
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Epidemiol., 14 July 2022
Sec. Cardiovascular Epidemiology
Volume 2 - 2022 | https://doi.org/10.3389/fepid.2022.925464
This article is part of the Research TopicCardiometabolic Diseases in Understudied PopulationsView all 5 articles
 Lily D. Yan1,2*
Lily D. Yan1,2* Vanessa Rouzier2,3Jean Lookens Pierre3
Vanessa Rouzier2,3Jean Lookens Pierre3 Eliezer Dade3Rodney Sufra3Mark D. Huffman4,5Alexandra Apollon3
Eliezer Dade3Rodney Sufra3Mark D. Huffman4,5Alexandra Apollon3 Stephano St Preux3
Stephano St Preux3 Miranda Metz2
Miranda Metz2 Shalom Sabwa2Béatrice Morisset6Marie Deschamps3
Shalom Sabwa2Béatrice Morisset6Marie Deschamps3 Jean W. Pape3Margaret L. McNairy1,2
Jean W. Pape3Margaret L. McNairy1,2Background: Multidrug therapy is a World Health Organization “best buy” for the prevention and control of noncommunicable diseases. CVD polypills, including ≥2 blood pressure medications, and a statin with or without aspirin, are an effective, scalable strategy to close the treatment gap that exists in many low- and middle-income countries, including Haiti. We estimated the number of Haitian adults eligible for an atherosclerotic CVD (ASCVD) polypill, and the number of potentially preventable CVD events if polypills were implemented nationally.
Methods: We used cross-sectional data from the Haiti CVD Cohort, a population-based cohort of 3,005 adults ≥18 years in Port-au-Prince, to compare two polypill implementation strategies: high-risk primary prevention and secondary prevention. High-risk primary prevention included three scenarios: (a) age ≥40 years, (b) hypertension, or (c) predicted 10-year ASCVD risk ≥7.5%. Secondary prevention eligibility included history of stroke or myocardial infarction. We then used the 2019 Global Burden of Disease database and published polypill trials to estimate preventable CVD events, defined as nonfatal MI, nonfatal stroke, and cardiovascular death over a 5-year timeline.
Results: Among 2,880 participants, the proportion of eligible adults for primary prevention were: 51.6% for age, 32.5% for hypertension, 19.3% for high ASCVD risk, and 5.8% for secondary prevention. Based on current trends, an estimated 462,509 CVD events (95% CI: 369,089–578,475) would occur among adults ≥40 years in Haiti from 2019–2024. Compared with no polypill therapy, we found 32% or 148,003 CVD events (95% CI: 70,126–248,744) could be prevented by a combined primary and secondary prevention approach in Haiti if polypills were fully implemented over 5 years.
Conclusion: These modeling estimates underscore the potential magnitude of preventable CVD events in low-income settings like Haiti. Model calibration using observed CVD events, costs, and implementation assumptions are future directions.
Clinical trial registration: clinicaltrials.gov, identifier: NCT03892265.
Cardiovascular diseases (CVD) are the leading cause of morbidity and mortality in low- and middle-income countries (LMICs), with 4.6 million deaths in 2019, yet large gaps in modifiable risk factor control for hypertension and hyperlipidemia persist (1–3). Atherosclerotic CVD polypills, which are fixed-dose combinations of low doses of two or more blood pressure (BP) medications and a statin with or without aspirin, have been shown to be effective at reducing CVD risk (4). In randomized trials across high and low-income settings and populations, ASCVD polypills lower BP, low density lipoprotein cholesterol (LDLc), and CVD events (5–9).
Patients who may benefit from ASCVD polypills are typically categorized into high-risk primary or secondary CVD prevention (10). Primary prevention strategies identify individuals more likely to benefit based on a single risk factor (e.g., age, raised BP) or based on predicted, multivariable CVD risk scores (10). Secondary prevention targets a narrower population among individuals with history of ASCVD events, like stroke or myocardial infarction (MI).
We estimated the potential impact of ASCVD polypills in Haiti, a low-income country where CVD is the leading cause of adult mortality (11) and hypertension prevalence is 29%, but only 13% have controlled BP (12). We explored the number of adults who would be eligible for polypills based on high-risk primary prevention and secondary prevention. We then estimated the potential number of preventable CVD events nationally with each strategy.
Our study design combines a cross-sectional analysis with a modeling estimation. We compared two ASCVD polypill implementation strategies: high-risk primary and secondary prevention (10). Primary prevention included three eligibility scenarios: (a) age ≥40 years, (b) essential hypertension defined as BP ≥140/90 mm Hg per World Health Organization (WHO) guidelines, and (c) predicted 10-year CVD high risk ≥7.5% calculated by the Pooled Cohort Equations (13). Although other polypill trials used older age thresholds for primary prevention (7), we chose age ≥40 given the Haitian population is very young [48% is <40 years, life expectancy = 64 years (14)], and ASCVD risk prediction begins at age 40. Secondary prevention included eligibility based on history of prior stroke or MI. Polypill trial data are listed in Supplementary Table S1.
The primary outcome of this analysis was the proportion of Haitian adults eligible for a ASCVD polypill under various scenarios. The secondary outcome was the number of potentially preventable CVD events under national implementation of various prevention strategies over a 5-year timeline in Haiti assuming static population size, population structure, risk factor levels, and background event rate.
For the primary outcome, we used cross-sectional enrollment data within the Haiti CVD Cohort Study, a longitudinal population-based cohort of 3,005 adults living in Port-au-Prince that aims to measure prevalence and incidence of CVD and risk factors (15). This cohort is one of the first population-based studies in Haiti that systematically measured laboratory values including serum lipids. We included all participants ≥18 years, with enrollment from March 2019 to August 2021. Participants missing required data for ASCVD risk estimation were excluded (n = 125, 4.2%).
For the secondary outcome, we used the 2019 Global Burden of Disease (GBD) estimates of incident CVD events in Haiti. CVD events included nonfatal MI, nonfatal stroke, and CVD death (16). We then used results from published randomized controlled trials of ASCVD polypills to determine the hazard ratio for CVD events in adults receiving the polypill vs. placebo. Given lack of dedicated trial data for secondary prevention, we used the same hazard ratio for a combined primary and secondary prevention approach from an individual participant meta-analysis on polypill use for CVD prevention (polypill without aspirin, HR 0.68, 95% CI 0.57–0.81), including one study using treatment based on age with additional clinical criteria regardless of prior CVD events, and two using treatment based on high predicted 10-year ASCVD risk (9).
We collected sociodemographic data, medical history, health behaviors, and a clinical exam during an enrollment survey using standardized World Health Organization (WHO) STEPs instruments (17). Three unobserved BP measurements were taken according to WHO guidelines with an Omron HEM-905, with the second and third BP measurements averaged for all analyses (17).
Hypertension was defined as any of the following: systolic BP (SBP) ≥140 mmHg, diastolic BP (DBP) ≥90 mmHg, on hypertension medications, or clinician diagnosis of hypertension based on WHO thresholds (17). Hypercholesterolemia was defined as any of the following: low density lipoprotein cholesterol ≥160 mg/dl, on a statin, or clinician diagnosis of hypercholesterolemia (18). Diabetes mellitus was defined as any of the following: random glucose ≥200 mg/dl, fasting glucose ≥126 mg/dl, on diabetes medications, or clinician diagnosis (19). CVD history was measured as self-reported history of stroke or MI.
We summarized the proportion of the Haiti CVD Cohort that was polypill eligible under primary prevention and secondary prevention scenarios with descriptive statistics. We followed four steps to estimate potentially preventable ASCVD events. First, we assumed a timeline of 5 years given polypill trial data have a median follow up period of 5 years (9). Second, we used 2019 GBD estimates of incident CVD events for adults ≥40 years to calculate the number of incident CVD events over 5 years, assuming static population size and structure and without any changes in risk factor levels or annual rates of incident events. Third, we calculated incident and recurrent CVD events under nationwide polypill implementation under a combined primary and secondary prevention approach by applying clinical trial hazard ratios and corresponding 95% confidence intervals to GBD estimates of 5-year incident CVD events. Lastly, we calculated preventable CVD events by subtracting the number of incident and recurrent CVD events under a national polypill strategy from the estimated number of CVD events without polypill implementation.
This study was approved by institutional review boards at Weill Cornell Medicine and Groupe Haitien d'Etude du Sarcome de Kaposi et des Infections Opportunistes (GHESKIO) (1803019037), with written participant consent.
Out of 3,005 participants, 2,880 (95.8%) had complete data and were included (Supplementary Figure S1). Table 1 describes the participants' demographics and proportion of the cohort who would be polypill eligible under various primary or secondary prevention strategies. Sex-stratified demographics are reported in Supplementary Table S2.
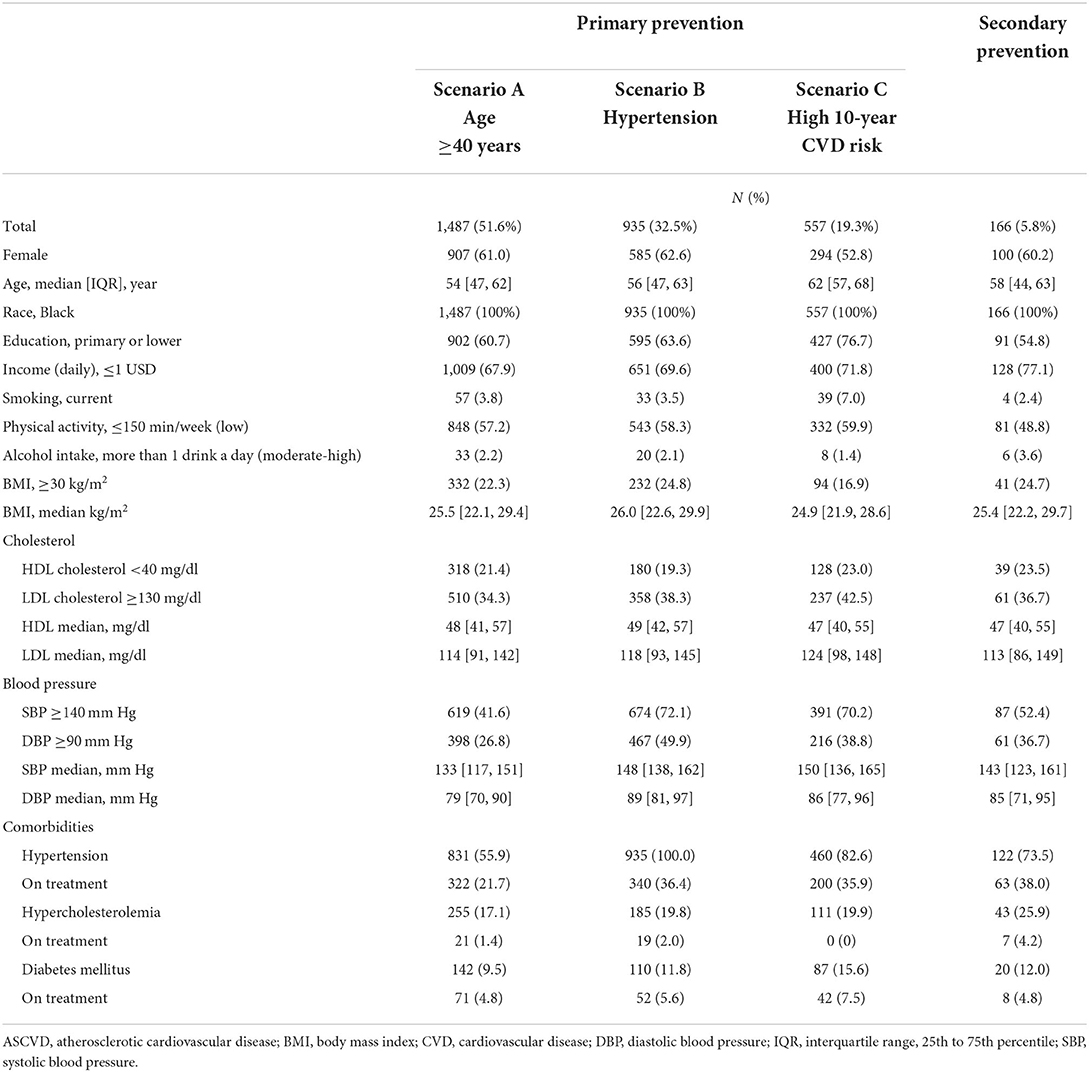
Table 1. Characteristics of adults eligible for ASCVD polypill in the Haiti CVD cohort.
The highest proportion (51.6%, 1,487/2,880) of adults in the Haiti CVD Cohort were eligible for an ASCVD polypill under a primary prevention strategy using eligibility scenario of age ≥40 years (Figure 1). Under primary prevention based on hypertension, 32.5% were eligible, while primary prevention based on high 10-year predicted ASCVD risk resulted in 19.3% being eligible. Using a secondary prevention strategy, 5.8% of adults within the Haiti CVD Cohort had a polypill indication, including 3.4% based on past MI and 2.6% on past stroke.
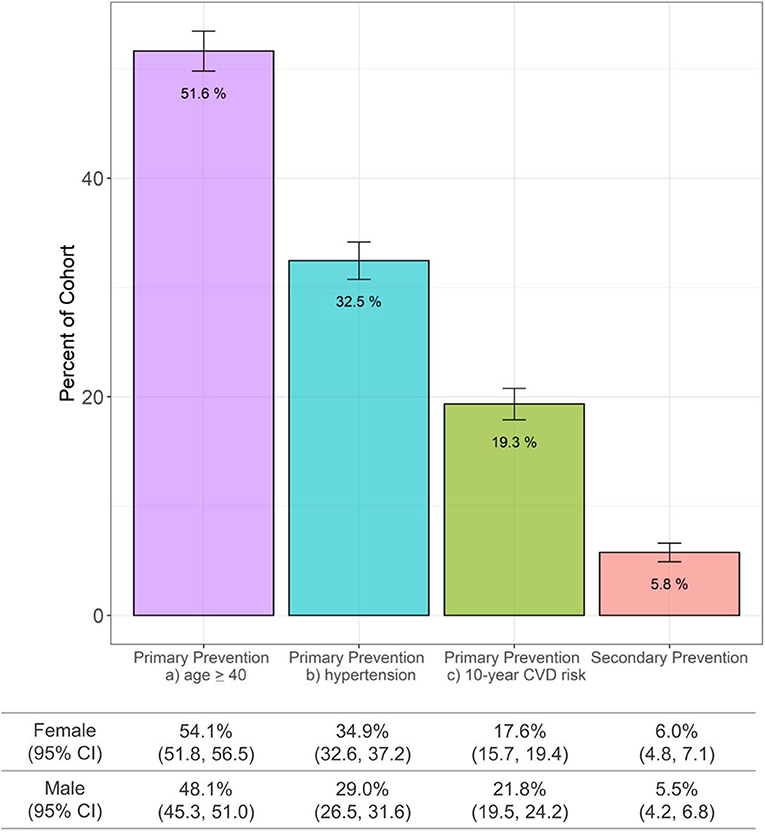
Figure 1. ASCVD polypill eligibility in Haiti using the Haiti CVD Cohort (N = 2,880 participants age ≥ 18 years). ASCVD, atherosclerotic cardiovascular disease; CI, confidence intervals; CVD, cardiovascular disease.
Based on GBD estimates, over a 5-year period, 462,509 incident and recurrent CVD events (95% CI: 369,089–578,475) among people aged ≥40 years are predicted to occur assuming no changes in population size, structure, disease incidence, or risk factor levels (Table 2). Using the hazard ratio from published ASCVD polypill trials, 148,003 CVD events (95% CI: 70,126–248,744) or 32% could be potentially preventable with a nation-wide polypill strategy based on a combined primary and secondary prevention strategy.
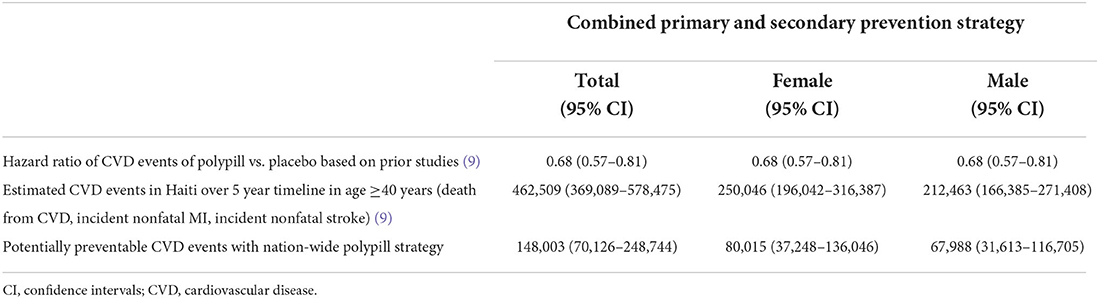
Table 2. Potentially preventable CVD events over 5-year timeline under nation-wide polypill strategy in Haiti.
We estimate the potential impact of polypills for ASCVD prevention in Haiti, finding it could result in a 32% (95% CI: 15%−54%) reduction in CVD-related events that would have a substantial effect on the CVD epidemic in Haiti.
Premature CVD deaths continue to grow in LMIC, and epidemiological studies have found that modifiable risk factors such as hypertension, dyslipidemia, tobacco use, diet, physical inactivity, obesity, diabetes, psychological stress, and unhealthy alcohol use account for as much as 90% of CVD events (20, 21). ASCVD polypills are recommended by the WHO as a “best buy” for noncommunicable disease prevention and control (22). Polypills represent a pragmatic intervention and may be particularly relevant for fragile health systems where high costs of accessing repeated clinic-based care make medication titration challenging. Haiti is the poorest country in the Western Hemisphere, and CVD risk in Haiti is driven primarily by hypertension (23). In middle and high-income countries, polypills reduced systolic BP by 7–19 mm Hg, and LDLc by 11–14 mg/dl (5, 24, 25). These gains in CVD risk factor control have translated into longer-term reductions, including reduced CVD mortality, in varied settings from Canada to Tanzania (7, 9, 26).
This study uses some of the first available population-based CVD epidemiological data on prevalence of CVD risk factors in a low-income country to estimate the potential impact of ASCVD polypill implementation. Limitations include potentially over-optimistic hazard ratios based on randomized trials compared with general populations due to limited access to medical care, limited medication supplies or diagnostic capacity, and suboptimal adherence, and potential over-estimation of eligibility with age ≥40 years. Additional calibrations are needed to fine tune these estimates using adjudicated CVD events in Haiti and accounting for longitudinal changes in population size, structure, risk factors, and event rates. Implementation studies are needed to evaluate acceptability and feasibility of implementation and cost in Haiti, among other settings.
In summary, practical and effective interventions to reduce CVD risk are urgently needed in LMICs, which disproportionately bear the burden of CVD mortality. In this case study of a LMIC with high CVD mortality, a significant proportion of adults would be eligible for primary and secondary prevention with potentially large reductions in CVD events over time if implemented on a national level.
Deidentified data used for this analysis are available upon request after signing a data access and use agreement, provision of approval by the GHESKIO ethics board, and demonstration that the external investigative team is qualified and has documented evidence of human research protection training. Requests to access the datasets should be directed at: LY, bGl5OTAzMkBtZWQuY29ybmVsbC5lZHU=.
The studies involving human participants were reviewed and approved by Weill Cornell Medicine and Groupe Haitien d'Etude du Sarcome de Kaposi et des Infections Opportunistes (GHESKIO) (1803019037). The patients/participants provided their written informed consent to participate in this study.
This study was conceived and the initial draft was written by LY and MMc. Project administration, and data curation were completed by LY, VR, JPi, ED, RS, AA, SSt, MMe, SSa, MD, JPa, and MMc. Formal analysis was completed by LY. Investigation, methodology, and interpretation were completed by LY, VR, JPi, ED, RS, MH, MMc, SSa, BM, MD, JPi, and MMc. All authors have read and approved the manuscript, and confirm that they meet ICMJE criteria for authorship.
Funding for this study comes from the National Heart, Lung, and Blood Institute, Grant Number R01HL143788 and Fogarty International Center, Grant Number D43TW011972.
We acknowledge the valuable input from the Haitian College of Cardiology, the community health workers, and the study participants for entrusting us with their care.
VR, JPi, JPa, and MMc report a grant from NHLBI R01HL143788. VR reports a grant from NHLBI R01HL143788-S01. MMc reports a grant from the NIH D43TW011972. MH has pending patents for heart failure polypills. The George Institute for Global Health's wholly owned enterprise, George Health Enterprises, has received investment funds to develop fixed-dose combination products containing aspirin, statin and blood pressure lowering drugs.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fepid.2022.925464/full#supplementary-material
1. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Geldsetzer P, Manne-Goehler J, Marcus ME, Ebert C, Zhumadilov Z, Wesseh CS, et al. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. Lancet. (2019) 394:652–62. doi: 10.1016/S0140-6736(19)30955-9
3. Marcus ME, Ebert C, Geldsetzer P, Theilmann M, Bicaba BW, Andall-Brereton G, et al. Unmet need for hypercholesterolemia care in 35 low- and middle-income countries: a cross-sectional study of nationally representative surveys. PLoS Med. (2021) 18:e1003841. doi: 10.1371/journal.pmed.1003841
4. Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. BMJ. (2003) 326:1419. doi: 10.1136/bmj.326.7404.1419
5. Muñoz D, Uzoije P, Reynolds C, Miller R, Walkley D, Pappalardo S, et al. Polypill for cardiovascular disease prevention in an underserved population. N Engl J Med. (2019) 381:1114–23. doi: 10.1056/NEJMoa1815359
6. Chow CK, Thakkar J, Bennett A, Hillis G, Burke M, Usherwood T, et al. Quarter-dose quadruple combination therapy for initial treatment of hypertension: placebo-controlled, crossover, randomised trial and systematic review. Lancet. (2017) 389:1035–42. doi: 10.1016/S0140-6736(17)30260-X
7. Roshandel G, Khoshnia M, Poustchi H, Hemming K, Kamangar F, Gharavi A, et al. Effectiveness of polypill for primary and secondary prevention of cardiovascular diseases (PolyIran): a pragmatic, cluster-randomised trial. Lancet. (2019) 394:672–83. doi: 10.1016/S0140-6736(19)31791-X
8. Yusuf S, Joseph P, Dans A, Gao P, Teo K, Xavier D, et al. Polypill with or without aspirin in persons without cardiovascular disease. N Engl J Med. (2020) 398:1133–46. doi: 10.1056/NEJMoa2028220
9. Joseph P, Roshandel G, Gao P, Pais P, Lonn E, Xavier D, et al. Fixed-dose combination therapies with and without aspirin for primary prevention of cardiovascular disease: an individual participant data meta-analysis. Lancet. (2021) 398:1133–46. doi: 10.1016/S0140-6736(21)01827-4
10. Huffman MD, Xavier D, Perel P. Uses of polypills for cardiovascular disease and evidence to date. Lancet. (2017) 389:1055–65. doi: 10.1016/S0140-6736(17)30553-6
11. GBD. GBD Compare | IHME Viz Hub. Available online at: http://vizhub.healthdata.org/gbd-compare (accessed January 22, 2021)
12. Metz M, Pierre JL, Yan LD, Rouzier V, St-Preux S, Exantus S, et al. Hypertension continuum of care: Blood pressure screening, diagnosis, treatment, and control in a population-based cohort in Haiti. J Clin Hypertens. (2022) 24:246–54. doi: 10.1111/jch.14399
13. Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. (2014) 129(25 Suppl 2):S49–73. doi: 10.1161/01.cir.0000437741.48606.98
14. World Bank. Life expectancy at birth, total (years) - Haiti | Data. Available online at: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=HT (accessed February 17, 2022).
15. Lookens J, Tymejczyk O, Rouzier V, Smith C, Preval F, Joseph I, et al. The Haiti cardiovascular disease cohort: study protocol for a population-based longitudinal cohort. BMC Public Health. (2020) 20:1633. doi: 10.1186/s12889-020-09734-x
16. GBD Results Tool | GHDx. Available online at: http://ghdx.healthdata.org/gbd-results-tool (accessed September 1, 2021).
17. WHO. WHO STEPS. Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. Geneva: WHO (2017).
18. Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. (2019) 139:e1082–143. doi: 10.1161/CIR.0000000000000624
19. World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of a WHO/IDF Consultation. Geneva: WHO (2006).
20. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. (2004) 364:937–52. doi: 10.1016/S0140-6736(04)17018-9
21. O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. (2010) 376:112–23. doi: 10.1016/S0140-6736(10)60834-3
22. WHO-Wellcome Trust Meeting on Secondary Prevention, Organization WH, Trust (London) W. Secondary prevention of noncommunicable diseases in low- and middle-income countries through community-based and health service interventions : World Health Organization-Wellcome Trust meeting report, 1-3 August 2001. Geneva: World Health Organization (2002). Report No.: WHO/MPN/CVD/2002.01. Available online at: https://apps.who.int/iris/handle/10665/42567 (accessed May 5, 2022).
23. Tymejczyk O, McNairy ML, Petion JS, Rivera VR, Dorélien A, Peck M, et al. Hypertension prevalence and risk factors among residents of four slum communities: population-representative findings from Port-au-Prince, Haiti. J Hypertens. (2019) 37:685–95. doi: 10.1097/HJH.0000000000001966
24. PILL Collaborative Group. An international randomised placebo-controlled trial of a four-component combination pill (“Polypill”) in people with raised cardiovascular risk. PLoS ONE. (2011) 6:e19857. doi: 10.1371/journal.pone.0019857
25. The Indian Plycap Study (TIPS). Effects of a polypill (Polycap) on risk factors in middle-aged individuals without cardiovascular disease (TIPS): a phase II, double-blind, randomised trial. Lancet. (2009) 373:1341–51. doi: 10.1016/S0140-6736(09)60611-5
Keywords: Haiti, low-middle income country, global health, preventive cardiology, epidemiology
Citation: Yan LD, Rouzier V, Pierre JL, Dade E, Sufra R, Huffman MD, Apollon A, St Preux S, Metz M, Sabwa S, Morisset B, Deschamps M, Pape JW and McNairy ML (2022) Polypill for atherosclerotic cardiovascular disease prevention in Haiti: Eligibility estimates in a low-income country. Front. Epidemiol. 2:925464. doi: 10.3389/fepid.2022.925464
Received: 21 April 2022; Accepted: 27 June 2022;
Published: 14 July 2022.
Edited by:
Victor Zhong, Shanghai Jiao Tong University, ChinaReviewed by:
Pei Xue, Uppsala University, SwedenCopyright © 2022 Yan, Rouzier, Pierre, Dade, Sufra, Huffman, Apollon, St Preux, Metz, Sabwa, Morisset, Deschamps, Pape and McNairy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lily D. Yan, bGl5OTAzMkBtZWQuY29ybmVsbC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.