 Elizabeth A. Mosley1*
Elizabeth A. Mosley1* Sequoia Ayala2Zainab Jah2,3Tiffany Hailstorks1,4Dázon Dixon Diallo2Natalie Hernandez5Kwajelyn Jackson6Indya Hairston2Kelli S. Hall1,7
Sequoia Ayala2Zainab Jah2,3Tiffany Hailstorks1,4Dázon Dixon Diallo2Natalie Hernandez5Kwajelyn Jackson6Indya Hairston2Kelli S. Hall1,7- 1Center for Reproductive Health Research in the Southeast (RISE), Emory University School of Public Health, Atlanta, GA, United States
- 2SisterLove, Inc., Atlanta, GA, United States
- 3National Birth Equity Collaborative, Washington, DC, United States
- 4Department of Gynecology and Obstetrics, Emory University School of Medicine, Atlanta, GA, United States
- 5Center for Maternal Health Equity, Morehouse School of Medicine, Atlanta, GA, United States
- 6Feminist Women's Health Center, Atlanta, GA, United States
- 7Department of Population and Family Health, Columbia University Mailman School of Public Health, New York, NY, United States
Introduction: While reproductive injustice indicators are improving globally, they are worsening in the United States particularly for Black and other marginalized communities. Eugenics and obstetric violence against low-income and communities of color create well-founded distrust of sexual and reproductive health (SRH). Transformational, reparative ways of conducting SRH research are needed.
Proposed principles of community-led research for reproductive justice: Drawing on our collective experience as reproductive justice leaders, SRH researchers, and clinicians, we propose the following principles of community-led research for reproductive justice: 1) Center the marginalized community members most affected by SRH inequities as leaders of research; 2) Facilitate equitable, collaborative partnership through all phases of SRH research; 3) Honor multiple ways of knowing (experiential, cultural, empirical) for knowledge justice and cross-directional learning across the team; 4) Build on strengths (not deficits) within the community; 5) Implement the tenets of reproductive justice including structural-level analysis and the human rights framework; 6) Prioritize disseminating useful findings to community members first then to other audiences; 7) Take action to address social and reproductive injustices.
SisterLove's community-led georgia medication abortion project: We offer the community-led Georgia Medication Abortion (GAMA) Project by reproductive justice organization SisterLove from 2018–2022 as a case study to demonstrate these principles along with the strengths and challenges of reproductive justice research.
Discussion: Community-led reproductive justice research offers innovative and transformational methods for truly advancing SRH in an era of increasing policy restrictions and decreasing access to care. Yet existing funding, research administrative, and publishing systems will require structural change.
Introduction
Current landscape of U.S. reproductive health
While reproductive health and justice indicators are improving globally, they are worsening in the United States (1–3). For every 100,000 U.S. live births, there are 17 maternal deaths—over double that of other high-income nations (1). Non-Hispanic Black women die from pregnancy-related causes at 3 to 4 times the rate of non-Hispanic white women, and rates of maternal mortality are particularly high in the South (3). In Georgia, the statewide rate is 26 maternal deaths per 100,000 live births, but that is 17.4 for white Georgians and 47 for Black Georgians (4). Among high income nations, the United States also has the second-worst supply of midwives and obstetrician-gynecologists (only 15 per 1,000 live births) (1). Maternity care deserts are particularly dire across the rural South. In Georgia, an estimated 50% of counties have no OBGYN services and 40% of the state's rural labor and delivery units have closed since 1994 (5).
Despite the worsening maternal health crisis, conservative U.S. leaders continue to dismantle protections for abortion care. The Supreme Court of the United States is posed to overturn Roe v. Wade this month, thus eliminating federal abortion protection and allowing states to regulate or outlaw abortion (6, 7). Since Roe v. Wade in 1973, federal (e.g., the Hyde Amendment that prohibits federal funding to cover abortion for public insurance patients) and state-level (e.g., gestational age limits) policies have restricted access, particularly for people of color, low-income communities, and young people (8, 9). This creates treacherous double binds, particularly for Black and low-income people, who have the highest risk of maternal mortality and highest rates of abortion demand (due to poverty and lower access to contraception), but the worst barriers to safe abortion care (10).
Moreover, given historical and ongoing eugenics and obstetric violence against low-income and communities of color, they have widespread and well-founded medical distrust (11–14). Modern U.S. obstetric and gynecological techniques were developed on Black enslaved women, who did not consent and were given no anesthesia (15). The U.S. eugenics movement from 1900 to the 1970s—based in racist, classist, and ableist “science” and aimed at eliminating “social ills” through population control—forcibly sterilized over 60,000 individuals (14). Most of them were living with disabilities, from low-income backgrounds, or people of color. In fact, incarcerated and detained Latina women in the U.S. continue to be forcibly sterilized—most recently in 2020 at a detention center in rural Georgia (16, 17). And early U.S. contraceptive trials were conducted on Latinx Puerto Rican women, which resulted in infertility, reproductive cancers, and other health consequences (18).
Given this context, we need transformational, reparative ways of conducting SRH research that advance a human rights framework for reproductive justice—in the United States and globally.
Reproductive justice framework and movement
Reproductive justice is an intersectional feminist theoretical framework, community organizing strategy, and social movement that is well-suited for transformational and reparative research and praxis (19, 20). It was first developed in the 1980s by Founding Mothers of color (including co-author Dázon Dixon Diallo1), who were marginalized by the white-led reproductive rights movement both in the United States and in global forums (such as the 1994 United Nations International Conference on Population and Development in Cairo) that focused almost exclusively on contraceptive and abortion access (19, 20). Grounded in the comprehensive human rights framework (21–24), reproductive justice leaders call for an expansive approach to sexual and reproductive autonomy that centers the experiences of Black, Brown, indigenous, immigrant, LGBTQ, and other marginalized communities (25–27). It uses an intersectional framework, based on Kimberlé Crenshaw (28) and other scholars' work, that emphasizes how social systems of oppression—such as racism, sexism, ethnocentrism, capitalism, colonialism, ableism, heterosexism—intersect and create unique experiences of social disadvantage and privilege. In other words, the SRH struggles of high-income white cisgender women (e.g., legal access to abortion and contraception) are distinct from the SRH struggles of low-income queer women of color (e.g., forced sterilization, low wages, employment and housing discrimination). Because of these intersectional oppressions and identities, true reproductive autonomy cannot be achieved for all without fulfillment of these conditions:
• The human right to have children.
• The human right not to have children.
• The human right to parent one's children in safe, supportive environments.
• Free of reproductive coercion or violence.
Today, the reproductive justice movement has grown to include hundreds of community-based organizations across the United States and internationally, who are leading grassroots social movements for voting rights, safe working and housing conditions, healthcare access, and more.
Community-engaged and participatory action research
Traditional research approaches, where academic researchers are upheld as experts and community members most affected by negative health outcomes are exploited for data, are antithetical to reproductive justice and counter-productive for achieving SRH equity. Conversely, reproductive justice leaders utilize a research justice (29) approach, wherein Black, indigenous, and other marginalized community members are equally valued as experts. A research justice approach challenges the traditional knowledge hierarchy, where mainstream so-called scientific knowledge is privileged (has greater political power) over other ways of knowing: experiential, cultural, and spiritual knowledge. This is well aligned with community-based participatory research methods and similar approaches like community-engaged research and participatory action research (30, 31). Community-based participatory research is guided by these principles:
• Acknowledge community as a unit of identity.
• Build on community strengths and resources.
• Facilitate collaborative, equitable partnership in all phases of the research.
• Foster co-learning among all partners.
• Integrate and achieve a balance between knowledge generation and intervention.
• Focus on local relevance and multi-level ecological perspectives.
• Involve systems development using cyclical, iterative processes.
• Disseminate results to all partners, who are all involved in dissemination efforts.
• Engage in long-term process and commitment to sustainability (31).
Proposed principles of community-led research for reproductive justice
Rooted in the reproductive justice and community-engaged research approaches and drawing from our collective experience as reproductive justice advocates, community-engaged SRH researchers, and clinicians, we propose these corresponding yet more specific principles of community-led research for reproductive justice (see Table 1):
• Center the marginalized community members most affected by SRH inequities as leaders of research
• Facilitate equitable, collaborative partnership through all phases of SRH research
• Honor multiple ways of knowing (experiential, cultural, empirical) for knowledge justice and cross-directional learning across the team
• Build on strengths (not deficits) within the community
• Implement the tenets of reproductive justice including structural-level analysis and the human rights framework
• Prioritize disseminating useful findings to community members first then to other audiences
• Take action to address social and reproductive injustices
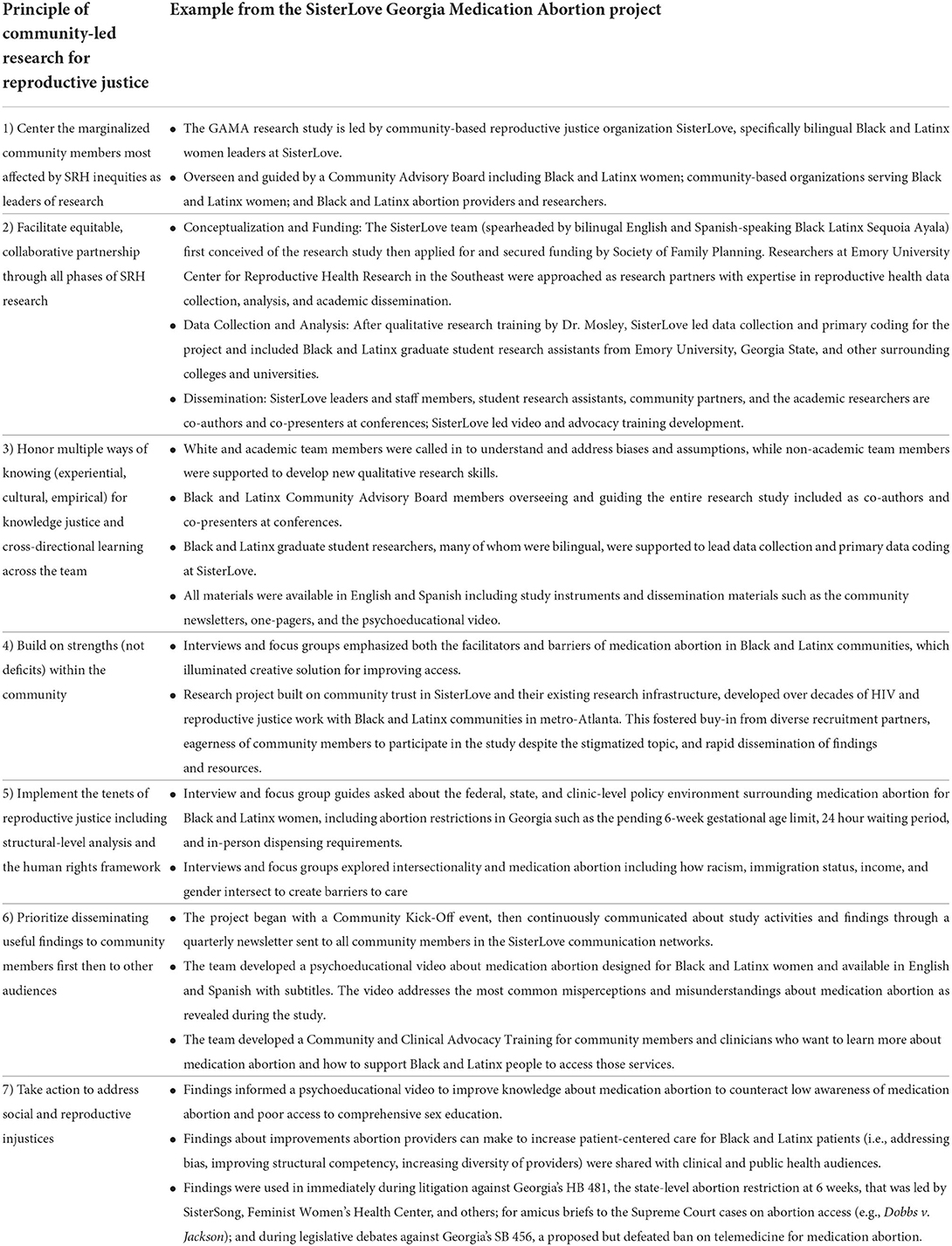
Table 1. Principles of community-led research for reproductive justice in the SisterLove Georgia medication abortion project.
Case study: The Georgia Medication Abortion project by SisterLove
Study overview
We offer the community-led Georgia Medication Abortion (GAMA) Project from 2018–2022 as a case study to demonstrate these principles. The study was first conceptualized by bilingual, Black, and Latinx co-author Sequoia Ayala at SisterLove—an HIV and reproductive justice organization focused on women affected by HIV in metro-Atlanta since 1989. Ayala had observed disproportionate barriers to medication abortion for Black women and saw the need to investigate medication abortion perceptions and experiences among Black and other women of color. Meanwhile, the Society of Family Planning Research Fund had opened a medication abortion funding opportunity, to which SisterLove applied. With great excitement about this novel community-led approach, the Society of Family Planning invited SisterLove to submit a full proposal, but encouraged them to partner with a local academic research center to increase rigor of the proposed research methods. SisterLove intentionally selected Emory University's Center for Reproductive Health Research in the Southeast (RISE) given the University's positive research partnership record with SisterLove and given RISE's emphasis on reproductive health equity research, practice, and policy. Specifically, the RISE team included two monolingual, White researchers (Elizabeth Mosley and Kelli Hall) and one monolingual Black clinician-researcher and abortion provider (Tiffany Hailstorks). Collaboratively, the SisterLove and RISE team proposed a mixed methods study to explore Black and Latinx women's perceptions and experiences with medication abortion in Georgia. Our proposal was funded and became the first community-led research study by the Society of Family Planning. Notably, all Society of Family Planning funding applications now require explicit attention to community engagement, partnership, and dissemination.
The SisterLove-RISE team hosted a community kick-off event then organized a Community Advisory Board (CAB) with Black and Latinx women, researchers specializing in Black and Latinx reproductive health (including co-author Natalie Hernandez) Black and Latinx community-based organizations, abortion providers and clinic administrators (including co-author Kwajelyn Jackson), and religious leaders. This CAB helped develop data collection instruments; recruit participants; interpret preliminary results; and disseminate findings at conferences, in manuscripts, at clinics, and in community. From April 2019 to December 2020, the team conducted 10 key informant interviews with abortion providers (broadly defined to include physicians, nurses, receptionists, educators, administrators, and abortion funds) and 10 with leaders of Black and Latinx community-based organizations; 32 in-depth interviews with Black and Latinx women, and 6 focus groups with Black and Latinx women. The abortion provider interviews covered experiences with Black and Latinx abortion patients, their abortion method preferences and choices, and the facilitators and challenges of access. The Black and Latinx community-based organization interviews covered perspectives on abortion, awareness of medication abortion, and perceived barriers and facilitators of abortion access for their Black and Latinx clients. The in-depth interviews with Black and Latinx women covered awareness, knowledge, perspectives, and personal experiences with medication abortion as well as suggested solutions for improving access. Finally, the focus groups explored public attitudes toward medication abortion. Interviews and focus groups were conducted, transcribed, and analyzed by Black and/or Latinx Graduate Research Assistants at SisterLove with training and guidance from RISE researchers. Thematic analysis utilized memo-ing, coding, matrices, and group discussion to connect across codes, look for group differences (e.g., between Black and Latinx women, between patients and providers), and develop overarching themes.
Main findings from the Georgia Medication Abortion project
The SisterLove-RISE team identified four overarching themes about medication abortion among Black and Latinx women. First, at the socio-cultural level, intersectional oppression, intersectional stigma, and medical exploitation of Black and Latinx communities lead to systemic barriers. For example, participants shared how population control and medical experimentation on Black and Latinx communities has led to distrust and fear of taking medication abortion pills, particularly from White providers. To address these barriers at the socio-cultural level, participants suggested medication abortion social marketing campaigns and story-sharing. Second, at the policy level, participants described how policies from the federal (e.g., Hyde amendment), state (e.g., Georgia's impending 6-week gestational age limit), and institutional level (e.g., in-clinic medication abortion requirements) disproportionately affect Black and Latinx women. They emphasized the importance of policy advocacy and political engagement to improve policies at the national and state level, while encouraging clinics to center Black and Latinx patients in their protocols for patient-centered, equitable access to care. Third, at the clinic and provider levels, participants described factors that inadvertently made abortion services less accessible or less patient-centered for Black and Latinx patients. This included lack of representative (Black, Latinx, Spanish-speaking) abortion providers and clinic staff, provider knowledge gaps in structural competency, implicit provider bias (e.g., recommending surgical abortion and not offering medication abortion to Black patients because of adherence concerns), and high costs of medication abortion. Solutions included diversifying the abortion clinic team, flexible scheduling, sliding scale fees, holistic reproductive justice abortion funds, and de-medicalization including at-home telemedicine for medication abortion. Finally, at the individual-level, Black and Latinx women faced numerous barriers including “lack of information…education… money…fear of…shaming…lack of public transportation…fear of [immigration] raids.” In other words, the common stigma-related barriers to medication abortion are compounded by “all the things that make life difficult” for Black and Latinx communities. Participants offered inspiring solutions including social support (e.g., from one's own network and from abortion doulas, holistic reproductive justice abortion funds) and word-of-mouth story-telling by Black and Latinx people about medication abortion.
Community-based and policy-focused dissemination of findings
The study's main findings have been presented at conferences, as published abstracts, and are currently under review with peer-reviewed journals (32, 33). More importantly, the findings have been disseminated back to Black and Latinx communities in metro-Atlanta and beyond through quarterly newsletters, fact sheets about medication abortion, a psychoeducational video, and a community-clinical advocacy training. To address low levels of awareness and knowledge about medication abortion, the team developed a psychoeducational video about medication abortion designed specifically for and by Black and Latinx women (see Figure 1). The 2.5 min video is narrated by Damaris, a Black health educator at SisterLove, and set at the MotherHouse—a home-turned-office and clinic in Southwest Atlanta shared by SisterLove and the SisterSong Women of Color Reproductive Justice Collective. The video, available in English and Spanish, provides information about how medication abortion works and where to access it, addresses common misconceptions we heard in the GAMA study, and explains the policies regulating medication abortion. The psychoeducational video has been pilot tested with 850 people, which showed the video significantly increases knowledge and reduces racial/ethnic disparities in medication abortion knowledge. An ongoing evaluation with a representative sample of Black and Latinx women is being conducted, once updates are made for changes in telemedicine for abortion and the impending Supreme Court decision. After that, the video will be widely disseminated at abortion clinics, at reproductive health and justice organizations, on social media, and in sex education programs.

Figure 1. My health in my hands medication abortion psychoeducational video and the community-clinical advocacy training.
The team also developed a community-clinical advocacy training for community-based organizations and clinical providers, who want to learn more about medication abortion and support Black and Latinx community members to safely access medication abortion (see Figure 1). This webinar-style training is self-paced and provides more detailed instruction about medication abortion, policies regulating medication abortion, and how to connect people to medication abortion care. It is currently being pilot tested at SisterLove and will then be disseminated to Black and Latinx serving clinics and community-based organizations nationally.
Findings from GAMA were also leveraged for reproductive health policy advocacy including in amicus briefs for Supreme Court cases on abortion restriction well as for testimony and legislator education about state-level bans on telemedicine for abortion. Qualitative data from GAMA were included in the Dobbs v. Jackson case to emphasize how abortion restrictions disproportionate and unjustly affect Black and Latinx patients, as well as to catalog the numerous barriers they already face when trying to access abortion care. In 2022, conservative Georgia legislators introduced a ban on telemedicine for abortion (SB 456). This came shortly after the U.S. Food and Drug Administration had eliminated in-person physician dispensing of mifepristone and in the wake of COVID-19, when other in-person clinical requirements had been loosened. GAMA researcher Elizabeth Mosley testified twice against the bill, and she mentored GAMA Graduate Student Researcher Priya Shah to develop a legislator education toolkit about the safety of telemedicine for medication abortion, which was distributed to all Georgia legislators. SB 456 did not pass.
Strengths and challenges of SisterLove's Georgia Medication Abortion project
Notable strengths of this community-led reproductive justice approach to research include:
• Emphasis on community-based dissemination leading to timely, impactful community resources.
• Policy relevant data collected by advocacy-focused community organizations are efficiently and effectively leveraged for community organizing and policy advocacy.
• Capacity building for research within the communities most impacted by sexual and reproductive health disparities.
• Capacity building for community engagement, cultural humility, and structural competency among academic researchers.
• Novel findings imperative for improving reproductive health outcomes and equity, which are obscured by traditional research methods.
Despite these successes, the project faced structural challenges including:
• Underfunding of community-led and community-engaged research by federal, foundation, and other funders.
• Project team member turnover for both the community and academic partners.
• Institutional barriers to community-academic research collaboration.
• Devaluation of community-engaged research at leading family planning peer-reviewed journals.
SisterLove, like all community-based and reproductive justice organizations, is structurally under-funded. For example, the GAMA project originally proposed a state-wide survey in addition to the qualitative study—all in 2 years. With a budget of only $300,000, our team lacked the staff capacity and resources to execute a full mixed methods study in that timeline. Ultimately, we prioritized the psychoeducational video and community-clinical advocacy training over the quantitative survey, because this was of greatest importance to community members. Another major challenge was team turnover both at SisterLove and RISE. Institutional barriers to community-academic collaborations included requirement of IRB approval before any funding is released, academic professional advancement requiring peer-reviewed and first-author publications in high impact journals, and relatively lower capacity at community-based organizations to be the primary administrator of large research grants. Finally, as the team has turned toward academic dissemination via publishing in peer-reviewed journals, we met startling resistance from some SRH colleagues. When submitting our results to leading SRH journals, we mostly received constructive feedback and encouragement. However, there were still reviewers who called community-led research “less rigorous” and accused us of prejudice against white abortion providers.
Discussion
Community-led reproductive justice research offers innovative and transformational methods for truly advancing SRH. This approach is needed in the United States now more than ever given the impending overturn of Roe v. Wade and with it the federal protection of abortion rights. States controlled by conservative governments, such as Georgia, will severely restrict access to abortion (i.e., at 6 weeks or possibly worse). This will undoubtedly affect Black, Latinx, and low-income communities most. The GAMA project led by SisterLove offers an important example of how community-led reproductive justice research can produce high-quality scientific evidence, disseminate benefits back to affected communities, and advocate against unjust reproductive healthcare restrictions. Yet existing funding, research administration, and publishing systems are not designed for community-led research for reproductive justice. Private foundations, federal institutions (e.g., National Institutes of Health), universities, professional organizations (e.g., Society of Family Planning, American College of Obstetricians and Gynecologists), and peer-reviewed journals will require considerable evolution to promote research and SRH equity.
Data availability statement
De-identified qualitative datasets generated for this study can be accessed by contacting SisterLove, Inc. at cmVzZWFyY2hAc2lzdGVybG92ZS5vcmc= for an application. Requests to access the datasets should be directed to cmVzZWFyY2hAc2lzdGVybG92ZS5vcmc=.
Ethics statement
The studies involving human participants were reviewed and approved by Emory University Institutional Review Board. The participants provided their verbal informed consent to participate in this study.
Author contributions
EM wrote the first draft of this manuscript. SA, ZJ, TH, DD, NH, KJ, IH, and KH provided revisions on the manuscript. SA originally conceived of the Georgia Medication Abortion project. DD, KH, SA, EM, and IH secured original and ongoing funding for the Georgia Medication Abortion project. SA, ZJ, and IH coordinated research for the Georgia Medication Abortion project including all data collection and analysis. KJ and NH led the Community Advisory Board including instrument development, recruitment, and dissemination. All authors contributed to the article and approved the submitted version.
Funding
The Georgia Medication Abortion Project is funded by the Society of Family Planning Research Fund, an Anonymous Foundation, and through the Center for Reproductive Health Research in the Southeast (RISE) including support from the Collaborative for Gender and Reproductive Equity, a sponsored project of Rockefeller Philanthropy Advisors.
Acknowledgments
We would like to thank all members of the Georgia Medication Abortion Community Advisory Board and partnering organizations including Feminist Women's Health Center, Caminar Latino, and the Center for Black Women's Wellness.
Conflict of interest
Author EM works as a consultant for SisterLove, Inc. providing community-based qualitative research methods training. Authors SA, ZJ, DD, and IH are employed by SisterLove, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor MM declared a past co-authorship with the author SA.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Founding Mothers of reproductive justice also include Toni M. Bond Leonard, Reverend Alma Crawford, Evelyn S. Field, Terri James, Bisola Marignay, Cassandra McConnell, Cynthia Newbille, Loretta Ross, Elizabeth Terry, ‘Able' Mable Thomas, Winnette P. Willis, and Kim Youngblood.
References
1. Tikkanen R, Gunja MZ, FizGerald M, Zephyrin L. Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries. The Commonwealth Fund. (2020). (Improving Health Care Quality). Available from: https://www.commonwealthfund.org/publications/issue-briefs/2020/nov/maternal-mortality-maternity-care-us-compared-10-countries (accessed May 3, 2021)
2. Louis JM, Menard MK, Gee RE. Racial and ethnic disparities in maternal morbidity and mortality. Obstetr Gynecol. (2015) 125:690–4. doi: 10.1097/AOG.0000000000000704
3. Building U,.S. Capacity to Review Prevent Maternal Deaths. Report from Nine Maternal Mortality Review Committees [Internet]. Review to Action; (2018). Available online at: http://reviewtoaction.org/Report_from_Nine_MMRCs (accessed January 3, 2022)
4. Department of Public Health Maternal Mortality Review Committee. Maternal Mortality Report 2014. Atlanta, GA: Department of Public Health (2019). Available online at: https://dph.georgia.gov/document/publication/maternal-mortality-2014-case-review/download (accessed May 3, 2021)
5. Zertuche A. Georgia's Obstetric Crisis. Origins, Consequences, and Potential Solutions. In: Georgia Senate Study Committee on Women's Adequate Healthcare. (2015).
6. Harris LH. Navigating loss of abortion services — a large academic medical center prepares for the overturn of Roe v. Wade. N Engl J Med. (2022) 386:2061–4. doi: 10.1056/NEJMp2206246
7. The New York Times. How state abortion laws could change if Roe is overturned. The New York Times. (2022). Available online at: https://www.nytimes.com/interactive/2022/us/abortion-laws-roe-v-wade.html (accessed Jun 9, 2022).
8. Redd SK, Rice WS, Aswani MS, Blake S, Julian Z, Sen B, et al. Racial/ethnic and educational inequities in restrictive abortion policy variation and adverse birth outcomes in the United States. BMC Health Serv Res. (2021) 21:1139. doi: 10.1186/s12913-021-07165-x
9. Upadhyay UD, Weitz TA, Jones RK, Barar RE, Foster DG. Denial of abortion because of provider gestational age limits in the United States. Am J Public Health. (2013) 104:1687–94. doi: 10.2105/AJPH.2013.301378
10. Dehlendorf C, Harris LH, Weitz TA. Disparities in abortion rates: A public health approach. Am J Public Health. (2013) 103:1772–9. doi: 10.2105/AJPH.2013.301339
11. Davis A. Racism, birth control, and reproductive rights. In: Feminist Postcolonial Theory- A reader. (2003). p. 353–67. doi: 10.1515/9781474470254-019
12. Davis DA. Obstetric racism: the racial politics of pregnancy, labor, and birthing. Med Anthropol. (2019) 38:560–73. doi: 10.1080/01459740.2018.1549389
13. Roberts D. Killing the Black Body: Race, Reproduction, and the Meaning of Liberty. New York: Random House LLC. (1997).
14. Schoen J. Choice & Coercion: Birth Control, Sterilization, and Abortion in Public Health and Welfare. Chapel Hill, NC: University of North Carolina Press. (2005).
15. Owens DC. Medical Bondage: Race, Gender, and the Origins of American Gynecology. 1st ed Athens, Georgia: University of Georgia Press. (2017). doi: 10.2307/j.ctt1pwt69x
16. Stern AM. Sterilized in the name of public health: race, immigration, and reproductive control in modern California. Am J Public Health. (2005) 95:1128–38. doi: 10.2105/AJPH.2004.041608
17. Judd A. At Georgia immigration jail, warnings about women's medical care went unheeded. The Atlanta Journal-Constitution. (2021). Available online at: https://www.ajc.com/news/at-georgia-immigration-jail-warnings-about-womens-medical-care-went-unheeded/NGAUKGZAXJGZLPZXTWZH5T3QWQ/ (accessed Jun 9, 2022).
18. Briggs L. Reproducing Empire Race, Sex, Science, U.S. Imperialism in Puerto Rico. 1st ed. California: University of California Press (2003). Available online at: https://www.ucpress.edu/book/9780520232587/reproducing-empire
19. Ross L. Understanding reproductive justice. Atlanta, Georgia: SisterSong; (2006). Available online at: http://www.trustblackwomen.org/our-work/what-is-reproductive-justice/9-what-is-reproductive-justice (accessed May 27, 2015).
20. Ross LJ. Reproductive justice as intersectional feminist activism. Souls. (2017) 19:286–314. doi: 10.1080/10999949.2017.1389634
21. United Nations Human Rights. International Covenant on Civil and Political Rights. United Nations Human Rights. (2014). Available online at: http://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx (accessed Oct 15, 2014).
22. United Nations. Convention on the Elimination of All Forms of Discrimination Against Women [Internet]. United Nations Treaty Collection. (2014). Available online at: https://treaties.un.org/pages/viewdetails.aspx?src=treaty&mtdsg_no=iv-8&chapter=4&lang=en (accessed September 28, 2014).
23. United Nations. International Covenant on Economic, Social, and Cultural Rights. (2022). http://www.unesco.org/new/en/social-and-human-sciences/themes/advancement/networks/larno/economic-social-and-cultural-rights/ (accessed August 2, 2022).
24. Assembly UNG. Universal Declaration of Human rRghts. United Nations; (1948). Available online at: http://www.tandfonline.com.proxy.lib.umich.edu/doi/abs/10.1080/00221473.1968.10619091?journalCode=ujrd18#.VB4suEtspIc (accessed September 20, 2014).
25. Pérez M. Queering Reproductive Justice. Rewire. (2007). Available online at: https://rewire.news/article/2007/05/31/queering-reproductive-justice/ (accessed May 31, 2007).
26. Asian Communities for Reproductive Justice. A New Vision for Advancing Our Movement for Reproductive Health, Reproductive Rights, and Reproductive Justice. Oakland, California; (2005). Available online at: http://strongfamiliesmovement.org/assets/docs/ACRJ-A-New-Vision.pdf (accessed May 29, 2015).
27. Luna Z, Luker K. Reproductive justice. Ann Rev Law Soc Sci. (2013) 9:327–52. doi: 10.1146/annurev-lawsocsci-102612-134037
28. Crenshaw K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. University of Chicago Legal Forum. (1989) 139–69.
29. Jolivétte AJ. Research Justice: Methodologies for Social Change. 1st ed. Bristol University Press. (2015). (Methodologies for social change). Available online at: http://www.jstor.org/stable/j.ctt1t89jrt.24 (accessed August 1, 2021).
30. Duran B, Oetzel J, Magarati M, Parker M, Zhou C, Roubideaux Y, et al. Toward health equity: a national study of promising practices in community-based participatory research. Progress Commun Health Partnerships. (2019) 13:337–52. doi: 10.1353/cpr.2019.0067
31. Israel B, Eng E, Schulz AJ, Parker E. Methods in Community-Based Participatory Research for Health. 2nd ed Jossey-Bass. (2013).
Keywords: community-led research, community-based participatory research, reproductive justice, abortion, reproductive coercion, medical distrust
Citation: Mosley EA, Ayala S, Jah Z, Hailstorks T, Dixon Diallo D, Hernandez N, Jackson K, Hairston I and Hall KS (2022) Community-led research for reproductive justice: Exploring the SisterLove Georgia Medication Abortion project. Front. Glob. Womens Health 3:969182. doi: 10.3389/fgwh.2022.969182
Received: 14 June 2022; Accepted: 26 July 2022;
Published: 12 August 2022.
Edited by:
Monica McLemore, University of California, San Francisco, United StatesReviewed by:
Aline Camille Gubrium, University of Massachusetts Amherst, United StatesCopyright © 2022 Mosley, Ayala, Jah, Hailstorks, Dixon Diallo, Hernandez, Jackson, Hairston and Hall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elizabeth A. Mosley, ZWFtb3NsZUBlbW9yeS5lZHU=