 Hege Svean Koksvik1*
Hege Svean Koksvik1* Ingrid Nilssen1
Ingrid Nilssen1 Bente Jakobsen1Hilde Bjørngaard1
Bente Jakobsen1Hilde Bjørngaard1 Marianne Wallenius1,2
Marianne Wallenius1,2 Kjersti Grønning3,4
Kjersti Grønning3,4
- 1The Norwegian National Network of Pregnancy and Rheumatic Diseases, Department of Rheumatology, St Olavs Hospital Trondheim University Hospital, Trondheim, Norway
- 2Department of Neuromedicine and Movement Science, The Norwegian University of Science and Technology, Trondheim, Norway
- 3Department of Research, Nord-Trøndelag Hospital Trust, Levanger, Norway
- 4Department of Public Health and Nursing, The Norwegian University of Science and Technology, Trondheim, Norway
Objectives: More knowledge about health related quality of life (HRQoL) among mothers with inflammatory joint disease (IJD) is needed to understand the complex challenges for this group of patients. The overall aim of this study was to investigate changes in HRQoL among mothers with IJD from year 2000 to year 2020.
Methods: This study had a comparative cross-sectional design with two study groups 20 years apart, year 2000 (n = 77) and year 2020 (n = 197). Patients were identified from RevNatus, a Norwegian nationwide medical quality register (2020 cohort) and from a national centre for pregnancy and rheumatic disease (2000 cohort). Mothers with the diagnoses of rheumatoid arthritis, juvenile idiopathic arthritis, axial spondyloarthritis and psoriatic arthritis with children aged 0–6 were included. Data on HRQoL were self-reported and assessed by the RAND-36 (SF-36) questionnaire, along with data on educational status, number of children, months since last childbirth and eight questions on experienced motherhood limitations and experienced anxiety and distress for the children. Descriptive statistics were performed using the Mann-Whitney U-test, the Pearson chi-squared test and independent samples t-test. Multivariable linear regression were used to investigate changes and association between the RAND36 (SF-36) scores and the two study groups and possible confouders.
Results: The 2020 cohort had significantly higher scores on bodily pain (p < 0.001), physical function (p < 0.001), and role physical (p = 0.01) scales compared to the 2000 cohort, indicating better health. There were no significant differences between the two cohorts in the mental health (MH) (p = 0.81), vitality (p = 0.09), general health (p = 0.06), social function (p = 0.83), and role emotional (p = 0.93) scales. Compared to the calculated norm scores, the 2020 cohort had significantly lower scores on all scales (p < 0.01) except on the MH scale (p = 0.37).
Conclusion: Mothers with IJD were affected in most dimensions of RAND-36 (SF-36) both in year 2000 and year 2020. The findings emphasize the importance of understanding the intrusiveness of being a mother with IJD despite the improved medical treatment options over the last 20 years.
1 Introduction
The impact of inflammatory joint diseases (IJD) like rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) is pervasive and can affect patients' physical and psychological health, social functioning, quality of life and work ability. Untreated, IJD may cause irreversible joint damage and is associated with substantial morbidity and disability compared to the general population. The severity of symptoms and disease activity may fluctuate over time (1–7).
Although there is still no cure for IJD, early diagnosis and aggressive treatment with biological therapies have resulted in substantial major clinical improvements over the past 25 years with significant improvement in symptoms, function, and quality of life. However, many patients still experience that the disease affects many aspects of daily life, even though advances in medical treatment can reduce symptoms (8–15).
The assessment of health related quality of life (HRQoL) in IJD is becoming increasingly common in both research and clinical practice. HRQoL refers to “how health impacts on an individual's ability to function and his or her perceived well-being in physical, mental and social domains of life” (16, 17). One of the most widely used tools for measuring HRQoL is the RAND-36 (equivalent to version 1 of the SF-36 Health Survey) (16–18).
Being a mother is generally considered to be one of the most fulfilling experiences for a woman, but the strain can often be great, having to cope with the problems of the illness and at the same time care for a small child (19). The presence of a painful, disabling chronic disease may have implications for the woman's perceived ability to fulfil a parenting role. Coping with motherhood and having IJD presents not only physical, but also psychological challenges (19). Women with IJD face a range of difficulties with early parenting due to fluctuations in disease activity, treatments for their disease, and difficulties with physical function, pain and fatigue (20–22). The women often stigmatize and blame themselves because they do not live up to their own and society's expectations (23), which may influence their HRQoL. Moreover, the identities of mothers with chronic diseases have been described as dynamic and complex, often experiencing disruption and requiring renegotiation during times of illness relapse or progression (24).
During the last 25 years the literature focus on many of the same challenges in being a mother with IJD with physical limitations; practical and caring issues; social factors; emotional response; hereditary risks; lack of receiving holistic care and appropriate information and education (19, 22, 23, 25–33).
At the Department of Rheumatology, St Olavs Hospital Trondheim University Hospital, a cross-sectional study on HRQoL and experienced limitations in motherhood among mothers with IJD was performed 25 years ago (29). The results showed that the HRQoL scores in the IJD group were lower on most dimensions compared with data from healthy controls. The IJD group also experienced several limitations in motherhood and anxiety/distress about the disease causing extra demands on the children (29).
More integrated care and better information and counselling around early parenting for women with IJD have been recommended (20–22, 33). Previous studies conclude that women with IJD want their motherhood identities and associated preferences to be taken into account in decisions about their healthcare (21, 22, 33). In addition, health professionals need to consider women's multiple and sometimes conflicting identities, and include both their condition and family-associated goals and values in the healthcare (33), in alignment with the core elements of person-centered care. Person-centered care is considered a key component of effective illness management and high-quality care (34, 35) and is by the Word Heath Organization (WHO) emphasized as a core competency of health workers in this endeavor to change and improve the health care system (36). Hence, more knowledge about HRQoL among mothers with IJD is needed to develop individually tailored person-centred care for this group of patients.
The overall aim of this study is to investigate changes in HRQoL among mothers with IJD from year 2000 to year 2020.
The main objectives:
• Study differences in HRQoL among two cohorts of mothers with IJD from 2000 to 2020
• Study similarities and differences in HRQoL among mothers with IJD with the norm population
• Study similarities and differences in experienced motherhood limitations and anxiety/distress about the disease among mothers with IJD in 2000 and 2020
2 Materials and methods
2.1 Study population
This study has a comparative cross-sectional design. The inclusion criteria were women with an IJD diagnosis M05.8, M05.9, M06.0, M07.3+ L40.5, M45, M46.8, M46.9, M08.0 and M08.9, before pregnancy, having one or more children in the age group 0–6.
2.1.1 The 2020 cohort
Patients fulfilling the inclusion criteria were identified from RevNatus, a Norwegian nationwide medical quality register operated by the Norwegian National Network of Pregnancy and Rheumatic Diseases (NKSR). Women with inflammatory rheumatic diseases are prospectively followed in the registry from the time of planning a pregnancy until one year after delivery (37). Patients giving birth in the period 2014–2019 were invited by a postal questionnaire including a written informed consent. The questionnaire included the RAND-36 (SF-36), eight questions about special concerns about being a rheumatic mother, educational status, number of children and months since last childbirth.
Demographic variables and disease-related variables were retrieved from RevNatus.
There were 375 eligible patients with IJD in the register with children aged 0–6 (given birth in the period 2014–2019).
2.1.2 The 2000 cohort
All patients in contact with a national centre for pregnancy and rheumatic disease (located at Department of Rheumatology, St Olavs Hospital Trondheim University Hospital), in the period from January 1996 to May 1999 fulfilling the inclusion criteria were invited to participate (29). There were 119 patients with children aged 0–6 eligible for the study. The eligible patients received a postal invitation letter containing a questionnaire with the RAND-36 (SF-36), eight questions about special concerns about being a rheumatic mother, educational status, number of children and months since last childbirth. The patients consented to participate by returning the questionnaire with no identifiable information.
2.1.3 Reference values/norm data
Norwegian reference values for the RAND-36 (SF-36) were published in 2018 based on a randomly drawn sample representative of the general Norwegian population with respect to age, gender, and place of residence. A norm calculator was conducted by the authors of the Norwegian reference study based on the reference values. The calculator (an excel sheet) is available for free. After entering the characteristics of the study sample, itcalculates expected means based on the characteristics of the study sample (age and gender). This calculator was used for the norm data (38).
2.2 Ethics and patient involvement
The 2000 cohort: A letter of invitation to eligible patients across Norway was sent with no identifications on the returned questionnaires, making the data unidentifiable. The Research Ethics Committee Health Region IV considered the study, for what approval was granted in March 1999 (REK 42-99).
The 2020 cohort: A written informed consent is required before inclusion in RevNatus. The registry was approved by the Regional Committee for Medical and Health Research Ethics (REK) Mid Norway in 2006. The present study also required informed consent and was approved by REK Sout/East Norway in April 2019 (2019/817/REK sor-ost).
Two patient representatives were involved in this study and commented on the design, development and dissemination plans of the project according to EULAR recommendations for the involvement of patient research partners in rheumatology research (39).
2.3 Variables
2.3.1 The rand-36 (SF-36)
The RAND-36 (equivalent to version 1 of the SF-36 Health Survey), is freely available and a widely used measure of generic HRQoL (17, 18, 40) and has been translated and validated in Norwegian patients with RA (41). Previous international and Norwegian studies have found RAND-36 (SF36) to be a valid, reliable, and suitable measurement of HRQoL in patients with IJD (41–43) and for young mothers with IJD (29).
The Norwegian version of the RAND-36 (SF36) version 1 was used in both the cohorts and in the reference study (38, 41). RAND-36 (SF-36) consists of 36 items, grouped into eight multi-item scales that measure physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE) and mental health (MH) (44). Item scores were transformed to 0–100 point scales (0 = worst, 100 = best) using the SF-36 algorithm (44). As per the SF36 algorithm, single imputation was employed meaning that missing values were replaced with the subjects' mean score for the completed items on the same scale if more than 50% of the scale's items were completed (44).
Eight questions on experienced motherhood limitations in caring for the children due to the disease, and experienced anxiety and distress about the disease causing extra demands on the children, were also included in the questionnaire (see Table 1). The questions were derived based on discussions, workshop and a final agreement between five specialist in psychology and a clinical nurse working with mothers with rheumatic diseases. A mean score for the six questions on experienced motherhood and two questions on anxiety/distress was calculated on a scale from 1 (No, none of the time/not limited at all) to 3 (Yes, often/limited a lot).
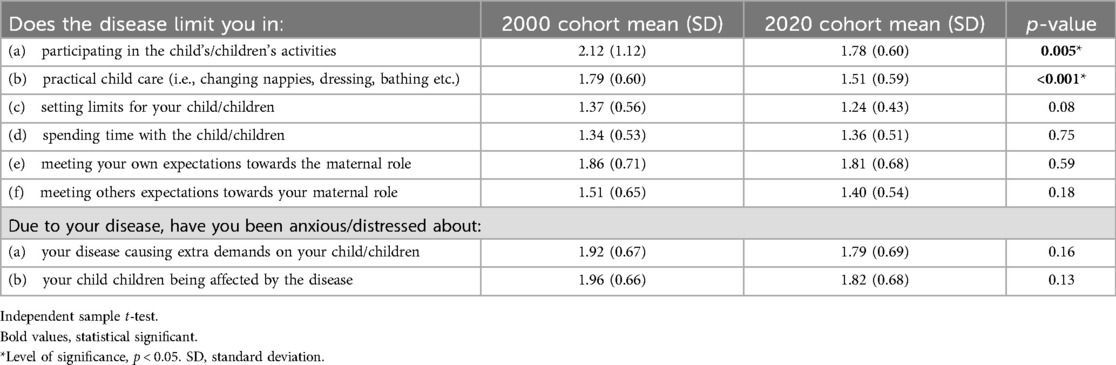
Table 1. Experienced limitations in motherhood and anxiety/distress for the children.
2.3.2 Other variables
Age of respondents at data collection, diagnosis and disease duration were retrieved from patient records (year 2000) or from RevNatus (year 2020) while educational status, number of children and months since last childbirth were self-reported through questionnaire.
2.4 Statistical analyses
Characteristics of the study populations are presented as median and inter quartile range or raw numbers and percentages. Descriptive statistics were performed using a non-parametric t-test of two samples, The Mann-Whitney U-test for non parametric continuous variables and the Pearson chi-squared test for categorical variables and independent samples t-test for parametric data. Pearson correlation and multivariable linear regression were used to investigate changes and association between the RAND36 (SF-36) scores and the two study groups, age, number of children, months since last childbirth, educational status, type of disease and disease duration. One sample t-test and standardized effect size (Cohens d) was used comparing the RAND-36 (SF-36) of the study population with expected population mean from the norm calculator. The independent samples t-test was used to compare the eight questions on “experienced motherhood limitations” and “experienced anxiety and distress” between the two study cohorts. For all statistical tests, a significance threshold of p < 0.05 was used. The statistical analyses were performed using IBM SPSS Statistics for Windows, version 29.0.1.
3 Results
3.1 Response rates
The 2000 cohort: Of the 125 questionnaires sent out, 6 were returned because of incorrect address, making a total of 119 eligible for the study. 77 questionnaires were returned, i.e., 65% of eligible subjects responded. No reminder was sent. The characteristics of the non-respondents are unknown.
The 2020 cohort: Of the 375 questionnaires sent out, 3 were returned because of incorrect address, making a total of 372 eligible for the study. 197 questionnaires were returned, i.e., 53% of eligible subjects responded. A reminder was sent with the possibility of a web-based response. The characteristics of the non-respondents are unknown.
3.2 Descriptive characteristic of the cohorts
Disease distribution, disease duration, age and number of children were similar in the two cohorts. Months since the last childbirth were higher in the 2000 cohort (27.9 months vs. 22.8 months) and there was a difference in educational level with more women in 2020 cohort with higher education (Table 2).
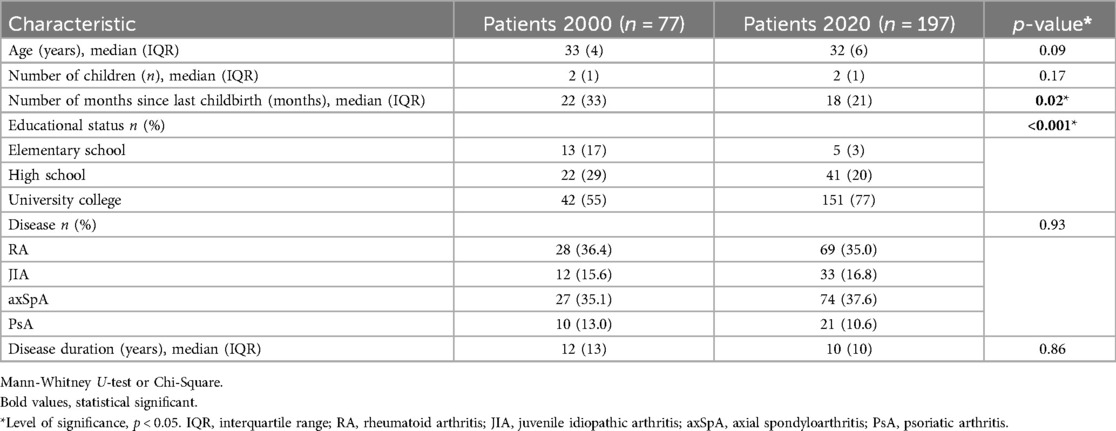
Table 2. Characteristics patient groups.
3.3 Comparison of HRQoL between the cohorts and with norm scores
The 2020 cohort had a significant higher score on the BP andPF scales compared to the 2000 cohort when adjusting for possible confounders. There was no significant difference between the two cohorts in the MH, VT, GH, SF, RP and RE scales (Table 3).
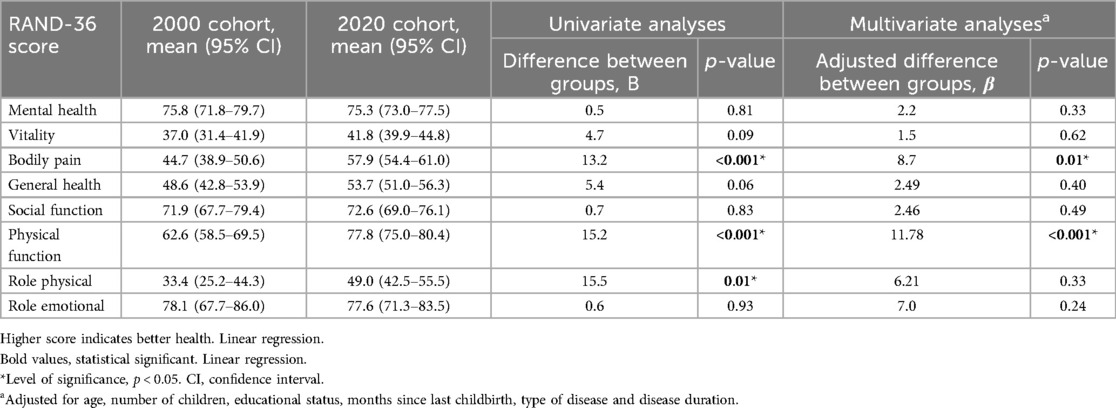
Table 3. Linear regression for the SF-36/RAND-36 scales by the two cohorts.
We performed univariable linear regression analysis on all eight domains on the possible confounding factors age, number of children, months since last childbirth, number of children, educational level, type of disease and disease duration. For all analysis, the only variable with a linear association in any eight domain was educational level with a linear association with all domains with a p value of < 0.05.
In the adjusted analyses the possible confounders; age, number of children, months since last childbirth, number of children, educational level, type of disease and disease duration were in the model. The p-value for the score “Role physical” changed from 0.01 to 0.33 after adjusting for confounders.
3.4 Comparison of HRQoL between 2020 cohort and norm scores
Compared to the calculated norm score, the 2020 cohort had significantly lower scores on all scales (p < 0.01) except the MH scale (p = 0.31). The mental health score of 75.3 is of particular interest as high score is described as “feels peaceful, happy and calm all of the time” (Table 4).
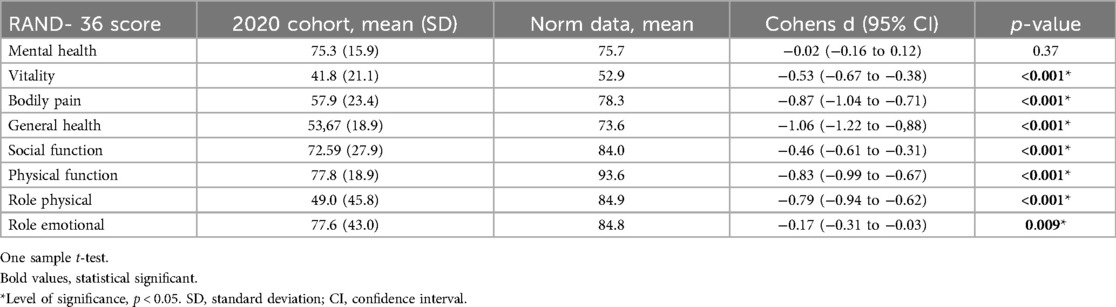
Table 4. Descriptive statistics for the RAND-36 (SF-36) for 2020 cohort compared to norm data.
3.5 Motherhood limitations
Table 1 present the distributions for the items hypothesized to measure motherhood limitations (LIM) and anxiety/distress (ANX) for the children. The scores are summarized making two sum scores; the mean score for LIM on a scale from 1 (No, not limited at all) to 3 (Yes, limited a lot) is 1.7 in the 2000 cohort and 1.5 the 2020 cohort. This might indicate that the mothers are limited to a certain extent. The mean score for ANX on a scale from 1 (No, none of the time) to 3 (Yes, often) is 1.94 in the 2000 cohort and 1.80 in the 2020 cohort indicating that the average of the women are anxious some of the time. There are significant differences in the items “participating in the child's/children's activities” and “looking after the child/children”, with less anxiety/distress in 2020 compared to 2000. In all other items, there are no significant difference between the two cohorts in a 20-year perspective.
4 Discussion
This is the first study to examine HRQoL in young mothers with IJD in a 20-year perspective.
Norwegian mothers with IJD were affected in most dimensions of HRQoL in the years 2000 and 2020, compared to Norwegian norm data, indicating that being a mother with IJD still has a pervasive negative effect on many domains of quality of life.
The demographic characteristics of the two cohorts were similar except for the difference in educational level and months since the last childbirth. As expected, more women in 2020 had obtained a higher educational level, as in accordance with the general population in a 20 year perspective (45). We also saw an association with educational level and all the eight scales, with higher education indicating better HRQoL. The difference in months since the last childbirth was 5 months, and the 2020 cohort had the youngest children (23 months vs. 28 months). However, it is unclear whether these 5 months make a clinical difference in perceived mothering. One study has revealed that women generally perceive mothering to be especially demanding during the child's first year of life (46), while another study described the ages from 1 to 2 years to be the most demanding on the mothers (47). Both cohorts had children aged 0–6 years and the mean number of children was not statistical different, assuming the “work load” to be similar between the groups.
4.1 Clinical issues
4.1.1 Physical health
The literature states that the impact of IJD on patients is profound and causes considerable morbidity (48–53). Despite continuous improvements in anti-rheumatic pharmacological treatment, people with IJD in general still report substantial disease impact (10, 52, 54, 55).
This study demonstrates that the domains that were most affected among the mothers were the role physical (RP), physical functioning (PF), bodily pain (BP) and general health (GH). These are the most valid measures of physical health problems in RAND-36 (SF-36), and they are also the most valid scales to distinguish between serious and minor medical conditions (56). These domains deal with problems with work or other daily activities as a result of physical health. It is not surprising that RP, PF, GH and BP were most affected if one considers the aspects and consequences of IJD such as pain, stiffness and joint destruction. The 2020 cohort experienced better HRQoL in the BP, PF and RP compared to the 2000 cohort indicating that the physical health has improved during the 20 years, but the mothers still have decreased HRQoL in these domains compared to matched norm data.
We also know that fibromyalgia (FM) is a chronic painful condition frequently associated with IJD and that women with FM have challenges in fulfilling maternal role (57). A systematic review found that concomitant FM is common in chronic inflammatory arthritis, with overall prevalence of FM to be 21% in RA, 13% in ax SpA and 18% in PsA (58). In some cases, IJD inflammation is controlled but the patients still report high levels of pain and associated symptoms (59, 60). Hence, interpreting HRQoL scores may be challenging in IJD with concomitant FM (61).
Problems with daily activities may also include problems with childcare. This may include practical problems of holding the child, especially whilst (breast)-feeding, dressing a baby when fasteners are small and fiddly, and trying to pin down a wriggly baby whilst changing nappies or securing it in a car seat. Our results are in accordance with a qualitative study (62) where the women described RA as a burden. The disease created additional complexity in their daily lives as mothers, due to the physical experiences of fatigue, pain, limited movement, and restrictions to the ability to lift or hold weight (62).
When the child becomes older and more active, there are fears for their safety. Most rheumatic conditions lead to periods of fatigue and general slowness that can make discipline and control more difficult than for fit mothers. Despite improvements in treating joint disease, the extra-articular burden in IJD remains substantial, encompassing multiple comorbidities and psychosocial impairments (8). A recent systematic review shows that more than half of patients with axSpA experience fatigue, with poorer quality of life being associated with more fatigue (63), and fatigue is a frequent symptom in RA (64), in PsA (65) and in JIA (66), with a prevalence up to 70% (67).
4.1.2 Mental health
The mental health (MH) score reported by the 2020 cohort was not significantly different from the norm data, and there were no significant differences between the 2000 and 2020 cohorts either. This is not in concordance with other studies of psychological distress often reported in IJD, where IJD and depression or poor mental health are described as common comorbid pathologies (55, 68–71) that all affect quality of life (72).
A high score of MH in RAND-36 (SF-36) is described as “feels peaceful, happy and calm all of the time”. Interestingly, this study shows that young mothers with IJD, with impairments in many aspects of life, maintain feelings of peacefulness, happiness and calmness. Many factors could account for this, such as the absence of psychiatric disorders, the presence of social supports, the relatively young age and response shift (73, 74) occurring with the management of a chronic disorder. When an individual come to terms with the fact of a long-term illness, adjustments occur that preserve life satisfaction. Thus, chronically ill persons can consider their quality of life as good even when there are severe limitations of their physical ability (73, 75). A previous study also found that personality traits have a considerable influence on how impactful/disrupting patients perceive their disease to be, with decisive consequences on their quality of life (76).
Despite the positive effects associated with motherhood in general, it may also have negative on mothers for mental health. A recent review demonstrates that mothers are at an increased risk for mental distress both during the postpartum period and in the years following postpartum, including an increased risk for depression in the years following childbirth (77). However, this study shows that the great majority of the rheumatic mothers have good mental health.
It has been found that maternal mental health is closely connected to the mother's social support system (78). One can assume that a young woman with a rheumatic disease carefully plans her pregnancy, and makes sure to have a good social support system. Previous studies have also shown that living with a spouse or partner seems to have a positive impact on mental health and life satisfaction (79).
Norway's parental leave policies are generous. Parents have up to 52 weeks of paid parental leave before and after delivery, with at least 15 of these weeks reserved for the father/co-parent. If a new mother is too ill to take care of her infant, the father/co-parent is entitled to take over her part of the leave (80). Universal perinatal programs are in place to safeguard the physical and mental health of the mother and child during pregnancy and after birth. All pregnant women are entitled to free maternity care from a midwife at a maternal and child health (MCH) center or from their general practitioner, and all costs related to delivery and hospital stay are covered. Within the first week postpartum, mothers receive a home visit by a midwife or a public health nurse (81). The MCH centers offer both individual and group-based support for families, addressing difficulties with the child, the parental role and interaction problems. An increasing number of MCH centers have access to psychologists, which has strengthened the implementation of early prevention and treatment efforts for perinatal mental disorders. The maternity and parental well fare system in Norway, might be one of the factors influencing why our finding of good mental health are not in concordance with international literature.
Even though the MH domain was not significantly different from the norm data, it is important to consider that two other domains (SF and RE) that correlate with the summary score for mental health in RAND 36 (SF36) were significantly lower in the patient cohorts than in the norm data. However, these domains also contain elements of physical character (accomplished less, and time spent on social activities) that might be influenced by physical limitations due to the disease.
4.1.3 Experienced limitation and anxiety/distress
Between the two cohorts, the only statistically significant differences were found in experienced limitations in—“participating in the child/children's activities” and—“practical child care (i.e., changing nappies, dressing, bathing etc.)”, with more experienced limitations in 2000 than in 2020. This may reflect the trend in lesser physical limitations due to better medical treatment during the last 20 years.
All other items on experienced limitations and anxiety/distress were not different from 2000 to 2020, with both cohorts experiencing limitation in motherhood and anxiety/distress about the disease affecting their children. We know from other studies that not being able to fulfil their own and others' expectations of their role as a mother can make the women feel dissatisfied (82, 83). The women are concerned about their children and whether the children are experiencing distress, including “health anxiety”, due to witnessing their mother coping with IJD (62). A previous study also reported that women perform self-stigmatization in the form of self-blame and guilt when they cannot accomplish what they want in the mother role because of fatigue, pain, or physical limitations (23), and the women strive to be “good, nurturing mothers”, who are attentive to their children and do what they can to meet their needs (23).
4.1.4 Future recommendations for HRQoL research concerning mothers with IJD
Satisfactory quality of life despite having a rheumatic disease is one of the aims in rheumatology care (2, 84). This implies that explorative research regarding different aspects of quality of life in young mothers with a rheumatic disease is important in the future. In practice, it is less important to know that mothers with IJD have lower mean quality of life scores than healthy controls. The most important question is: what interventions may lead to improved quality of life. Issues under study in rheumatic-related quality of life must therefore have relevance for the care of people with a rheumatic disease.
It would be interesting to explore the basis for the mental health of young mothers with a rheumatic disease. What makes the mental health score of the women in this study higher than in previous studies and research?
Recommendations from EULAR highlight that specific patient educational or self-management programs, at important life and disease course stages, is critical and support patients to make informed choices about how to manage their IJD and facilitate collaborative care (85, 86). It would be interesting to explore if use of person-centered care instruments (34, 35), with targeted patient educational or self-management programs in a rheumatology-led pregnancy clinic (87), would improve the information quality and promote more collaborative decision-making with regard to motherhood and healthcare choices. Since the 2020 cohort have reduced HRQoL in all scores associated with physical health, one can assume that increased improvement in medical care and individualized physical exercises programs could improve these physical aspects of HRQoL and therefore the overall HRqOL.
4.2 Strengths and limitations
The main strength of this study is its nationwide patient population and the comparative design, which make it possible to compare two cohorts in a 20 years life span.
A possible limitation is that several different IJD diagnoses are included. One might assume that the HRQoL and disease burden vary across diagnosis. However, Norwegian studies indicate that disease burden in RA, PsA and ax-SpA may be more similar than previously demonstrated (42, 88).
The generic indicator used in this study [RAND-36 (SF36)] does not cover specific aspects required for outcome assessment in patients with RA, JIA, axSpA and PsA. For example, finger function is an important aspect for the assessment of physical health in patients with RA, JIA and PsA, but is not captured by any of the 10 items in the RAND-36 (SF-36) physical functioning scale. Also, we do not have data on clinical disease activity scores nor comorbidity that might influence the HRQoL. Particularly, we know that FM comorbidity impacts overall self-perceived health status (58).
The norm data are matched for age and sex, but not for parity. The total fertility rate in Norway was 1.5 in 2020 (89) and our 2020 cohort had an average of 1.7 children.
5 Conclusion
The findings emphasize the importance of understanding the intrusiveness of being a mother with IJD despite the improved medical treatment options over the last 20 years. An understanding of the physical and psychological impact of being a mother with IJD combined with multidisciplinary person-centered care may be a useful goal.
Data availability statement
The datasets presented in this article are not readily available because the data cannot be shared publicly due to the requirements of the involved register holders and the general data protection regulation, to protect the privacy of individuals. Requests to access the datasets should be directed to Hege Koksvik,aGVnZS5rb2tzdmlrQHN0b2xhdi5ubw==.
Ethics statement
The studies involving humans were approved by Regional Committee for Medical and Health Research Ethics South/East Norway. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HK: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing, Data curation, Funding acquisition. IN: Conceptualization, Data curation, Project administration, Writing – original draft, Writing – review & editing, Methodology. BJ: Conceptualization, Data curation, Project administration, Writing – original draft, Writing – review & editing, Methodology. HB: Data curation, Project administration, Writing – original draft, Writing – review & editing. MW: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. KG: Conceptualization, Formal Analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Trondheim Rheumatism League and a research grant from St Olavs Hospital Trondheim University Hospital (reference number 19/11223-69). They were not involved in the collection, analysis, or interpretation of the data, nor the writing or submission for publication.
Acknowledgments
The authors would like to express our gratitude to the patients who responded to our questionnaire and we also thank the participating departments of rheumatology at the following hospitals for including patients in RevNatus: Betanien Hospital, Skien; Diakonhjemmet Hospital, Oslo; Haugesund hospital for rheumatic diseases (HSR), Haugesund; Haukeland University Hospital, Bergen; Førde Hospital, Førde; Ålesund hospital, Ålesund; Lillehammer Hospital for Rheumatic Diseases, Nordland Hospital Trust, Bodø; St. Olavs hospital Trondheim University Hospital, Trondheim; Sørlandet Hospital Trust, Kristiansand; University Hospital of North Norway, Tromsø; Vestre Viken Hospital Trust, Drammen; Østfold Hospital, Moss; The Helgeland Hospital Trust, Mo i Rana, Nord-Trøndelag Hospital Trust, Levanger.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Smolen JS, Landewé RBM, Bergstra SA, Kerschbaumer A, Sepriano A, Aletaha D, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. (2023) 82(1):3–18. doi: 10.1136/ard-2022-223356
2. Ramiro S, Nikiphorou E, Sepriano A, Ortolan A, Webers C, Baraliakos X, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. (2023) 82(1):19–34. doi: 10.1136/ard-2022-223296
3. Coates L, Gossec L. The updated GRAPPA and EULAR recommendations for the management of psoriatic arthritis: similarities and differences. Joint Bone Spine. (2023) 90(1):105469. doi: 10.1016/j.jbspin.2022.105469
4. Nikiphorou E, Santos EJF, Marques A, Böhm P, Bijlsma JW, Daien CI, et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann Rheum Dis. (2021) 80(10):1278–85. doi: 10.1136/annrheumdis-2021-220249
5. Navarro-Compán V, Sepriano A, El-Zorkany B, van der Heijde D. Axial spondyloarthritis. Ann Rheum Dis. (2021) 80(12):1511–21. doi: 10.1136/annrheumdis-2021-221035
6. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. (2016) 388(10055):2023–38. doi: 10.1016/S0140-6736(16)30173-8
7. Garner AJ, Saatchi R, Ward O, Hawley DP. Juvenile idiopathic arthritis: a review of novel diagnostic and monitoring technologies. Healthcare (Basel). (2021) 9(12):1683. doi: 10.3390/healthcare9121683
8. Cutolo M, Kitas GD, van Riel PL. Burden of disease in treated rheumatoid arthritis patients: going beyond the joint. Semin Arthritis Rheum. (2014) 43(4):479–88. doi: 10.1016/j.semarthrit.2013.08.004
9. Galloway J, Edwards J, Bhagat S, Parker B, Tan AL, Maxwell J, et al. Direct healthcare resource utilisation, health-related quality of life, and work productivity in patients with moderate rheumatoid arthritis: an observational study. BMC Musculoskelet Disord. (2021) 22(1):277. doi: 10.1186/s12891-021-04110-1
10. Ishida M, Kuroiwa Y, Yoshida E, Sato M, Krupa D, Henry N, et al. Residual symptoms and disease burden among patients with rheumatoid arthritis in remission or low disease activity: a systematic literature review. Mod Rheumatol. (2018) 28(5):789–99. doi: 10.1080/14397595.2017.1416940
11. Lubrano E, Massimo Perrotta F, Manara M, D’Angelo S, Addimanda O, Ramonda R, et al. Predictors of loss of remission and disease flares in patients with axial spondyloarthritis receiving antitumor necrosis factor treatment: a retrospective study. J Rheumatol. (2016) 43(8):1541–6. doi: 10.3899/jrheum.160363
12. Lubrano E, Scriffignano S, Perrotta FM. Residual disease activity and associated factors in psoriatic arthritis. J Rheumatol. (2020) 47(10):1490–5. doi: 10.3899/jrheum.190679
13. Lucasson F, Balanescu A, Kiltz U, Leung YY, Aydin SZ, Gaydukova I, et al. Residual patient-reported burden in 444 patients with psoriatic arthritis in remission or low disease: a cross-sectional analysis. Joint Bone Spine. (2022) 89(5):105372. doi: 10.1016/j.jbspin.2022.105372
14. Perrotta FM, De Socio A, Scriffignano S, Lubrano E. From clinical remission to residual disease activity in spondyloarthritis and its potential treatment implications. Expert Rev Clin Immunol. (2018) 14(3):207–13. doi: 10.1080/1744666X.2018.1429918
15. Perrotta FM, De Socio A, Scriffignano S, Lubrano E. Residual disease activity in rheumatoid arthritis patients treated with subcutaneous biologic drugs that achieved remission or low disease activity: a longitudinal observational study. Clin Rheumatol. (2018) 37(6):1449–55. doi: 10.1007/s10067-018-4038-x
16. Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med. (2001) 33(5):350–7. doi: 10.3109/07853890109002089
17. Hays RD, Sherbourne CD, Mazel RM. The RAND 36-item health survey 1.0. Health Econ. (1993) 2(3):217–27. doi: 10.1002/hec.4730020305
18. Andersen JR, Breivik K, Engelund IE, Iversen MM, Kirkeleit J, Norekvål TM, et al. Correlated physical and mental health composite scores for the RAND-36 and RAND-12 health surveys: can we keep them simple? Health Qual Life Outcomes. (2022) 20(1):89. doi: 10.1186/s12955-022-01992-0
19. Mitton DL, Treharne GJ, Hale ED, Williams RA, Kitas GD. The health and life experiences of mothers with rheumatoid arthritis: a phenomenological study. Musculoskeletal Care. (2007) 5(4):191–205. doi: 10.1002/msc.116
20. Phillips R, Pell B, Grant A, Bowen D, Sanders J, Taylor A, et al. Identifying the unmet information and support needs of women with autoimmune rheumatic diseases during pregnancy planning, pregnancy and early parenting: mixed-methods study. BMC Rheumatol. (2018) 2:21. doi: 10.1186/s41927-018-0029-4
21. Phillips R, Williams D, Bowen D, Morris D, Grant A, Pell B, et al. Reaching a consensus on research priorities for supporting women with autoimmune rheumatic diseases during pre-conception, pregnancy and early parenting: a nominal group technique exercise with lay and professional stakeholders. Wellcome Open Res. (2018) 3:75. doi: 10.12688/wellcomeopenres.14658.1
22. Ackerman IN, Jordan JE, Van Doornum S, Ricardo M, Briggs AM. Understanding the information needs of women with rheumatoid arthritis concerning pregnancy, post-natal care and early parenting: a mixed-methods study. BMC Musculoskelet Disord. (2015) 16:194. doi: 10.1186/s12891-015-0657-4
23. Feddersen H, Mechlenborg Kristiansen T, Tanggaard Andersen P, Hørslev-Petersen K, Primdahl J. Juggling identities of rheumatoid arthritis, motherhood and paid work—a grounded theory study. Disabil Rehabil. (2019) 41(13):1536–44. doi: 10.1080/09638288.2018.1433723
24. Parton C, Katz T, Ussher JM. “Normal” and “failing” mothers: women’s constructions of maternal subjectivity while living with multiple sclerosis. Health (London). (2019) 23(5):516–32. doi: 10.1177/1363459317739442
25. Backman CL, Smith Ldel F, Smith S, Montie PL, Suto M. Experiences of mothers living with inflammatory arthritis. Arthritis Rheum. (2007) 57(3):381–8. doi: 10.1002/art.22609
26. Barlow JH, Cullen LA, Foster NE, Harrison K, Wade M. Does arthritis influence perceived ability to fulfill a parenting role? Perceptions of mothers, fathers and grandparents. Patient Educ Couns. (1999) 37(2):141–51. doi: 10.1016/S0738-3991(98)00136-0
27. Katz PP, Pasch LA, Wong B. Development of an instrument to measure disability in parenting activity among women with rheumatoid arthritis. Arthritis Rheum. (2003) 48(4):935–43. doi: 10.1002/art.10990
28. Ehrmann Feldman D, Vinet É, Sylvestre MP, Hazel B, Duffy C, Bérard A, et al. Postpartum complications in new mothers with juvenile idiopathic arthritis: a population-based cohort study. Rheumatology (Oxford). (2017) 56(8):1378–85. doi: 10.1093/rheumatology/kex168
29. Koksvik HS. Health-related quality of life in mothers with a chronic inflammatory rheumatic disease (Thesis). Trondheim, Norway: NTNU (2001).
30. Meade T, Sharpe L, Hallab L, Aspanell D, Manolios N. Navigating motherhood choices in the context of rheumatoid arthritis: women’s stories. Musculoskeletal Care. (2013) 11(2):73–82. doi: 10.1002/msc.1031
31. Marinello D, Zucchi D, Palla I, Aguilera S, Galetti I, Holmner M, et al. Exploring patient’s experience and unmet needs on pregnancy and family planning in rare and complex connective tissue diseases: a narrative medicine approach. RMD Open. (2022) 8(2):e002643. doi: 10.1136/rmdopen-2022-002643
32. Feddersen H, Kristiansen TM, Andersen PT, Hørslev-Petersen K, Primdahl J. Construction of meaningful identities in the context of rheumatoid arthritis, motherhood and paid work: a meta-ethnography. J Clin Nurs. (2017) 26(23–24):4117–28. doi: 10.1111/jocn.13940
33. Williams D, Pell B, Grant A, Sanders J, Taylor A, Edwards A, et al. Identities of women who have an autoimmune rheumatic disease [ARD] during pregnancy planning, pregnancy and early parenting: a qualitative study. PLoS One. (2022) 17(11):e0263910. doi: 10.1371/journal.pone.0263910
34. Bala SV, Forslind K, Fridlund B, Samuelson K, Svensson B, Hagell P. Person-centred care in nurse-led outpatient rheumatology clinics: conceptualization and initial development of a measurement instrument. Musculoskeletal Care. (2018) 16(2):287–95. doi: 10.1002/msc.1233
35. Gasser F, Bala SV, Westergren A, Ekstrand J, Hagell P. Further development and evaluation of a questionnaire targeting person-centred outpatient care for persons with long-term conditions. J Patient Rep Outcomes. (2023) 7(1):85. doi: 10.1186/s41687-023-00623-6
36. World Health Organization. WHO global strategy on people-centred and integrated health services: interim report. Geneva: World Health Organization (2015). Available online at: https://iris.who.int/handle/10665/155002 (Accessed June 20, 2024).
37. Meissner Y, Strangfeld A, Costedoat-Chalumeau N, Förger F, Goll D, Molto A, et al. European network of pregnancy registers in rheumatology (EuNeP)—an overview of procedures and data collection. Arthritis Res Ther. (2019) 21(1):241. doi: 10.1186/s13075-019-2019-3
38. Jacobsen EL, Bye A, Aass N, Fosså SD, Grotmol KS, Kaasa S, et al. Norwegian reference values for the short-form health survey 36: development over time. Qual Life Res. (2018) 27(5):1201–12. doi: 10.1007/s11136-017-1684-4
39. de Wit M, Aouad K, Elhai M, Benavent D, Bertheussen H, Blackburn S, et al. EULAR recommendations for the involvement of patient research partners in rheumatology research: 2023 update. Ann Rheum Dis. (2024) 83(11):1443–53. doi: 10.1136/ard-2024-225566
40. Ware JE Jr, Gandek B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J Clin Epidemiol. (1998) 51(11):903–12. doi: 10.1016/S0895-4356(98)00081-X
41. Loge JH, Kaasa S, Hjermstad MJ, Kvien TK. Translation and performance of the Norwegian SF-36 health survey in patients with rheumatoid arthritis. I. Data quality, scaling assumptions, reliability, and construct validity. J Clin Epidemiol. (1998) 51(11):1069–76. doi: 10.1016/s0895-4356(98)00098-5
42. Michelsen B, Uhlig T, Sexton J, van der Heijde D, Hammer HB, Kristianslund EK, et al. Health-related quality of life in patients with psoriatic and rheumatoid arthritis: data from the prospective multicentre NOR-DMARD study compared with Norwegian general population controls. Ann Rheum Dis. (2018) 77(9):1290–4. doi: 10.1136/annrheumdis-2018-213286
43. Matcham F, Scott IC, Rayner L, Hotopf M, Kingsley GH, Norton S, et al. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis. Semin Arthritis Rheum. (2014) 44(2):123–30. doi: 10.1016/j.semarthrit.2014.05.001
44. Ware J, Snow K, Ma K, Bg G. SF36 Health Survey: Manual and Interpretation Guide. Lincoln, RI: Quality Metric, Inc, 1993 (1993). p. 30.
46. Small R, Astbury J, Brown S, Lumley J. Depression after childbirth. Does social context matter? Med J Aust. (1994) 161(8):473–7. doi: 10.5694/j.1326-5377.1994.tb127559.x
47. Olson AL, DiBrigida LA. Depressive symptoms and work role satisfaction in mothers of toddlers. Pediatrics. (1994) 94(3):363–7. doi: 10.1542/peds.94.3.363
48. Smolen JS, Aletaha D, Barton A, Burmester GR, Emery P, Firestein GS, et al. Rheumatoid arthritis. Nat Rev Dis Primers. (2018) 4:18001. doi: 10.1038/nrdp.2018.1
49. Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. (2017) 390(10089):73–84. doi: 10.1016/S0140-6736(16)31591-4
50. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic arthritis. N Engl J Med. (2017) 376(10):957–70. doi: 10.1056/NEJMra1505557
51. Giancane G, Consolaro A, Lanni S, Davì S, Schiappapietra B, Ravelli A. Juvenile idiopathic arthritis: diagnosis and treatment. Rheumatol Ther. (2016) 3(2):187–207. doi: 10.1007/s40744-016-0040-4
52. Garrido-Cumbrera M, Poddubnyy D, Sommerfleck F, Bundy C, Makri S, Correa-Fernández J, et al. International map of axial spondyloarthritis (IMAS): results from the perspective of 5557 patients from 27 countries around the globe. RMD Open. (2024) 10(2):e003504. doi: 10.1136/rmdopen-2023-003504
53. Figus FA, Piga M, Azzolin I, McConnell R, Iagnocco A. Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev. (2021) 20(4):102776. doi: 10.1016/j.autrev.2021.102776
54. Liu V, Fong W, Kwan YH, Leung YY. Residual disease burden in patients with axial spondyloarthritis and psoriatic arthritis despite low disease activity states in a multiethnic Asian population. J Rheumatol. (2021) 48(5):677–84. doi: 10.3899/jrheum.200934
55. Garrido-Cumbrera M, Navarro-Compán V, Poddubnyy D, Sommerfleck F, Makri S, Correa-Fernández J, et al. Factors associated with poor mental health in patients with axial spondyloarthritis: results from the international map of axial spondyloarthritis (IMAS). RMD Open. (2024) 10(2):e004218. doi: 10.1136/rmdopen-2024-004218
56. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-item short-form health survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. (1993) 31(3):247–63. doi: 10.1097/00005650-199303000-00006
57. Lo Monaco M, Alblooshi S, Mallaci Bocchio R, Natoli G, Landa ML, Corrao S. The lived experience of mothers living with fibromyalgia syndrome: a phenomenological inquiry. Musculoskeletal Care. (2024) 22(2):e1889. doi: 10.1002/msc.1889
58. Duffield SJ, Miller N, Zhao S, Goodson NJ. Concomitant fibromyalgia complicating chronic inflammatory arthritis: a systematic review and meta-analysis. Rheumatology (Oxford). (2018) 57(8):1453–60. doi: 10.1093/rheumatology/key112
59. Haliloglu S, Carlioglu A, Akdeniz D, Karaaslan Y, Kosar A. Fibromyalgia in patients with other rheumatic diseases: prevalence and relationship with disease activity. Rheumatol Int. (2014) 34(9):1275–80. doi: 10.1007/s00296-014-2972-8
60. Drouet J, López-Medina C, Granger B, Fautrel B, Landewe RBM, Molto A, et al. Disease activity and widespread pain are main contributors to patient-reported global health in axial spondyloarthritis: an analysis of 6064 patients. Rheumatol Int. (2024) 44(8):1455–68. doi: 10.1007/s00296-024-05576-7
61. Kancharla H, Jain S, Mishra S, Acharya N, Grover S, Dogra S, et al. Fibromyalgia influences health-related quality of life and disease activity in psoriatic arthritis. Rheumatol Int. (2022) 42(3):511–7. doi: 10.1007/s00296-021-04925-0
62. Parton C, Ussher JM, Perz J. Mothers’ experiences of wellbeing and coping while living with rheumatoid arthritis: a qualitative study. BMC Womens Health. (2022) 22(1):185. doi: 10.1186/s12905-022-01767-1
63. Tang H, Singh BSM, Fong W. Prevalence and factors associated with fatigue in patients with axial spondyloarthritis: a systematic review and meta-analysis. Rheumatol Adv Pract. (2023) 7(3):rkad084. doi: 10.1093/rap/rkad084
64. Holten K, Paulshus Sundlisater N, Lillegraven S, Sexton J, Nordberg LB, Moholt E, et al. Fatigue in patients with early rheumatoid arthritis undergoing treat-to-target therapy: predictors and response to treatment. Ann Rheum Dis. (2022) 81(3):344–50. doi: 10.1136/annrheumdis-2021-220750
65. Nymand L, Kristensen LE, Thomsen SF, Thyssen JP, Egeberg A. Characteristics and drivers of fatigue in patients with psoriasis and psoriatic arthritis: a cross sectional study. J Am Acad Dermatol. (2024) 91(1):57–63. doi: 10.1016/j.jaad.2024.02.026
66. Tharwat S, Nassar MK, Salem KM, Nassar MK. Extraarticular manifestations of juvenile idiopathic arthritis and their impact on health-related quality of life. Clin Rheumatol. (2024) 43(7):2295–305. doi: 10.1007/s10067-024-07008-0
67. Hewlett S, Chalder T, Choy E, Cramp F, Davis B, Dures E, et al. Fatigue in rheumatoid arthritis: time for a conceptual model. Rheumatology (Oxford). (2011) 50(6):1004–6. doi: 10.1093/rheumatology/keq282
68. Morf H, da Rocha Castelar-Pinheiro G, Vargas-Santos AB, Baerwald C, Seifert O. Impact of clinical and psychological factors associated with depression in patients with rheumatoid arthritis: comparative study between Germany and Brazil. Clin Rheumatol. (2021) 40(5):1779–87. doi: 10.1007/s10067-020-05470-0
69. Ionescu CE, Popescu CC, Agache M, Dinache G, Codreanu C. Depression in rheumatoid arthritis: prevalence and effects on disease activity. J Clin Med. (2024) 13(7):2058. doi: 10.3390/jcm13072058
70. Sautner J, Puchner R, Alkin A, Pieringer H. Depression: a common comorbidity in women with rheumatoid arthritis-results from an Austrian cross-sectional study. BMJ Open. (2020) 10(1):e033958. doi: 10.1136/bmjopen-2019-033958
71. Chimenti MS, Fonti GL, Conigliaro P, Triggianese P, Bianciardi E, Coviello M, et al. The burden of depressive disorders in musculoskeletal diseases: is there an association between mood and inflammation? Ann Gen Psychiatry. (2021) 20(1):1. doi: 10.1186/s12991-020-00322-2
72. Nerurkar L, Siebert S, McInnes IB, Cavanagh J. Rheumatoid arthritis and depression: an inflammatory perspective. Lancet Psychiatry. (2019) 6(2):164–73. doi: 10.1016/S2215-0366(18)30255-4
73. Ortega-Gómez E, Vicente-Galindo P, Martín-Rodero H, Galindo-Villardón P. Detection of response shift in health-related quality of life studies: a systematic review. Health Qual Life Outcomes. (2022) 20(1):20. doi: 10.1186/s12955-022-01926-w
74. Vanier A, Oort FJ, McClimans L, Ow N, Gulek BG, Böhnke JR, et al. Response shift in patient-reported outcomes: definition, theory, and a revised model. Qual Life Res. (2021) 30(12):3309–22. doi: 10.1007/s11136-021-02846-w
75. Sinclair VG, Blackburn DS. Adaptive coping with rheumatoid arthritis: the transforming nature of response shift. Chronic Illn. (2008) 4(3):219–30. doi: 10.1177/1742395308095356
76. Santos EJF, Duarte C, Ferreira RJO, Pinto AM, Geenen R, da silva JAP. Determinants of happiness and quality of life in patients with rheumatoid arthritis: a structural equation modelling approach. Ann Rheum Dis. (2018) 77(8):1118–24. doi: 10.1136/annrheumdis-2017-212934
77. Hunter TR, Chiew BA, McDonald S, Adhikari K. The prevalence of maternal depression and anxiety beyond 1 year postpartum: a systematic review. Matern Child Health J. (2024) 28(8):1283–307. doi: 10.1007/s10995-024-03930-6
78. Kay TL, Moulson MC, Vigod SN, Schoueri-Mychasiw N, Singla DR. The role of social support in perinatal mental health and psychosocial stimulation. Yale J Biol Med. (2024) 97(1):3–16. doi: 10.59249/WMGE9032
79. Evans A, Gray E, Reimondos A. Having a partner or living with a partner: differences in life satisfaction and mental health. Appl Res Qual Life. (2023) 18(5):2295–313. doi: 10.1007/s11482-023-10186-9
80. Høivik MS, Eberhard-Gran M, Wang CEA, Dørheim SK. Perinatal mental health around the world: priorities for research and service development in Norway. BJPsych Int. (2021) 18(4):102–5. doi: 10.1192/bji.2021.2
81. Helsedirektoratet BR. Nytt liv og Trygg Barseltid for Familien Nasjonal Faglig Retningslinje for Barselomsorgen. Oslo: Helsedirektoratet (2014).
82. Feldthusen C, Björk M, Forsblad-d’Elia H, Mannerkorpi K. Perception, consequences, communication, and strategies for handling fatigue in persons with rheumatoid arthritis of working age–a focus group study. Clin Rheumatol. (2013) 32(5):557–66. doi: 10.1007/s10067-012-2133-y
83. Kristiansen TM, Primdahl J, Antoft R, Hørslev-Petersen K. Everyday life with rheumatoid arthritis and implications for patient education and clinical practice: a focus group study. Musculoskeletal Care. (2012) 10(1):29–38. doi: 10.1002/msc.224
84. Smolen JS, Breedveld FC, Burmester GR, Bykerk V, Dougados M, Emery P, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. (2016) 75(1):3–15. doi: 10.1136/annrheumdis-2015-207524
85. Zangi HA, Ndosi M, Adams J, Andersen L, Bode C, Boström C, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. (2015) 74(6):954–62. doi: 10.1136/annrheumdis-2014-206807
86. Jones B, Bennett S, Larsson I, Zangi H, Boström C, Van der Elst K, et al. Disseminating and assessing implementation of the EULAR recommendations for patient education in inflammatory arthritis: a mixed-methods study with patients’ perspectives. RMD Open. (2022) 8(1):e002256. doi: 10.1136/rmdopen-2022-002256
87. Miedany YE, Palmer D. Rheumatology-led pregnancy clinic: patient-centred approach. Clin Rheumatol. (2021) 40(10):3875–82. doi: 10.1007/s10067-021-05690-y
88. Michelsen B, Fiane R, Diamantopoulos AP, Soldal DM, Hansen IJ, Sokka T, et al. A comparison of disease burden in rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis. PLoS One. (2015) 10(4):e0123582. doi: 10.1371/journal.pone.0123582
89. StatisticsNorway. Total Fertility Rate, Women, by Contents and Year. Oslo: Statistics Norway (2024). Available online at: https://www.ssb.no/en/statbank/table/04232/tableViewLayout1/ (updated 02.07.2024).
Keywords: motherhood, rheumatic diseases, arthritis, inflammatory joint disease, health related quality of life, women's health, RAND-36
Citation: Koksvik HS, Nilssen I, Jakobsen B, Bjørngaard H, Wallenius M and Grønning K (2025) Changes in health related quality of life in mothers with inflammatory joint disease from year 2000 to 2020 – a comparative cross-sectional study. Front. Glob. Womens Health 5:1458390. doi: 10.3389/fgwh.2024.1458390
Received: 2 July 2024; Accepted: 19 December 2024;
Published: 8 January 2025.
Edited by:
Angela Tincani, Rheumatology Unit ASST-Spedali Civili and University of Brescia, ItalyReviewed by:
Gloria Riitano, Sapienza University of Rome, ItalyRangi Kandane-Rathnayake, Monash University, Australia
Copyright: © 2025 Koksvik, Nilssen, Jakobsen, Bjørngaard, Wallenius and Grønning. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hege Svean Koksvik, aGVnZS5rb2tzdmlrQHN0b2xhdi5ubw==