
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Epidemiol., 29 November 2023
Sec. Clinical Epidemiology
Volume 3 - 2023 | https://doi.org/10.3389/fepid.2023.1233323
 Matthew O. Wiens1,2,3*
Matthew O. Wiens1,2,3* Jessica Trawin1
Jessica Trawin1 Yashodani Pillay1,2
Yashodani Pillay1,2 Vuong Nguyen1
Vuong Nguyen1 Clare Komugisha3Nathan Kenya-Mugisha3Angella Namala4Lisa M. Bebell5
Clare Komugisha3Nathan Kenya-Mugisha3Angella Namala4Lisa M. Bebell5 J. Mark Ansermino1,2Niranjan Kissoon1,6
J. Mark Ansermino1,2Niranjan Kissoon1,6 Beth A. Payne7,8
Beth A. Payne7,8 Marianne Vidler9Astrid Christoffersen-Deb9
Marianne Vidler9Astrid Christoffersen-Deb9 Pascal M. Lavoie6,7
Pascal M. Lavoie6,7 Joseph Ngonzi10
Joseph Ngonzi10
Introduction: In low-income country settings, the first six weeks after birth remain a critical period of vulnerability for both mother and newborn. Despite recommendations for routine follow-up after delivery and facility discharge, few mothers and newborns receive guideline recommended care during this period. Prediction modelling of post-delivery outcomes has the potential to improve outcomes for both mother and newborn by identifying high-risk dyads, improving risk communication, and informing a patient-centered approach to postnatal care interventions. This study aims to derive post-discharge risk prediction algorithms that identify mother-newborn dyads who are at risk of re-admission or death in the first six weeks after delivery at a health facility.
Methods: This prospective observational study will enroll 7,000 mother-newborn dyads from two regional referral hospitals in southwestern and eastern Uganda. Women and adolescent girls aged 12 and above delivering singletons and twins at the study hospitals will be eligible to participate. Candidate predictor variables will be collected prospectively by research nurses. Outcomes will be captured six weeks following delivery through a follow-up phone call, or an in-person visit if not reachable by phone. Two separate sets of prediction models will be built, one set of models for newborn outcomes and one set for maternal outcomes. Derivation of models will be based on optimization of the area under the receiver operator curve (AUROC) and specificity using an elastic net regression modelling approach. Internal validation will be conducted using 10-fold cross-validation. Our focus will be on the development of parsimonious models (5–10 predictor variables) with high sensitivity (>80%). AUROC, sensitivity, and specificity will be reported for each model, along with positive and negative predictive values.
Discussion: The current recommendations for routine postnatal care are largely absent of benefit to most mothers and newborns due to poor adherence. Data-driven improvements to postnatal care can facilitate a more patient-centered approach to such care. Increasing digitization of facility care across low-income settings can further facilitate the integration of prediction algorithms as decision support tools for routine care, leading to improved quality and efficiency. Such strategies are urgently required to improve newborn and maternal postnatal outcomes.
Clinical trial registration: https://clinicaltrials.gov/, identifier (NCT05730387).
Worldwide, approximately 290,000 maternal and 2.4 million neonate deaths occurred in 2020 (1, 2). Sub-Saharan Africa accounts for the largest burden of these deaths, which could be prevented through improved care coverage and quality (2, 3). While important global efforts are underway to improve outcomes immediately following birth, care following facility discharge remains a challenge. The postnatal period accounts for a high proportion of overall maternal and neonatal morbidity, representing a time of exceptional risk for mothers and their infants (4).
In facilities across sub-Saharan Africa, women and their newborn infants are routinely discharged from facility within 24 h of birth. Yet, 30% of mothers and 55% of newborns who die during the first 6 weeks do so more than 24 h after birth, with deaths often occurring within the community setting (5, 6). Despite this, studies focusing specifically on the post-discharge period following delivery, are rare (7, 8). Understanding the risk factors for maternal and newborns complications and death during the post-discharge period is an important first step to designing effective interventions.
Furthermore, maternal and neonate outcomes are inextricably connected. Recent evidence suggests maternal mortality and complications are associated with neonatal mortality and failure to thrive (9–11). Hence, considering the mother and child as a pair or dyad, offers an opportunity to potentially prevent interrelated causes of postpartum maternal and neonate complications (12). However, this approach has rarely been utilized in such studies.
The settings most affected by high rates of post-discharge morbidity and mortality suffer from overburdened and underinvested health systems and impoverished communities. Together, these greatly hinder adherence to the recommended frequency of postnatal visits resulting in many mothers and newborns not receiving timely lifesaving interventions (13). Currently, the World Health Organization (WHO) recommends three in-person postnatal visits for all mothers and newborn infants born at a health facility within the first six weeks of life (14). However, achieving sufficient postpartum follow-up care remains a major challenge in low-income settings, with a significant proportion of mothers and newborns not receiving even a single follow-up visit prior to the first 6-week newborn vaccination (13).
Given the persistent challenges in achieving high levels of post-partum care for mothers and newborns, as well as significant resource challenges within health facilities, there is an important opportunity to tailor recommendations for timing and frequency of follow-up to individual risk (15). This not only conserves the use of scarce resources but allows health workers to emphasize the importance of follow-up with individualized data on risk. Personalized risk scores can help frontline healthcare providers identify high-risk dyads before discharge from hospital, and guide recommendations for essential postnatal care.
The aim of this study, therefore, is to derive post-discharge risk prediction algorithms that identify high-risk dyads prior to hospital discharge, following facility birth. The ultimate goal of this work is to combine risk prediction algorithms with interventions that target prevention or treatment of critical causes of death or illness, inform evidence-based recommendations for postnatal care (PNC), and improve health outcomes for dyads.
This prospective observational study will enroll mother and newborn dyads from two regional referral hospitals in Uganda: The Mbarara Regional Referral Hospital in southwestern Uganda and Jinja Regional Referral Hospital in eastern Uganda. These two facilities serve a catchment covering 2 districts and a population of approximately 973,000 individuals. Together they provide a reasonable representation of the Ugandan population outside of the capital city of Kampala. Study results will be reported using the TRIPOD Checklist for Prediction Model Development and Validation (https://www.tripod-statement.org/) (Supplementary Data Sheet 1) and the STROBE Checklist for Cohort Studies (https://www.strobe-statement.org/) (Supplementary Data Sheet 2).
This study will be conducted between April 2022 and September 2023, and will enroll women and adolescent girls aged 12 and above delivering single or multiple babies. Only participants living in districts within the catchment area will be eligible for inclusion. Exclusion criteria includes those unable to speak the dominant local languages (Runyankole or Lusoga), refusal or inability to provide consent, residing in a refugee camp, as well as those with no access to a phone during the post-discharge period.
A systematic sampling method for participant selection based on time of arrival will be used to reduce sampling bias. In order to capture a representative sample of all patients arriving within a 24-h period, the proportion of day and night admissions will be determined using hospital records. We will define daytime admissions as patients admitted for delivery between 8am and 8pm, and nighttime admissions as patients admitted for delivery between 8pm and 8am. Nighttime admissions will be assigned numbers based on order of arrival taken from hospital records and proportionately and randomly screened and selected using a random number generator application installed on an android tablet on the morning following their arrival. If the patient is not eligible for enrolment, nurses will continue using the random generator until the target for night enrolment is met. Daytime admissions will be screened and selected using time cut-offs whereby study nurses will be instructed to screen the first patient arriving after each 30-min interval. If the screened patient is not eligible, the next patient arriving after the time cut-off will be selected. These intervals will be staggered on shifts with multiple nurses to improve efficiency and length will be determined based on time spent with each patient during the screening, consenting and enrolment process. The daytime and nighttime assignments will be implemented for practical reasons to accommodate ward staffing, as well as to ensure budget efficiency. This process will allow us to capture a pseudo-random sample that was representative of admissions for delivery within a 24-h period, and not weighted towards either daytime or nighttime arrivals.
Research nurses will recruit and obtain consent from eligible women after they have been admitted to the facility for delivery and prior to discharge. Eligible women will be informed of the study and asked if they wish to participate. If the eligible participant is a minor, the parent or legal guardians(s) of the participant will be approached first by the research nurse. In accordance with the expectations of the Uganda National Council for Science and Technology Research Guidelines for Research involving Humans, consent will not be sought until after the patient has received an initial assessment by health workers at the time of admission for delivery, and research nurses may wait until after delivery to approach eligible women so as to not interfere with standard care. Women who suffer a loss or who are caring for a severely ill infant will be given the option to defer the interview portion of data collection until the six-week postnatal follow-up period. During the consenting process, all women will be told they are free to withdraw from the study at any point without needing to give a reason for withdrawal. Data collected up to the point of withdrawal will be de-identified and retained for analysis.
Following informed consent of the mother, data collection will be represented by four data collection periods: Admission, delivery, discharge and 6-week post-discharge follow-up (Figure 1) (16). We will prioritize data collection from the hospital medical record, followed by interviews with the mother and finally confirmation with the medical team if there are discrepancies, missing information, or questions the mother is unable to answer. For the admission data collection period, the study team will collect data related to both pregnancy history (e.g., parity and co-morbidities), admission data (e.g., vital signs) and basic demographic details (e.g., age and socio-economic details) (Supplementary Data Sheet 3). The delivery phase will represent the delivery details of both the mother (e.g., delivery mode) and the newborn (e.g., resuscitation and birth weight). At discharge, we will obtain and record clinical data for mothers and their newborns discharged alive from the hospital. Blood pressure will be measured using a Microlife Cradle VSA semi-automated blood pressure monitor (Microlife Corporation, Widnau, Switzerland). Oxygen saturation (SpO2) and heart rate will be collected using the Masimo iSpO2® (Masimo Corporation, California, USA) and Nellcor Oxicable (Medtronic, Minnesota, USA), and respiratory rates will be measured using the RRate Application (17, 18). Maternal hematocrit will be determined using a microhematocrit centrifuge. Anthropometric data of infants (length and weight) will also be measured and recorded by study nurses. All dyads will receive routine care during admission and are discharged at the discretion of their medical teams. In cases where study nurses note danger signs while collecting discharge measurements referrals to the pediatric unit will be made and recorded.
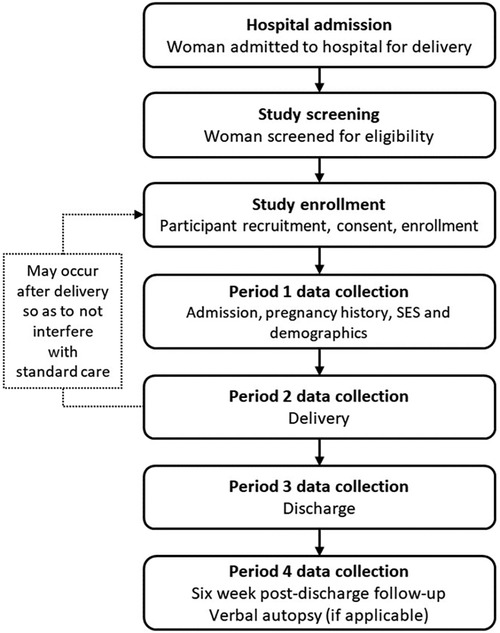
Figure 1. Study procedures.
Six weeks following discharge, all mothers will be contacted by phone for the follow-up data collection phase which will capture outcomes, including health seeking, re-admissions and deaths. Verbal autopsies will be conducted in all cases of maternal or newborn death at least one month after a death has occurred. In the event that the mother has died, verbal autopsy data will be collected from the study participant's spouse or other family member. If study participants cannot be reached by phone they will be followed up in person by field officers in order to reduce loss to follow-up.
Candidate predictor variables were selected based on results from a pilot study conducted at Mbarara Regional Referral Hospital (2019–2020) (15) and updated using literature and consultation with experts on the study team to ensure variables were likely to be predictive and available in low-resourced settings.
We will build two separate sets of prediction models to predict re-admission or death within six weeks of hospital discharge. The primary outcome for the first set of models will be newborn death or readmission while the primary outcome for the second will be maternal death or readmission. Secondary outcomes will include a list of risk factors associated with death and readmission among mothers and newborns, the proportion of mothers and newborns receiving routine postnatal care as well as predictors of postnatal care visits.
With a sample size of 6,700 and expected outcome rates of 2.7% for mothers and 4.4% for newborns, we will be able to measure the prevalence of maternal and newborn hospital readmission or death within a margin of error of 1%. We will be able to develop prediction models with up to 30 candidate predictors for both maternal and newborn outcomes separately, ensuring a mean absolute prediction error of no more than 1%, a uniform shrinkage factor of 90%, a Cox-Snell R2 value of at least 0.10, a maximum R2 of 0.05 and expected optimism of 0.05. The R2 value and number of predictor variables are based on findings from our epidemiological study.
We will summarise all risk factors for mothers and newborns that do and do not experience poor outcomes and estimate univariate associations. For newborns, data will be reported by sex. Derivation of prediction models will be based on optimization of the AUROC and specificity using elastic net regression. Internal validation will be assessed using 10-fold cross validation (19, 20). As in our other cohorts, we will focus on developing parsimonious predictive models (e.g., 5–10 predictor variables) with high sensitivity (>80%). This reduces false negatives and maximizes its use in resource-limited settings where frontline health workers are the main providers of postnatal care. AUROC, sensitivity, and specificity will be reported for each model, along with positive and negative predictive values. Site specific metrics will be compared to ensure consistency across settings, and recalibration may be considered if individual site performance is lower than expected. Finally, we will assess combined sensitivity and specificity when each individual model is applied to the dyad. Outside of prediction modelling, our sample size will allow us to detect an odds ratio of at least 1.30 for a given risk factor with 80% power and 5% significance and relative precision of 25%.
Study data will be managed using customized Research Electronic Data Capture (REDCap) tools hosted at the University of British Columbia, with secure access by all investigators in Uganda and Canada. REDCap is a secure, web-based application designed to support data capture for research studies. Data will be entered into the REDCap database by a trained research nurse or research assistant after each activity is completed and audio recordings are transcribed.
After the study period, a de-identified copy of the data will be prepared for deposition in a repository with open access with proper governance mechanisms. We will make every effort to prevent re-identification of subjects by coding data that has the potential of being identifiable.
Using a prospective cohort of women delivering at two regional referral hospitals in Uganda, this study aims to derive risk prediction models for post-discharge mortality among mother-newborn dyads. A large proportion of post-discharge deaths occurring during the postnatal period are treatable and preventable through early recognition and high-quality care, fostering an emphasis on facility births and ongoing postnatal care as an early intervention (6, 21, 22). Despite the three recommended postnatal care visits in the first six weeks after delivery (14), only 7%–10% of postpartum women and approximately one third of newborns attend at least one postnatal care visit in Uganda (23–25). New approaches to postnatal care are therefore urgently required to improve maternal and infant outcomes during the postnatal period.
Precision health is a strategy that focuses on individualized assessment to optimize care provision at the patient level. Our previous work in pediatric sepsis has shown that linking the risk of post-discharge mortality to the intensity of discharge and post-discharge care has the potential to improve outcomes and also increase care compliance during the post-discharge period (26–28). By enabling effective allocation of scarce resources, such approaches are more likely to be sustainable in economically strained countries.
Building a tool to assess risk must consider the context in which it is to be implemented. In resource limited settings, a key consideration is that the variables used to assess risk (i.e., the candidate predictor variables) should be simple, objective and easily collected during routine care. Second, these tools must be functionally capable of integrating into routine care processes. As health systems in low-resourced settings increasingly adopt digital health systems, the integration of algorithms to augment clinical decisions (such as follow-up intensity) is becoming increasingly feasible (29, 30). As such, the traditional paper-based approaches to risk classification will be replaced by data-driven approaches such as algorithmic scoring. Our analysis plan and algorithmic output is especially conducive to such an approach. Through EMR integration, risk-prediction algorithms tied to effective care pathways have potential to both improve care and resource efficiency, both being critical in settings with low resources and high disease burden.
Individualized risk assessment in the absence of effective interventions is of limited utility. Likewise, an effective intervention in the absence of adherence is also of limited utility. The current recommendations for routine postnatal care, even if effective, are largely absent of benefit to the vast majority of mothers and newborns due to poor adherence. Improved timing of these visits, alongside a more personalized intensity of these visits, may both improve outcomes and adherence. Indeed, risk communication itself may influence outcomes, especially for those at risk who may not accurately perceive their own risk (31, 32). There is currently no way to accurately prognosticate risk among a general population of mothers and newborns. There is a dearth of literature in low-income countries examining overlapping outcomes and care seeking between mothers and infants during the postnatal period which we hope to address (33, 34). Using the data generated from this study, we aim to develop, plan and implement patient centered interventions to reduce mortality and readmission in the postnatal period in low-resourced settings.
This study is subject to several potential limitations. First, loss to follow-up may reduce our effective sample size, thus diminishing our power to detect significance in some variables. The exclusion criteria of no access to a mobile phone will improve follow-up potential, though this does limit generalizability to those with no phone access, who themselves may be more vulnerable. Our prior work, however, suggests that while many women do not own their own phone, fewer than 1% do not have access to a phone. Our prior work doing similar studies also suggests that our loss to follow-up will be less than 5%. Furthermore, our study sample size has compensated for potential loss to follow-up, thus we do not anticipate this to be an issue. Second, heterogeneity in outcomes may impact modelling of post-discharge events. We observed this to be a potential limitation in our prior work as predictors were different between newborns and mothers, and between mothers with caesarean sections and those who delivered vaginally. Therefore, we calculated our sample size estimates to be able to model at least 3 separate outcomes. We anticipate that this will be sufficient to create a set of models which are comprehensive to capture various outcomes. Finally, this study is limited to a single country, which limits its generalizability beyond Uganda. However, it is our intent to expand and validate in other countries if model building is successful in this study.
Ethics approvals have been obtained from the Makerere University School of Public Health (MakSPH) Institutional Review Board (SPH-2021-177), the Uganda National Council of Science and Technology (UNCST) in Uganda (HS2174ES) and the University of British Columbia in Canada (H21-03709).
Conceptualization: MOW, NK-M, JA, NK, BAP, MV, AC-D, and JN. Funding Acquisition: MOW and JN. Methodology: MOW, YP, VN, and JN. Supervision: MOW and JN. Writing Original Draft: YP, MOW, JT, NK-M, and JN. Writing-Review and Editing: MOW, YP, JN, VN, JT, CK, NK-M, AN, LMB, JA, NK, BAP, MV, AC-D, PML, and JB. All authors contributed to the article and approved the submitted version.
Funding for this study is from the Canadian Institutes for Health Research (CIHR) (AWD-019909) through the University of British Columbia (UBC) in Canada. YP and MW have received salary support through the Michael Smith Health Research BC (MSHR BC) (RT-2022-2583; SCH-2021-1581) through UBC. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors JN, PML, MV, JMA, and MOW declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fepid.2023.1233323/full#supplementary-material
Supplementary Data Sheet 1
TRIPOD Checklist
Supplementary Data Sheet 2
STROBE Statement Checklist
Supplementary Data Sheet 3
Data Dictionary
1. World Health Organization. Newborn Mortality. (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-mortality-report-2021 (Accessed May 5, 2023).
2. World Health Organization. Maternal Mortality. (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (Accessed May 1, 2023).
3. Countdown to 2030 Collaboration. Countdown to 2030: tracking progress towards universal coverage for reproductive, maternal, newborn, and child health. Lancet. (2018) 391(10129):1538–48. doi: 10.1016/S0140-6736(18)30104-1
4. World Health Organization. WHO recommendations on postnatal care of the mother and newborn. Geneva PP—Geneva: World Health Organization. (2014). Available at: https://apps.who.int/iris/handle/10665/97603 (Accessed May 5, 2023).
5. Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and Sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. (2018) 6(12):e1297–308. doi: 10.1016/S2214-109X(18)30385-1
6. Say L, Chou D, Gemmill A, Tunçalp Ö, Moller A-B, Daniels J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Heal. (2014) 2(6):e323–33. doi: 10.1016/S2214-109X(14)70227-X
7. Willcox ML, Kumbakumba E, Diallo D, Mubangizi V, Kirabira P, Nakaggwa F, et al. Circumstances of child deaths in Mali and Uganda: a community-based confidential enquiry. Lancet Glob Heal. (2018) 6(6):e691–702. doi: 10.1016/S2214-109X(18)30215-8
8. Symonds NE, Vidler M, Wiens MO, Omar S, English LL, Ukah UV, et al. Risk factors for postpartum maternal mortality and hospital readmission in low- and middle-income countries: a systematic review. BMC Pregnancy Childbirth. (2023) 23(1):303. doi: 10.1186/s12884-023-05459-y
9. Finlay JE, Moucheraud C, Goshev S, Levira F, Mrema S, Canning D, et al. The effects of maternal mortality on infant and child survival in rural Tanzania: a cohort study. Matern Child Health J. (2015) 19(11):2393–402. doi: 10.1007/s10995-015-1758-2
10. Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet. (2005) 365(9462):891–900. doi: 10.1016/S0140-6736(05)71048-5
11. Moucheraud C, Worku A, Molla M, Finlay JE, Leaning J, Yamin A. Consequences of maternal mortality on infant and child survival: a 25-year longitudinal analysis in Butajira Ethiopia (1987-2011). Reprod Health. (2015) 12(Suppl 1):S4. doi: 10.1186/1742-4755-12-S1-S4
12. World Health Organization, World Bank, United Nations Population Fund, United Nations Children’s Fund (UNICEF). Trends in maternal mortality: 1990 to 2010: WHO, UNICEF, UNFPA and The World Bank estimates. World Health Organization. (2012). Available at: https://apps.who.int/iris/handle/10665/44874 (Accessed May 5, 2023).
13. Tessema ZT, Yazachew L, Tesema GA, Teshale AB. Determinants of postnatal care utilization in sub-saharan Africa: a meta and multilevel analysis of data from 36 Sub-Saharan countries. Ital J Pediatr. (2020) 46(1):175. doi: 10.1186/s13052-020-00944-y
14. Wojcieszek AM, Bonet M, Portela A, Althabe F, Bahl R, Chowdhary N, et al. WHO Recommendations on maternal and newborn care for a positive postnatal experience: strengthening the maternal and newborn care continuum. BMJ Glob Heal. (2023) 8(Suppl 2):e010992. doi: 10.1136/bmjgh-2022-010992
15. Pillay Y, Ngonzi J, Bone J, Christoffersen-Deb A, Vidler M. Payne BA, et al. PP114 [Global health » Resource limited settings]: SMART DISCHARGES FOR MOM+BABY: IDENTIFYING VULNERABLE DYADS TO GUIDE DELIVERY OF POST-DISCHARGE CARE. Pediatric Critical Care Medicine. (2022) 23(Supplement 1 11S). doi: 10.1097/01.pcc.0000900368.62030.76
16. Wiens MO, Kenya-Mugisha N, Namala A, Tagoola A, Bebell L, Pillay Y, et al. Smart discharges for mom & baby: a cohort study to develop prognostic algorithms for post-discharge readmission and mortality among mother-infant dyads. Borealis. (2023). doi: 10.5683/SP3/EIUHJF
17. Dunsmuir D, Karlen W, Gan H, Chiu M, Petersen C, Dumont G, et al. A Mobile application for measuring respiratory rate. Conference: canadian pediatric anesthesia society (CPAS) meeting 2014; Montreal, QC (2014).
18. Dunsmuir D, Petersen C, Karlen W, Dumont GA, Ansermino J. The phone oximeter for Mobile spot-check. Annual meeting of the society for technology in anesthesia (STA 2012); Florida: Palm Beach (2012).
19. Stone M. An asymptotic equivalence of choice of model by cross-validation and Akaike’s criterion. J R Stat Soc Ser B. (1977) 39(1):44–7. doi: 10.1111/j.2517-6161.1977.tb01603.x
20. Shibata R. Bootstrap estimate of Kullback-Leibler information model selection. StatSin. (1997) 7:375–94. Available at: https://www3.stat.sinica.edu.tw/statistica/oldpdf/A7n27.pdf (Accessed May 5, 2023).
21. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. (2015) 385(9963):117–71. doi: 10.1016/S0140-6736(14)61682-2
22. Campbell OMR, Cegolon L, Macleod D, Benova L. Length of stay after childbirth in 92 countries and associated factors in 30 low- and middle-income countries: compilation of reported data and a cross-sectional analysis from nationally representative surveys. PLoS Med. (2016) 13(3):e1001972. doi: 10.1371/journal.pmed.1001972
23. Ndugga P, Namiyonga NK, Sebuwufu D. Determinants of early postnatal care attendance: analysis of the 2016 Uganda demographic and health survey. BMC Pregnancy Childbirth. (2020) 20(1):163. doi: 10.1186/s12884-020-02866-3
24. Sserwanja Q, Mukunya D, Nabachenje P, Kemigisa A, Kiondo P, Wandabwa JN, et al. Continuum of care for maternal health in Uganda: a national cross-sectional study. PLoS One. (2022) 17(2):e0264190. doi: 10.1371/journal.pone.0264190
25. Arunda MO, Agardh A, Asamoah BO. Determinants of continued maternal care seeking during pregnancy, birth and postnatal and associated neonatal survival outcomes in Kenya and Uganda: analysis of cross-sectional, demographic and health surveys data. BMJ Open. (2021) 11(12):e054136. doi: 10.1136/bmjopen-2021-054136
26. Wiens MO, Kumbakumba E, Larson CP, Moschovis PP, Barigye C, Kabakyenga J, et al. Scheduled follow-up referrals and simple prevention kits including counseling to improve post-discharge outcomes among children in Uganda: a proof-of-concept study. Glob Heal Sci Pract. (2016) 4(3):422–34. doi: 10.9745/GHSP-D-16-00069
27. Wiens MO, Kissoon N, Kabakyenga J. Smart hospital discharges to address a neglected epidemic in sepsis in low- and middle-income countries. JAMA Pediatr. (2018) 172(3):213. doi: 10.1001/jamapediatrics.2017.4519
28. Wiens MO, Kumbakumba E, Larson CP, Ansermino JM, Singer J, Kissoon N, et al. Postdischarge mortality in children with acute infectious diseases: derivation of postdischarge mortality prediction models. BMJ Open. (2015) 5(11):e009449. doi: 10.1136/bmjopen-2015-009449
29. Mitchell M, Kan L. Digital technology and the future of health systems. Heal Syst Reform. (2019) 5(2):113–20. doi: 10.1080/23288604.2019.1583040
30. Sharma V, Ali I, van der Veer S, Martin G, Ainsworth J, Augustine T. Adoption of clinical risk prediction tools is limited by a lack of integration with electronic health records. BMJ Health Care Inform. (2021) 28(1):e100253. doi: 10.1136/bmjhci-2020-100253
31. Rysavy MA. Prognosis as an intervention. Clin Perinatol. (2018) 45(2):231–40. doi: 10.1016/j.clp.2018.01.009
32. Zipkin DA, Umscheid CA, Keating NL, Allen E, Aung K, Beyth R, et al. Evidence-based risk communication. Ann Intern Med. (2014) 161(4):270–80. doi: 10.7326/M14-0295
33. de Groot N, Birnie E, Vermolen JH, Dorscheidt JJA, Bonsel GJ. The prevalence of adverse postnatal outcomes for mother and infant in The Netherlands. PLoS One. (2018) 13(9):e0202960. doi: 10.1371/journal.pone.0202960
Keywords: sepsis, discharge, post-discharge, maternal health, neonatal health
Citation: Wiens MO, Trawin J, Pillay Y, Nguyen V, Komugisha C, Kenya-Mugisha N, Namala A, Bebell LM, Ansermino JM, Kissoon N, Payne BA, Vidler M, Christoffersen-Deb A, Lavoie PM and Ngonzi J (2023) Prognostic algorithms for post-discharge readmission and mortality among mother-infant dyads: an observational study protocol. Front. Epidemiol. 3:1233323. doi: 10.3389/fepid.2023.1233323
Received: 1 June 2023; Accepted: 13 November 2023;
Published: 29 November 2023.
Edited by:
Juan Manuel Mejia-Arangure, Universidad Nacional Autonoma de Mexico, MexicoReviewed by:
Adenike Ogah, University of Zambia, Zambia© 2023 Wiens, Trawin, Pillay, Nguyen, Komugisha, Kenya-Mugisha, Namala, Bebell, Ansermino, Kissoon, Payne, Vidler, Christoffersen-Deb, Lavoie and Ngonzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthew O. Wiens bWF0dGhldy53aWVuc0BiY2Noci5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.