houston Methodist Research Institute, United StatesJoe M. Das, Imperial College London, United Kingdom
Copyright: © 2025 Roland, Froelich and Weill. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alain Weill, YWxhaW4ud2VpbGxAYXNzdXJhbmNlLW1hbGFkaWUuZnI=