 Galana Mamo Ayana1
Galana Mamo Ayana1 Temam Beshir Raru1*
Temam Beshir Raru1* Alemayehu Deressa1
Alemayehu Deressa1 Lemma Demissie Regassa1
Lemma Demissie Regassa1 Mulugeta Gamachu2,3
Mulugeta Gamachu2,3 Belay Negash1
Belay Negash1 Abdi Birhanu2
Abdi Birhanu2 Bedasa Taye Merga1
Bedasa Taye Merga1
- 1School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
- 2School Medicine, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
- 3Department of Public Health, Rift Valley University, Harar, Ethiopia
Background: A miscarriage or a spontaneous loss of a pregnancy that occurs before the 20th week is an abortion. Even though numerous recommendations state that pregnant women should abstain from alcohol at all stages of pregnancy, alcohol intake among pregnant women is common. However, there are few papers addressing the effect of alcohol use on miscarriage using nationally representative data. Moreover, the association of alcohol use with abortion and its mechanisms is not well studied in the Ethiopian region. Therefore, the objective of the current study was to estimate the association of alcohol use with abortion rates among reproductive age (15–49) women in Ethiopia.
Methods: Using the most recent findings of the Ethiopian Demographic and Health Survey (EDHS), secondary data analysis was performed among pregnant women in Ethiopia. A total of 11,396 women between the ages of 15 and 49 years who were of reproductive age were included in the research. To characterize the study population, descriptive statistics were used. The variability was considered using the multilevel binary logistic regression model. A multilevel binary logistic model was used to determine the effect of alcohol intake on abortion while controlling for potential confounders. In the multivariable analysis, variables with a P-value of less than 0.05 were considered statistically significant for the response variable.
Results: The proportion of women who had an abortion was 10.46% with a 95% CI of 9.92–11.03. In the final model of the multilevel analysis, age group [adjusted odds ratio (AOR) = 6.13; 95% CI: 3.86–9.73], education level (AOR = 1.29; 95 and CI: 1.10–1.51), alcohol consumption (AOR = 1.38; 95% CI: 1.18–1.61), age at first sex (AOR = 1.20; 95% CI: 1.03–1.39), media exposure (AOR = 1.28, CI: 1.10–1.48), contraceptive use (AOR = 1.34, CI: 1.16–1.56), and occupation of respondent (AOR = 1.21, CI: 1.06–1.38) were identified to be significant determinants of abortion in Ethiopia.
Conclusion: Sexual and reproductive health education and family planning programs should target older women in the reproductive age group, women with primary educational status, working women, and those who initiated sexual intercourse at a younger age considering it could reduce abortion and unintended pregnancy. Furthermore, as part of sexual and reproductive health education, the adverse effect of alcohol consumption on abortion should be emphasized.
Background
Abortion, often known as a miscarriage or a spontaneous loss of pregnancy, occurs frequently before the 28th week all over the world (1, 2). Alcohol consumption during pregnancy in sub-Saharan Africa (SSA) was high, including in Ethiopia (3), and also alcohol consumption-related pregnancy loss among pregnant women was prevalent (4). The consumption of alcohol among pregnant women has been analyzed, and the potential consumption effects of these substances use majorly increase pregnancy loss among pregnant women (5, 6). Alcohol use during pregnancy is a serious public health issue since it has several detrimental impacts on the mother's and the unborn child's health (7).
There should be targeted interventions, screening programs, and education campaigns for women of childbearing age due to the high prevalence of alcohol consumption and binge drinking during pregnancy in some African nations (8). This is because these behaviors have been linked to a number of negative birth outcomes, including stillbirth, spontaneous abortion, intrauterine growth retardation, low birth weight, preterm birth, congenital malformations, and fetal alcohol spectrum disorder (8–10).
A prospective study conducted in northwest Ethiopia stated that the incidences of low birth weight, pregnancy loss, and stillbirth in Ethiopia were 12.63%, 6.05%, and 4.27%, respectively (11). Additionally, among those who only consume five drinks a week or less, every extra drink was linked to a 6% higher chance of miscarriage (12). In most circumstances, abortion cannot be stopped. However, by leading a healthy lifestyle and avoiding unhealthy risk factors, including smoking, secondhand smoke, alcohol use, and drug use, the odds of a healthy pregnancy may be enhanced and perhaps the risk of miscarriage can be reduced (13, 14). High levels of alcohol intake can result in insulin resistance and a high body mass index (BMI), both of which are risk factors for a higher chance of spontaneous miscarriage (15, 16).
Various studies have revealed that a large proportion of pregnant women still drink alcohol, which is a risk factor for abortion. However, to protect the baby intrauterine from hazards like abortion, they should have to abstain from doing so during their pregnancies (3, 17–19). Due to the fact that many expecting moms, especially those in Ethiopia, have not given enough thought to the consequences of alcohol use during pregnancy, a large percentage of pregnant women drink alcohol (20, 21).
The high prevalence of alcohol use during pregnancy may indicate that all women who are trying to conceive and pregnant women should receive comprehensive interventions and strategies to address the burden of the issue through antenatal care (ANC), reproductive health services, and other mechanisms. One of the few avoidable and modifiable risk factors for unfavorable pregnancy and delivery outcomes is alcohol use during pregnancy. However, Ethiopia lacks sufficient research that examines the effects of alcohol use on miscarriage or spontaneous abortion using nationally representative data. Moreover, the association of alcohol use with abortion and its mechanisms is not well studied in the region. Therefore, this aimed to find out whether alcohol use is associated with abortion in Ethiopia using a multilevel mixed-effects model.
Methods and Material
Study setting and data source
Secondary data analysis was conducted based on the 2016 EDHS data. The EDHS is a nationally representative survey conducted in the nine regional states [Afar; Amhara; Benishangul-Gumuz; Gambela; Harari; Oromia; Somali; Southern Nations, Nationalities, and People's Region (SNNPR); and Tigray] and two administrative cities (Addis Ababa and Dire Dawa) of Ethiopia every 5 years (22). The 2007 Population and Housing Census was used as the sampling frame for the EDHS, and a stratified two-stage cluster sampling procedure was used. In the initial stage, 645 enumeration areas (EAs) were chosen independently within each sampling stratum with a probability proportionate to the EA size. In the second stage, 28 households on average were systematically chosen. The full EDHS 2016 report contains detailed information on the sampling process (22).
The demographic and health survey (DHS) program's official database, www.measuredhs.com, was used for the purposes of the current investigation after permission was obtained through an online request that detailed the objectives of the study. From the individual Record (IR file) data set, significant independent and dependent factors were retrieved. The DHS program conducts face-to-face interviews with women of reproductive age (15–49 years) to obtain data on abortion/termination of pregnancy using a single dichotomous (Yes/No) question. The pertinent data were gathered from qualified ever-married women between the ages of 15 and 49 years.
Population
The source/study population for this study was all reproductive-age (15–49 years) women in the selected enumeration areas within 5 years before the survey in Ethiopia who were ever married. Specific women with no data for the outcome variable and alcohol use were excluded from the study. Accordingly, a total of 15,683 reproductive-age women were found from the 2016 DHS survey. From the total 15,683 reproductive-age women who were not ever married, who had no abortion, and who had alcohol consumption records were excluded from the study. Finally, 11,396 reproductive-age women who met the requirements for inclusion criteria were considered for final analysis.
Variables of the study
Outcome Variables
The study's dependent variable was abortion. The dichotomous answer variable is recorded as 1 if a woman has experienced an abortion and 0 if not.
Independent variables
Independent variables of the study were selected by reviewing previously conducted studies. The independent variables were age at first sex, age at marriage, current age, place of residence, marital status, education, occupation, alcohol consumption, cigarette smoking, wealth, region, number of children, contraceptive use, wanted pregnancy, and media exposure. Four statistical models were fitted for these independent variables. The first model was a null model, which was fitted without independent variables. The second model was Model I, which was fitted with individual-level variables (age at first sex, age at marriage, current age, marital status, education, occupation, alcohol consumption, cigarette smoking, wealth, number of children, contraceptive use, wanted pregnancy, and media exposure). The third model was Model II, which was fitted with community-level variables (residence and region). The fourth model was Model III, which was fitted with individual-level and community-level variables.
Data processing and management
Data were accessed and analyzed using STATA version 14 statistical software. The data were weighted using sampling weight, primary sampling unit, and strata before any statistical analysis to ensure the representativeness of the survey and to take into account the sampling design when calculating standard errors to get reliable statistical estimates.
Statistical analysis
Descriptive statistics were performed and summarized using tables, graphs, and texts. The frequency and percentage were used for categorical variables, and the mean with standard deviation was used to summarize the continuous variables. The important assumptions such as chi-square and multicollinearity assumptions were checked prior to fitting the statistical model. Since the participants in the same cluster share similar characteristics, the independence of observations and equal variance across clusters’ independence assumption was violated. Therefore, to ensure the reliability of standard errors and unbiased estimates, multilevel advanced statistical modeling is important to overcome the violated independence assumption and to consider the variability between clusters.
The bivariable multilevel mixed-effects logistic regression model was fitted for all independent variables, and the variables with P-value 0.20 in the bivariable multilevel mixed-effects logistic regression analysis were candidates for the multivariable two-stage mixed-effects logistic regression. Four different mixed-effects models were fitted (Table 1). A mixed-effects model with the lowest information criteria [Akaike information criteria (AIC) and Bayesian information criteria (BIC)] was selected. Variables with a P-value ≤0.05 were declared significant determinants of abortion. An odds ratio with a 95% confidence interval was used to measure the strength of the association. A fixed-effects submodel was used to estimate the association between abortion and explanatory variables. To measure cluster variations, an intra-class correlation coefficient (ICC) with standard deviation was used. In addition, the model comparison was done based on AIC and BIC.

Table 1. Basic characteristics of ever-married reproductive-age Women in Ethiopia.
Ethical approval
We obtained the data from the DHS website. It is accessible at http://www.dhsprogram.com after registration. The information gathered was solely for the purpose of conducting a research study. We kept all information private and avoided identifying any specific families or people. The National Research Ethics Review Committee (NRERC) of the Ministry of Science and Technology in Ethiopia and the Ethiopian Health Nutrition and Research Institute (EHNRI) Review Board have given their approval for EDHS.
Results
Women's characteristics
A total of 11,632 ever-married reproductive-age women were included in the final analysis. Most of the women (2,611, 22.44%) lie in the age group of 25–29 years. More than one-third (36.28%) of the women consume alcohol, but only 91 (0.78%) smoke cigarettes. Nearly two-thirds (67.19%) of the women had sex below the age of 18 years. Most of the women included were followers of the Orthodox religion (4,963, 42.66%) (Table 1).
Alcohol consumption
The proportion of women who had abortions was 10.46% with a 95% CI of 9.92–11.03. The highest [35.46% with 95% CI (32.82, 38.19)] and lowest [0.18% with 95% CI (0.05, 0. 67) abortion rates were reported in Oromia and Gambella, respectively. There is a significant association between abortion and the educational status of the mothers. The majority (60.60%) of the participants reported not having a formal education, while 4.04% had higher education. Alcohol consumption was significantly associated with abortion. The odds of abortion were 1.52 [crude odds ratio (COR) = 1.52; 95% CI: 1.30–1.76] times higher among the women who consume alcohol compared to those who did not consume (Table 2).
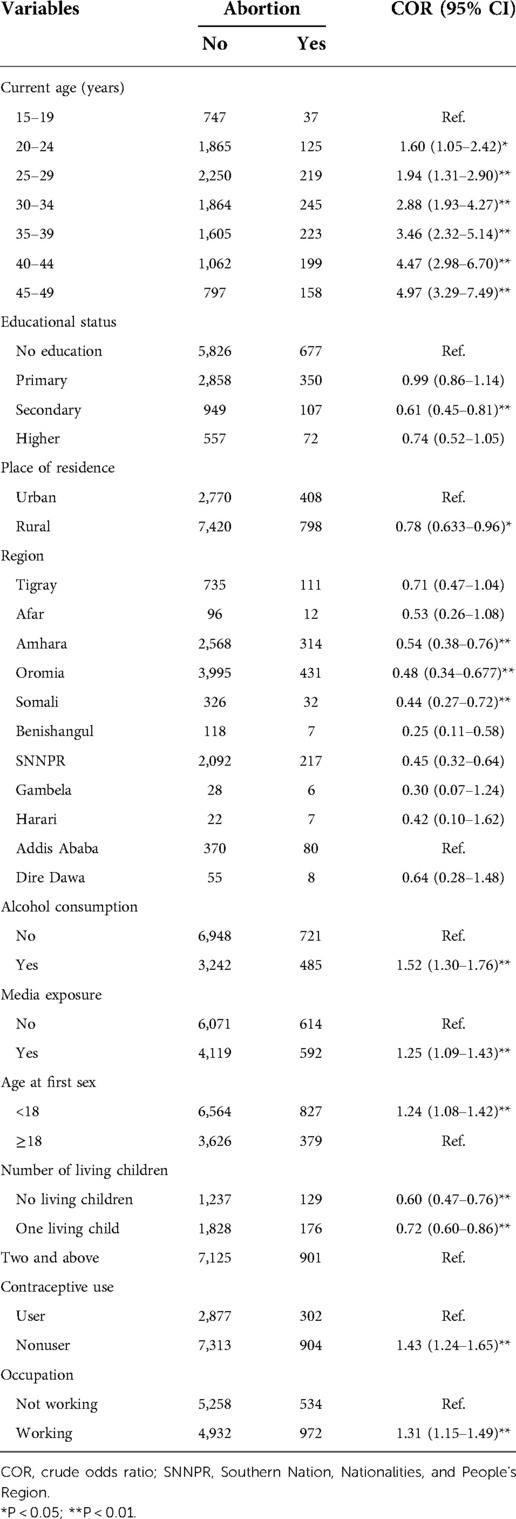
Table 2. Description of background factors associated with abortion and bivariable multilevel mixed-effects logistic regression in COR.
Determinants of abortion
Random effects
The null model's findings indicated no statistically significant variation in the odds of abortion, with a community variance of 0.35. The null model's ICC also indicated that only 9.62% of the total variation in the odds of abortion could be attributed to differences between communities, indicating that there are no cluster differences. Community variance in the individual-level model (model corrected for individual-level characteristics) was 0.34; an SE of 0.05 was still nonsignificant but decreased, and 9.40% of the overall variation of abortion might be attributed to the community, which still means that there are no cluster differences (Table 3).
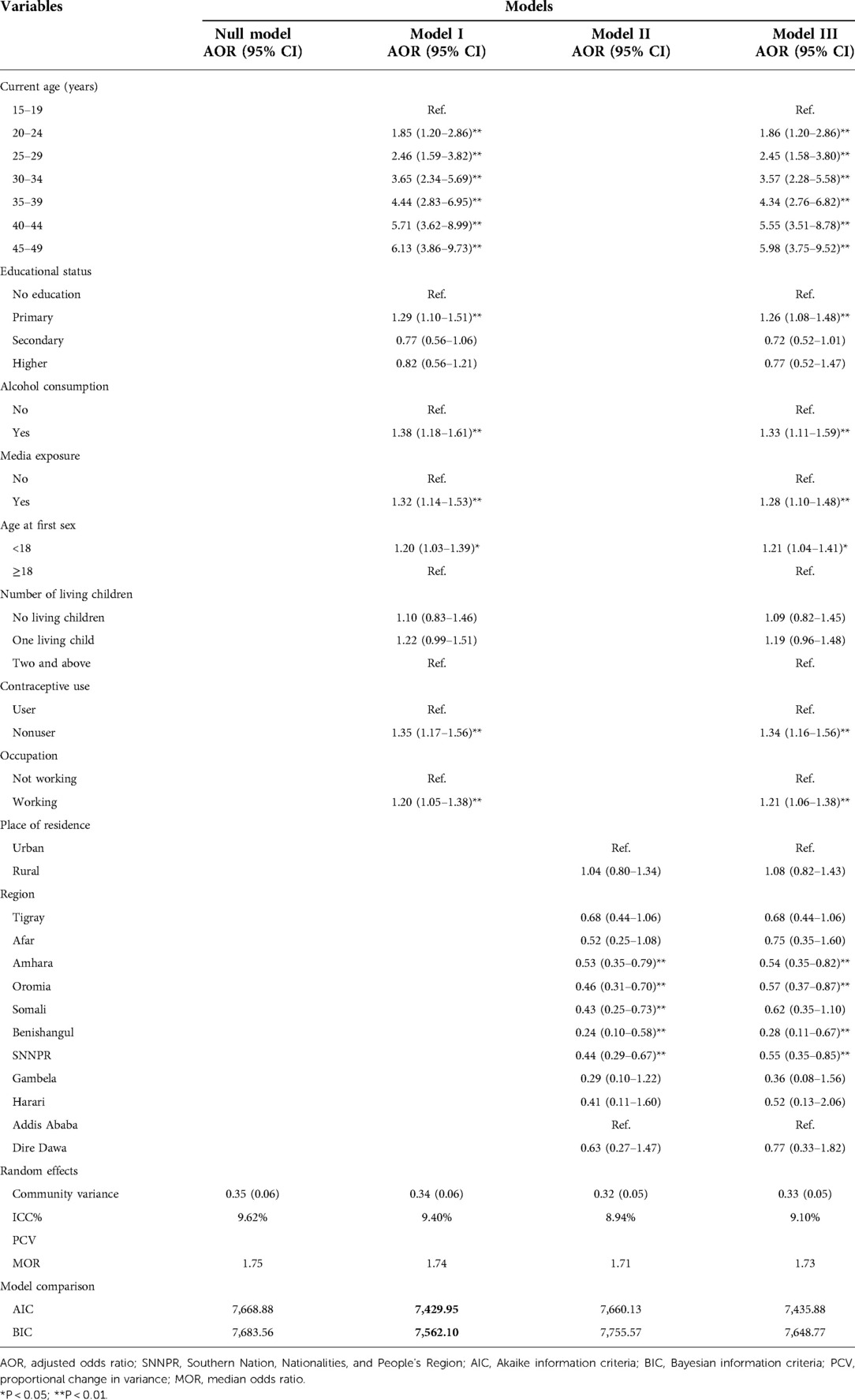
Table 3. Multivariable multilevel mixed-effects logistic regression analysis of factors associated with abortion among ever-married reproductive-age women in Ethiopia
Fixed effects
The interpretation of the fixed effects was based on the parsimonious model, which was determined to have lesser AIC and BIC. Compared to previous models, Model I was modified for only individual-level components with minimal AIC and BIC, and this model successfully fitted the data. Age, education, alcohol usage, media exposure, contraceptive use, age at first sex, and employment of the respondent were significant predictors of abortion in Ethiopia in the multivariable analysis at a 5% level of significance.
The odds of abortion were 6.13 [adjusted odds ratio (AOR) = 6.13; 95% CI: 3.86–9.73] times higher among the women in the age group of 45–49 years compared to the women in the age group of 15–19 years. The women who had primary education were 1.29 times more likely to have an abortion compared to those with no formal education (AOR = 1.29; 95 and CI: 1.10–1.51). Women who consume alcohol were 1.38 times more likely to have an abortion compared to their counterparts (AOR = 1.38; 95% CI: 1.18–1.61). Women who had their first sex below the age of 18 years were 1.20 times more likely to have an abortion compared to those who had their first sex at the age of 18 years and above (AOR = 1.20; 95% CI: 1.03–1.39) (Table 3).
Discussion
The current study depicts the association between alcohol consumption and abortion among ever-married reproductive-age women in Ethiopia. The odds of abortion among ever-married reproductive-age women who consume alcohol were higher compared to those who had no history of alcohol consumption. This is consistent with the available evidence on the relationship between alcohol and risky sexual behaviors. A narrative review conducted in sub-Saharan Africa concluded that alcohol was strongly associated with the increased practice of unsafe sexual intercourse including inconsistent condom use (23). The increased odds of abortion among alcohol consumers might be related to the associated risk of unprotected sex that results in unintended pregnancy and abortion.
Compared to their younger peers (15–19 years), older women (20–49 years) had a greater abortion rate. The results are consistent with the Nigerian DHS, which found that young adults aged 20–24 years had higher odds of abortion than those aged 15–19 years (24). Another study from Ethiopia also indicated that older age is associated with higher odds of abortion compared to younger women (25). The possible explanation might be the increased risk of medical and pregnancy-related complications that might make the pregnancy more difficult and raise the likelihood of an unfavorable pregnancy result, such as abortion (26). Furthermore, chromosomal abnormality risk rises with maternal age and uterine and hormonal function declines, all of which ultimately lead to miscarriage or abortion if women become pregnant later in life (27).
Compared to women who had not been exposed to the media, the likelihood of abortion was higher among those who had media exposure. This result is consistent with research from Ethiopia (25) and Ghana (28). This might be related to the access to information about the availability of abortion services (29). Moreover, women who have media exposure might know available laws related to abortion and be less stigmatized (30).
Educational status was identified as an independent determinant of abortion among ever-married reproductive-age women. Women who attended primary education had higher odds of abortion than women who had no formal education. This finding is supported by evidence from a study conducted in India (31). It could be due to the reason that educated women might have information about the consequence of abortion on their health and access to abortion services (29). As shown in this study, the odds of abortion increased among working women compared to those not working. Other previous studies revealed a significant relationship between abortion and higher socioeconomic status including working status (32, 33). This might be because working women may have the ability to cover the cost of maternal healthcare services. In addition, unemployed women may face cost barriers like transportation costs that could hinder women from having an abortion.
The current study pinpointed the association between contraceptive use and abortion among ever-married reproductive-age women. The odds of abortion were higher among contraceptive nonusers compared to those who were contraceptive users. This might be related to higher rates of unintended pregnancy among contraceptive nonusers that result in abortion (34, 35). Early sexual debut at younger than 18 years was positively associated with abortion. Previous studies also indicated that early initiation of sexual intercourse increased the rate of unintended pregnancy and abortion (36). This study provided evidence of the association between alcohol consumption and abortion among ever-married reproductive women. Moreover, factors such as older age, media exposure, primary education, contraceptive use, age at first sex, and working status have shown an association with abortion. Therefore, the current study recommends sexual and reproductive health education and family planning programs targeting older women, women with primary educational status, working women, and those who initiated sexual intercourse at a younger age to reduce abortion and unintended pregnancy. Furthermore, as part of sexual and reproductive health education, the adverse effect of alcohol consumption on pregnancy outcomes should be emphasized.
Strengths and limitations of the study
The study has certain limitations. The cross-sectional nature of the data made it difficult to infer any conclusions concerning causality. Alcohol consumption's effects on other variables and spontaneous abortion could only be detected in this study, not their causal relationships. There might be recollection bias as the study relied on reproductive women's reports. There were some possible confounders, such as antenatal anxiety or depression and the quantity of alcohol consumed, that were not considered in the analysis due to the unavailability of data. The current study's conclusions were based on data that were nationally representative despite these limitations. As a result, they provide information that policymakers and programs used to reduce pregnancy loss in Ethiopia.
Conclusions
This study provided evidence of the association between alcohol consumption and abortion among ever-married reproductive-age women in Ethiopia. Moreover, factors such as older age, media exposure, primary education, contraceptive use, age at first sex, and working status have significant associations with abortion among ever-married reproductive-age women in Ethiopia. Sexual and reproductive health education and family planning programs should target older women, women with primary educational status, working women, and those who have initiated sexual intercourse at a younger age to reduce abortion and unintended pregnancy. Furthermore, as part of sexual and reproductive health education, the adverse effect of alcohol consumption on pregnancy outcomes should be emphasized.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
All authors contributed significantly to the work that has been published, whether it be in the ideation, study design, execution, data processing, analysis, and interpretation, or all of these areas. All authors have also participated in writing, revising, or critically evaluating the article, given their final approval for the version that will be published, chosen the journal to which the article will be submitted, and agreed to be held accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
Acknowledgment
The authors acknowledge the Measure DHS program for permitting them to access the Ethiopian DHS data sets.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AIC, Akaike information criteria; ANC, antenatal care; AOR, adjusted odds ratio; BIC, Bayesian information criteria; DHS, demographic and health survey; ICC, intra-class correlation coefficient; SSA, sub-Saharan Africa; WHO, World Health Organization.
References
1. World Health Organization. Medical management of abortion. Geneva: World Health Organization (2019).
2. Singh S, Remez L, Sedgh G, Kwok L, Onda T. Abortion worldwide 2017: uneven progress and unequal access. New York: Guttmacher Institute (2018).
3. Addila AE, Bisetegn TA, Gete YK, Mengistu MY, Beyene GM. Alcohol consumption and its associated factors among pregnant women in sub-Saharan Africa: a systematic review and meta-analysis’ as given in the submission system. Subst Abuse Treat Prev Policy. (2020) 15(1):29. doi: 10.1186/s13011-020-00269-3
4. Da Pilma Lekettey J, Dako-Gyeke P, Agyemang SA, Aikins M. Alcohol consumption among pregnant women in James Town Community, Accra, Ghana. Reprod Health. (2017) 14(1):120. doi: 10.1186/s12978-017-0384-4
5. Dejong K, Olyaei A, Lo JO. Alcohol use in pregnancy. Clin Obstet Gynecol. (2019) 62(1):142–55. doi: 10.1097/GRF.0000000000000414
6. Sebastiani G, Borras-Novell C, Casanova MA, Pascual Tutusaus M, Ferrero Martinez S, Gomez Roig MD, et al. The effects of alcohol and drugs of abuse on maternal nutritional profile during pregnancy. Nutrients. (2018) 10(8):1008. doi: 10.3390/nu10081008
7. Tesfaye G, Demlew D, Molla G, Habte F, Molla G, Kifle Y, et al. The prevalence and associated factors of alcohol use among pregnant women attending antenatal care at public hospitals Addis Ababa, Ethiopia, 2019. BMC Psychiatry. (2020) 20(1):337. doi: 10.1186/s12888-020-02747-1
8. Popova S, Lange S, Probst C, Shield K, Kraicer-Melamed H, Ferreira-Borges C, et al. Actual and predicted prevalence of alcohol consumption during pregnancy in the WHO African Region. Trop Med Int Health. (2016) 21(10):1209–39. doi: 10.1111/tmi.12755
9. Corrales-Gutierrez I, Mendoza R, Gomez-Baya D, Leon-Larios F. Understanding the relationship between predictors of alcohol consumption in pregnancy: towards effective prevention of FASD. Int J Environ Res Public Health. (2020) 17(4):1388. doi: 10.3390/ijerph17041388
10. Wang Y, Xie T, Wu Y, Liu Y, Zou Z, Bai J. Impacts of maternal diet and alcohol consumption during pregnancy on maternal and infant gut microbiota. Biomolecules. (2021) 11(3):369. doi: 10.3390/biom11030369
11. Addila AE, Azale T, Gete YK, Yitayal M. The effects of maternal alcohol consumption during pregnancy on adverse fetal outcomes among pregnant women attending antenatal care at public health facilities in Gondar town, Northwest Ethiopia: a prospective cohort study. Subst Abuse Treat Prev Policy. (2021) 16(1):64. doi: 10.1186/s13011-021-00401-x
12. Alexandra C, Sundermann B, Sifang Zhao MPH, Chantay L, Young BA, LeAnn Lam BS, et al. Alcohol use in pregnancy and miscarriage: a systematic review and meta-analysis. Nashville, TN: Arvind M. Parmar (2020).
13. Skagerstrom J, Haggstrom-Nordin E, Alehagen S. The voice of non-pregnant women on alcohol consumption during pregnancy: a focus group study among women in Sweden. BMC Public Health. (2015) 15:1193. doi: 10.1186/s12889-015-2519-2
14. Naja F, Ayoub J, Baydoun S, Nassour S, Zgheib P, Nasreddine L. Development of national dietary and lifestyle guidelines for pregnant women in Lebanon. Matern Child Nutr. (2021) 17(4):e13199. doi: 10.1111/mcn.13199
15. Sun YF, Zhang J, Xu YM, Cao ZY, Wang YZ, Hao GM, et al. High BMI and insulin resistance are risk factors for spontaneous abortion in patients with polycystic ovary syndrome undergoing assisted reproductive treatment: a systematic review and meta-analysis. Front Endocrinol (Lausanne). (2020) 11:592495. doi: 10.3389/fendo.2020.592495
16. Moradinazar M, Najafi F, Nazar ZM, Hamzeh B, Pasdar Y, Shakiba E. Lifetime prevalence of abortion and risk factors in women: evidence from a cohort study. J Pregnancy. (2020) 2020:4871494. doi: 10.1155/2020/4871494
17. Addila AE, Azale T, Gete YK, Yitayal M. Individual and community-level predictors of maternal alcohol consumption during pregnancy in Gondar town, northwest Ethiopia: a multilevel logistic regression analysis. BMC Pregnancy Childbirth. (2021) 21(1):419. doi: 10.1186/s12884-021-03885-4
18. Kingsland M, Doherty E, Anderson AE, Crooks K, Tully B, Tremain D, et al. A practice change intervention to improve antenatal care addressing alcohol consumption by women during pregnancy: research protocol for a randomised stepped-wedge cluster trial. Implement Sci. (2018) 13(1):112. doi: 10.1186/s13012-018-0806-x
19. May PA, Marais AS, De Vries MM, Buckley D, Kalberg WO, Hasken JM, et al. The prevalence, child characteristics, and maternal risk factors for the continuum of fetal alcohol spectrum disorders: a sixth population-based study in the same South African community. Drug Alcohol Depend. (2021) 218:108408. doi: 10.1016/j.drugalcdep.2020.108408
20. Addila AE, Azale T, Gete YK, Yitayal M. Determinants of hazardous alcohol use among pregnant women attending antenatal care at public health facilities in Gondar town, Northwest Ethiopia: a nested case-control study. PLoS One. (2021) 16(7):e0253162. doi: 10.1371/journal.pone.0253162
21. Thapa N, Aryal KK, Puri R, Shrestha S, Shrestha S, Thapa P, et al. Alcohol consumption practices among married women of reproductive age in Nepal: a population based household survey. PLoS One. (2016) 11(4):e0152535. doi: 10.1371/journal.pone.0152535
23. Woolf-King SE, Maisto SA. Alcohol use and high-risk sexual behavior in sub-Saharan Africa: a narrative review. Arch Sex Behav. (2011) 40(1):17–42. doi: 10.1007/s10508-009-9516-4
24. Onukwugha FI, Magadi MA, Sarki AM, Smith L. Trends in and predictors of pregnancy termination among 15–24 year-old women in Nigeria: a multilevel analysis of demographic and health surveys 2003–2018. BMC Pregnancy Childbirth. (2020) 20(1):1–13. doi: 10.1186/s12884-020-03164-8
25. Tesema GA, Mekonnen TH, Teshale AB. Spatial distribution and determinants of abortion among reproductive age women in Ethiopia, evidence from Ethiopian demographic and health survey 2016 data: spatial and mixed-effect analysis. PloS One. (2020) 15(6):e0235382. doi: 10.1371/journal.pone.0235382
26. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. (2008) 32(4):962–9. doi: 10.1183/09031936.00012408
27. Newberger DS. Down syndrome: prenatal risk assessment and diagnosis. Am Fam Physician. (2000) 62(4):825–32, 837–8. PMID: 10969860
28. Dickson KS, Adde KS, Ahinkorah BO. Socio-economic determinants of abortion among women in Mozambique and Ghana: evidence from demographic and health survey. Arch Public Health. (2018) 76(1):1–10. doi: 10.1186/s13690-018-0286-0
29. Erdman JN. Access to information on safe abortion: a harm reduction and human rights approach. Harvard J Law Gend. (2011) 34:413. doi: 10.1016/j.ijgo.2012.04.002
30. Cook RJ, Dickens BM. Reducing stigma in reproductive health. Int J Gynecol Obstet. (2014) 125(1):89–92. doi: 10.1016/j.ijgo.2014.01.002
31. Pallikadavath S, Stones RW. Maternal and social factors associated with abortion in India: a population-based study. Int Fam Plan Perspect. (2006) 32:120–5. doi: 10.1363/3212006
32. Shapiro D, Tambashe BO. The impact of women's Employment and education on contraceptive use and abortion in Kinshasa, Zaire. Stud Fam Plann. (1994) 25:96–110. doi: 10.2307/2138087
33. Sundaram A, Juarez F, Bankole A, Singh S. Factors associated with abortion-seeking and obtaining a safe abortion in Ghana. Stud Fam Plann. (2012) 43(4):273–86. doi: 10.1111/j.1728-4465.2012.00326.x
34. Cheng Y, Gno X, Li Y, Li S, Qu A, Kang B. Repeat induced abortions and contraceptive practices among unmarried young women seeking an abortion in China. Int J Gynecol Obstet. (2004) 87(2):199–202. doi: 10.1016/j.ijgo.2004.06.010
35. Erfani A, McQuillan K. Rates of induced abortion in Iran: the roles of contraceptive use and religiosity. Stud Fam Plann. (2008) 39(2):111–22. doi: 10.1111/j.1728-4465.2008.00158.x
Keywords: abortion, multilevel, consumption, alcohol, regression
Citation: Ayana GM, Raru TB, Deressa A, Regassa LD, Gamachu M, Negash B, Birhanu A and Merga B (2022) Association of alcohol consumption with abortion among ever-married reproductive age women in Ethiopia: A multilevel analysis. Front. Glob. Womens Health 3:1028166. doi: 10.3389/fgwh.2022.1028166
Received: 10 September 2022; Accepted: 10 November 2022;
Published: 14 December 2022.
Edited by:
Jitender Aneja, All India Institute of Medical Sciences, IndiaReviewed by:
Ashlesha Bagadia, The Green Oak Initiative, IndiaSidikiba Sidibe, Gamal Abdel Nasser University of Conakry, Guinea
© 2022 Ayana, Raru, Deressa, Regassa, Gamachu, Negash, Birhanu and Merga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Temam Beshir Raru dGVtYW0uYjFAZ21haWwuY29t
Specialty Section: This article was submitted to Women's Mental Health, a section of the journal Frontiers in Global Women's Health