
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Gastroenterol., 19 September 2023
Sec. Gastroenterology and Cancer
Volume 2 - 2023 | https://doi.org/10.3389/fgstr.2023.1258998
This article is part of the Research TopicPancreatic Cystic Lesions: Aiding in the Early Diagnosis of Pancreatic CancerView all 5 articles
 Daniel A. Sheik1*
Daniel A. Sheik1* Kaleb Byers1
Kaleb Byers1 Mini Thomas1
Mini Thomas1 Ummadisetti Chinna Rajesh1
Ummadisetti Chinna Rajesh1 Kelli Ifuku2
Kelli Ifuku2 Kimberly Kirkwood2
Kimberly Kirkwood2 Mohammed Al-Haddad3
Mohammed Al-Haddad3 Charles S. Craik4
Charles S. Craik4 V. Jo Davisson1,5†
V. Jo Davisson1,5†The incidental detection of pancreatic cysts, an opportunity for the early detection of pancreatic cancer, is increasing, owing to an aging population and improvements in imaging technology. The classification of pancreatic cystic precursors currently relies on imaging and cyst fluid evaluations, including cytology and protein and genomic analyses. However, there are persistent limitations that obstruct the accuracy and quality of information for clinicians, including the limited volume of the complex, often acellular, and proteinaceous milieu that comprises pancreatic cyst fluid. The constraints of currently available clinical assays lead clinicians to the subjective and inconsistent application of diagnostic tools, which can contribute to unnecessary surgery and missed pancreatic cancers. Herein, we describe the pathway toward pancreatic cyst classification and diagnosis, the volume requirements for several clinically available diagnostic tools, and some analytical and diagnostic limitations for each assay. We then discuss current and future work on novel markers and methods, and how to expand the utility of clinical pancreatic cyst fluid samples. Results of ongoing studies applying SERS as a detection mode suggest that 50 µL of pancreatic cyst fluid is more than sufficient to accurately rule out non-mucinous pancreatic cysts with no malignant potential from further evaluation. This process is expected to leave sufficient fluid to analyze a follow-up, rule-in panel of markers currently in development that can stratify grades of dysplasia in mucinous pancreatic cysts and improve clinical decision-making.
Pancreatic cancer continues to move toward the top of the list of deadliest cancers, with an estimated 5-year survival rate of around 10% (1). The grim outlook for this disease can be directly attributed to the late stage at which an accurate diagnosis is typically achieved. Pancreatic cystic lesions are potential predictors of progression to cancer, and understanding the progression from cyst to cancer provides an avenue for early pancreatic cancer detection. Pancreatic cystic lesions are incidentally detected in 3 million (and growing) patients annually in the USA and present a real-world clinical problem for diagnosing early-stage malignancy accurately (2). Several studies have estimated from post mortem autopsy analysis that 24% of people over 60 years old could pass away with an unidentified pancreatic cyst of variable clinical signficance (3–5). An impediment to early-stage detection is the lack of noticeable symptoms during progression from non-malignant pancreatic cyst to invasive pancreatic cancer until it is too late for meaningful intervention (6–8). At the time of this publication, there are no approved screening methods to detect pancreatic cysts or cancer for the population at large. Thus, a significant problem in the management of pancreatic cystic lesions is simply finding patients in whom a potentially malignant pancreatic cyst has developed and identifying those patients for whom surgical resection is necessary. Conversely, patients with indolent pancreatic cysts that will never progress to malignancy should also be identified to avoid unnecessary surgery. As a result, a significant number of people remain undiagnosed or untreated at a time when surgical resection would be beneficial.
Over the past decade, efforts have focused on improving diagnostic resolution in pancreatic cancer. Novel diagnostic tools, markers, and analytical methods are providing more information about effective approaches to diagnosis. Still, there remains an unmet need for such tools to be translated into clinical settings. This work will discuss the current pathway to diagnosis, including the limitations of clinical diagnostic tools for pancreatic cancer, followed by advances being made in laboratories for translation into clinical settings. This article is not intended to be a comprehensive analysis of every marker and tool reported. Instead, the intention is to identify unmet needs associated with the accurate clinical diagnosis of pancreatic cysts, focusing on the current standards of care, and examine select projects that are seeking translation to the clinic to address these unmet needs and enhance the resolution for this troublesome diagnosis.
Pancreatic cyst patient management is shaped by three main guidelines (ACG, AGA, and Fukuoka), which seek to incorporate imaging and cyst fluid analyses to guide the management of a pancreatic cyst for surveillance or surgical resection (9–11). Most patients with pancreatic cysts have “indeterminate” cysts in which both the type (mucinous vs. non-mucinous) and histologic grade are radiographically uncertain (12, 13). These patients are often referred for endoscopic ultrasound with fine needle aspiration (EUS-FNA) to extract pancreatic cyst fluid samples for chemical and genomic analyses. Although EUS-FNA is a complex and invasive process, it is preferred to endoscopic solid tissue biopsy with microforceps because of the elevated risks associated with the tissue biopsy procedure and an estimated diagnostic improvement of only 10% (14, 15). As discussed throughout this article, pancreatic cyst fluid is a commonly acellular, highly proteinaceous, and viscous biofluid that contains a wealth of bioinformation and substances that could potentially interfere with clinical assays.
Ideally, the first step in diagnosis is to rule out potential malignancy by differentiating between non-mucinous pancreatic cysts that are predominantly benign from mucinous cysts that have a 10%–50% chance of progressing to cancer (16). With these two cohorts identified, different treatment plans can be crafted, wherein patients in need of further testing of a potentially malignant mucinous pancreatic cyst are prioritized. In this situation, the roughly 20%–40% of patients that undergo an EUS-FNA procedure and are confirmed to have a non-mucinous cyst are spared from further surveillance and the attendant emotional, physical, and financial burdens of repeat doctor visits, diagnostic testing, and monitoring (16, 17). Next, clinicians strive to stratify the mucinous population based on the actual risk of progression to cancer (the rule-in phase). This second diagnosis phase is decidedly more challenging, as the established markers for the rule-out diagnosis have not proven to be adequate predictors of progression to cancer for rule-in determinations (18). As a result, although new marker discoveries are ongoing, there is not currently an accepted method by which pancreatic cysts with high-grade dysplasia or early invasive cancer can be quickly and accurately identified. It is also important to note that this process is rarely as straightforward as presented here or in Figure 1. However, multiple technologies have been developed, and continue to be improved, that can accurately determine the type of pancreatic cyst present.
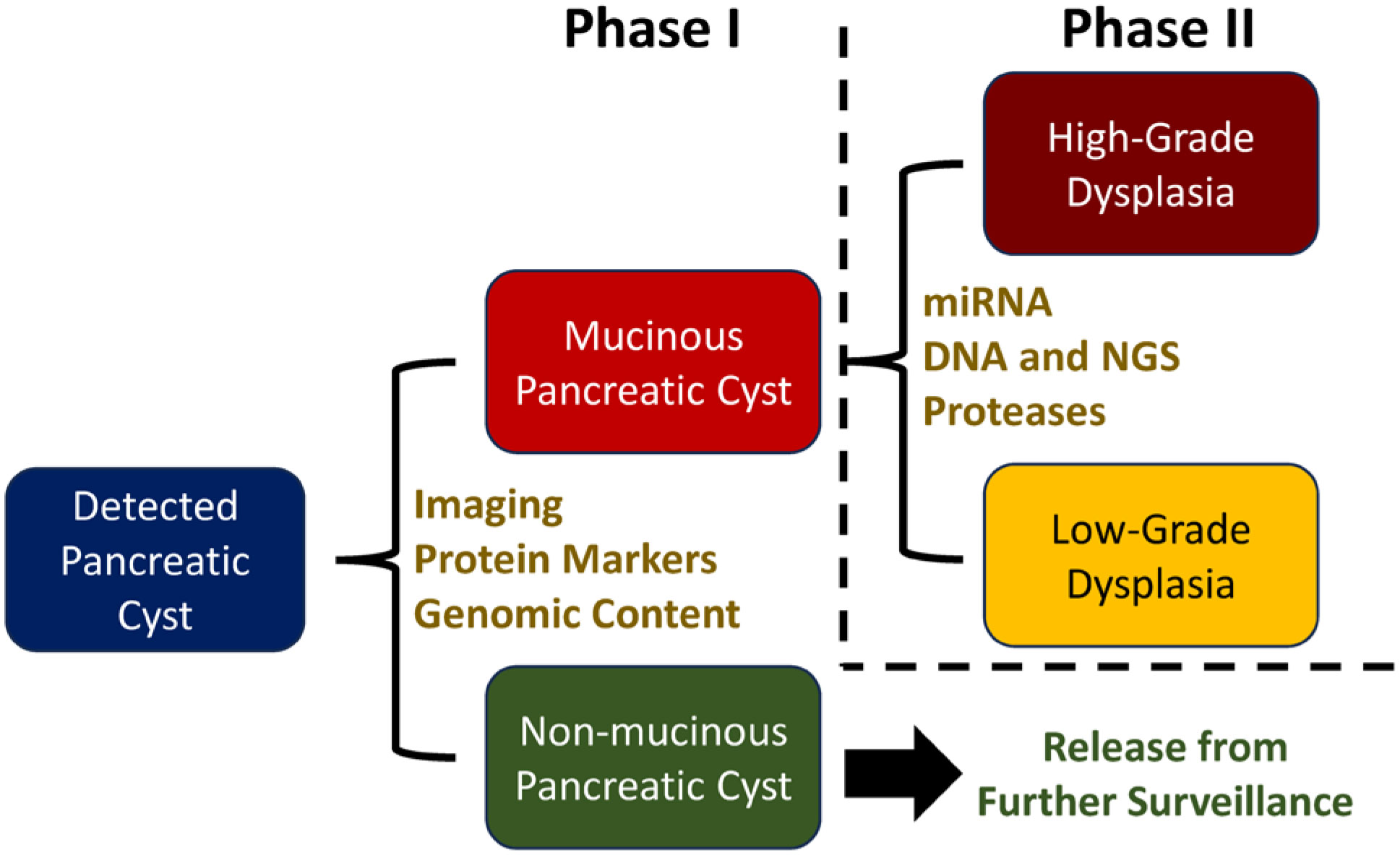
Figure 1 General pancreatic cyst diagnosis strategy and example tests for each phase.
Pancreatic cysts are commonly found incidentally during routine imaging for unrelated disorders. Advances in CT and MRI imaging have improved resolution such that more and smaller pancreatic cysts can now be identified, providing an opportunity for earlier diagnosis (19). However, this comes with the drawback that smaller cysts are more challenging to classify and produce less cyst fluid for biochemical analyses. The primary utility of imaging for classification relies on shape/size and location. It has been established over the years that cysts that form within the main pancreatic duct and those that have grown beyond 3 cm are more likely to progress to cancerous lesions than cysts that form in other regions of the pancreas or smaller cysts, however the risk remains highly variable (10). Although helpful, as with any image analysis, this approach comes with a subjective bias that hinders accurate diagnosis. Efforts to avoid image interpretation errors have focused on using machine learning and artificial intelligence methods (ML-AI) to process all available images and more accurately determine the classification of a pancreatic cyst. This work is mainly in the nascent stage, and it shows greater promise in organs like the lung in which the tumor signal-to-background ratio is high. In contrast, the solid components of pancreatic tumors are frequently camouflaged, making them difficult to detect (20). For patients with indeterminate cystic lesions of sufficient size, the next logical step is often to sample the cyst fluid and conduct (bio)chemical analyses.
Use of the EUS-FNA procedure has become more widespread, as the information contained within pancreatic cyst fluid has proven valuable (21–23). This section, and the following sections, will focus on EUS-FNA fluid analysis. In the case of pancreatic cyst fluid, microscopic examination of fluid contents (cytology) has the potential to accurately diagnose a pancreatic cyst with high-grade dysplasia or adenocarcinoma. However, the examination is often non-diagnostic because of the paucity of tumor cells in the fluid, with an estimated 31% success rate for obtaining cells for cytological analysis (24). Furthermore, the sample volume required for slide preparation may exceed 500 µL, which is often unavailable. Although this is a common clinical practice for diagnosing pancreatic cysts, the limited cellularity of pancreatic cyst fluid yields relatively low clinical utility; thus, we will omit any further discussion of cytology.
Biomarkers indicative of cancer have been studied, published, and established in the clinic as screening and diagnostic tools. Every cancer is different, but several biomarkers consistently present themselves during clinical investigations (25, 26). Their ubiquity makes them generally poor predictors of cancer type, but they unquestionably retain utility as indicators of cancer or progression toward cancer when the possibility of cancer arises. In the case of pancreatic cancer, carcinoembryonic antigen (CEA) and amylase have been used extensively in the clinic to support rule-out diagnoses. However, neither marker is individually indicative of either non-mucinous or mucinous pancreatic cyst fluid, with low sensitivity and/or specificity (27, 28). Other markers that suffer similar fates in clinical settings include CA19-9 and glucose; however, glucose has maintained clinical relevance for determining mucinous pancreatic cysts, with a sensitivity and specificity over 80% (29–32). For clinical labs, however, any of these markers represent a seemingly sensible method, as they are all amenable to automated processing on clinical analyzers, with little training or upgrades needed. Importantly, this reliance on convenience is still rife, causing clinical problems for diagnosis.
Clinical analyzers and their associated assays have been developed to work with highly proteinaceous fluids such as blood, serum, or plasma, and some are compatible with alternative biofluids such as urine or saliva. None of these fluids compare with pancreatic cyst fluid’s relatively high complexity and inter-sample variability. A basic review of published investigations into proteomic analyses of pancreatic cyst fluid reveals thousands of individual biomaterials present in any given sample (18, 33, 34). Still more problematic is that high concentrations of biomaterials have been established to cause inaccuracy and/or decreased reproducibility/repeatability in standard assay formats (35–37). For example, viscous materials like mucins present challenges in basic liquid handling, leading to erroneous sample volume transfers and assay results. Furthermore, the sample volume requirements for clinical analyzers often preclude the replicate analysis of multiple markers in single pancreatic cyst fluid samples. The balance at hospital clinics between high-throughput analysis and sample preservation is certainly skewed toward high throughput. Furthermore, the standards set by the analysis of readily available blood samples are often inappropriate for pancreatic cyst fluid samples. Although assays for markers of interest could be run at lower volumes, the analyzers employed in the clinic often require 200–500 µL of sample per run. When these factors are taken together, it is unsurprising that assays of biomarkers that lack sensitivity and specificity, and inhibit multiple-marker analyses due to sample consumption, inevitably lack the capacity for accurate diagnosis.
However, there are alternative protein markers still undergoing translational research that can provide useful diagnostic information. For instance, vascular endothelial growth factor (VEGF) has been shown to be a reliable marker of notoriously difficult to diagnose serous cystic neoplasms (SCNs) (38–40). SCNs are non-mucinous pancreatic cysts that are difficult to distinguish from potentially malignant intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms (MCNs) using imaging or the previously described protein markers (41). Although they constitute an estimated 1%–2% of all pancreatic cysts, avoiding unnecessary surgical intervention for SCNs will improve the quality of life for patients (42). In addition to VEGF, the monoclonal antibody Das-1, originally used as a marker of colonic epithelial phenotype, has shown utility in predicting malignancy in conditions of the upper GI tract (43, 44). Importantly, Das-1 has displayed the unique ability to stratify low- and high-grade dysplasia and invasive cancer in mucinous pancreatic cyst fluid.
Research into the genetic drivers of pancreatic cancer has found long lists of markers in DNA, RNA, miRNA, and mRNA, and has recently made the logical step toward combination marker panels investigating several genetic components at once. Again, most of the tools have not translated into clinical utility, except for DNA markers that can be amplified and quantified in high-throughput platforms (45, 46). Next-generation sequencing (NGS) is a technique that emerged on the market in the mid-2000s, and has provided a wealth of information for researchers in biology and biochemistry. Every clinical sample prepared for extraction is subject to volume requirements to meet the demand of the extraction method. Although sample preparation for NGS can be conducted with lower volumes, to counter low-genomic-content samples, general estimates for required sample volume are around 500 µL (47). This means that NGS is expected to consume significant resources from a limited pancreatic cyst fluid sample, further constraining the utility of other diagnostic tools.
Regardless, although the fluid is typically acellular, NGS has produced rich genetic information from pancreatic cyst fluid samples. Studies investigating genetic markers or defects have found that NGS can accurately diagnose specific cyst types. A prime recent example of this is the study by Paniccia et al., wherein they investigated 1,933 pancreatic cyst fluid samples for genomic content and were able to diagnose those cysts with negative predictive values (NPVs) and positive predictive values (PPVs) greater than 90% in most cases (48). They also made use of imaging where available to supplement NGS data and further improve the NPV and PPV in select cases. With the cyst type identified, a more practical treatment course can be determined, and this information indeed leads to better diagnostic outcomes for patients. But it is again important to note that cyst type alone does not confer sufficient information about the degree of risk of progression to cancer. Recent efforts have focused on improving analysis algorithms to identify cyst types better and eventually stratify dysplasia.
Recent years have seen a tremendous increase in interest in biological exosomes (49). Broadly speaking, exosomes are vesicles ranging in size from 10—200 nm that are released from cells and contain unique chemical and genetic information. Exosomes are found in many distinct human biofluids, with the majority of research focused on blood-based exosomes, which contain information from any tissue source secreting into the bloodstream. Blood-based exosomes are ideal targets for the analysis of most disease states, including, if not especially, cancer (50). It has been hypothesized that cells use exosomes to inform their local community of different signals and activation patterns (51). Until recently, however, efficient isolation of such material from biological sources was complicated at best, and near impossible at worst.
Multiple methods, including ultracentrifugation, size exclusion chromatography, and immunoaffinity have been used to isolate exosomes with varying degrees of success and recovery. However, a recent study by Hinestrosa et al. demonstrated a clever method for isolating exosomes from plasma, wherein they used an electrode array to attract the charged membrane of exosomes to a solid support from which they can be washed and resuspended for analysis (52). This study investigated exosomes to identify pancreatic, ovarian, and bladder cancers, and analyzed the resulting samples with commercially available protein quantification kits. The compiled data were used to train an algorithm for multiple markers that could accurately detect early-stage cancer, and displayed a high sensitivity for pancreatic cancer. These results suggest that exosomes should continue to be a source of diagnostic information, and it is likely that with some further marker optimization and refined assay development this isolation technology has the potential for widespread adoption in cancer diagnostics.
An underutilized approach in the search for clinically translatable diagnostic assays in pancreatic cancer has been the analysis of enzyme activity, as opposed to enzyme mass (53–56). Immunoassays dominate the landscape of biomarker analysis and have been readily adapted into automated systems that improve throughput, reproducibility, and sample handling. ELISA-based methods have provided an incomparable wealth of data about protein expression and are now a mainstay in research and clinical laboratories. However, immunoassays quantify the amount of protein present, which can be ambiguous when investigating enzyme markers as active (or activatable) enzymes are responsible for signaling cascades, metabolism, and phenotypical responses (57–59). There have been publications over the years examining protease cleavage, enzymatic redox reactions, and other activity measurements. Yet still, these assays have struggled to translate meaningfully to clinical settings in the same way that immunoassays have over the decades. One possible reason is that, although protease cleavages are an amplification process, proteolytic activity on substrates is not necessarily as efficient or rapid a process as the commonly used secondary reactions in ELISA formats. Due to the lower amplification of optically active products, it is difficult for traditional optical methods to detect and quantify low activity. It is even more complicated when sample volumes are limited.
Clinical assays rely on optical detection methods including luminescence, fluorescence, and absorbance. New protein biomarkers are routinely identified using mass spectrometry (MS) methods. However, for many of these candidate markers, the expression level is below the limits of detection for traditional optical methods. A path forward is the use of alternative detection technologies such as Raman spectroscopy. Raman spectroscopy is based on an inelastic light scattering event that imbues the scattered photons with chemical and structural information owing to the excitation of molecular vibrational modes. Although only approximately 1 in 100,000,000 photons are predicted to produce Raman scattering, the introduction of a coinage metal (Au, Ag, or Cu) surface has been shown to enhance the Raman scattering intensity by multiple orders of magnitude, leading to ultrasensitive detection limits (60, 61). First discovered in 1974, surface-enhanced Raman spectroscopy (SERS) has become a more practical tool as the cost and size of Raman equipment have dramatically decreased (62, 63). Recent investigators have used SERS to detect single-molecule Raman signals (SMSERS), which provides additional support for the utility of SERS in clinical assays for low-concentration and/or low-volume samples (64–66). Furthermore, the chemical fingerprint information provided by Raman scattering enables discrimination of multiple dye classes (i.e., fluoresceins, rhodamines, cyanines), or dyes with variable isotopic labeling, enabling intrasample multiplexing at incredibly low concentrations (67–70).
The authors of this review have translated assays using Raman-active dyes that have shown detection limits below those of traditional fluorescence measurements (71). Furthermore, Suresh et al. have published the first example of translating a SERS assay for protease activity of gastricsin to a clinically ready platform with a small cohort of human pancreatic cyst fluid samples (72). Pancreatic cyst fluid is a notoriously tricky medium with which to run assays or optically quantify results, and the simplest solution is significant sample dilution to diminish interfering substances. The ultrasensitivity of SERS and a protease activity assay that displayed reduced interference from the sample milieu provided an ideal assay platform for high-dilution quantification. Importantly, the published results were from assays of 1 µL of pancreatic cyst fluid, supporting the analysis of multiple markers indicative of pancreatic cancer from single pancreatic cyst fluid samples without high volume requirements. Currently the group is engaged in a statistically powered study with a larger cohort and a panel of three biomarker assays that is expected to produce an NPV of >95% for identifying non-mucinous pancreatic cyst fluid. Again, all three assays are run using only 12 μL of clinical sample, meaning that these efforts do not disrupt current standards of clinical care, and analyze a sample volume that would be incompatible with contemporary clinical assays.
Each area of research described in this article has produced undeniable advances in support of decision-making for patients in whom a pancreatic cyst has been detected. However, more work, creativity, and translatable development of new tools are required to produce the desired outcomes for patients. Modifications to assay platforms, or preanalytical steps paired with assays that consume less sample volume, will undeniably expand the utility of limited clinical samples. There are also other approaches seeking to use multimodal analyses to diagnose pancreatic cysts (47, 73). It is undeniable that incorporation of standard clinical data from imaging and cytology into biomarker analyses provides the best diagnostic resolution for patients and clinicians. However, most of the work described here identifies patients who can be ruled out from further consideration. It is the remaining mucinous pancreatic cyst population that requires attention moving forward. Marker identification and translation, combination panels, and collaboration will be vital in addressing the unmet need for dysplasia grading in pancreatic cyst fluid.
DS: Conceptualization, Writing – original draft, Writing – review & editing. KB: Writing – review & editing. MT: Writing – review & editing. UR: Writing – review & editing. KI: Writing – review & editing. KK: Writing – review & editing. MA: Writing – review & editing. CC: Writing – review & editing. VD: Conceptualization, Writing – review & editing.
DS, KB, MT, and UR acknowledge support from NCI SBIR grant 1R43CA277913-01A1. KI and KK are supported by NIH grant U01CA271250. CC is supported by NIAID grant U19AI171110. VD acknowledges support from grant 40004015 from the Elevate Ventures Innovation Voucher Program.
Authors DS, KB, UR, and MT are employed by Amplified Sciences. KK, MA-H, and CC consult and advise for Amplified Sciences. Author VD is the owner/founder of Amplified Sciences.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bengtsson A, Andersson R, Ansari D. The actual 5-year survivors of pancreatic ductal adenocarcinoma based on real-world data. Sci Rep (2020) 10(1):16425. doi: 10.1038/s41598-020-73525-y
2. Sharib J, Esserman L, Koay EJ, Maitra A, Shen Y, Kirkwood KS, et al. Cost-effectiveness of consensus guideline based management of pancreatic cysts: the sensitivity and specificity required for guidelines to be cost-effective. Surgery (2020) 168(4):601–9. doi: 10.1016/j.surg.2020.04.052
3. Kromrey M-L, Bülow R, Hübner J, Paperlein C, Lerch MM, Ittermann T, et al. Prospective study on the incidence, prevalence and 5-year pancreatic-related mortality of pancreatic cysts in a population-based study. Gut (2018) 67(1):138–45. doi: 10.1136/gutjnl-2016-313127
4. Kimura W, Nagai H, Kuroda A, Muto T, Esaki Y. Analysis of small cystic lesions of the pancreas. Int J Pancreatol (1995) 18(3):197–206. doi: 10.1007/BF02784942
5. Zaheer A, Pokharel SS, Wolfgang C, Fishman EK, Horton KM. Incidentally detected cystic lesions of the pancreas on CT: review of literature and management suggestions. Abdom Imaging (2013) 38(2):331–41. doi: 10.1007/s00261-012-9898-y
6. Brugge WR. Diagnosis and management of cystic lesions of the pancreas. J Gastrointestinal Oncol (2015) 6(4):103–18. doi: 10.3978/j.issn.2078-6891.2015.057
7. Yoon WJ, Brugge WR. Pancreatic cystic neoplasms: diagnosis and management. Gastroenterol Clinics North America (2012) 41(1):103–18. doi: 10.1016/j.gtc.2011.12.016
8. Farrell JJ. Prevalence, diagnosis and management of pancreatic cystic neoplasms: current status and future directions. Gut Liver (2015) 9(5):571–89. doi: 10.5009/gnl15063
9. Vege SS, Ziring B, Jain R, Moayyedi P, Adams MA, Dorn SD, et al. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology (2015) 148(4):819–22. doi: 10.1053/j.gastro.2015.01.015
10. Elta G, Enestvedt B, Sauer B, Lennon A. ACG clinical guideline: diagnosis and management of pancreatic cysts. Am J Gastroenterol (2018) 113(4):464–79. doi: 10.1038/ajg.2018.14
11. Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang J-Y, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology (2012) 12(3):183–97. doi: 10.1016/j.pan.2012.04.004
12. Mccoy EM, Chung DS, Chhablani RK, Pham BV, Reicher S, Eysselein VE. T1485: natural history and management of indeterminate cystic lesions of the pancreas. Gastrointestinal Endoscopy (2010) 71(5):AB289. doi: 10.1016/j.gie.2010.03.698
13. Park J, Park J, Lee YS, Jung K, Jung IH, Lee J-C, et al. Increased incidence of indeterminate pancreatic cysts and changes of management pattern: evidence from nationwide data. Hepatobiliary Pancreatic Dis Int (2023) 22(3):294–301. doi: 10.1016/j.hbpd.2022.06.002
14. Kovacevic B, Klausen P, Rift CV, Toxværd A, Grossjohann H, Karstensen JG, et al. Clinical impact of endoscopic ultrasound-guided through-the-needle microbiopsy in patients with pancreatic cysts. Endoscopy (2021) 53(01):44–52. doi: 10.1055/a-1214-6043
15. Cho SH, Song TJ, Seo D-W, Oh D, Park DH, Lee SS, et al. Efficacy and safety of EUS-guided through-the-needle microforceps biopsy sampling in categorizing the type of pancreatic cystic lesions. Gastrointestinal Endoscopy (2022) 95(2):299–309. doi: 10.1016/j.gie.2021.09.035
16. Valsangkar NP, Morales-Oyarvide V, Thayer SP, Ferrone CR, Wargo JA, Warshaw AL, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the massachusetts general hospital. Surgery (2012) 152(3, Supplement):S4–S12. doi: 10.1016/j.surg.2012.05.033
17. Lekkerkerker SJ, Besselink MG, Busch OR, Verheij J, Engelbrecht MR, Rauws EA, et al. Comparing 3 guidelines on the management of surgically removed pancreatic cysts with regard to pathological outcome. Gastrointestinal Endoscopy (2017) 85(5):1025–31. doi: 10.1016/j.gie.2016.09.027
18. Do M, Kim H, Shin D, Park J, Kim H, Han Y, et al. Marker identification of the grade of dysplasia of intraductal papillary mucinous neoplasm in pancreatic cyst fluid by quantitative proteomic profiling. Cancers (2020) 12(9):2383. doi: 10.3390/cancers12092383
19. Miller FH, Lopes Vendrami C, Recht HS, Wood CG, Mittal P, Keswani RN, et al. Pancreatic cystic lesions and Malignancy: assessment, guidelines, and the field defect. RadioGraphics (2022) 42(1):87–105. doi: 10.1148/rg.210056
20. Liu M, Wu J, Wang N, Zhang X, Bai Y, Guo J, et al. The value of artificial intelligence in the diagnosis of lung cancer: A systematic review and meta-analysis. PloS One (2023) 18(3):e0273445. doi: 10.1371/journal.pone.0273445
21. Lariño-Noia J, Iglesias-Garcia J, de la Iglesia-Garcia D, Dominguez-Muñoz JE. EUS-FNA in cystic pancreatic lesions: where are we now and where are we headed in the future? Endosc Ultrasound (2018) 7(2):102–9. doi: 10.4103/eus.eus_93_17
22. Faias S, Cravo M, Pereira da Silva J, Chaves P, Dias Pereira A. Endoscopic ultrasound with fine needle aspiration is useful in pancreatic cysts smaller than 3 cm. BMC Gastroenterol (2020) 20(1):413. doi: 10.1186/s12876-020-01565-9
23. Pan S, Liu J, Guo J, Zhu Q, Wang L, Shi X. The clinical impact of endoscopic ultrasound-guided fine-needle aspiration on the patients with low-risk pancreatic cystic lesions. Front Oncol (2022) 12. doi: 10.3389/fonc.2022.961293
24. de Jong K, Poley J-W, van Hooft JE, Visser M, Bruno MJ, Fockens P. Endoscopic ultrasound-guided fine-needle aspiration of pancreatic cystic lesions provides inadequate material for cytology and laboratory analysis: initial results from a prospective study. Endoscopy (2011) 43(7):585–90. doi: 10.1055/s-0030-1256440
25. Sarhadi VK, Armengol G. Molecular biomarkers in cancer. Biomolecules (2022) 12(8):1021. doi: 10.3390/biom12081021
26. Chatterjee SK, Zetter BR. Cancer biomarkers: knowing the present and predicting the future. Future Oncol (2005) 1(1):37–50. doi: 10.1517/14796694.1.1.37
27. Nagula S, Kennedy T, Schattner MA, Brennan MF, Gerdes H, Markowitz AJ, et al. Evaluation of cyst fluid CEA analysis in the diagnosis of mucinous cysts of the pancreas. J Gastrointest Surg (2010) 14(12):1997–2003. doi: 10.1007/s11605-010-1281-0
28. Talar−Wojnarowska R, Pazurek M, Durko L, Degowska M, Rydzewska G, Smigielski J, et al. Pancreatic cyst fluid analysis for differential diagnosis between benign and Malignant lesions. Oncol Lett (2013) 5(2):613–6. doi: 10.3892/ol.2012.1071
29. Zamir E, Yovel DZ, Scapa E, Shnell M, Bar N, Yishay IB, et al. Pancreatic cyst fluid glucose: A rapid on-site diagnostic test for mucinous cysts. Ther Adv Gastroenterol (2022) 15:17562848221133580. doi: 10.1177/17562848221133581
30. Zikos T, Pham K, Bowen R, Chen A, Banerjee S, Friedland S, et al. Cyst fluid glucose is rapidly feasible and accurate in diagnosing mucinous pancreatic cysts. Am J Gastroenterol (2015) 110(6):909–14. doi: 10.1038/ajg.2015.148
31. Yip-Schneider MT, Wu H, Allison HR, Easler JJ, Sherman S, Al-Haddad MA, et al. Biomarker risk score algorithm and preoperative stratification of patients with pancreatic cystic lesions. J Am Coll Surgeons (2021) 233(3):426–34. doi: 10.1016/j.jamcollsurg.2021.05.030
32. Carr RA, Yip-Schneider MT, Simpson RE, Dolejs S, Schneider JG, Wu H, et al. Pancreatic cyst fluid glucose: rapid, inexpensive, and accurate diagnosis of mucinous pancreatic cysts. Surgery (2018) 163(3):600–5. doi: 10.1016/j.surg.2017.09.051
33. Paziewska A, Polkowski M, Rubel T, Karczmarski J, Wiechowska-Kozlowska A, Dabrowska M, et al. Mass spectrometry-based comprehensive analysis of pancreatic cyst fluids. BioMed Res Int (2018) 2018:7169595. doi: 10.1155/2018/7169595
34. Park J, Yun HS, Lee KH, Lee KT, Lee JK, Lee S-Y. Discovery and validation of biomarkers that distinguish mucinous and nonmucinous pancreatic cysts. Cancer Res (2015) 75(16):3227–35. doi: 10.1158/0008-5472.CAN-14-2896
35. Sundermann J, Sydow S, Burmeister L, Hoffmann A, Menzel H, Bunjes H. ELISA- and activity assay-based quantification of BMP-2 released in vitro can be biased by solubility in “Physiological” Buffers and an interfering effect of chitosan. Pharmaceutics (2021) 13(4):582. doi: 10.3390/pharmaceutics13040582
36. Huang Y, Lü X, Qian W, Tang Z, Zhong Y. Competitive protein adsorption on biomaterial surface studied with reflectometric interference spectroscopy. Acta Biomaterialia (2010) 6(6):2083–90. doi: 10.1016/j.actbio.2009.12.035
37. Bowen RAR, Remaley AT. Interferences from blood collection tube components on clinical chemistry assays. Biochem Med (2014) 24(1):31–44. doi: 10.11613/BM.2014.006
38. Yip-Schneider MT, Wu H, Dumas RP, Hancock BA, Agaram N, Radovich M, et al. Vascular endothelial growth factor, a novel and highly accurate pancreatic fluid biomarker for serous pancreatic cysts. J Am Coll Surgeons (2014) 218(4):608–17. doi: 10.1016/j.jamcollsurg.2013.12.019
39. Carr RA, Yip-Schneider MT, Dolejs S, Hancock BA, Wu H, Radovich M, et al. Pancreatic cyst fluid vascular endothelial growth factor A and carcinoembryonic antigen: A highly accurate test for the diagnosis of serous cystic neoplasm. J Am Coll Surgeons (2017) 225(1):93–100. doi: 10.1016/j.jamcollsurg.2017.05.003
40. Yip-Schneider MT, Wu H, Schmidt CM. Novel expression of vascular endothelial growth factor isoforms in the pancreas and pancreatic cystic lesions. Biochimie (2021) 181:234–9. doi: 10.1016/j.biochi.2020.12.016
41. Reid MD, Choi H, Balci S, Akkas G, Adsay V. Serous cystic neoplasms of the pancreas: clinicopathologic and molecular characteristics. Semin Diagn Pathol (2014) 31(6):475–83. doi: 10.1053/j.semdp.2014.08.009
42. Scholten L, van Huijgevoort NCM, van Hooft JE, Besselink MG, Chiaro MD. Pancreatic cystic neoplasms: different types, different management, new guidelines. VIS (2018) 34(3):173–7. doi: 10.1159/000489641
43. Das KK, Brown JW, Fernandez del-Castillo C, Huynh T, Mills JC, Matsuda Y, et al. MAb das-1 identifies pancreatic ductal adenocarcinoma and high-grade pancreatic intraepithelial neoplasia with high accuracy. Hum Pathol (2021) 111:36–44. doi: 10.1016/j.humpath.2021.01.003
44. Das KK, Xiao H, Geng X, Fernandez-del-Castillo C, Morales-Oyarvide V, Daglilar E, et al. MAb das-1 is specific for high-risk and Malignant intraductal papillary mucinous neoplasm (IPMN). Gut (2014) 63(10):1626–34. doi: 10.1136/gutjnl-2013-306219
45. Al-Haddad M, DeWitt J, Sherman S, Schmidt CM, LeBlanc JK, McHenry L, et al. Performance characteristics of molecular (DNA) analysis for the diagnosis of mucinous pancreatic cysts. Gastrointestinal Endoscopy (2014) 79(1):79–87. doi: 10.1016/j.gie.2013.05.026
46. Singhi AD, McGrath K, Brand RE, Khalid A, Zeh HJ, Chennat JS, et al. Preoperative next-generation sequencing of pancreatic cyst fluid is highly accurate in cyst classification and detection of advanced neoplasia. Gut (2018) 67(12):2131–41. doi: 10.1136/gutjnl-2016-313586
47. Springer S, Masica DL, Molin MD, Douville C, Thoburn CJ, Afsari B, et al. A multimodality test to guide the management of patients with a pancreatic cyst. Sci Trans Med (2019) 11(501):eaav4772. doi: 10.1126/scitranslmed.aav4772
48. Paniccia A, Polanco PM, Boone BA, Wald AI, McGrath K, Brand RE, et al. Prospective, multi-institutional, real-time next-generation sequencing of pancreatic cyst fluid reveals diverse genomic alterations that improve the clinical management of pancreatic cysts. Gastroenterology (2023) 164(1):117–33.e7. doi: 10.1053/j.gastro.2022.09.028
49. Li X, Corbett AL, Taatizadeh E, Tasnim N, Little JP, Garnis C, et al. Challenges and opportunities in exosome research—Perspectives from biology, engineering, and cancer therapy. APL Bioeng (2019) 3(1):011503. doi: 10.1063/1.5087122
50. Sauter ER. Exosomes in blood and cancer. Trans Cancer Res (2017) 6(Suppl 8):S1316–20. doi: 10.21037/tcr.2017.08.13
51. Maia J, Caja S, Strano Moraes MC, Couto N, Costa-Silva B. Exosome-based cell-cell communication in the tumor microenvironment. Front Cell Dev Biol (2018) 6. doi: 10.3389/fcell.2018.00018
52. Hinestrosa JP, Kurzrock R, Lewis JM, Schork NJ, Schroeder G, Kamat AM, et al. Early-stage multi-cancer detection using an extracellular vesicle protein-based blood test. Commun Med (2022) 2(1):29. doi: 10.1038/s43856-022-00088-6
53. Mumtaz T, Qindeel M, Asim.ur.Rehman, Tarhini M, Ahmed N, Elaissari A. Exploiting proteases for cancer theranostic through molecular imaging and drug delivery. Int J Pharmaceutics (2020) 587:119712. doi: 10.1016/j.ijpharm.2020.119712
54. Soleimany AP, Bhatia SN. Activity-based diagnostics: an emerging paradigm for disease detection and monitoring. Trends Mol Med (2020) 26(5):450–68. doi: 10.1016/j.molmed.2020.01.013
55. Vizovisek M, Ristanovic D, Menghini S, Christiansen MG, Schuerle S. The tumor proteolytic landscape: A challenging frontier in cancer diagnosis and therapy. Int J Mol Sci (2021) 22(5):2514. doi: 10.3390/ijms22052514
56. Amini AP, Kirkpatrick JD, Wang CS, Jaeger AM, Su S, Naranjo S, et al. Multiscale profiling of protease activity in cancer. Nat Commun (2022) 13(1):5745. doi: 10.1038/s41467-022-32988-5
57. O’Donoghue AJ, Ivry SL, Chaudhury C, Hostetter DR, Hanahan D, Craik CS. Procathepsin E is highly abundant but minimally active in pancreatic ductal adenocarcinoma tumors. Biol Chem (2016) 397(9):871–81. doi: 10.1515/hsz-2016-0138
58. Ivry SL, Sharib JM, Dominguez DA, Roy N, Hatcher SE, Yip-Schneider MT, et al. Global protease activity profiling provides differential diagnosis of pancreatic cysts. Clin Cancer Res (2017) 23(16):4865–74. doi: 10.1158/1078-0432.CCR-16-2987
59. Pontious C, Kaul S, Hong M, Hart PA, Krishna SG, Lara LF, et al. Cathepsin E expression and activity: role in the detection and treatment of pancreatic cancer. Pancreatology (2019) 19(7):951–6. doi: 10.1016/j.pan.2019.09.009
60. Downes A, Elfick A. Raman spectroscopy and related techniques in biomedicine. Sensors (Basel) (2010) 10(3):1871–89. doi: 10.3390/s100301871
61. Jones RR, Hooper DC, Zhang L, Wolverson D, Valev VK. Raman techniques: fundamentals and frontiers. Nanoscale Res Lett (2019) 14:231. doi: 10.1186/s11671-019-3039-2
62. Fleischmann M, Hendra PJ, McQuillan AJ. Raman spectra of pyridine adsorbed at a silver electrode. Chem Phys Lett (1974) 26(2):163–6. doi: 10.1016/0009-2614(74)85388-1
63. Emmanuel N, Nair RB, Abraham B, Yoosaf K. Fabricating a low-cost raman spectrometer to introduce students to spectroscopy basics and applied instrument design. J Chem Educ (2021) 98(6):2109–16. doi: 10.1021/acs.jchemed.0c01028
64. Dieringer JA, Wustholz KL, Masiello DJ, Camden JP, Kleinman SL, Schatz GC, et al. Surface-enhanced raman excitation spectroscopy of a single rhodamine 6G molecule. J Am Chem Soc (2009) 131(2):849–54. doi: 10.1021/ja8080154
65. Kleinman SL, Ringe E, Valley N, Wustholz KL, Phillips E, Scheidt KA, et al. Single-molecule surface-enhanced raman spectroscopy of crystal violet isotopologues: theory and experiment. J Am Chem Soc (2011) 133(11):4115–22. doi: 10.1021/ja110964d
66. Sharma B, Frontiera RR, Henry A-I, Ringe E, Van Duyne RP. SERS: materials, applications, and the future. Materials Today (2012) 15(1–2):16–25. doi: 10.1016/S1369-7021(12)70017-2
67. Eremina OE, Czaja AT, Fernando A, Aron A, Eremin DB, Zavaleta C. Expanding the multiplexing capabilities of raman imaging to reveal highly specific molecular expression and enable spatial profiling. ACS Nano (2022) 16(7):10341–53. doi: 10.1021/acsnano.2c00353
68. Zhang W, Tang S, Jin Y, Yang C, He L, Wang J, et al. Multiplex SERS-based lateral flow immunosensor for the detection of major mycotoxins in maize utilizing dual raman labels and triple test lines. J Hazardous Materials (2020) 393:122348. doi: 10.1016/j.jhazmat.2020.122348
69. Fujioka H, Shou J, Kojima R, Urano Y, Ozeki Y, Kamiya M. Multicolor activatable raman probes for simultaneous detection of plural enzyme activities. J Am Chem Soc (2020) 142(49):20701–7. doi: 10.1021/jacs.0c09200
70. Bartolowits MD, Xin M, Petrov DP, Tague TJ, Davisson VJ. Multimeric rhodamine dye-induced aggregation of silver nanoparticles for surface-enhanced raman scattering. ACS Omega (2019) 4(1):140–5. doi: 10.1021/acsomega.8b02970
71. Suresh V, Sheik DA, Detomasi TC, Zhao T, Zepeda T, Saladi S, et al. Prototype assay multiplexing SARS-coV-2 3CL-protease and angiotensin-converting enzyme 2 for saliva-based diagnostics in COVID-19. Biosensors (2023) 13(7):682. doi: 10.3390/bios13070682
72. Suresh V, Byers K, Rajesh UC, Caiazza F, Zhu G, Craik CS, et al. Translation of a protease turnover assay for clinical discrimination of mucinous pancreatic cysts. Diagnostics (2022) 12(6):1343. doi: 10.3390/diagnostics12061343
Keywords: rule-out, rule-in, dysplasia, early diagnosis, surface-enhanced Raman spectroscopy, pancreatic cancer, pancreatic cystic lesions
Citation: Sheik DA, Byers K, Thomas M, Rajesh UC, Ifuku K, Kirkwood K, Al-Haddad M, Craik CS and Davisson VJ (2023) Addressing the unmet clinical need for low-volume assays in early diagnosis of pancreatic cancer. Front. Gastroenterol. 2:1258998. doi: 10.3389/fgstr.2023.1258998
Received: 14 July 2023; Accepted: 23 August 2023;
Published: 19 September 2023.
Edited by:
Ravi Kumar Sharma, Chandigarh University, IndiaReviewed by:
Utpreksha Vaish, University of Alabama at Birmingham, United StatesCopyright © 2023 Sheik, Byers, Thomas, Rajesh, Ifuku, Kirkwood, Al-Haddad, Craik and Davisson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel A. Sheik, RGFuLlNoZWlrQGFtcGxpZmllZHNjaS5jb20=
†ORCID: V. Jo Davisson, orcid.org/0000-0003-1182-0007
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.