
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Genet., 12 January 2023
Sec. Genetics of Common and Rare Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fgene.2022.1052179
This article is part of the Research TopicBuilding Capacity for Sickle Cell Disease Research and HealthcareView all 16 articles
 Vivian Paintsil1,2*
Vivian Paintsil1,2* Mwashungi Ally3
Mwashungi Ally3 Hezekiah Isa4
Hezekiah Isa4 Kofi A. Anie5
Kofi A. Anie5 Josephine Mgaya3
Josephine Mgaya3 Malula Nkanyemka3
Malula Nkanyemka3 Victoria Nembaware6
Victoria Nembaware6 Yaa Gyamfua Oppong-Mensah2Flora Ndobho3Lulu Chirande3Abel Makubi3
Yaa Gyamfua Oppong-Mensah2Flora Ndobho3Lulu Chirande3Abel Makubi3 Obiageli Nnodu4
Obiageli Nnodu4 Ambroise Wonkam6
Ambroise Wonkam6 Julie Makani3
Julie Makani3 Kwaku Ohene-Frempong7
Kwaku Ohene-Frempong7Introduction: Sickle Cell Disease (SCD) causes significant morbidity and mortality particularly in sub-Saharan Africa (SSA) where it contributes to early childhood deaths. There is need to standardize treatment guidelines to help improve overall SCD patient health outcomes. We set out to review existing guidelines on SCD and to set minimum standards for management of SCD for the different referral levels of healthcare.
Methods: A standards of care working group (SoC-WG) was established to develop the SoC recommendations. About 15 available SCD management guidelines and protocols were reviewed and themes extracted from them. The first draft was on chosen themes with 64 major headings and subtopics. Using a summarised WHO levels of referral document, we were able to get six different referral levels of healthcare. The highest referral level was the tertiary facilities whilst the lowest level was the home setting. Recommendations for SCD management for the regional, district, sub-districts, health posts and CHPs compounds were also drafted.
Results: The results from this review yielded a guidelines document which had recommendations for management of SCD on 64 topics and subtopic for all the six (6) different referral levels.
Discussions: Every child with SCD need to receive comprehensive care that is coordinated at each level. This recommendation is unique in terms of the availability of recommendations for different levels of care as compared to the traditional guidelines which is more focused at the tertiary levels. Patients can access care at any of the other lower referral hospitals and be managed with recommendations that are in keeping with institutional resources at that level. When such patients need care that requires expertise that is not available at that level, the recommendations will be to refer to the appropriate referral level where those expertise are available. This encourages patients to have good clinical care nearer their homes but also having access to specialist screening modalities and expertise at the tertiary hospitals if need be. With this, patient are not limited to a specific referral level when interventions cannot be instituted for them.
Conclusion: This SoC recommendations document is a useful material that can be used for consistent standards of treatment in SSA.
Sickle Cell Disease (SCD) is a group of inherited red blood cell disorders characterized by presence of abnormal haemoglobin resulting in formation of hard and sticky C-shaped red cells (CDC, 2022). This is caused by a single base-pair point mutation in the 6th position of the beta globin chain leading to substitution of the amino acid glutamic acid to valine (GAG to GTG) (Genetic Mutation, 2022). The most common types of SCD are SCD-SS, SCD-SC and SCD-S beta thalassemia. SCD causes significant morbidity and mortality particularly in SSA. SCD is one of the leading causes of hospitalization and mortality in under-fives in Africa. The clinical manifestation of SCD are varied and due to the short life span of sickled red blood cells and their tendency to get stuck in the blood vessels and impair the blood flow. Symptoms and signs include anaemia, pain episodes, infections, stroke, and other symptoms depending on the organ involved.
Over 300,000 babies are born annually worldwide with SCD and most of them are found in low and middle income countries (LMICs). About 75% or more of these births are in Sub-Saharan Africa (SSA) (Piel et al., 2013). SCD contributes to the high health burden in SSA and to early childhood deaths if no interventions are put in place. If existing evidence-based cost-effective interventions were implemented in SSA, they could prevent about 70% of these childhood deaths. Therefore, there is need to implement strategies and treatment guidelines to help improve overall SCD patient health outcomes through standardization of quality care. A commonly used approach is the use of “Standard of Care” guidelines for healthcare professionals.
In September 2015, the National Heart, Lung and Blood Institute (NHLBI) of the National Institute of Health (NIH) of the United States of America issued a Request for Application (RFA-HL-17-006) for establishment of a “Sickle Cell Disease in Sub-Saharan Africa: Collaborative Consortium”. A multinational collaboration among Muhimbili University of Health and Allied Sciences (MUHAS), Dar es Salaam, Tanzania as hub and three sites; MUHAS, Dar es Salaam, Tanzania, University of Abuja, Abuja, Nigeria and The Kwame Nkrumah University of Science and Technology, Kumasi, Ghana applied for and was awarded the grant (U24HL135881) (Yoshizawa et al., 2019).
Sickle Pan Africa Research Consortium (SPARCo) was established with a vision to transform the health of individuals with SCD in SSA through the establishment of a robust and portable framework for research and healthcare. Its first goal was to reduce morbidity and mortality in SCD in Africa through implementation research that will demonstrate the feasibility of introducing newborn screening (NBS) and providing comprehensive care to prevent, identify, treat and manage acute and chronic complications. Specific aim two of the proposal was to develop, implement and evaluate a resource-based, multi-level “Guidelines for Management of SCD in SSA”. The specific objectives were as follows;
1. To review existing guidelines on SCD
2. To set minimum standards for management of SCD based on institutional and human resources
3. To field test the compiled SoC guidelines in the various countries (Makani et al., 2020).
The term “standard of care” (SoC) refers to the reasonable degree of care a person should provide to another person, typically in a professional or medical setting (Standard of Care, 2022). Medically, it refers to treatment guidelines that are accepted in the medical community as the most appropriate for the treatment of a certain disease or condition (NCI, 2011). SoC provide clinical practice guidelines which outline formal diagnostic and treatment processes that a doctor will follow in management of a patient with a specific illness. SoC are commonly developed by a medical society or organization working on the specific disease. The use of SoC has been found to improve quality of care for patients and reduce incidences of malpractice (Mccabe et al., 2009).
There are various SCD SoC guidelines worldwide (Heart and Institute, 2014; De Montalembert et al., 2011; Sicklecell Society, 2018; Wilson, 2019; MEDBOX, 2022). However, the majority of the existing guidelines are one level guidelines, developed to be used in tertiary level healthcare facilities where resources and expertise are available (Alli et al., 2014; Heart and Institute, 2014; Sicklecell Society, 2018). This is not feasible in many African settings where there are limited tertiary level healthcare facilities (see Table 1 for descriptions of classification of the different levels of healthcare facilities). Furthermore, some tertiary level healthcare facilities in Africa are not well-resourced, which results in some well-established SCD centres having to adapt existing SCD SoC based on the availability of resources. Given that anecdotal data shows that majority of patients are seen and managed at the lower level healthcare facilities before being referred to tertiary hospitals, the use of the tertiary level guidelines by the lower level healthcare facilities would be inappropriate. Although there are efforts to develop guidelines at the institutional and national levels, we decided to develop multiple recommendations for SoC guidelines to match the availability of facilities and expertise for different levels of healthcare facilities in SSA (Table 1).
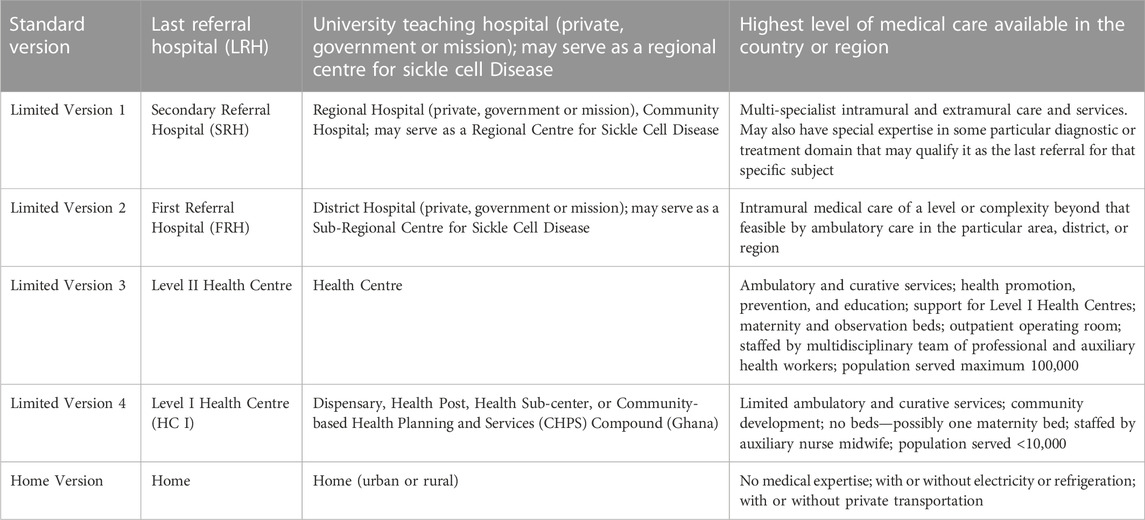
TABLE 1. Summary of WHO classification of healthcare facility levels.
The Sickle Cell Foundation of Ghana in 2012 were the first to develop SCD guidelines for each of the different referral levels of healthcare for Ghana. The current work adopted this multi-referral level guideline development. The Ghana guidelines recognises the disparities in the availability of resources at the different levels of healthcare facilities and incorporates it into the guidelines. These levels of healthcare was adopted from the WHO document on the levels of referral. This WHO document has five referral levels for healthcare facilities depending on resources available. The highest level of medical care available in the country comprise the tertiary level and mostly a University or teaching hospital. There was the inclusion of a 6th referral level which is the home SCD management guidelines targeted at the patient or their parents. The highest referral level is the tertiary level health facility. There are recommendations for the regional level facilities, district level facilities, health centres, health posts/dispensaries/Community-based health planning and services (CHPs) compound which is unique to Ghana and finally the home level recommendations. The highest level guideline is also denoted as the “Standard Version” for the tertiary healthcare facilities. This standard version is then also scaled down for the other lower-level health facilities. These are also denoted as limited Version 1 for the Regional hospitals, Limited Version 2 for the district hospitals, limited version 3 for the health centres and limited version 4 for the dispensary, health post or CHPs compounds. The Sickle Cell Foundation of Ghana has a unique guideline, the home management guideline as the last level.
The Sickle Pan Africa Research Consortium (SPARCO) adopted the SoC guidelines design approach developed by the Sickle Cell Foundation of Ghana. This design is especially suitable for developing countries where healthcare infrastructure and human resources are largely low with patients being managed with restricted resources. It is our expectation that the SPARCO SCD SoC recommendations will guide all cadres of healthcare providers at all the different referral levels of healthcare, therefore improving the quality of care given to individuals with SCD.
A standards of care working group (SoC-WG) was established to develop the SoC recommendations for use in the various referral levels of healthcare. The SoC-WG comprised of seven members who were elected from all the three sites (Ghana, Nigeria and Tanzania) in the Sickle Pan Africa Research Consortium (SPARCo). Each of the sites nominated two (2) doctors with a background in haematology to be part of the team. One member of the group who was a clinical psychologist, although not part of SPARCO, was co-opted to help with the section on psychosocial support for Sickle Cell Disease (SCD) patients as he had lots of experience with it. The chairperson of the working group was a Professor of Haematology with experience in guidelines development and the other members of the group were people who had helped with guidelines at their national levels.
A detailed work plan (Table 2) was developed according to the grant proposal and members worked according to the fixed timelines. To achieve our goals, assignments were initially discussed and distributed to members. Monthly online meetings were held and communications via email and WhatsApp were conducted to keep track of the work. In-person working meetings were also held during the consortium’s bi-annual meetings.
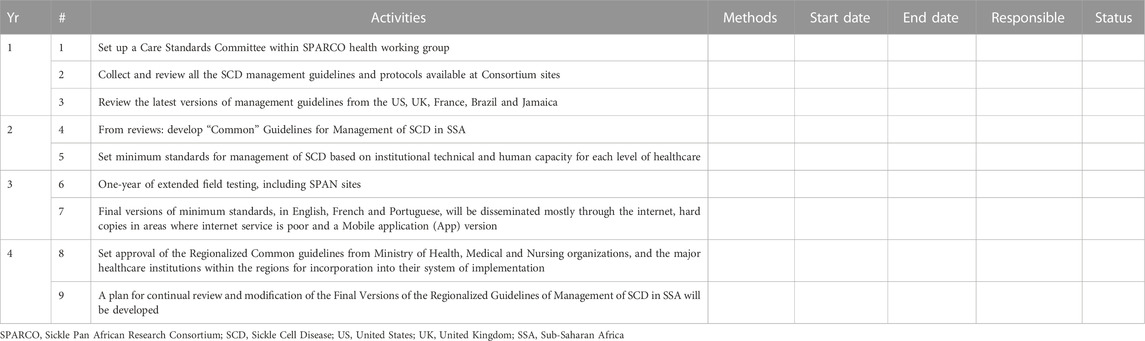
TABLE 2. SPARCO standards of care working group: Detailed work plan.
A database detailing the elements of the SoC recommendations with the activities to be conducted was developed by the members of the working group. These elements were agreed upon by consensus after appraisal of the literature available. This database for the review process included the contact information for members of the SoC WG, the workplan and activity tracker for the working group members. Metrics to analyse and compare guidelines were also developed. The first task was to review all the available SCD management guidelines and protocols.
Before the review process, several stakeholders in and outside Africa were contacted for a copy of their SCD management guidelines. The SoC WG members reviewed 15 guidelines from US, UK, France, Brazil and Jamaica and from the three sites in SPARCo and SADaCC. These guidelines were grouped into African (Alli et al., 2014; MEDBOX, 2022) and non-African guidelines (Sickle Cell Unit, 1997; Ali Susanna, 2008; Sicklecell Society, 2010; De Montalembert et al., 2011; NICE, 2012; CanHaem, 2014; Heart and Institute, 2014; Colombatti and Sainati, 2016; Sicklecell Society, 2018; Sirigaddi et al., 2018; Liem et al., 2019; Wilson, 2019). These guidelines were mostly national guidelines for the tertiary level healthcare (Table 3).
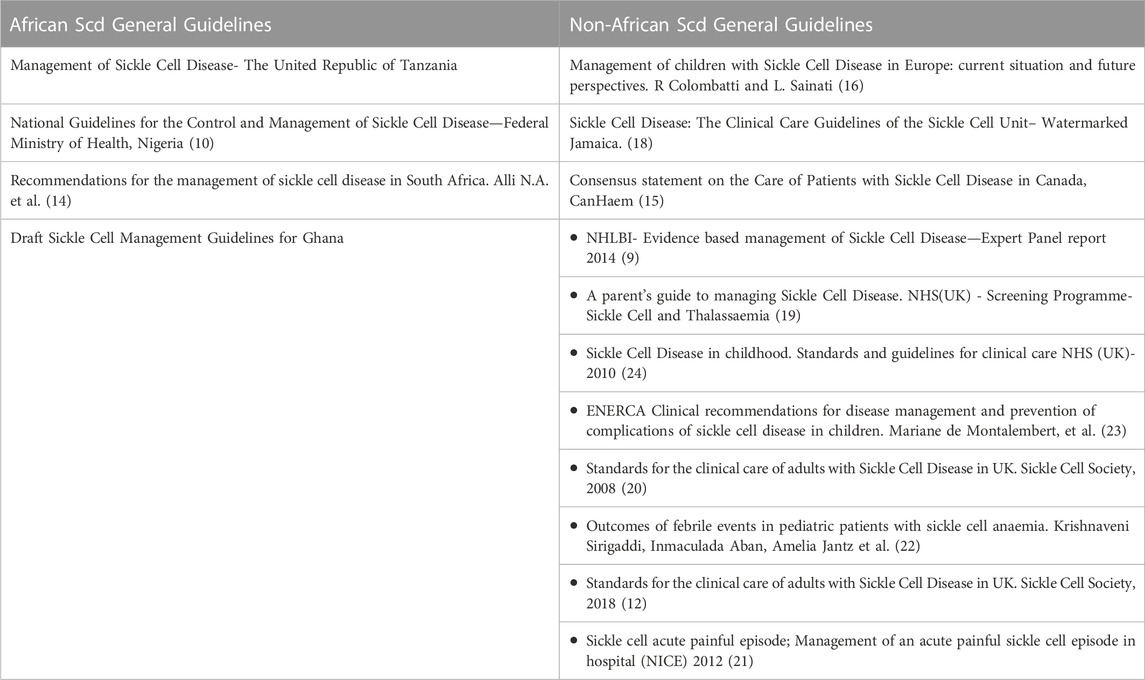
TABLE 3. Existing guidelines reviewed by the SoC working group.
The working group members were assigned sets of guidelines from the different countries other than their own country to review. They were assigned the guidelines based on their specialties and area of interests making sure that assignments were evenly distributed. From this review, sets of themes which were common in all the guidelines were documented and other themes which were deemed important but not common in all the guidelines were also extracted and agreed upon by the group. These themes were compiled into a single document and afterwards, an in-depth review was undertaken from which the detailed guidelines were written.
The themes that were chosen were grouped into the following major headings (Table 4): Diagnosis of sickle cell disease and related conditions, Health maintenance and preventive therapy, Screening for specific complications of SCD, management of acute complications of SCD, management of chronic complications of SCD and special management protocols e.g., hydration guide, analgesic therapy and their use in SCD and hydroxyurea therapy. Under these major headings were other sub topics for consideration. These sections made up 64 topics and subtopics.
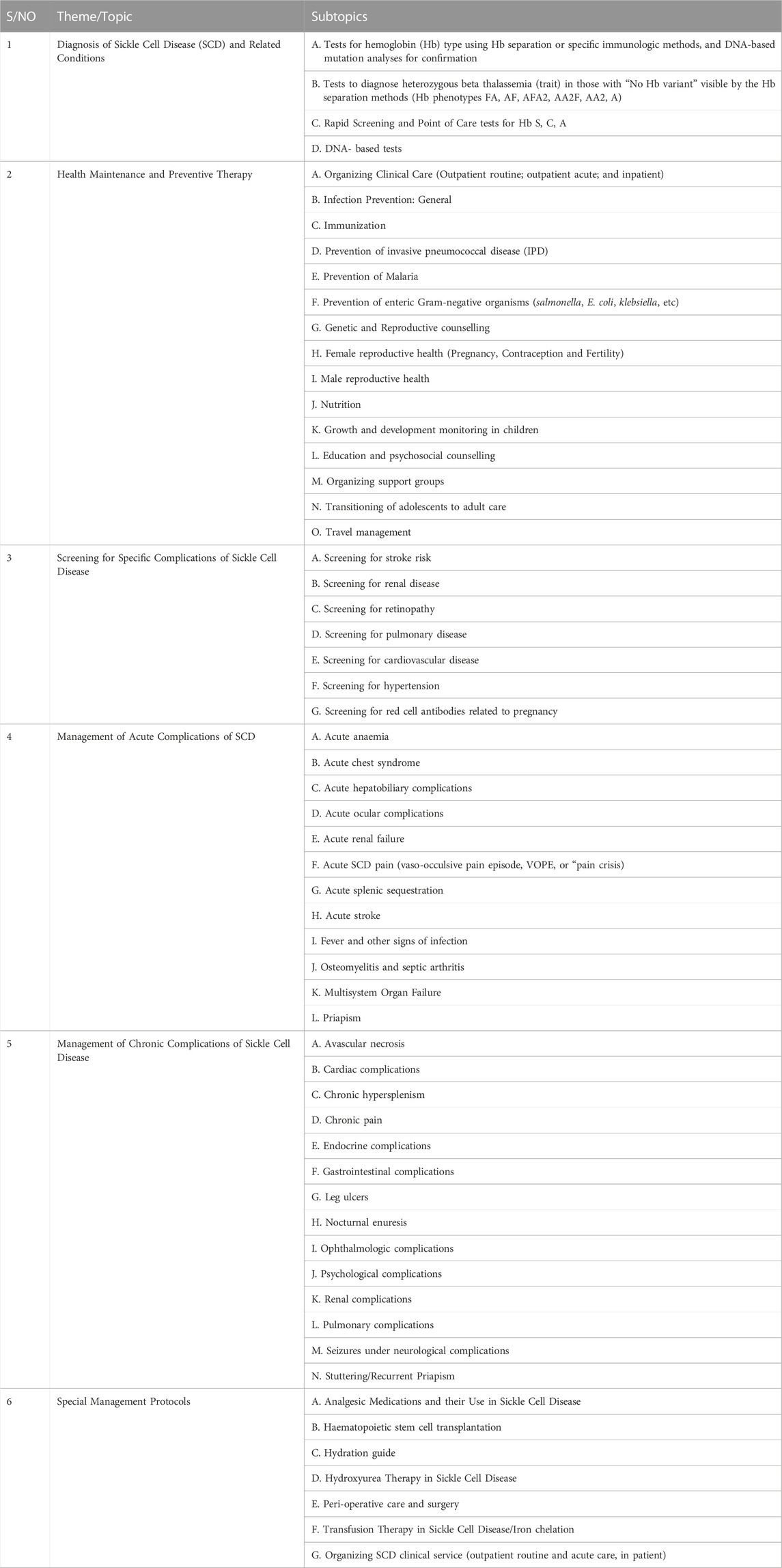
TABLE 4. Major themes/topics and subtopics identified.
Specific subtopics were then assigned to working group members to review the different guidelines and adapt them to suit our population. There was the need to develop the guidelines to also suit lower referral health facilities that also manage SCD patients. The working group adopted a classification of healthcare facilities based on the summarised WHO classification to get five referral health facility levels for the recommendations (Table 1).
Based on the review of the existing guidelines, the SPARCo WG developed guidelines for the management of SCD in SSA and set minimum standards for management of SCD aligned to institutional technical and human resources for each level of healthcare facility (see levels summarized in Table 1). In developing common guidelines for management of SCD in sub-Saharan Africa, the group successfully developed the first draft of the tertiary facility guidelines for management of SCD and the guidelines developed included all the thematic areas. The first drafts of the tertiary facility level guidelines also referred to as the standard version of the guidelines were internally reviewed by members of the group, and then by the consortium members before being sent out for external review. In developing the guidelines for all the other lower referral levels ie regional, district, health centres, health posts/dispensaries/CHPs level and home level, the same processes were taken but other members of the consortium from Ghana, Tanzania and Nigeria were co-opted into the working group to complete this final aspect of the work and the multi referral level SCD guidelines were compiled. They were reviewed by our senior haematologists in the group before being submitted for internal review by SPARCO hub to other consortium members and subsequently for external review. The processes for the review of the guidelines and drafting of the recommendations are represented in Figure 1.
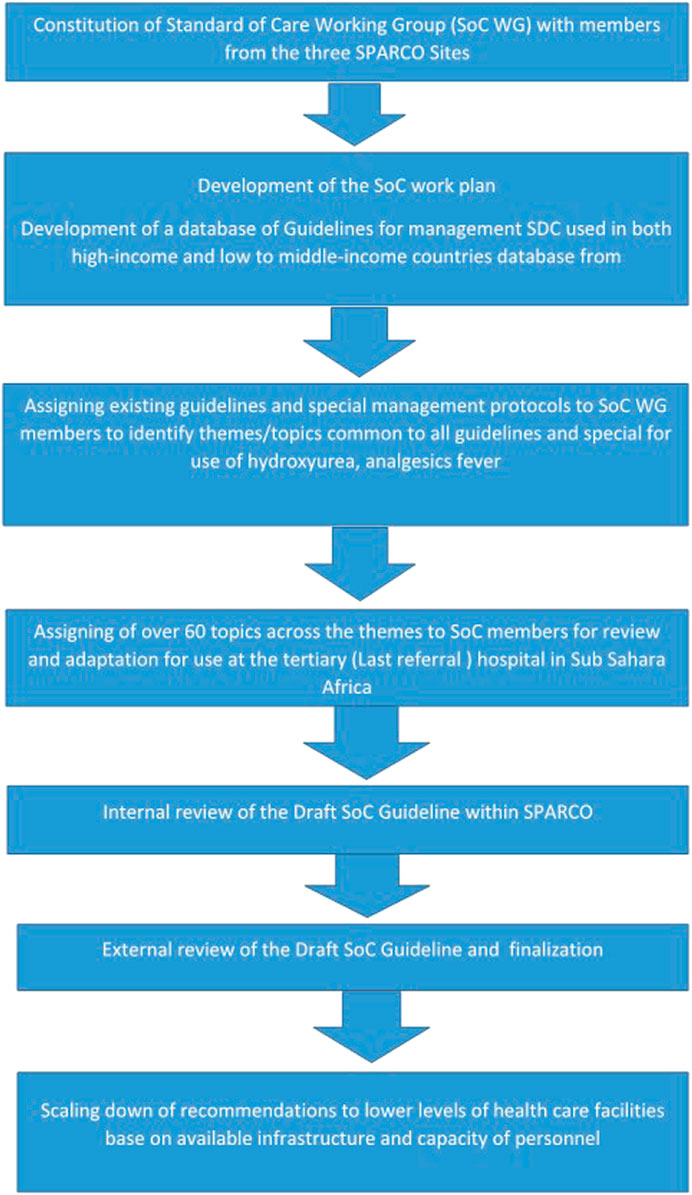
FIGURE 1. Graphical presentation of the process of development of the standard of care guidelines.
The results from this review yielded a guidelines document which had recommendations for management of SCD based on the institutional and human capacity. We developed recommendations for five different levels of healthcare and a sixth level being what has to be done in the home before patients were taken to the hospital. A total of 64 topics had recommendations written out for them (Table 4). The major themes and topics that had recommendations are as seen in Table 4. The recommendations showed what management guidelines could be instituted at each referral level with the option of referring a patient to another referral level health facility for specialist expertise. The home level guidelines focussed on what action was needed in the event of any complication at home and when the patient needed to go for screening for complications of SCD.
Tables 5, 6 are two examples out of the 64 guidelines written. These two illustrate the different recommendations for the screening of stroke and retinopathy in different levels of healthcare facilities and also in the house.
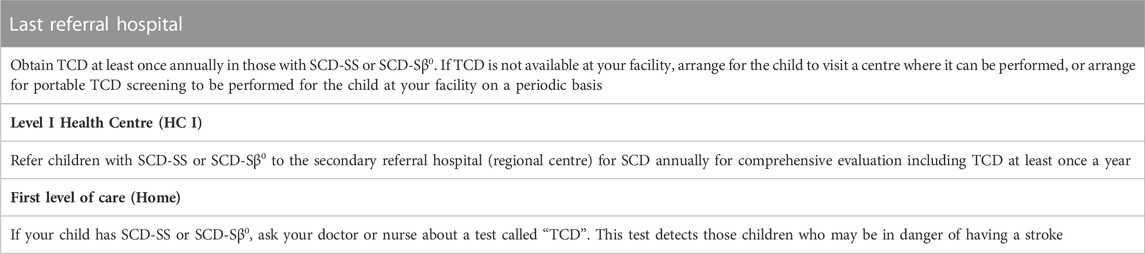
TABLE 5. Screening for stroke risk. Transcranial Doppler ultrasonography (TCD) for children at different levels of healthcare facilities.
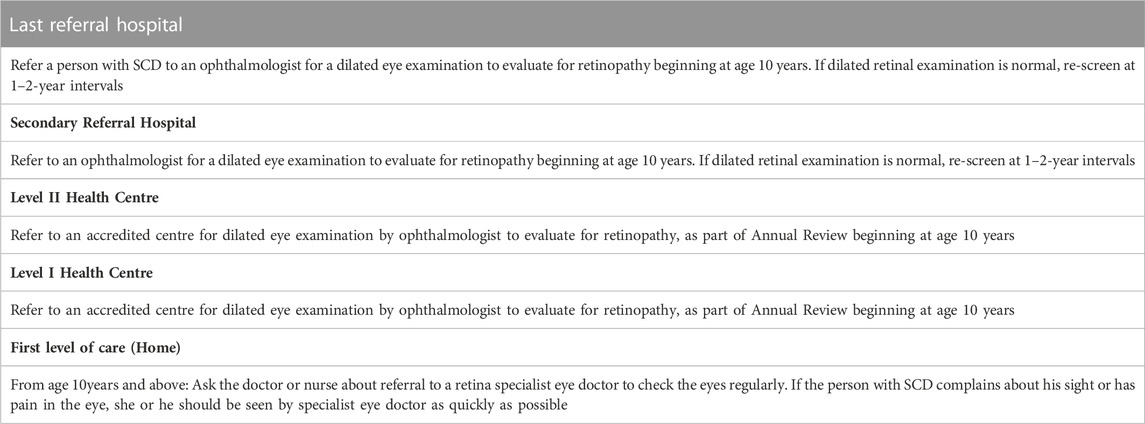
TABLE 6. Screening for retinopathy SCD disease patients for different healthcare levels.
Each of the recommendations were different for the different levels of healthcare for screening of stroke (Table 5). For home-based care, the caregiver was advised to ask about the TranscranialDoppler (TCD) ultrasound screening test so that it could be written out for them by the healthcare practitioner. At the level 1 facility which is the Health posts or CHPs compound and Level 11 referral centre which is the health centre, healthcare workers (HCW) are required to refer to the tertiary centre or regional centres where TCD facilities are commonly available. The last referral hospital which are tertiary facilities mostly have TCD facilities available and can perform TCD for children 2–16 years annually.
In Table 6, the primary physician/haematologist are prompted to let the ophthalmologist do a fundoscopy for patients from age 10 at the tertiary level. In the regional hospitals where ophthalmologists are available, patients can be referred to them at the regional facility or to the tertiary hospitals for fundoscopy. Healthcare facilities at lower referral levels are recommended to refer to either the regional or tertiary facilities whilst the home guidelines will alert the parent or patient to ask about the ophthalmology review.
It is essential that every patient with SCD receives comprehensive care that is coordinated at each level by medical experts. The availability of treatment guidelines normally leads to a harmonised way of treating patients. The existing guidelines are commonly developed for the last referral levels or tertiary facility making adaption for use by the primary healthcare very difficult. This can lead to misuse of these available guidelines. The compilation of this document brought to the forefront a harmonised way of treatment of SCD in SSA based on our resources and constraints. The lowest level of comprehensive care for patients with sickle cell disease is available at the healthposts/dispenasaries/CHPs compounds which are mainly manned by nurses and with available recommendations, they will know what can be done at their end and when to refer.
Patients can access care at any of the other lower referral healthcare facilities and be managed with recommendations that are in keeping with institutional resources at that level. When such patients need care that requires expertise that is not available at that level, the recommendations will be to refer to the appropriate referral level where those expertise are available (mainly a higher referral level facility like the regional or tertiary facility). This encourages patients to have good clinical care nearer their homes but also having access to specialist screening modalities and expertise at the tertiary hospitals if need be. With this, patients are not limited to a specific referral level when interventions cannot be instituted for them at that level of healthcare.
One of the lessons learnt during this process was the benefits of task sharing and teamwork. The SoC WG worked as a team with every member carrying out his or her writing assignment dutifully. Another benefit derived from the exercise was the mentorship from the SoC WG Chair, Professor Kwaku Ohene-Frempong to the younger members of the team. It is also noteworthy that with little or no financial resources the SoC WG was able to put together this valuable SoC document which if implemented has potential to improve the care and management of SCD in sub-Saharan Africa.
It is unique in terms of the availability of recommendations for different levels of care as compared to the traditional guidelines which is more focussed at the tertiary levels. With the traditional guidelines, those in the primary healthcare settings find it difficult adapting it for their use.
Time constraint was a challenge for both writers and reviewers as most members are very busy in other equally important duties such as clinical work and teaching at their respective institutions thus often missing timelines and delaying the process though not compromising the quality of work.
This SoC recommendations for SCD is a useful material that can be used for consistent standards of treatment in SSA. We will need to create awareness and advocate for adoption and use among governments and stakeholders such as Paediatricians and Haematologists as well as other specialties involved in managing the complications of SCD.
We recommend the training of stakeholders across medical disciplines, professions and cadres on the use of the guideline and possibly incorporating it in the training curricular of nursing schools, community health workers’ schools and other allied health workers. We will also recommend the distribution of both online/mobile App and both full and short (pocket) versions of the SoC recommendations for SCD and adapted in a local context for implementation in all SSA countries.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
VP, MA, and HI conceived the idea and wrote the first draft. VP, MA, HI, KA, JM, MN, VN, YO-M, FN, LC, AM, ON, AW, JM, and KO-F wrote the guidelines, contributed sections and critically reviewed the manuscript. All the authors approved the submission.
This work was received from the United States (United States) National Heart, Lung and Blood Institute (NHLBI) (Grant numbers U24HL135881 the Sickle Pan African Research Consortium (04/01/2017–03/31/2021) and U24HL135600 and Sickle Data Coordinating Center, (04/01/2017–03/31/2021).
Lucio Luzzatto: SPARCo Scientific adviser and for your review and comments. We sincerely thank the external reviewer Baba Inusa for creating time out of his busy schedule to review the recommendations and provide valuable insights.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ali Susanna, B. (2008). Sickle cell disease: The clinical care guidelines of the sickle cell unit TMRI UWI Jamaica. Kingston, Jamaica: Sickle Cell Unit, 128.
Alli, N. A., Patel, M., Alli, H. D., Bassa, F., Coetzee, M. J., Davidson, A., et al. (2014). Recommendations for the management of sickle cell disease in South Africa. Afr. Med. J. 104 (11), 743–751. doi:10.7196/samj.8470
CanHaem (2014). Consensus statement on the care of patients with siCkle cell disease in Canada artwork entitled “tree of life” by deon best. Ottawa: Canadian Haemoglobinopathy Association.
CDC 2022 What is sickle cell disease? Available from: https://www.cdc.gov/ncbddd/sicklecell/facts.html (accesed Mar 28, 2022)
Colombatti, R., and Sainati, L. (2016). Management of children with sickle cell disease in europe: Current situation and future perspectives. EMJ Hematol. 4, 129–135. doi:10.33590/emjhematol/10310534
De Montalembert, M., Ferster, A., Colombatti, R., Rees, D. C., and Gulbis, B. (2011). ENERCA clinical recommendations for disease management and prevention of complications of sickle cell disease in children. Am. J. Hematol. 86 (1), 72–75. doi:10.1002/ajh.21865
Genetic Mutation (2022). Genetic mutation | learn science at scitable. Available from: https://www.nature.com/scitable/topicpage/genetic-mutation-441/(accesed Mar 28, 2022).
Heart, N., and Institute, B. (2014). Evidence-based management of sickle cell disease. Bethesda: National Heart, Lung, and Blood Institute. Accessed from: http://www.nhlbi.nih.gov.
Liem, R. I., Lanzkron, S., Coates, T. D., DeCastro, L., Desai, A. A., Ataga, K. I., et al. (2019). American Society of Hematology 2019 guidelines for sickle cell disease: Cardiopulmonary and kidney disease. Blood Adv. 3 (23), 3867–3897. doi:10.1182/bloodadvances.2019000916
Makani, J., Sangeda, R. Z., Nnodu, O., Nembaware, V., Osei-Akoto, A., Paintsil, V., et al. (2020). Sick. Lancet Haematol. 7 (2), e98–e99. doi:10.1016/S2352-3026(20)30006-5
Mccabe, C., Kirchner, C., Zhang, H., Daley, J., and Fisman, D. N. (2009). Guideline-concordant therapy and reduced mortality and length of stay in adults with community-acquired pneumonia playing by the rules. Arch. Intern Med. 169 (16), 1525–1531. doi:10.1001/archinternmed.2009.259
MEDBOX (2022). Nigeria: National guideline for the control and management of sickle. Available from: https://www.medbox.org/document/nigeria-national-guideline-for-the-control-and-management-of-sickle-cell-disease#GO (accesed Aug 17, 2022).
NCI (2011). Definition of standard medical care - NCI dictionary of cancer terms - NCI. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/standard-medical-care (accesed Nov 24, 2022).
NICE (2012). Sickle cell acute painful episode Management of an acute painful sickle cell episode in hospital. London, United Kingdom: NICE.
Piel, F. B., Hay, S. I., Gupta, S., Weatherall, D. J., and Williams, T. N. (2013). Global burden of sickle cell anaemia in children under five, 2010–2050: Modelling based on demographics, excess mortality, and interventions. PLoS Med. 10 (7), e1001484. doi:10.1371/journal.pmed.1001484
Sickle Cell Unit (1997). A parent’s guide to managing sickle cell disease. Kingston, Jamaica: Sickle Cell Unit.
Sicklecell Society (2010). Screening programmes sickle cell disease in childhood standards and guidelines for clinical care. United Kingdom: SicklecellSociety.
Sicklecell Society (2018). Standards for clinical care of adults with sickle cell disease in the UK-2018. United Kingdom: Sicklecell Society.
Sirigaddi, K., Aban, I., Jantz, A., Pernell, B. M., Hilliard, L. M., Bhatia, S., et al. (2018). Outcomes of febrile events in pediatric patients with sickle cell anemia. Pediatr. Blood Cancer 65 (11), e27379. doi:10.1002/pbc.27379
Standard of Care (2022). Standard of care - definition, examples, cases, processes. Available from: https://legaldictionary.net/standard-of-care/(accesed Mar 27, 2022).
Wilson, J. (2019). Sickle cell disease in childhood: Standards and recommendations for clinical care. United Kingdom: Sicklecell Society.
Keywords: standards of care, Sickle Cell Disease, SickleInAfrica, Sickle Pan African Research Consortium (SPARCO), Sub-Saharan Africa
Citation: Paintsil V, Ally M, Isa H, Anie KA, Mgaya J, Nkanyemka M, Nembaware V, Oppong-Mensah YG, Ndobho F, Chirande L, Makubi A, Nnodu O, Wonkam A, Makani J and Ohene-Frempong K (2023) Development of multi-level standards of care recommendations for sickle cell disease: Experience from SickleInAfrica. Front. Genet. 13:1052179. doi: 10.3389/fgene.2022.1052179
Received: 23 September 2022; Accepted: 29 December 2022;
Published: 12 January 2023.
Edited by:
Sergey S. Shevkoplyas, University of Houston, United StatesReviewed by:
Julie Kanter, University of Alabama at Birmingham, United StatesCopyright © 2023 Paintsil, Ally, Isa, Anie, Mgaya, Nkanyemka, Nembaware, Oppong-Mensah, Ndobho, Chirande, Makubi, Nnodu, Wonkam, Makani and Ohene-Frempong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vivian Paintsil, dml2cGVlQHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.