 Liyuan Chen1†
Liyuan Chen1† Haishan Hu
Haishan Hu Yuan Zhan
Yuan Zhan Zhilin Zeng
Zhilin Zeng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Genet. , 15 July 2022
Sec. Genetics of Common and Rare Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fgene.2022.908482
Introduction: Down syndrome (DS) is the leading cause of genetically defined intellectual disability and congenital birth defects worldwide. A large population of people diagnosed with DS globally is posing an enormous socioeconomic burden. However, the global burden and trends of DS have not been reported.
Methods: Based on the data from the Global Burden of Disease database in 2019, we analyzed the incidence, prevalence, disability-adjusted life years (DALYs), and death of DS from 1990 to 2019 according to sex, age, regions, and social-demographic index (SDI). Then, age-standardized rates (ASRs) and estimated annual percentage change (EAPC) of these aforementioned indexes were calculated to evaluate the temporal trend of DS. Finally, the association of SDI with DS epidemiological parameters was assessed.
Results: In the past 30 years, the incident cases, age-standardized incident rate (ASIR), and age-standardized prevalent rate (ASPR) of DS first decreased slightly and subsequently increased globally. The number of prevalent cases increased steadily, while the number and age-standardized rate (ASRs) of DALYs and deaths decreased gradually from 1990 to 2019. In the meantime, disease burdens were different across various SDI regions. The prevalent cases and ASPR for both sexes were increasing in all SDI regions except for the high-middle SDI region. At the national level, Brunei Darussalam, Ireland, and Haiti were the top three countries with the highest ASIR in 2019. Georgia was in the top three with the highest increase in ASRs of four parameters, while Serbia was consistently ranked in the top three with fastest declining. Furthermore, we found that ASIR and ASPR were positively correlated with SDI, yet the age-standardized DALYs and age-standardized death rate (ASDR) were negatively correlated with SDI.
Conclusion: In the past 30 years, the burden and trends of DS were heterogeneous across different regions and countries with different sociodemographic characteristics. Great improvements had been achieved in reducing DALYs and deaths globally. However, the increased number and ASRs of incident and prevalent cases in some regions, especially in low SDI regions, were contributing to numerous challenges to public health. The findings may provide valuable information to the development or implementation of more effective measures.
Annually, an estimated 7.9 million children are born with a severe birth defect due to genetic or partially genetic origin (Christianson et al., 2006). Every year, an estimated number of a minimum of 3.3 million children under 5 years of age die from birth defects and 3.2 million survivors may be disabled for life (Christianson et al., 2006). The most common severe aneuploid condition at the time of birth is Down syndrome (DS) (Arbuzova et al., 2002), which was first described by the British physician Dr. John Langdon H. Down in 1866 (Mercer et al., 2004). The presence of extra chromosome 21 has been recognized as the cause of DS, manifested with mental and motor developmental impairment, facial dysmorphia, and congenital malformations, which is often accompanied by congenital heart disease (Verstegen and Kusters, 2020). The onset of DS usually occurs during prenatal development (Dierssen, 2012), with approximately one case in 1,000 births (Grimm et al., 2021). DS is generally diagnosed prenatally or at the time of birth by means of cell-free prenatal screening with parallel sequencing of maternal plasma cell-free DNA or genetic karyotype testing (Grieco et al., 2015; Bull, 2020). DS patients have an increased susceptibility to develop infections, autoimmune disorders, and hematologic and oncologic abnormalities (Lal et al., 2015; Verstegen and Kusters, 2020). Respiratory infection is the most common reason of death in childhood with DS (McDowell and Craven, 2011; Bull, 2020), while dementia is the direct reason of death in 70% older people with DS (Bull, 2020; McGlinchey et al., 2020). Individuals with DS are usually institutionalized; therefore, family is suffering from a heavy nursing and economic burden (Megarbane et al., 2009). Involvement in community life has become increasingly important as persons with DS survive longer and achieve greater degrees of independence (Churchill et al., 2012). An emphasis on transitions of employment, source of health care, and community involvement, as well as on legal issues and financial support, has been found to be essential for the long-term well-being of persons with DS and their families (Nugent et al., 2018). In addition, evidence-based clinical guidelines have been developed to provide recommendation to support primary care of adults with DS (Tsou et al., 2020). Owing to elevated consciousness, modified treatment protocols, and advanced social supportive medical care (Verstegen et al., 2020), the average life expectancy for persons with DS is on the rise from 25 years in 1983 to 60 years in 2020 (Tsou et al., 2020).
As the average age of pregnant women increased, the number of fetuses with DS had risen (Roizen and Patterson, 2003). The prevalence of DS is correlated positively with maternal age and inversely with gestational age (De Leon-Luis et al., 2014). It was estimated that there is an overall 30% reduction in the numbers of babies with DS from 2006 to 2010 due to elective pregnancy terminations. It is well known that the practice of prenatal screening and selective termination of pregnancy have exerted significant impact on the burden of DS. In addition, researchers also found that lower participation rates are obtained in the prenatal test among women from a lower socioeconomic background (Kuppermann et al., 2006). The percentage of women aged greater than 35, who do not have universal screening, prenatal diagnosis, and associated services, was high in middle- and low-income countries (Christianson et al., 2006). In addition, many studies indicated that sociodemographic characteristics impacted the survival and the risk of mortality for patients with DS (Fiscella et al., 2000; de Campos Gomes et al., 2020). Therefore, maternal age, participation rates in prenatal screening and selective termination of pregnancy, and sociodemographic index (SDI) level were associated with burden of DS.
As one of the important public health issues worldwide, DS imposes a heavy burden on the family and society. However, there is lack of research studies to assess the global burden of DS at present, to our knowledge. In this study, we aim to show the global burden and epidemiology trend of DS stratified by age, SDI, regions, and countries from 1990 to 2019.
As the unit of analysis for measuring the relative magnitude of losses of healthy life associated with specific causes, the disability-adjusted life year (DALYs) is a summary measure of the years lived with disability and the years of life lost (Salomon, 2014). The DALYs has been proposed by the World Bank and the WHO as a measure of the global impact of disease on individual illness status (FerrucciC et al., 2007).
SDI, scaled from 0 to 1, is a composite indicator of overall development based on the rankings of incomes per capita, years of schooling, and fertility rates in females younger than 25 years. The larger the SDI is, the more developed the country is. Age-standardized rates (ASRs) refer to the method of statistical processing of demographic data according to the same standard age composition (Mohsen Naghavi et al., 2015). The purpose is to eliminate the influence of different age compositions of the population among different geographical areas and ensure comparability of statistical indicators (Omar et al., 2001).
We collected the annual incident cases, prevalent cases, the DALYs and death, and the age-standardized data of DS from 1990 to 2019 from the Global Burden of Disease (GBD) 2019, which measures epidemiological levels and trends among communicable diseases, noncommunicable diseases, and injuries globally (Diseases and Injuries, 2020). The methodology of GBD 2019 study has been described in previous studies (Diseases and Injuries, 2020).
Information on age, SDI and geographic location was also obtained to further analyze the disease burden. To better exhibit the age distribution of DS burden, we divided population into 4 groups according to age, including those below 5 years old, 5–14 years old, 15–49 years old, and above 50 years old. In order to explore the association between SDI and DS burden, countries and territories were divided into five regions according to the SDI, including namely the low, low-middle, middle, high-middle and high SDI. Moreover, the world was divided into 21 regions according to the geographic location.
The Institutional Review Board of Wuhan No.1 Hospital determined that approval was waived because of publicly available data. The GBD 2019 complies with the Guidelines for Accurate and Transparent Health Estimates Reporting statement (Stevens et al., 2016). The standardized methods of the GBD 2019 have been extensively reported (Diseases and Injuries, 2020). Annual number of incident cases, prevalent cases, death and DALY, and corresponding ASRs (number per 100,000 population) were used to describe the disease burden. Incidence measures the rapidity of disease occurrence, while prevalence measures the proportion of the population with disease.
ASRs were calculated on the basis of the following formula:
The estimated annual percentage change (EAPC) was calculated using the following regression model to assess the trends of ASRs: Y = α+βX+ε, where Y refers to ln (ASRs), X represents calendar year, ε means error term, and β determines the positive or negative trends in ASRs. The EAPC could be given by 100*(exp(β)-1). The ASRs were considered to be on the rise when the estimation of EAPC and its lower boundary of 95% uncertainty interval [UI] were both positive. On the contrary, the ASRs were considered to be in a downward trend when EAPC and its upper boundary of 95% UI were both negative. Otherwise, the ASRs were considered to be stable over time (Chen et al., 2021).
The Spearman’s correlation coefficients were used to assess the relationships between the ASRs and SDI. In the correlation analysis, if the Pearson correlation coefficient was >0 and the p value was <0.05, there was a significant positive correlation between the two variables. The maps were made using ECharts software. The p-value less than 0.05 is considered statistically significant.
As presented in Figure 1A and Supplementary Figure S1A, there were almost no changes both in the incidence cases and the age-standardized incident rate (ASIR) of DS from 80,060 (95% uncertainty interval [UI] 61,960-102,450) and 1.22 (95% UI 0.94–1.56) per 100,000 population in 1990 to 78,430 (95% UI 60,130-101,730) and 1.21 (95% UI 0.93–1.57) in 2019, respectively. Although the EAPC (0.03, 95% UI -0.14-0.20) of ASIR signified the basically unchanged trend from 1990 to 2019 worldwide, both of incident cases and ASIR were first in downward trends and then in upward with the turning point in 2001 (69,638, 95% UI 54,913-87,017) and 1996 (1.08, 95% CI 0.86–1.35), respectively (Supplementary Table S1 and Supplementary Table S7).
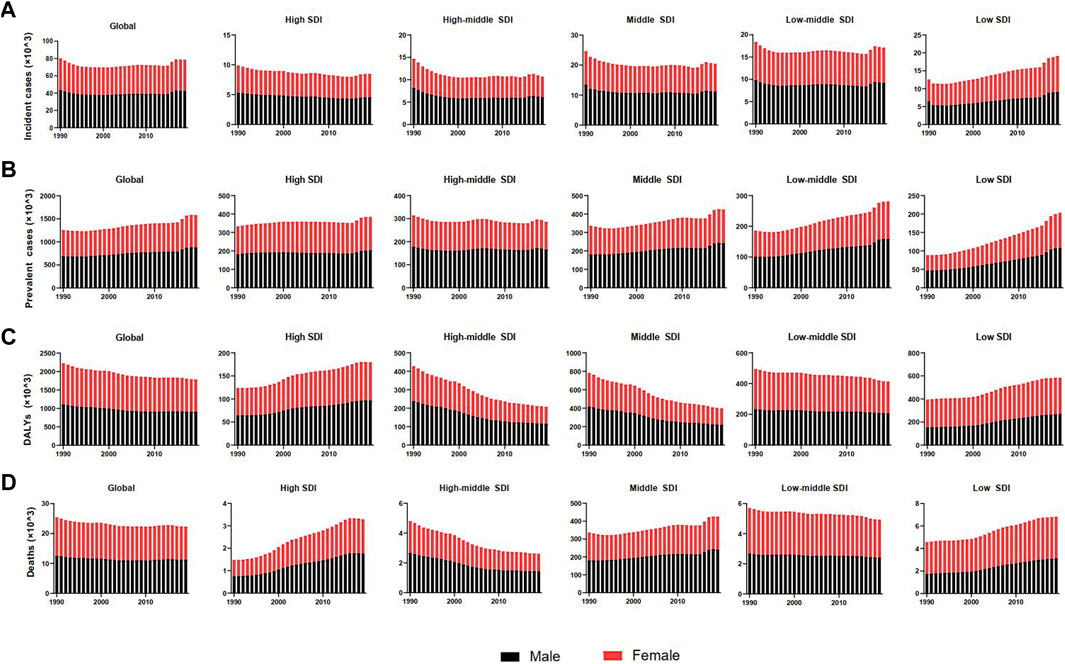
FIGURE 1. Burden and trends of Down syndrome globally and in five SDI quintiles from 1990 to 2019. (A) Incident cases. (B) Prevalent cases. (C) Disability-adjusted life-years (DALYs). (D) Deaths. Black bars represent males, and red bars represent females. Note: DALYs, disability-adjusted life-years; SDI, social-demographic index.
The incidences of different SDI regions were divergent while males had more incident cases and ASIR from DS than females except for the low SDI region (Figure 1A, Supplementary Figure S1A, Figure 2A and Table 1). The middle SDI region had the most incidence cases in 1990 (24,610, 95%UI 19,070-32,050) and 2019 (20,450, 95%UI 15,610-26,390). The low-middle SDI region held the lowest ASIR both in 1990 (1.01, 95%UI 0.76–1.31) and in 2019 (1.01, 95%UI 0.77–1.32). The high SDI region simultaneously obtained the lowest incident cases and the most ASIR at that time in the past 3 years (Table 1). Interestingly, the high SDI region with the most ASIR had the biggest downward trend (EAPC -0.28, 95%UI -0.40 to -0.16) from 1990 to 2019 (Table 1). Among the 21 regions divided according to geographical characteristics, the ASIR of South Asia maintained the lowest value both in 1990 (0.77, 95%UI 0.57–1.01) and in 2019 (0.79, 95%UI 0.59–1.04), but the Australasia with the highest ASIR in 1990 (2.40, 95%UI 1.90–2.96) was replaced to Southern Latin America (2.53, 95%UI 2.02–3.17) in 2019, which also had the highest growth rate with EAPC value of 1.02 (95%UI 0.74–1.30). High-income North America declined fastest in ASIR from 1990 to 2019 with EAPC value of -1.06 (95%UI −1.31 to −0.81) (Figure 3A, Figure 4A, Table 1). The top three countries with the highest ASIR in 2019 were Brunei Darussalam (3.94, 95%UI 3.02–4.97), Ireland (3.80, 95%UI 2.73–5.14), and Haiti (3.54, 95%UI 2.50–5.00), while America had the lowest ASIR (0.60, 95%UI 0.46–0.80) among all the countries (Figure 3A, Supplementary Table S3). The ASIR rose fastest in Georgia (EAPC 2.36, 95%UI 2.00–2.72) and decreased fastest in Serbia (EAPC -2.09, 95%UI -2.22 to -1.96) (Figure 4A, Supplementary Table S4). In Figure 5A, ASIR and SDI had a positive correlation (R = 0.58, p < 0.0001), which meant ASIR seems to be higher in relatively developed regions.
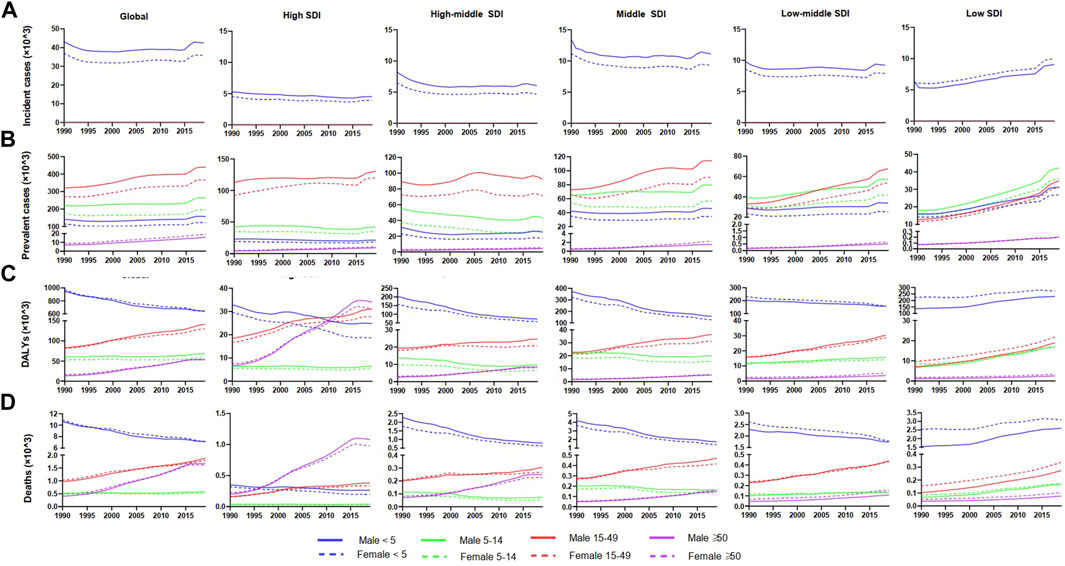
FIGURE 2. Change trends of Down syndrome incident cases, prevalent cases, DALYs, and deaths from 1990 to 2019 in different age groups. (A) Change trends of incident cases. (B) Change trends of prevalent cases. (C) Change trends of DALYs. (D) Change trends of deaths. Note: DALYs, disability-adjusted life-years.
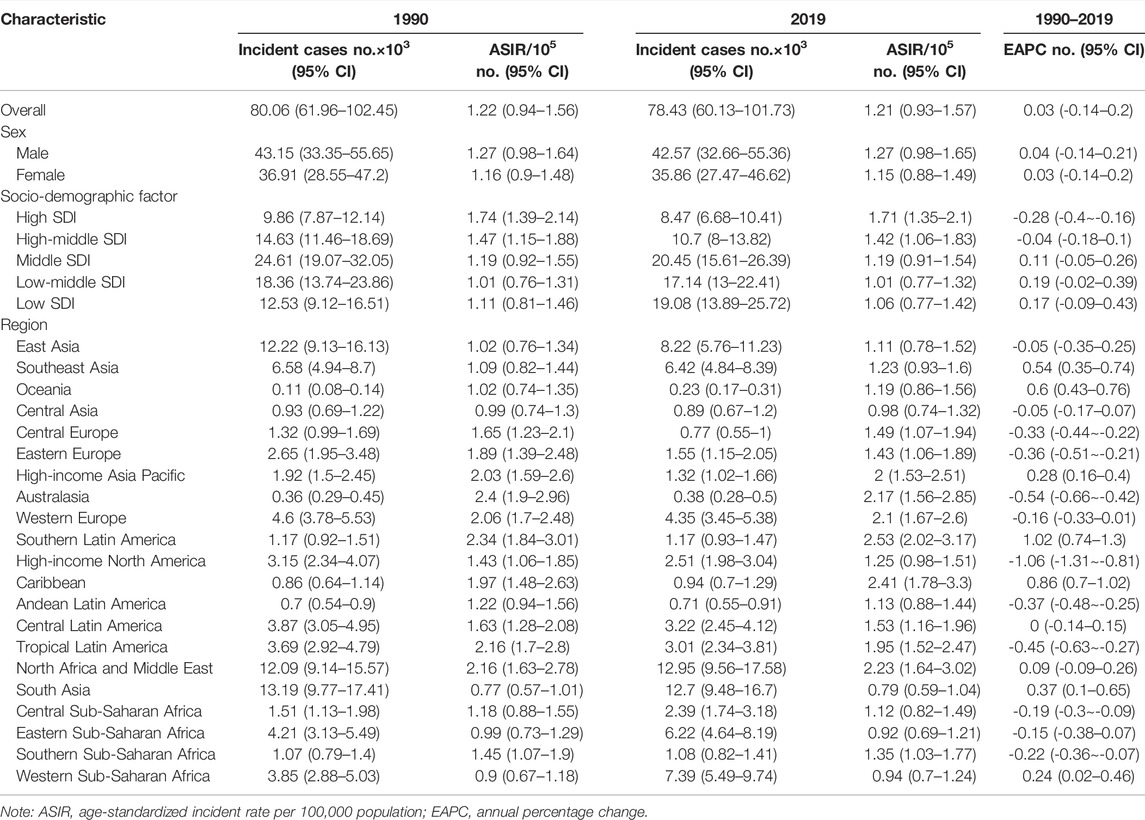
TABLE 1. Incidence of Down syndrome in 1990/2019 and temporal trends.
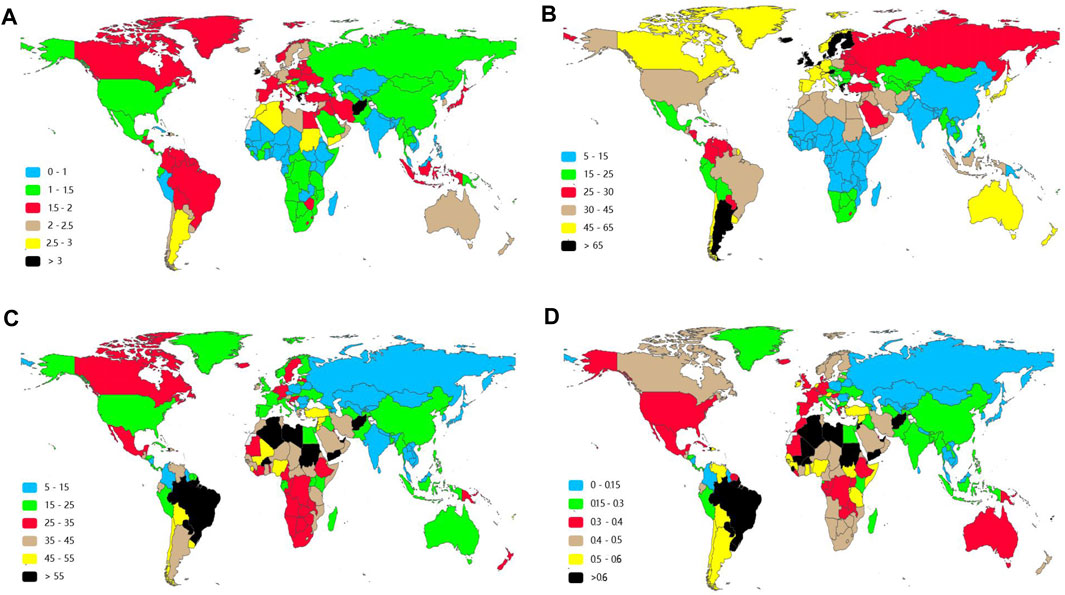
FIGURE 3. Age-standardized rate of Down syndrome in 2019 in 204 countries and territories. (A) Age-standardized incident rate (ASIR). (B)Age-standardized prevalent rate (ASPR). (C) Age-standardized DALY rates. (D) Age-standardized death rates (ASDRs).
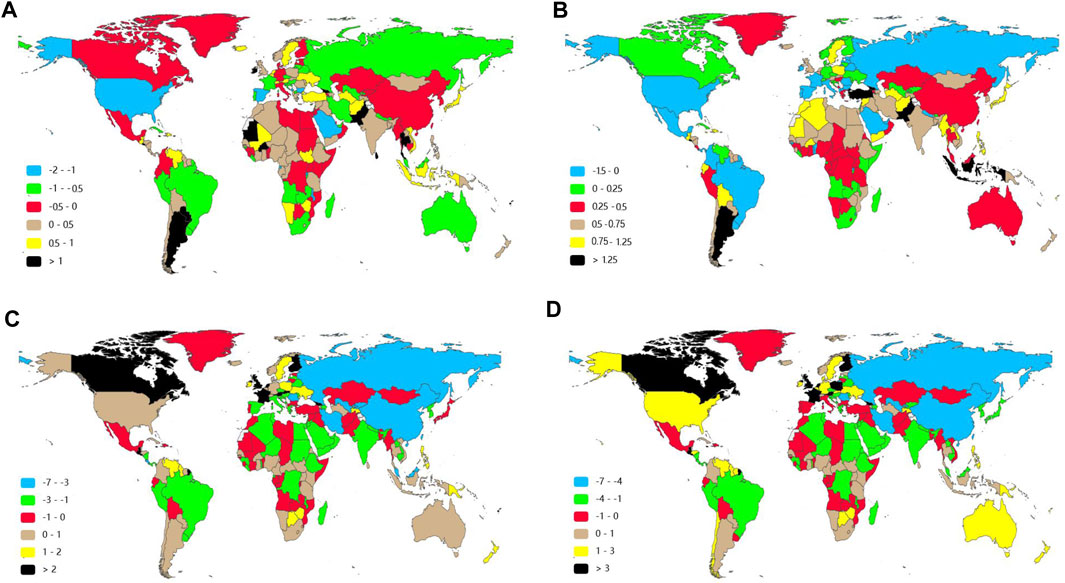
FIGURE 4. Estimated annual percentage changes of Down syndrome in 204 countries and territories between 1990 and 2019. (A) EAPC of age-standardized incident rates (ASIRs). (B) EAPC of age-standardized prevalent rates (ASPRs). (C) EAPC of age-standardized disability-adjusted life-year (DALY) rates. (D) EAPC of age-standardized death rates (ASDRs). Note: DALYs, disability-adjusted life-years; EAPC, estimated annual percentage changes.
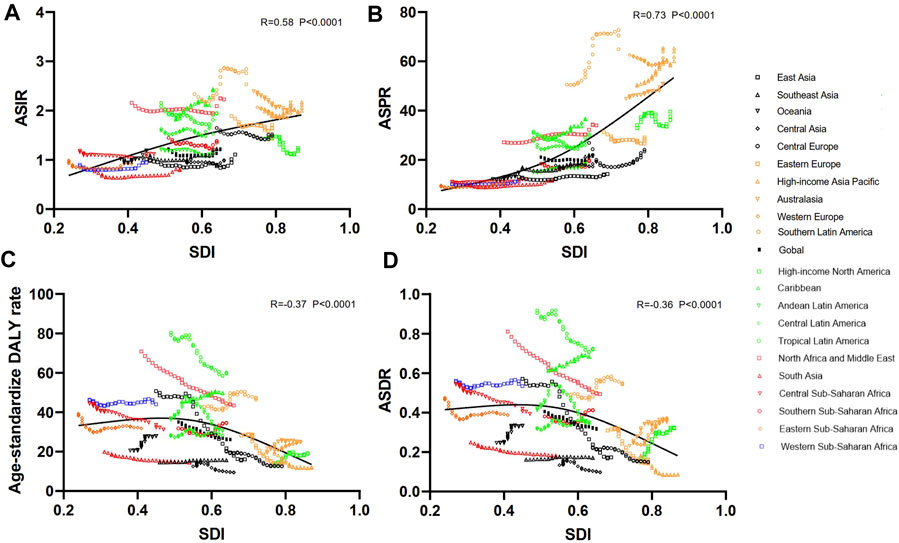
FIGURE 5. Association between ASRs of Down syndrome and SDI in 21 regions from 1990 to 2019. The SDI was positively correlated with the ASIR (A) and ASPR (B) in 21 regions from 1990 to 2019. The SDI was negatively correlated with the age-standardized DALY rate (C) and ASDR (D). Note: ASRs, age-standardized rates; ASIR, age-standardized incident rate; ASPR, age-standardized prevalent rate; ASDR, age-standardized death; DALYs, disability-adjusted life-years; SDI, social-demographic index.
The prevalent cases of all the SDI regions for both sexes were increasing except for the high-middle SDI region in the past three decades (Figure 1B and Table 2). The prevalent cases of DS reached 1,579,784 (95%UI 1,251,955-1,962,089) in 2019 from 1,257,110 (95%UI 989,416-1,573,671) in 1990. The ASPR of DS decreased from 1990 to 1997 and subsequently increased from 1998 to 2019 around the world (Table 2). At the regional level, the high SDI region had the most ASPR both in 1990 (44.67, 95%UI 36.06–54.88) and in 2019 (49.11, 95%UI 39.84–59.50), while low SDI region had the lowest in 1990 (11.83, 95% UI 8.96–15.42) and in 2019 (13.53, 95%UI 10.30–17.65) all the time. From the data in Figure 1B and Supplementary Figure S1B, males had more prevalent cases and ASPR than females regardless of the SDI region. From 1990 to 2019, prevalent cases between 15 and 49 years old were the largest group of DS patients in the global and in different SDI regions except low SDI region.
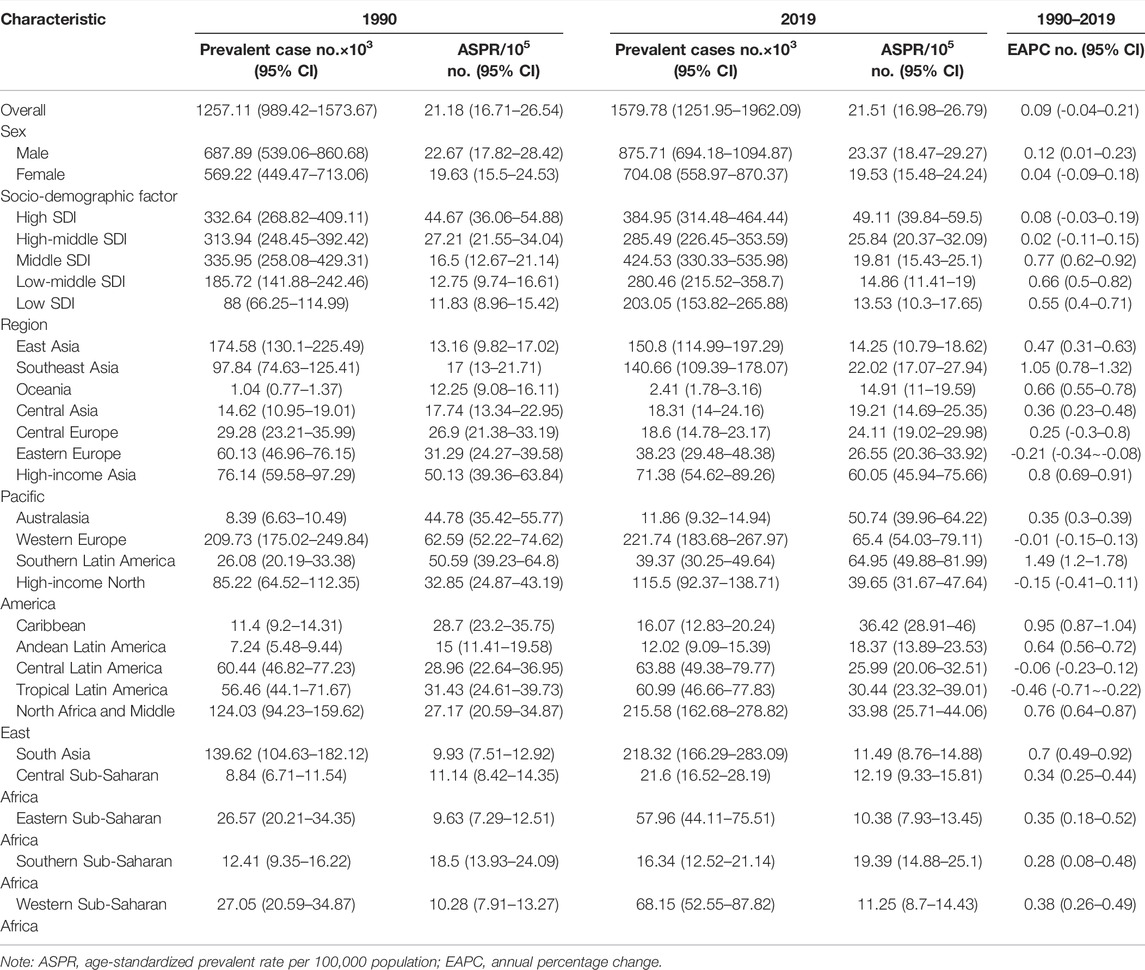
TABLE 2. Prevalence of Down syndrome in 1990/2019 and temporal trends.
By contrasting the data in Table 1 and Table 2, there was greater inter-regional variation in prevalence compared to incidence. The EAPC of ASPR was positive in most regions apart from Central Europe, Eastern Europe, Western Europe, Central Latin America, High-income North America, and Tropical Latin America, which signified that the ASPR was on the rise in the past 30 years in most regions. From 1990 to 2019, Western Europe presented the highest prevalent cases and ASPR with no significant annual variability (Figure 3B and Table 2). Southern Latin America, which held the second place of ASPR (64.95, 95%UI 49.88–81.99) in 2019, had the highest EAPC of ASPR (1.49, 95%UI 1.20–1.78). Also, the region with the lowest EAPC of ASPR went to Tropical Latin America (-0.46, 95%UI −0.71to −0.22) (Figure 4B and Table 2). At the national level, Malta (98.86, 95%UI 79.10–122.11), Brunei Darussalam (97.20, 95%UI 74.28–122.16), and Ireland (93.00, 95%UI 73.15–116.70) were the top three countries of highest ASPR in 2019, with Brunei Darussalam and Ireland also having the highest ASIR (Figure 3A, Figure 3B and Supplementary Figure S3). The three nations with the fastest dropping ASPR were the same as the ASIR: Serbia (EAPC 2.09, 95%UI: −2.22 to −1.96), Bulgaria (EAPC -1.75, 95%UI -2.06 to-1.44), and Spain (EAPC -1.66, 95%UI −2.01 to −1.31). Argentina (1.96, 95% UI 1.65–2.28) and Georgia (1.75, 95% UI 1.46–2.03) had the highest EAPC of ASPR (Figure 4B and Supplementary Figure S4). We can find that the ASPR was positively correlated with SDI (R = 0.58, p < 0.0001) (Figure 5B) which corresponded to the data in Table 2.
The DALYs attributable to DS were on a downside globally from 2,223,900 (95%UI 1,499,510-4,609,110) in 1990 to 1,783,570 (95%UI 1,374,190-2,747,160) in 2019 (Table 3). In the globe, age-standardized DALYs declined by 25.95% gradually from 35.14 per 100,000 population (95%UI 23.81–72.35) in 1990 to 26.02 (95%UI 19.83–40.75) with an EAPC value of -1.05 (95% UI -1.11 to -0.99). Contrary to the global changing trend, the high SDI region and low SDI region had an uptrend in DALYs (Figure 1C). The middle SDI region got the highest number of DALYs both in 1990 and 2019 as the low SDI region had the lowest. The high SDI region retained the lowest of age-standardized DALYs in 1990 and 2019, while the highest age-standardized DALYs changed from the high-middle region to the low SDI region (Table3). The EAPC of age-standardized DALYs was negative except for the High SDI region in both sexes (Supplementary Figure S1C and Table 3).
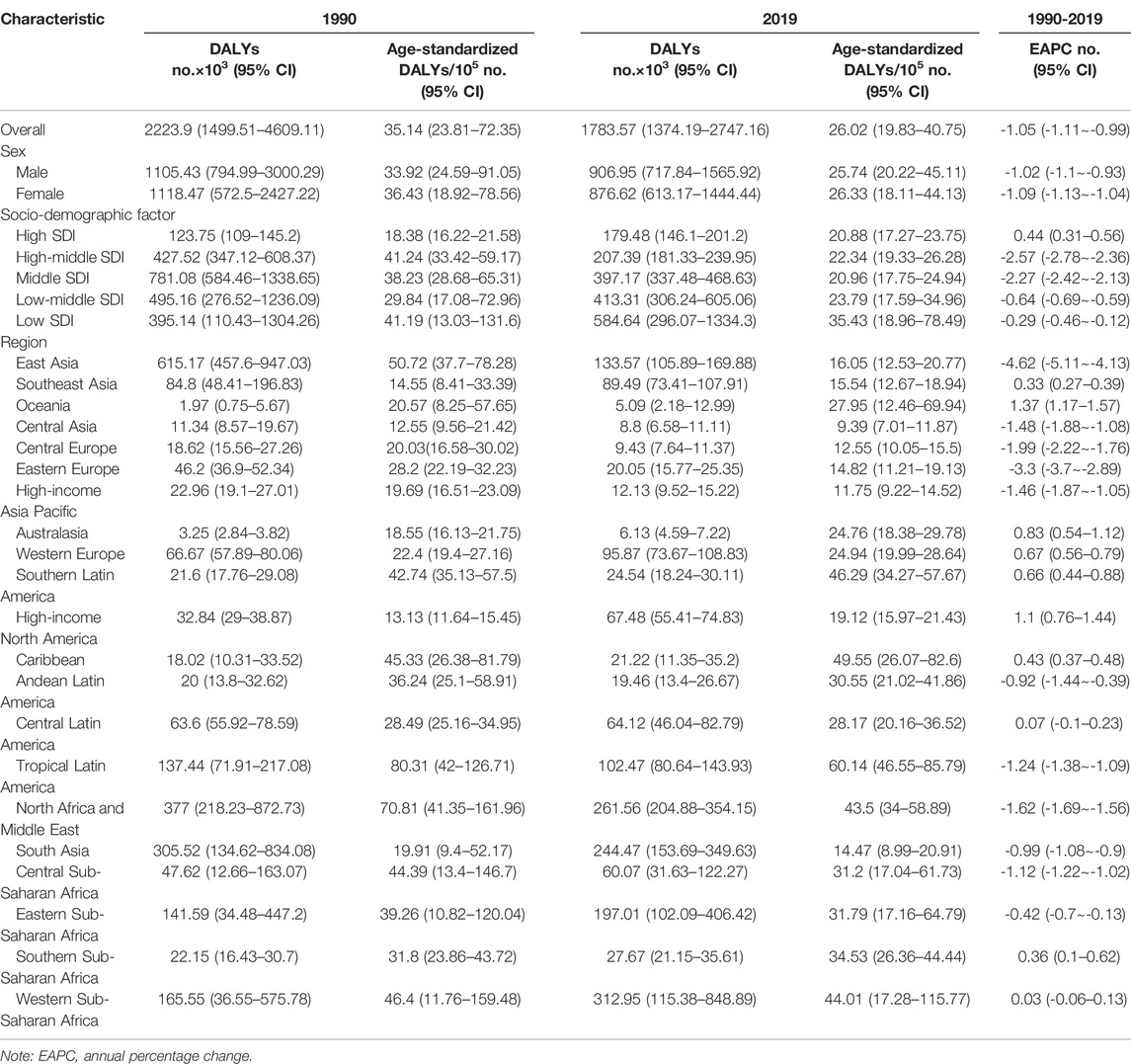
TABLE 3. DALYs of Down syndrome in 1990/2019 and temporal trends.
Regionally, the DALYs were found to be the highest in East Asia in 1990 (615,170, 95%UI 457,600-947,030) and in Western Sub-Saharan Africa in 2019 (312,950, 95%UI 115,380-848,890) (Table3). Tropical Latin America was the top one in terms of the age-standardized DALYs both in 1990 (80.31, 95%UI 42.00–126.71) and in 2019 (60.14, 95%UI 46.55–85.79). On the contrary Central Asia held the lowest age-standardized DALYs in 1990 (12.55, 95%UI 9.56–21.42) and in 2019 (9.39, 95%UI 7.01–11.87) (Table 3). East Asia had the most rapid decline of age-standardized DALYs in the past three decades with an EAPC value of -4.77 (95%UI −5.11 to −4.13) (Table 3 and Figure 4C).
At the country/territory level, Paraguay (82.26, 95%UI 59.98–122.98), Haiti (80.39, 95%UI 22.55–165.20), and Algeria (79.28, 95%UI 49.15–128.46) had the highest age-standardized DALYs in 2019. Palau (4.56, 95%UI 3.19–6.34), Cook Islands (4.91, 95%UI 2.63–8.64), as well as Romania (5.35, 95%UI 4.15–6.88) had the lowest one (Figure 3C and Supplementary Table S3). Among the countries mentioned previously, Haiti and Palau also had relatively high and low ASIRs, respectively, as previously written. Guatemala (7.14, 95%UI 5.72–8.57), Georgia (4.72, 95%UI 3.88–5.56), and Bahrain (4.37, 95%UI 3.58–5.18) had the highest EAPC of age-standardized DALYs. Serbia (−7.48, 95%UI −8.31 to -6.64), China (−4.71, 95%UI −5.22 to −4.20), and Uzbekistan (−4.67, 95%UI −5.52 to −3.81) had the lowest EAPC of age-standardized DALYs (Figure 4C and Supplementary Table S4). The SDI negatively correlated with age-standardized DALYs (R = 0.37, p < 0.0001), which meant that the more developed region may be more likely to have lower DALYs (Figure 5C).
At the global level, the number of deaths due to DS had a slide downward trend in the last 30 years from 28,380 cases (95%UI 16,900-52,830) in 1990 to 22,280 (95% UI 17,760-33,170) in 2019 (Table 4). The age-standardized death rate (ASDR) and their changing trends varied among different SDI regions and countries. Interestingly, the distribution and variation related to death were similar to those in DALYs (Figures 3C,D, Figures 4C,D, Table 3 and Table 4). The high-middle SDI region held the highest ASDR (0.46, 95%UI 0.37–0.67) in 1990, while the low SDI region (0.43, 95%UI 0.24–0.93) had the highest in 2019 (Table 4). Same as DALYs, the ASDR was gradually declining in all except the high SDI region (Supplementary Figure S1D, Table 4). Most of the patients who died were younger than 5 years old in all SDI regions except high SDI, in which the majority of deaths were among patients over 50 years old.
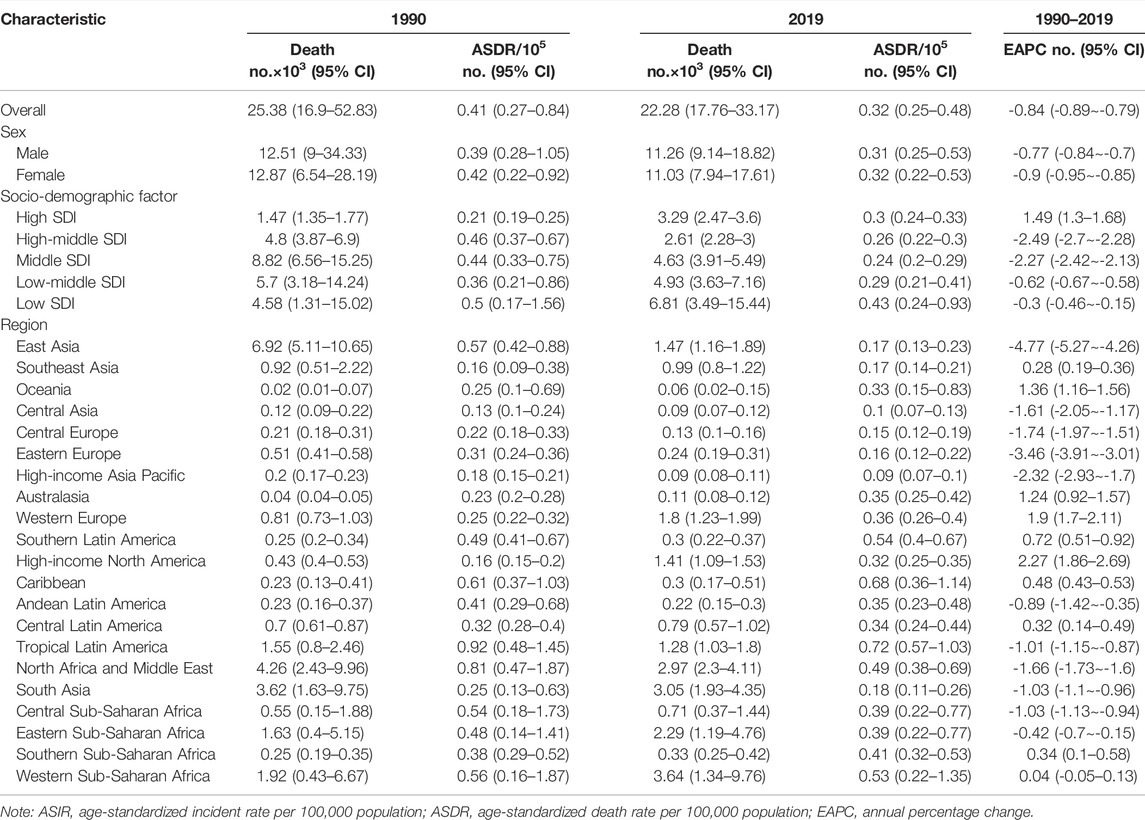
TABLE 4. Death of Down syndrome in 1990/2019 and temporal trends.
At the regional scale, East Asia had the largest number of deaths in 1990 (6,920, 95%UI 5,110-10,650) with the lowest EAPC of ASDR (−4.77, 95%UI -5.27 to −4.26) (Table 2). Central Asia displayed the lowest and the second-lowest ASDR in 1990 (0.13, 95%UI 0.10–0.24) and 2019 (0.10, 95%UI 0.07–0.13), respectively. Tropical Latin America had the highest ASDR both in 1990 (0.92, 95%UI 0.48–1.45) and 2019 (0.72, 95%UI 0.57–1.03) (Figure 3D, Figure 4D and Table 4).
The ASDR was the highest in Haiti (1.20, 95%UI 0.30–2.66), followed by Paraguay (1.00, 95%UI 0.65–1.48) and Algeria (0.91, 95%UI 0.56–1.53) in 2019, which were also top 3 countries in the ranking of the age-standardized DALYs in 2019. The three countries with the lowest ASDR in 2019 were San Marino (0.04, 95%UI 0.02–0.06), Romania (0.05, 95%UI 0.03–0.06), and Palau (0.05, 95%UI 0.03–0.07) (Figure 3D and Supplementary Table S3).
As reported in Figure 4D and Supplementary Table S4, the fastest growth of ASDR was in Guatemala (EAPC 7.95, 95% UI 6.35–9.56), the United Kingdom (EAPC 6.34, 95%UI 5.29–7.40), and Georgia (EAPC 5.22, 95%UI 4.31–6.14), whereas the fastest decrease was in Serbia (EAPC −7.44, 95%UI −8.28 to −6.60), Uzbekistan (EAPC −5.38, 95%UI −6.34 to −4.40), and Singapore (EAPC −5.19, 95%UI −6.31 to −4.06). Importantly, Georgia was in the top three in all the EAPC rankings while Serbia was consistently in the top three fastest declining of those (Figures 4A–D and Supplementary Table S4). The ASDR was negatively correlated with SDI (R = −0.36, p < 0.0001), which meant that the more developed region might be more likely to have lower ASDR (Figure 5).
DS is one of the main causes of intellectual disability, and these patients face a variety of health problems (Asim et al., 2015). Charleton et al. once formulated almost 44 particular medical problems that existed more regularly in people with DS (Stores and Stores, 2013). DS imposes a huge medical and social cost; therefore, an exploration of the global burden and trends of DS through SDI and region stratification is a valuable reference for public health leaders, researchers, and clinical doctors. In this study, we noticed that the incident cases, ASIR, and ASPR declined slightly first, then increased, especially in recent 5 years, and ultimately were unchanged in the past three decades. The prevalent cases were rising around the world, whereas the number and ASRs of DALYs and deaths decreased gradually from 1990 to 2019. Substantial diversity of disease burden and trends were discovered in different SDI or geographic regions, and individual countries. In addition, the ASIR and ASPR had a positive correlation with corresponding SDI value; on the contrary, age-standardized DALYs and ASDR had a negative correlation with SDI.
The results from early studies demonstrated that human aneuploidy may be induced by environmental factors, such as chemotherapy, cigarette smoking, endocrine-disrupting chemicals, or exogenous hormones (Munne et al., 1997; Yang et al., 1999; Frias et al., 2003; Allard and Colaiacovo, 2010; Brieno-Enriquez et al., 2011). It is challenging to identify such factors due to multifactorial nature of the process and the potential complexity of the interactions.
The increasingly widespread practice of prenatal screening and selective termination of pregnancy have exerted significant positive impact on alleviating the burden of DS. de Graaf et al. (2015) estimated an overall 30% reduction in the numbers of babies with DS from 2006 to 2010 due to elective pregnancy terminations. Although gynecologists and midwives are legally obliged to inform each pregnant woman about the options for prenatal screening at the booking visit, the willingness to receive those tests is not the same, despite the absolute benefit of prenatal screening. Morris showed that receipt of antenatal diagnosis was observed in 70% of mothers aged greater than 37 years, while in 43% of younger mothers in England and Wales (Morris and Alberman, 2009). Many expectant couples choose not to pursue prenatal screening or diagnostic test altogether (de Graaf et al., 2017). Two studies reported that antenatal diagnosis occurred in about 15% of mothers in Arab Emirates and Ireland, which were relatively high-income countries (Corder et al., 2017). There is no doubt that this reason partially explained why Ireland was in the top three countries with the highest number and ASRs of incident and prevalent cases. Researchers also found the lower participation rates in prenatal test among women from a lower socioeconomic background (Kuppermann et al., 2006; Rowe et al., 2008; Fransen et al., 2010). The percentage of women aged greater than 35, who do not have universal screening, prenatal diagnosis, and associated services, was high in middle- and low-income countries (Christianson et al., 2006). Keeping in line with that finding, we observed the incident cases in high SDI region showed a downward trend but in the low SDI region presented an upward trend. In addition, an important finding was reported that, especially women from Turkish and Moroccan ethnic origin were less likely to participate in prenatal screening for DS in Dutch even after adjustment for differences in socioeconomic background and age (Fransen et al., 2010). The white race was much more aware of the availability terminating fetuses, and therefore, the impact of this procedure was greater among the white race than among those of other races after identification with DS (Krivchenia et al., 1993). These differences in prenatal screening and termination could partly be attributed to policies, provisions, and uptake of prenatal screening, socioeconomic background, awareness, and ethnic and religious beliefs. Those differences between countries partially lead to wide variation in incidence and prevalence of DS. Earlier detection of DS prenatally and selective termination of pregnancy timely could undoubtedly decrease burden of DS. Therefore, it would be meaningful to take the prenatal screening and selective termination of pregnancy to equip healthcare programs in less developed countries.
It is well known that advancing maternal age increases the risk of DS (Loane et al., 2013). In the 1980s, women started waiting to have children until later years (de Graaf et al., 2017). The mean age of women at the birth of their first child increased across all European Union Member States in the last three decades (EuropenState, 2015).‘Late childbirth’ is an increasingly popular trend in many countries and regions (Kenny et al., 2013). Technically, advanced maternal age refers to women who are 35 years of age or older at the time of the delivery of her baby. Loane et al. (2013) found that ten out of twelve European countries reported more than 50% of mothers to be 35 years of age or older). In our study, relatively stable number and ASRs of incident were observed in different regions and in the global level except for the low SDI region from 1990 to 2019. This is consistent with other studies reporting no increasing trends in many areas of the world (Baird and Sadovnick, 1988; Loane et al., 2013). The increasingly widespread termination of pregnancy had, on average, counteracted the effect of maternal age and resulted in a relatively stable incidence of DS in different regions except for the low SDI region. This overall change of incident cases globally may be attributed to a decline in the number of incident cases in high, high-middle, and middle SDI, offset by an increase in the low SDI region. The increased and upward trends of incidence in low SDI region should raise concern, which poses a serious challenge to children health.
The most common cause of death in childhood and adulthood with DS remains respiratory infection, while congenital heart defects cause most deaths in early childhood (Bull, 2020). Children with DS were now mandated by federal law to have their congenital heart defects repaired, leading to another boost in childhood survival rates (de Graaf et al., 2017). Experience from high-income countries shows that up to 70% of birth defects can either be prevented, or that affected children can be offered care, which could be lifesaving or would reduce the severity of disability. These interventions include appropriate treatment, particularly surgery and prevention, especially before conception or in very early pregnancy (Christianson et al., 2006). Better medication and improved care for complications related to DS have increased the life expectancy (Verstegen and Kusters, 2020). In our study, high SDI region showed the less incident cases of DS than lower SDI region but higher ASIR in the past three decades when the impacts of ageing were removed by converting counts number to ASRs. In the meantime, high SDI region suffered from higher number and ASRs of prevalent cases than those of low SDI region. Moreover, the SDI was positively correlated with the ASIR and ASPR in 21 regions from 1990 to 2019. Based on the definition of SDI and the aforementioned finding, we suggested that the incidence and prevalence of patients with DS might be associated with SDI level, medical service condition, and community support.
The higher incidence of birth with DS has also been reported in consanguineous marriage (CM) families, which suggests families with consanguinity might be a risk factors for DS (Corder et al., 2017), (Ray et al., 2018). Consanguinity results in an excess of homozygosity for recessive traits and has been reported in association with a higher frequency of cardiac malformations in patient with DS (El Mouzan et al., 2008). CM is a common practice in many parts of the world, especially in the Eastern Mediterranean and North Africa (Christianson et al., 2006). Regional differences are distinctive in our study. We found the relative higher number and ASRs of incident and prevalent cases in North Africa and Middle East partially attributable to common CM in those regions.
In line with a previous article, there were differences in the burden of DS according to the geographic region (Bull, 2020). Geographical variation was great in incidence and prevalence of DS in our study. We found that Ireland was among the top three countries with the highest ASIR and ASPR. Termination of pregnancy for fetal anomaly was illegal in Ireland and Malta. Therefore, it was potentially owing to differences in maternal age and prenatal screening (Nordstrøm et al., 2020); in addition to that, willingness to participate in prenatal screening, healthcare policy, and national legislation should also be taken into account (Churchill et al., 2012). Furthermore, Western Europe remained the first place of prevalent cases and ASPR all the time; we also found that the ASPR was positively correlated with SDI, which meant that ASPR seemed to be higher in relatively developed regions. To our knowledge, in developed countries, relatively good success had been made to meet the needs of children with DS through an early intervention procedure. As a result, they lived longer and healthier in the community in a family environment due to life-saving advances in health care, such as pediatric cardiac surgery and modified social housing (Churchill et al., 2012). Interestingly, Georgia is in the top three in all the EAPC rankings, while Serbia is consistently in the top three fastest declining of those. We should pay more attention to these two countries to get a better understanding of promoting or inhabiting factors influencing DS burden and trends.
It has been previously described that the proportion of males is higher in patients with DS. (Takeuchi et al., 2008; Glivetic et al., 2015). Consistent with previous studies, our study found that the males prevalent cases exceeded that of females regardless of the SDI region, which might be related to a differential rate for fetus survival in utero between sexes (Bishop et al., 1997; Agopian et al., 2012; Corona-Rivera et al., 2019).
The DALYs and death toll increased in both high and low SDI over the past three decades. After eliminating the influence of different age compositions, the trend of age-standardized DALY rate and ASDR in those regions were distinctive with an upward trend in high SDI region and a downward trend in low SDI region. Christianson et al. (2006) reported that 65% of the infants and children with DS had died by the age of two in South Africa in the early and mid-1990s. Coinciding with the report in Brazil that children were more susceptible to death (de Campos Gomes et al., 2020), the majority of deaths occurred in the children less than 5 years old in different SDI region except high SDI region. Prioritizing a reduction in deaths of newborns and children is one of the seventeen Sustainable Development Goals (Nations, 2014). To achieve this goal to fall well below United Nations projections, more efforts should be made to decrease the death of DS globally. In addition, we found that most of the deaths were over 50 years old in high SDI region. This might be due to high proportion of older DS patients in high SDI region where DS patients have a longer life expectancy. Both age-standardized DALYs and ASDR were negatively correlated with SDI, indicating that difference might be partly attributed to social and economic factors. Analogously, many studies indicated that sociodemographic characteristics impacted the survival and the risk of mortality for patients with DS (Fiscella et al., 2000; de Campos Gomes et al., 2020). According to the literature, the most common reason of death in childhood and adulthood remained as respiratory infection (Bull, 2020); dementia was the direct reason of death in 70% of dead older people with DS (McGlinchey et al., 2020). Cardiovascular and pulmonary diseases accounted for ∼75% of the death rate in people with DS (Colvin and Yeager, 2017). Without doubt, improved medical care for complications related to DS has increased the life expectancy of DS and decreased mortality and morbidity in good economic-social countries and regions (Verstegen and Kusters, 2020). The lives of persons with DS and of their families had been improved greatly by guidelines development, their propagated extension to medical staff, and advancement in medical treatment protocol with social support (Crissman et al., 2006; Asim et al., 2015). The United States reported a remarkable 46% decline in infant mortality rates from birth defects over the period 1980 to 2001, and much of this reduction can be attributed to improvements in diagnosis, care, and prevention (Christianson et al., 2006).
Our research is the first comprehensive report on the DS epidemiology, which fills a gap in the global burden and trends of DS. People with DS are living longer than they have before. Increased utilization of prenatal testing and DS-related elective terminations had counterbalancing effects on population growth, resulting in relatively stable numbers of people with DS (de Graaf et al., 2017). However, several limitations should be noted when interpreting our results. First, the diagnosis of DS might be underreported and may result in bias in DS registration, especially in nations with limited medical resources or low economic regions, which could lead to an underestimation of the disease burden. Second, as data are lacking in some parts of the world, information bias is unavoidable with respect to the epidemiologic assessment of DS. Third, the roles of risk factors (except SDI) for DS were not estimated in this study. Some risk factors might help to explain geographic and temporal patterns in the disease burden.
In general, our results implied that substantial diversities of DS burden and trends were across different regions and countries with different sociodemographic characteristics. Our results implied that significant improvement had been made in reducing DALYs and deaths worldwide from 1990 to 2019. However, the increased number and ASRs of incident and prevalent cases in some regions, especially in low SDI regions, are raising concerns, which pose a serious challenge to children health. We hope to draw the attention of policy makers in order to facilitate funding and resources allocation. Information provided by this article should help to elucidate the global disease burden and trends of DS and to build more effective intervention.
The datasets used in the present study are available in the Global Burden of Disease 2019.
LDL had full access to the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final manuscript. Concept and design: LDL and LYC. Acquisition, analysis, and interpretation of data: LYC, LFW, YW, HSH, and YZ. Drafting of the manuscript: LYC and LFW. Revision of the manuscript: LDL and ZLZ. Statistical analysis: LYC and LFW. Supervision: LDL. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are grateful to all staffs of the Global Burden of Disease Study for their work.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgene.2022.908482/full#supplementary-material
ASR, age-standardized rate; ASIR, age-standardized incident rate; ASDR, age-standardized death rate; CI, certainty interval; DALY, disability-adjusted life year; DS, Down syndrome; EAPC, estimated annual percentage change; GBD, global burden of disease; SDI, social-demographic index.
Agopian, A. J., Marengo, L. K., and Mitchell, L. E. (2012). Predictors of Trisomy 21 in the Offspring of Older and Younger Women. Birth Defects Res. A Clin. Mol. Teratol. 94, 31–35. doi:10.1002/bdra.22870
Allard, P., and Colaiacovo, M. P. (2010). Bisphenol A Impairs the Double-Strand Break Repair Machinery in the Germline and Causes Chromosome Abnormalities. Proc. Natl. Acad. Sci. U. S. A. 107, 20405–20410. doi:10.1073/pnas.1010386107
Arbuzova, S., Hutchin, T., and Cuckle, H. (2002). Mitochondrial Dysfunction and Down's Syndrome. Bioessays 24, 681–684. doi:10.1002/bies.10138
Asim, A., Kumar, A., Muthuswamy, S., Jain, S., and Agarwal, S. (2015). Down Syndrome: an Insight of the Disease. J. Biomed. Sci. 22, 41. doi:10.1186/s12929-015-0138-y
Baird, P. A., and Sadovnick, A. D. (1988). Maternal Age-specific Rates for Down Syndrome: Changes over Time. Am. J. Med. Genet. 29, 917–927. doi:10.1002/ajmg.1320290424
Bishop, J., Huether, C. A., Torfs, C., Lorey, F., and Deddens, J. (1997). Epidemiologic Study of Down Syndrome in a Racially Diverse California Population, 1989-1991. Am. J. Epidemiol. 145, 134–147. doi:10.1093/oxfordjournals.aje.a009084
Brieno-Enriquez, M. A., Robles, P., Camats-Tarruella, N., Garcia-Cruz, R., Roig, I., Cabero, L., et al. (2011). Human Meiotic Progression and Recombination Are Affected by Bisphenol A Exposure during In Vitro Human Oocyte Development. Hum. Reprod. 26, 2807–2818. doi:10.1093/humrep/der249
Chen, L., Wang, Q., Gao, Y., Zhang, J., Cheng, S., Chen, H., et al. (2021). The Global Burden and Trends of Maternal Sepsis and Other Maternal Infections in 204 Countries and Territories from 1990 to 2019. BMC Infect. Dis. 21, 1074. doi:10.1186/s12879-021-06779-0
Christianson, J. H., Modell, C. P., and Modell, B. (2006). March of Dimes Global Report on Birth Defects The Hidden Toll of Dying and Disabled Children. USA: White Plains, 2
Churchill, S. S., Kieckhefer, G. M., Landis, C. A., and Ward, T. M. (2012). Sleep Measurement and Monitoring in Children with Down Syndrome: a Review of the Literature. Sleep. Med. Rev. 16, 477–488. doi:10.1016/j.smrv.2011.10.003
Colvin, K. L., and Yeager, M. E. (2017). What People with Down Syndrome Can Teach Us about Cardiopulmonary Disease. Eur. Respir. Rev. official J. Eur. Respir. Soc. 26. doi:10.1183/16000617.0098-2016
Corder, J. P., Al Ahbabi, F. J. S., Al Dhaheri, H. S., and Chedid, F. (2017). Demographics and Co-occurring Conditions in a Clinic-Based Cohort with Down Syndrome in the United Arab Emirates. Am. J. Med. Genet. Part A 173, 2395–2407. doi:10.1002/ajmg.a.38338
Corona-Rivera, J. R., Martínez-Macías, F. J., Bobadilla-Morales, L., Corona-Rivera, A., Peña-Padilla, C., Rios-Flores, I. M., et al. (2019). Prevalence and Risk Factors for Down Syndrome: A Hospital-Based Single-Center Study in Western Mexico. Am. J. Med. Genet. Part A 179, 435–441. doi:10.1002/ajmg.a.61044
Crissman, B. G., Worley, G., Roizen, N., and Kishnani, P. S. (2006). Current Perspectives on Down Syndrome: Selected Medical and Social Issues. Am. J. Med. Genet. Part C Seminars Med. Genet. 142, 127–130. doi:10.1002/ajmg.c.30099
de Campos Gomes, F., de Melo-Neto, J. S., Goloni-Bertollo, E. M., and Pavarino, E. C. (2020). Trends and Predictions for Survival and Mortality in Individuals with Down Syndrome in Brazil: A 21-year Analysis. J. Intellect. Disabil. Res. 64, 551–560. doi:10.1111/jir.12735
de Graaf, G., Buckley, F., Dever, J., and Skotko, B. G. (2017). Estimation of Live Birth and Population Prevalence of Down Syndrome in Nine U.S. States. Am. J. Med. Genet. Part A 173, 2710–2719. doi:10.1002/ajmg.a.38402
de Graaf, G., Buckley, F., and Skotko, B. G. (2015). Estimates of the Live Births, Natural Losses, and Elective Terminations with Down Syndrome in the United States. Am. J. Med. Genet. Part A 167, 756–767. doi:10.1002/ajmg.a.37001
De Leon-Luis, J., Gamez, F., Bravo, C., Tenias, J. M., Arias, A., Perez, R., et al. (2014). Second-trimester Fetal Aberrant Right Subclavian Artery: Original Study, Systematic Review and Meta-Analysis of Performance in Detection of Down Syndrome. Int. Soc. Ultrasound Obstetrics Gynecol. 44, 147–153. doi:10.1002/uog.13336
Dierssen, M. (2012). Down Syndrome: the Brain in Trisomic Mode. Nat. Rev. Neurosci. 13, 844–858. doi:10.1038/nrn3314
Diseases, G. B. D., and Injuries, C. (2020). Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: a Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 396, 1204–1222. doi:10.1016/S0140-6736(20)30925-9
El Mouzan, M. I., Al Salloum, A. A., Al Herbish, A. S., Qurachi, M. M., and Al Omar, A. A. (2008). Consanguinity and Major Genetic Disorders in Saudi Children: A Community-Based Cross-Sectional Study. Ann. Saudi Med. 28, 169–173. doi:10.4103/0256-4947.51726
European Commission, and Eurostat (2015). Being young in Europe Today: 2015 Edn. Publications Office. doi:10.2785/59267
FerrucciC, L., BandinelliJ, KohS., and Guralnik, M. (2007). Disability, Functional Status, and Activities of Daily Living. Encycl. Gerontology 2007, 427–436. doi:10.1016/b0-12-370870-2/00075-5
Fiscella, K., Franks, P., Gold, M. R., and Clancy, C. M. (2000). Inequality in Quality: Addressing Socioeconomic, Racial and Ethnic Disparities in Health Care. J. Am. Med. Assoc. 283, 2579–2584. doi:10.1001/jama.283.19.2579
Fransen, M. P., Schoonen, M. H., Mackenbach, J. P., Steegers, E. A., de Koning, H. J., Laudy, J. A., et al. (2010). Ethnic Differences in Participation in Prenatal Screening for Down Syndrome: a Register-Based Study. Prenat. Diagn. 30, 988–994. doi:10.1002/pd.2603
Frias, S., Van Hummelen, P., Meistrich, M. L., Lowe, X. R., Hagemeister, F. B., Shelby, M. D., et al. (2003). NOVP Chemotherapy for Hodgkin's Disease Transiently Induces Sperm Aneuploidies Associated with the Major Clinical Aneuploidy Syndromes Involving Chromosomes X, Y, 18, and 21. Cancer Res. 63, 44–51.
Glivetic, T., Rodin, U., Milosevic, M., Mayer, D., Filipovic-Grcic, B., and Seferovic Saric, M. (2015). Prevalence, Prenatal Screening and Neonatal Features in Children with Down Syndrome: A Registry- Based National Study. Italian J. Pediatr. 41, 81. doi:10.1186/s13052-015-0192-9
Grieco, J., Pulsifer, M., Seligsohn, K., Skotko, B., and Schwartz, A. (2015). Down Syndrome: Cognitive and Behavioral Functioning across the Lifespan. Am. J. Med. Genet. Part C, Seminars Med. Genet. 169, 135–149. doi:10.1002/ajmg.c.31439
Grimm, J., Heckl, D., and Klusmann, J. H. (2021). Molecular Mechanisms of the Genetic Predisposition to Acute Megakaryoblastic Leukemia in Infants With Down Syndrome. Front. Oncol. 11, 636633. doi:10.3389/fonc.2021.636633
Kenny, L. C., Lavender, T., McNamee, R., O'Neill, S. M., Mills, T., and Khashan, A. S. (2013). Advanced Maternal Age and Adverse Pregnancy Outcome: Evidence from a Large Contemporary Cohort. PLoS ONE 8, e56583. doi:10.1371/journal.pone.0056583
Krivchenia, E., Huether, C. A., Edmonds, L. D., May, D. S., and Guckenberger, S. (1993). Comparative Epidemiology of Down Syndrome in Two United States Populations, 1970-1989. Am. J. Epidemiol. 137, 815–828. doi:10.1093/oxfordjournals.aje.a116743
Kuppermann, M., Learman, L. A., Gates, E., Gregorich, S. E., Nease, R. F., Lewis, J., et al. (2006). Beyond Race or Ethnicity and Socioeconomic Status: Predictors of Prenatal Testing for Down Syndrome. Obstetrics Gynecol. 107, 1087–1097. doi:10.1097/01.aog.0000214953.90248.db
Lal, C., White, D. R., Joseph, J. E., van Bakergem, K., and LaRosa, A. (2015). Sleep-disordered Breathing in Down Syndrome. Chest 147, 570–579. doi:10.1378/chest.14-0266
Loane, M., Morris, J. K., Addor, M. C., Arriola, L., Budd, J., Doray, B., et al. (2013). Twenty-year Trends in the Prevalence of Down Syndrome and Other Trisomies in Europe: Impact of Maternal Age and Prenatal Screening. Eur. J. Hum. Genet. 21, 27–33. doi:10.1038/ejhg.2012.94
McDowell, K. M., and Craven, D. I. (2011). Pulmonary Complications of Down Syndrome during Childhood. J. Pediatr. 158, 319–325. doi:10.1016/j.jpeds.2010.07.023
McGlinchey, E., McCallion, P., and McCarron, M. (2020). Down Syndrome and Dementia: Advances in the Field. Curr. Opin. Psychiatry 33, 278–283. doi:10.1097/yco.0000000000000589
Megarbane, A., Ravel, A., Mircher, C., Sturtz, F., Grattau, Y., Rethore, M. O., et al. (2009). The 50th Anniversary of the Discovery of Trisomy 21: the Past, Present, and Future of Research and Treatment of Down Syndrome. Genet. Med. 11, 611–616. doi:10.1097/gim.0b013e3181b2e34c
Mercer, E. S., Broecker, B., Smith, E. A., Kirsch, A. J., Scherz, H. C., and Massad, A. C. (2004). Urological Manifestations of Down Syndrome. J. urology 171, 1250–1253. doi:10.1097/01.ju.0000112915.69436.91
Mohsen Naghavi, H. W., Lozano, Rafael, Davis, Adrian, and Liang, Xiaofeng (2015). Maigeng Zhou, Stein Emil Vollset, Ayse Abbasoglu Ozgoren, Safa Abdalla, Foad Abd-Allah et al, Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385, 117–171.
Morris, J. K., and Alberman, E. (2009). Trends in Down's Syndrome Live Births and Antenatal Diagnoses in England and Wales from 1989 to 2008: Analysis of Data from the National Down Syndrome Cytogenetic Register. BMJ (Online) 339, 1188. doi:10.1136/bmj.b3794
Munne, S., Magli, C., Adler, A., Wright, G., de Boer, K., Mortimer, D., et al. (1997). Treatment-related Chromosome Abnormalities in Human Embryos. Hum. Reprod. 12, 780–784. doi:10.1093/humrep/12.4.780
Nations, U. (2014). Report of the Open Working Group of the General Assembly. United Stsates: Sustainable Development Goals.
Nordstrøm, M., Retterstøl, K., Hope, S., and Kolset, S. O. (2020). Nutritional Challenges in Children and Adolescents with Down Syndrome. Lancet Child Adolesc. Health 4, 455–464.
Nugent, J., Gorman, G., and Erdie-Lalena, C. R. (2018). Disparities in Access to Healthcare Transition Services for Adolescents with Down Syndrome. J. Pediatr. 197, 214–220. doi:10.1016/j.jpeds.2018.01.072
Omar, C. B.-P., Ahmad, B., Lopez, A. D., Murray, C. J. L., Lozano, R., and Inoue, M. (2001). Age Standardization of Rates: A New WHO Standard. GPE Discussion Paper Series: No 31, World Health.
Ray, A., Oliver, T. R., Halder, P., Pal, U., Sarkar, S., Dutta, S., et al. (2018). Risk of Down Syndrome Birth: Consanguineous Marriage Is Associated with Maternal Meiosis-II Nondisjunction at Younger Age and without Any Detectable Recombination Error. Am. J. Med. Genet. Part A 176, 2342–2349. doi:10.1002/ajmg.a.40511
Roizen, N. J., and Patterson, D. (2003). Down's Syndrome. Lancet 361, 1281–1289. doi:10.1016/s0140-6736(03)12987-x
Rowe, R., Puddicombe, D., Hockley, C., and Redshaw, M. (2008). Offer and Uptake of Prenatal Screening for Down Syndrome in Women from Different Social and Ethnic Backgrounds. Prenat. Diagn. 28, 1245–1250. doi:10.1002/pd.2125
Salomon, J. A. (2014). Disability-Adjusted Life Years. Encycl. Health Econ. 2014, 200–203. doi:10.1016/b978-0-12-375678-7.00511-3
Stevens, G. A., Alkema, L., Black, R. E., Boerma, J. T., Collins, G. S., Ezzati, M., et al. (2016). Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER Statement. Lancet 388, e19–e23. doi:10.1016/s0140-6736(16)30388-9
Stores, G., and Stores, R. (2013). Sleep Disorders and Their Clinical Significance in Children with Down Syndrome. Dev. Med. child neurology 55, 126–130. doi:10.1111/j.1469-8749.2012.04422.x
Takeuchi, A., Ehara, H., Ohtani, K., Maegaki, Y., Nanba, Y., Nagata, I., et al. (2008). Live Birth Prevalence of Down Syndrome in Tottori, Japan, 1980-1999. Am. J. Med. Genet. Part A 146, 1381–1386. doi:10.1002/ajmg.a.32279
Tsou, A. Y., Bulova, P., Capone, G., Chicoine, B., Gelaro, B., Harville, T. O., et al. (2020). Down Syndrome Foundation Medical Care Guidelines for Adults with Down Syndrome, Medical Care of Adults With Down Syndrome: A Clinical Guideline. Jama 324, 1543–1556. doi:10.1001/jama.2020.17024
Verstegen, R. H. J., Chang, K. J. J., and Kusters, M. A. A. (2020). Clinical Implications of Immune-Mediated Diseases in Children with Down Syndrome. Eur. Soc. Pediatr. Allergy Immunol. 31, 117–123.doi:10.1111/pai.13133
Verstegen, R. H. J., and Kusters, M. A. A. (2020). Inborn Errors of Adaptive Immunity in Down Syndrome. J. Clin. Immunol. 40, 791–806. doi:10.1007/s10875-020-00805-7
Keywords: down syndrome, GBD 2019, social demographic index, incidence, mortality, disability-adjusted life years
Citation: Chen L, Wang L, Wang Y, Hu H, Zhan Y, Zeng Z and Liu L (2022) Global, Regional, and National Burden and Trends of Down Syndrome From 1990 to 2019. Front. Genet. 13:908482. doi: 10.3389/fgene.2022.908482
Received: 28 April 2022; Accepted: 15 June 2022;
Published: 15 July 2022.
Edited by:
Valentina Massa, University of Milan, ItalyReviewed by:
Emilia Severin, Carol Davila University of Medicine and Pharmacy, RomaniaCopyright © 2022 Chen, Wang, Wang, Hu, Zhan, Zeng and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lidan Liu, MTM4NjU4N0BxcS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.