
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Genet. , 07 January 2016
Sec. Pharmacogenetics and Pharmacogenomics
Volume 6 - 2015 | https://doi.org/10.3389/fgene.2015.00356
 Marelize Swart1
Marelize Swart1 Jonathan Evans1Michelle Skelton1Sandra Castel2
Jonathan Evans1Michelle Skelton1Sandra Castel2 Lubbe Wiesner2
Lubbe Wiesner2 Peter J. Smith2
Peter J. Smith2 Collet Dandara1*
Collet Dandara1*Introduction: Efavirenz (EFV) is a non-nucleoside reverse transcriptase inhibitor prescribed as part of first-line highly active antiretroviral therapy (HAART) in South Africa. Despite administration of fixed doses of EFV, inter-individual variability in plasma concentrations has been reported. Poor treatment outcomes such as development of adverse drug reactions or treatment failure have been linked to EFV plasma concentrations outside the therapeutic range (1–4 μg/mL) in some studies. The drug metabolizing enzyme (DME), CYP2B6, is primarily responsible for EFV metabolism with minor contributions by CYP1A2, CYP2A6, CYP3A4, CYP3A5, and UGT2B7. DME coding genes are also regulated by microRNAs through targeting the 3′-untranslated region. Expanded analysis of 30 single nucleotide polymorphisms (SNPs), including those in the 3′-UTR, was performed to identify pharmacogenetics determinants of EFV plasma concentrations in addition to CYP2B6 c.516G>T and c.983T>C SNPs.
Methods: SNPs in CYP1A2, CYP2B6, UGT2B7, and NR1I2 (PXR) were selected for genotyping among 222 Bantu-speaking South African HIV-infected patients receiving EFV-containing HAART. This study is a continuation of earlier pharmacogenetics studies emphasizing the role of genetic variation in the 3′-UTR of genes which products are either pharmacokinetic or pharmacodynamic targets of EFV.
Results: Despite evaluating thirty SNPs, CYP2B6 c.516G>T and c.983T>C SNPs remain the most prominent predictors of EFV plasma concentration.
Conclusion: We have shown that CYP2B6 c.516G>T and c.983T>C SNPs are the most important predictors of EFV plasma concentration after taking into account all other SNPs, including genetic variation in the 3′-UTR, and variables affecting EFV metabolism.
Efavirenz (EFV) is a non-nucleoside reverse transcriptase inhibitor (NNRTI) used as part of highly active antiretroviral therapy (HAART) in the treatment of human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS). Approximately 70% of the 2.5 million HIV-infected South Africans on HAART as part of first-line antiretroviral therapy (ART) is now given EFV once-daily (600 mg) in the following combination; tenofovir disoproxil fumarate (TDF) + emtricitabine (FTC) or lamivudine (3TC) + EFV (UNAIDS, 2013). EFV has a half-life of 40–55 h and is preferred because of its effective virologic suppression (Raffi et al., 2014). Multiple large randomized controlled trials and cohort studies have shown potent EFV-related viral suppression with many patients having viral RNA levels < 50 copies/mL for up to 6 years of follow-up (Gulick et al., 2006; Cassetti et al., 2007).
Despite its efficacy and virologic potency, EFV exposure has been linked to development of serious central nervous system (CNS) side effects in 20–74% of patients (Fumaz et al., 2002; Hawkins et al., 2005; Abah et al., 2015). The side effects include dizziness, headaches, depression, nightmares, and insomnia (Adkins and Noble, 1998; Marzolini et al., 2001). Abah et al. (2015) reported an incidence rate of 40.5 adverse drug reactions (ADRs) per 1000 person-years on EFV-based treatment among Nigerian HIV/AIDS patients, while up to 74% of HIV/AIDS patients from Uganda reportedly experienced at least one EFV-related neuropsychiatric symptom within 12 weeks of therapy (Mukonzo et al., 2013). Nearly 43% of Zimbabwean HIV/AIDS patients reported CNS toxicity after initiation of EFV-containing HAART (Dhoro et al., 2015). EFV associated symptoms range from mild to moderate in severity and subside progressively within a month after treatment initiation (Moyle, 1999a,b). The severity or persistence of adverse effects can result in EFV discontinuation and has been reported in about 4–50% of patients (Marzolini et al., 2001; Ward and Curtin, 2006; Kenedi and Goforth, 2011; Leutscher et al., 2013). EFV concentrations in plasma have been shown to be predictive of treatment outcomes in certain studies, with low concentrations potentially resulting in treatment failure, while CNS toxicity being observed three-times more frequent among patients with high EFV plasma concentrations (Marzolini et al., 2001; Kenedi and Goforth, 2011; Leutscher et al., 2013). Achieving the correct EFV dosage and plasma concentrations within the suggested therapeutic range of 1–4 μg/mL is, thus, crucial. This observation led to research focusing on identifying genetic causes of slow or fast EFV metabolism and risk factors of CNS toxicity.
EFV is metabolized to 8-hydroxy-EFV (major metabolite) primarily by cytochrome P450 (CYP) 2B6 and to a minor extent by CYP3A. 7-hydroxy-EFV and N-glucuronide-EFV metabolites are formed by CYP2A6 and UDP glucoronosyltransferases (UGT) 2B7, respectively (Ward et al., 2003; Arab-Alameddine et al., 2009; di Iulio et al., 2009). The formation rate of both 8-hydroxy-EFV and N-glucuronide-EFV is variable between human microsomal samples and points to the involvement of genetic variation in genes coding for drug metabolizing enzymes (DMEs) (Ogburn et al., 2010; Bae et al., 2011).
CYP2B6 genetic variants, specifically rs3745274 (c.516G>T) and rs28399499 (c.983T>C), have been investigated in relation to EFV pharmacokinetics. Numerous studies have reported an association between the CYP2B6 c.516T-allele and increased EFV plasma concentrations, reduced clearance, or increased drug exposure (Wyen et al., 2008; Holzinger et al., 2012; Cortes et al., 2013; Swart et al., 2013; Sinxadi et al., 2015). Patients with the CYP2B6 c.516G/T and c.516T/T genotypes are reported to be at risk of EFV plasma concentrations associated with toxicity (Lee et al., 2014). Several recent studies performed in Africa have reported a CYP2B6 c.516T-allele frequency ranging from 0.20 to 0.49 (Haas et al., 2004; Klein et al., 2005; Mehlotra et al., 2006; Penzak et al., 2007; Gross et al., 2008; Nyakutira et al., 2008; Mukonzo et al., 2009; Parathyras et al., 2009; Ciccacci et al., 2010; Gounden et al., 2010; Jamshidi et al., 2010; Ikediobi et al., 2011; Brown et al., 2012; Li et al., 2012; Maimbo et al., 2012; Swart et al., 2012b; Ngaimisi et al., 2013; Sarfo et al., 2014; Colic et al., 2015). These studies also reported an association of the CYP2B6 c.516T-allele with high EFV plasma concentrations (Mukonzo et al., 2014; Naidoo et al., 2014; Sarfo et al., 2014; Bisaso et al., 2015; Colic et al., 2015; Dhoro et al., 2015; Dickinson et al., 2015; Sinxadi et al., 2015). Thus, CYP2B6 c.516G>T genotyping has been suggested to identify poor metabolizers as part of precision medicine (Haas, 2005; Haas et al., 2005; Nolan et al., 2006; Cabrera et al., 2009; Swart et al., 2013). Another CYP2B6 allele, CYP2B6 c.983C is also a predictor of deficient CYP2B6 activity associated with increased EFV plasma concentrations in certain populations (Wyen et al., 2008; Holzinger et al., 2012; Sarfo et al., 2013; Swart et al., 2013).
Focus on the pharmacogenetics of EFV has mostly been on genetic variation in CYP2B6 with recent studies also investigating the role of other genetic variants in CYP1A2, CYP2A6, CYP3A4, CYP3A5, UGT2B7, ATP binding cassette subfamily B member 1 (ABCB1) and nuclear receptors pregnane X receptor (PXR, NR1I2) and constitutive androstane receptor (CAR, NR1I3) in EFV metabolism (Mukonzo et al., 2009; Burhenne et al., 2010; Elens et al., 2010; Wyen et al., 2011; Swart et al., 2012a,c; Cortes et al., 2013; Sarfo et al., 2013; Sukasem et al., 2014; Haas et al., 2014a,b). The weakness with most of the studies has been characterization of each gene in isolation, making it difficult to evaluate the contribution of each variant together with other variants that cause deficient activity. Thus, in this study we assessed the effects of other variants, including 3′-untranslated region (UTR) variation in genes coding for DMEs involved in EFV metabolism, on EFV plasma concentration. Previous studies trying to account for the genetic contribution to inter-individual differences in EFV plasma concentration were only able to explain a portion of the observed variability (Holzinger et al., 2012; Swart et al., 2013). The aim of the current study was to investigate the role of genetic variation in CYP1A2, CYP2B6, UGT2B7, and NR1I2 especially polymorphisms within the 3′-UTR on EFV metabolism.
Bantu-speaking South African HIV/AIDS patients (n = 301) were recruited from Themba Lethu Clinic, Gauteng, South Africa and were receiving EFV-based treatment for at least 6 months. The participants were unrelated adults as explained previously in Swart et al. (2013). A whole blood sample (5 mL) was obtained from each subject and used for plasma preparation (14–18 h after EFV dose) and DNA extraction as described previously by Swart et al. (2013). Ethical and study approval (HREC REF 103/2009 and M080124) was provided by the University of Cape Town Health Sciences Faculty Human Research Ethics Committee, Cape Town, South Africa, and the University of Witwatersrand Human Research Ethics Committee, Gauteng, South Africa. Written informed consent was obtained from all participants and this study was performed in accordance with guidelines of the Helsinki Declaration of 2008.
Earlier studies have mostly investigated the role of exonic and promoter single nucleotide polymorphisms (SNPs) in CYP1A2, CYP2A6, CYP2B6, and CYP3A on EFV plasma concentration (Wyen et al., 2008; Holzinger et al., 2012; Swart et al., 2012a,c, 2013; Cortes et al., 2013; Sarfo et al., 2013; Evans et al., 2015; Sinxadi et al., 2015). This study is a continuation emphasizing the role of genetic variation in the 3′-UTR of genes which products are either pharmacokinetic or pharmacodynamic targets of EFV. Thus, additional SNPs in CYP1A2 [EMBL: ENSG00000140505; Genbank: NC_000015.10, NM_000761], CYP2B6 [EMBL: ENSG00000197408; Genbank: NC_000019.10, NM_000767], UGT2B7 [EMBL: ENSG00000171234; Genbank: NC_000004.12, NM_001074], and NR1I2 [ENSG000000144852; Genbank: NC_000003.12, NM_022002] were selected for genotyping. The SNPs were selected for investigation based on functional significance. SNPs were genotyped using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP), SNaPshot mini-sequencing or cycle sequencing. PCR-RFLP genotyping and SNaPshot mini-sequencing methods were designed and PCR amplification conditions, digestion patterns and internal SNaPshot primer sequences are shown in Supplementary Table S1.
PCR amplification for the 3′-UTR of CYP1A2, CYP2B6, and NR1I2 was performed as described by Swart and Dandara (2014). PCR amplification was followed by digestion using the appropriate restriction endonuclease (Supplementary Table S1) when PCR-RFLP genotyping was used. Direct cycle sequencing of the 3′-end of NR1I2 3′-UTR with the reverse primer (Supplementary Table S1) was also used for further genotyping. The CYP1A2 (c.9-154C>A), CYP2A6 (c.1093G>A), CYP2B6 (c.136A>G, c.485-18C>T, c.516G>T, c.785A>G, c.983T>C), CYP3A4 (c.-392G>A), CYP3A5 (c.219-237G>A, c.624G>A, c.1035_1036insT, c.14T>C), ABCB1 (c.1236T>C, c.193A>G,c.3435T>C, c.2677G>T/A), NR1I2 (c.448+72G>T, c.96-7659C>T, c.912-93G>A), and NR1I3 (c.540C>T, c.239-1089T>C, c.239-99C>T) SNPs were genotyped using either PCR-RFLP or SNaPshot mini-sequencing as described previously by Swart et al. (2012a), Swart et al. (2012b), Swart et al. (2012c), Swart et al. (2013), and Evans et al. (2015).
PCR amplification of UGT2B7 was performed using the following conditions: 3 min at 94°C; 40 cycles of 94°C for 30 s, an annealing temperature of 58°C (PCR fragment including UGT2B7 c.-161T>C, c.372A>G, c.211G>T, and c.673G>A) or 60°C (PCR fragment including UGT2B7 c.733A>G and c.802T>C) for 30 s, 72°C for 2 min; and 10 min at 72°C for final extension (Supplementary Table S1). PCR reactions were carried out using a “T100 Thermal cycler” from Bio-Rad (Bio-Rad Laboratories, Hercules, CA, USA). Each PCR reaction contained the following reagents; 50–100 ng of genomic DNA, 1 X Green GoTaq Reaction Buffer (Promega Corporation, Madison, WI, USA), 0.2 mM of each of the deoxynucleotide triphosphates (dNTPs) (Bioline, London, UK); 1.5 mM MgCl2 (Promega Corporation, Madison, WI, USA); 40 pmol of the forward and reverse primers (Integrated DNA Technologies, Inc., Coralville, IA, USA); and 1 U of GoTaq DNA Polymerase (Promega Corporation, Madison, WI, USA).
For SNaPshot genotyping of four UGT2B7 SNPs, 5 μL of each PCR product was pooled and cleaned-up using 1 U FastAP and 2 U ExonucleaseI (Fermentas Life Sciences, Burlington, Canada). The FastAP and ExonucleaseI reaction was incubated at 37°C for 1 h followed by inactivation of the enzymes at 75°C for 15 min. SNaPshot single base extension was performed on the “GeneAmp® PCR System 2700” (Applied Biosystems, Carlsbad, CA, USA) using the following conditions; 96°C for 10 s, 50°C for 5 s and 60°C for 30 s for 25 cycles. One microliter SNaPshot™ Multiplex Mix (Applied Biosystems, California, USA) and the pooled internal SNaPshot primers (Supplementary Table S1) were used in the SNaPshot reaction (10 μL) (Integrated DNA Technologies, Inc., Coralville, IA, USA). The clean-up reaction was repeated using cycling conditions as mentioned before. An ABI 3130xl Genetic Analyzer (Applied Biosystems, Carlsbad, CA, USA) was used for capillary electrophoresis and GeneMapper© Software version 4.1 (Applied Biosystems, Carlsbad, CA, USA) was used to analyse results.
SHEsis statistical program (Shi and He, 2005; Li et al., 2009) was used for linkage disequilibrium (D' and r2) analysis. Statistical analyses were performed using Graphpad Prism (Version 5, GraphPad Software Inc., San Diego, CA) and STATA (Version 11, StatSoft, USA) statistical programs. Mann Whitney or Kruskal-Wallis (with Dunn's Multiple Comparison) tests were used to assess association between clinical parameters, genotypes for each SNP or haplotypes and median EFV plasma concentration. EFV plasma concentrations were allocated to each of the observed haplotypes (i.e., in the event of homozygosity, the value was counted as two observations). Multivariate logistic regression analysis was performed to identify predictors of EFV plasma concentration by including covariates from the univariate analysis with a p ≤ 0.15, followed by stepwise backward removal. Statistical significance for the univariate analysis was defined as p < 0.05/N (N = number of SNPs or haplotypes in the analysis), while significance for the multivariate analysis was defined as p < 0.05/N (N = number of covariates in the analysis) to correct for multiple testing. Sensitivity, specificity, positive, and negative predictive values were calculated to determine the predictive value of each SNP in predicting EFV plasma concentration above 4 μg/mL.
Variant allele frequencies in the South African population group were compared to frequencies in other world populations obtained from literature. The populations included; Luhya in Webuye (Kenya), Yoruba in Ibadan (Nigeria), Utah residents with Northern, and Western European ancestry, Finnish, British, and Scottish, Iberians (Spain), Toscani (Italy), Han Chinese, Southern Han Chinese, Japanese, Colombians, Mexican ancestry from Los Angeles USA, Puerto Ricans, and Americans of African ancestry in SW USA (1000 Genomes Project and International HapMap Project). Pearson's χ2-test or Fisher's exact test were used to compare the allele frequencies of the South Africans to previously published frequencies in other populations.
The majority (75%) of participants were women of median age 40 years (range: 22–75 years). Only 7% of the patients smoked tobacco and 10% consumed alcohol. EFV plasma concentrations were available for 74% (n = 222∕301) of the patients. Information on clinical parameters including; disease stage, BMI, CD-4 cell count and viral load were available from hospital records and were reported previously by Swart et al. (2012a), Swart et al. (2012c), and Swart et al. (2013). Adherence to ARV therapy was self-reported and four patients reported missing a day of treatment. Non-ARV medication co-administrated with EFV included vitamin B and rifampicin and 38% (n = 113) of HIV/AIDS patients were treated for opportunistic infections.
UGT2B7 c.211G>T, c.673G>A, and c.733A>G SNPs which have been reported in other populations (Guillemette, 2003; Zhang et al., 2008; Tian et al., 2012; Kim et al., 2014), were monomorphic in this South African group. Genotype frequencies for SNPs in the South African HIV/AIDS patients are shown in Table 1. Hardy-Weinberg equilibrium (HWE) was calculated for each SNP and only the genotype frequencies of the UGT2B7 c.372A>G SNP deviated. Linkage disequilibrium (LD) analysis was performed for all SNPs in CYP1A2, CYP2A6, CYP2B6, CYP3A4, CYP3A5, UGT2B7, ABCB1, NR1I2, and NR1I3 (including SNPs genotyped previously, Swart et al., 2012a,c, 2013; Swart and Dandara, 2014; Evans et al., 2015). D′ and r2 (correlation coefficient preferred by the HapMap project) are both measures of linkage disequilibrium, however, these coefficients are not independent of allelic frequencies. Figures 1A–D show LD plots with D′ or r2 for SNP pairs in CYP1A2, CYP2B6, UGT2B7, and NR1I2. Similar to previously reported findings (Mehlotra et al., 2007; Swart et al., 2013; Haas et al., 2014a), the r2 LD coefficient was low for CYP2B6 c.516G>T-c.983T>C SNP pair (r2 = 0.034), whereas D′ was 0.901.
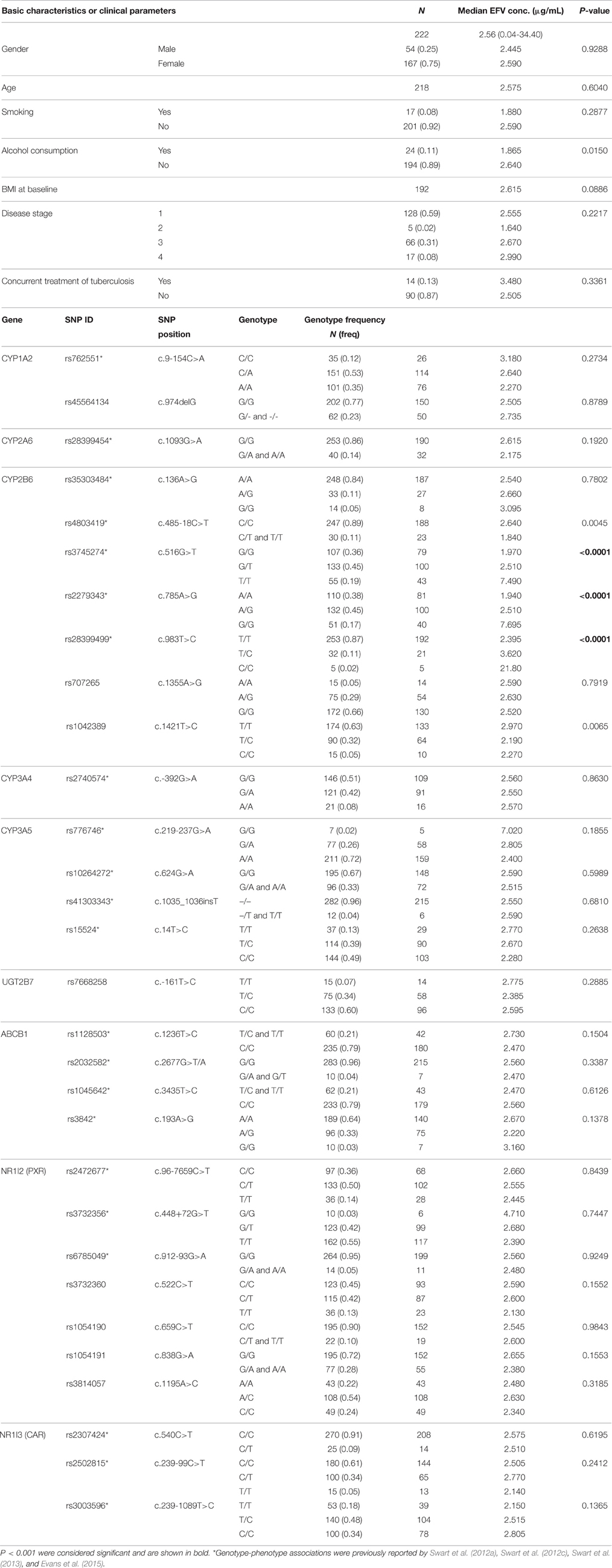
Table 1. Association of basic characteristics, clinical parameters, and genetic variation in CYP1A2, CYP2A6, CYP2B6, CYP3A4, CYP3A5, UGT2B7, ABCB1, NR1I2, and NR1I3 with median efavirenz plasma concentration.
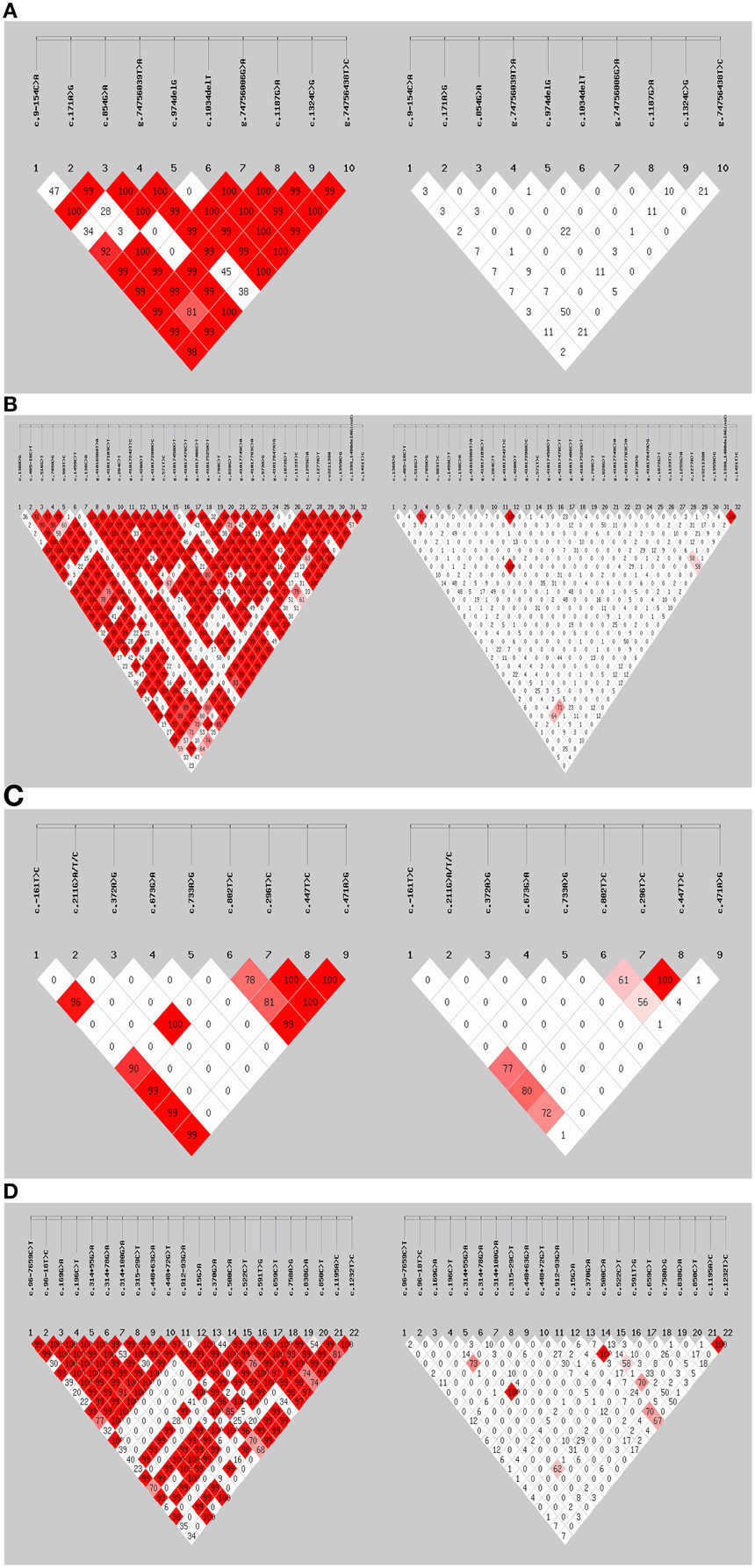
Figure 1. Linkage disequilibrium analysis. (A) CYP1A2, (B) CYP2B6, (C) UGT2B7, and (D) NR1I2. For each, the left figure represents D′-values while the right figure represents r2-values, respectively.
The median EFV plasma concentration was 2.6 μg/mL (range: 0.04–34.4 μg/mL). A large degree of inter-individual variability (860-fold) was observed which has implications for ART response. Three percent (n = 7) of patients had EFV plasma concentrations below therapeutic range (1–4 μg/mL), while 31% (n = 69) of patients presented with EFV plasma concentrations above 4 μg/mL. Gender, age, smoking, body mass index (BMI) at baseline, disease stage, and concurrent treatment of tuberculosis (TB) did not have a significant effect on median EFV plasma concentrations, while a trend towards low EFV plasma concentration was observed for alcohol consumption (p = 0.015; Table 1). The genotypes of each SNP were correlated with EFV plasma concentration and data is presented for SNPs which were successfully genotyped in at least 75% of participants. As expected, high median EFV plasma concentrations were observed among carriers of the following genotypes: CYP2B6 c.516T/T (7.49 μg/mL), CYP2B6 c.785G/G (7.70 μg/mL), and CYP2B6 c.983C/C (21.80 μg/mL; Table 1). A trend towards low EFV plasma concentrations for CYP2B6 c.485-18C/T and T/T genotype carriers (p = 0.0045) and CYP2B6 c.1421T/C and C/C genotype carriers (p = 0.0065) was observed (Table 1).
Haplotypes were inferred for each patient by including SNPs with a variant allele frequency greater than 0.1 for CYP1A2, CYP2B6, and NR1I2 (Supplementary Table S2). No significant differences in median EFV plasma concentrations were observed among haplotypes in CYP1A2, UGT2B7, and NR1I2 (Supplementary Table S2).
Comparison of median EFV plasma concentrations for CYP2B6 haplotypes (c.136A>G-c.516G>T-c.785A>G-c.284C>T-c.571T>C-c.799C>T-c.1072G>T-c.1277A>T-c.1355A>G-c.1399_1400delAGinsCA-c.1421T>C) showed significantly higher EFV plasma concentrations for the CYP2B6 A-T-G-T-(C or T)-C-G-(T or A)-G-AG-T haplotype compared to the A-G-A-T-C-C-G-A-G-AG-T (p < 0.0001) and A-G-A-T-C-C-G-A-G-CA-C (p < 0.0001) haplotypes (Supplementary Table S2). The CYP2B6 A-T-G-T-C-C-(G or T)-A-G-CA-C, A-T-G-T-C-C-G-A-A-AG-(T or C) and G-T-G-C-C-C-G-T-G-AG-T haplotypes presented with EFV plasma concentrations above the recommended therapeutic range (8.55, 5.98, and 9.29 μg/mL). What is common in these haplotypes, is the CYP2B6 c.516T-allele further demonstrating its effect on CYP2B6 activity and, therefore, EFV plasma concentration.
Multivariate logistic regression analysis was performed to determine variables predictive of EFV plasma concentration by evaluating the effect of covariates (Table 2). Variables were prioritized for inclusion in the multivariate analysis based on having p < 0.15 in the univariate analysis. Stepwise removal of variables was performed to assess the effect of each covariate. Multivariate logistic regression analysis showed that CYP2B6 c.516G>T and c.983T>C SNPs were the two most significant predictors of EFV plasma concentration above 4 μg/mL (after correction for multiple testing with p < 0.006). The NR1I2 c.239-1089T>C SNP played a minor role (p = 0.011) in explaining variability in EFV plasma concentrations (Table 2).
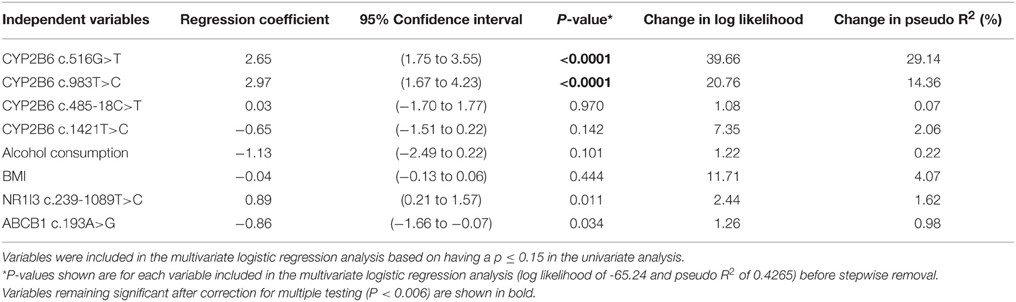
Table 2. Multivariate logistic regression analysis of efavirenz plasma concentrations above or below 4 μg/mL.
Expanding our investigation to find genetic variants that are important in predicting EFV plasma concentration, was motivated by the need to come up with a test for EFV dosing. Thus, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for individual SNP genotypes and combinations, considering SNPs included in multivariate logistic regression analysis. Genotypes and their combinations were used to predict EFV plasma concentrations above 4 μg/mL (Table 3 and Supplementary Table S3). Seventy-seven percent (n = 33∕43) of patients with the CYP2B6 c.516T/T genotype had EFV plasma concentrations above 4 μg/mL (Supplementary Table S3). Thus, the CYP2B6 c.516T/T genotype was associated with the following parameters; sensitivity of 48% and specificity of 94% in predicting EFV plasma concentrations > 4 μg/mL. Sensitivity of the CYP2B6 c.983C/C genotype (7%) in predicting EFV plasma concentrations > 4 μg/mL was low, but the specificity (100%) was high. Sensitivity and NPV of the CYP2B6 c.485-18C/C and c.1421T/T genotypes were high, but the specificity and PPV were low. Using the CYP2B6 c.516G>T and c.983T>C SNPs to come up with the CYP2B6 poor metabolizer phenotype (CYP2B6 c.516T/T or CYP2B6 c.983C/C or CYP2B6 c.516G/T+CYP2B6 c.983T/C) showed the best predictive model with 68% sensitivity, 93% specificity, 83% PPV, and 87% NPV, respectively (Table 3).
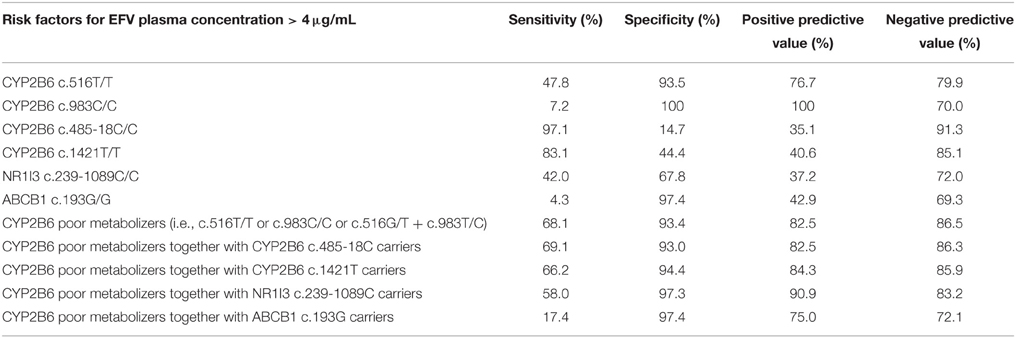
Table 3. Validity of genotypes in predicting efavirenz plasma concentrations above 4 μg/mL.
Allele frequencies of SNPs for other world ethnic groups were obtained from the National Centre for Biotechnology Information (NCBI) dbSNP database (http://www.ncbi.nlm.nih.gov/) and the 1000 Genomes Project (http://www.1000genomes.org/). Statistically significant differences were clearly observed when the South African group was compared to American, Asian, and European groups. In addition, differences were also observed when the South African group was compared to the Yoruba and Luhya (Table 4). For example, NR1I2 c.659T-allele was present at a frequency of 0.05 in the South African group, absent among Asians, yet comparable to that of the Americans (0.07–0.13). In contrast, the UGT2B7 c.211T-allele was absent among South Africans, other Africans, and Europeans, but present among Asians (0.11–0.14). Comparison of the NR1I2 c.758G-allele showed a significantly higher frequency among the Yoruba (0.19), the Luhya (0.10), and African Americans (0.11) compared to a frequency of 0.06 among South Africans.
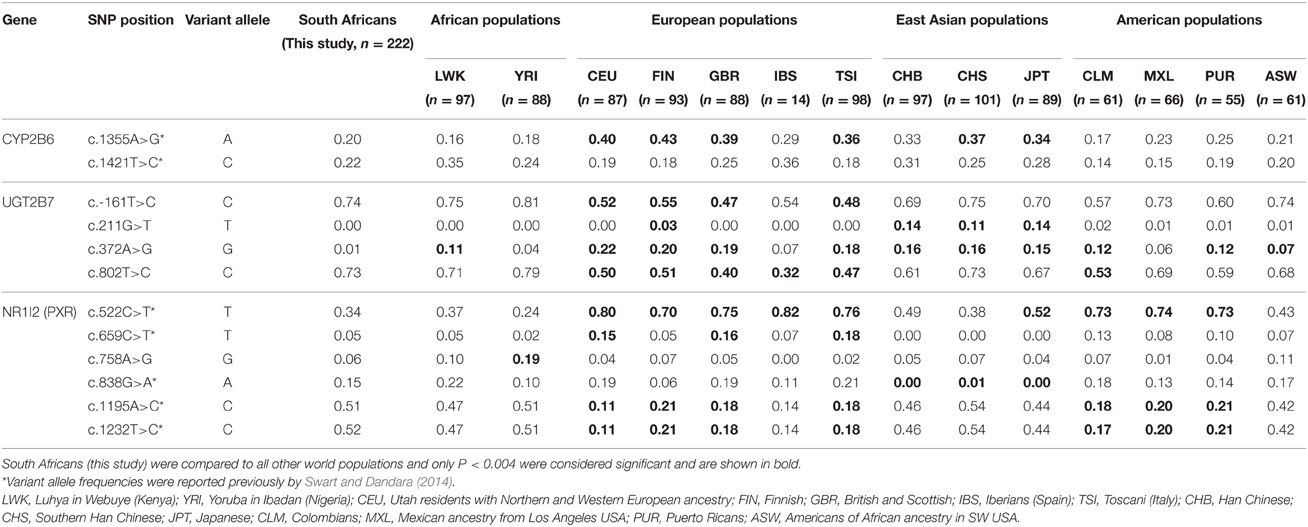
Table 4. Variant allele frequencies in the South African population compared to other world populations.
This study has taken investigation into pharmacogenetics determinants of EFV plasma concentration further by evaluating the contribution of 30 SNPs, especially those in the 3′-UTR of genes that code for DMEs metabolizing EFV. Most studies have concentrated on the role of CYP2B6 c.516G>T and c.983T>C SNPs in predicting EFV plasma concentration. We report on large inter-individual variability in EFV plasma concentration supporting previous studies among South Africans (Gounden et al., 2010) and Swiss patients (Marzolini et al., 2001; Colombo et al., 2006). Thirty-four percent of the patients presented with EFV plasma concentrations outside the therapeutic range (3% below and 31% above) and are at risk of failing therapy or presenting with ADRs, respectively. This is similar to observations by Marzolini et al. (2001), Ståhle et al. (2004), Lubomirov et al. (2011), Mukonzo et al. (2013), and Sanchez Martin et al. (2013). Poor virologic suppression and ADRs lead to patient's health deteriorating which could lead to increased non-adherence to treatment (ter Heine et al., 2008).
Drug response is a complex phenotype and multiple factors including ethnicity, sex, age, body weight, drug-drug, and drug-food interactions, hepatic impairment, disease state, pregnancy, and host genetic variation can influence the pharmacokinetic variability of EFV (Burger et al., 2006; Rotger et al., 2006; Stohr et al., 2008). Alcohol consumption and BMI were included in the multivariate logistic regression analysis as potential contributors to EFV plasma concentrations > 4 μg/mL. However, the majority of HIV/AIDS patients were females which might be the reason for the very low smoking and alcohol consumption among the patients. Smoking and alcohol consumption is generally a less common lifestyle among female Bantu-speaking South Africans, compared to other racial groups. In this study, EFV plasma concentrations were higher in patients with a lower BMI supporting observations by Poeta et al. (2011) and Stohr et al. (2008).
Genetic variation in genes coding for DMEs responsible for EFV metabolism is known to affect EFV plasma concentrations, thus, a comprehensive analysis on the contribution of genetic variants in genes coding for enzymes involved in EFV metabolism was carried out. CYP2B6 c.516G>T and c.983T>C SNPs are well-characterized predictors of EFV plasma concentration (Haas et al., 2004; Swart et al., 2013) and here we re-confirm their importance. Dhoro et al. (2015) reported that Zimbabwean HIV/AIDS patients carrying the CYP2B6 c.516T/T genotype had 63% decreased EFV clearance. Mukonzo et al. (2014) also reported an association of CYP2B6 c.516T/T genotype with increased EFV exposure among Ugandan patients leading to their recommendation of daily doses of 300 mg for CYP2B6 c.516T/T genotype carriers.
Five individuals with the CYP2B6 c.983C/C genotype were identified in this study and four of these patients had nearly five-fold higher EFV plasma concentrations (34.4, 21.8, 12.1, and 22.3 μg/mL) with respect to the therapeutic range upper limit of 4 μg/mL. CYP2B6 c.983C-allele has been associated with significant differences in EFV exposure among individuals of African and Caucasian ancestry (Gatanaga et al., 2007; Wyen et al., 2008; Haas et al., 2009). Multivariate logistic regression analysis showed an additive effect between the CYP2B6 c.516G>T and c.983T>C SNPs with an almost two-fold higher EFV plasma concentration, a finding in agreement with reports by Wyen et al. (2008) and Schipani et al. (2011). These observations suggest that CYP2B6 polymorphisms can be used as biomarkers of EFV plasma concentration, further arguing for genotype-assisted dosing with respect to the use of EFV-containing HAART (Rotger et al., 2007; Rotger and Telenti, 2008; Schipani et al., 2011). Recommendations based on pharmacogenetics knowledge are being proposed, such as gradual reductions in EFV dose from 600 to 400 or 200 mg/day for intermediate metabolizer and poor metabolizer patient groups, respectively (Gatanaga et al., 2007; Cabrera et al., 2009; Mukonzo et al., 2014). The recently completed ENCORE1 study (including 37% African individuals) concluded that HIV suppression was comparable between EFV doses of 400 and 600 mg daily (Dickinson et al., 2015). Bisaso et al. (2015) suggested a 7% reduction in neuropsychological impairment probability at an EFV dose of 450 mg/day. The cost-effectiveness of using CYP2B6 genotyping to adjust EFV dosage was assessed recently by Schackman et al. (2015). The cost-effectiveness ratio of genotype-assisted dosing compared to a lower universal dose remains greater than $ 100,000/quality-adjusted life years, unless HIV RNA suppression is decreased by more than 15% (Schackman et al., 2015).
In addition to univariate analysis, haplotypes were inferred for each HIV/AIDS patient and median EFV plasma concentrations were compared between haplotype groups. The effect of the CYP2B6 c.516G>T SNP is shown by the significantly higher median EFV plasma concentration for the CYP2B6 A-T-G-T-(C or T)-C-G-(T or A)-G-AG-T haplotype compared to the A-G-A-T-C-C-G-A-G-AG-T and A-G-A-T-C-C-G-A-G-CA-C haplotypes. However, only four of the nine haplotypes with the CYP2B6 c.516T-allele, had median EFV plasma concentrations above 4 μg/mL. This observation points to the potential involvement of additional SNPs in CYP2B6 or other genes coding for DMEs that play a role in EFV metabolism.
Furthermore, multivariate logistic regression analysis was performed to identify additional contributors to variability in EFV plasma concentration. Few studies have investigated the effect of SNPs in the 3′-UTR of genes coding for DMEs in drug response. A trend towards low EFV plasma concentration was observed for the CYP2B6 c.1421C-allele which is located in the 3′-UTR. The CYP2B6 c.1421T>C SNP is predicted to affect the binding of miR-3612, miR-650, miR-4266, miR-4779, miR-4695-5p, miR-765, miR-4476, miR-6077, miR-6876-5p, and miR-8065 (Swart and Dandara, 2014) and, thus, potentially alter levels of CYP2B6 mRNA.
In addition to CYP2B6 c.516G>T and c.983T>C SNPs, the NR1I3 c.239-1089T>C, ABCB1 c.193A>G, CYP2B6 c.485-18C>T, and CYP2B6 c.1421T>C SNPs potentially further contribute to variability in EFV plasma concentration. However, sensitivity, specificity, positive, and negative predictive values for each SNP alone was low, but combining the CYP2B6 c.516G>T and c.983T>C SNPs improved the predictive values further arguing for their utility in a pharmacogenetics-based test. Further, addition of the CYP2B6 c.485-18C>T SNP improved the sensitivity from 68 to 69%. Inclusion of the NR1I3 c.239-1089T>C, ABCB1 c.193A>G, and CYP2B6 c.1421T>C SNPs did not improve predictive ability of the CYP2B6 poor metabolizers (PMs) genotyping test.
The current study shows major differences in variant allele frequencies of SNPs between ethnic groups. Allele frequencies were significantly different between African and other populations especially for NR1I2 c.522C>T, NR1I2 c.1195A>C, and NR1I2 c.1232T>C SNPs. NR1I2 codes for the nuclear receptor PXR and is responsible for regulating most genes coding for Phase I, Phase II enzymes, and transporters. PXR is activated by many ligands including the antimalarial drug artemisinin (Burk et al., 2005) and EFV (Healan-Greenberg et al., 2008). Furthermore, it appears the UGT2B7 c.211G>T SNP is specific to Asian populations, while NR1I2 c.659C>T and c.838G>A SNPs are rare among Asians. Differences in allele distribution are likely to contribute to the observed ethnic variability in drug levels.
Inter-ethnic variations in drug exposure may possibly result in varying clinical treatment outcome or adverse event profiles between populations (Ngaimisi et al., 2013). African populations are the most genetically diverse, thus, should be utilized in clinical trials to enable the teasing out of genetic correlates of drug response. The high prevalence of HIV/AIDS in South Africa, combined with the exposure to ARVs necessitates characterizing the genetic variation of pharmacogenetically relevant genes to improve drug response (Colic et al., 2015).
The current study is a continuation of earlier studies to assess the contribution of 30 SNPs, especially those in the 3′-UTR of genes that code for DMEs metabolizing EFV. The association or trend toward low median EFV plasma concentration observed for the NR1I3 c.239-1089T-allele, the ABCB1 c.193A-allele, the CYP2B6 c.485-18T-allele, and the CYP2B6 c.1421C-allele need to be investigated in further replication and larger cohorts. Compared to CYP2B6 c.516G>T and c.983T>C SNPs, the NR1I3 c.239-1089T>C, ABCB1 c.193A>G, CYP2B6 c.485-18C>T, and CYP2B6 c.1421T>C SNPs seem to play minor roles in predicting EFV plasma concentrations above 4 μg/mL.
CD conceived of the study, designed, coordinated the study, recruited all the participants, and did all the sampling, also assisted with statistical data analysis, helped to draft the manuscript and approved the final version. MSW, JE, MSK carried out the molecular genetic characterization experiments and MSW drafted the manuscript. SC, LW, and PS carried out the LC/MS/MS analysis of EFV concentration. All authors read and approved the final manuscript.
Research reported in this publication was supported by the South African Medical Research Council (SAMRC) Self-Initiated Research Grant awarded to CD for pharmacogenetics research. MSW was awarded study bursaries by the SAMRC and University of Cape Town Carnegie Corporation Developing the Next Generation of Academics Program (infectious diseases research focus). The views and opinions expressed are not those of the SAMRC but of the authors of the material published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: http://journal.frontiersin.org/article/10.3389/fgene.2015.00356
Abah, I. O., Akanbi, M., Abah, M. E., Finangwai, A. I., Dady, C. W., Falang, K. D., et al. (2015). Incidence and predictors of adverse drug events in an African cohort of HIV-infected adults treated with efavirenz. Germs 5, 83–91. doi: 10.11599/germs.2015.1075
Adkins, J. C., and Noble, S. (1998). Efavirenz. Drugs 56, 1055–1064, Discussion: 1065–1056. doi: 10.2165/00003495-199856060-00014
Arab-Alameddine, M., Di Iulio, J., Buclin, T., Rotger, M., Lubomirov, R., Cavassini, M., et al. (2009). Pharmacogenetics-based population pharmacokinetic analysis of efavirenz in HIV-1-infected individuals. Clin. Pharmacol. Ther. 85, 485–494. doi: 10.1038/clpt.2008.271
Bae, S. K., Jeong, Y. J., Lee, C., and Liu, K. H. (2011). Identification of human UGT isoforms responsible for glucuronidation of efavirenz and its three hydroxy metabolites. Xenobiotica 41, 437–444. doi: 10.3109/00498254.2011.551849
Bisaso, K. R., Mukonzo, J. K., and Ette, E. I. (2015). Markov model for characterizing neuropsychologic impairment and Monte Carlo simulation for optimizing efavirenz therapy. J. Clin. Pharmacol. 55, 1229–1235. doi: 10.1002/jcph.533
Brown, K. C., Hosseinipour, M. C., Hoskins, J. M., Thirumaran, R. K., Tien, H. C., Weigel, R., et al. (2012). Exploration of CYP450 and drug transporter genotypes and correlations with nevirapine exposure in Malawians. Pharmacogenomics 13, 113–121. doi: 10.2217/pgs.11.132
Burger, D., van der Heiden, I., La Porte, C., van der Ende, M., Groeneveld, P., Richter, C., et al. (2006). Interpatient variability in the pharmacokinetics of the HIV non-nucleoside reverse transcriptase inhibitor efavirenz: the effect of gender, race, and CYP2B6 polymorphism. Br. J. Clin. Pharmacol. 61, 148–154. doi: 10.1111/j.1365-2125.2005.02536.x
Burhenne, J., Matthée, A. K., Pasáková, I., Röder, C., Heinrich, T., Haefeli, W. E., et al. (2010). No evidence for induction of ABC transporters in peripheral blood mononuclear cells in humans after 14 days of efavirenz treatment. Antimicrob. Agents Chemother. 54, 4185–4191. doi: 10.1128/AAC.00283-10
Burk, O., Arnold, K. A., Nussler, A. K., Schaeffeler, E., Efimova, E., Avery, B. A., et al. (2005). Antimalarial artemisinin drugs induce cytochrome P450 and MDR1 expression by activation of xenosensors pregnane X receptor and constitutive androstane receptor. Mol. Pharmacol. 67, 1954–1965. doi: 10.1124/mol.104.009019
Cabrera, S. E., Santos, D., Valverde, M. P., Domínguez-Gil, A., Gonzalez, F., Luna, G., et al. (2009). Influence of the cytochrome P450 2B6 genotype on population pharmacokinetics of efavirenz in human immunodeficiency virus patients. Antimicrob. Agents Chemother. 53, 2791–2798. doi: 10.1128/AAC.01537-08
Cassetti, I., Madruga, J. V., Suleiman, J. M., Etzel, A., Zhong, L., Cheng, A. K., et al. (2007). The safety and efficacy of tenofovir DF in combination with lamivudine and efavirenz through 6 years in antiretroviral-naive HIV-1-infected patients. HIV Clin. Trials 8, 164–172. doi: 10.1310/hct0803-164
Ciccacci, C., Borgiani, P., Ceffa, S., Sirianni, E., Marazzi, M. C., Altan, A. M., et al. (2010). Nevirapine-induced hepatotoxicity and pharmacogenetics: a retrospective study in a population from Mozambique. Pharmacogenomics 11, 23–31. doi: 10.2217/pgs.09.142
Colic, A., Alessandrini, M., and Pepper, M. S. (2015). Pharmacogenetics of CYP2B6, CYP2A6 and UGT2B7 in HIV treatment in African populations: focus on efavirenz and nevirapine. Drug Metab. Rev. 47, 111–123. doi: 10.3109/03602532.2014.982864
Colombo, S., Telenti, A., Buclin, T., Furrer, H., Lee, B. L., Biollaz, J., et al. (2006). Are plasma levels valid surrogates for cellular concentrations of antiretroviral drugs in HIV-infected patients? Ther. Drug Monit. 28, 332–338. doi: 10.1097/01.ftd.0000211807.74192.62
Cortes, C. P., Siccardi, M., Chaikan, A., Owen, A., Zhang, G., and La Porte, C. J. (2013). Correlates of efavirenz exposure in Chilean patients affected with human immunodeficiency virus reveals a novel association with a polymorphism in the constitutive androstane receptor. Ther. Drug Monit. 35, 78–83. doi: 10.1097/FTD.0b013e318274197e
Dhoro, M., Zvada, S., Ngara, B., Nhachi, C., Kadzirange, G., Chonzi, P., et al. (2015). CYP2B6*6, CYP2B6*18, Body weight and sex are predictors of efavirenz pharmacokinetics and treatment response: population pharmacokinetic modeling in an HIV/AIDS and TB cohort in Zimbabwe. BMC Pharmacol. Toxicol. 16:4. doi: 10.1186/s40360-015-0004-2
Dickinson, L., Amin, J., Else, L., Boffito, M., Egan, D., Owen, A., et al. (2015). Pharmacokinetic and pharmacodynamic comparison of once-daily efavirenz (400 mg vs. 600 mg) in treatment-Naive HIV-infected patients: results of the ENCORE1 study. Clin. Pharmacol. Ther. 98, 406–416. doi: 10.1002/cpt.156
di Iulio, J., Fayet, A., Arab-Alameddine, M., Rotger, M., Lubomirov, R., Cavassini, M., et al. (2009). In vivo analysis of efavirenz metabolism in individuals with impaired CYP2A6 function. Pharmacogenet. Genomics 19, 300–309. doi: 10.1097/FPC.0b013e328328d577
Elens, L., Vandercam, B., Yombi, J. C., Lison, D., Wallemacq, P., and Haufroid, V. (2010). Influence of host genetic factors on efavirenz plasma and intracellular pharmacokinetics in HIV-1-infected patients. Pharmacogenomics 11, 1223–1234. doi: 10.2217/pgs.10.94
Evans, J., Swart, M., Soko, N., Wonkam, A., Huzair, F., and Dandara, C. (2015). A global health diagnostic for personalized medicine in resource-constrained world settings: a simple PCR-RFLP method for genotyping CYP2B6 g.15582C>T and science and policy relevance for optimal use of antiretroviral drug efavirenz. OMICS 19, 332–338. doi: 10.1089/omi.2015.0039
Fumaz, C. R., Tuldra, A., Ferrer, M. J., Paredes, R., Bonjoch, A., Jou, T., et al. (2002). Quality of life, emotional status, and adherence of HIV-1-infected patients treated with efavirenz versus protease inhibitor-containing regimens. J. Acquir. Immune Defic. Syndr. 29, 244–253. doi: 10.1097/00042560-200203010-00004
Gatanaga, H., Hayashida, T., Tsuchiya, K., Yoshino, M., Kuwahara, T., Tsukada, H., et al. (2007). Successful efavirenz dose reduction in HIV type 1-infected individuals with cytochrome P450 2B6 *6 and *26. Clin. Infect. Dis. 45, 1230–1237. doi: 10.1086/522175
Gounden, V., van Niekerk, C., Snyman, T., and George, J. A. (2010). Presence of the CYP2B6 516G> T polymorphism, increased plasma Efavirenz concentrations and early neuropsychiatric side effects in South African HIV-infected patients. AIDS Res. Ther. 7:32. doi: 10.1186/1742-6405-7-32
Gross, R., Aplenc, R., Tenhave, T., Foulkes, A. S., Thakur, R., Mosepele, M., et al. (2008). Slow efavirenz metabolism genotype is common in Botswana. J. Acquir. Immune Defic. Syndr. 49, 336–337. doi: 10.1097/QAI.0b013e31817c1ed0
Guillemette, C. (2003). Pharmacogenomics of human UDP-glucuronosyltransferase enzymes. Pharmacogenomics J. 3, 136–158. doi: 10.1038/sj.tpj.6500171
Gulick, R. M., Ribaudo, H. J., Shikuma, C. M., Lalama, C., Schackman, B. R., Meyer, W. A., et al. (2006). Three- vs four-drug antiretroviral regimens for the initial treatment of HIV-1 infection: a randomized controlled trial. JAMA 296, 769–781. doi: 10.1001/jama.296.7.769
Haas, D. W. (2005). Will pharmacogenomic discoveries improve HIV therapeutics? Top. HIV Med. 13, 90–95.
Haas, D. W., Gebretsadik, T., Mayo, G., Menon, U. N., Acosta, E. P., Shintani, A., et al. (2009). Associations between CYP2B6 polymorphisms and pharmacokinetics after a single dose of nevirapine or efavirenz in African americans. J. Infect. Dis. 199, 872–880. doi: 10.1086/597125
Haas, D. W., Kwara, A., Richardson, D. M., Baker, P., Papageorgiou, I., Acosta, E. P., et al. (2014a). Secondary metabolism pathway polymorphisms and plasma efavirenz concentrations in HIV-infected adults with CYP2B6 slow metabolizer genotypes. J. Antimicrob. Chemother. 69, 2175–2182. doi: 10.1093/jac/dku110
Haas, D. W., Ribaudo, H. J., Kim, R. B., Tierney, C., Wilkinson, G. R., Gulick, R. M., et al. (2004). Pharmacogenetics of efavirenz and central nervous system side effects: an adult AIDS clinical trials group study. AIDS 18, 2391–2400.
Haas, D. W., Severe, P., Jean Juste, M. A., Pape, J. W., and Fitzgerald, D. W. (2014b). Functional CYP2B6 variants and virologic response to an efavirenz-containing regimen in Port-au-Prince, Haiti. J. Antimicrob. Chemother. 69, 2187–2190. doi: 10.1093/jac/dku088
Haas, D. W., Smeaton, L. M., Shafer, R. W., Robbins, G. K., Morse, G. D., Labbe, L., et al. (2005). Pharmacogenetics of long-term responses to antiretroviral regimens containing Efavirenz and/or Nelfinavir: an Adult Aids Clinical Trials Group Study. J. Infect. Dis. 192, 1931–1942. doi: 10.1086/497610
Hawkins, T., Geist, C., Young, B., Giblin, A., Mercier, R. C., Thornton, K., et al. (2005). Comparison of neuropsychiatric side effects in an observational cohort of efavirenz- and protease inhibitor-treated patients. HIV Clin. Trials 6, 187–196. doi: 10.1310/92VR-FP24-J8GA-B49Q
Healan-Greenberg, C., Waring, J. F., Kempf, D. J., Blomme, E. A., Tirona, R. G., and Kim, R. B. (2008). A human immunodeficiency virus protease inhibitor is a novel functional inhibitor of human pregnane X receptor. Drug Metab. Dispos. 36, 500–507. doi: 10.1124/dmd.107.019547
Holzinger, E. R., Grady, B., Ritchie, M. D., Ribaudo, H. J., Acosta, E. P., Morse, G. D., et al. (2012). Genome-wide association study of plasma efavirenz pharmacokinetics in AIDS Clinical Trials Group protocols implicates several CYP2B6 variants. Pharmacogenet. Genomics. 22, 858–867. doi: 10.1097/FPC.0b013e32835a450b
Ikediobi, O., Aouizerat, B., Xiao, Y., Gandhi, M., Gebhardt, S., and Warnich, L. (2011). Analysis of pharmacogenetic traits in two distinct South African populations. Hum. Genomics 5, 265–282. doi: 10.1186/1479-7364-5-4-265
Jamshidi, Y., Moreton, M., McKeown, D. A., Andrews, S., Nithiyananthan, T., Tinworth, L., et al. (2010). Tribal ethnicity and CYP2B6 genetics in Ugandan and Zimbabwean populations in the UK: implications for efavirenz dosing in HIV infection. J. Antimicrob. Chemother. 65, 2614–2619. doi: 10.1093/jac/dkq369
Kenedi, C. A., and Goforth, H. W. (2011). A systematic review of the psychiatric side-effects of efavirenz. AIDS Behav. 15, 1803–1818. doi: 10.1007/s10461-011-9939-5
Kim, J. Y., Cheong, H. S., Park, B. L., Kim, L. H., Namgoong, S., Kim, J. O., et al. (2014). Comprehensive variant screening of the UGT gene family. Yonsei Med. J. 55, 232–239. doi: 10.3349/ymj.2014.55.1.232
Klein, K., Lang, T., Saussele, T., Barbosa-Sicard, E., Schunck, W. H., Eichelbaum, M., et al. (2005). Genetic variability of CYP2B6 in populations of African and Asian origin: allele frequencies, novel functional variants, and possible implications for anti-HIV therapy with efavirenz. Pharmacogenet. Genomics 15, 861–873. doi: 10.1097/01213011-200512000-00004
Lee, S. S., To, K. W., Lee, M. P., Wong, N. S., Chan, D. P., Li, P. C., et al. (2014). Sleep quality in efavirenz-treated Chinese HIV patients—comparing between GT and GG genotype of CYP2B6-516 G/T polymorphisms. Int. J. STD AIDS 25, 193–200. doi: 10.1177/0956462413498581
Leutscher, P. D., Stecher, C., Storgaard, M., and Larsen, C. S. (2013). Discontinuation of efavirenz therapy in HIV patients due to neuropsychiatric adverse effects. Scand. J. Infect. Dis. 45, 645–651. doi: 10.3109/00365548.2013.773067
Li, J., Menard, V., Benish, R. L., Jurevic, R. J., Guillemette, C., Stoneking, M., et al. (2012). Worldwide variation in human drug-metabolism enzyme genes CYP2B6 and UGT2B7: implications for HIV/AIDS treatment. Pharmacogenomics 13, 555–570. doi: 10.2217/pgs.11.160
Li, Z., Zhang, Z., He, Z., Tang, W., Li, T., Zeng, Z., et al. (2009). A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers: update of the SHEsis (http://analysis.bio-x.cn). Cell Res. 19, 519–523. doi: 10.1038/cr.2009.33
Lubomirov, R., Colombo, S., di Iulio, J., Ledergerber, B., Martinez, R., Cavassini, M., et al. (2011). Association of pharmacogenetic markers with premature discontinuation of first-line anti-HIV therapy: an observational cohort study. J. Infect. Dis. 203, 246–257. doi: 10.1093/infdis/jiq043
Maimbo, M., Kiyotani, K., Mushiroda, T., Masimirembwa, C., and Nakamura, Y. (2012). CYP2B6 genotype is a strong predictor of systemic exposure to efavirenz in HIV-infected Zimbabweans. Eur. J. Clin. Pharmacol. 68, 267–271. doi: 10.1007/s00228-011-1118-0
Marzolini, C., Telenti, A., Decosterd, L. A., Greub, G., Biollaz, J., and Buclin, T. (2001). Efavirenz plasma levels can predict treatment failure and central nervous system side effects in HIV-1-infected patients. AIDS 15, 71–75. doi: 10.1097/00002030-200101050-00011
Mehlotra, R. K., Bockarie, M. J., and Zimmerman, P. A. (2007). CYP2B6 983T>C polymorphism is prevalent in West Africa but absent in Papua New Guinea: implications for HIV/AIDS treatment. Br. J. Clin. Pharmacol. 64, 391–395. doi: 10.1111/j.1365-2125.2007.02884.x
Mehlotra, R. K., Ziats, M. N., Bockarie, M. J., and Zimmerman, P. A. (2006). Prevalence of CYP2B6 alleles in malaria-endemic populations of West Africa and Papua New Guinea. Eur. J. Clin. Pharmacol. 62, 267–275. doi: 10.1007/s00228-005-0092-9
Moyle, G. (1999a). Efavirenz: practicalities, considerations and new issues. Int. J. Clin. Pract. Suppl. 103, 30–34.
Moyle, G. J. (1999b). Efavirenz: shifting the HAART paradigm in adult HIV-1 infection. Expert Opin. Investig. Drugs 8, 473–486.
Mukonzo, J. K., Okwera, A., Nakasujja, N., Luzze, H., Sebuwufu, D., Ogwal-Okeng, J., et al. (2013). Influence of efavirenz pharmacokinetics and pharmacogenetics on neuropsychological disorders in Ugandan HIV-positive patients with or without tuberculosis: a prospective cohort study. BMC Infect. Dis. 13:261. doi: 10.1186/1471-2334-13-261
Mukonzo, J. K., Owen, J. S., Ogwal-Okeng, J., Kuteesa, R. B., Nanzigu, S., Sewankambo, N., et al. (2014). Pharmacogenetic-based efavirenz dose modification: suggestions for an African population and the different CYP2B6 genotypes. PLoS ONE 9:e86919. doi: 10.1371/journal.pone.0086919
Mukonzo, J. K., Röshammar, D., Waako, P., Andersson, M., Fukasawa, T., Milani, L., et al. (2009). A novel polymorphism in ABCB1 gene, CYP2B6*6 and sex predict single-dose efavirenz population pharmacokinetics in Ugandans. Br. J. Clin. Pharmacol. 68, 690–699. doi: 10.1111/j.1365-2125.2009.03516.x
Naidoo, P., Chetty, V. V., and Chetty, M. (2014). Impact of CYP polymorphisms, ethnicity and sex differences in metabolism on dosing strategies: the case of efavirenz. Eur. J. Clin. Pharmacol. 70, 379–389. doi: 10.1007/s00228-013-1634-1
Ngaimisi, E., Habtewold, A., Minzi, O., Makonnen, E., Mugusi, S., Amogne, W., et al. (2013). Importance of ethnicity, CYP2B6 and ABCB1 genotype for efavirenz pharmacokinetics and treatment outcomes: a parallel-group prospective cohort study in two sub-Saharan Africa populations. PLoS ONE 8:e67946. doi: 10.1371/journal.pone.0067946
Nolan, D., Phillips, E., and Mallal, S. (2006). Efavirenz and CYP2B6 polymorphism: implications for drug toxicity and resistance. Clin. Infect. Dis. 42, 408–410. doi: 10.1086/499369
Nyakutira, C., Röshammar, D., Chigutsa, E., Chonzi, P., Ashton, M., Nhachi, C., et al. (2008). High prevalence of the CYP2B6 516G–>T(*6) variant and effect on the population pharmacokinetics of efavirenz in HIV/AIDS outpatients in Zimbabwe. Eur. J. Clin. Pharmacol. 64, 357–365. doi: 10.1007/s00228-007-0412-3
Ogburn, E. T., Jones, D. R., Masters, A. R., Xu, C., Guo, Y., and Desta, Z. (2010). Efavirenz primary and secondary metabolism in vitro and in vivo: identification of novel metabolic pathways and cytochrome P450 2A6 as the principal catalyst of efavirenz 7-hydroxylation. Drug Metab. Dispos. 38, 1218–1229. doi: 10.1124/dmd.109.031393
Parathyras, J., Gebhardt, S., Hillermann-Rebello, R., Grobbelaar, N., Venter, M., and Warnich, L. (2009). A pharmacogenetic study of CD4 recovery in response to HIV antiretroviral therapy in two South African population groups. J. Hum. Genet. 54, 261–265. doi: 10.1038/jhg.2009.20
Penzak, S. R., Kabuye, G., Mugyenyi, P., Mbamanya, F., Natarajan, V., Alfaro, R. M., et al. (2007). Cytochrome P450 2B6 (CYP2B6) G516T influences nevirapine plasma concentrations in HIV-infected patients in Uganda. HIV Med. 8, 86–91. doi: 10.1111/j.1468-1293.2007.00432.x
Poeta, J., Linden, R., Antunes, M. V., Real, L., Menezes, A. M., Ribeiro, J. P., et al. (2011). Plasma concentrations of efavirenz are associated with body weight in HIV-positive individuals. J. Antimicrob. Chemother. 66, 2601–2604. doi: 10.1093/jac/dkr360
Raffi, F., Pozniak, A. L., and Wainberg, M. A. (2014). Has the time come to abandon efavirenz for first-line antiretroviral therapy? J. Antimicrob. Chemother. 69, 1742–1747. doi: 10.1093/jac/dku058
Rotger, M., Lubomirov, R., Rodriguez-Novoa, S., and Barreiro, P. (2006). [Pharmacogenetics of antiretroviral therapy.]. Enferm. Infecc. Microbiol. Clin. 24(Suppl. 2), 13–18. doi: 10.1157/13096045
Rotger, M., Tegude, H., Colombo, S., Cavassini, M., Furrer, H., Décosterd, L., et al. (2007). Predictive value of known and novel alleles of CYP2B6 for efavirenz plasma concentrations in HIV-infected individuals. Clin. Pharmacol. Ther. 81, 557–566. doi: 10.1038/sj.clpt.6100072
Rotger, M., and Telenti, A. (2008). Optimizing efavirenz treatment: CYP2B6 genotyping or therapeutic drug monitoring? Eur. J. Clin. Pharmacol. 64, 335–336. doi: 10.1007/s00228-007-0440-z
Sanchez Martin, A., Cabrera Figueroa, S., Cruz Guerrero, R., Hurtado, L. P., Hurle, A. D., and Carracedo Alvarez, A. (2013). Impact of pharmacogenetics on CNS side effects related to efavirenz. Pharmacogenomics 14, 1167–1178. doi: 10.2217/pgs.13.111
Sarfo, F. S., Zhang, Y., Egan, D., Tetteh, L. A., Phillips, R., Bedu-Addo, G., et al. (2013). Pharmacogenetic associations with plasma efavirenz concentrations and clinical correlates in a retrospective cohort of Ghanaian HIV-infected patients. J. Antimicrob. Chemother. 69, 491–499. doi: 10.1093/jac/dkt372
Sarfo, F. S., Zhang, Y., Egan, D., Tetteh, L. A., Phillips, R., Bedu-Addo, G., et al. (2014). Pharmacogenetic associations with plasma efavirenz concentrations and clinical correlates in a retrospective cohort of Ghanaian HIV-infected patients. J. Antimicrob. Chemother. 69, 491–499. doi: 10.1093/jac/dkt372
Schackman, B. R., Haas, D. W., Park, S. S., Li, X. C., and Freedberg, K. A. (2015). Cost-effectiveness of CYP2B6 genotyping to optimize efavirenz dosing in HIV clinical practice. Pharmacogenomics 16, 2007–2018. doi: 10.2217/pgs.15.142
Schipani, A., Wyen, C., Mahungu, T., Hendra, H., Egan, D., Siccardi, M., et al. (2011). Integration of population pharmacokinetics and pharmacogenetics: an aid to optimal nevirapine dose selection in HIV-infected individuals. J. Antimicrob. Chemother. 66, 1332–1339. doi: 10.1093/jac/dkr087
Shi, Y. Y., and He, L. (2005). SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Res. 15, 97–98. doi: 10.1038/sj.cr.7290272
Sinxadi, P. Z., Leger, P. D., McIlleron, H. M., Smith, P. J., Dave, J. A., Levitt, N. S., et al. (2015). Pharmacogenetics of plasma efavirenz exposure in HIV-infected adults and children in South Africa. Br. J. Clin. Pharmacol. 80, 146–156. doi: 10.1111/bcp.12590
Ståhle, L., Moberg, L., Svensson, J. O., and Sönnerborg, A. (2004). Efavirenz plasma concentrations in HIV-infected patients: inter- and intraindividual variability and clinical effects. Ther. Drug Monit. 26, 267–270. doi: 10.1097/00007691-200406000-00008
Stöhr, W., Back, D., Dunn, D., Sabin, C., Winston, A., Gilson, R., et al. (2008). Factors influencing efavirenz and nevirapine plasma concentration: effect of ethnicity, weight and co-medication. Antivir. Ther. 13, 675–685.
Sukasem, C., Manosuthi, W., Koomdee, N., Santon, S., Jantararoungtong, T., Prommas, S., et al. (2014). Low level of efavirenz in HIV-1-infected Thai adults is associated with the CYP2B6 polymorphism. Infection 42, 469–474. doi: 10.1007/s15010-013-0560-6
Swart, M., and Dandara, C. (2014). Genetic variation in the 3′-UTR of CYP1A2, CYP2B6, CYP2D6, CYP3A4, NR1I2, and UGT2B7: potential effects on regulation by microRNA and pharmacogenomics relevance. Front. Genet. 5:167. doi: 10.3389/fgene.2014.00167
Swart, M., Ren, Y., Smith, P., and Dandara, C. (2012a). ABCB1 4036A>G and 1236C>T polymorphisms affect plasma efavirenz levels in South African HIV/AIDS patients. Front. Genet. 3:236. doi: 10.3389/fgene.2012.00236
Swart, M., Skelton, M., Ren, Y., Smith, P., Takuva, S., and Dandara, C. (2013). High predictive value of CYP2B6 SNPs for steady-state plasma efavirenz levels in South African HIV/AIDS patients. Pharmacogenet. Genomics 23, 415–427. doi: 10.1097/FPC.0b013e328363176f
Swart, M., Skelton, M., Wonkam, A., Kannemeyer, L., Chin'Ombe, N., and Dandara, C. (2012b). CYP1A2, CYP2A6, CYP2B6, CYP3A4 and CYP3A5 polymorphisms in two bantu-speaking populations from cameroon and South Africa: implications for global pharmacogenetics. Curr. Pharmacogenomics Person. Med. 10, 43–53. doi: 10.2174/1875692111201010043
Swart, M., Whitehorn, H., Ren, Y., Smith, P., Ramesar, R. S., and Dandara, C. (2012c). PXR and CAR single nucleotide polymorphisms influence plasma efavirenz levels in South African HIV/AIDS patients. BMC Med. Genet. 13:112. doi: 10.1186/1471-2350-13-112
ter Heine, R., Scherpbier, H. J., Crommentuyn, K. M., Bekker, V., Beijnen, J. H., Kuijpers, T. W., et al. (2008). A pharmacokinetic and pharmacogenetic study of efavirenz in children: dosing guidelines can result in subtherapeutic concentrations. Antivir. Ther. 13, 779–787.
Tian, J. N., Ho, I. K., Tsou, H. H., Fang, C. P., Hsiao, C. F., Chen, C. H., et al. (2012). UGT2B7 genetic polymorphisms are associated with the withdrawal symptoms in methadone maintenance patients. Pharmacogenomics 13, 879–888. doi: 10.2217/pgs.12.69
Ward, B. A., Gorski, J. C., Jones, D. R., Hall, S. D., Flockhart, D. A., and Desta, Z. (2003). The cytochrome P450 2B6 (CYP2B6) is the main catalyst of efavirenz primary and secondary metabolism: implication for HIV/AIDS therapy and utility of efavirenz as a substrate marker of CYP2B6 catalytic activity. J. Pharmacol. Exp. Ther. 306, 287–300. doi: 10.1124/jpet.103.049601
Ward, D. J., and Curtin, J. M. (2006). Switch from efavirenz to nevirapine associated with resolution of efavirenz-related neuropsychiatric adverse events and improvement in lipid profiles. AIDS Patient Care STDS 20, 542–548. doi: 10.1089/apc.2006.20.542
Wyen, C., Hendra, H., Siccardi, M., Platten, M., Jaeger, H., Harrer, T., et al. (2011). Cytochrome P450 2B6 (CYP2B6) and constitutive androstane receptor (CAR) polymorphisms are associated with early discontinuation of efavirenz-containing regimens. J. Antimicrob. Chemother. 66, 2092–2098. doi: 10.1093/jac/dkr272
Wyen, C., Hendra, H., Vogel, M., Hoffmann, C., Knechten, H., Brockmeyer, N. H., et al. (2008). Impact of CYP2B6 983T>C polymorphism on non-nucleoside reverse transcriptase inhibitor plasma concentrations in HIV-infected patients. J. Antimicrob. Chemother. 61, 914–918. doi: 10.1093/jac/dkn029
Zhang, W. X., Chen, B., Jin, Z., Yu, Z., Wang, X., Chen, H., et al. (2008). Influence of uridine diphosphate (UDP)-glucuronosyltransferases and ABCC2 genetic polymorphisms on the pharmacokinetics of mycophenolic acid and its metabolites in Chinese renal transplant recipients. Xenobiotica 38, 1422–1436. doi: 10.1080/00498250802488585
Keywords: 3′-UTR, efavirenz, HIV/AIDS, pharmacogenetics, sensitivity, single nucleotide polymorphism, specificity, South Africa
Citation: Swart M, Evans J, Skelton M, Castel S, Wiesner L, Smith PJ and Dandara C (2016) An Expanded Analysis of Pharmacogenetics Determinants of Efavirenz Response that Includes 3′-UTR Single Nucleotide Polymorphisms among Black South African HIV/AIDS Patients. Front. Genet. 6:356. doi: 10.3389/fgene.2015.00356
Received: 29 October 2015; Accepted: 10 December 2015;
Published: 07 January 2016.
Edited by:
Guilherme Suarez-Kurtz, Instituto Nacional de Cancer, BrazilReviewed by:
Eleni Aklillu, Karolinska Institute, SwedenCopyright © 2016 Swart, Evans, Skelton, Castel, Wiesner, Smith and Dandara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Collet Dandara, Y29sbGV0LmRhbmRhcmFAdWN0LmFjLnph
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.