 Sereen Hawsawi1
Sereen Hawsawi1 Abeer Orabi
Abeer Orabi- 1Jeddah East Hospital, Jeddah, Saudi Arabia
- 2Nursing Department, College of Nursing, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia
- 3King Abdullah International Medical Research Center, Jeddah, Saudi Arabia
Introduction: Since the COVID-19 pandemic started, it has significantly impacted health systems and societies worldwide. Pregnancy increases the risk of severe illness when associated with COVID-19. Pregnant women are likely to experience COVID-19-related pregnancy complications however many of them were hesitant to receive the vaccine. This study aimed to assess the acceptance and hesitancy of COVID-19 vaccination among pregnant women in Jeddah.
Methods: The present study utilized a descriptive cross-sectional research design to include pregnant women through convenience sampling at the obstetrics and gynecology outpatient department and antenatal ward at King Abdul-Aziz Medical City, Jeddah. Data was collected from August to October 2022 using a structured questionnaire.
Results: Approximately one-third of the 264 participants (36.4%) strongly disagreed that they had developed immunity against COVID-19. More than half of them (61% and 66.3% respectively) had heard that the vaccine was unsafe for them and their babies during pregnancy, and it would contain the COVID-19 virus. However, half of them 50% agreed that vaccination would ease precautionary measures. A high acceptance score toward COVID-19 vaccination was observed among pregnant women working in the health sector. The most frequently reported reason for vaccination refusal was the belief that it was unsafe for the mother and her baby during pregnancy.
Discussion: Most of the participants perceived their susceptibility to COVID-19 infection as low and were hesitant to take the vaccine because of their worry about its effectiveness. However, they indicated a willingness to take the vaccine if it was mandatory and if they received adequate information about it. These findings correspond with previous studies conducted in Saudi Arabia that explore the reluctance of pregnant and breastfeeding women to receive COVID-19 vaccination.
1 Introduction
The COVID-19 pandemic was initiated by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and was first documented in Wuhan, China, at the end of 2019 (1). Globally, it has led to over 496 million cases and approximately 6 million deaths (2). In Saudi Arabia, up until 2022, the Ministry of Health reported a total of 752,078 confirmed COVID-19 cases and 9,060 deaths (3). It is important to note that pregnancy is a significant factor that increases the risk of severe illness when associated with COVID-19 infection (4). This heightened vulnerability can be attributed to transient immunosuppression and physiological changes in the respiratory and cardiovascular systems during pregnancy (5–8). A study in Saudi Arabia from March to October 2020 revealed a prevalence rate of 4.2% among pregnant women. Notably, 62% of these women were asymptomatic at diagnosis, and there was one reported death due to respiratory failure in this group (9).
Pregnant women are more likely to experience COVID-19-related pregnancy complications, such as preterm deliveries, neonatal intensive care unit admissions, and even mortality when infected with the virus (10). Several studies have demonstrated that pregnant women are highly susceptible to the SARS-CoV-2 virus, resulting in severe symptoms and worsened pregnancy outcomes (4, 11, 12). Furthermore, research from China and the United States has indicated a comparable risk of severity among pregnant patients when compared to the general population (13–15).
Symptoms of COVID-19 in pregnant women encompass fever, fatigue, dyspnea, and cough, with severity ranging from mild to severe instances, potentially progressing to acute respiratory distress syndrome, which can adversely affect the gastrointestinal, cardiovascular, and neurological systems, leading to multiple organ failures (16). Notably, Breslin et al. (14) reported two cases of maternal mortality, while Liu et al. (11) described several organ dysfunction syndromes, including acute respiratory distress syndrome resulting in fetal loss. Additional COVID-19-related pregnancy comorbidities include maternal hyperglycemia, hypertension, pneumonia, and venous thromboembolism (17, 18). Furthermore, there have been reports of increased intensive care unit admissions, mechanical ventilation, caesarean sections, intubations, miscarriages, preeclampsia, coagulopathy, and premature rupture of membranes among pregnant women infected with COVID-19 (19). Infant complications resulting from COVID-19 infection during pregnancy include prematurity, low birthweight, intrauterine transmission of infection, stillbirth, and fetal growth restriction (20–24).
In response to the negative consequences of the pandemic, governments have implemented preventive measures to curb the virus's spread. These measures encompass working from home, school closures, and the suspension of recreational and social activities. Preventive strategies such as hand washing, social distancing, and COVID-19 vaccination have been employed (25). The WHO has introduced The Global COVID-19 Vaccination Strategy to minimize deaths, reduce severe diseases, and mitigate the impact on healthcare systems, while facilitating the resumption of socioeconomic activities and reducing the risk of new variants. This is contingent on achieving widespread immunity by fully vaccinating at least 70% of the world's population, which includes most adults, adolescents, and individuals at risk for severe disease, including pregnant women (26). A study from Brazil highlighted the dynamics of COVID-19 vaccine uptake among pregnant women, showing an uptake rate of 53%. Factors influencing vaccine uptake included age, more antenatal care appointments, and a history of child loss (27).
Despite the recommendations of the Saudi Ministry of Health, which encouraged receiving COVID-19 vaccines as a preventive strategy for both males and females, including the elderly and pregnant women (3), many pregnant women have expressed vaccine hesitancy due to concerns about its safety during pregnancy and lactation. This hesitancy has hindered the vaccination strategy (10, 28). Factors influencing COVID-19 vaccine acceptance among pregnant women were being mandatory vaccination in many countries (29), to unclear information regarding the advantages, safety, and effectiveness of the vaccine, as well as fears of side effects for both the pregnant woman and her fetus, preference for other methods of COVID-19 prevention, and concerns that the vaccine could lead to COVID-19 infection (10, 30).
Nurses and midwives can play a significant role in preventing the spread of COVID-19 among pregnant women by assessing the factors contributing to vaccine hesitancy, outlining strategies to address these concerns, promoting preventive measures, and adhering to strict hygiene and isolation protocols in maternity wards. Additionally, they should provide comprehensive care to pregnant women infected with COVID-19, including monitoring vital signs, maintaining electrolyte balance, preventing dehydration, and offering psychological support (31, 32). Furthermore, they should engage in postnatal education and enlightenment programs (33).
In the Middle East, there is a paucity of studies concerning acceptance and hesitancy about COVID-19 vaccination among pregnant women, with most research focused on the adult general population and healthcare workers. However, a study conducted in Saudi Arabia focused on examining pregnant women's acceptance and hesitancy, revealing that pregnant women and those planning to become pregnant had a moderate score in terms of their perceptions of COVID-19 vaccination, reluctance, perceived benefits, and reasons for action (34). Previous studies have highlighted significant variations in COVID-19 vaccination acceptance rates and hesitancy among pregnant women in different countries. Therefore, it is essential to assess the hesitancy and acceptance of COVID-19 vaccines among pregnant women in Saudi Arabia to understand the factors influencing their decisions and design programs that empower women to make informed choices based on current scientific evidence. This approach will not only promote pandemic prevention but also enhance women's healthcare in general.
2 Materials and methods
2.1 Study design and setting
A descriptive cross-sectional design was employed in this study to assess the acceptance and hesitancy of COVID-19 vaccination among Saudi pregnant women. The study was conducted at the antenatal and gynecology ward (Ward 1), as well as the obstetrics and gynecology outpatient department (OPD), in King Abdulaziz Medical City, Western Region.
2.2 Sample and sampling
The study included 264 pregnant women equally recruited from the ward and the OPD, using convenience sampling. This nonprobability sampling method relies on readily available data sources. The inclusion criteria were Saudi women aged 18 years or older, who were able to read and write, and willing to participate in the study. The sample size was determined using G-Power online calculator, considering the average monthly admissions in the ward and the antenatal care visits at the outpatient department, with a confidence level of 95% and a margin of error of 5%.
2.3 Instrument and data collection
Data was collected from August to October 2022 using a self-administered structured questionnaire adapted from previous studies (34, 35). The questionnaire is divided into five sections. The first section gathers demographic characteristics like age, education, occupation, medical history, gestational age, number of pregnancies, children, previous COVID-19 infection, and vaccination status. The second section assesses perceptions of COVID-19’s severity and susceptibility, including personal experiences and perceived risk in Saudi Arabia. The third section explores hesitancy towards the COVID-19 vaccine, addressing concerns about safety, allergies, misinformation, and vaccine components. The fourth section delves into the perceived benefits of vaccination, such as easing precautionary measures and protecting against COVID-19 complications. The final section focuses on reasons for receiving the COVID-19 vaccine, including mandatory policies, public acceptance, and the need for adequate information. Each item was scored using a five-item Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly agree). The questionnaire was developed in English, then translated into simple Arabic using competent services then back-translated into English and revised accordingly to ensure that the intended meaning of the items is kept.
The validity of the questionnaire was confirmed by a panel of experts in the nursing and obstetrics fields who rated each item in terms of its relevance to the underlying construct and clarity. Then I-CVI and S-CVI/Ave were computed. To confirm the reliability of the questionnaire, the degree of error was assessed through pilot testing to make sure it was sufficiently comprehensive and well-structured. The reliability results through Cronbach's Alpha testing for Likert scales was (0.824) which was satisfactory. A pilot study was conducted by distributing the questionnaire to 53 pregnant women (20% of the sample size) who met the inclusion criteria to assess its completeness and applicability. No modifications were needed and collected data for piloting was not a part of the whole study.
2.4 Data analysis
The collected data was coded for entry and analyzed using statistical software (SPSS) version 28 for Windows. Descriptive statistics, such as frequencies, percentages, means, and standard deviations, were used to present the data. Inferential statistics, including ANOVA test and Pearson correlation, were employed to examine the association and significance of comparisons between study variables. A P-value of ≤0.05 was considered statistically significant.
2.5 Ethical consideration
The study was conducted with the approval of the Research Unit at the College of Nursing, King Abdullah International Medical Research Center, and the Institutional Review Board at King Abdulaziz Medical City-Western Region (IRB Approval No: IRB/1218/22). The researcher explained the study's aim and obtained informed consent from each participant; also, they were assured of the voluntary nature of their participation, with the right to discontinue or refuse to participate at any time. Confidentiality and privacy of responses were maintained.
3 Results
Among the 264 women surveyed with a response rate of 100%, equally recruited from the ward and the OPD, 45.1% were less than 30 years old, 43.6% had a high school education, and 65.2% were housewives. Results from the medical history data indicated that over half of the participants 56.1% had no pre-existing medical conditions, while 17.4% had diabetes mellitus. More than half of the participants were in their third trimester of pregnancy, and had 1–3 children 60.2% and 54.9%, respectively. Further, 68.2% of them had not experienced a previous COVID-19 infection (Table 1). Concerning COVID-19 vaccination, 41.7% of the participants had received two vaccine doses of those only 0.4% received during pregnancy while 6.8% had not been vaccinated (Figure 1).
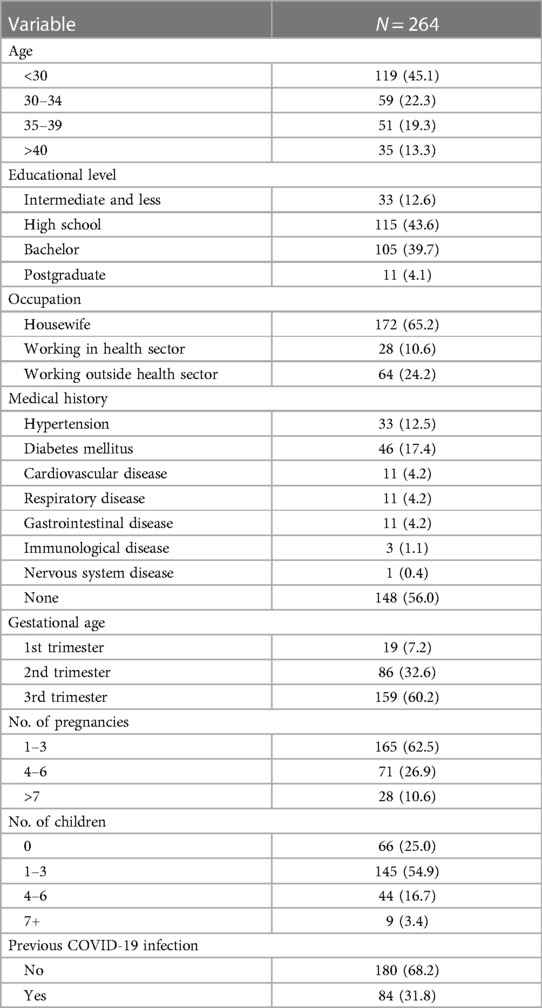
Table 1. Basic demographic characteristics of the participants.
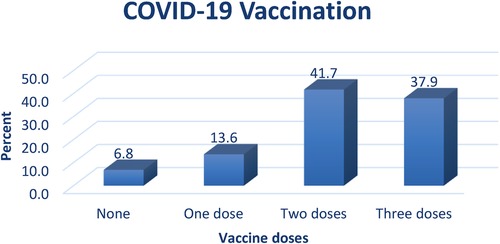
Figure 1. COVID-19 vaccination among the participants.
Regarding to perception of COVID-19 severity and susceptibility, more than one-third of the participants 36.4% strongly disagreed that they had developed immunity against COVID-19 infection. Additionally, 32.6% of them strongly disagreed that people they know had experienced a mild form of COVID-19, while 24.6% disagreed that the infection is not serious. On the other hand, almost half 48.9% of the participants agreed that the likelihood of contracting a COVID-19 infection is low in Saudi Arabia (Table 2).
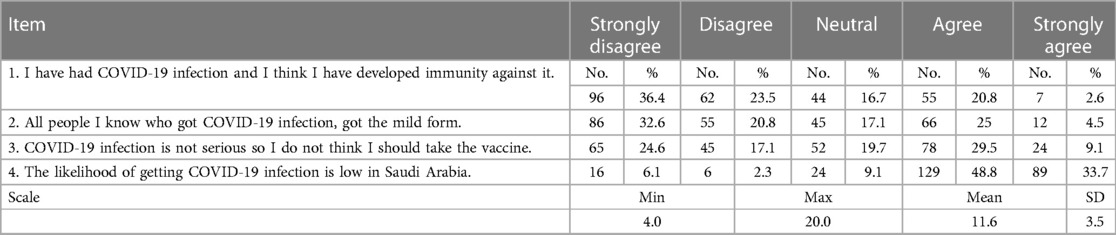
Table 2. Perception of COVID-19 severity and susceptibility among the participants.
Considering hesitancy to receive COVID-19 vaccination, more than half of the participants 61%, 61.7%, and 56.8%, respectively reported that they had heard that the vaccine is unsafe for them and their babies during pregnancy, blood clotting is a common side effect of the vaccine, and they were uncertain about its effectiveness during pregnancy (Table 3).
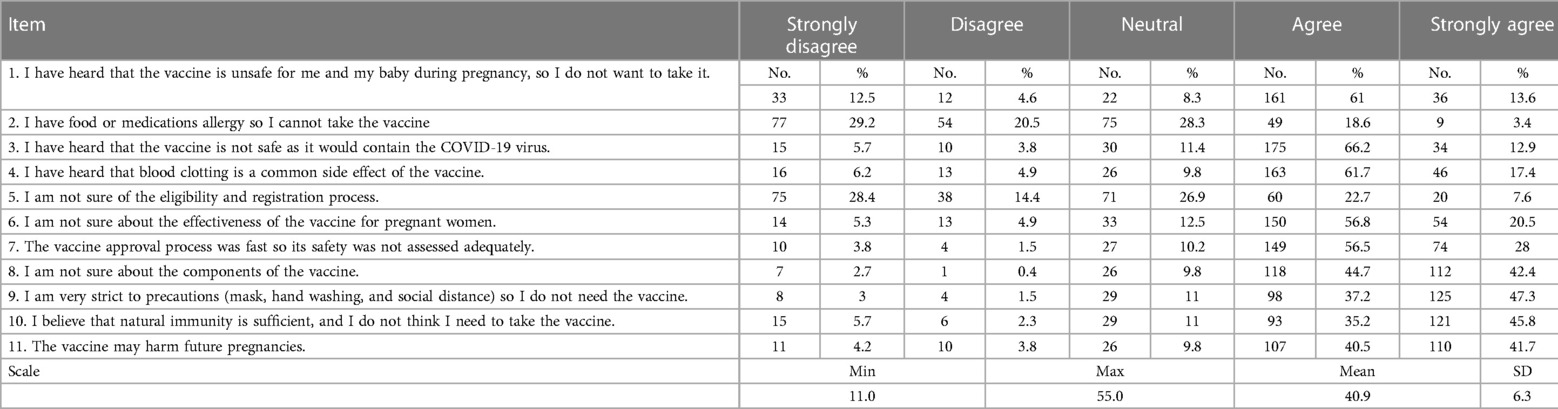
Table 3. Hesitancy to receive COVID-19 vaccination among the participants.
As regards perception of benefits of COVID-19 vaccination, half of the participants 50% agreed that vaccination would alleviate the precautionary measures, including lockdown, quarantine, work permit, and travel bans. Additionally, 40.9% of them agreed that COVID-19 complications are more serious in pregnant women and that the vaccine would provide protection (Table 4).

Table 4. Perception of benefits of COVID-19 vaccination among the participants.
Reasons for receiving COVID-19 vaccination were variable, less than half of the participants 45.8%, 45.8%, and 41.3%, respectively agreed that they would only take the COVID-19 vaccine if it was made mandatory and widely accepted by the public, or if they were provided with adequate information about it (Table 5).

Table 5. Reasons for receiving COVID-19 vaccination among the participants.
The results revealed significant differences in the perception scale scores based on the number of children a participant had (P = 0.026) with participants with a higher number of children were found to have higher scores. Regarding the hesitancy scale, significant differences in scores were identified based on occupation and the vaccination status variables (P = 0.003 and P = 0.033, respectively). Participants working in the health sector exhibited lower hesitancy scores compared to others while non-vaccinated participants had a higher mean score compared to vaccinated participants. The study also demonstrated significant differences in the scores of the benefits and reasons scales based on gestational age (P = 0.020). Participants in the second trimester had lower mean scores compared to others in both the benefits and reasons for COVID-19 vaccination scales. Furthermore, significant differences in the scores of the reasons scale based on gestational age were observed (P = 0.010). Participants in the second trimester had lower mean scores compared to others in both the benefits and reasons for COVID-19 vaccination scales (Table 6). The Pearson correlation coefficients revealed significant relationships among participants' perceptions of COVID-19 severity, vaccine hesitancy, perceived benefits, and reasons for vaccination (Table 7).
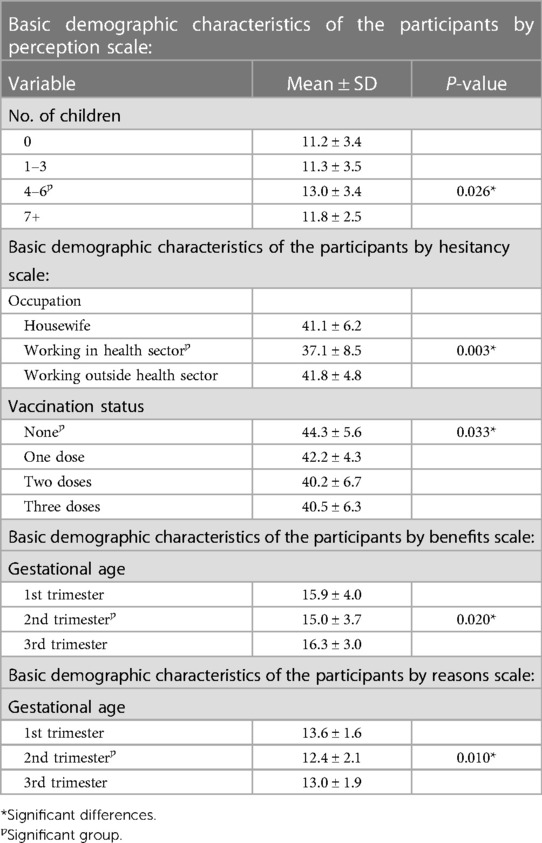
Table 6. Basic demographic characteristics of the participants by perception, hesitancy, benefits, and reasons scale.
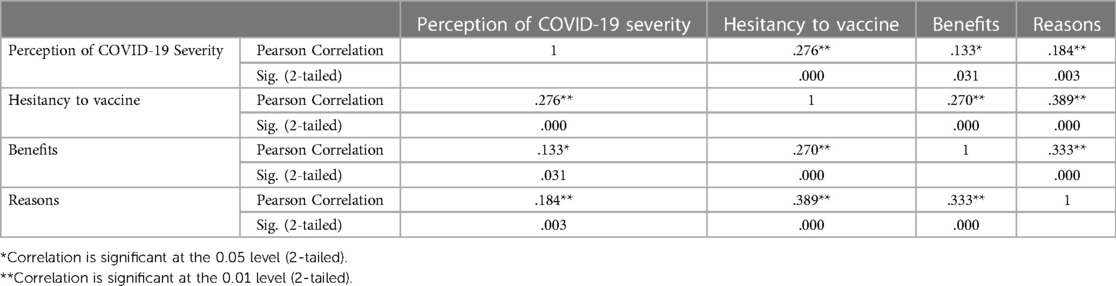
Table 7. Correlation between perception, hesitancy, benefits, and reasons scales.
4 Discussion
In the present study, approximately half (48.9%) of the participants agreed that the likelihood of contracting a COVID-19 infection is low in Saudi Arabia. This perception aligns with the reported decrease in COVID-19 cases in the country from 13.7% to 10.9%. These reductions reflect the effectiveness of the implemented prevention strategies (3, 36).
The most reported reasons for hesitancy to receive COVID-19 vaccination among the study participants were their concerns about the vaccine safety, side effects and effectiveness during pregnancy. These findings are consistent with a study conducted by Goncu Ayhan et al. (37), which aimed to assess acceptance and hesitancy toward COVID-19 vaccines among pregnant women. The study found that those who would refuse the vaccine cited a lack of data on COVID-19 vaccine safety during pregnancy and potential harm to the fetus as their main concerns. These findings can be due to the exclusion of pregnant women from clinical trials.
Half of the participants in the present study stated that vaccination would ease precautionary measures, including lockdowns, quarantine, work permits, and travel bans. Additionally, 40.9% of them believed that COVID-19 complications are more severe during pregnancy and that the vaccine would protect them. These results are in line with a study conducted to assess the attitude toward COVID-19 vaccination among pregnant and breastfeeding women in Italy, which revealed that a significant percentage of the pregnant women believed they were at a considerable risk of contracting SARS-CoV-2, emphasizing the importance of receiving the COVID-19 vaccine (38).
Less than half of the participants in the present study agreed that they would only take the COVID-19 vaccine if it was made mandatory or widely accepted by the public. These findings correspond with a study conducted in Saudi Arabia, which aimed to explore the acceptability and reluctance of pregnant and breastfeeding women to receive COVID-19 vaccination. The study reported that about half of the women stated they would receive the COVID-19 vaccine if it were recommended for pregnant and breastfeeding women (39).
Significant differences in perception scores of COVID-19 severity and susceptibility were found based on the number of children, where participants with a higher number of children had higher scores on the scale. This can be explained by the heightened worry and concern of the mothers about themselves and their children. However, no such correlation was identified between COVID-19 vaccine perception scores of severity and susceptibility and the number of children (P > 0.05) in a study conducted by Goncu Ayhan et al. (37) in Turkey.
Furthermore, significant differences in hesitancy scale scores were observed based on occupation and COVID-19 vaccination status, with participants working in the health sector having lower scores compared to others. This could be attributed to the increased health awareness among those in the health sector regarding the importance of vaccination. This finding contrasts with a cross-sectional study that found no statistically significant relationships between COVID-19 vaccine acceptance and occupation status among the participants (39).
Moreover, participants who had not received the COVID-19 vaccine exhibited higher mean scores for hesitancy, which accounts for their decision to not get vaccinated. This is consistent with the results of an institutional-based cross-sectional study conducted by Mose and Yeshaneh (10) in an antenatal care clinic in Southwest Ethiopia, which revealed that pregnant women who exhibited hesitancy toward the influenza H1N1 vaccine displayed similar concerns regarding COVID-19 vaccination.
The results of the benefits and reasons for receiving the vaccine scales showed significant differences in scores among participants in the second trimester, who had lower mean scores compared to others. Another study found no significant relationship between gestational age and the scores of benefits and reasons for receiving the vaccine scales (39).
The study's findings highlight the vital role of healthcare providers in the vaccination decision-making process of pregnant women. These professionals are pivotal in enhancing vaccine acceptance, particularly by offering tailored health education during antenatal visits that focuses on the severity of COVID-19, the susceptibility of pregnant women to the infection, and the benefits of vaccination. The provision of printed materials outlining preventive strategies and the safety of COVID-19 vaccines can further support their efforts in improving vaccine uptake among this population.
A notable limitation of this study is the use of a self-administered survey instrument, which raises concerns regarding the risk of response bias. Additionally, the employment of non-probability sampling may restrict the generalizability of the study's results. These methodological limitations suggest that future research should employ more robust sampling techniques to enhance the representativeness and reliability of the data.
To contribute to the growing body of knowledge on the subject, further research should be undertaken in diverse settings. This research should prioritize the evaluation of the safety of COVID-19 vaccines specifically in pregnant women, addressing their unique healthcare needs. In the clinical context, counseling services should be provided to pregnant women. These sessions should address their specific concerns related to COVID-19 vaccination. By doing so, healthcare professionals can play a crucial role in enhancing awareness and acceptance of the COVID-19 vaccine among pregnant women.
The findings of the present study showed that the majority of participants perceived a low susceptibility to COVID-19 infection and expressed hesitancy toward the vaccine, with uncertainty about its effectiveness. However, they indicated a willingness to receive the COVID-19 vaccine if it was made mandatory and if they were provided with adequate information.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by King Abdullah International Medical Research Center, and the Institutional Review Board at King Abdulaziz Medical City-Western Region. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. AO: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. HA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare financial support was received for the publication of this article.
Funding source is the Saudi National Institute for Health Research (Saudi NIH) (Grant number: 37389668).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. López M, Gonce A, Meler E, Plaza A, Hernández S, Martinez-Portilla RJ, et al. Coronavirus disease 2019 in pregnancy: a clinical management protocol and considerations for practice. Fetal Diagn Ther. (2020) 47:519–28. doi: 10.1159/000508487
2. WHO. World Health Organization. Ten threats to global health in 2019; 2019 (2022). Available online at: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (Accessed March 9, 2022).
3. MOH. COVID-19 & vaccine FAQs. Ministry of health Saudi Arabia (2022). Available online at: https://www.moh.gov.sa/en/Ministry/HotTopics/Pages/COVID-19-Vaccine.aspx (Accessed March 31, 2022).
4. Ellington S, Strid P, Tong VT, Woodworth K, Galang RR, Zambrano LD, et al. Characteristics of women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy Status — United States, January 22–June 7, 2020. Morb Mortal Wkly Rep. (2020) 69:769–75. doi: 10.15585/mmwr.mm6925a1
5. Weetman AP. Immunity, thyroid function and pregnancy: molecular mechanisms. Nat Rev Endocrinol. (2010) 6(6):311–8. doi: 10.1038/nrendo.2010.46
6. Pazos M, Sperling RS, Moran TM, Kraus TA. The influence of pregnancy on systemic immunity. Immunol Res. (2012) 54(1–3):254–61. doi: 10.1007/s12026-012-8303-9
7. Rasmussen SA, Smulian JC, Lednicky JA, Wen TS, Jamieson DJ. Coronavirus disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. (2020) 222(5):415–26. doi: 10.1016/j.ajog.2020.02.017
8. Guo F, Yang X. A comprehensive review of the management of pregnant women with COVID-19: useful information for obstetricians. Infect Drug Resist. (2021) 14:3363–78. doi: 10.2147/IDR.S325496
9. Shams T, Alhashemi H, Madkhali A, Noorelahi A, Allarakia S, Faden Y, et al. Comparing pregnancy outcomes between symptomatic and asymptomatic COVID-19 positive unvaccinated women: multicenter study in Saudi Arabia. J Infect Public Health. (2022) 15(8):845–52. doi: 10.1016/j.jiph.2022.06.002
10. Mose A, Yeshaneh A. COVID-19 vaccine acceptance and its associated factors among pregnant women attending antenatal care clinic in Southwest Ethiopia: institutional-based cross-sectional study. Int J Gen Med. (2021) 14:2385–95. doi: 10.2147/IJGM.S314346
11. Liu Y, Chen H, Tang K, Guo Y. Clinical manifestations and outcome of SARS CoV-2 infection during pregnancy. J Infect. (2020) 4453(20):30109–2. doi: 10.1016/j.jinf.2020.02.028
12. Wang CL, Liu YY, Wu CH, Wang CY, Wang CH, Long CY. Impact of COVID-19 on pregnancy. Int J Med Sci. (2021) 18(3):763–7. doi: 10.7150/ijms.49923
13. Chen H, Guo J, Wang C. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. (2020) 395(10226):809–15. doi: 10.1016/S0140-6736(20)30360-3
14. Breslin N, Baptiste C, Miller R. COVID-19 in pregnancy: early lessons. Am J Obstet Gynecol. (2020) 2(2):100111. doi: 10.1016/j.ajogmf.2020.100111
15. Lokken EM, Walker CL, Delaney S. Clinical characteristics of 46 pregnant women with a severe acute respiratory syndrome coronavirus 2 infection in Washington state. Am J Obstet Gynecol. (2020) 223(6):911.e1–911.e14. doi: 10.1016/j.ajog.2020.05.031
16. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
17. Ramos IF, Guardino CM, Mansolf M, Glynn LM, Sandman CA, Hobel CJ. Pregnancy anxiety predicts shorter gestation in Latina and non-Latina white women: the role of placental corticotrophin-releasing hormone. Psychoneuroendocrinology. (2019) 99:166–73. doi: 10.1016/j.psyneuen.2018.09.008
18. Hunt B, Retter A, McClintock C. Practical Guidance for the Prevention of Thrombosis and Management of Coagulopathy and Disseminated Intravascular Coagulation of Patients Infected With COVID-19. Llanwrda, UK: Thrombosis UK (2020).
19. Zambrano LD, Ellington S, Strid P. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status — United States. MMWR Morb Mortal Wkly Rep. (2020) 69:1641–7. doi: 10.15585/mmwr.mm6944e3
20. Mendoza M, Garcia-Ruiz I, Maiz N, Rodo C, Garcia-Manau P, Serrano B, et al. Preeclampsia-like syndrome induced by severe COVID-19: a prospective observational study. BJOG. (2020) 127(11):1374–80. doi: 10.1111/1471-0528.16339
21. Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, Kew T, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. Br Med J. (2020) 370:m3320. doi: 10.1136/bmj.m3320
22. Pereira A, Cruz-Melguizo S, Adrien M, Fuentes L, Marin E, Perez-Medina T. Clinical course of coronavirus disease-2019 in pregnancy. Acta Obstet Gynecol Scand. (2020) 99(7):839–47. doi: 10.1111/aogs.13921
23. Blitz MJ, Rochelson B, Meirowitz N, Prasannan L, Rafael TJ. Maternal mortality among women with coronavirus disease 2019. Am J Obstetrics Gynecol. (2019) 223(4):595–9. doi: 10.1016/j.ajog.2020.06.020
24. Xu L, Yang Q, Shi H, Lei S, Liu X, Zhu Y, et al. Clinical presentations and outcomes of SARS-CoV-2 infected pneumonia in pregnant women and health status of their neonates. Science Bulletin. (2020) 65(18):1537–42. doi: 10.1016/j.scib.2020.04.040
25. Ceulemans M, Foulon V, Panchaud A, Winterfeld U, Pomar L, Lambelet V, et al. Vaccine willingness and impact of the COVID-19 pandemic on women’s perinatal experiences and practices—a multinational, cross-sectional study covering the first wave of the pandemic. Int J Environ Res Public Health. (2021) 18(7):3367. doi: 10.3390/ijerph18073367
26. WHO. Strategy to achieve global COVID-19 vaccination by mid-2022. WHO World Health Organization (2021). Available online at: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 April 2022 (Accessed May 31, 2022).
27. Borges MASB, Florentino PTV, Cerqueira-Silva T, Carvalho LF, Oliveira VA, Aguilar GMO, et al. Factors associated with COVID-19 vaccination among pregnant women in rio De janeiro city, Brazil. Sci Rep. (2023) 13:18235. doi: 10.1038/s41598-023-44370-6
28. Nguyen L, Hoang M, Nguyen L, Ninh L, Nguyen H, Nguyen A, et al. Acceptance and willingness to pay for COVID-19 vaccines among pregnant women in Vietnam. Trop Med Int Health. (2021) 26(10):1303–13. doi: 10.1111/tmi.13666
29. Kilich E, Dada S, Francis MR, Tazare J, Chico RM, Paterson P, et al. Factors that influence vaccination decision-making among pregnant women: a systematic review and meta-analysis. PLoS One. (2020) 15(7 July 2020):1–28. doi: 10.1371/journal.pone.0234827
30. Glanz JM, Wagner NM, Narwaney KJ, Kraus CR, Shoup JA, Xu S, et al. Web-based social Media intervention to increase vaccine acceptance: a randomized controlled trial. Paediatrics. (2017) 140(6):e20171117. doi: 10.1542/peds.2017-1117
31. Qin Y, Zhou R, Wu Q, Huang X, Chen X, Wang W, et al. The effect of nursing participation in the design of a critical care information system: a case study in a Chinese hospital. BMC. (2017) 17(1):165. doi: 10.1186/s12911-017-0569-3
32. Bichovsky Y, Klein M, Brotfain E. A positive cumulative fluid balance in critically ill patients: is it really harm for everybody? Kardiol Pol. (2019) 77(12):1121–2. doi: 10.33963/KP.15111
33. Liu J, Cao Y, Xu C, Zhou C, Wei W, Yuan J, et al. Midwifery and nursing strategies to protect against COVID-19 during the third trimester of pregnancy. Midwifery. (2021) 92:102876. doi: 10.1016/j.midw.2020.102876
34. Samannodi M. COVID-19 vaccine acceptability among women who are pregnant or planning for pregnancy in Saudi Arabia: a cross-sectional study. Patient Prefer Adherence. (2021) 15:2609–18. doi: 10.2147/PPA.S338932
35. Almaghaslah D, Alsayari A, Kandasamy G, Vasudevan R. COVID-19 vaccine hesitancy among young adults in Saudi Arabia: a cross-sectional web-based study. Vaccines. (2021) 9(4):330. doi: 10.3390/vaccines9040330
36. WHO. Weekly operational update on COVID-19 - 10 April 2022 (2022). Available onlin at: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—12-april-2022 (Accessed May 31, 2022).
37. Goncu Ayhan S, Oluklu D, Atalay A, Menekse Beser D, Tanacan A, Moraloglu Tekin O, et al. COVID-19 vaccine acceptance in pregnant women. Int J Gynaecol Obstet. (2021) 154(2):291–6. doi: 10.1002/ijgo.13713
38. Carbone L, Mappa I, Sirico A, Di Girolamo R, Saccone G, Di Mascio D, et al. Pregnant women’s perspectives on severe acute respiratory syndrome coronavirus 2 vaccine. Am J Obstet Gynecol MFM. (2021) 3(4):100352. doi: 10.1016/j.ajogmf.2021.100352
Keywords: COVID-19, pandemic, vaccine hesitancy, acceptance, pregnant women, Saudi Arabia
Citation: Hawsawi S, Orabi A and Alnajjar H (2024) Acceptance and hesitancy of COVID-19 vaccination among Saudi pregnant women. Front. Glob. Womens Health 5:1336766. doi: 10.3389/fgwh.2024.1336766
Received: 11 November 2023; Accepted: 5 January 2024;
Published: 26 January 2024.
Edited by:
Aida Bianco, University Magna Graecia of Catanzaro, ItalyReviewed by:
Nongyao Kasatpibal, Chiang Mai University, ThailandFrancesca Licata, University Magna Graecia of Catanzaro, Italy
© 2024 Hawsawi, Orabi and Alnajjar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abeer Orabi YWJlZXJtb2todGFyMzFAeWFob28uY29t