
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Epidemiol. , 22 August 2023
Sec. Infectious Disease Epidemiology
Volume 3 - 2023 | https://doi.org/10.3389/fepid.2023.1193369
This article is part of the Research Topic Long Covid: A New Chronic Disease? Understanding a Multi-faceted Condition View all 6 articles
 Raquel Gómez Bravo1,2
Raquel Gómez Bravo1,2 Alexandre Infanti2
Alexandre Infanti2 Joël Billieux3Mark Ritzen1Psy-Long-COVID Consortium
Joël Billieux3Mark Ritzen1Psy-Long-COVID Consortium Claus Vögele2,†Charles Benoy1,4,5*†
Claus Vögele2,†Charles Benoy1,4,5*†
Introduction: Chronic post-viral syndromes, including Long-COVID, are characterized by a range of persistent symptoms that occur following a viral infection. Psychological symptoms are prevalent in Long-COVID patients and can have a significant impact on their quality of life. However, the specific patterns of psychological symptoms, their associations with physical symptoms, and the factors predicting their severity remain poorly understood.
Aims: This study aims to explore and systematically assess psychological symptoms in Long-COVID, to identify syndrome clusters based on these symptoms, to examine their relationship with physical symptoms, and to investigate the influence of pandemic-related variables.
Methods: Descriptive, cross-sectional study with data collected through an online questionnaire across several EU countries, from February 2020 to December 2022. Participants were recruited using public relations, the social media and information campaigns directed at the public and health professionals using snowball sampling.
Results: The findings will allow to phenotype Long-COVID related psychological symptom clusters based on self-reports. facilitating improved assessment and treatment approaches.
Conclusions: The results will provide important knowledge for the public health management of the public healh management of Long COVID. The findings will contribute to a better understanding of the psychological symptoms associated with Long-COVID and the development of specific treatment guidelines for psychological burden associated with Long-COVID, thereby supporting management strategies to combat the after-effects of the COVID-19 pandemic, enhancing their overall well-being and quality of life.
Chronic post-viral syndromes refer to a range of symptoms that persist for a prolonged period after a person has recovered from a viral infection. These symptoms can include physical, psychological, and neuropsychological symptoms, which are common and have a significant impact on individuals’ quality of life, ability to work or attend school, and their mental health. For example, chronic Post-SARS (Severe Acute Respiratory Syndrome) that emerged from South East Asia in early 2003, was characterized by persistent fatigue, diffuse myalgia, weakness, depression and non-restorative sleep (1). These symptoms can vary widely, involving either one or more persistent COVID-19 related symptoms, or even new symptoms, and occurring weeks and months after the infection. They have been described under the terms Long-COVID or Post-COVID (2).
Long-COVID may result in long-term disability or chronic illness. A considerable proportion of Long-COVID patients report persistent distress and impairment in their global level of functioning (3). In a Swedish study (initially investigating long-term immunity after mild COVID-19), it was found that even low risk individuals with mild COVID-19 reported a range of long-term symptoms that disrupted work, social and home life (4).
The prevalence of Long-COVID-syndrome varies widely depending on the population studied, the length of time used to define persistence of symptoms and study design. In a recent study published in January 2023, it has been estimated that 50%–70% of hospitalized cases and 10%–30% of COVID-19 non-hospitalized patients experience long-term symptoms (2, 5–7). Further research is needed to better understand not only the prevalence, risk factors, and long-term outcomes of Long COVID, but also the underlying mechanisms to develop effective treatments. Several post-COVID syndrome categories have been described, including multisystemic physical, persistent psychological and neuropsychological symptoms [e.g., (3, 8, 9)].
Even though the available evidence has methodological limitations, a recent systematic review and a meta-analysis suggest that fatigue and sleep disturbance are the most prevalent symptoms in Long-COVID syndrome (10, 11). Other frequently reported symptoms include anxiety, depression or other mental health conditions, headaches, cognitive impairment (also known as “brain fog”), loss of concentration, and muscle aches/myalgia (3, 4, 8, 12–14). In a retrospective cohort study of 273.618 survivors of COVID-19, Taquet et al. (15) found that anxiety and depression were the most common features of Long-COVID. They also observed higher incidences of cognitive symptoms in the elderly and in hospitalized patients or intensive treatment unit (ITU) patients. The prevalence of persistent symptoms was higher after COVID 19 compared to influenza, suggesting that the infection with SARS-CoV-2 might be involved (15).
Some studies suggest similarities between the clinical presentation of Long-COVID syndrome and the better-known Myalgic Encephalomyelitis/Chronic Fatigue syndrome (ME/CFS). It is important to note that Long-COVID is a newly recognized condition, and the underlying mechanisms are still not well understood. It remains unclear, therefore, whether they are the result of direct neurological damage from the virus, immune system dysregulation or other factors and their long-term implications. Current evidence seems to suggest that both viral and host factors may play a role. For example, viral factors such as persistent viral replication or ongoing immune activation may contribute to ongoing symptoms. Host factors such as genetics, age, and pre-existing medical conditions may also influence an individual's susceptibility to developing chronic post-viral symptoms. In addition, there are some differences in the clinical presentation of Long-COVID and ME/CFS, and the two conditions may have different underlying causes (2). Nevertheless, the similarities between the two conditions suggest that there may be some overlap in the mechanisms that lead to chronic post-viral syndromes (16, 17).
As described in the previous section, the current evidence shows a high number of long-COVID patients with psychological symptoms [e.g., (15)]. Although little is known about the risk factors for persistent psychological symptoms associated with Long-COVID, the currently most widely accepted factors include the severity of COVID-19, female sex, a history of mental disorders, the presence of comorbidities, and elevated levels of inflammatory markers. In a similar vein, the pathophysiological mechanisms underlying Long-COVID remain only partially explained, whereas the role of other factors for the development of Long-COVID, for example those associated with the treatment of COVID-19 (e.g., ITU admission), has not been investigated yet. The potential impact of indirect effects of the COVID-19 pandemic such as uncertainty, social isolation, financial constraints, and health recovery on Long-COVID has been highlighted but also remains largely unexplored (18, 19).
In summary, (1) a considerable proportion of individuals who are diagnosed with COVID-19 report a Long-COVID syndrome, (2) this syndrome includes a range of physical, psychological and neuropsychological symptoms, (3) the incidence of psychological symptoms in Long-COVID is high, and (4) these syndromes have not yet been sufficiently and adequately assessed.
In general, it is well established that many patients with physical diseases also experience psychological symptoms or even have a mental disorder comorbid with the physical condition (20). This may be (1) a direct result of pathophysiological processes associated with the physical condition, (2) be indirectly linked as an indirect consequence of the challenging situation of being diagnosed with a physical condition, (3) be a result of medical interventions to treat the physical condition, or (4) present an interaction of any of these (21). The present study aims to identify patterns of psychological symptoms that are specific for Long-COVID, thus contributing to better assessment and treatment.
The overall research goals concern the exploration and systematic assessment of psychological symptoms of Long-COVID and the factors associated with it.
Specific objectives are:
1) To describe different syndromes associated with psychological symptoms in relation with Long-COVID and generate different groups based on their psychological symptoms (anxiety, depression and somatoform disorders)
2) To investigate whether these syndrome clusters differ in relation to physical symptoms.
3) To examine whether syndrome clusters show differences in terms of other pandemic-related variables, including psychosocial and medical factors.
Data on the psychological symptoms of Long-COVID were collected using an online survey from February 2020 to December 2022. The project will allow for the retrospective assessment of predictive factors, which are associated with more severe mental health symptoms linked to a Post Covid syndrome (e.g., pre-existing mental disorders, social context, other treatments, blood type).
This study involves an online, descriptive, cross-sectional survey including 184 items. Participation was voluntary, anonymous and could be withdrawn at any time. The questionnaire was available in German and French. Its completion took 30 min on average.
Questions asked covered a broad range of psychological symptoms (e.g., depression, overall anxiety, specific anxiety, fatigue, impact of health on life quality, perceived stress, traumatic experiences, somatic symptoms experiences) and person- and pandemic-related factors (e.g., sociodemographic factors, vaccination status, time of infection, acute phase, acute treatment setting, health-related factors, impact of the pandemic on several domains of personal life). To control for the effects of pre-existing conditions, we included a comprehensive assessment of possibly confounding variables in the survey. In addition, a range of possible risk factors that may have chronologically preceded the Coronavirus infection were also collected (Table 1).
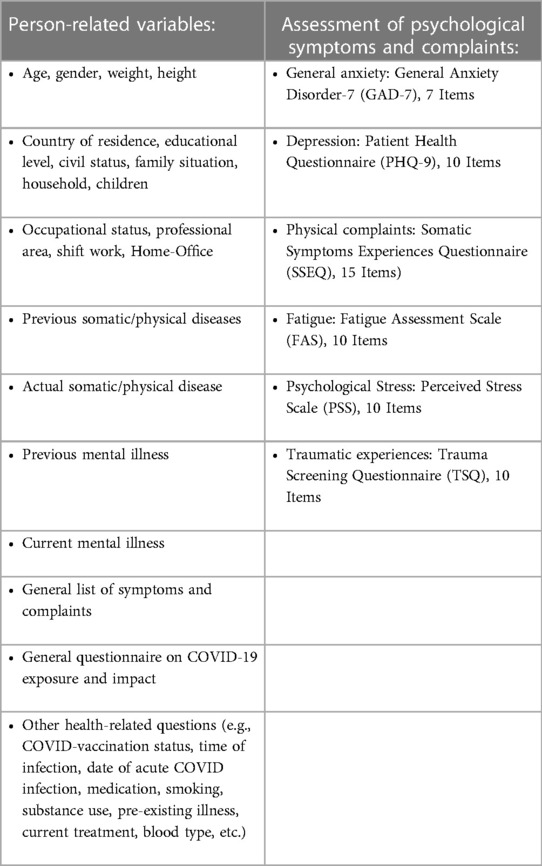
Table 1. Variable groups collected.
Participants were recruited through public relations and information campaigns directed at the public and to health professionals. In addition, we collaborated with several Long-COVID units, intensive care units, infectious diseases departments and mental health care departments (e.g., psychiatry departments), so that individuals with Long-COVID were directly referred to the present study. This study is part of a multi-center and international project, and the procedure was the same in all participating institutions.
Snowball sampling was used to conduct this research.
Any volunteer was welcome to participate in this project. For the present study, respondents were selected according to the WHO definition of Long COVID: those experiencing new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months without other explanation (22).
Data analysis and interpretation of the results will be carried out from January to April 2023.
We will compute a cluster analysis following the recommendations provided by Hair et al. (23), which consist of combining hierarchical and non-hierarchical approaches. For the cluster generation, we will use the total scores of the GAD-7, PHQ-4 (PHQ-9 excluding items which refer to physical symptoms), and all the SEEQ dimensions. These variables will be scaled and centered for the analyses. Before running the cluster analyses, it will be ensured that no collinearity between these variables exists, and the distribution the scales verified. Hierarchical clustering will provide us with a suggested number of clusters using the Ward method with squared Euclidian distances. To obtain a suggested number of clusters, the NbClust R package (24) will be used. In this package, several indices are computed (kl, ch, hartigan, ccc, scott, marriot, trcovw, tracew, friedman, rubin, cindex, db, silhouette, duda, pseudot2, beale, ratkowsky, ball, ptbiserial, frey, mcclain, dunn, hubert, sdindex, dindex, sdbw). For each index, a suggested number of clusters will be obtained, the most outstanding suggested number of clusters is then highlighted and recommended for further steps (non-hierarchical clustering). Once the suggested number of clusters is obtained, we will assess its relevance for our main assumptions to decide the final number of clusters to generate. Then, the generation of the clusters will be followed by non-hierarchical K-means cluster analysis. As an alternative solution, a supervised machine learning model called Affinity Propagation will be computed. This model is relevant since it represents a completely data driven approach method. Unlike other clustering algorithms, such as K-means, Affinity Propagation does not require the number of clusters to be pre-defined. Instead, the algorithm automatically determines the number of clusters from a data driven perspective. The algorithm works by iteratively exchanging messages between data points, which convey information about how well one data point can serve as an exemplar for another data point. The messages are used to update the availability and responsibility matrices, which represents the confidence that a data point has in its potential exemplar and the confidence that an exemplar has in its responsibility to represent a particular data point. During each iteration, the availability and responsibility matrices are updated until they converge to a stable solution. The exemplars for the data points are determined by finding the data points with the highest net responsibility. The results of both cluster generation approaches will then be compared regarding their scores on the PHQ-4 (without physical symptoms), GAD-7, and SSEQ dimensions. The more relevant cluster solution will be chosen for further analyses.
To compare the clusters regarding physical symptoms, we will compute a contingency table and report Chi-Squared tests, Cramer's V and effect sizes. Moreover, we will compute post hoc analyses using the chisq.post hoc.test R package (25) which uses Bonferroni correction, and is based on residuals of Pearson's Chi-squared Test for Count Data.
The same procedure will be applied to examine whether syndrome clusters show differences in terms of other pandemic-related variables, including psychosocial and medical factors. If the external variables are continuous, a Kruskal–Wallis test will be computed with Dunn's test as post hoc analysis with Bonferroni correction.
- Ethical approval
The study was conducted according to the guidelines laid down in the Declaration of Helsinki. Ethical approval was not required as non-identifiable data was collected anonymously. This was confirmed by the respective responsible institutions [for example Ethical Commission of the Max-Planck-Institut für Psychiatrie, Munich, Germany, the Ethics Committee for Northwest and Central Switzerland (EKNZ) and the Ministry of Health Luxembourg].
- Participants’ information and consent
Online informed consent was requested from all participants before starting the questionnaire, including the right to withdraw from the study at any point. Volunteers did not receive any incentive for their participation.
If participants wished to be informed of the results of the project and relevant publications, they could contact the principal investigator through the contact provided in the online survey.
At the end of the study, participants could create a personal and completely anonymous code. If they wished to be informed of their own results, participants could receive these by sending this code to an email address, explicitly requesting this information (total scores of the questionnaires as well as an explanation of the interpretation scheme of the results).
- Data protection
Data was collected anonymously through the UNIPARK online software (www.unipark.com), taking into ccount the EU GDPR. The online survey was implemented via the following link: https://ww3.unipark.de/uc/long-covid/. IP addresses were not collected, and the data gathered did not allow for the identification of respondents.
Upon completion of data collection, data was downloaded and stored on a centrally managed server at the University of Luxembourg (UL). Afterwards, the data was deleted from the UNIPARK software. Data was stored in an AES encrypted ZIP archive to ensure its confidentiality and following the principles of privacy. The password is only known to CV and CB, the owners of the project file, and is not shared with any third party. If requested, access will be provided by the IP department upon authorization and data will be available for re-analysis during this period, following the Open Science policy for transparency, exchange, reproducibility, and accountability. The ZIP archive will be kept for 10 years in the shared drive and destroyed after this period, following the ethics guidelines of the University of Luxembourg.
The results will allow to phenotype Long-COVID related symptom clusters based on a broad range of self-reported psychological symptoms in a large international sample. These clusters based on psychological symptoms associated with Long-COVID may provide insight into the heterogeneity of psychological presentations among affected individuals. Additionally, the study aims to examine the relationship between psychological syndrome clusters and physical symptoms, shedding light on the interplay between physical and psychological aspects of Long-COVID. Furthermore, the associations between syndrome clusters and pandemic-related variables will provide valuable information regarding the impact of psychosocial and medical factors on Long-COVID outcomes. Finally, the results will help to identify different clusters of Long-COVID patients and support the design of tailored interventions.
Findings will be disseminated at scientific conferences after April 2023, by peer reviewed publications and different social media channels to reach both levels, the public and professionals.
Most of the extant literature only reports results of studies considering psychological symptoms among others, without specifically focusing on them. To date it is unclear whether psychological symptoms in the context of COVID-19 and Long-COVID are directly or indirectly related to the viral infection. Nevertheless, the range of physical symptoms is so broad, that it is unlikely that there is only one indirect negative effect of Long COVID on mental health, but several, potentially amplified by other factors [such as factors pertaining to the pandemic-related experience of social isolation, increased stress etc.; (2, 15, 26, 27)].
We aim to identify clusters of psychological symptoms associated with Long-COVID and determine their prevalence. Moreover, we intend to investigate whether the identified syndrome clusters differ in relation to physical symptoms. Understanding the relationship between physical and psychological symptoms in Long-COVID can shed light on the interplay between these aspects and potentially uncover common underlying mechanisms.
The research includes the retrospective assessment of predictive factors associated with more severe mental health symptoms in Long-COVID, which may include pre-existing mental disorders, social context, other treatments, and blood type. Identifying predictive factors can help in identifying individuals at higher risk for developing severe psychological symptoms and inform targeted interventions. We include the investigation of pandemic-related variables, to examine the question, if syndrome clusters differ in terms of other pandemic-related variables, including psychosocial and medical factors. This broader assessment can provide a comprehensive understanding of the contextual factors that influence the development and manifestation of psychological symptoms in Long-COVID.
The results of the present study will provide important knowledge for public health management. The findings can contribute to better assessment and treatment of psychological symptoms in Long-COVID, inform the development of targeted interventions, enhance our understanding of the complex interactions between physical and psychological aspects of the condition and inform strategies to combat the after-effects of the COVID-19 pandemic.
The main limitations of this study are related to the use of the online questionnaire and online psychological and neuropsychological assessments that can be subject to various biases.
Online assessments are typically completed by individuals who have Internet access and feel comfortable using technology, which may exclude certain populations, such as those with limited Internet access or older individuals who may not have a sufficient level of eHealth literacy. Moreover, participation is voluntary, which introduces the potential for self-selection bias. Individuals who choose to participate may have specific motivations or characteristics that differ from those who opt out. This selection bias can impact the generalizability of the findings. Furthermore, the use of snowball sampling in this study can lead to biased sample selection, limiting the study's generalizability. Nevertheless, due to the pandemic situation, other recruitment methods such as random or convenience sampling were not feasible. Therefore, the study's findings should be interpreted with caution, and further research is needed. The referral process could also introduce biases as participants may refer others who share common characteristics. In addition, online assessments may not fully account for cultural or linguistic differences. Items and response options may not be applicable or adequately translated for diverse populations, leading to biased or inaccurate results across different cultural contexts.
Online questionnaires rely on self-reporting, which is also prone to response bias as participants may provide socially desirable responses, exaggerate, or downplay certain aspects of their behavior or symptoms. This bias can distort the accuracy of the assessment results as well. In addition, slow Internet connections or compatibility problems with specific devices or browsers, can introduce biases in the data and participants experiencing this kind of technical issues may rush through the assessment or abandon it altogether, leading to incomplete or skewed data.
The physical absence of a researcher or clinician who can observe and interpret non-verbal cues and behavior may affect the accuracy and depth of the assessment, as some conditions or symptoms may not be adequately captured through self-reporting alone. The lack of follow up in the online assessments might limit the validity of the results, compared to traditional assessments conducted by clinicians, where follow-up questions can help clarify ambiguous or inconsistent responses.
We acknowledge these drawbacks when interpreting the results of our study and recognize the limitations in capturing the complexity of psychological and neuropsychological phenomena. Nevertheless, the advantages of an online assessment are significant and therefore, important to consider. Online access to a survey increases the accessibility for participants and provides a standardized approach to assessing psychological and neuropsychological factors in long COVID patients, ensuring consistency in the assessment process, making it easier to compare results across patients and track changes over time. Long COVID is a complex condition that can have fluctuating symptoms and online questionnaires and assessments can be used to track their progress and identify changes in symptoms, allowing timely evaluation of these symptoms. This enables healthcare professionals to better understand the impact of long COVID on patients’ mental health and cognitive functioning, and to adjust treatment plans accordingly. Remote support can be provided in the future based on these assessments, through guidance, education, and treatment recommendations, improving access to care for individuals who may have limited access to specialized healthcare facilities. In addition, online assessments give long COVID patients an active role in their healthcare by supporting shared decision-making with their healthcare providers. Patient empowerment can play a crucial role in the management and recovery of long COVID patients.
This study aims to contribute to a better understanding of the psychological symptoms associated with Long-COVID and their related factors. By identifying syndrome clusters and investigating their relationships with physical symptoms and pandemic-related variables, this research can provide valuable insight for improved assessment and treatment approaches for individuals with Long-COVID. Ultimately, these findings may help enhance the overall management and support provided to those affected by this chronic post-viral syndrome.
CB and CV designed the study. CB and RG conducted the literature review, and AI and JB advised on the data analytic strategy. CB, CV, RG, AI, and JB edited the manuscript prior to submission, making substantial intellectual contributions to it, reviewed the different versions and approved the final one, after reading it critically. All authors contributed to the article and approved the submitted version.
Steffen Mortiz: Universitätsklinikum Hamburg-Eppendorf, Germany. Angelika Erhardt: Max-Planck-Institut für Psychiatrie, Munich, Germany. Thérèse Staub: Centre Hospitalier du Luxembourg. Christian Huber and Undine Lang: Universitäre Psychiatrische Kliniken Basel, Switzerland; University of Basel, Switzerland. Steffi Weidt: Psychiatrische Universitätsklinik Zurich, Switzerland; University of Zurich, Switzerland. Kira Wolff and Juliane Müller: Universitätsklinikum Frankfurt am Main, Germany.
The project was supported by the Luxembourg National Research Fund (COVID-19/2021/16874342/Psy-Long-COVID).
We would like to thank the following partners for their contributions and participation in this study: Zentrum fir Psychotherapie, Rehaklinik, Centre Hospitalier Neuro-Psychiatrie (CHNP), Ettelbruck (Luxembourg), University of Luxembourg (Luxembourg), University of Lausanne (UNIL), Centre Hospitalier du Luxembourg (CHL), Max-Planck-Institut, Munich (Germany), Psychiatrische Universitätsklinik, Zurich (Switzerland), Universitäre Psychiatrische Kliniken, Basel (Switzerland), University of Basel, (Switzerland), Universitätsklinikum Frankfurt am Main (Germany), Universitätsklinikum Hamburg-Eppendorf (Germany). We acknowledge the consent to use the scales freely after permission was obtained.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Moldofsky H, Patcai J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. (2011) 11(1):1–7. doi: 10.1186/1471-2377-11-37
2. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. (2023) 21(3):133–46. doi: 10.1038/s41579-022-00846-2
3. Raveendran AV, Jayadevan R, Sashidharan S. Long COVID: an overview. Diabetes Metab Syndr. (2021) 15(3):869–75. doi: 10.1016/j.dsx.2021.04.007
4. Havervall S, Rosell A, Phillipson M, Mangsbo SM, Nilsson P, Hober S, et al. Symptoms and functional impairment assessed 8 months after mild COVID-19 among health care workers. J Am Med Assoc. (2021) 325(19):2015–6. doi: 10.1001/jama.2021.5612
5. Ceban F, Ling S, Lui LMW, Lee Y, Gill H, Teopiz KM, et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain Behav Immun. (2022) 101:93–135. doi: 10.1016/j.bbi.2021.12.020
6. Gold JE, Okyay RA, Licht WE, Hurley DJ. Investigation of long COVID prevalence and its relationship to epstein-barr virus reactivation. Pathogens. (2021) 10(6):763. doi: 10.3390/pathogens10060763
7. Logue JK, Franko NM, McCulloch DJ, McDonald D, Magedson A, Wolf CR, et al. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw Open. (2021) 4(2):e210830. doi: 10.1001/jamanetworkopen.2021.0830
8. Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, et al. Attributes and predictors of long COVID. Nat Med. (2021) 27(4):626–31. doi: 10.1038/s41591-021-01292-y
9. Nguyen NN, Hoang VT, Dao TL, Dudouet P, Eldin C, Gautret P. Clinical patterns of somatic symptoms in patients suffering from post-acute long COVID: a systematic review. Eur J Clin Microbiol Infect Dis. (2022) 41(4):515–45. doi: 10.1007/s10096-022-04417-4
10. Iqbal FM, Lam K, Sounderajah V, Clarke JM, Ashrafian H, Darzi A. Characteristics and predictors of acute and chronic post-COVID syndrome: a systematic review and meta-analysis. EClinicalMedicine. (2021) 36:100899. doi: 10.1016/j.eclinm.2021.100899
11. Salari N, Khodayari Y, Hosseinian-Far A, Zarei H, Rasoulpoor S, Akbari H, et al. Global prevalence of chronic fatigue syndrome among long COVID-19 patients: a systematic review and meta-analysis. BioPsychoSoc Med. (2022) 16(1):21. doi: 10.1186/s13030-022-00250-5
12. Orrù G, Bertelloni D, Diolaiuti F, Mucci F, Di Giuseppe M, Biella M, et al. Long-COVID syndrome? A study on the persistence of neurological, psychological and physiological symptoms. Healthcare. (2021) 9(5):575. doi: 10.3390/healthcare9050575
13. Patel UK, Mehta N, Patel A, Patel N, Ortiz JF, Khurana M, et al. Long-term neurological sequelae among severe COVID-19 patients: a systematic review and meta-analysis. Cureus. (2022) 14(9):e29694. doi: 10.7759/cureus.29694
14. Townsend L, Dyer AH, Jones K, Dunne J, Mooney A, Gaffney F, et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. Plos One. (2020) 15(11):e0240784. doi: 10.1371/journal.pone.0240784
15. Taquet M, Dercon Q, Luciano S, Geddes JR, Husain M, Harrison PJ. Incidence, co-occurrence, and evolution of long-COVID features: a 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. (2021) 18(9):e1003773. doi: 10.1371/journal.pmed.1003773
16. Komaroff AL, Bateman L. Will COVID-19 lead to myalgic encephalomyelitis/chronic fatigue syndrome? Front Med. (2021) 7:1132. doi: 10.3389/fmed.2020.606824
17. Wong TL, Weitzer DJ. Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)—a systemic review and comparison of clinical presentation and symptomatology. Medicina. (2021) 57(5):418. doi: 10.3390/medicina57050418
18. Efstathiou V, Stefanou MI, Demetriou M, Siafakas N, Makris M, Tsivgoulis G, et al. Long COVID and neuropsychiatric manifestations (review). Exp Ther Med. (2022) 23(5):363. doi: 10.3892/etm.2022.11290
19. Gemelli Against COVID-19 Post-Acute Care Study Group. Post-COVID-19 global health strategies: the need for an interdisciplinary approach. Aging Clin Exp Res. (2020) 32:1613–1620. doi: 10.1007/s40520-020-01616-x
20. Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, et al. No health without mental health. Lancet. (2007) 370:859–77. doi: 10.1016/S0140-6736(07)61238-0
21. Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. (2005) 58:175–89. doi: 10.1016/j.biopsych.2005.05.001
22. WHO. Post COVID-19 condition (long COVID) (2022). Available at: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition#:∼:text=It%20is%20defined%20as%20the,months%20with%20no%20other%20explanation.
23. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. A global perspective. 7th ed. Upper Saddle River (N.J.): Pearson education (2010).
24. Charrad M, Ghazzali N, Boiteau V, Niknafs A. Nbclust: an R package for determining the relevant number of clusters in a data set. J Stat Softw. (2014) 61(6):1–36. doi: 10.18637/jss.v061.i06
25. Ebbert D. chisq.posthoc.test: a post hoc analysis for Pearson’s chi-squared test for count data. R package version 0.1.2 (2019). Available at: https://CRAN.R-project.org/package=chisq.posthoc.test.
26. Ballering AV, van Zon SKR, Olde Hartman TC, Rosmalen JGM, Lifelines Corona Research Initiative. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. (2022) 400(10350):452–61. doi: 10.1016/S0140-6736(22)01214-4
Keywords: Long-COVID, COVID-19, persistent COVID-19 symptoms, post-COVID-19 syndrome, mental health
Citation: Gómez Bravo R, Infanti A, Billieux J, Ritzen M, Psy-Long-COVID Consortium, Vögele C and Benoy C (2023) The psychological syndrome associated with Long-COVID: A study protocol. Front. Epidemiol. 3:1193369. doi: 10.3389/fepid.2023.1193369
Received: 17 April 2023; Accepted: 27 June 2023;
Published: 22 August 2023.
Edited by:
Giulia Carla Marchetti, University of Milan, ItalyReviewed by:
Francesca Bai, University of Milan, Italy© 2023 Gómez Bravo, Infanti, Billieux, Ritzen, Psy-Long-COVID Consortium, Vögele and Benoy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Charles Benoy Y2hhcmxlcy5iZW5veUBjaG5wLmx1
†These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.