
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Genet., 19 May 2022
Sec. Pharmacogenetics and Pharmacogenomics
Volume 13 - 2022 | https://doi.org/10.3389/fgene.2022.836970
This article is part of the Research TopicPharmacogenomics in Asians: Differences and Similarities with other Human PopulationsView all 6 articles
 Serim Kim1†
Serim Kim1† Jong Do Seo2†
Jong Do Seo2† Yeo-Min Yun2,3*Hanah Kim2,3Tae-Eun Kim4Taeheon Lee5Tae-Rim Lee5
Yeo-Min Yun2,3*Hanah Kim2,3Tae-Eun Kim4Taeheon Lee5Tae-Rim Lee5 Jun Hyung Lee6Eun-Hae Cho5
Jun Hyung Lee6Eun-Hae Cho5 Chang-Seok Ki5
Chang-Seok Ki5Background: Statins are the most popular agents for the primary and secondary prevention of cardiovascular disease; however, the pharmacokinetic parameters and associated genetic factors in the Korean population have not been fully elucidated. This study explored the pharmacokinetic properties of atorvastatin and the association between genetic variations and atorvastatin pharmacokinetics in healthy Korean subjects.
Methods: Atorvastatin (80 mg) was administered to 35 healthy Korean volunteers. Plasma levels of atorvastatin and its metabolites were measured sequentially using liquid chromatography-tandem mass spectrometry from 0 to 24 h after atorvastatin administration. Customized next-generation sequencing analysis was performed covering all coding exons of 15 genes, as well as 46 single-nucleotide variants in 29 genes related to statin pharmacokinetics.
Results: The mean area under the concentration-time (AUC) and Cmax (maximum peak concentration) were 269.0 ng/ml∙h and 84.3 ng/ml, respectively, which were approximately two times higher than those reported in Caucasians. Genetic analysis revealed that eight genetic variants in ABCB1, ABCG2, APOA5, CETP, and CYP7A1 contributed to the AUC of atorvastatin. The atorvastatin AUC0–24 h prediction model was developed based on age and eight genetic variants using multivariate linear regression (adjusted R2 = 0.878, p < 0.0001).
Conclusion: This study shows that the pharmacokinetic properties of atorvastatin in Koreans are different from those in Caucasians and that atorvastatin AUC0–24 h could be predicted based on age and eight genetic variants of ABCB1, ABCG2, APOA5, CETP, and CYP7A1.
Statins are used as a first-line treatment for the primary prevention of atherosclerotic cardiovascular disease (ASCVD) in patients with elevated low-density lipoprotein cholesterol (LDL-C) levels, those with diabetes mellitus between the age of 40–75 years, and those who are at sufficient ASCVD risk as assessed by clinician-patient risk discussion (Arnett et al., 2019). Atorvastatin and rosuvastatin are prescribed as drugs of choice for high-or medium-intensity statin therapy (Adams et al., 2015).
Adverse events associated with statin use are a major cause of noncompliance; the most common being statin myositis and statin-associated muscle symptoms (SAMS) (Law and Rudnicka, 2006). Although the mechanisms of SAMS are not completely understood, it is considered that the risk of myopathy is dose-related and dependent on systemic drug exposure (Holbrook et al., 2011). However, not all patients receiving the same dose experience adverse events or have the same LDL-C lowering effect, implying that genetic variants affecting statin pharmacokinetics (PK) may influence the incidence and severity of statin adverse events. The Clinical Pharmacogenetics Implementation Consortium (CPIC) prescribing guidelines for simvastatin based on the SLCO1B1 variant is a commonly cited example of formal guidance regarding pharmacogenetics related to statin toxicity (Ramsey et al., 2014).
Reports on the effects of genetic variations on statin pharmacokinetics have been inconsistently replicated, and there are limited data available in Asian populations (Gandelman et al., 2012). Moreover, there are many variations in metabolic processes according to statin type, frequency of genetic variants, and responses to statins according to ethnic background (Liao, 2007). Results of the HPS2-THRIVE study evaluating the effect of extended release niacin plus laropiprant (ERN/LRPT) on statin adverse events indicated that the incidence rate of myopathy and increased liver enzymes in the Chinese population was approximately 3 times higher than that in Europeans with the same statin dose (simvastatin 40 mg daily) and it can increased up to 10 times higher with additional ERN/LRPT regimen (Group, 2013).
The aim of our study was to explore the PK properties of atorvastatin, to investigate the association between atorvastatin PK and genetic variants during the early phase of PK after oral administration of atorvastatin in healthy Korean subjects, and to establish a PK prediction model based on genetics.
This study was approved by the Institutional Review Board of Konkuk University Medical Center (KUH1200102) and the Korean Ministry of Food and Drug Safety (KMFDS). Thirty-five healthy Korean volunteers between the ages of 20 and 55 were enrolled, with written informed consent from each participant. All the subjects were confirmed to be eligible for the study, not having any current or pre-existing medical condition, not taking any medications, and showing no abnormal findings on the laboratory tests. Medical record review and routine check for admission of inpatients, including physical examination, vital signs, electrocardiogram, and laboratory tests, were performed. The subjects received a single oral dose of 80 mg atorvastatin calcium at 8:30 a.m. in an overnight fasting state. After 4 h of additional fasting, lunch and dinner were permitted. Venous blood was collected via an intravenous catheter prior to drug administration (0 h) and at 0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, 8, 11, and 24 h after dosing for pharmacokinetic analysis. After collection, all samples were immediately centrifuged, aliquoted, and stored frozen. Genetic analysis was performed using the first blood sample (0 h).
The plasma concentrations of atorvastatin and its two active metabolites [para-hydroxy (p-OH) and ortho-hydroxy (o-OH) atorvastatin] were measured by liquid chromatography-tandem mass spectrometry (LC-MS/MS) using a 5500 QTRAP mass spectrometer (Sciex, Framingham, MA, United States) at Green Cross Laboratories (Yongin-si, Gyeonggi-do, South Korea). Standard compounds of atorvastatin, p-OH atorvastatin, o-OH atorvastatin, and deuterium-labeled atorvastatin (atorvastatin-d5) were purchased from TLC Pharmaceutical Standards Ltd. (Newmarket, Ontario, Canada). LC-MS/MS analysis was performed with the protocol that authors have presented as poster at the 11th Annual North American Conference of The Association for Mass Spectrometry: Applications to the Clinical Lab (Kim et al., 2019), by using atorvastatin-d5 (1 μg/ml in 50% acetonitrile) as an internal standard (IS).
The actual concentration-time profile was plotted, and the PK parameters were determined using non-compartmental analyses by BA-Calc 2007 (Ministry of Food and Drug Safety, Osong, South Korea) and PKSolver (Zhang et al., 2010). The maximum plasma concentration (Cmax) and time to achieve Cmax (Tmax) were determined directly from the plasma concentration. The rate constant was calculated by performing a linear regression of the logarithmic concentration-time curve in the terminal phase. The area under the plasma concentration curve from 0 h to infinity (AUC∞) was calculated using a combination of the linear trapezoidal method and extrapolation to infinity by the elimination rate constant.
As shown in Supplementary Table S1, 15 genes and 46 non-exon single nucleotide polymorphisms (SNPs) in 29 genes were selected for genetic analysis based on associations with the absorption, distribution, metabolism, and elimination (ADME) of statins and their effects on lipid metabolism, as compiled by the PharmGKB database and previous studies (Mangravite et al., 2006; Wang et al., 2011; Canestaro et al., 2014; Leusink et al., 2016; Maxwell et al., 2017). The SNP of TCF7L2 is also added to this panel, which is known to be associated with the risk of diabetes mellitus (DM) as a side effect of statins (Chen et al., 2018). Genomic DNA was extracted from EDTA whole blood using a Chemagen DNA Blood Kit (PerkinElmer, Baesweiler, Germany). A custom panel (Integrated DNA Technologies, Coralville, Iowa, United States) was used for library preparation, and sequencing was performed on an Illumina MiSeqDX (Illumina Inc., San Diego, CA, Unites States), generating 2 × 150 bp paired-end reads. Alignment of sequence reads, indexing of the reference genome (hg19), and variant calling with a pipeline were based on Genome Analysis Tool Kit (GATK) Best Practices (DePristo et al., 2011). Alignment was performed using Burrows-Wheeler Aligner-maximum exact matches (BWA-MEM), version 0.7.12 (http://bio-bwa.sourceforge.net), and duplicated reads were marked with Picard, version 1.138 (http://picard.sourceforge.net). Local alignment, base quality recalibration, and variant calling of each sample was performed using the HaplotypeCaller of GATK, version 3.5 (Broad Institute, Cambridge, MA, United States) (McKenna et al., 2010) in the -ERC GVCF mode. After generating GVCFs for all samples, joint genotyping was performed using GATK GenotypeGVCFs. The VCF cohort was converted to a PLINK format using PLINK v1.9. Variant annotation was performed using Variant Effect Predictor (VEP) (McLaren et al., 2016) and non-synonymous functional predictions (dbNSFP) (Liu et al., 2016).
Prior to conducting statistical analysis, quality control procedures were implemented on both genotype and phenotype data. SNPs with missing rates of >5%, minor allele frequencies of <0.01, or significant deviation from Hardy–Weinberg equilibrium (p < 0.00001) were removed. The removed SNPs were rs4987144, rs1985842, rs111564371, rs112568578, rs113889384, rs28371713, and rs111606937 in CYP2D6. As quantitative trait association analysis assumes that the phenotypes are normally distributed, a rank-based inverse normal transformation method was applied to the raw phenotype values according to a previous report (Goh and Yap, 2009). Linear regression analysis for each SNP was performed using PLINK v1.9 (http://pngu.mgh.harvard.edu/purcell/plink) (Purcell et al., 2007) after adjusting for age, sex, and body weight.
From the results of linear regression for each of 467 SNPs, 24 SNPs were used for variable selection with p-value ≤0.05. Stepwise regression was performed in order to develop Statin AUC prediction model. The regression was run in R version 4.0.5 using the stepAIC() function from the MASS library. Starting from a model that included all variables (24 SNPs and age), either deleted the variable that was least helpful to the standard statistic or added the variable that improved the standard statistic most, among the missing variables in the model. Then, the addition or deletion of these SNP variables had been repeated. As a result, eight of the 24 variants were selected with age as the essential variable, and the dosage information of all 35 samples was the same as 80 mg. We adjusted the formula using the dosage value/80 (Equation in Table 3). The genotypes were coded as 0, 1, or 2 (additive effect model). Statistical analyses were performed using R version 4.0.5.
The baseline characteristics of the 35 participants are summarized in Table 1. The male to female ratio was 6:4, and the average age, height, and weight were 34.5 years (range, 22–52 years), 168.7 cm (range, 151.1–182.9 cm), and 68.6 kg (range, 52.5–90.7 kg), respectively. Mean plasma concentrations (mg/dl) were as follows: total cholesterol, 171.98; HDL-C, 50.30; LDL-C, 99.62; triglycerides, 103.70; ApoA-I, 135.41; ApoA-II, 29.91; ApoB, 82.17 7, and Lp(a),27.48 nmol/L.
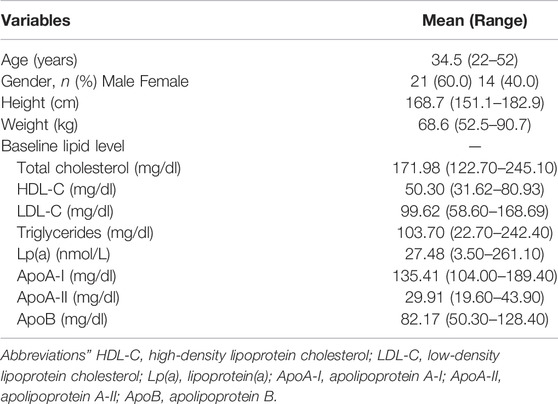
TABLE 1. Characteristics of the study population (n = 35).
The PK parameters of atorvastatin were as follows: the mean AUC0–24 h was 269.0 ng∙h/mL; AUC∞ was 279.4 ng∙h/mL; Cmax was 84.3 ng/ml; time to reach maximum plasma concentration (Tmax) was 1.4 h, and elimination half-life (T1/2) was 5.5 h (Table 2). PK parameters showed marked inter-individual variability, with a coefficient of variation ranging from 17.8 to 60.8%. The values of AUC0–24 h and Cmax obtained in this study were about two times higher than those obtained in a white population (269.0 vs. 146.8 ng∙h/mL and 84.3 vs. 34.8 ng/ml, respectively) (Gandelman et al., 2011).
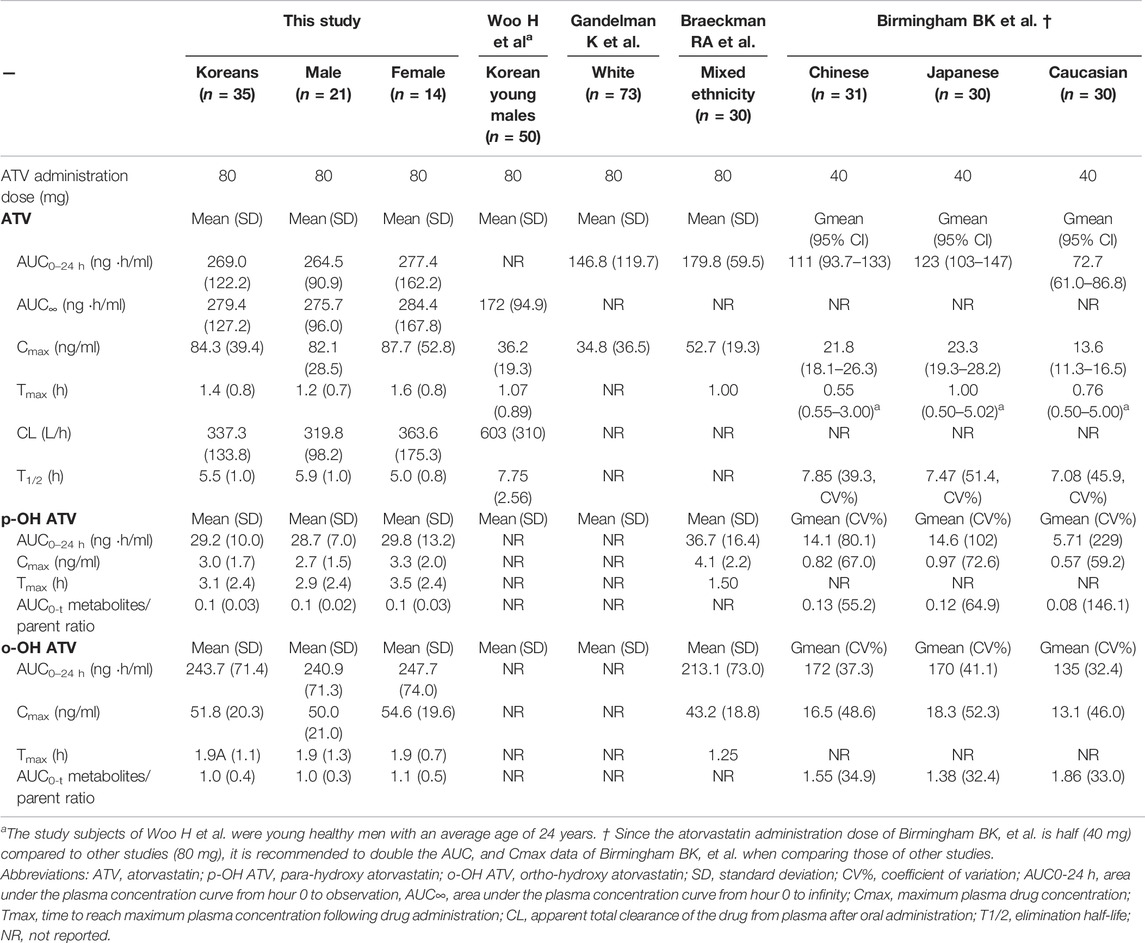
TABLE 2. Comparison of pharmacokinetic parameters of atorvastatin and its metabolites between our study subjects and other reports.
The plasma concentration-time plots of atorvastatin after administration are shown as mean ± standard deviation (SD) values in Figure 1A. Figures 1B–D show the mean plasma concentration-time profile and the gender-differentiated profile after excluding one female outlier whose PK characteristics for atorvastatin were extremely high.
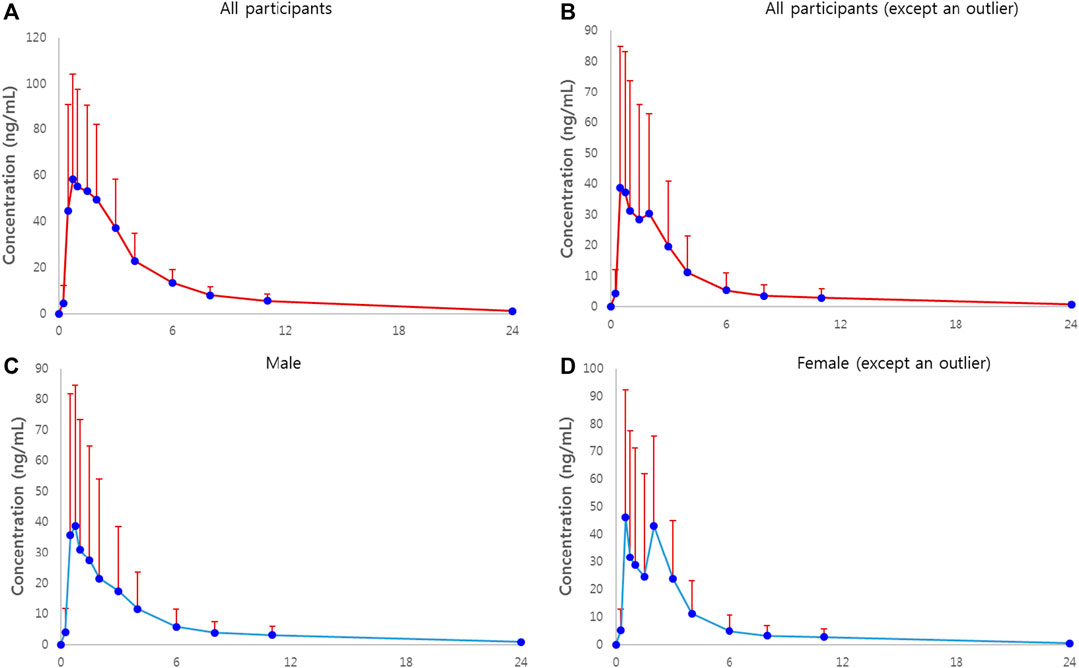
FIGURE 1. Plasma concentration-time plots of atorvastatin in healthy subjects receiving a single dose of 80 mg atorvastatin. (A) Plot of all participants. Solid circles represent mean concentrations of plasma atorvastatin, and bars represent standard deviations. (B) Plot of all participants, excluding an outlier of AUC∞ of atorvastatin. (C) Plot of all male participants. (D) Plot of all female participants, excluding an outlier of AUC∞ of atorvastatin.
A total of 467 variants were identified. Twenty-one genetic variants from seven genes were associated with PK parameters according to genotype (p < 0.01 in linear regression analysis; Supplementary Table S2). However, no genetic variants had a false discovery rate (FDR) p-value of <0.05.
In multivariate linear regression using stepwise selection to create a statin AUC prediction model, eight genetic variants of ABCB1, ABCG2, APOA5, CETP, and CYP7A1 were selected, with age as the essential variable to predict atorvastatin AUC0–24 h (adjusted R2 = 0.878, p < 0.0001) (Table 3).
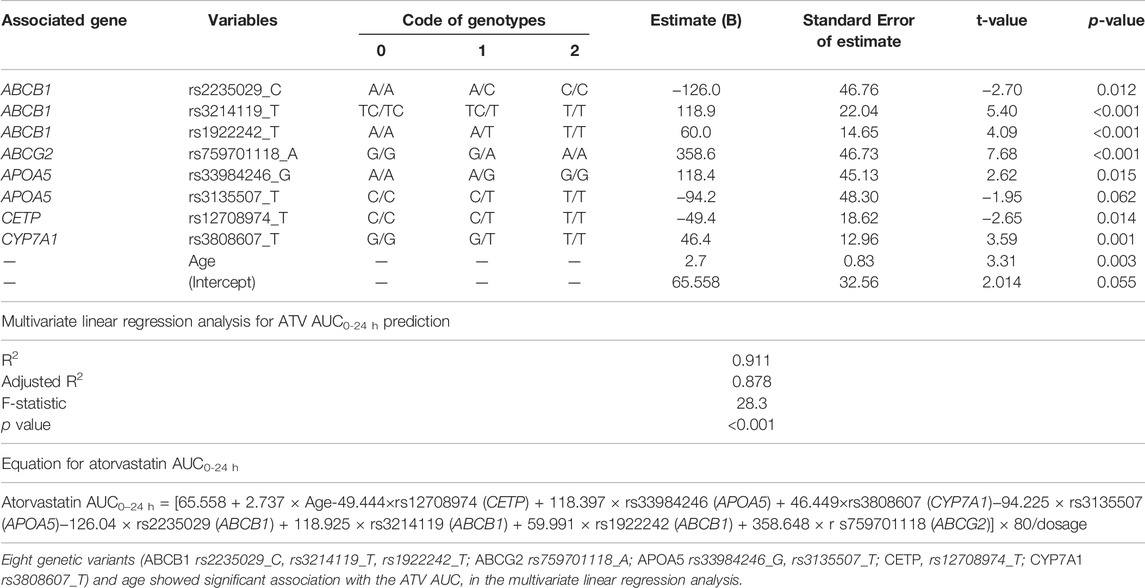
TABLE 3. Multivariate linear regression analysis for AUC0–24 h prediction based on the genetic variants affecting the pharmacokinetics of atorvastatin.
Two individuals had PK parameter values higher than twice the average values for the other patients: one in AUC∞ and Cmax of atorvastatin (Participant 16: 40 years old, woman), and the other in AUC0-24 h and Cmax of metabolites (Participant 11: 51 years old, man). Genetic variants identified only in these two individuals are shown in Supplementary Table S3, and their plasma drug concentration-time plots are shown in Supplementary Figure S1.
In this study, the PK properties of atorvastatin in healthy Korean subjects differed from those previously reported (Table 2). The average atorvastatin AUC0–24 h and Cmax in this study were relatively higher than those reported by Woo et al. for the Korean population, which may be associated with the relative decrease in atorvastatin elimination capability (relatively low CL/F of 56% compared to that of Woo et al.) due to differences in the composition of the study subjects (age range from 21 to 51 years, including women vs. young, healthy men with an average age of 24 years) (Woo et al., 2017). In the multivariate linear regression analysis to estimate atorvastatin AUC, old age showed a significant association with the increasing atorvastatin AUC (Table 3), and this finding agrees well with a previous study that revealed a decrease in ATV elimination with increasing age (Gibson et al., 1996). This previous study revealed the shorter half-life in women agree with present study, however it showed lower AUC in female contrary to our study.
In addition, the average AUC0–24 h and Cmax in this study were about two times higher than those reported in a white population (269.0 vs. 146.8 ng∙h/mL and 84.3 vs. 34.8 ng/ml, respectively) (Gandelman et al., 2011). This finding suggests that with a high-dose (80 mg) treatment, atorvastatin exposure is relatively higher in the Korean population than in the Western population. Previous studies have reported higher rosuvastatin exposure in Asian populations compared to that in Caucasians (Lee et al., 2005; Li et al., 2007). The AUC for Asians was approximately twice that of Caucasians with the same dose of rosuvastatin, suggesting that Asians are more sensitive to statins (Lee et al., 2005). A comparative study on the systemic exposure of rosuvastatin, atorvastatin, and simvastatin in Caucasian and Asian subjects indicated that not only rosuvastatin but also atorvastatin exposure is higher in the Asian population than in the Caucasian population (Birmingham et al., 2015). The geometric mean AUC from time zero to the last quantifiable concentration was 86% (90% confidence interval, 51–130%) and 55% (26–91%) higher for rosuvastatin in Chinese and Japanese subjects than in Caucasians, respectively, and 53% (25–88%) and 69% (37–108%) higher for atorvastatin (Birmingham et al., 2015). Furthermore, the genetic variants in SLCO1B1 T521 > C or ABCG2 C421 > A were associated with higher exposure to rosuvastatin, atorvastatin, and simvastatin acid (Birmingham et al., 2015). However, even in the absence of both these genetic variants, ethnic differences in exposure were still observed; the underlying mechanism is suggested to be related to increased statin absorption in Asians compared with Caucasians (Birmingham et al., 2015). The finding of relatively high AUC and Cmax in this study is consistent with a previous report demonstrating higher statin exposure in Asian subjects compared to Caucasians, suggesting that increased statin exposure may be associated with the higher incidence rate of statin side effects in Asian populations than in Western populations.
We selected 15 genes and 46 non-exon SNPs in 29 genes for analysis. A total of 467 genetic variants were found in the 35 Korean subjects, and among them, 21 variants from seven genes were associated with PK parameters according to genotype (p < 0.01 in linear regression analysis; Supplementary Table S1). In multivariate linear regression using stepwise selection for the creation of a statin AUC prediction model, eight genetic variants of ABCB1 (rs2235029_C, rs3214119_T, rs1922242_T), ABCG2 (rs759701118_A), APOA5 (rs33984246_G, rs3135507_T), CETP (rs12708974_T), and CYP7A1 (rs3808607_T) and age were selected to predict atorvastatin AUC0–24 h (adjusted R2 = 0.878, p < 0.0001) (Table 3).
In our study, genetic variants of ABCB1 (rs2235029_C, rs3214119_T, rs1922242_T) and ABCG2 (rs759701118_A) were significantly associated with the level of atorvastatin exposure (AUC) (Table 3). The efflux ATP-binding cassette transporters of ABCB1 and ABCG2 play a key role in the pharmacokinetics, safety, and lipid-lowering efficacy of statins (Niemi, 2010; Tomlinson et al., 2010; Chasman et al., 2012). ABCB1 transport protein is involved in hepato-biliary and renal-urinary transport of statins and metabolites. Functional genetic variants in ABCB1 and ABCG2 related to reduced activity of the transporters have been found to be significantly associated with increased statin exposure (Niemi, 2010) and affect the safety and lipid-lowering efficacy of statins (Hu et al., 2010; Chasman et al., 2012). The functional genetic variant of 421 C > A (rs2231142) in ABCG2, that reduces transporter activity has been found to be associated with increased systemic exposure and lipid-lowering effect of statins (Hu et al., 2010; Chasman et al., 2012). The functional genetic variant of 421 C > A (rs2231142) in ABCG2 to reduce transporter activity was associated with increased systemic exposure and the lipid-lowering effect of statins (Hu et al., 2010; Tomlinson et al., 2010; Chasman et al., 2012). Genetic variants in ABCG2 C421 > A are associated with higher exposure to atorvastatin in Chinese and Japanese subjects than in Caucasians (Birmingham et al., 2015). However, since an ethnic difference in exposure was still observed in the absence of the ABCG2 421 C > A variant, another genetic change could differentially impact the function of ABCG2 between populations (Birmingham et al., 2015). Since ABCB1 and ABCG2 play an essential role in statin transport, the genetic variations of ABCB1 and ABCG2 may be related to differences in the degree of statin exposure between individuals or races.
Bile acid biosynthesis by cholesterol 7α-hydroxylase (CYP7A1) is a major pathway for the removal of cholesterol into bile. A common promoter variant in CYP7A1 (A-204C, rs3808607) is significantly associated with a poor response to atorvastatin (Kajinami et al., 2005; Kadam et al., 2016), which may be due to reduced gene expression (Pullinger et al., 2002). Patients with the GG or GT genotype of CYP7A1 (rs3808607) may have a decreased response to atorvastatin compared to patients with the TT genotype (Kajinami et al., 2005; Kadam et al., 2016). In this study, subjects with GG or GT genotypes of CYP7A1 (rs3808607) showed lower atorvastatin AUC values than those with the TT genotype (Supplementary Figure S2), which suggests that a decreased response to atorvastatin in subjects with the GG or GT genotype may be due to the lower atorvastatin AUC values in the GG or GT genotype compared to the TT genotype.
Our study also showed that the genetic variants of APOA5 (rs33984246_G, rs3135507_T) and CETP (rs12708974_T) are associated with the AUC of atorvastatin. CETP plays an important role in cholesterol metabolism by bringing cholesterol esters into the liver and transferring triglycerides from LDL to HDL (Freeman et al., 1994). Genetic variants of CETP have been associated with cholesterol levels, response to statins, and clinical outcomes, such as myocardial infarction or stroke (Freeman et al., 1994; Kuivenhoven et al., 1998). Apolipoprotein A5 plays a key role in lipid metabolism, especially in the regulation of triglycerides. APOA5 genetic variants are associated with hypertriglyceridemia (Martin-Campos et al., 2014). The APOA5 variants (rs3135506) elevate triglyceride levels and shift the entire lipoprotein subclass distribution to atherosclerotic dyslipidemia in patients with high cardiovascular risk (Wang et al., 2008). Collectively, although the genetic variants of CETP might affect the efficacy of statins to reduce cardiovascular risk, and the variants of APOA5 may be associated with hypertriglyceridemia, further studies are needed to elucidate the exact meaning of the findings in this study.
In this prospective study, we investigated the PK characteristics and lipid-related efficacy of a single high-dose atorvastatin administration in healthy Korean individuals. However, we acknowledge the limitations of our study. Because of the small sample size, our study may not have sufficient power to detect potentially relevant differences. Therefore, most associations could have been missed or underestimated. Moreover, a considerable number of statistically significant SNPs have not been previously studied. It will also be important to verify our results in prospective studies performed on a larger scale, with various ethnic populations, including other Asian subjects, because the nonreproducibility of results commonly undermines genetic association studies.
The strength of our study is that this is the first demonstration to estimate atorvastatin AUC based on the information of genetic variants associated with atorvastatin pharmacokinetics. Moreover, because this study utilized next-generation sequencing (NGS) technology for genomic analysis, it provides more comprehensive information than previous sequencing studies. Our findings may contribute to the basic data needed for therapeutic drug monitoring. Further studies on the correlation between the AUC or Cmax of atorvastatin and the side effects of atorvastatin could support the value of further pharmacogenomic studies on inter-individual PK of atorvastatin.
We demonstrated the PK parameters of atorvastatin and its active metabolites and analyzed the values 24 h after single high-dose statin administration in a healthy Korean population. The mean atorvastatin area under the concentration-time and maximum peak concentration was approximately two times higher than that reported in Caucasians, which is consistent with a previous report of increased statin sensitivity in Asian subjects. Furthermore, we also developed an atorvastatin AUC0–24 h prediction model based on the eight genetic variants related to atorvastatin pharmacokinetics. This study suggests that genetic variants of ABCB1, ABCG2, APOA5, CETP, and CYP7A1 contribute to the variability of atorvastatin exposure in the Korean population.
The original contributions presented in the study are publicly available. This data can be found on NCBI SRA, BioProject: PRJNA791416 (https://www.ncbi.nlm.nih.gov/bioproject/PRJNA791416).
The studies involving human participants were reviewed and approved by the Institutional Review Board of Konkuk University Medical Center Institutional Review Board of Korean Ministry of Food and Drug Safety. The patients/participants provided their written informed consent to participate in this study.
SK, JDS, and Y-MY drafted the manuscript. SK, HK, and E-HC aquisited data. SK, TL and T-RL analyzed data and interpreted the result. Y-MY, T-EK, TL, and E-HC designed the study. Y-MY, JDS and JHL revised and approved final manuscript. JS and C-SK drafted revised manuscript. All authors reviewed the manuscript and provided critical feedback.
This study funded by Korea-Czech bilateral joint fund international joint technology development project of the Ministry of Trade, Industry and Energy, Korea (No. 2017-52, Task Number N061700001). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authors TL, T-RL, E-HC, and C-SK were employed by the company GC Genome.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgene.2022.836970/full#supplementary-material
Adams, S. P., Tsang, M., and Wright, J. M. (2015). Atorvastatin for Lowering Lipids. Cochrane Database Syst. Rev. 3, CD008226. doi:10.1002/14651858.CD008226.pub3
Arnett, D. K., Blumenthal, R. S., Albert, M. A., Buroker, A. B., Goldberger, Z. D., Hahn, E. J., et al. (2019). 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 140 (11), e596–e646. doi:10.1161/CIR.0000000000000678
Birmingham, B. K., Bujac, S. R., Elsby, R., Azumaya, C. T., Wei, C., Chen, Y., et al. (2015). Impact of ABCG2 and SLCO1B1 Polymorphisms on Pharmacokinetics of Rosuvastatin, Atorvastatin and Simvastatin Acid in Caucasian and Asian Subjects: a Class Effect? Eur. J. Clin. Pharmacol. 71 (3), 341–355. doi:10.1007/s00228-014-1801-z
Canestaro, W. J., Austin, M. A., and Thummel, K. E. (2014). Genetic Factors Affecting Statin Concentrations and Subsequent Myopathy: a HuGENet Systematic Review. Genet. Med. 16 (11), 810–819. doi:10.1038/gim.2014.41
Chasman, D. I., Giulianini, F., MacFadyen, J., Barratt, B. J., Nyberg, F., and Ridker, P. M. (2012). Genetic Determinants of Statin-Induced Low-Density Lipoprotein Cholesterol Reduction. Circ. Cardiovasc. Genet. 5 (2), 257–264. doi:10.1161/CIRCGENETICS.111.961144
Chen, X., Ayala, I., Shannon, C., Fourcaudot, M., Acharya, N. K., Jenkinson, C. P., et al. (2018). The Diabetes Gene and Wnt Pathway Effector TCF7L2 Regulates Adipocyte Development and Function. Diabetes 67 (4), 554–568. doi:10.2337/db17-0318
DePristo, M. A., Banks, E., Poplin, R., Garimella, K. V., Maguire, J. R., Hartl, C., et al. (2011). A Framework for Variation Discovery and Genotyping Using Next-Generation DNA Sequencing Data. Nat. Genet. 43 (5), 491–498. doi:10.1038/ng.806
Freeman, D. J., Griffin, B. A., Holmes, A. P., Lindsay, G. M., Gaffney, D., Packard, C. J., et al. (1994). Regulation of Plasma HDL Cholesterol and Subfraction Distribution by Genetic and Environmental Factors. Associations between the TaqI B RFLP in the CETP Gene and Smoking and Obesity. Arterioscler Thromb. 14 (3), 336–344. doi:10.1161/01.atv.14.3.336
Gandelman, K., Malhotra, B., R. LaBadie, R., Crownover, P., and Bergstrom, T. (2011). Analytes of Interest and Choice of Dose: Two Important Considerations in the Design of Bioequivalence Studies with Atorvastatin. Jbb 03 (4), 062–068. doi:10.4172/jbb.1000060
Gandelman, K., Fung, G. L., Messig, M., and Laskey, R. (2012). Systemic Exposure to Atorvastatin between Asian and Caucasian Subjects. Am. J. Ther. 19 (3), 164–173. doi:10.1097/MJT.0b013e3181f28fb5
Gibson, D. M., Bron, N. J., Richens, M. A., Hounslow, N. J., Sedman, A. J., and Whitfield, L. R. (1996). Effect of Age and Gender on Pharmacokinetics of Atorvastatin in Humans. J. Clin. Pharmacol. 36 (3), 242–246. doi:10.1002/j.1552-4604.1996.tb04194.x
Goh, L., and Yap, V. B. (2009). Effects of Normalization on Quantitative Traits in Association Test. BMC Bioinformatics 10, 415. doi:10.1186/1471-2105-10-415
Group, H. T. C., Haynes, R., Jiang, L., Hopewell, J. C., Li, J., Chen, F., et al. (2013). HPS2-THRIVE Randomized Placebo-Controlled Trial in 25 673 High-Risk Patients of ER Niacin/laropiprant: Trial Design, Pre-specified Muscle and Liver Outcomes, and Reasons for Stopping Study Treatment. Eur. Heart J. 34 (17), 1279–1291. doi:10.1093/eurheartj/eht055
Holbrook, A., Wright, M., Sung, M., Ribic, C., and Baker, S. (2011). Statin-associated Rhabdomyolysis: Is There a Dose-Response Relationship? Can. J. Cardiol. 27 (2), 146–151. doi:10.1016/j.cjca.2010.12.024
Hu, M., Lui, S. S. H., Mak, V. W. L., Chu, T. T. W., Lee, V. W. Y., Poon, E. W. M., et al. (2010). Pharmacogenetic Analysis of Lipid Responses to Rosuvastatin in Chinese Patients. Pharmacogenet Genomics 20 (10), 634–637. doi:10.1097/FPC.0b013e32833de489
Kadam, P., Ashavaid, T. F., Ponde, C. K., and Rajani, R. M. (2016). Genetic Determinants of Lipid-Lowering Response to Atorvastatin Therapy in an Indian Population. J. Clin. Pharm. Ther. 41 (3), 329–333. doi:10.1111/jcpt.12369
Kajinami, K., Brousseau, M. E., Ordovas, J. M., and Schaefer, E. J. (2005). A Promoter Polymorphism in Cholesterol 7α-Hydroxylase Interacts with Apolipoprotein E Genotype in the LDL-Lowering Response to Atorvastatin. Atherosclerosis 180 (2), 407–415. doi:10.1016/j.atherosclerosis.2004.12.019
Kim, S. P., Kim, H., and Yun, Y. M. (2019). Validation of a LC-MS/MS Method for the Quantification of Plasma Atorvastatin, Rosuvastatin, and Their Metabolites. Palm Springs, CA: MSACL 2019 US, 94.
Kuivenhoven, J. A., Jukema, J. W., Zwinderman, A. H., de Knijff, P., McPherson, R., Bruschke, A. V. G., et al. (1998). The Role of a Common Variant of the Cholesteryl Ester Transfer Protein Gene in the Progression of Coronary Atherosclerosis. N. Engl. J. Med. 338 (2), 86–93. doi:10.1056/NEJM199801083380203
Law, M., and Rudnicka, A. R. (2006). Statin Safety: a Systematic Review. Am. J. Cardiol. 97 (8A), S52–S60. doi:10.1016/j.amjcard.2005.12.010
Lee, E., Ryan, S., Birmingham, B., Zalikowski, J., March, R., Ambrose, H., et al. (2005). Rosuvastatin Pharmacokinetics and Pharmacogenetics in white and Asian Subjects Residing in the Same Environment. Clin. Pharmacol. Ther. 78 (4), 330–341. doi:10.1016/j.clpt.2005.06.013
Leusink, M., Onland-Moret, N. C., de Bakker, P. I., de Boer, A., and Maitland-van der Zee, A. H. (2016). Seventeen Years of Statin Pharmacogenetics: a Systematic Review. Pharmacogenomics 17 (2), 163–180. doi:10.2217/pgs.15.158
Li, Y., Jiang, X., Lan, K., Zhang, R., Li, X., and Jiang, Q. (2007). Pharmacokinetic Properties of Rosuvastatin after Single-Dose, Oral Administration in Chinese Volunteers: a Randomized, Open-Label, Three-Way Crossover Study. Clin. Ther. 29 (10), 2194–2203. doi:10.1016/j.clinthera.2007.10.005
Liao, J. K. (2007). Safety and Efficacy of Statins in Asians. Am. J. Cardiol. 99 (3), 410–414. doi:10.1016/j.amjcard.2006.08.051
Liu, X., Wu, C., Li, C., and Boerwinkle, E. (2016). dbNSFP v3.0: A One-Stop Database of Functional Predictions and Annotations for Human Nonsynonymous and Splice-Site SNVs. Hum. Mutat. 37 (3), 235–241. doi:10.1002/humu.22932
Mangravite, L. M., Thorn, C. F., and Krauss, R. M. (2006). Clinical Implications of Pharmacogenomics of Statin Treatment. Pharmacogenomics J. 6 (6), 360–374. doi:10.1038/sj.tpj.6500384
Martín-Campos, J. M., Julve, J., Roig, R., Martínez, S., Errico, T. L., Martínez-Couselo, S., et al. (2014). Molecular Analysis of Chylomicronemia in a Clinical Laboratory Setting: Diagnosis of 13 Cases of Lipoprotein Lipase Deficiency. Clinica Chim. Acta 429, 61–68. doi:10.1016/j.cca.2013.11.025
Maxwell, W. D., Ramsey, L. B., Johnson, S. G., Moore, K. G., Shtutman, M., Schoonover, J. H., et al. (2017). Impact of Pharmacogenetics on Efficacy and Safety of Statin Therapy for Dyslipidemia. Pharmacotherapy 37 (9), 1172–1190. doi:10.1002/phar.1981
McKenna, A., Hanna, M., Banks, E., Sivachenko, A., Cibulskis, K., Kernytsky, A., et al. (2010). The Genome Analysis Toolkit: a MapReduce Framework for Analyzing Next-Generation DNA Sequencing Data. Genome Res. 20 (9), 1297–1303. doi:10.1101/gr.107524.110
McLaren, W., Gil, L., Hunt, S. E., Riat, H. S., Ritchie, G. R. S., Thormann, A., et al. (2016). The Ensembl Variant Effect Predictor. Genome Biol. 17 (1), 122. doi:10.1186/s13059-016-0974-4
Niemi, M. (2010). Transporter Pharmacogenetics and Statin Toxicity. Clin. Pharmacol. Ther. 87 (1), 130–133. doi:10.1038/clpt.2009.197
Pullinger, C. R., Eng, C., Salen, G., Shefer, S., Batta, A. K., Erickson, S. K., et al. (2002). Human Cholesterol 7α-Hydroxylase (CYP7A1) Deficiency Has a Hypercholesterolemic Phenotype. J. Clin. Invest. 110 (1), 109–117. doi:10.1172/JCI1538710.1172/jci0215387
Purcell, S., Neale, B., Todd-Brown, K., Thomas, L., Ferreira, M. A. R., Bender, D., et al. (2007). PLINK: a Tool Set for Whole-Genome Association and Population-Based Linkage Analyses. Am. J. Hum. Genet. 81 (3), 559–575. doi:10.1086/519795
Ramsey, L. B., Johnson, S. G., Caudle, K. E., Haidar, C. E., Voora, D., Wilke, R. A., et al. (2014). The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1 and Simvastatin-Induced Myopathy: 2014 Update. Clin. Pharmacol. Ther. 96 (4), 423–428. doi:10.1038/clpt.2014.125
Tomlinson, B., Hu, M., Lee, V. W. Y., Lui, S. S. H., Chu, T. T. W., Poon, E. W. M., et al. (2010). ABCG2 Polymorphism Is Associated with the Low-Density Lipoprotein Cholesterol Response to Rosuvastatin. Clin. Pharmacol. Ther. 87 (5), 558–562. doi:10.1038/clpt.2009.232
Wang, J., Ban, M. R., Kennedy, B. A., Anand, S., Yusuf, S., Huff, M. W., et al. (2008). APOA5 Genetic Variants Are Markers for Classic Hyperlipoproteinemia Phenotypes and Hypertriglyceridemia. Nat. Rev. Cardiol. 5 (11), 730–737. doi:10.1038/ncpcardio1326
Wang, D., Guo, Y., Wrighton, S. A., Cooke, G. E., and Sadee, W. (2011). Intronic Polymorphism in CYP3A4 Affects Hepatic Expression and Response to Statin Drugs. Pharmacogenomics J. 11 (4), 274–286. doi:10.1038/tpj.2010.28
Woo, H. I., Kim, S. R., Huh, W., Ko, J.-W., and Lee, S.-Y. (2017). Association of Genetic Variations with Pharmacokinetics and Lipid-Lowering Response to Atorvastatin in Healthy Korean Subjects. Dddt 11, 1135–1146. doi:10.2147/DDDT.S131487
Keywords: atorvastatin, pharmacokinetic parameter, pharmacogenetics, next-generation sequencing, liquid chromatography-tandem mass spectrometry
Citation: Kim S, Seo JD, Yun Y-M, Kim H, Kim T-E, Lee T, Lee T-R, Lee JH, Cho E-H and Ki C-S (2022) Pharmacokinetics and Genetic Factors of Atorvastatin in Healthy Korean Subjects. Front. Genet. 13:836970. doi: 10.3389/fgene.2022.836970
Received: 16 December 2021; Accepted: 13 April 2022;
Published: 19 May 2022.
Edited by:
Ryosuke Nakamura, National Institute of Health Sciences (NIHS), JapanReviewed by:
Ingrid Fricke-Galindo, Instituto Nacional de Enfermedades Respiratorias-México (INER), MexicoCopyright © 2022 Kim, Seo, Yun, Kim, Kim, Lee, Lee, Lee, Cho and Ki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yeo-Min Yun, eW15dW5Aa3VoLmFjLmty
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.