 María González
María González Ana B. Rodríguez
Ana B. Rodríguez Cristina Carrasco
Cristina Carrasco- 1Grupo de investigación Neuroinmunofisiología y Crononutrición, Departamento de Fisiología, Universidad de Extremadura, Badajoz, Spain
- 2Obstetrics & Gynecology Clinics “Miriam Gine”, Badajoz, Spain
Introduction: Four years after the start of the pandemic, there is limited evidence on the impact of COVID-19 on the women's health regardless of their reproductive status.
Objective: The aim was to analyze the prevalence and associated factors of menstrual-related disturbances in formerly menstruating women following SARS-CoV-2 infection.
Study design: A retrospective observational study of adult women in Spain was conducted during the month of December 2021 using an online survey (N = 17,512). The present analysis includes a subpopulation of SARS-CoV-2-infected and formerly menstruating women (n = 72). The collected data included general characteristics, medical history, and specific information on COVID-19. Chi-square and Mann-Whitney U-tests were performed. Bivariate logistic regression analysis was then performed to investigate possible associations between the occurrence of menstrual-related disturbances after SARS-CoV-2 infection.
Results: 38.8% of participants experienced menstrual-related disturbances following COVID-19. Among these, unexpected vaginal bleeding (20.8%) was the most common event, followed by spotting (11.1%) ( Table 1). Other reported changes were in the length (shorter = 12.5%) and flow (heavier = 30.3%) of menstrual bleeding in comparison to their previous experience. Regression analysis revealed that being a perimenopausal woman [adjusted odds ratio (AOR) 4.721, CI 95%, 1.022–21.796, p = 0.047] and having a previous diagnosis of menorrhagia (AOR 5.824 CI 95%, 1.521–22.310, p = 0.010) were factors associated with the event.
Conclusion: These findings could help health professionals provide their patients with up-to-date scientific information to empower them to actively manage their reproductive health, especially in societies where menstrual health is still taboo.
1 Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been reported to trigger multisystem complications (1, 2). This is due to the ubiquitous expression of the membrane protein angiotensin-converting enzyme 2 (ACE2) (2, 3) and other co-receptors (4), for example in the ovaries, independent of age and ovarian reserve (5). ACE2 has a significant role in the different phases of the menstrual cycle through angiotensin-(1–7) (6, 7). Changes in this molecular pathway and other neuroendocrine axes due to COVID-19 may result in menstrual cycle irregularities (4, 8) as well as the corresponding immune response (8). Thus, it would be expected that SARS-CoV-2 could temporarily or even permanently impair female fertility. Unfortunately, our knowledge of the basic uterine and menstrual physiology is insufficient to understand more complex processes of this kind.
Previous studies have linked viral infections to changes in women's reproductive health (9–11). However, there are conflicting results regarding SARS-CoV-2 infection in menstruating women (12–14). In addition, the prevalence of menstrual-related disturbances following COVID-19 (MRD-COVID19) in formerly menstruating women (FMW)—that is, those who were not menstruating at the time of infection for various reasons−remains unknown. The medical term for this is “secondary amenorrhea”. It is characterized by missing three menstrual periods in a row or not having periods for at least 6 months after menstruating normally. Common causes include pregnancy, breastfeeding, menopause, the use of contraceptives, and gynecological conditions (15, 16), most of which are exclusion criteria in similar studies. For this reason, the aim was to analyze the health factors that might be associated with the occurrence of MRD-COVID19 in FMW at the time of infection.
2 Method
2.1 Experimental design
A retrospective observational study was conducted among adult Spanish women using an online survey (Microsoft Forms®, Microsoft Corporation, Washington, USA). The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of University of Extremadura (ref. 180/2021).
2.2 Recruitment, data collection and participants
The online survey was published in Spain in December 2021 through social networks, using the snowball method. Informed consent was only obtained from those who agreed to be contacted by the research group by email for additional data collection. A total of 17,512 women were recruited within 15 days, regardless of their menstrual status. These results describe a subgroup analysis (n = 72 FMW, Figure 1) of this larger study; thus, the inclusion criteria were women: (i) over 18 years of age, (ii) with secondary amenorrhea of any cause prior to COVID-19 diagnosis, and (iii) with a diagnosis of COVID-19 (positive PCR test). The research sample excluded women who were currently menstruating at the time of infection or had not been diagnosed with the disease. The minimum representative sample size of the total population of Spanish women of reproductive age (N = 8,431,595) was calculated, considering an estimated prevalence of secondary amenorrhea of 4.0% (17). The following parameters were considered: statistical power 80.0%, alpha = 0.5 and effect size 1. This resulted in a sample size of 60 formerly menstruating women.
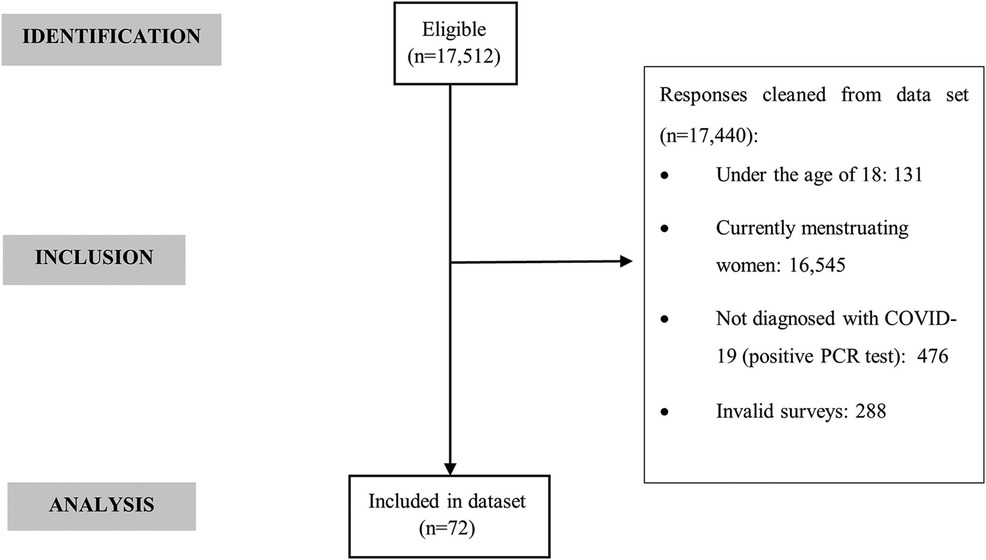
Figure 1. STROBE (strengthening the reporting of observational studies in epidemiology) flow diagram.
2.3 Survey information
A customized questionnaire was designed based on the survey conducted by Lee et al. (18) in April 2021. It consisted of 56 multiple-choice and text-entry questions divided into 6 sections. Participants were asked about (1) the general characteristics of their menstrual cycles—or its absence and the cause −, (2) SARS-CoV-2 infection, (3) COVID-19 vaccine, (4) menstrual experiences both after the SARS-CoV-2 infection and COVID-19 vaccination in comparison with the expected period symptoms−e.g., shorter/longer/same, heavier/lighter/same…−, (5) other menstrual changes−e.g., spotting, breast pain, hot flashes, premenstrual syndrome and abnormal bleeding −, (6) time between infection/vaccine and menstrual changes, (7) duration of the menstrual changes, (8) adverse events from each dose of the vaccine, (9) reproductive history, (10) medical history, and (11) demographics. The survey took 20–25 min to complete.
2.4 Statistical analysis
Participants were categorized according to the occurrence (MRD subgroup) or non-occurrence (n-MRD subgroup) of MRD-COVID19. Values were expressed as median and interquartile range, and as number of participants and frequency (%) for qualitative and quantitative variables, respectively. Chi-square and Mann-Whitney U-tests were performed. Bivariate logistic regression analysis was then performed. Results were presented as adjusted odds ratios (AORs) with 95% confidence intervals (CI). The above analyses were performed using the Statistical Package for Social Sciences (SPSS v.25, IBM, New York, USA) for Windows. Statistical significance was set at p ≤ 0.05.
3 Results
56.9% of the FMW [N = 72, median age 40.0 (33.0–51.8) years] had normal weight (median BMI value 24.0 (21.6–27.8), 19.4% had autoimmune diseases, and 27.1% had other clinical conditions. The most common cause of secondary amenorrhea in the study population was contraceptive use (31.9%), followed by postmenopause (22.2%). A total of 52.8% reported having been diagnosed with a gynecological disease, mainly menorrhagia (19.4%) (Supplementary Material S1).
38.8% of participants experienced MRD-COVID19. Among these, unexpected vaginal bleeding (20.8%) was the most common, followed by spotting (11.1%) (Table 1). Other reported changes were in the length (shorter = 12.5%) and flow (heavier = 30.3%) of menstrual bleeding in comparison to their previous experience. When asked about the time between the SARS-CoV-2 infection and the onset of menstrual bleeding, a 20.8% of the FMW answered “more than 14 days”; in 53.3% of cases, it was unexpected compared to the expected period date. Additionally, 27.8% reported that these symptoms had lasted “to date.”

Table 1. COVID-19 and the occurrence of MRD in the study population (formerly menstruating women, N = 72).
Comparative analysis (Table 2) showed significant differences between subgroups with respect to factors such as perimenopause, menorrhagia, and pandemic waves. Binary logistic regression (Table 3) confirmed that being a perimenopausal woman (AOR 4.721, CI 95%, 1.022–21.796, p = 0.047) and having a previous diagnosis of menorrhagia (AOR 5.824 CI 95%, 1.521–22.310, p = 0.010) were associated with MRD-COVID19 in FMW.
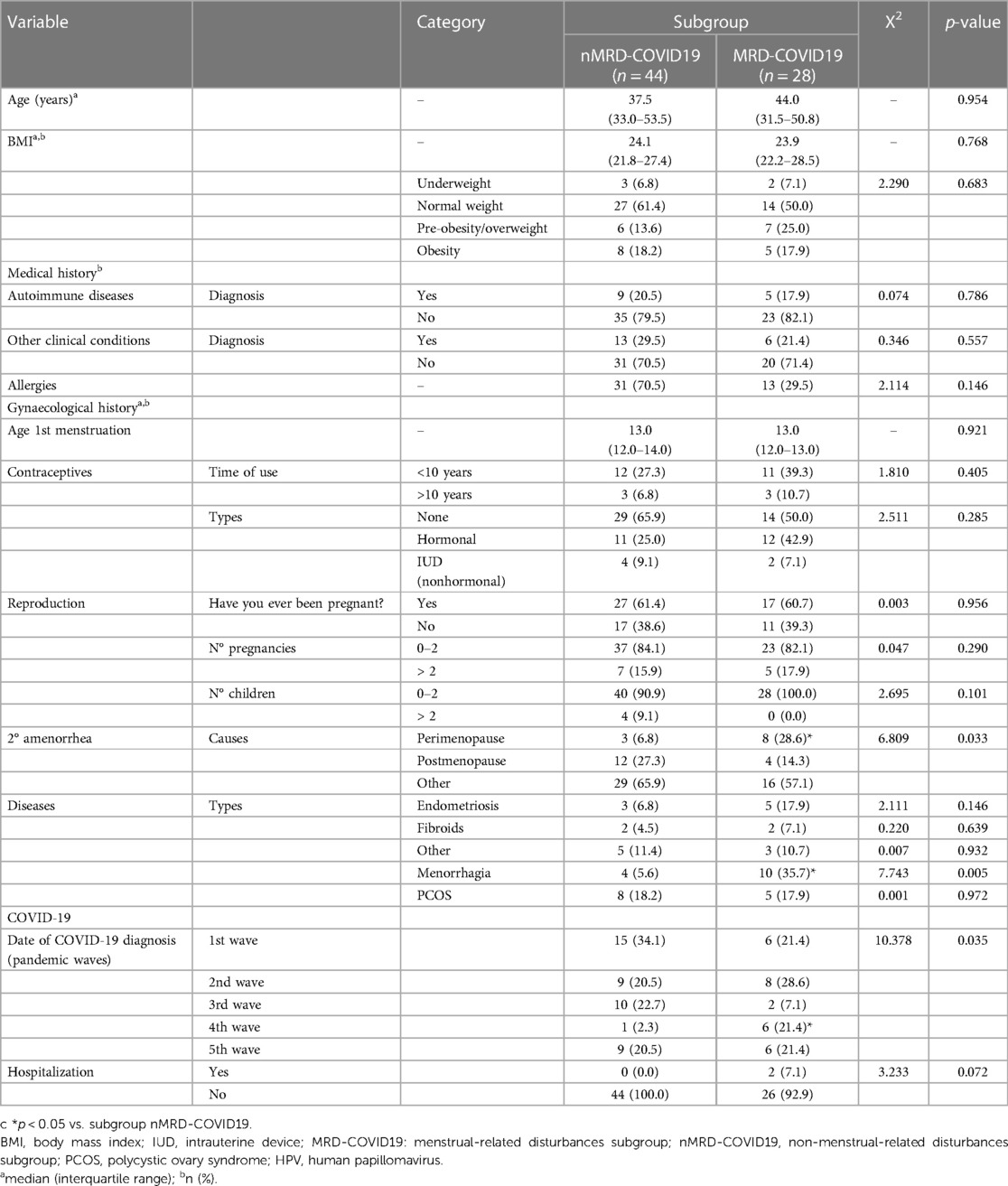
Table 2. Differences in the study variables according to the occurrence or not of MRD-COVID19 in the study population (formerly menstruating women, N = 72).

Table 3. Factors associated with the occurrence of nMRD-COVID19 (formerly menstruating women, N = 72): binary logistic regression.
4 Discussion
Although it is now well established that COVID-19 exhibits sex differences due to several biological factors, very few studies have analyzed the impact of this disease on the female reproductive system during the different stages of a woman's life. Based on the limited scientific evidence available, menstrual changes might affect 16%–25% of women of childbearing age infected with SARS-CoV-2 (12, 19, 20). The most commonly reported disturbances are worsened premenstrual syndrome, irregular and infrequent menstruation (20), and decreased menstrual volume (12, 19). In addition, other authors have reported a high prevalence of post-COVID-19 menstrual/period issues in women aged 30–60 years (21–23), including cycle length, menstrual flow and menses duration (23). One of the most notable findings of our study is that women who were not menstruating at the time of infection due mainly to contraceptive use or perimenopause/menopause, also experience unexpected menstrual cycle-related events, such as vaginal bleeding, spotting or changes in the length/flow of menstrual bleeding. Overall, this evidence suggests that there are differences in the prevalence and characteristics of the menstrual changes between young and middle-aged women. which need to be confirmed by further research. Indeed, the regression analysis showed that being a perimenopausal woman was a factor associated with MRD-COVID-19. Furthermore, it cannot exclude that some women may also experience long-term menstrual changes (12, 19, 21).
As Khan et al. (20) point out, the menstrual cycle involves complex interactions and can therefore be influenced by a variety of factors, including viral infections (9–11, 24). Therefore, potential direct and indirect effects of SARS-CoV-2 on the occurrence of menstrual changes need to be considered. Systemically, the damage is thought to be mediated by a direct viral role, pro-inflammatory immune responses, imbalances in physiological systems −e.g., the renin-angiotensin-aldosterone system and the ACE2/angiotensin-(1–7)/mitochondrial angiotensin axis, and the HPG and HPA axes −, and the downregulation of ACE2 expression (2, 25). This adverse context could be exacerbated by local direct effects in the female reproductive system with undefined consequences for menstrual physiology (13, 26). It should be noted that estrogens are well known to act in a coordinated manner with the immune system and metabolism (2, 18, 26). Estradiol has been suggested to play a protective role in COVID-19 through several pathways (26, 27). Therefore, the abnormal sex hormone secretion resulting from the SARS-CoV-2 infection may also alter the immune-neuro-endocrine network. However, the evidence remains inconclusive (12, 13). This raises the question of whether the prevalence and the characteristics of menstrual disturbances may be subject to the fluctuations in hormone levels at different stages not only of the menstrual cycle, but also of a woman's life. This assumption may also explain the reported differences in primary COVID-19 outcomes according to the menstrual status and contraceptive use (28, 29). Considering that perimenopause is a transitional phase mainly characterized by lower circulating levels of estradiol, it is suggested that the resulting dampened immune response, the downregulation of autophagy and the altered expression of ACE2 and other co-receptors such as transmembrane protease serine subtype 2, dipeptidyl peptidase-4 and furin (26, 27) may underlie the increased risk of experiencing this unexpected event. Conversely, high levels of estrogen, and consequently increased estrogen receptor signaling, may prevent further respiratory complications in SARS-CoV-2-infected pregnant women (29, 30). For this reason, estrogen supplementation has been proposed as a therapeutic approach to reduce the severity of the COVID-19 (30, 31). For Mateus et al. (32), not only estrogen, but sex hormones as a whole could justify the differences between sexes and age rates, which makes sense given the opposite effects of testosterone on immune response and virus clearance compared to estradiol (26, 27).
On the other hand, other concurrent factors in the prevalence of MRD-COVID19 in FMW should not be ignored, including comorbidity (12, 30). Severe acute illnesses can affect ACE2 levels (33) and HPG axis, leading to reduced levels of progesterone and estrogens (34). Surprisingly, the prevalence of autoimmune diseases or allergies did not differ between subgroups in our study. Only menorrhagia was associated with the MRD-COVID19; in this case, the imbalance between estrogens and progesterone levels may underlie this unexpected event (35, 36). Overall, it is worth considering whether the endocrine disorder observed in female COVID-19 patients is a consequence of systemic rather than local effects, such as nervous system injury (37) and pituitary dysfunction (13). However, there are conflicting results on SARS-CoV-2 neuroinvasion (37). Stress-associated, neuroendocrine-immune mechanisms should also be considered (18, 19, 22, 38), particularly during hospitalization (7), as well as genetics, socio-demographics, culture, and lifestyle factors (19, 21, 32, 39). Finally, the distinct levels of infectivity and transmissibility of the SARS-CoV-2 variants (40) could also have influenced this event. However, we could not prove this hypothesis and only found significant differences for the fourth wave in Spain (alpha variant or B.1.1.7).
This study is one of the few worldwide to focus on the impact of COVID-19 in FMW, demonstrating that women may experience menstrual-related disturbances regardless of their reproductive status at the time of SARS-CoV-2 infection. Some of the limitations include the small sample size, risk of recall bias or self-selection and the experimental design, as well as the lack of knowledge about the existence and importance of certain covariates −and the potential confounding effects −. In addition, the heterogeneity of the study population makes it difficult to fully understand the phenomenon due to the different nature of the underlying factors of secondary amenorrhea. However, we consider that this is a starting point for future research on the impact on viral infection in this subpopulation. Our findings here may not be applicable to other countries than Spain. A longitudinal and multinational study could help to establish the cause-effect relationship and to determine more precisely the factors associated with the occurrence of MRD-COVID19.
In conclusion, menstrual disturbances may be more likely to occur in perimenopausal FMW after COVID-19. The lack of knowledge about various aspects of women's health continues to lead to underestimation or direct ignorance of this phenomenon. These findings could help healthcare professionals to provide their patients with scientifically up-to-date information to enable them to make informed decisions about their reproductive choices.
Data availability statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to ethical restrictions.
Ethics statement
The studies involving humans were approved by Institutional Review Board of University of Extremadura (ref. 180/2021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MG: Investigation, Writing – original draft, Writing – review & editing. MA-A: Writing – review & editing, Conceptualization, Methodology. AR: Conceptualization, Methodology, Writing – review & editing, Supervision, Visualization. CC: Conceptualization, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the Regional Government of Extremadura-ERDF funds under Grant BBB021- GR21042; Cumlaude Lab under research agreement with the University of Extremadura (ref. 431/22). Neither the government agency nor the sponsoring company have played a role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Acknowledgments
The research team would like to thank all the participants who have collaborated in the study in an unselfish manner.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgwh.2024.1393765/full#supplementary-material
References
1. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. Kirtipal N, Kumar S, Dubey SK, Dwivedi VD, Gireesh Babu K, Malý P, et al. Understanding on the possible routes for SARS CoV-2 invasion via ACE2 in the host linked with multiple organs damage. Infect Genet Evol. (2022) 99:105254. doi: 10.1016/j.meegid.2022.105254
3. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579(7798):270–3. doi: 10.1038/s41586-020-2012-7
4. Bechmann N, Maccio U, Kotb R, Dweik RA, Cherfane M, Moch H, et al. COVID-19 Infections in gonads: consequences on fertility? Horm Metab Res. (2022) 54(8):549–55. doi: 10.1055/a-1891-6621
5. Wu M, Ma L, Xue L, Zhu Q, Zhou S, Dai J, et al. Co-expression of the SARS-CoV-2 entry molecules ACE2 and TMPRSS2 in human ovaries: identification of cell types and trends with age. Genomics. (2021) 113(6):3449–60. doi: 10.1016/j.ygeno.2021.08.012
6. Reis FM, Reis AM. Angiotensin-converting enzyme 2 (ACE2), angiotensin-(1–7) and Mas receptor in gonadal and reproductive functions. Clin Sci. (2020) 134:2929–41. doi: 10.1042/CS20200865
7. Carp-Veliscu A, Mehedintu C, Frincu F, Bratila E, Rasu S, Iordache I, et al. The effects of SARS-CoV-2 infection on female fertility: a review of the literature. Int J Environ Res Public Health. (2022) 19:984. doi: 10.3390/ijerph19020984
8. Male V. Menstrual changes after COVID-19 vaccination. Br Med J. (2021) 374:n2211. doi: 10.1136/bmj.n2211
9. Schoenbaum EE, Hartel D, Lo Y, Howard AA, Floris-Moore M, Arnsten JH, et al. HIV Infection, drug use, and onset of natural menopause. Clin Infect Dis. (2005) 41(10):1517–24. doi: 10.1086/497270
10. Giakoumelou S, Wheelhouse N, Cuschieri K, Entrican G, Howie SE, Horne AW. The role of infection in miscarriage. Hum Reprod Update. (2016) 22(1):116–33. doi: 10.1093/humupd/dmv041
11. Kurmanova AM, Kurmanova GM, Lokshin VN. Reproductive dysfunctions in viral hepatitis. Gynecol Endocrinol. (2016) 32(sup2):37–40. doi: 10.1080/09513590.2016.1232780
12. Li K, Chen G, Hou H, Liao Q, Chen J, Bai H, et al. Analysis of sex hormones and menstruation in COVID-19 women of child-bearing age. Reprod Biomed Online. (2021) 42(1):260–7. doi: 10.1016/j.rbmo.2020.09.020
13. Ding T, Wang T, Zhang J, Cui P, Chen Z, Zhou S, et al. Analysis of ovarian injury associated with COVID-19 disease in reproductive-aged women in Wuhan, China: an observational study. Front Med (Lausanne). (2021) 8:635255. doi: 10.3389/fmed.2021.635255
14. Wang M, Yang Q, Ren X, Hu J, Li Z, Long R, et al. Investigating the impact of asymptomatic or mild SARS-CoV-2 infection on female fertility and in vitro fertilization outcomes: a retrospective cohort study. EClinicalMedicine. (2021) 38:101013. doi: 10.1016/j.eclinm.2021.101013
15. Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), “Amenorrhea” (United States Government. (2021). Available online at: https://www.nichd.nih.gov/health/topics/amenorrhea (Accessed October 3, 2023).
16. Lord M, Sahni M. “Secondary Amenorrhea” in StatPearls. Treasure Island (FL): StatPearls Publishing (2022). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK431055
17. Sociedad Española de Ginecología y Obstetricia (SEGO). Estudio y tratamiento de las amenorreas hipotálamo-hipofisarias (2017) [study and treatment of hyo-pamo-pituitary amenorrhoea (2017)]. Prog Obstet Ginecol. (2017) (Ed. impr.) 60(5):495–504.
18. Lee KMN, Junkins EJ, Luo C, Fatima UA, Cox ML, Clancy KBH. Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. Sci Adv. (2022) 8(28):eabm7201. doi: 10.1126/sciadv.abm7201
19. Amer AA, Amer SA, Alrufaidi KM, Abd-Elatif EE, Alafandi BZ, Yousif DA, et al. Menstrual changes after COVID-19 vaccination and/or SARS-CoV-2 infection and their demographic, mood, and lifestyle determinants in Arab women of childbearing age. Front Reprod Health. (2022) 4:927211. doi: 10.3389/frph.2022.927211
20. Khan SM, Shilen A, Heslin KM, Ishimwe P, Allen AM, Jacobs ET, et al. SARS-CoV-2 infection and subsequent changes in the menstrual cycle among participants in the Arizona CoVHORT study. Am J Obstet Gynecol. (2022) 226(2):270–3. doi: 10.1016/j.ajog.2021.09.016
21. Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re'em Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. (2021) 38:101019. doi: 10.1016/j.eclinm.2021.101019
22. Barabás K, Makkai B, Farkas N, Horváth HR, Nagy Z, Váradi K, et al. Influence of COVID-19 pandemic and vaccination on the menstrual cycle: a retrospective study in Hungary. Front Endocrinol (Lausanne). (2022) 13:974788. doi: 10.3389/fendo.2022.974788
23. Li J, Bai J, Xiang X, Guo Y, Yu H. Effect of COVID-19 on menstruation and lower reproductive tract health. Int J Womens Health. (2023) 15:1999–2013. doi: 10.2147/IJWH.S433516
24. Kallio ER, Helle H, Koskela E, Mappes T, Vapalahti O. Age-related effects of chronic hantavirus infection on female host fecundity. J Anim Ecol. (2015) 84:1264–72. doi: 10.1111/1365-2656.12387
25. Ni W, Yang X, Yang D, Bao J, Li R, Xiao Y, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care. (2020) 24(1):422. doi: 10.1186/s13054-020-03120-0
26. Ho JQ, Sepand MR, Bigdelou B, Shekarian T, Esfandyarpour R, Chauhan P, et al. The immune response to COVID-19: does sex matter? Immunology. (2022) 166(4):429–43. doi: 10.1111/imm.13487
27. Khan N. Possible protective role of 17β-estradiol against COVID-19. J Allergy Infect Dis. (2020) 1(2):38–48. doi: 10.46439/allergy.1.010
28. Ding T, Zhang J, Wang T, Cui P, Chen Z, Jiang J, et al. Potential influence of menstrual Status and sex hormones on female severe acute respiratory syndrome coronavirus 2 infection: a cross-sectional multicenter study in Wuhan, China. Clin Infect Dis. (2021) 72(9):e240–8. doi: 10.1093/cid/ciaa1022
29. Costeira R, Lee KA, Murray B, Christiansen C, Castillo-Fernandez J, Ni Lochlainn M, et al. Estrogen and COVID-19 symptoms: associations in women from the COVID symptom study. PLoS One. (2021) 16(9):e0257051. doi: 10.1371/journal.pone.0257051
30. Seeland U, Coluzzi F, Simmaco M, Mura C, Bourne PE, Heiland M, et al. Evidence for treatment with estradiol for women with SARS-CoV-2 infection. BMC Med. (2020) 18(1):369. doi: 10.1186/s12916-020-01851-z
31. Suba Z. Prevention and therapy of COVID-19 via exogenous estrogen treatment for both male and female patients. J Pharm Sci. (2020) 23(1):75–85. doi: 10.18433/jpps31069
32. Mateus D, Sebastião AI, Carrascal MA, Carmo AD, Matos AM, Cruz MT. Crosstalk between estrogen, dendritic cells, and SARS-CoV-2 infection. Rev Med Virol. (2022) 32(3):e2290. doi: 10.1002/rmv.2290
33. Salamanna F, Maglio M, Landini MP, Fini M. Body localization of ACE-2: on the trail of the keyhole of SARS-CoV-2. Front Med (Lausanne. (2020) 7:594495. doi: 10.3389/fmed.2020.594495
34. Madjunkov M, Dviri M, Librach C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: a Canadian perspective. J Ovarian Res. (2020) 13(1):140. doi: 10.1186/s13048-020-00737-1
35. Sweet MG, Schmidt-Dalton TA, Weiss PM, Madsen KP. Evaluation and management of abnormal uterine bleeding in premenopausal women. Am Fam Physician. (2012) 85(1):35–43.22230306
36. Ray S, Ray A. Non-surgical interventions for treating heavy menstrual bleeding (menorrhagia) in women with bleeding disorders. Cochrane Database Syst Rev. (2016) 11(11):CD010338. doi: 10.1002/14651858.CD010338.pub3
37. Taga A, Lauria G. COVID-19 and the peripheral nervous system. A 2-year review from the pandemic to the vaccine era. J Peripher Nerv Syst. (2022) 27(1):4–30. doi: 10.1111/jns.12482
38. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. (2015) 40(4):219–21. doi: 10.1503/jpn.150205
39. Cherenack EM, Salazar AS, Nogueira NF, Raccamarich P, Rodriguez VJ, Mantero AM, et al. Infection with SARS-CoV-2 is associated with menstrual irregularities among women of reproductive age. PLoS One. (2022) 17(10):e0276131. doi: 10.1371/journal.pone.0276131
40. European Centre for Disease Prevention and Control (ECDPC). “SARS-CoV-2 variants of concern as of 15 June 2023”. (2023). Available online at: https://www.ecdc.europa.eu/en/covid-19/variants-concern (Accessed September 20, 2023).
Keywords: COVID-19, menstruation disturbances, amenorrhea, perimenopause, menorrhagia, women
Citation: González M, Al-Adib M, Rodríguez AB and Carrasco C (2024) COVID-19 and menstrual-related disturbances: a Spanish retrospective observational study in formerly menstruating women. Front. Glob. Womens Health 5: 1393765. doi: 10.3389/fgwh.2024.1393765
Received: 29 February 2024; Accepted: 16 July 2024;
Published: 30 July 2024.
Edited by:
Apurvakumar Pandya, Indian Institute of Public Health Gandhinagar (IIPHG), IndiaReviewed by:
Amirreza Keyvanfar, Shahid Beheshti University of Medical Sciences, IranGhadeer Khan, National Guard Hospital, Saudi Arabia
© 2024 González, Al-Adib, Rodríguez and Carrasco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Carrasco, Y2Nhcm9tQHVuZXguZXM=
†These authors have contributed equally to this work and share first authorship