 Marina Masih
Marina Masih Christopher Wagstaff
Christopher Wagstaff Harjinder Kaur-Aujla
Harjinder Kaur-Aujla- College of Medical and Dental Sciences, Institute of Clinical Sciences School of Nursing and Midwifery University of Birmingham Edgbaston, University of Birmingham, Birmingham, United Kingdom
Introduction: The purpose of this review is to systematically extract and analyse global academic literature to determine the physical and psychological effects of domestic abuse and violence on South Asian women.
Design: This review employs a qualitative systematic approach and thematic analysis to synthesize the narratives of affected women found in the literature. Given that domestic violence is often concealed and downplayed by various social factors, statistical reports and prevalence data offer only a limited view of the issue due to underreporting. Therefore, qualitative literature is deemed more dependable in this subjective domain as it captures and interprets the experiences and meanings within this under-studied group.
Data sources: Embase, PsycINFO, Google Scholar, Web Of Science, MEDLINE, and ASSIA were searched.
Review methods: All included studies were critically appraised using the CASP tool for qualitative research. Thematic analysis was conducted to develop six themes. Studies excluded did not address the research question, although intersecting population issues could be valuable topics for further research.
Results: The literature indicates severe mental and physical health consequences of domestic violence and abuse, with some traits persisting long-term. The analysis underscores the significant role of resilience, suggesting that individuals can overcome traumatic social experiences without enduring lifelong labels or a deficit model.
Conclusion: The findings provide support for future interventions aimed at recognizing signs of abuse and preventing severe psychological and physical consequences, particularly among South Asian women. Further research is needed to understand the impact on children and other family members affected by the victim's abuse, which falls beyond the scope of this review.
1 Introduction & background
Domestic violence and abuse encompass a range of coercive, threatening, controlling, degrading, and violent behaviours (1). Globally, intimate partner violence affects 641 million women and is the most common form of violence against women (2). In UK law and reports, the term is broadly recognized and includes various forms of abuse.
Demographically, the highest rates of Intimate Partner Violence (IPV) are recorded in South Asia, Sub-Saharan Africa, and Oceania, with prevalence rates between 33% and 51% among women aged 15–49 years (2). This study examines the impact of domestic violence on South Asian women, particularly in India, Pakistan, Bangladesh, Bhutan, Nepal, Afghanistan, the Maldives, and Sri Lanka (3). In South Asia, domestic violence remains a significant social issue, influenced by social, economic, and cultural factors that may normalize violence experiences (4). Research indicates that South Asian women are less likely to report violence due to the associated stigma, shame, fear of community isolation, and the importance placed on family reputation (5, 6). It is important to note that statistics do not capture unreported cases, making it challenging to assess the impact of these barriers on reporting behaviours. Therefore, this qualitative review will focus on the experiences of women who have participated in research, not those who remain undisclosed. The study also recognizes the distinct experiences of South Asian migrants and immigrants, acknowledging that both groups may have different experiences.
To summarize, the preliminary search for this review identified a single systematic review by Kalokhe et al. (7), which investigated the impact of domestic violence on physical and mental health. Focusing on 137 quantitative studies from India, it highlighted the need for a more extensive global search. The current review aims to compile and scrutinize all pertinent literature that describes the physical and psychological consequences of domestic abuse on South Asian women.
2 Methodology
2.1 Design
A qualitative systematic review of primary data was conducted to examine the physical and psychological effects of domestic violence and abuse on South Asian women. The aim was to comprehend the psychological and physical impacts through the lens of women's rich experiences. Consequently, a qualitative methodology was essential to foster understanding and provide insight into the researched situation, as the results are descriptive and interpretive (8). The review adhered to the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines, which enhance the transparency, completeness, and accuracy of systematic review reporting (9). This review exclusively concentrated on qualitative data, analysing women's experiences via interviews, and included pertinent mixed-method studies. In this case, quantitative data were omitted, focusing solely on the analysis of interviews detailing lived experiences.
2.2 Search methods
The key themes of the research question were identified using the PEO framework. This includes identifying the population (P), exposure (E), and outcome (O) (10). The following research question was formulated…
1) What are the psychological and physical effects (O) of domestic violence and abuse (E) on South Asian women (P)?
The same search terms were utilized across all databases, but the format was adjusted to meet each database's specific requirements. The search terms, being relevant to the question were constructed using the themes that were identified utilising the PEO framework, (as seen in Table 1 below). Medical Subject Headings (MeSH) were employed in databases like MEDLINE, supplemented by keyword searches. Truncation was used to capture multiple suffix variations of a key term (8). To prevent bias in the search results and ensure no relevant literature was overlooked, searches were conducted without any pre-set limits (11).
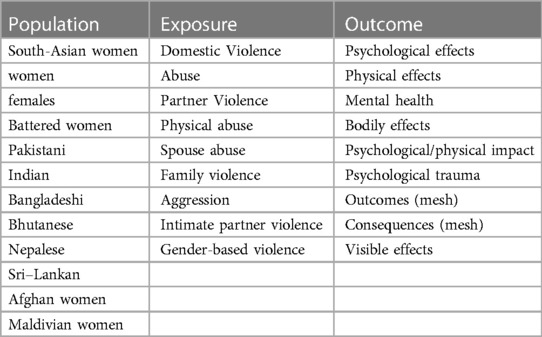
Table 1. The PEO framework and the search terms that were used to answer the question.
Beyond electronic database searches, additional strategies were employed to ensure a comprehensive literature review, following the recommendations of Cochrane (12) as well as Greenhalgh and Peacock (13). This included examining relevant journals at academic institutions and local libraries. A basic internet search with the search terms was also performed. Furthermore, the grey literature database OpenGrey (14) was explored using the keywords, but it yielded no pertinent literature, as noted by Bettany-Saltikov (10).
2.3 Screening
An online reference management website “Rayyan” was used to import the results of the screening searches. The exclusion and inclusion criteria (Table 2) were established before beginning the screening process. Once the results of the searches were uploaded, the titles and abstracts of the literature were examined, selecting those that met the predetermined inclusion criteria.
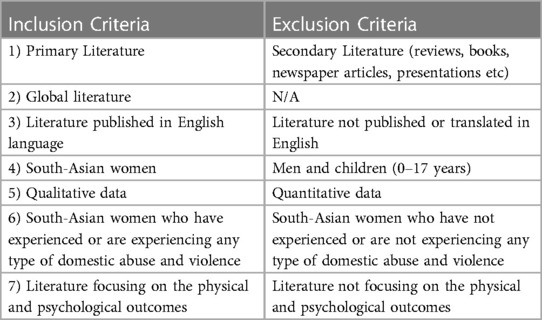
Table 2. A table showing the criteria established to assess the relevance of the literature and to maintain the focus of the review.
2.4 Critical appraisal
The quality appraisal was based on criteria from the Critical Appraisal Skills Programme (CASP) tools for qualitative, cross-sectional studies, and case-controlled studies.
2.5 Data abstraction
Data extracted from each of the studies followed guidance by Cochrane (15). This included author(s), date, and location of publication, aim(s), design and data collection, sample, data analysis, key findings, and limitations (15). This is shown in Table 3.
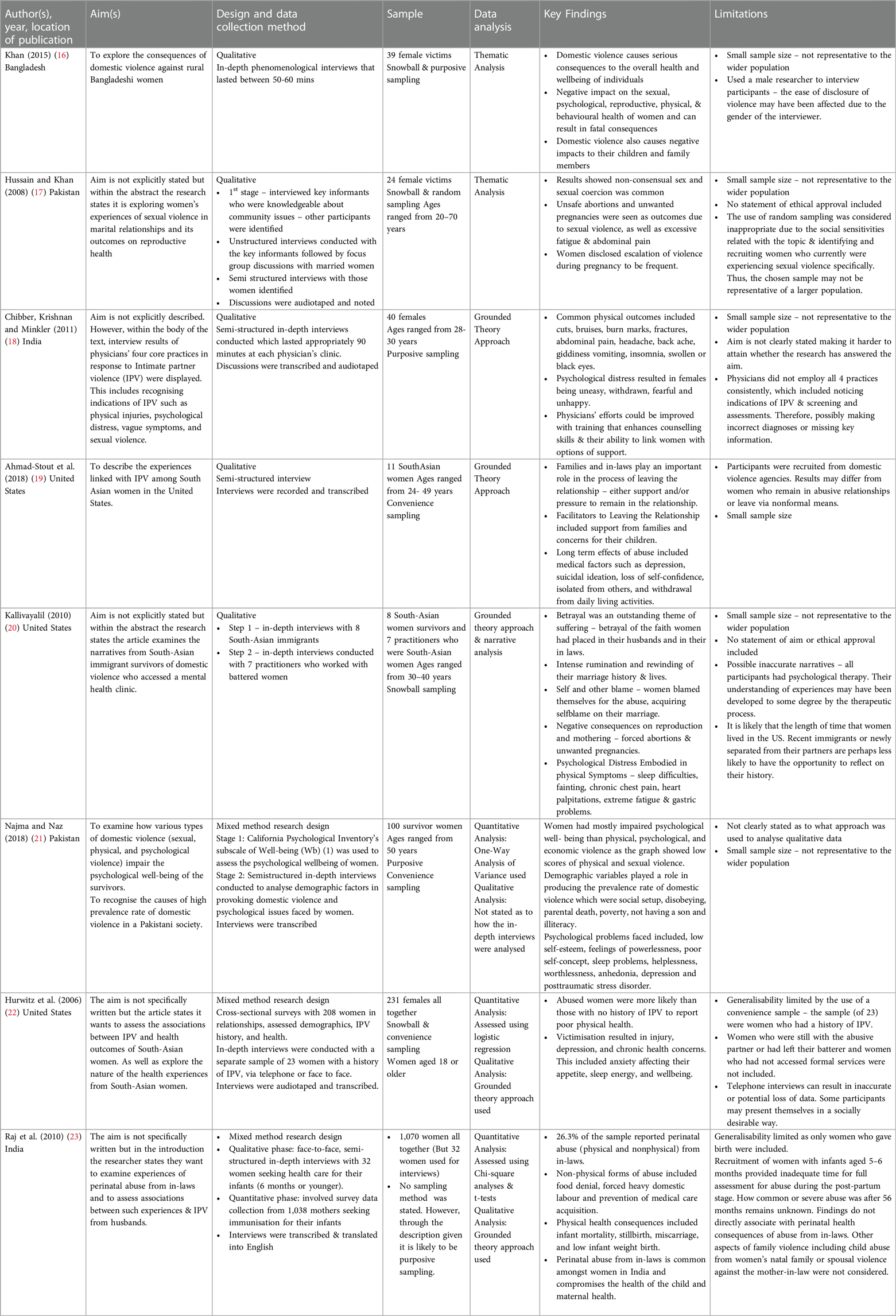
Table 3. Table showing an analysis of the appropriate data extracted from each article.
Following the process from Braun and Clark (24), an inductive approach was undertaken to analyse the data from the literature from where six themes were developed: visible injuries, reproductive health problems, temporary disabilities, psychosomatic symptoms, isolation, and withdrawal symptom and lastly, mental health disorders and suicidal ideation.
3.2 Critical appraisal of results
All studies included were appraised for quality, finding diversity in the quality of the articles. The results of the critical appraisal are displayed in Table 4. Out of eight studies, three explicitly stated receiving ethics committee approval or detailed the procedures to uphold ethical standards. Five studies did not mention ethical approval or participant confidentiality measures (17–20, 22). However, only Chibber et al. (18), Ahmad-Stout et al. (19), and Najma and Naz (21) clearly stated that they obtained consent. The publication dates of four studies (2006, 2008, 2010, and 2011) might reflect different publication guidelines from current standards, explaining the lack of explicit ethics statements. Additionally, the publication's location could influence the process of obtaining ethical approval, with low-income countries less likely to seek such approvals for health studies, as seen with Hussain and Khan (17) in Pakistan and Chibber et al. (18) in India (27). The need for ethical works for underserved communities is important and forefront of a good study.
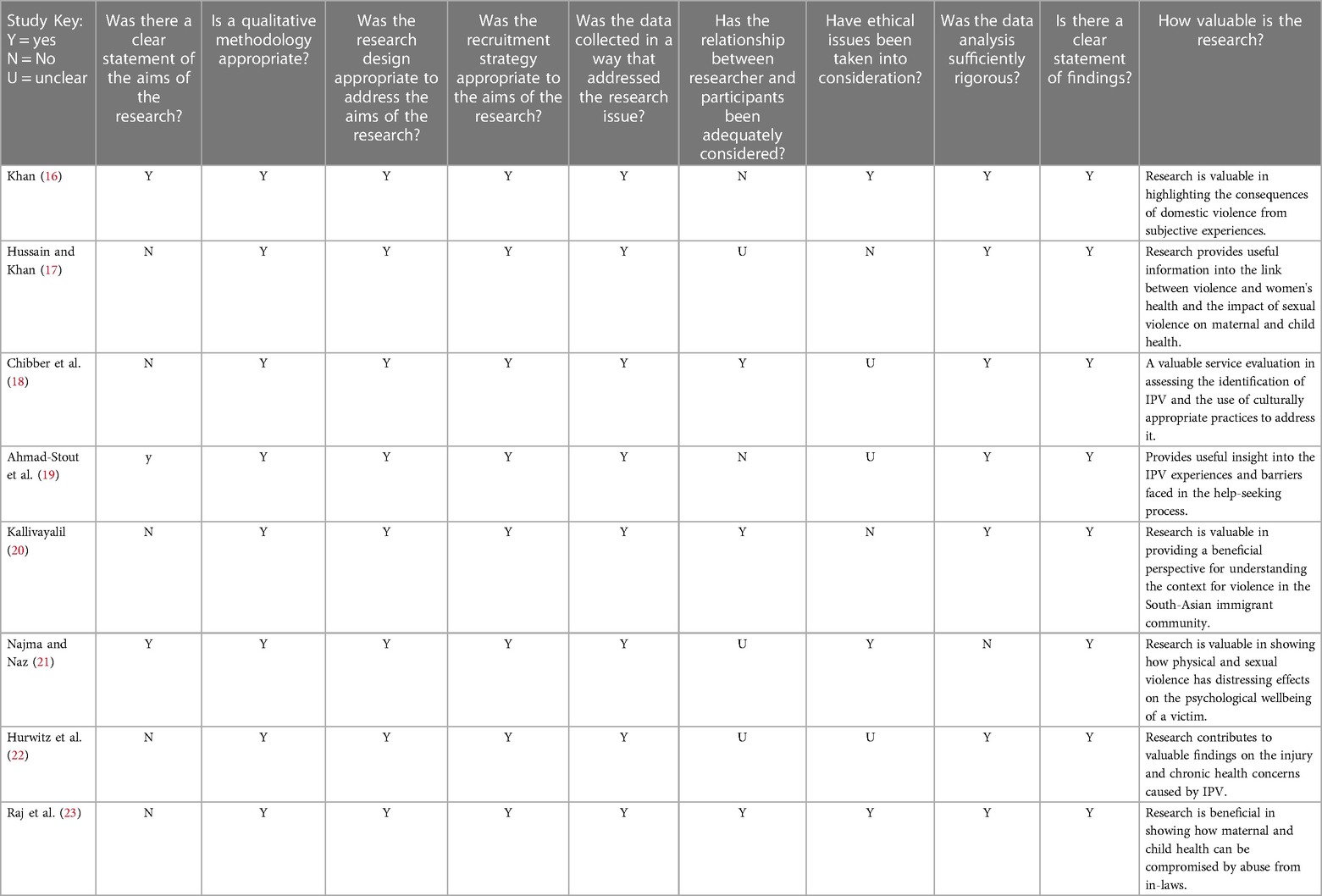
Table 4. A table showing all the studies utilised that were appraised for quality.
2.6 Data analysis
The six-step method by Braun and Clarke (24) gave the guidance for conducting a thematic analysis of the literature; this was selected due to its simplified and adapted method that helps in identifying themes within qualitative data (25). To reduce bias in the findings, an inductive technique was used to construct the themes from the literature based on the content of the data (24). This method recognised themes from the literature rather than predetermining them (26).
3 Findings
3.1 Summary of findings
A total of 374 results were retrieved from six online databases, with an additional two results manually added, bringing the total to 376. The breakdown of results from the databases is as follows: Embase (112), PsycINFO (12), Web of Science (75), Google Scholar (50), MEDLINE (108), and ASSIA (17). Due to the large number of results from Google Scholar, only the first 50 were considered. The software “Rayyan” facilitated the exportation of results, during which 126 duplicates were removed. Further exclusions were made based on title (59) and abstract (68). After applying the predetermined inclusion and exclusion criteria, eight studies were selected for detailed review (Figure 1).
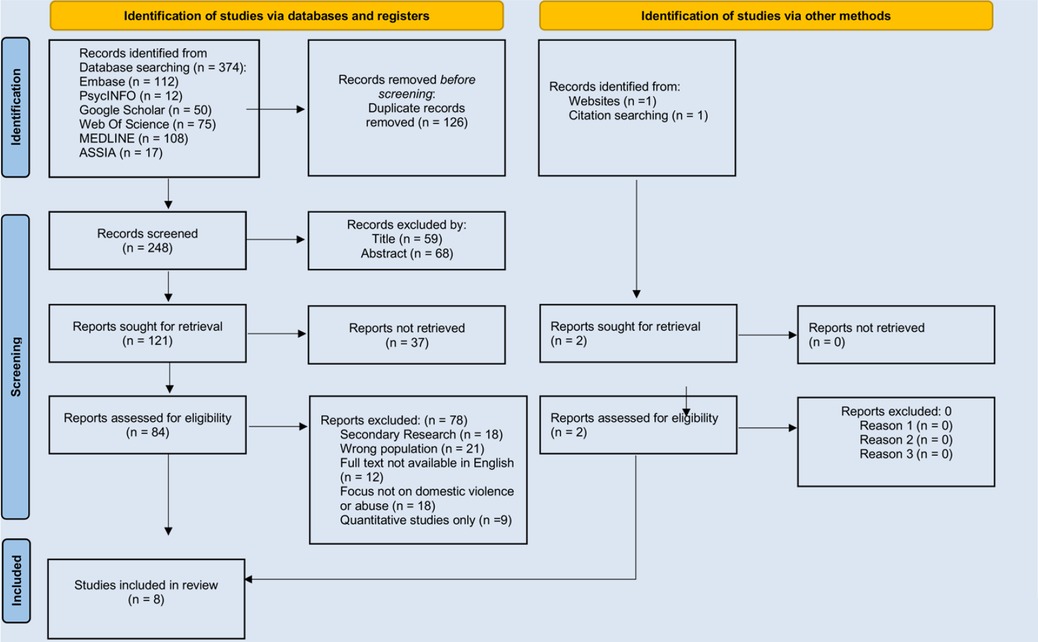
Figure 1 PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
The included studies were conducted across four different countries from 2006 to 2018. Although this provides a wider range of information universally, generalisability is still limited as most of the data is present from countries of a South Asian background, where the highest prevalence rates of intimate partner violence are identified (2).
A common issue across all studies was the small sample size of women interviewed. This not only limits the generalizability of the results but also heightens the risk of type I or type II errors (28). It also undermines the validity of the results, as small sample sizes are unlikely to yield reliable outcomes (29). Nonetheless, within the context of this review, a small sample size may be considered suitable as it allows qualitative researchers to engage closely with participants, facilitating in-depth data collection through interviews (30).
Snowball sampling was utilized in four studies (16, 17, 20, 22), which heightens the risk of uncontrollable bias. This is because key workers or participants might recommend others who share their perspectives or experiences of abuse, potentially leading to a non-representative sample of the population (29). Additionally, purposive sampling was employed in three studies (16, 18, 21), which compromises study reliability and introduces significant bias, as researchers handpick participants that they deem most suitable (31).
Methodological issues were identified regarding the relationship between the researcher and participants not being considered. Interviewing female participants could have been affected using a male interviewer in the study conducted by Khan (16). This could result in the ease of disclosure of violence being affected (32). The risk of data being overlooked, or inaccurate information being reported, results in internal validity being reduced.
Only one study (22) conducted telephone interviews, which might have compromised the validity and reliability of the results due to the inability to observe the participants’ body language or facial expressions, potentially leading to data loss and distortion (29). This limitation could impair the interviewer's capacity to detect emotions such as discomfort, anger, or sorrow. Moreover, the difficulty in establishing rapport over the phone may also impact the quality of the findings (33). However, the fact that all interviews across the studies were recorded and transcribed enhanced inter-rater reliability, as it allows multiple researchers to participate in the analysis (34).
No studies were excluded because they were all deemed valuable and recognised as decent quality in helping to answer the research question.
3.3 Themes
3.3.1 Physical
3.3.1.1 Visible injuries
From the studies included in the review, one of the common themes was that women often described their experiences of physical violence as a use of force against their bodies resulting in visible outcomes. These ranged from minor to severe injuries. The discussion of visible injuries was seen in four studies (16, 18, 20, 22). Visible injuries varied from minor cuts and scratches (30) to more serious injuries such as swollen or black eyes, burn marks and bruises (16, 20, 22).
Severe head injuries which resulted in serious long-term consequences of neurological damage were reported. For example, one participant commented: “he banged my head against a wooden pillar of the house. He did it several times. My skull hurt badly” [(16), p.214]. Additionally, another visible long-term consequence was reported by a participant who stated her husband punched her in the face, knocking her front teeth out (16). Some injuries reported were acknowledged as not so distinct due to facial injuries not endured by the victim. For example, one participant stated “he used to squeeze my thighs and leave marks’’ [(20), p.804]. Another participant reported that her husband hit her with a stick several times, targeting her breasts and leaving scars (16).
3.3.1.2 Reproductive health problems
A second theme that emerged from the interviews was that women suffered serious reproductive health problems resulting from domestic violence. Physical violence imposed by their partners was a dangerous experience for women during their pregnancy. The role of the mother-in-law in domestic violence is discussed in Kaur-Aujla (6), and evidence of extended family abuse is commonplace.
Miscarriages were associated with domestic violence in two studies (16, 23). A married 20-year-old participant discussed how her mother-in-law limiting her food intake during pregnancy resulted in a miscarriage: “I was without food for two and half days; then I ran from my in-laws' place. I just went to my sister place. After a week I felt feverish and at that time my bleeding (miscarriage) started” [(23), p.705]. Furthermore, another victim reported her husband kicking her abdomen and as a result, she experienced heavy bleeding and consequently suffered a miscarriage (16). Low infant birth weight was also identified and associated with reproductive health problems due to a victim's mother-in-law restricting her food intake (23).
Similarities were also noticed when victims reported unwanted forced pregnancies in three studies (16, 17, 20). One victim's husband did not like her using contraceptives and did not allow her to use any birth control methods: resulting in both her and her child suffering from chronic malnutrition (16). Hurwitz et al. (22) also documented malnutrition as a physical consequence. Hussain and Khan (17) found victims have difficulties in negotiating safe sex controlled by the husband which resulted in unwanted pregnancies, “My husband still wants to have more children and wants to keep on having unprotected sex” (p.474).
A widespread practice in dealing with unwanted pregnancies often led to the act of induced abortions as seen by Kallivayalil (16) and Chibber et al. (18). Evidentially, some victims had to terminate their pregnancies to contribute to the household income and continue working (18). Those that were unable to terminate their pregnancies gave birth to a stillborn baby. Even though the reason was unknown, she still blamed her husband; “He used to do that thing (sex) during the whole period of my pregnancy. I gave birth to a stillborn baby. I am sure it is the consequence of his activity” [(16), p.216].
3.3.1.3 Temporary disabilities
Health consequences that kept victims incapacitated or out of work for a while were discussed across four studies (Table 5). Demonstratable outcomes of physical violence included longer-lasting medical effects such as requiring surgery due to broken bones (19). In another study, physician associates noticed indications of IPV through observations of broken limbs and fractures in their assessments (18). Fractures were also noted from one victim from Khan (16) who reported her husband fractured her leg after attacking her with a piece of stone. Similarly, another victim disclosed her husband fractured her leg after hitting her with an iron rod. During the interview, the researcher recognised that she could not walk normally (16). However, as this statement was from the researcher and not the victim, it questions how accurate and truthful this statement was, due to the presence of only one observer. Thus, lacking in inter-rater reliability (34). Mobility issues were reported by Hurwitz et al. (22); “That day he hurt me too bad with the beer bottle, my ankle got hurt and I was not able to walk properly … There were times when I would go to class with the limping” (p.255). This statement supports and shows how such profound consequences are affecting everyday life for participants and the resilience that victims show in continuing their daily activities despite coping with injury.
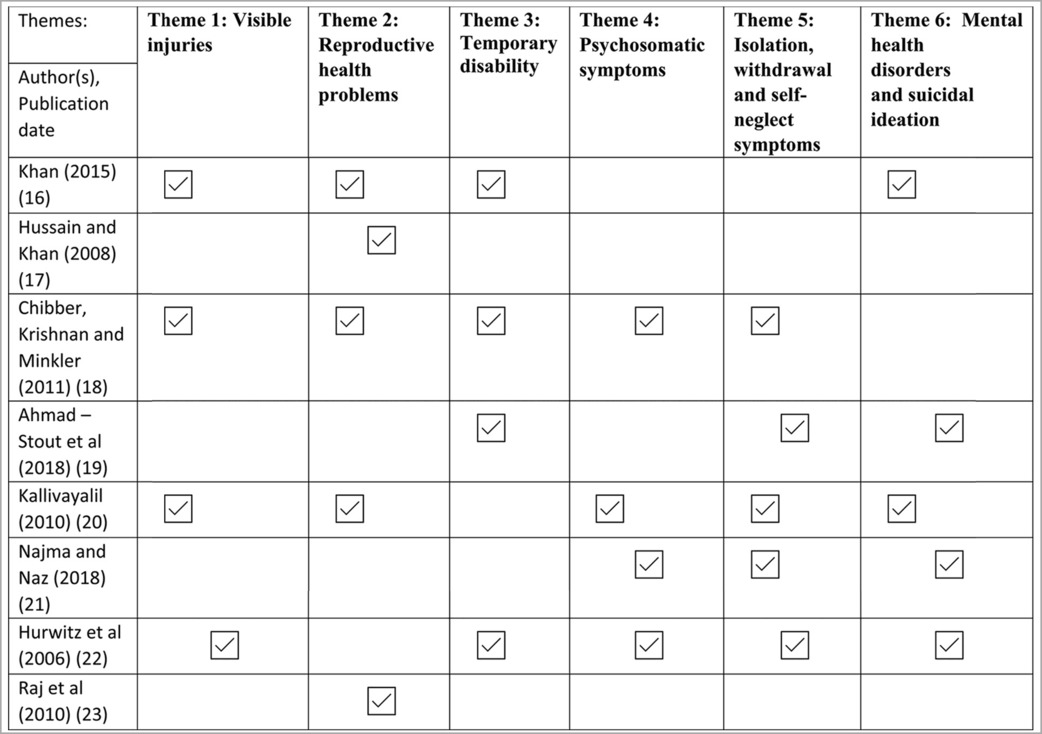
Table 5. A table showing how themes have been deduced and allocated through analysis.
3.3.2 Psychological
3.3.2.1 Psychosomatic symptoms
Psychosomatic symptoms refer to physical health problems such as sleep disturbances, fatigue, respiratory problems, headaches, back pains, stomach aches, or unexplained pains. These do not have a physical cause but may have an emotional or mental cause (35).
Body aches in different forms varied between victims and in reporting mechanisms (18, 20, 22). Severe headaches, back aches and general body aches were frequently reported due to physical stress. Victims seamlessly associated their suffering narratives on both psychological and physical dimensions as they made meaning of their abuse experiences (20).
Difficulties in sleeping were frequently seen in the literature. In the sample, women who were no longer with their abusers explained how they are haunted by nightmares recalling the abuse and consequently fearing bedtime, “ I still have the emotional stress. I mean, I even dream about the things that occurred with him when I was there… It is such a disturbed sleep now I do not want to go to bed” [(22), p.257]. Similarly, another participant stated, “I feel depressed, I cannot sleep” [(20), p.803]. The findings from Najma and Naz (21) demonstrate the major psychological problems faced by women after experiencing domestic violence included sleep problems, however, the article did not state the type of qualitative analysis conducted and thus no elements of interviews were included, resulting in no understanding of contextual data.
Women often recognised their physical expression of stress and directly associated the stress they were experiencing with the breakdown of their bodies. For example, heart palpitations, gastric problems and respiratory problems identified as psychosomatic symptoms were described by a participant; “Physically when you stress out too much, especially my body, I take everything inside me, I didn't share with no one. And finally, what happened, my stomach got upset and problems…. or I have a heart palpitation or something like my hands are blue, and I have breathing problem” [(20), p.805]. This statement highlights how unexplained pains can relate to the mental well-being of the patient. Psychological distress was embodied in physical symptoms, and this is particularly important when assessing this group in medical situations.
3.3.2.2 Isolation, withdrawal, and self-neglect symptoms
Isolation and withdrawal symptoms in the context of this theme are associated with symptoms of an already existing mental health condition, such as anxiety or depression. Individuals that are experiencing withdrawal or isolation will not participate in activities, they would usually enjoy being alone or with others (36). Indicators of isolation and withdrawal may include a change in appetite, lowered self-esteem, feeling helpless, lowered energy or motivation, recurring feelings of guilt, worthlessness, and self-loathing (37).
The loss of self-confidence was identified in two studies. Ahmad-Stout et al. (28) describe how a participant sample mentioned struggling with a reduced sense of confidence which they then associated with a feeling that they had lost a part of themselves. Female speakers explained how their lost capacity to enjoy life contributed to their impaired functioning: “(After the abuse) I started to lose my self-confidence and the, because earlier I used to be very bubbly, full of energy. But then I … I just lost everything …” [(22), p.257]. This statement also implies feelings of lowered energy and motivation.
Many victims also expressed feeling hopeless, helpless, and isolated from others even including their families of origin. “I was feeling … helpless and just like my life doesn't make sense” [(19), p.948]. Similarly, Najma and Naz (21) also found feelings of helplessness, worthlessness, and hopelessness to be emotions expressed by surviving women. Additionally, women who remained in the relationships were seen to display self-loathing behaviours; “At first (in the abusive relationship), I questioned my own sanity and wondered if there was something wrong with me. I felt very helpless’’ [(22), p.256]. However, these behaviours may have been induced because of the abuse and the perpetrator's gradual degradation of the victim.
Appetite and eating concerns were a recurring theme in the interviews shown in three studies (18, 20, 22). Isolation from family members often resulted in a change in eating behaviours as one woman described how she would cook for her children but not eat with them and preferred to sit in her room alone (20). Here, women described how the stress of abuse affected their appetite; “ I lost my appetite (in the abusive relationship). I mean I was not able to eat properly. I mean because the emotional stress maybe” [(22), p.257]. Similarly, loss of appetite was also reported by Chibber et al. (18).
Signs of psychological distress among women were noted as being uneasy, withdrawn, fearful or unhappy (18). Whereas Najma and Naz (21) highlighted key psychological issues faced by the survivors were anhedonia, poor self-concept, and low self-esteem, all of which were deemed appropriate to be categorised in this theme.
3.3.2.3 Mental health disorders and suicidal ideation
A range of mental health disorders stated by victims were commonly reported through the interviews. Examples of reported diagnoses seen throughout the literature included depression and post-traumatic stress disorder (PTSD) can be with or without suicidal ideation or attempts. Three studies investigated PTSD because of domestic abuse and violence (20–22). Women described mental health concerns once they had left the relationship, “ I have PTSD (posttraumatic stress disorder) … I've been losing some of my memory and I cannot pay attention to anything…” [(22), p.256]. Women in this sample had episodes of PTSD and found it challenging to fulfil their roles as mothers (20). The findings from Najma and Naz (21) also found PTSD to be a significant psychological problem faced by survivor women. However, again, the pathologisation of women in these circumstances must be acknowledged and rather, trauma informed responses are key. In that, there are women who have been great mothers to their children despite incurring abuse, battling with mental health, and these successes are less emphasised in medical works due to the “disease model”, Syme and Hagen (38).
The diagnosis of depression was stated in four studies. IPV was significantly associated with mental health resulting in impacting the general health of individuals, “My doctor says I am in depression. It does affect my health” [(22), p.256]. Depression was stated by Ahmad-Stout et al. (19) and Najma and Naz (21) through suicidal attempts and thoughts. One woman also discussed how her depression because of her abortion caused her to neglect her family, “I feel depressed, I cannot sleep, and I was negligent of the second child” [(20), p.803].
Three studies showed how women often discussed suicide attempts as they thought death appeared to be a better option than life; “one time I went to the river to commit suicide” [(22), p.256]. Another participant described, “I had a knife in my bathroom to slit myself” (19). Ideas of taking their own life remained in women's thoughts, “Often, I think so many people are dying every day so why not me?” [(16), p.216].
4 Discussion
This qualitative systematic review sought to gather and analyse relevant studies on the impact of domestic abuse and violence against South Asian women (39). Although the quality of research varied, consistent themes emerged across the studies. These included visible injuries, reproductive health issues, temporary disabilities, psychosomatic symptoms, isolation, withdrawal symptoms, and mental health disorders with suicidal ideation. Nevertheless, Kaur-Aujla et al. (6) recommend exercising caution when applying mental health labels and pathologizing women who are coping with challenging life situations.
Upon reviewing the methodologies of the studies examined, it was found that the studies relied on interviews to gather data. The validity of these studies has been challenged due to the reliance on self-reported data, which subjects the qualitative findings to recall bias and an increase in social desirability bias (40). There is a possibility that participants may have responded in a manner they believed the researcher desired, thus not providing an accurate representation of their true opinions and thoughts. However, social desirability is more likely to lead to the underreporting rather than overreporting of domestic violence (41). It is advisable for researchers to incorporate a social desirability scale in the development of their interviews to reduce the tendency of socially desirable responses, thereby controlling for social desirability bias in data analysis (42). Furthermore, as previously indicated in the introduction, evidence suggests that women from South Asian backgrounds are less inclined to report violence due to the associated stigma and shame, as well as the importance placed on family reputation (6, 43). This reluctance to disclose may also contribute to the questioned validity, as nondisclosure can lead to a lack of belief or validation, causing additional trauma and re-traumatization.
This review confirms that psychological repercussions of domestic abuse, such as mental health problems and psychosomatic symptoms, are important health consequences. However, cultural conflict in South Asian women is frequently blamed for the emergence of these effects (6, 44). The validity of reporting somatisation symptoms, as observed in interviews with South Asian women, is debated since somatisation is a prevalent concept among non-Western populations (45). Kirmayer and Young (46) suggest that enhanced psychological insight could lead to fewer reported somatic symptoms. Women in these interviews frequently associated their psychological distress with physical ailments. Burr (47) recommends that such interpretations be examined to address both symptom sets thoroughly. It is posited that a lack of mental health literacy exists in South Asian communities, prompting the need for medical practitioners to screen all women for domestic violence and abuse. Nonetheless, the analysis of various studies indicates that psychological symptoms, particularly depression and anxiety, were consistently reported.
Ali et al. (48) observed that depression in married women was linked to marital rape, domestic abuse by in-laws, early marriage, and lack of autonomy in marriage decisions. Marital rape, as noted in this review, is associated with reproductive health issues. In South Asian countries like Bangladesh, Maldives, India, and Sri Lanka, there are no laws criminalizing marital rape (49), indicating that women are unable to report their husbands for such acts due to the absence of legal provisions. This relates to the earlier point that intimate partner violence is the most common form of violence against women, with South Asian women experiencing the highest rates of such violence. The systematic review's primary findings corroborate these observations.
It was found that physical health concerns stem both directly from injury and indirectly from the stress of domestic violence. Chronic problems included backache, headache, and other body pain such as gastrointestinal problems. Women stated these issues started during the abuse in the relationship and continued even when they were no longer with their partner. Other researchers support this finding that physical health problems persist long-term, even after the abuse has ended (33, 50, 51). Even though these physical injuries reported were common amongst all studies, it relates to the notion as discussed above, whether these symptoms such as headaches were a result of somatisation. Questions asked to participants should be discussed in advance, so physical and psychological symptoms are addressed comprehensively.
The findings from this review have demonstrated substantial severe consequences on women's health. Sadly, society has contributed to escalating the incident rates of domestic violence through old traditions and norms and propaganda. These findings are in line with Grose and Grabe (52) findings, which showed that adopting a nonserious attitude toward domestic violence allowed society to enhance its severity. This connects to the introduction's discussion of the persistence of domestic violence and how societal and cultural factors can normalise violent experiences (4). Thus, re-iterating the idea that this nonserious attitude toward domestic violence within the South Asian community, viewing domestic violence as normal in a key factor in the continuation of the issue.
Factors such as poverty and autonomy among women have been seen to provoke the occurrence rate of domestic violence. One study found that the failure to fulfil the basic needs of a man towards his family creates tension and stress which is released through acts of violence against his family (53). These findings are also consistent with findings from Purvin (54), and Keenan et al. (55) who found that women in low-income families or marriages, who experienced domestic violence continuously stayed in that abusive relationships, just because of their dependency on their husbands in terms of money. Sarkar (56) discovered that a husband's final say on household autonomy was a risk factor. A wife's autonomy in managing her earnings and having joint autonomy in household decision-making were protective factors. Therefore, among the males who had grown up with parental abuse, perceptions of relationship rights and autonomy in this study suggested a belief system that enabled the justification for “beating” their wives (56). As mentioned in the introduction, economic factors were found to be a partial result of domestic violence being a persistent issue and thus as a result leads to South Asian women finding it difficult to leave their marriage in situations, albeit this is not a heterogenous group and more specific intergroup work in needed.
Suicidal ideation and attempts were identified as a common recurring theme throughout the literature. It was identified that married South Asian women were specifically more at risk of suicide attempts due to isolation from others, gender stereotyping, cultural conflict, and poor self-esteem. Consequently, a clear and positive correlation between domestic abuse and mental health can be identified (57). However, as congruent as the evidence is, the pathologisation of women because of Western diagnostic criteria is fraught with frustration (6). Therefore further research is required to explore the sociocultural needs of this homogenous group given the global geopolitical diaspora.
5 Strengths and limitations
This review's strength lies in its comprehensive search, which utilized various databases, extensive internet searches, and hand-searching of reference lists, thus identifying a broad spectrum of literature. A limitation of this review is the possibility of bias introduced during the initial stages by a novice researcher, although this was later checked by a more experienced researcher. To reduce bias, strategies like using an inductive approach for developing themes, instead of a pre-established one, were employed. Additionally, the language proficiency of the author led to the exclusion of non-English papers due to limited resources and lack of translations. This resulted in the omission of potentially relevant articles for South Asian women in languages such as Punjabi, Hindi, and Bengali.
This review is exclusively cantered on qualitative data. This approach is necessary because quantitative measures might not accurately capture the experiences of victims, although they can help researchers identify actions that contribute to understanding the various forms of violence (58). Quantitative methods for investigating domestic violence often present challenges and lack depth, as they are tied to contextual factors like cultural beliefs and practices (59).
6 Conclusion
This review was conducted to examine the psychological and physical impacts of domestic abuse and violence on South Asian women. It involved a systematic search, critical appraisal, and thematic analysis of studies relevant to the objective. The study is both crucial and timely, as domestic violence has been recognized as a rising global issue, particularly after the COVID-19 pandemic, which saw an increase in cases during lockdown periods.
In summary, six themes emerged: visible injuries, reproductive health issues, temporary disabilities, psychosomatic symptoms, isolation, and withdrawal symptoms, and finally, mental health disorders and suicidal thoughts. These themes contribute to understanding the experiences of these women, which can guide future interventions aimed at recognizing abuse and, hopefully, preventing its severe consequences.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MM: Writing – original draft. CW: Project administration, Writing – review & editing. HK-A: Investigation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgment
University of Birmingham, School of Nursing and Midwifery.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. NICE. Introduction | Domestic violence and abuse | Quality standards | NICE. Nice.org.uk. (2016). Available online at: https://www.nice.org.uk/guidance/qs116/chapter/introduction (Accessed May 2, 2024).
2. World Health Organization. Devastatingly pervasive: 1 in 3 women globally experience violence. www.who.int (2021). Available online at: https://www.who.int/news/item/09-03-2021-devastatingly-pervasive-1-in-3-womenglobally-experience-violence (Accessed May 2, 2024).
3. Britannica. South Asia | region, Asia. Encyclopaedia Britannica. (2024). Available online at: https://www.britannica.com/place/South-Asia (Accessed May 2, 2024).
4. Niaz U, Hassan S, Tariq Q. Situational analysis of intimate partner violence interventions in south Asian and middle eastern countries. Partner Abuse. (2017) 8(1):47–88. doi: 10.1891/1946-6560.8.1.47
5. Bhandari S, Sabri B. Patterns of abuse among south Asian women experiencing domestic violence in the United States. Int Soc Work. (2018) 63(1):2–3.
6. Kaur-Aujla H, Shain F, Lillie AK. A gap exposed what is known about sikh victims of domestic violence abuse (DVA) and their mental health? Eur J Mental Health. (2019) 14(1):179–89. doi: 10.5708/EJMH.14.2019.1.10
7. Kalokhe A, del Rio C, Dunkle K, Stephenson R, Metheny N, Paranjape A, et al. Domestic violence against women in India: a systematic review of a decade of quantitative studies. Glob Public Health. (2016) 12(4):498–513. doi: 10.1080/17441692.2015.1119293
8. Aveyard H. Doing a Literature Review in Health and Social Care: A Practical Guide. 4th ed S.L.: Open University Press (2019).
9. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 Explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. Br Med J. (2021) 372:n160. doi: 10.1136/bmj.n160
10. Bettany-Saltikov J. How to do a Systematic Literature Review in Nursing: A Step-by-Step Guide. Maidenhead, England: Open University Press (2012).
11. Cooper C, Booth A, Varley-Campbell J, Britten N, Garside R. Defining the process to literature searching in systematic reviews: a literature review of guidance and supporting studies. BMC Med Res Methodol. (2018) 18(1):7–9. Available online at: https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-018-0545-329321002
12. Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4: searching for and selecting studies. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). London: Cochrane (2021). Available online at: www.training.cochrane.org/handbook (Accessed May 2, 2024).
13. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ (Clinical Research ed). (2005) 331(7524):1064–5. doi: 10.1136/bmj.38636.593461.68
15. Li T, Higgins JPT, Deeks JJ. Chapter 5: collecting data. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). London: Cochrane (2021). Available online at: www.training.cochrane.org/handbook (Accessed May 2, 2024).
16. Khan AR. Consequences of domestic violence against women: some reflections from rural Bangladesh. Asian Soc Work Policy Rev. (2015) 9(3):210–23. doi: 10.1111/aswp.12059
17. Hussain R, Khan A. Women’s perceptions and experiences of sexual violence in marital relationships and its effect on reproductive health. Health Care Women Int. (2008) 29(5):468–83. doi: 10.1080/07399330801949541
18. Chibber KS, Krishnan S, Minkler M. Physician practices in response to intimate partner violence in Southern India: insights from a qualitative study. Women Health. (2011) 51(2):168–85. doi: 10.1080/03630242.2010.550993
19. Ahmad-Stout F, Nath SR, Khoury NM, Huang H. Experiences of intimate partner violence: findings from interviews with South Asian women in the United States. J Interpers Violence. (2018) 36(3-4):088626051775385. Available online at: https://journals.sagepub.com/doi/full/10.1177/0886260517753850#_i6
20. Kallivayalil D. Narratives of suffering of South Asian immigrant survivors of domestic violence. Violence Against Women. (2010) 16(7):789–811. doi: 10.1177/1077801210374209
21. Najma M, Naz S. Domestic violence and psychological well-being of survivor women in Punjab, Pakistan. J Psychol Clin Psychiatry. (2018) 9(2):187–8. doi: 10.15406/jpcpy.2018.09.00519
22. Hurwitz EJH, Gupta J, Liu R, Silverman JG, Raj A. Intimate partner violence associated with poor health outcomes in U.S. South Asian women. J Immigr Minor Health. (2006) 8(3):251–61. doi: 10.1007/s10903-006-9330-1
23. Raj A, Sabarwal S, Decker MR, Nair S, Jethva M, Krishnan S, et al. Abuse from in-laws during pregnancy and post-partum: qualitative and quantitative findings from low-income mothers of infants in Mumbai, India. Matern Child Health J. (2010) 15(6):700–12. doi: 10.1007/s10995-010-0651-2
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3(2):77–101. doi: 10.1191/1478088706qp063oa
25. Maguire M, Delahunt B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. AISHE-J. (2017) 9(3):3351.
26. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. (2017) 16(1):1–13. doi: 10.1177/1609406917733847
27. Teijlingen EV, Simkhada P. Failure to apply for ethical approval for health studies in low-income countries. Nepal J Epidemiol. (2015) 5(3):511–5. doi: 10.3126/nje.v5i3.13609
28. Akobeng AK. Understanding type I and type II errors, statistical power, and sample size. Acta Paediatr. (2016) 105(6):605–9. doi: 10.1111/apa.13384
30. Crouch M, McKenzie H. The logic of small samples in interview-based qualitative research. Soc Sci Info. (2006) 45(4):483–99. doi: 10.1177/0539018406069584
31. Robinson OC. Sampling in interview-based qualitative research: a theoretical and practical guide. Qual Res Psychol. (2014) 11(1):25–41. doi: 10.1080/14780887.2013.801543
32. Ellsberg M, Heise L, Pena R, Agurto S, Winkvist A. Researching domestic violence against women: methodological and ethical considerations. Stud Fam Plann. (2001) 32(1):1–16. doi: 10.1111/j.1728-4465.2001.00001.x
33. Campbell JC. Health consequences of intimate partner violence. Lancet. (2002) 359(9314):1331–6. doi: 10.1016/S0140-6736(02)08336-8
34. McAlister A, Lee D, Ehlert K, Kajfez R, Faber C, Kennedy M. Qualitative coding: an approach to assess inter-rater reliability. 2017 ASEE Annual Conference & Exposition Proceedings. (2017). p. 5–7. Available online at: https://www.researchgate.net/publication/323343316_Qualitative_Coding_An_Approach_to_Assess_Inter-Rater_Reliability
35. Ackerman K, Dimartini AF. Psychosomatic Medicine. Oxford, New York: Oxford University Press (2015). Available online at: https://ebookcentral.proquest.com/lib/bham/detail.action?docID=2012686
36. Kato TA, Kanba S, Teo AR. Defining pathological social withdrawal: proposed diagnostic criteria for hikikomori. World Psychiatry. (2020) 19(1):116–7. doi: 10.1002/wps.20705
37. HSR Psychology. Isolation and withdrawal—Conditions—HSR Psychology—Clinical and educational psychology service for children and young people, based in Manchester. www.hsrpsychology.co.uk (2021). Available online at: https://www.hsrpsychology.co.uk/conditions/mental-health/isolation-and-withdrawal/ (Accessed May 14, 2024).
38. Syme KL, Hagen EH. Mental health is biological health: why tackling “diseases of the mind” is an imperative for biological anthropology in the 21st century. Am J Phys Anthropol. (2020) 171:87–117. doi: 10.1002/ajpa.23965
39. Bramer WM, Rethlefsen ML, Kleijnen J, Franco OH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. (2017) 6(1):9–11. doi: 10.1186/s13643-017-0644-y
40. Visschers J, Jaspaert E, Vervaeke G. Social desirability in intimate partner violence and relationship satisfaction reports: an exploratory analysis. J Interpers Violence. (2015) 32(9):1401–20. doi: 10.1177/0886260515588922
41. Raj A, Silverman JG. Intimate partner violence against South Asian women in greater Boston. J Am Med Women’s Assoc. (2002) 57(2):111–4.
42. van de Mortel TF. Faking it: social desirability response bias in self-report research. Aust J Adv Nurs. (2008) 25(4):40–8. Available online at: https://search.informit.org/doi/abs/10.3316/INFORMIT.210155003844269
43. Mirza N. South Asian women’s experience of family abuse: the role of the husband’s mother (centre for research on families and relationships: briefing 80). Edinburgh: The University of Edinburgh (2016). p. 1–3. Available online at: https://www.era.lib.ed.ac.uk/bitstream/handle/1842/14199/CRFR%20briefing%2080.pdf?sequence=1&isAllowed=y (Accessed May 2, 2024).
44. Merrill J, Owens J. Ethnic differences in self-poisoning: a comparison of Asian and white groups. Br J Psychiatry. (1986) 148(6):708–12. doi: 10.1192/bjp.148.6.708
45. Isaac M, Janca A, Orley J. Somatization—a culture-bound or universal syndrome? J Mental Health. (1996) 5(3):219–22. doi: 10.1080/09638239650036884
46. Kirmayer LJ, Young A. Culture and somatization. Psychosom Med. (1998) 60(4):420–30. doi: 10.1097/00006842-199807000-00006
47. Burr J. Cultural stereotypes of women from South Asian communities: mental health care professionals’ explanations for patterns of suicide and depression. Soc Sci Med. (2002) 55(5):835–45. doi: 10.1016/S0277-9536(01)00220-9
48. Ali FA, Israr SM, Ali BS, Janjua NZ. Association of various reproductive rights, domestic violence, and marital rape with depression among Pakistani women. BMC Psychiatry. (2009) 9:77. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2791762/ doi: 10.1186/1471-244X-9-77
49. Oppenheim M. Sexual violence reports steadily surge in South Asia “with rape victims facing stigma.” The Independent. (2021). Available online at: https://www.independent.co.uk/asia/south-asia/sexual-violence-south-asia-rapeb1833944.html (Accessed May 14, 2024).
50. Koss MP, Koss PG, Woodruff WJ. Deleterious effects of criminal victimization on women’s health and medical utilization. Arch Intern Med. (1991) 151(2):342–7. doi: 10.1001/archinte.1991.00400020092019
51. Mouton CP, Rovi S, Furniss K, Lasser NL. The associations between health and domestic violence in older women: results of a pilot study. J Women Health Gend Based Med. (1999) 8(9):1173–9. doi: 10.1089/jwh.1.1999.8.1173
52. Grose RG, Grabe S. The explanatory role of relationship power and control in domestic violence against women in Nicaragua. Violence Against Women. (2014) 20(8):972–93. doi: 10.1177/1077801214546231
53. Slabbert I. Domestic violence and poverty. Res Soc Work Pract. (2016) 27(2):223–30. doi: 10.1177/1049731516662321
54. Purvin DM. At the crossroads and in the crosshairs: social welfare policy and low-income women’s vulnerability to domestic violence. Soc Probl. (2007) 54(2):188–210. doi: 10.1525/sp.2007.54.2.188
55. Keenan CK, El-Hadad A, Balian SA. Factors associated with domestic violence in low-income Lebanese families. Image J Nurs Sch. (1998) 30(4):357–62. doi: 10.1111/j.1547-5069.1998.tb01333.x
56. Sarkar NN. The cause and consequence of domestic violence on pregnant women in India. J Obstet Gynaecol. (2013) 33(3):250–3. doi: 10.3109/01443615.2012.747493
57. Bhugra D, Desai M. Attempted suicide in South Asian women. Adv Psychiatr Treat. (2002) 8(6):418–23. doi: 10.1192/apt.8.6.418
58. Gondolf EW, Beeman AK. Women’s accounts of domestic violence versus tactics-based outcome categories. Violence Against Women. (2003) 9(3):278–301. doi: 10.1177/1077801202250072
Keywords: mental health, sikh, South Asian, physical injury, physical health and mental illness
Citation: Masih M, Wagstaff C and Kaur-Aujla H (2024) The global psychological and physical effects of domestic abuse and violence on South Asian women: a qualitative systematic review. Front. Glob. Womens Health 5:1365883. doi: 10.3389/fgwh.2024.1365883
Received: 5 January 2024; Accepted: 6 June 2024;
Published: 9 July 2024.
Edited by:
Jayashri Kulkarni, Monash University, AustraliaReviewed by:
Neltjie Van Wyk, University of Pretoria, South AfricaRoelf Van Niekerk, Nelson Mandela University, South Africa
© 2024 Masih, Wagstaff and Kaur-Aujla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Harjinder Kaur-Aujla, aC5rYXVyLWF1amxhQGJoYW0uYWMudWs=