 Ry Yves Tweedie-Cullen1
Ry Yves Tweedie-Cullen1 Brooke C. Wilson1
Brooke C. Wilson1 José G. B. Derraik1,2
José G. B. Derraik1,2 Benjamin B. Albert1,3
Benjamin B. Albert1,3 Keri Opai4
Keri Opai4 Taygen Edwards1
Taygen Edwards1 Justin M. O’Sullivan1,5
Justin M. O’Sullivan1,5 Wayne S. Cutfield1,3*
Wayne S. Cutfield1,3*- 1Liggins Institute, University of Auckland, Auckland, New Zealand
- 2Department of Paediatrics, Child and Youth Health, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand
- 3A Better Start, National Science Challenge, University of Auckland, Auckland, New Zealand
- 4Tui Ora, New Plymouth, Taranaki, New Zealand
- 5The Maurice Wilkins Centre, University of Auckland, Auckland, New Zealand
Introduction: Gut microbiome transfer (GMT or faecal microbiome transfer) is gaining increasing attention as a potential treatment for a range of medical conditions. However, public awareness and acceptance are not well understood.
Methods: To better understand the public perception of microbiome transfer in New Zealand, we undertook a nationwide online survey. The anonymous survey was designed and distributed between 2022-2023. Inclusion criteria included being aged 16 years or older and a resident of New Zealand. Distribution channels included social media advertising, posters in public areas, e-mail newsletters, and a survey facilitation company.
Results: A total of 2441 completed surveys were analyzed. Most respondents (71%) had tertiary education, 59% were female, with 62% identifying as NZ European, 12% as Māori, and 3% as Pacific peoples. The findings identified a high level of awareness and acceptability, with 76% of respondents having heard of GMT, and 96% indicating they would consider it if proven efficacious for a health condition they had. High levels of acceptance were observed across all ethnicities. Encapsulated oral FMT treatment was the preferred transfer method.
Discussion: Primary concerns related to GMT included the diet, health, and screening of stool donors, as well as the demonstration of safety and efficacy. These findings will help inform health professionals and researchers about the public’s needs and preferences regarding GMT.
Introduction
Faecal microbiome transfer (GMT), also known as faecal microbiota transplant, is a procedure that involves transferring the gut microbiome contained in healthy donor faeces to a recipient with a dysbiotic gut microbiome (1). GMT has been shown to be highly effective in resolving recurrent Clostridioides difficile infection (CDI) (2–4) —the most common pathogen responsible for bacteria-induced diarrhoea in hospitalised patients (5). CDI causes marked morbidity and mortality worldwide (6), and GMT can rapidly restore the diversity and functions of the gut microbiome curing clinical disease in these patients (7). GMT is currently the recommended treatment for patients with multiple CDI recurrences (2–4).
GMT has also been trialled as a potential therapy for disorders associated with less severe forms of gut dysbiosis than CDI, such as obesity (8–10), metabolic syndrome (11–14), inflammatory bowel disease (15, 16), irritable bowel syndrome (17), autism (18), and neuropsychiatric conditions (19, 20). Whilst GMT has not been demonstrated to cure these multi-faceted conditions, the resulting alterations in the gut microbiome have been associated with various therapeutic benefits among recipients, including improvements in metabolic syndrome and insulin sensitivity (10–12), intestinal permeability (21), gut inflammation (22), gastrointestinal symptoms (23), and social behaviours (24). As a result, the gut microbiome and GMT have been increasingly covered in the media (25–31), and high-rates of self-administration of GMT have been reported in some patient populations (25, 32).
Patients who received GMT for recurrent CDI have generally reported high levels of satisfaction and indicated it was their preferred treatment for the disease (33). Patients have noted rapid improvements in their symptoms following GMT, and side effects were not only uncommon but also mild and self-limiting (34). However, greater reservation amongst physicians has been noted due to concerns around the potential risks of adverse events, disease transmission, potential adverse alterations of the gut microbiome, the lack of evidence of efficacy, and a belief that patients will be averse to the aesthetics of GMT (34–39). This opinion is widely held amongst clinicians even though there have been few reports of serious GMT-associated adverse events (40). Despite reports of initial aversions to the concept of GMT, surveys to date showed that respondents are interested in learning more (38, 41, 42). Notably, CDI patients provided with efficacy data for their range of possible treatments, usually opted for GMT over other treatments (43). Thus, the concept of using faecal material as a treatment is not a deterrent for recipients (i.e. patients), although the acceptance of GMT depends on the context in which it is offered (38).
Respondents in previous surveys have reported concerns regarding GMT (41, 42, 44, 45), including fears of transmissible infections, the potential financial costs associated with what is portrayed as an experimental therapy, and questions regarding the screening of stool donors’ lifestyle and health status. Amongst specific patient populations, those with ulcerative colitis were reportedly concerned about screening for infections, cleanliness of the GMT procedure, and its efficacy (46, 47). However, when provided with supporting research information and evidence of appropriate donor selection and screening, these patients were willing to consider GMT as a treatment option (44, 48). Further, conditions associated with severe symptoms and lack of effective treatment options (e.g., recurrent CDI) have been shown to be powerful motivators for acceptance of alternative treatments such as GMT (49). However, some patients offered GMT have seen it as a treatment of last resort (41).
Previous surveys on the acceptability of GMT have typically been small or targeted specific populations (33, 36, 50). The largest published survey (n=1828) sampled Chinese medical students (36), and thus may not be broadly representative of wider opinions. Despite strong evidence supporting the efficacy and safety of GMT for CDI (17) and inclusion in treatment guidelines in some countries (3, 4), uptake has been variable (51). In spite of high levels of patient-reported satisfaction following GMT, reservations amongst physicians remains high with close to half of respondents in surveys of physicians expressing concerns, and/or would only considering GMT when traditional methods had been exhausted (34, 52).
Importantly, it is essential to understand the public’s views and potential acceptability of microbiome-related therapies. Identifying ethical, social, and/or cultural issues that may act as barriers or facilitators to GMT acceptability is critical for the design and testing of GMT therapies (42, 45, 46, 50).
Materials and methods
Respondent screening and survey design
The survey was designed and administered using an online platform (Qualtrics Labs Inc., Provo, UT, USA). The questionnaire was anonymous, and no personally identifiable information was collected. Potential participants were first screened for the inclusion criteria (age ≥16 years and current residence in New Zealand), and respondents not meeting these criteria were unable to proceed further. Conversely, those meeting the study criteria were then provided with a brief explanation about the study and the type of data being collected (see Supplementary Table 1) and given access to a participant information sheet.
The questionnaire comprised 18 questions (see Supplementary Table 1), and respondents were not obliged to answer every question. Some questions were associated with a branching logic (specifically Q7/9/11/12/13/17/18), so that certain questions were displayed or not depending on the respondent’s answer. Multiple choice or ranked questions (e.g. Q14) were presented to each respondent in a random order to each respondent to avoid presentation bias.
Demographic data recorded included the participant’s gender, age range, highest completed qualification, and ethnicity. The latter was self-reported, and the respective question allowed respondents to choose multiple ethnicities. However, respondents were allocated to a single prioritised ethnicity using the NZ Ministry of Health hierarchical system of classification (53) as follows: Māori, Pacific Peoples, European, Chinese, Indian, Other Asian, “MEELA” (Middle Eastern, Latin American, or African) and New Zealand European.
Survey distribution
The survey was carried out over 5 months (September 2022 until January 2023) with a link distributed through a range of channels. These included targeted advertisements (based on geography, age, or gender) on Facebook and Instagram, e-mail newsletters sent out within the University of Auckland, posters displayed in public areas throughout New Zealand, and through distribution of physical flyers to letterboxes. To ensure we had a more balanced ethnic, gender and educational background of respondents, an additional 200 paid responses were provided by a survey facilitation company (Dynata LLC, New Zealand branch).
Quantitative analyses
Only data on submitted surveys underwent quantitative analyses. Data were analysed using SAS (v9.4, SAS Institute Inc., Cary, NC, USA) and Prism (v.9.5.1, GraphPad Software, San Diego, California USA). All tests were two-tailed and statistical significance set at p<0.05). “The likelihood of a binary outcome (e.g., answering “Yes” to a given question) was examined using multivariable generalized linear regression models based on a Poisson distribution, with effect sizes expressed as the adjusted relative risks (aRR) and respective 95% confidence intervals (CI). Models adjusted for the participant’s age band and level of education (both as ranked continuous variables), as well as gut issues and IBD (both coded as either “yes” or “no” for each respondent).
Thematic analyses
Five questions allowed respondents to provide free text responses (see Supplementary Table 1): Q11, Q12, Q13, Q17 and Q18. Reflexive thematic analyses (54) were performed on these free text responses using NVivo (v20.7.1, QSR International Pty Ltd., MA, USA). Q13 was excluded for having only three responses recorded.
Ethics
Ethics approval was granted by the University of Auckland Human Participants Ethics Committee (UAHPEC24594). Informed consent was only deemed as provided when respondents began the survey.
Results
Survey respondents
A total of 2441 submitted surveys were analysed. Responses were received from a diverse range of respondents in terms of gender, age, ethnicity, and highest educational level achieved (see Table 1). The majority of respondents (63%) rated their health as good to excellent, and 8% as poor or very poor. Most respondents who had underlying medical conditions self-rated these as mild or moderate (see Supplementary Figure 1).
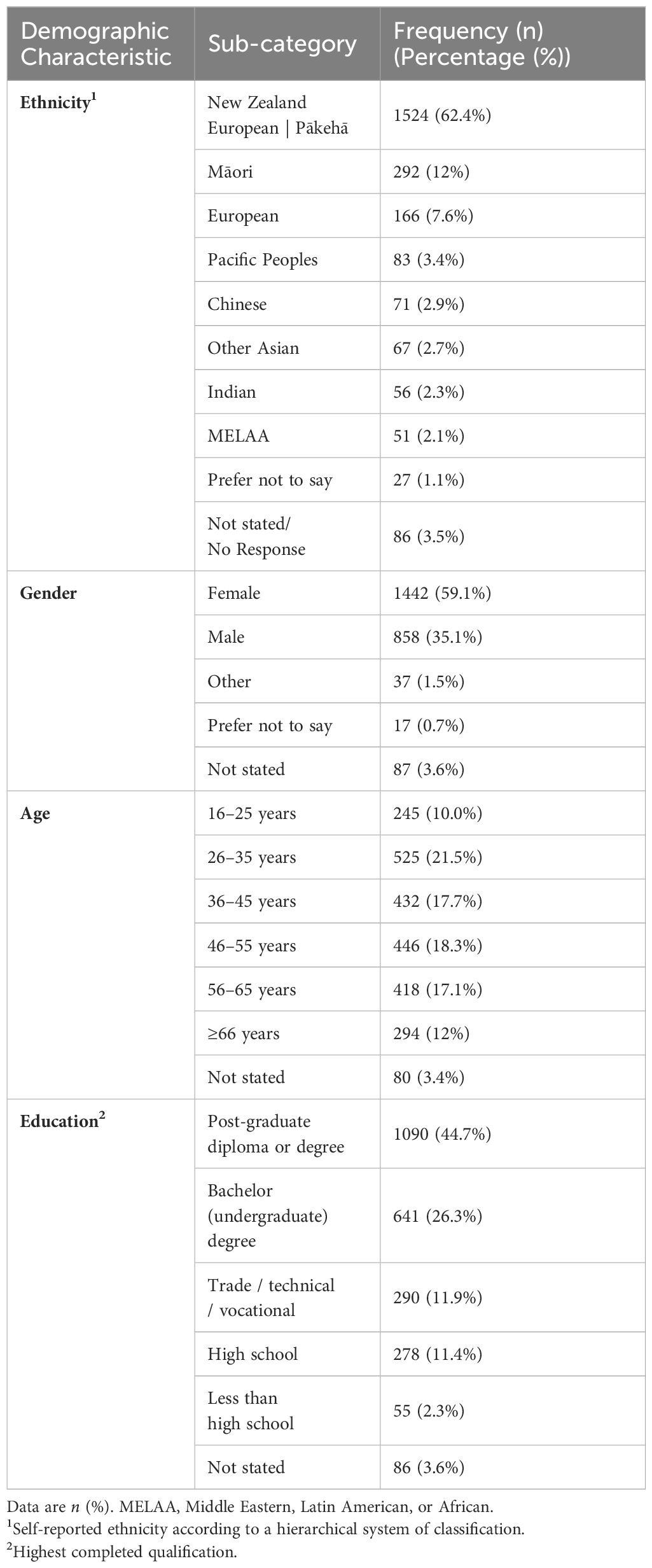
Table 1 Demographic characteristics of 2441 respondents of a nationwide online survey on GMT knowledge and acceptance.
Awareness of GMT
Awareness of GMT was high with 76% of respondents having heard of GMT previously (see Figure 1A). Respondents in this group also reported high knowledge with only 5% knowing “nothing at all”, and 32% “knowing a lot” or “a moderate amount”. Higher education level and greater age were associated with awareness of GMT (p<0.001 for both). Of those with a bachelor’s or post-graduate degree, 83% were aware of GMT versus only 34% of those without (see Figures 1A–C).

Figure 1 Awareness of GMT amongst survey respondents. (A) Overall awareness of GMT; (B) Knowledge of GMT amongst those reporting awareness of it; (C) GMT awareness in association with the respondent's highest level of education.
Willingness to undergo GMT
After being presented with a brief overview of GMT, respondents were asked if they would consider undergoing the procedure if proven effective for a health condition affecting them. Almost all (95%) were receptive to undergoing GMT if it could effectively treat their condition, with 73% and 22% responding “yes” or “maybe”, respectively (Figure 2A). Although receptiveness to GMT was high overall, there was greater willingness towards GMT amongst the highly educated respondents (p<0.001; Figure 2B). No association was observed between overall reported health status or illness severity and willingness to undergo an GMT (see Supplementary Figure 1) (p=0.32). However, those reporting gut issues were more willing to undergo GMT than those without (p<0.001).
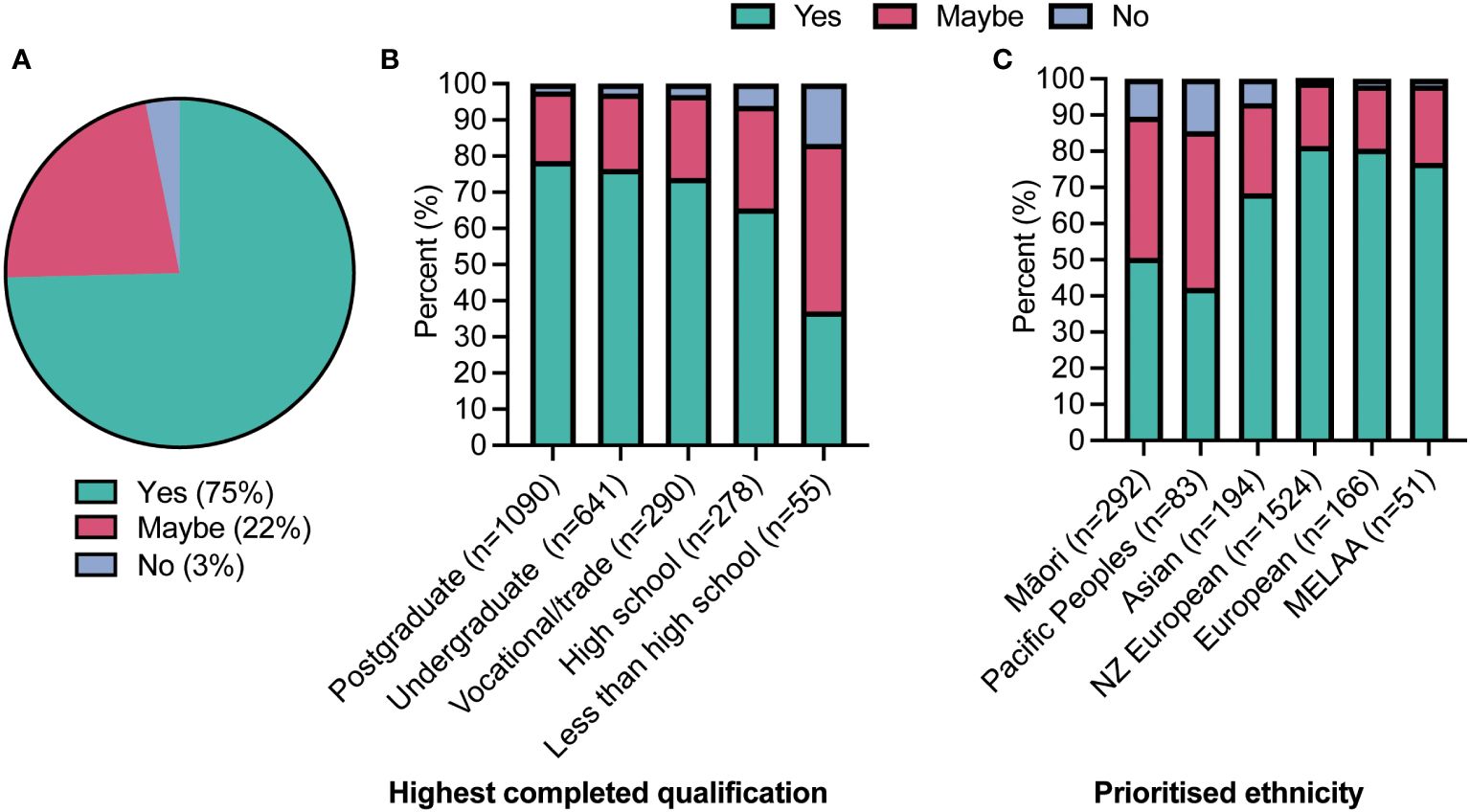
Figure 2 The willingness of respondents to undergo faecal microbiome transfer (GMT). (A) If GMT was proven effective for a condition they had; (B) According to their highest level of education (p<0.0001 from a Chi-square test); and (C) according to their prioritised ethnicity (p<0.0001).
Acceptability amongst Māori (indigenous peoples) was similarly high, with 90% being receptive (“yes” or “maybe”) to GMT if it was appropriate. A similar pattern was seen amongst Pacific Peoples, with 85% being open to GMT. However, slightly more respondents from both these groups were more likely to select “no” when asked whether they would undergo an GMT, compared to other ethnic groups surveyed (p<0.001) (see Figure 2C). Importantly this difference remained when taking into account education levels, age, and the presence of gut issues (p<0.05). When queried on “Cultural or religious values that would affect your decision?” only three responses were received which mentioned spiritual beliefs.
Those respondents who would “maybe” consider undergoing GMT (22%) were asked a follow-up question regarding what information would help their decision-making process. The three most reported responses to this were the strength of the evidence of GMT effectiveness (81%), the severity of their health issue (69%), and the other treatment options available (60%) (see Figure 3). Notably, social/cultural acceptance (i.e., “What others in my whānau/family thought about it”) was only chosen by 11% of respondents. A qualitative analysis of the 47 free text answers to this question demonstrated themes related to worries about potential side effects, safety, and efficacy. They also showed concerns regarding the transfer of undiagnosed conditions and overcoming discomfort with ingesting faecal matter. Safety concerns encompassed the presence of “unhealthy bacteria” and the donor’s health. Respondents favoured capsules for delivery and emphasised understanding the source and processing of donor stool.
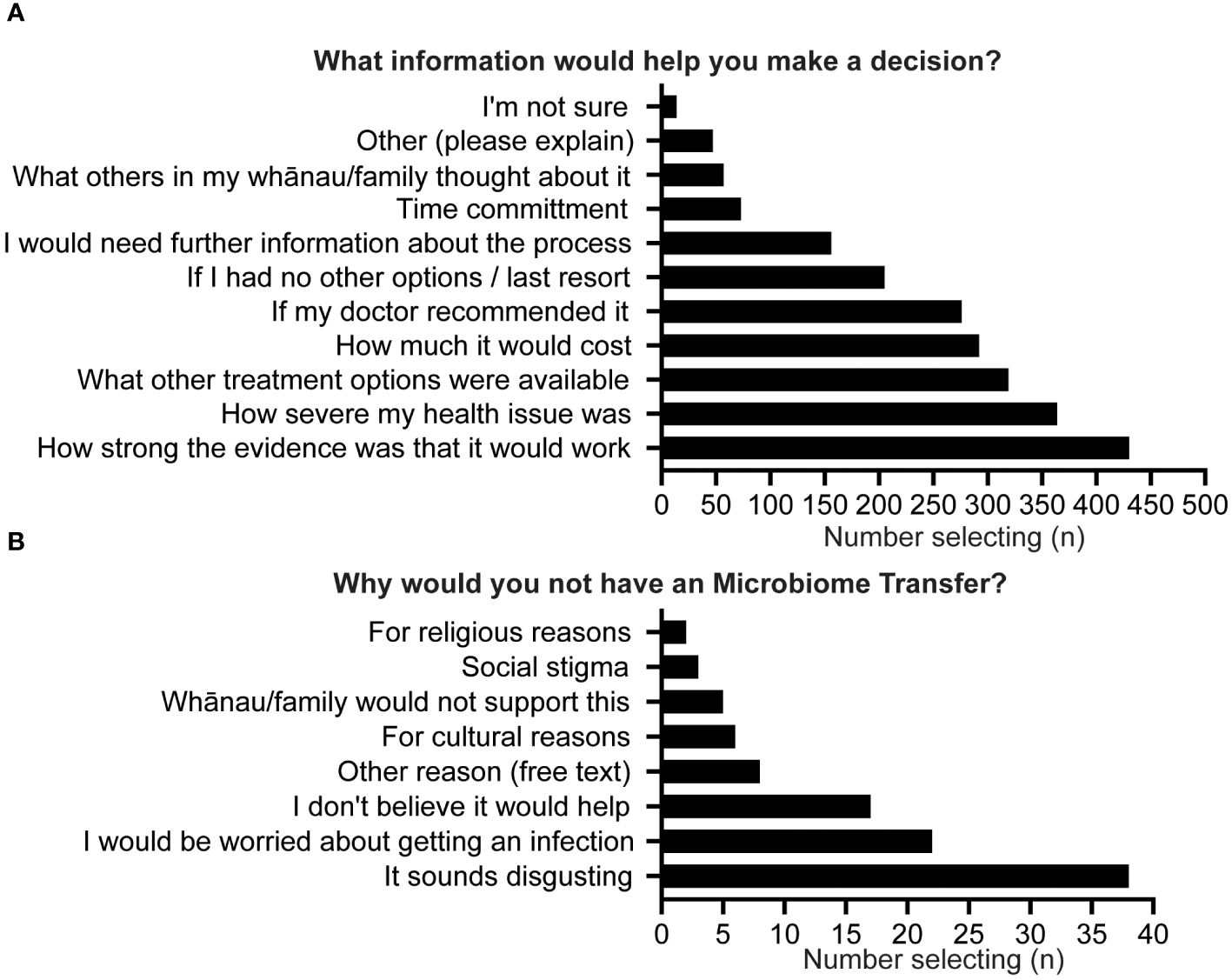
Figure 3 (A) What information would help you decide; (B) Why would you not have an GMT.
The 3% of respondents who would not undergo GMT were asked a follow-up question about their reasoning. Half selected “It sounds disgusting” as a justification; 29% reported concerns about the risk of infection, while 23% of respondents did not believe GMT would be effective (see Figure 3B). A qualitative analysis of 14 free text responses to this question covered themes related to personal dietary preferences, with some individuals hesitant due to donor diet. Others cited the personal absence of any health conditions, an aversion or discomfort with the concept, and a lack of familiarity with GMT. Scepticism about the effectiveness of microbiome transfers for chronic illnesses was mentioned, as was a preference for natural approaches to microbiome health. Safety and potential side effects were also raised as concerns, with respondents indicating a need for proof of safety before considering such a procedure.
Administration routes
When survey respondents ranked their preferred method of GMT, a significant majority ranked capsules as their first choice (72%). In contrast, only 11% preferred enema, 11% lower endoscopy, and 6% upper endoscopy (p<0.0001) (see Figure 4D).
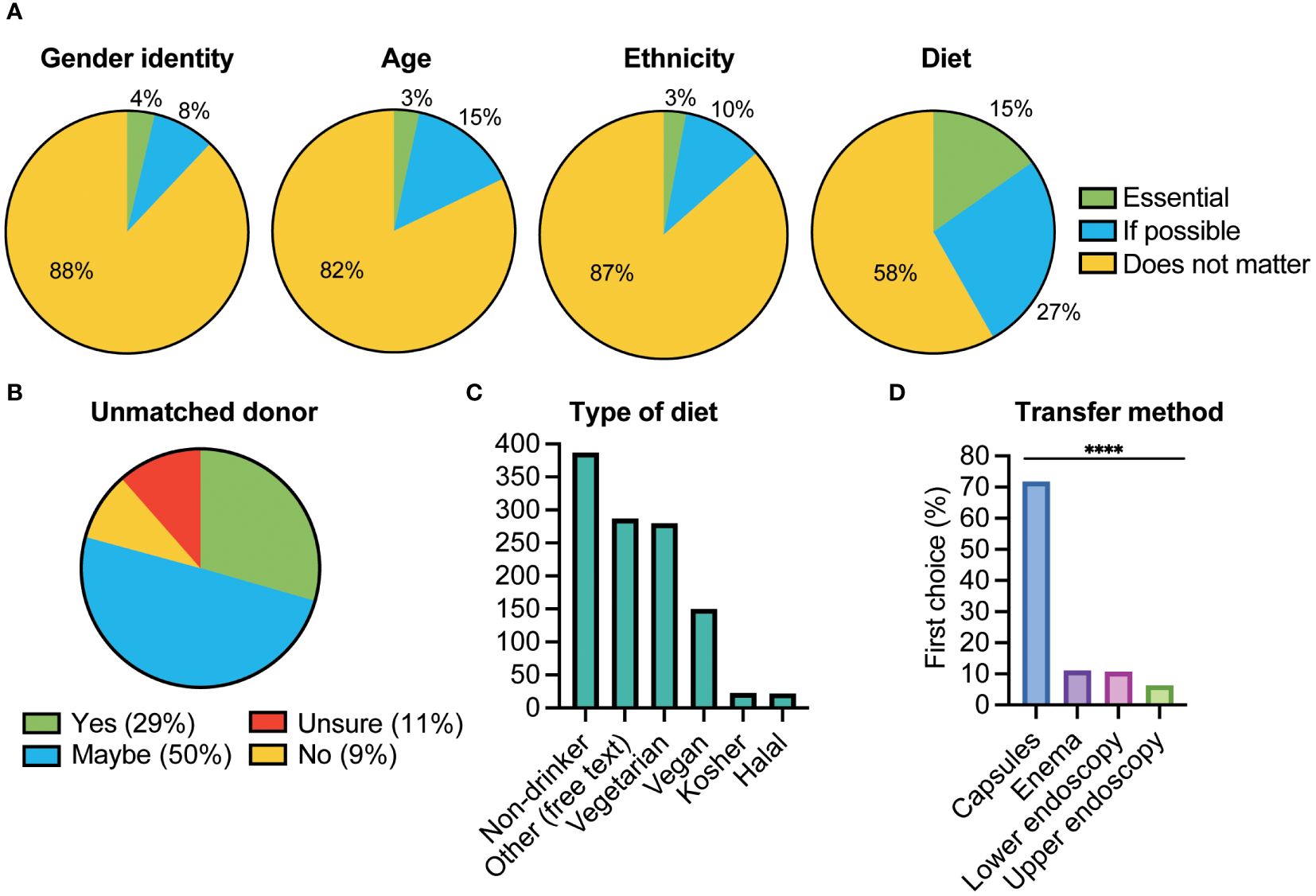
Figure 4 Donor preferences and administration route. (A) Respondents were asked whether it was “essential”, “if possible” or did not matter” regarding matching themselves with a potential stool donor in terms of Gender identity, Age, Ethnicity, or Diet; (B) Whether they would still accept an GMT from an unmatched donor; (C) What preferences they had in terms of their donor’s diet. Other refers to free text responses that respondents could enter; (D) Respondents were asked to rank the four alternatives 1-4, the percentage ranking each option as their first choice is shown. There was a significant difference between the four options with GMT being delivered via capsule the preferred option (****p <0.0001).
Donor preferences
Amongst respondents willing to undergo GMT, the primary concern was that donors would be “healthy and appropriate” (71%). Approximately 1 in 4 (27%) would prefer anonymous donors, but only 6% preferred donors they knew. Respondents were also asked about the importance of having stool donors ‘matching’ their preferences on “gender identity”, “age”, “ethnicity,” or “diet”. A significant proportion (p<0.001) of respondents expressed that it was either “essential” (15%) or “if possible” (27%) to be matched based on diet (see Figure 4A). Only 3% of respondents indicated that it was essential to be matched on the other characteristics (ethnicity 3%, age 3%, gender 4%). Primary dietary preferences included being a non-alcoholic drinker and having a vegetarian or vegan diet (280 and 150 respondents respectively) (see Figure 4C). A total of 281 free text answers to this question were recorded. A qualitative thematic analysis of respondents’ preferences for the donor’s diet revealed a variety of expectations. Themes included a desire for a healthy diet, emphasising factors like vegetables, low fat, low sugar, and whole foods. Respondents mentioned avoiding processed foods, alcohol, smoking, and illicit drugs as important criteria. Some emphasised the importance of dietary diversity, particularly a plant-based diet akin to the Mediterranean diet, for enhancing microbiome richness and resilience. Others indicated a preference for a donor with a diet similar or “compatible” to their own, citing personal taste and medical conditions, such as coeliac disease or food allergies.
Among the 462 respondents reporting at least one “essential” preference regarding stool donor characteristics, 79% remained open to undergoing GMT even if donors didn’t match their preferences. Only 9% stated that they would refuse an GMT unless they could be matched with a donor who met their preference (see Figure 4B). A total of 10 respondents gave free text answers as to this question, a qualitative analysis demonstrated that respondents prioritised medical advice, treatment effectiveness, personal preferences (such diet and lifestyle), and drew parallels to blood transfusions.
Discussion
This large nationwide survey of adults in New Zealand found a high level of awareness of GMT and a striking level of acceptability and willingness to undergo GMT if it could be of clinical value. Of those unwilling to undergo GMT, some of their concerns could likely be addressed, albeit technically challenging, by donor-recipient diet matching. Respondents raised the importance of support from their physician, and the need for evidence of safety and clinical efficacy in considering its use for their medical condition/s. Whilst most respondents had minimal expectations of donors, some specified the need for considerations such as diet and health. The high level of awareness seen in our survey can likely be attributed to the increasing attention beyond medical literature (e.g. online and in traditional media) directed at the more health literate (27–29, 39) and recent surveys have also shown a rise in awareness (39, 55).
Cultural and religious aspects of GMT have been examined in previous studies (44, 56), identifying concerns in terms of informed consent, specifically regarding recipients being aware of the donor’s diet, alcohol intake, and religion (56). Our study indicated that Māori showed were more likely to decline or express uncertainty about GMT compared to most ethnic groups, excluding Pacific Peoples. This reluctance may be attributed to historical and cultural factors, institutional bias and discrimination, socioeconomic disparities, health literacy, and a lack of cultural safety and representation in healthcare (57). These factors may ultimately lead to mistrust, limited access, and inadequate culturally appropriate care for Māori. Addressing these issues requires comprehensive approaches that prioritise cultural safety, equitable access, and inclusion of Māori voices in healthcare decision-making.
The survey indicated that most respondents preferred oral encapsulated GMT compared to other delivery methods. Previous studies have primarily focused on nasogastric, upper/lower endoscopy, or enema (44, 47, 49, 50), but when given the choice, patients generally prefer capsules, perceiving it to be more acceptable and less unpleasant (43, 46, 55, 58). For instance, a higher proportion of patients receiving GMT via capsules reported their experience as “not at all unpleasant” compared to those undergoing colonoscopy (59). Encapsulated GMT offers additional benefits such as being non-invasive, easier to deliver, carrying a lower risk of procedure-related complications, and not requiring sedation or anaesthesia. Meta-analyses have shown that encapsulated GMT is comparable to other methods in terms of clinical outcomes for CDI (17, 60). Moreover, its ability to be self-administered in a clinic or at home enhances convenience and accessibility.
At present GMT is performed using stool from a human donor (15). The donor health status (including colonisation by pathogens) is important when considering GMT, necessitating stringent testing of any potential donor (3, 15, 61–64). Patient views on the selection of stool donors have been explored in previous research and demonstrated that major concerns from potential recipients relate to donor selection and screening (44, 45, 52, 65). In our study, respondents emphasised having knowledge of the source of faecal matter, what donor health checks were undertaken, and assurance regarding the possible transfer of harmful pathogens. Most preferred a donor with a healthy, vegetable-rich diet, limited alcohol intake, and non-smoking habits, similar to perspectives reported previously (56). Although many were indifferent to the diet of a healthy donor, some preferred donors with diets similar to their own, such as vegetarian or vegan (see Figure 4C). The responses underscore an interest in the donor’s health, diet and facilitation of diet matching was indicated as essential for a small number of respondents (see Figure 4B). In agreement with previous research, this survey demonstrated that many people compare GMT to a blood transfusion (44, 49) supporting this being an generally acceptable approach in the future (66).
We additionally wanted to explore whether involvement in donor selection would be a facilitator or barrier to the adoption of GMT and what other selection criteria were important. Most respondents would prefer a “healthy and appropriate donor” and/or a preference for an anonymous donor, with a smaller proportion (6%) preferring a donor whom they knew. This is in line with previous studies, for instance, a survey of 183 GMT-naïve patients reported that 28% of patients found the prospect of needing to select their own donor as too unappealing to consider GMT as a treatment with all respondents preferring an unrelated anonymous donor (43). Other studies have also demonstrated that patients preferred their doctor to decide on the appropriate stool donor/s (47, 55). Conversely, some studies have also reported that many respondents (38-80%) would prefer to have a family member/spouse as their donor (45, 47, 49).
Both higher levels of education and older age were associated with greater awareness and willingness to undergo GMT amongst our respondents, consistent with previous research (33, 43). Education has previously been demonstrated as a key determinant of health literacy and engagement (67). The high proportion of respondents with a vocational or higher education (83%) could indicate a greater familiarity with the science behind GMT, leading to a better understanding of its potential benefits and risks. In addition, higher levels of education have been shown to increases the likelihood of trusting medical professionals and research (67). Older individuals may also be more accepting due to experience with chronic gastrointestinal disorders. Further, studies have also demonstrated an association between education levels and knowledge about and utilisation of complementary and alternative medicine (44, 68). Many survey respondents associated GMT as a “natural” therapy, which made them more receptive to it. This perception of GMT as a natural treatment aligns with previous observations comparing GMT and probiotics, which were also considered attractive due to their perceived natural or holistic nature (38, 41, 42, 44). Conversely, younger individuals may be less accepting of GMT due to limited exposure, fewer chronic issues, and perceived social stigma relating to its unconventional nature (41).
In our survey we saw no association between overall self-reported health status and willingness to undergo GMT (see Supplementary Figure 1). However, those respondents who reported having “gut issues” were more willing to undergo an GMT than those without. The perceived severity of the health condition that could be treated by the GMT has previously been shown to increase acceptance (44). For instance, 89% of people with well-controlled ulcerative colitis (85/95) were either willing or would maybe undergo GMT, with only 11% being unwilling, in addition previous hospitalisation for their condition was linked to increased willingness (47). Further, whilst initial distaste has frequently been reported as a barrier to GMT, disease burden, perceived benefits, and desire for an effective treatment have all been shown to be greater motivating factors (33, 44). Patients with CDI had higher willingness to undergo GMT than healthy controls, with greater willingness in those with multiple episodes of CDI (69). In addition, patients in previous surveys with chronic gastrointestinal disorders were likely more willing to try GMT if they perceived their current treatments as ineffective or unsatisfactory (41).
Respondents in our study emphasised the need to understand the safety, efficacy, and potential complications of GMT. Amongst those unwilling to undergo an GMT, the primary reasons were due to concerns about ingesting faecal matter or lack of perceived benefit. Similarly, research has shown that a large portion of physicians are reluctant to recommend GMT (4, 34, 52) due to concerns about long-term safety (38, 70, 71), the potential impacts of altering the gut microbiome (26, 28–31), and lack of clinical utility beyond CDI. For our respondents, the doctor-patient relationship and medical advice were crucial for acceptance of GMT, aligning with previous research (44). Whilst many prioritised medical advice, personal preferences and specific medical conditions also influenced their decisions, in line with findings from earlier studies (41, 43).
There are several limitations associated with this study. Firstly, the respondents in the study were primarily individuals with a higher level of education. However, the willingness to participate in the study was relatively similar across different education levels beyond high school/college. Furthermore, the study was conducted in New Zealand, which may affect the generalisability of the findings to an international context. Nevertheless, most respondents were of European descent (New Zealand European/Pākehā), increasing the relevance of the results to other Western countries with similar demographic profiles. It should be noted that although the respondents did not fully represent the ethnic diversity of New Zealand, the sample size was adequate to detect any potential ethnic differences in willingness to undergo GMT. Notably, this study is one of the largest conducted on this topic to date and additionally, it diverged from prior research that has targeted specific subgroups, such as patients with chronic gut issues or medical students, by instead surveying the general public.
This survey gives new insights into the views and attitudes of the public in New Zealand and has implications for the possible future development and application of GMT as a therapeutic modality if utility beyond CDI can be demonstrated. Whilst the survey demonstrated both high awareness and willingness regarding GMT, this contrasts with greater reservations amongst physician and demonstrates a need for greater education, research, and communication efforts to better inform clinicians and the public about GMT to address concerns and misconceptions. It also indicates that there may be segments of the population for which the design and delivery of personalised and patient centred GMT interventions are warranted. Ultimately, greater availability of GMT is dependent not only on institutional acceptance and provision but also demonstration of clinical utility and efficacy.
Data availability statement
Anonymous respondent response data will be made available at date of publication upon valid requests to the Liggins Institute’s Data Oversight Committee. Requestors will need to provide a methodologically sound proposal, obtain appropriate ethical approval, and sign a Data Access Agreement. The data access agreement will include a commitment to using the data only for the specified proposal, not to attempt to identify any individual respondent, a commitment to secure storage and use of data, and to destroy or return the data after completion of the project.
Ethics statement
The studies involving humans were approved by the University of Auckland Human Participants Ethics Committee (UAHPEC24594). Informed consent was only deemed as provided when respondents began the survey. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RT: Writing – original draft, Writing – review & editing. BW: Writing – review & editing. JD: Writing – review & editing. BA: Writing – review & editing. KO: Writing – review & editing. TE: Writing – review & editing. JO’S: Writing – review & editing. WC: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by a Philanthropic grant from the Rockfield Trust. The funders had no involvement in the design of the study, or involvement in the collection, analyses, interpretation of data or in the writing and decision to publish.
Acknowledgments
Dr Sophie Farrow and Dr Farha Ramzan for assistance with distribution of the survey.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgstr.2024.1411898/full#supplementary-material
Supplementary Figure 1 | (A) Self-reported and self-scored condition severity. Each column represents the individuals who reported they had a specific condition and their proportional severity rating; (B) Overall self-rated health; (C) There was no significant difference regarding willingness of people to undergo GMT who either reported no health conditions, or rated at least one severe, moderate, or mild; (D) Willingness to undergo an GMT and overall self-reported health, ns.
References
1. Lavelle A, Sokol H. Understanding and predicting the efficacy of FMT. Nat Med. (2022) 28:1759–60. doi: 10.1038/s41591-022-01991-0
2. Cammarota G, Ianiro G, Gasbarrini A. Fecal microbiota transplantation for the treatment of clostridium difficile infection: A systematic review. J Clin Gastroenterol. (2014) 48:693. doi: 10.1097/MCG.0000000000000046
3. Sokol H, Galperine T, Kapel N, Bourlioux P, Seksik P, Barbut F, et al. Faecal microbiota transplantation in recurrent Clostridium difficile infection: Recommendations from the French Group of Faecal microbiota Transplantation. Dig Liver Dis. (2016) 48:242–7. doi: 10.1016/j.dld.2015.08.017
4. Trubiano JA, Cheng AC, Korman TM, Roder C, Campbell A, May MLA, et al. Australasian Society of Infectious Diseases updated guidelines for the management of Clostridium difficile infection in adults and children in Australia and New Zealand: CDI management guidelines. Intern Med J. (2016) 46:479–93. doi: 10.1111/imj.13027
5. Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. Multistate point-prevalence survey of health care–associated infections. N Engl J Med. (2014) 370:1198–208. doi: 10.1056/NEJMoa1306801
6. Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. (2015) 372:1539–48. doi: 10.1056/NEJMra1403772
7. Borgia G, Maraolo AE, Foggia M, Buonomo AR, Gentile I. Fecal microbiota transplantation for Clostridium difficile infection: back to the future. Expert Opin Biol Ther. (2015) 15:1001–14. doi: 10.1517/14712598.2015.1045872
8. Yu EW, Gao L, Stastka P, Cheney MC, Mahabamunuge J, Torres Soto M, et al. Fecal microbiota transplantation for the improvement of metabolism in obesity: The FMT-TRIM double-blind placebo-controlled pilot trial. Basu S editor. PloS Med. (2020) 17:e1003051. doi: 10.1371/journal.pmed.1003051
9. Allegretti JR, Kassam Z, Hurtado J, Marchesi JR, Mullish BH, Chiang A, et al. Impact of fecal microbiota transplantation with capsules on the prevention of metabolic syndrome among patients with obesity. Hormones. (2021) 20:209–11. doi: 10.1007/s42000-020-00265-z
10. Leong KSW, Jayasinghe TN, Wilson BC, Derraik JGB, Albert BB, Chiavaroli V, et al. Effects of fecal microbiome transfer in adolescents with obesity: the gut bugs randomized controlled trial. JAMA Netw Open. (2020) 3:e2030415. doi: 10.1001/jamanetworkopen.2020.30415
11. Vrieze A, Van Nood E, Holleman F, Salojärvi J, Kootte RS, Bartelsman JFWM, et al. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology. (2012) 143:913–6.e7. doi: 10.1053/j.gastro.2012.06.031
12. Kootte RS, Levin E, Salojärvi J, Smits LP, Hartstra AV, Udayappan SD, et al. Improvement of insulin sensitivity after lean donor feces in metabolic syndrome is driven by baseline intestinal microbiota composition. Cell Metab. (2017) 26:611–9.e6. doi: 10.1016/j.cmet.2017.09.008
13. Smits LP, Kootte RS, Levin E, Prodan A, Fuentes S, Zoetendal EG, et al. Effect of vegan fecal microbiota transplantation on carnitine- and choline-derived trimethylamine-N-oxide production and vascular inflammation in patients with metabolic syndrome. J Am Heart Assoc. (2018) 7:e008342. doi: 10.1161/JAHA.117.008342
14. de Groot P, Scheithauer T, Bakker GJ, Prodan A, Levin E, Khan MT, et al. Donor metabolic characteristics drive effects of faecal microbiota transplantation on recipient insulin sensitivity, energy expenditure and intestinal transit time. Gut. (2019) 69:502–12. doi: 10.1136/gutjnl-2019-318320
15. Bibbò S, Settanni CR, Porcari S, Bocchino E, Ianiro G, Cammarota G, et al. Fecal microbiota transplantation: screening and selection to choose the optimal donor. J Clin Med. (2020) 9:1757. doi: 10.3390/jcm9061757
16. Paramsothy S, Paramsothy R, Rubin DT, Kamm MA, Kaakoush NO, Mitchell HM, et al. Faecal microbiota transplantation for inflammatory bowel disease: a systematic review and meta-analysis. J Crohns Colitis. (2017) 11:1180–99. doi: 10.1093/ecco-jcc/jjx063
17. Ianiro G, Eusebi LH, Black CJ, Gasbarrini A, Cammarota G, Ford AC. Systematic review with meta-analysis: efficacy of faecal microbiota transplantation for the treatment of irritable bowel syndrome. Alimentary Pharmacol Ther. (2019) 50:240–8. doi: 10.1111/apt.15330
18. Fattorusso A, Di Genova L, Dell’isola GB, Mencaroni E, Esposito S. Autism spectrum disorders and the gut microbiota. Nutrients. (2019) 11:521. doi: 10.3390/nu11030521
19. Diaz Heijtz R, Gressens P, Swann JR. Targeting microbial metabolites to treat autism. Nat Med. (2022) 28(3):448–50. doi: 10.1038/s41591-022-01711-8
20. De Clercq NC, Frissen MN, Davids M, Groen AK, Nieuwdorp M. Weight Gain after Fecal Microbiota Transplantation in a Patient with Recurrent Underweight following Clinical Recovery from Anorexia Nervosa. Psychother Psychosom. (2019) 88:52–4. doi: 10.1159/000495044
21. Craven L, Rahman A, Nair Parvathy S, Beaton M, Silverman J, Qumosani K, et al. Allogenic fecal microbiota transplantation in patients with nonalcoholic fatty liver disease improves abnormal small intestinal permeability: a randomized control trial. Am J Gastroenterol. (2020) 115:1055–65. doi: 10.14309/ajg.0000000000000661
22. Paramsothy S, Kamm MA, Kaakoush NO, Walsh AJ, van den Bogaerde J, Samuel D, et al. Multidonor intensive faecal microbiota transplantation for active ulcerative colitis: a randomised placebo-controlled trial. Lancet. (2017) 389:1218–28. doi: 10.1016/S0140-6736(17)30182-4
23. Tian H, Ge X, Nie Y, Yang L, Ding C, McFarland LV, et al. Fecal microbiota transplantation in patients with slow-transit constipation: a randomized, clinical trial. PloS One. (2017) 12:e0171308. doi: 10.1371/journal.pone.0171308
24. Kang DW, Adams JB, Gregory AC, Borody T, Chittick L, Fasano A, et al. Microbiota transfer therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome. (2017) 5:10. doi: 10.1186/s40168-016-0225-7
25. Ekekezie C, Perler BK, Wexler A, Duff C, Lillis CJ, Kelly CR. Understanding the scope of do-it-yourself fecal microbiota transplant. Am J Gastroenterol. (2020) 115:603–7. doi: 10.14309/ajg.0000000000000499
26. Marcon AR, Turvey S, Caulfield T. ‘Gut health’ and the microbiome in the popular press: a content analysis. BMJ Open. (2021) 11:e052446. doi: 10.1136/bmjopen-2021-052446
27. Sample I. What are the real signs of a healthy gut? A user’s guide. Guardian. (2023) Available at: https://www.theguardian.com/lifeandstyle/2023/mar/18/what-are-the-real-signs-of-a-healthy-gut-a-users-guide.
28. McLeod C, Nerlich B, Jaspal R. Fecal microbiota transplants: emerging social representations in the English-language print media. New Genet Soc. (2019) 38:331–51. doi: 10.1080/14636778.2019.1637721
29. Davis N. Gut feelings: why drugs that nurture your microbes could be the future of mental health. Guardian. (2023) Available at: https://www.theguardian.com/lifeandstyle/2023/mar/21/gut-feelings-why-drugs-that-nurture-your-microbes-could-be-the-future-of-mental-health.
30. Chidambaram S, Maheswaran Y, Chan C, Hanna L, Ashrafian H, Markar S, et al. (Mis) Communicating The Gut Microbiome: A Cross-Sectional Assessment of Social Media Video Content. Public Global Health. (2022). doi: 10.1101/2022.01.16.22269387
31. Prados-Bo A, Casino G. How have quality newspapers covered the microbiome? A content analysis of The New York Times, The Times, and El País. Journalism. (2022) 24(8):1752–71. doi: 10.1177/14648849211067858
32. Bauer CM, Zhang X, Long MD, Sandler RS. Characteristics of fecal microbiota transplantation use in inflammatory bowel disease cohort. Crohns Colitis 360. (2020) 2:otaa024. doi: 10.1093/crocol/otaa024
33. Park L, Mone A, Price JC, Tzimas D, Hirsh J, Poles MA, et al. Perceptions of fecal microbiota transplantation for Clostridium difficile infection: Factors that predict acceptance. Ann Gastroenterol. (2017) 30:83–8. doi: 10.20524/aog.2016.0098
34. Gill M, Blacketer C, Chitti F, Telfer K, Papanicolas L, Dann LM, et al. Physician and patient perceptions of fecal microbiota transplant for recurrent or refractory Clostridioides difficile in the first 6 years of a central stool bank. JGH Open. (2020) 4:950–7. doi: 10.1002/jgh3.12396
35. Brandt LJ. Editorial commentary: Fecal microbiota transplantation: Patient and physician attitudes. Clin Infect Dis. (2012) 55:1659–60. doi: 10.1093/cid/cis812
36. Wu X, Dai M, Buch H, Bai J, Long W, Long C, et al. The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study. Ther Adv Gastroenterol. (2019) 12:1756284819869144. doi: 10.1177/1756284819869144
37. Ma Y, Yang J, Cui B, Xu H, Xiao C, Zhang F. How Chinese clinicians face ethical and social challenges in fecal microbiota transplantation: a questionnaire study. BMC Med Ethics. (2017) 18(1):39. doi: 10.1186/s12910-017-0200-2
38. Paramsothy S, Walsh AJ, Borody T, Samuel D, Van Den Bogaerde J, Leong RWL, et al. Gastroenterologist perceptions of faecal microbiota transplantation. World J Gastroenterol. (2015) 21:10907–14. doi: 10.3748/wjg.v21.i38.10907
39. Zhang Y, Xue X, Su S, Zhou H, Jin Y, Shi Y, et al. Patients and physicians’ attitudes change on fecal microbiota transplantation for inflammatory bowel disease over the past 3 years. Ann Transl Med. (2021) 9:1619–9. doi: 10.21037/atm
40. Kelly CR, Ihunnah C, Fischer M, Khoruts A, Surawicz C, Afzali A, et al. Fecal microbiota transplant for treatment of clostridium difficile infection in immunocompromised patients. Am J Gastroenterol. (2014) 109:1065–71. doi: 10.1038/ajg.2014.133
41. Chauhan U, Popov J, Farbod Y, Kalantar M, Wolfe M, Moayyedi P, et al. Fecal microbiota transplantation for the treatment of ulcerative colitis: A qualitative assessment of patient perceptions and experiences. J Can Assoc Gastroenterol. (2021) 4:e120–9. doi: 10.1093/jcag/gwab007
42. Chauhan U, Popov J, Kalantar M, Marshall J, Halder S, Wolfe M, et al. P018 understanding patients’ Perceptions of fecal microbiota transplant. Am J Gastroenterology. (2019) 114:S5–5. doi: 10.14309/01.ajg.0000613040.97231.4d
43. Zipursky JS, Sidorsky TI, Freedman CA, Sidorsky MN, Kirkland KB. Patient attitudes toward the use of fecal microbiota transplantation in the treatment of recurrent Clostridium difficile infection. Clin Infect Dis. (2012) 55:1652–8. doi: 10.1093/cid/cis809
44. Kahn SA, Gorawara-Bhat R, Rubin DT. Fecal bacteriotherapy for ulcerative colitis: Patients are ready, are we? Inflammation Bowel Dis. (2012) 18:676–84. doi: 10.1002/ibd.21775
45. Zeitz J, Bissig M, Barthel C, Biedermann L, Scharl S, Pohl D, et al. Patients’ views on fecal microbiota transplantation: an acceptable therapeutic option in inflammatory bowel disease? Eur J Gastroenterol Hepatol. (2017) 29:322. doi: 10.1097/MEG.0000000000000783
46. Schulte LA, Schäfer A, Steding K, Rauschek L, Klaus J. Acceptance of fecal microbiota transfer among patients with chronic inflammatory bowel diseases in a highly specialized outpatient department: a questionnaire-based survey. Z Gastroenterol. (2019) 57:1291–7. doi: 10.1055/a-1010-6920
47. Kahn SA, Vachon A, Rodriquez D, Goeppinger SR, Surma B, Marks J, et al. Patient perceptions of fecal microbiota transplantation for ulcerative colitis. Inflammation Bowel Dis. (2013) 19:1506–13. doi: 10.1097/MIB.0b013e318281f520
48. Green JE, Davis JA, Berk M, Hair C, Loughman A, Castle D, et al. Efficacy and safety of fecal microbiota transplantation for the treatment of diseases other than Clostridium difficile infection: a systematic review and meta-analysis. Gut Microbes. (2020) 12:1854640. doi: 10.1080/19490976.2020.1854640
49. Zellmer C, De Wolfe TJ, Van Hoof S, Blakney R, Safdar N. Patient perspectives on fecal microbiota transplantation for clostridium difficile infection. Infect Dis Ther. (2016) 5:155–64. doi: 10.1007/s40121-016-0106-1
50. Gundling F, Roggenbrod S, Schleifer S, Sohn M, Schepp W. Patient perception and approval of faecal microbiota transplantation (GMT) as an alternative treatment option for obesity. Obes Sci Pract. (2019) 5:68–74. doi: 10.1002/osp4.302
51. Quraishi MN, Segal J, Mullish B, McCune VL, Hawkey P, Colville A, et al. National survey of practice of faecal microbiota transplantation for Clostridium difficile infection in the UK. J Hosp Infect. (2017) 95:444–5. doi: 10.1016/j.jhin.2016.10.023
52. Gweon TG, Lee YJ, Yim SK, Kim SY, Choi CH, Cho YS, et al. Recognition and attitudes of Korean physicians toward fecal microbiota transplantation: a survey study. Korean J Intern Med. (2023) 38:48–55. doi: 10.3904/kjim.2022.206
53. HISO 10001: ethnicity data protocols (2017). Available online at: https://www.tewhatuora.govt.nz/our-health-system/digital-health/health-information-standards-2/approved-standards-2/identity-standards.
54. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
55. Roggenbrod S, Schuler C, Haller B, Sohn M, Storr M, Schepp W, et al. Akzeptanz des fäkalen Mikrobiota-Transfers (Stuhltransplantation) als alternative Therapie bei Patienten mit Colitis ulcerosa [Patient perception and approval of fecal microbiota transplantation (FMT) as an alternative treatment option for ulcerative colitis]. Z Gastroenterol. (2019) 57(3):296–303. German. doi: 10.1055/a-0821-7166
56. Al-Bakri AG, Akour AA, Al-Delaimy WK. Knowledge, attitudes, ethical and social perspectives towards fecal microbiota transplantation (GMT) among Jordanian healthcare providers. BMC Med Ethics. (2021) 22:19. doi: 10.1186/s12910-021-00587-6
57. Hobbs M, Ahuriri-Driscoll A, Marek L, Campbell M, Tomintz M, Kingham S. Reducing health inequity for Māori people in New Zealand. Lancet. (2019) 394:1613–4. doi: 10.1016/S0140-6736(19)30044-3
58. Downs IA, Brandt LJ., Oneto C, Feuerstadt P, Aroniadis OC. Perceptions of fecal microbiota transplantation for diarrhea predominant irritable bowel syndrome. Am J Gastroenterol. (2016) 111:S1250–1. doi: 10.1038/ajg.2016.384
59. Kao D, Roach B, Silva M, Beck P, Rioux K, Kaplan GG, et al. Effect of Oral Capsule– vs Colonoscopy-Delivered Fecal Microbiota Transplantation on Recurrent Clostridium difficile Infection: A Randomized Clinical Trial. JAMA. (2017) 318:1985. doi: 10.1001/jama.2017.17077
60. Belsey J, Crosta C, Epstein O, Fischbach W, Layer P, Parente F, et al. Meta-analysis: the relative efficacy of oral bowel preparations for colonoscopy 1985-2010: Meta-analysis: bowel preparation. Aliment Pharmacol Ther. (2012) 35:222–37. doi: 10.1111/j.1365-2036.2011.04927.x
61. Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, et al. Treating clostridium difficile infection with fecal microbiota transplantation. Clin Gastroenterol Hepatol. (2011) 9:1044–9. doi: 10.1016/j.cgh.2011.08.014
62. Detailed Eligibility Criteria. New Zealand Blood Service. Available at: https://www.nzblood.co.nz//become-a-donor/am-i-eligible/detailed-eligibility-criteria/.
63. Cammarota G, Ianiro G, Tilg H, Rajilić-Stojanović M, Kump P, Satokari R, et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut. (2017) 66:569–80. doi: 10.1136/gutjnl-2016-313017
64. Mullish BH, Quraishi MN, Segal JP, McCune VL, Baxter M, Marsden GL, et al. The use of faecal microbiota transplant as treatment for recurrent or refractory Clostridium difficile infection and other potential indications: joint British Society of Gastroenterology (BSG) and Healthcare Infection Society (HIS) guidelines. Gut. (2018) 67:1920–41. doi: 10.1136/gutjnl-2018-316818
65. Madar PC, Petre O, Baban A, Dumitrascu DL. Medical students’ perception on fecal microbiota transplantation. BMC Med Educ. (2019) 19(1):368. doi: 10.1186/s12909-019-1804-7
66. Cammarota G, Ianiro G, Kelly CR, Mullish BH, Allegretti JR, Kassam Z, et al. International consensus conference on stool banking for faecal microbiota transplantation in clinical practice. Gut. (2019) 68:2111–21. doi: 10.1136/gutjnl-2019-319548
67. Stormacq C, Van Den Broucke S, Wosinski J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot Int. (2019) 34:e1–17. doi: 10.1093/heapro/day062
68. Langhorst J, Anthonisen IB, Steder-Neukamm U, Lüdtke R, Spahn G, Michalsen A, et al. Amount of systemic steroid medication is a strong predictor for the use of complementary and alternative medicine in patients with inflammatory bowel disease.: results from a german national survey. Inflammation Bowel Dis. (2005) 11:287–95. doi: 10.1097/01.MIB.0000160771.71328.6c
69. Baunwall SMD, Terveer EM, Dahlerup JF, Erikstrup C, Arkkila P, Vehreschild MJ, et al. The use of Faecal Microbiota Transplantation (GMT) in Europe: A Europe-wide survey. Lancet Reg Health - Eur. (2021) 9:100181. doi: 10.1016/j.lanepe.2021.100181
70. Fadda HM. The route to palatable fecal microbiota transplantation. AAPS PharmSciTech. (2020) 21:114. doi: 10.1208/s12249-020-1637-z
Keywords: faecal microbiome transfer, public opinion, gastroenterology, survey, microbiome
Citation: Tweedie-Cullen RY, Wilson BC, Derraik JGB, Albert BB, Opai K, Edwards T, O’Sullivan JM and Cutfield WS (2024) Awareness and acceptability of gut microbiome transfer. Front. Gastroenterol. 3:1411898. doi: 10.3389/fgstr.2024.1411898
Received: 03 April 2024; Accepted: 12 July 2024;
Published: 09 August 2024.
Edited by:
Michele Di Stefano, IRCCS S. Matteo Hospital Foundation, ItalyReviewed by:
Claudio Nicoletti, University of Siena, ItalyDiana Gabriela Iacob, Bucharest University Emergency Hospital, Romania
Copyright © 2024 Tweedie-Cullen, Wilson, Derraik, Albert, Opai, Edwards, O’Sullivan and Cutfield. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wayne S. Cutfield, dy5jdXRmaWVsZEBhdWNrbGFuZC5hYy5ueg==