 Alix Boisson-Walsh1*
Alix Boisson-Walsh1* Noro L. R. Ravelomanana2Martine Tabala2Fathy Malongo2Bienvenu Kawende2Pélagie Babakazo2Marcel Yotebieng3
Noro L. R. Ravelomanana2Martine Tabala2Fathy Malongo2Bienvenu Kawende2Pélagie Babakazo2Marcel Yotebieng3
- 1Department of Health Policy and Management, University of Carolina at Chapel Hill, Chapel Hill, NC, United States
- 2School of Public Health, University of Kinshasa, Kinshasa, Democratic Republic of Congo
- 3Division of General Internal Medicine, Department of Medicine, Albert Einstein College of Medicine, Bronx, NY, United States
Introduction: Worldwide, over two-thirds of people living with HIV are on antiretroviral therapy (ART). Despite increased ART access, high virological suppression prevalence remains out of reach. Few studies consider the quality of ART services and their impact on recipients' viral suppression. We assessed the association between ART service readiness and HIV viral load suppression among pregnant and breastfeeding women living with HIV (WLH) receiving ART in maternal and child health (MCH) clinics in Kinshasa, Democratic Republic of Congo.
Methods: We performed a cross-sectional analysis leveraging data from a continuous quality improvement intervention on WLH's long-term ART outcomes. From November 2016 to May 2020, we enrolled WLH from the three largest clinics in each of Kinshasa'Łs 35 health zones. We measured clinic's readiness using three WHO-identified ART care quality indicators: relevant guidelines in ART service area, stocks of essential ART medicines, and relevant staff training in ≥24 months, scoring clinics 0-3 based on observed indicators. We defined viral load suppression as ≤1,000 cp/ml. Multilevel mixed-effect logistic models were used to estimate prevalence odds ratios (ORs) measuring the strength of the association between ART service readiness and viral suppression.
Results: Of 2,295 WLH, only 1.9% received care from a clinic with a score of 3, 24.1% received care from a 0-scoring clinic, and overall, 66.5% achieved virologically suppression. Suppression increased from 65% among WLH receiving care in 0-scoring clinics to 66.9% in 1-scoring clinics, 65.8% in 2-scoring clinics, and 76.1% in 3-scoring clinics. We did not observe a statistically significant association between ART service readiness score and increased viral suppression prevalence, however we did find associations between other factors, such as the location of the health center and pharmacist availability with suppressed viral load.
Discussion: A lack of comprehensive ART care underscores the need for enhanced structural and organizational support to improve virological suppression and overall health outcomes for women living with HIV..
1 Introduction
Despite significant advances in antiretroviral (ART) services contributing to an estimated 12.1 million AIDS-related deaths, (1, 2) achieving the ambitious UNAIDS 90-90-90 targets [90% of people living with HIV (PLHIV) are aware of their status, of whom 90% have initiated ART treatment, and of whom 90% have achieved virologic suppression by 2020] remains a challenge as of December 2022, with considerable disparities across regions and population groups (3–5). Due to an unprecedented initiative to eliminate mother-to-child transmission, pregnant women have generally had better access to HIV testing and ART than the general population during antenatal care visits to maternal and child health (MCH) clinics. However, the provision of longitudinal chronic ART care through maternal and child health (MCH) clinics, designed for episodic acute care, has not been conclusively shown to yield high viral suppression. Furthermore, while pregnant and breastfeeding women living with HIV (WLH) receive treatment, viral suppression remains suboptimal, and significant variability in suppression rates across facilities remains (6).
Existing literature has predominantly focused on individual-level factors affecting virological suppression among pregnant and breastfeeding WLH, (7, 8) with scant attention to the healthcare delivery system's design, which is integral to performance and health outcomes (9). Our study aims to bridge this gap by examining the association between clinic-level ART service quality and the prevalence of virological suppression among pregnant and postpartum WLH in the Kinshasa Province, Democratic Republic of Congo (DRC).
Underpinned by the Systems Theory of Management, (10) which posits that the interrelationships among its subsystems determine an organization's effectiveness, this study scrutinizes the structural and process aspects of ART service delivery within MCH clinics. The theory guides our investigation into how systemic attributes such as service readiness, staff capacity, and clinic management practices influence the ultimate goal of virological suppression. By aligning our research design with this framework, we aim to highlight the complexities of service delivery and provide insights into system-level interventions that can enhance outcomes for WLH in the DRC.
2 Methods
2.1 Study design, setting, and population
We performed a cross-sectional analysis of data from the baseline enrollment assessment of the continuous quality intervention-prevention-of-mother-to-child transmission (CQI-PMTCT) study: a cluster randomized trial to evaluate the effect of CQIs on long-term ART outcomes among pregnant and breastfeeding women (NCT03048669) (11). The study selected the three clinics with the highest patient volume in each of the 35 health zones of the Kinshasa province in the Democratic Republic of Congo. From June to May 2017, study staff visited each of the 105 MCH clinics and interviewed departmental supervisors or managers to collect clinic-level information using a facility survey tool modeled after a facility audit of service quality developed by MEASURE Evaluation to assess the quality and provision of district-level health services (12). The same study staff completed the entire questionnaire within a facility. From November 2016 to May 2020, pregnant or breastfeeding (≤1-year post-delivery) WLH receiving ART in the clinics were approached for enrollment. Participants were enrolled at any time during antenatal care visits, immediately after delivery (in the maternity ward during the 1–3 days post-delivery observation), or during routine well-child visits in the postpartum period. All participants were informed about the study and provided written consent. The Institutional Review Board of the Ohio State University and the Kinshasa School of Public Health committee approved the protocol. After receiving consent, the study team collected five 50 ml blood spots obtained by a finger prick on Whatman paper from each participant. The samples were sent to the national HIV reference laboratory for viral load measurement.
2.2 Ethical considerations
Ethical approval was received from the Institutional Review Boards at Ohio State University and the Kinshasa School of Public Health in the Democratic Republic of the Congo. Participants' written consent to participate in this study was obtained during enrollment. Participants' identification were anonymized in the study data using participant identification codes in the relevant dataset.
2.3 Variables
2.3.1 Virological suppression
The primary outcome of this analysis was virological suppression, defined as a viral load of ≤1,000 copies/ml.
2.3.2 ART service readiness
The study's primary exposure was ART service readiness. The ART service readiness variable was calculated for each maternity clinic, using three WHO-identified inputs to quantify service-specific readiness obtained from the facility survey data (13): (1) whether relevant health staff member(s) received ART service-related training within the last 24 months; (2) whether country-specific ART service guidelines were available in the service area; (3) whether first-line ART regimens were available (TDF + 3TC + EFV, TDF + FTC + EFV, AZT + 3TC + EFV, TDF + 3TC + NVP, TDF + FTC + NVP, and AZT + 3TC + NVP). We assigned equal weight to each component in line with the WHO approach. The study team attributed a score of one for each indicator that was observed during the clinic survey. Indicators that were reported but not observed received a score of 0. Each clinic received a final measure of ART service readiness ranging from 0 (no indicator observed) to 3 (all three indicators observed) based on the number of indicators observed.
2.3.3 Other covariables
Covariates at the MCH clinic level included: clinic type (hospital or health center), operational entity (public, private-for-profit, or non-profit), location (urban or peri-urban/rural), support by a PEPFAR implementing partner (yes or no), external supervision provided by the health zone bureau (yes or no), and the number of healthcare staff (continuous). Covariates at the individual level included: the participant's ART regimen (TDF + 3TC + FEV, AZT + 3TC + NVP, or Lopinavir-based), (14–16) her age in years (≤24, 25–34, or 35+), her marital status (married/cohabitating or divorced/separated/widowed/never married), her duration of ART treatment (<12, 12–24, or 24 months), (15, 17–23) her educational attainment (primary, secondary, or tertiary), (16, 17) whether she disclosed her HIV status (yes or no), (17) and her wealth index score. To compute the wealth index score, we employed principal component analysis considering the following factors: years of education, number of household members per room, number of sleeping beds in the household, household water source (communal vs. private pipe), cooking fuel type (electrical stove vs. wood/charcoal), and status of ownership of prosaic household goods (mobile phone, radio, fridge, vehicle, bike, and motorcycle). To replicate previous studies, (6, 24) we retained the first component accounting for the most significant variability in the dataset (20.7%). We categorized the first component into quintiles from lowest to highest SES (0–4) to produce the wealth index score.
2.4 Statistical analysis
We calculated the proportion of women with virologic suppression and compared it across levels of ART service readiness and other key variables. We used bivariate multilevel mixed-effect logistic models regressions to estimate prevalence odds ratios (ORs) and 95% confidence intervals (95% CIs), measuring the strength of association between potential confounders and the outcome. We included variables found in bivariate analyses to be associated with viral load suppression (P <= 0.20) in the multivariate model. We employed a backward selection methodology to select the most parsimonious final model that minimized bias and optimized the precision of the effect estimate. We retained confounders in the final model if their exclusion changed the estimate (OR) of the association between exposure and outcome by >10%. Each model accounts for clustering at the MCH clinic and the health zone level. We ran the model with the ART readiness indicator, but also with the three individual readiness indicators to assess model sensitivity to exposure definition. We conducted all statistical analyses using Stata Version 15.0 (StataCorp, College Station, TX, USA), and all statistical tests were two-sided with an alpha level of 0.05 except when otherwise indicated.
3 Results
3.1 Participant characteristics
The parent study enrolled 2,343 WLH, of whom 55 WLH had no viral load results for a total effective sample size of 2,295 WLH. Most participants (62%) were enrolled during pregnancy or at delivery (Table 1). One thousand three hundred ten (57.1%) participants were diagnosed during their past pregnancy. Over half of the participants (52.1%) fell within the 25–34 age category. Most were married or cohabitating (69.3%), had secondary education (71.7%), and were taking tenofovir-lamivudine-efavirenz (78.2%). Most women received HIV care at a hospital (57.1%) funded by PEPFAR (66.7%) in an urban setting (92.7%).

Table 1. Characteristics of pregnant and breastfeeding women, enrolled in a trial evaluating the effect of data-driven continuous quality improvement on long-term ART outcomes in Kinshasa, DRC.
3.2 MCH clinic characteristics
Of the 99 facilities participating in the survey assessment, only 5 (5.1%) had an ART services readiness score of 3, 16 (16.2%) had a score of 2, 48 (48.5%) had a score of, and 30 (30.3%) had a score of 0. Among the facilities, 64 (64.7%) had country-specific ART service guidelines available in the service area, 19 (19.2%) provided ART service-related training, and 13 (13.1%) had first-line ART regimens available. The slight majority of health facilities were hospitals (52.5%), were located in urban settings (85.9%), were managed by a not-for-profit (44.4% vs. 23.2% private and 32.3% not-for-profit), were supported by a PEPFAR implementing partner (51.5%) and did receive external supervision by the health zone bureau within the last 6 months (96%) (Table 2). Most facilities (81.8%) did not have a pharmacist available. Of the 2,295 WLH included in the analysis, 24.1% (552) received care from a clinic with an ART readiness score of 0, 57.8% (1,326) from a clinic with a score of 1, 16.2%, (371) from a 2-scoring clinic, and only 2% (46) received care from a clinic with an ART readiness score of 3.
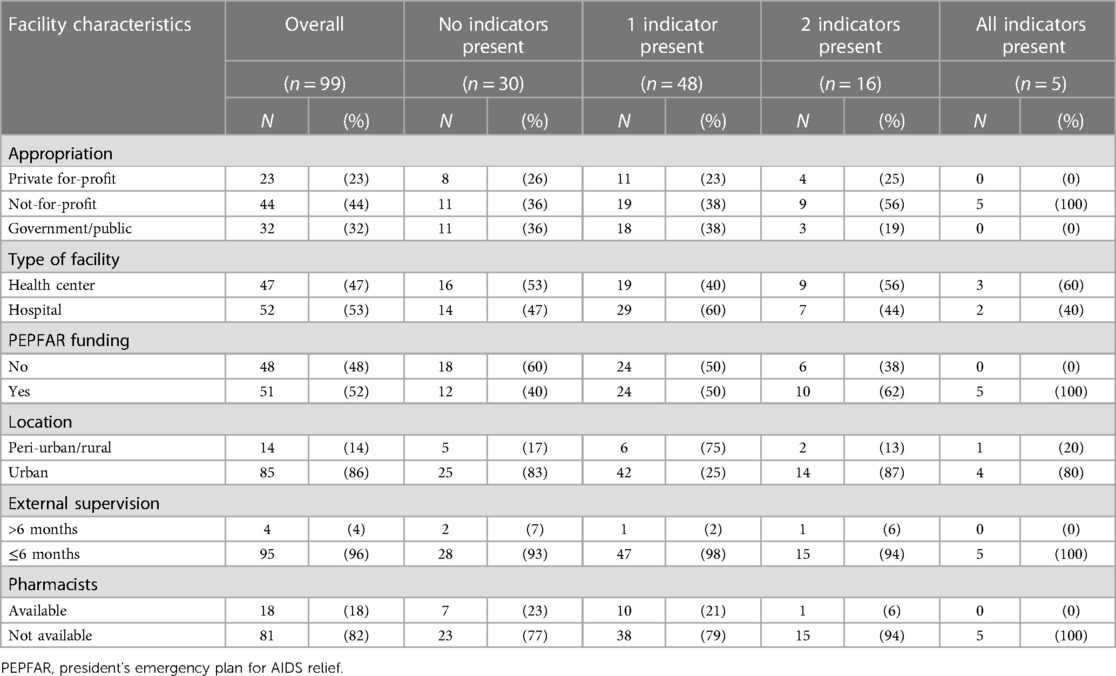
Table 2. Site characteristics; Kinshasa health facilities survey, 2016.
3.3 Bivariate analysis
From the analytical sample of 2,295 women, 66.5% (1,525) were virologically suppressed (Table 3).
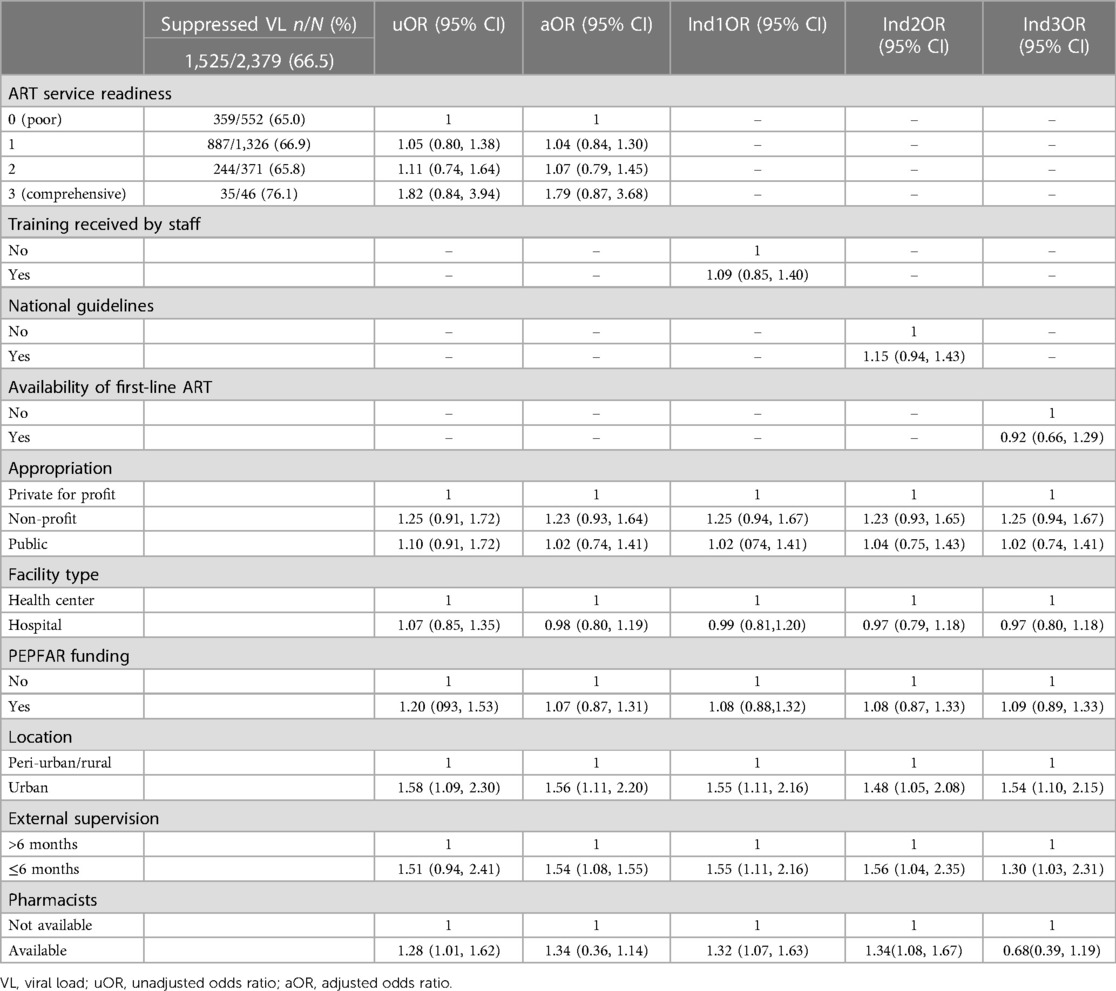
Table 3. Relationship between readiness of ART service and suppressed HIV viral load.
3.4 Association of comprehensiveness of ART service with suppressed viral load
The prevalence of virologic suppression was 65.0% among participants receiving care in a clinic with an ART readiness score of 0 compared to 66.9% among those receiving care in a 1-scoring clinic (cOR: 1.05, 95% CI: 0.80, 1.38), or 65.8% in those in 2-scoring clinics (cOR: 1.11, 95% CI: 0.74, 1.64), and 76.1% in 3-scoring clinics (cOR: 1.82, 95% CI: 0.84, 3.94). After adjusting for the operational entity, type of clinic, PEPFAR funding, routine quality assurance activities, external supervision of the clinic, and the pharmacists' availability at the health clinic, and study phase, the prevalence ratios estimate remain unchanged [aOR1: 1.04, 95% CI: 0.84, 1.38; aOR2: 1.07, 95% CI: 0.79, 1.45; aOR3: 1.79, 95% CI: 0.87, 3.68, respectively, (Table 3)]. Further, individual components of the ART readiness indicator did not yield statistically significant estimates (refer to Table 3, models Ind1ME, Ind2ME, and Ind3ME).
3.5 Association of covariates with suppressed viral load
In our investigation of factors correlated with suppressed viral load among HIV-positive individuals, the primary exposure variable, ART service readiness, did not show a statistically significant impact. However, our analysis identified two key covariates consistently associated with an increased likelihood of viral suppression. Patients treated in urban health centers had 1.58 times the odds of achieving viral suppression compared to those in peri-urban centers (95% CI: 1.09, 2.30). Patients also had 1.28 times the odds of achieving suppressed viral load if the health facility had a pharmacist available (95% CI: 1.01, 1.62). In addition, each model evaluating individual exposure variables and the adjusted model showed that the experience of external supervision within the past 6 months contributed positively to suppressed viral load.
4 Discussion
Among our sample of WLHs who had their first viral load collected, only 1.9% received care in a clinic with comprehensive ART services, despite every health facility reporting provision and access to antiretroviral (ART) services during the study team visits to the facilities. Our comprehensive analysis of the association between ART service readiness and virological suppression in MCH clinics revealed that, although the primary exposure variable of ART service readiness did not show a statistically significant impact, clinic location and pharmacist availability were critical in enhancing the likelihood of viral suppression. This aligns with previous findings that emphasize the importance of healthcare accessibility and professional support in managing chronic conditions like HIV.
Importantly, our study introduces novel insights into the role of systemic factors, particularly the impact of external supervision, in promoting positive health outcomes. The 44 percentage point increase in viral suppression probability due to such supervision suggests that oversight may catalyze improving service delivery quality, thus enhancing patient outcomes.
Despite these substantial findings, the lack of statistically significant associations in specific areas underlines the complex interplay of factors influencing virological outcomes and the necessity for multifaceted approaches to bolster the ART service framework within MCH clinics.
Among our sample, a higher percentage of participants seeking care at facilities with comprehensive ART service readiness scores (76.1%) achieved viral suppression compared to those seeking care at 0-scoring facilities (65%), however this finding is not statistically significant. Likewise, WLH seeking care in facilities with one or two ART readiness indicators were more likely to have a suppressed HIV viral load detected than those seeking care at facilities with no readiness indicators observed. Although these findings were not statistically significant, they highlight the importance of expanding the availability of core PMTCT interventions and strengthening the capacity of facilities and relevant personnel to offer these interventions.
Several possibilities might explain the increased viral load suppression among higher-scoring ART service readiness facilities at the organizational level. Unsupported staff may not possess the tools and training required to appropriately educate women on the risk of MTCT, (25) which also may impact adherence to ART treatment. Poorly trained healthcare staff may not have the necessary resources and training to counsel WLH, which could also act as a determinant of HIV viral load. Without clinical directives, WLH may fail to report their medical status to their sexual partners (26, 27). Further, a health system's fragmentation may deepen in cases where communication of updated guidelines and protocols related to ART service areas do not reach healthcare managers and staff (28). The resulting impact on quality of care, lack of organization, and inefficiency of services at an organizational level could lead to overcrowding of health facilities and long treatment and service delays (29–31). The limitations may severely deter a facility's attendance. We speculate maternal disengagement from the ART cascade may mediate the association between ART service readiness and viral load. A previous study found an association between quality improvement activities and WLH retention in public-sector clinics (32).
Stockouts of HIV commodities, such as ART, represent a structural inadequacy that broadly impacts PMTCT programs (33). International organizations, such as PEPFAR, offer logistical and technical support to alleviate structural barriers in low-resource settings, such as the DRC (34). However, decision-makers in health systems receiving such funds should conduct system-based monitoring to forecast approaches to provision for future international funding reductions (35, 36) This proves especially true given the inadequacies of DRC's public healthcare spending, which accounts for only 9% of its budget (37).
The interpretation of our findings should account for several limitations. First, departmental supervisors and managers reported survey data. As such, we could not preclude over or under-estimation of ART care readiness. We decreased the possibility of differential misclassification through regular surveys with departmental supervisors and managers instead of a composition of staff members. Another limitation was that our estimates account only for women receiving care in our study clinics. Therefore, we cannot adequately estimate the burden of HIV viral load among WLH seeking care in other MCH clinics or those not seeking clinical care. Dried blood spot viral load systematically underestimates plasma viral load (38, 39). We, therefore, undoubtedly underestimated the actual proportion of women without suppressed viral loads. Another limitation is that our data lack information on adherence between ART initiation and date of enrollment. We, therefore, cannot assess whether adherence is a mediator in the observed association between ART comprehensiveness and viral load suppression. In addition, the parent study recruited participants from the three MCH clinics with the highest patient volume in each of the 35 health zones in Kinshasa Province. Data from these clinics may not represent trends in other DRC-based MCH clinics. However, due to elevated patient rates, findings from the 105 clinics most likely reflect WLH receiving care in Kinshasa province. Finally, considering that the study involved high-volume clinics in Kinshasa, the results may suggest wider trends in ART service effectiveness and patient outcomes throughout the province, especially in resource-rich urban areas. Nevertheless, given the variability in clinic operations and resources, careful consideration is needed when applying these findings to all Kinshasa facilities. Further studies are warranted to explore how these findings might be scaled across the province's diverse healthcare settings
Our study found that, among the 99 MCH clinics in Kinshasa Province, only four had all three ART readiness indicators present, and 98.1% of WLH did not receive care in a facility with comprehensive ART care. Despite the non-statistically significant results, the trend suggests that comprehensive ART services correlate with better virological outcomes. Addressing the barriers to quality ART services is imperative for MCH clinics to enhance the care outcomes for WLH, particularly in achieving viral suppression. As we continue to unravel the complexities of healthcare delivery and its impact on HIV management, it is evident that robust structural and organizational support systems are essential. Our findings call for focused interventions that support WLH and strengthen the healthcare infrastructure catering to their needs. Through such concerted efforts, we can see a marked improvement in the health outcomes for WLH in Kinshasa and across similar settings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Institutional Review Boards at Ohio State University, Einstein University and the Kinshasa School of Public Health in the Democratic Republic of the Congo. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
A-BW: Formal Analysis, Writing – original draft. NR: Investigation, Writing – review & editing. MT: Investigation, Validation, Writing – review & editing. FM: Investigation, Writing – review & editing. BK: Investigation, Writing – review & editing. PB: Supervision, Writing – review & editing. MY: Conceptualization, Funding acquisition, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This research was supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) and the National Institute of Child Health and Human Development (NICHD 1R01H087993). MY are partially supported by the National Institutes of Health (NIAID U01AI096299, NICHD R01HD105526). The funders had no role in study design, data collection, data analysis and interpretation, preparation of the manuscript, or decision to submit.
Acknowledgments
This manuscript would not have been possible without the preliminary research conducted by Christian Mpody. We are extremely grateful for the support of our local partners: The national and provincial Ministries of Health through the National Program for the Fight against AIDS (PNLS), the “Bureau des Oeuvre Diocésain (BDOM)”, Salvation Army, and participating health facilities. We thank the local study staff who contributed to the collection and execution of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. District of Columbia Department of Health HIV/AIDS HS and TA (HAHSTA). Annual Epidemiology & Surveillance Report: Data Through December 2018. (2019). Available online at: http://doh.dc.gov/sites/default/files/dc/sites/doh/page_content/attachments/2013 (annual report final edit.pdf).
2. Joint United Nations Programme on HIV/AIDS. Seizing the Moment: Tackling Entrenched Inequalities to End Epidemics. (2020). Available online at: https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-report_en.pdf (accessed March 12, 2023).
3. Myer L, Dunning L, Lesosky M, Hsiao NY, Phillips T, Petro G, et al. Frequency of viremic episodes in HIV-infected women initiating antiretroviral therapy during pregnancy: a cohort study. Clin Infect Dis. (2017) 64:422–7. doi: 10.1093/cid/ciw792
4. Chetty T, Newell ML, Thorne C, Coutsoudis A. Viraemia before, during and after pregnancy in HIV-infected women on antiretroviral therapy in rural KwaZulu-natal, South Africa, 2010–2015. Trop Med Int Health. (2018) 23:79–91. doi: 10.1111/tmi.13001
5. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic. (2014). Available online at: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf (accessed April 17, 2024).
6. Yotebieng M, Mpody C, Ravelomanana NLR, Tabala M, Malongo F, Kawende B, et al. HIV viral suppression among pregnant and breastfeeding women in routine care in the Kinshasa province: a baseline evaluation of participants in CQI-PMTCT study. J Int AIDS Soc. (2019) 22:1–12. doi: 10.1002/jia2.25376
7. Omonaiye O, Kusljic S, Nicholson P, Manias E. Medication adherence in pregnant women with human immunodeficiency virus receiving antiretroviral therapy in Sub-Saharan Africa: a systematic review. BMC Public Health. (2018) 18:805. doi: 10.1186/s12889-018-5651-y
8. Psaros C, Remmert JE, Bangsberg DR, Safren SA, Smit JA. Adherence to HIV care after pregnancy among women in Sub-Saharan Africa: falling off the cliff of the treatment cascade. Curr HIV/AIDS Rep. (2015) 12:1–5. doi: 10.1007/s11904-014-0252-6
9. Cowing M, Davino-Ramaya CM, Ramaya K, Szmerekovsky J. Health care delivery performance: service, outcomes, and resource stewardship. Perm J. (2009) 13:72–8. doi: 10.7812/tpp/08-100
10. Johnson RA, Kast FE, Rosenzweig JE. Systems theory and management. Manage Sci. (1964) 10(2):367–84. doi: 10.1287/mnsc.10.2.367
11. Yotebieng M, Behets F, Kawende B, Ravelomanana NLR, Tabala M, Okitolonda EW. Continuous quality improvement interventions to improve long-term outcomes of antiretroviral therapy in women who initiated therapy during pregnancy or breastfeeding in the Democratic Republic of Congo: design of an open-label, parallel, group randomized. BMC Health Serv Res. (2017) 17:306. doi: 10.1186/s12913-017-2253-9
12. MEASURE Evaluation USAID. Profiles of Health Facility Assessment Methods MEASURE Evaluation USAID. (2008). Available online at: tr-06-36.pdf (accessed April 21, 2024).
13. World Health Organization (WHO). Service Availability and Readiness Assessment (SARA): An Annual Monitoring System for Service Delivery: Reference Manual, Version 2.2 2013. Available online at: https://cdn.who.int/media/docs/default-source/service-availability-and-readinessassessment(sara)/sara_reference_manual_chapter3.pdf (accessed April 17, 2024).
14. Cohan D, Natureeba P, Koss CA, Plenty A, Luwedde F, Mwesigwa J, et al. Efficacy and safety of lopinavir/ritonavir versus efavirenz-based antiretroviral therapy in HIV-infected pregnant Ugandan women. AIDS. (2015) 29:183–91. doi: 10.1097/qad.0000000000000531
15. Koss CA, Natureeba P, Nyafwono D, Plenty A, Mwesigwa J, Nzarubara B, et al. Brief report: food insufficiency is associated with lack of sustained viral suppression among HIV-infected pregnant and breastfeeding Ugandan women. J Acquir Immune Defic Syndr. (2016) 71:310–5. doi: 10.1097/qai.0000000000000860
16. Sam-Agudu NA, Ramadhani HO, Isah C, Anaba U, Erekaha S, Fan-Osuala C, et al. The impact of structured mentor mother programs on 6-month postpartum retention and viral suppression among HIV-positive women in rural Nigeria: a prospective paired cohort study. J Acquir Immune Defic Syndr. (2017) 75(Suppl 2):S173–81. doi: 10.1097/qai.0000000000001346
17. Gill MM, Hoffman HJ, Bobrow EA, Mugwaneza P, Ndatimana D, Ndayisaba GF, et al. Detectable viral load in late pregnancy among women in the Rwanda option B+ PMTCT program: enrollment results from the Kabeho study. PLoS One. (2016) 11:e0168671. doi: 10.1371/journal.pone.0168671
18. Onoya D, Sineke T, Brennan AT, Long L, Fox MP. Timing of pregnancy, postpartum risk of virologic failure and loss to follow-up among HIV-positive women. AIDS. (2017) 31:1593–602. doi: 10.1097/qad.0000000000001517
19. Denoeud-Ndam L, Fourcade C, Ogouyemi-Hounto A, Azon-Kouanou A, d’Almeida M, Azondékon A, et al. Predictive factors of plasma HIV suppression during pregnancy: a prospective cohort study in Benin. PLoS One. (2013) 8:e59446. doi: 10.1371/journal.pone.0059446
20. Chagomerana MB, Miller WC, Tang JH, Hoffman IF, Mthiko BC, Phulusa J, et al. Optimizing prevention of HIV mother to child transmission: duration of antiretroviral therapy and viral suppression at delivery among pregnant Malawian women. PLoS One. (2018) 13:e0195033. doi: 10.1371/journal.pone.0195033
21. Matthews LT, Ribaudo HB, Kaida A, Bennett K, Musinguzi N, Siedner MJ, et al. HIV-infected Ugandan women on antiretroviral therapy maintain HIV-1 RNA suppression across periconception, pregnancy, and postpartum periods. J Acquir Immune Defic Syndr. (2016) 71:399–406. doi: 10.1097/qai.0000000000000874
22. Koss CA, Natureeba P, Mwesigwa J, Cohan D, Nzarubara B, Bacchetti P, et al. Hair concentrations of antiretrovirals predict viral suppression in HIV-infected pregnant and breastfeeding Ugandan women. AIDS. (2015) 29:825–30. doi: 10.1097/qad.0000000000000619
23. Myer L, Phillips TK, McIntyre JA, Hsiao NY, Petro G, Zerbe A, et al. HIV viraemia and mother-to-child transmission risk after antiretroviral therapy initiation in pregnancy in Cape Town, South Africa. HIV Med. (2017) 18:80–8. doi: 10.1111/hiv.12397
24. Mpody C, Thompson P, Tabala M, Ravelomanana NLR, Malongo F, Kawende B, et al. Hepatitis B infection among pregnant and post-partum women living with HIV and on antiretroviral therapy in Kinshasa, DR Congo: a cross-sectional study. PLoS One. (2019) 14:1–14. doi: 10.1371/journal.pone.0216293
25. Yotebieng M, Moracco KE, Thirumurthy H, Edmonds A, Tabala M, Kawende B, et al. Conditional cash transfers improve retention in PMTCT services by mitigating the negative effect of not having money to come to the clinic. J Acquir Immune Defic Syndr. (2017) 74:150–7. doi: 10.1097/QAI.0000000000001219
26. Vreeman RC, Nyandiko WM, Braitstein P, Were MC, Ayaya SO, Ndege SK, et al. Acceptance of HIV testing for children ages 18 months to 13 years identified through voluntary, home-based HIV counseling and testing in western Kenya. J Acquir Immune Defic Syndr. (2010) 55:e3–10. doi: 10.1097/QAI.0b013e3181f0758f
27. Horwood C, Voce A, Vermaak K, Rollins N, Qazi S. Routine checks for HIV in children attending primary health care facilities in South Africa: attitudes of nurses and child caregivers. Soc Sci Med. (2010) 70:313–20. doi: 10.1016/j.socscimed.2009.10.002
28. Modi S, Broyles LN, Montandon M, Itoh M, Ochanda B, Langat A, et al. Beyond early infant diagnosis: changing the approach to HIV-exposed infants. J Acquir Immune Defic Syndr. (2018) 78:S107–14. doi: 10.1097/qai.0000000000001736
29. Chopra M, Daviaud E, Pattinson R, Fonn S, Lawn JE. Saving the lives of South Africa’s mothers, babies, and children: can the health system deliver? Lancet. (2009) 374:835–46. doi: 10.1016/S0140-6736(09)61123-5
30. Doherty T, Chopra M, Nsibande D, Mngoma D. Improving the coverage of the PMTCT programme through a participatory quality improvement intervention in South Africa. BMC Public Health. (2009) 9:406. doi: 10.1186/1471-2458-9-406
31. Agyepong IA. Reforming health service delivery at district level in Ghana: the perspective of a district medical officer. Health Policy Plan. (1999) 14:59–69. doi: 10.1093/heapol/14.1.59
32. Lipira L, Kemp C, Domercant JW, Honore JG, Francois K, Puttkammer N. The role of service readiness and health care facility factors in attrition from option B+ in Haiti: a joint examination of electronic medical records and service provision assessment survey data. Int Health. (2018) 10:54–62. doi: 10.1093/inthealth/ihx060
33. Shrinivas D, Panditrao M, Ritu P, Vinay K, Sanjeevani K, Janssen F. Systematic review of public health research on prevention of mother-to-child transmission of HIV in India with focus on provision and utilization of cascade of PMTCT services. BMC Public Health. (2012) 12(2 May 2012). doi: 10.1186/1471-2458-12-320
34. Gils T, Bossard C, Verdonck K, Owiti P, Casteels I, Mashako M, et al. Stockouts of HIV commodities in public health facilities in Kinshasa: barriers to end HIV. PLoS One. (2018) 13:e0191294. doi: 10.1371/journal.pone.0191294
35. Nsibu CN, Manianga C, Kapanga S, Mona E, Pululu P, Aloni MN. Determinants of antenatal care attendance among pregnant women living in endemic malaria settings: experience from the Democratic Republic of Congo. Obstet Gynecol Int. (2016) 2016:5423413. doi: 10.1155/2016/5423413
36. Kitahata MM, Gange SJ, Abraham AG, Merriman B, Saag MS, Justice AC, et al. Effect of early versus deferred antiretroviral therapy for HIV on survival. N Engl J Med. (2009) 360:1815–26. doi: 10.1056/NEJMoa0807252
37. Nachega JB, Hislop M, Dowdy DW, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann Intern Med. (2007) 146:564–73. doi: 10.7326/0003-4819-146-8-200704170-00007
38. Smit PW, Sollis KA, Fiscus S, Ford N, Vitoria M, Essajee S, et al. Systematic review of the use of dried blood spots for monitoring HIV viral load and for early infant diagnosis. PLoS One. (2014) 9:1–8. doi: 10.1371/journal.pone.0086461
39. Garrido C, Zahonero N, Corral A, Arredondo M, Soriano V, De Mendoza C. Correlation between human immunodeficiency virus type 1 (HIV-1) RNA measurements obtained with dried blood spots and those obtained with plasma by use of Nuclisens EasyQ HIV-1 and Abbott RealTime HIV load tests. J Clin Microbiol. (2009) 47:1031–6. doi: 10.1128/JCM.02099-08
Keywords: antiretroviral therapy, virological suppression, pregnant and breastfeeding women living with HIV, ART service readiness, Democratic Republic of Congo, maternal and child health clinics
Citation: Boisson-Walsh A, Ravelomanana NLR, Tabala M, Malongo F, Kawende B, Babakazo P and Yotebieng M (2024) Association of comprehensiveness of antiretroviral care and detectable HIV viral load suppression among pregnant and postpartum women in the Democratic Republic of the Congo: a cross-sectional study. Front. Glob. Womens Health 5:1308019. doi: 10.3389/fgwh.2024.1308019
Received: 5 October 2023; Accepted: 21 May 2024;
Published: 5 June 2024.
Edited by:
Grant Murewanhema, University of Zimbabwe, ZimbabweReviewed by:
Carl Lombard, South African Medical Research Council, South AfricaRaphael Zozimus Sangeda, Muhimbili University of Health and Allied Sciences, Tanzania
© 2024 Boisson-Walsh, Ravelomanana, Tabala, Malongo, Kawende, Babakazo and Yotebieng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alix Boisson-Walsh, YWJvaXNzb253YWxzaEBnbWFpbC5jb20=