 Addis Eyeberu1
Addis Eyeberu1 Adera Debella1*
Adera Debella1* Dechasa Adare Mengistu2
Dechasa Adare Mengistu2 Mesay Arkew3
Mesay Arkew3 Saba Hailu4Amanuel Oljira1
Saba Hailu4Amanuel Oljira1 Jemal Yusuf Kebira4
Jemal Yusuf Kebira4 Tamirat Getachew1Shamble Nigussie5
Tamirat Getachew1Shamble Nigussie5 Deribe Bekele1
Deribe Bekele1 Rebuma Belete3Degu Abate3Habtamu Bekele2
Rebuma Belete3Degu Abate3Habtamu Bekele2 Tigist Tefera6Addisu Alemu4
Tigist Tefera6Addisu Alemu4 Yadeta Dessie4
Yadeta Dessie4- 1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 2Department of Environmental Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
- 3Department of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 4School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 5School of Pharmacy, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 6Biochemistry Department, School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Background: The COVID-19 outbreak has now become a major international public health concern and a major challenge for the entire world. Poor adherence to COVID-19 prevention measures continues to be a challenge in managing COVID-19 pandemics, including in Ethiopia. As a result, the current study sought to identify the determinants of community adherence to COVID-19 preventive measures among the adult population of Harari Regional State in Eastern Ethiopia.
Methods: A community-based cross-sectional study was conducted in Harari Regional State, Eastern Ethiopia from January 5 to 30, 2021. All adults above the age of 18 who lived in Harari Regional State's selected kebeles were eligible to participate in the study. A systematic random sampling method was used to select the study participants. The study included a total of 1,320 participants. Pre-tested, structured, and self-administered questionnaires were used to collect data, which was then analyzed using STATA version 16 software. The consent was obtained from each individual and concerned body. Binary logistic regression was used to find the correlation between community adherence to COVID-19 preventive measures and sociodemographic, knowledge, self-efficacy, and risk perception. A P-value of 0.05 was used as the statistical significance cut-off point.
Results: One thousand two hundred fifty-five (1,255) people took the survey, yielding a 95.1 % response rate. Adherence to COVID-19 preventive measures resulted in a mean cumulative score of 29.8. Six hundred eight (48.5%) of the participants had good adherence to COVID-19 preventive measures, whereas 647 (51.5%) did not. The researchers also discovered a statistically significant link between participants' residence, educational status, risk perception, income, and adherence to COVID-19 preventive measures.
Conclusion: Appropriate implementation of COVID-19 preventive measures among community members is required to manage or control pandemics and reduce health-related consequences associated with COVID-19 pandemics. The current study, on the other hand, discovered that nearly half of the study participants had poor adherence. As a result, in order to manage this pandemic, the relevant organizations, including the government and non-governmental organizations, must take appropriate and timely measures.
Introduction
The novel-coronavirus disease is currently a global health threat and an international public health emergency. In 2012, another coronavirus-caused outbreak known as Middle Eastern Respiratory Syndrome (MERS) resulted in over 1,000 infections and 400 deaths through 2015, and now the new Coronavirus disease 2019 (COVID-19) has plagued the world (1, 2). COVID-19 is a newly emerging disease caused by a highly infectious novel coronavirus that primarily affects the respiratory system (3). COVID-19 was first detected and isolated from a pneumonia patient in late December 2019 from Wuhan, China. Then WHO declared COVID-19 as a pandemic on 11 March 2020 (4). The most common symptoms include fever (78%), cough (57%), and fatigue (31%), as well as severe viral pneumonia, which can lead to acute respiratory distress syndrome, which can be fatal. COVID-19 can be transmitted to humans by touching an infected object or surface and then touching their mouth, nose, or possibly their eyes (4, 5). Both the CDC and WHO recommend that coronavirus prevention measures be known and implemented. These urge countries around the world to prioritize strict non-pharmaceutical interventions to combat the pandemic, such as the (mandatory) use of face masks, physical separation, regular hand washing and use of sanitizers, and regularly disinfecting surfaces (6).
Ethiopia is the second most populous nation in Africa, with a 9% of the African population (7). Since COVID-19 was declared a global and national public health threat, the Ethiopian government has implemented additional preventive measures such as mandatory quarantine periods for all travelers, restrictions on public gatherings, school closures, and mandatory facemasks in public places, as well as fewer passengers using public transportation. Risk communication on measures such as physical separation, wearing face masks, and hygiene, including through the media and cell-phone ring tone reminders, are critical interventions, but the infection rate continues to rise (8).
Despite government-imposed restrictions, there are inconsistencies in the implementation of COVID-19 preventive measures. Low educational status, female gender, age, urban residence, and knowledge of COVID 19 were discovered to have a significant effect on adherence to COVID preventive measures (6, 9, 10).
Poor adherence to COVID-19 mitigation measures remains a problem (11). Understanding the level of adherence to non-pharmaceutical interventions is essential to control COVID-19 disease (6). However, there is no adequate and current evidence regarding community adherence to COVID-19 preventive measures. Thus, the current study aimed to determine and provide current evidence on the community's adherence toward COVID-19 preventive measures and root causes of poor adherence among residents of Harari Region, Eastern Ethiopia.
Materials and Methods
Study Period, Design, and Setting
A community-based cross-sectional study was conducted in Harari regional state, Eastern Ethiopia, from January 5 to 30, 2021. The region is located 510 kilometers east of Addis Ababa, Ethiopia's capital city. The region is divided into nine districts, three of which are rural and the other six are urban. According to the 2021 projection based on the 2007 Census, CSA, the region's total population is 270,000, with 136,000 males and 134,000 females (1). The Harari regional state had a total of 59,487 households. During the survey period, the information regarding COVID-19 has been disseminated by the concerned organizations, including the regional health bureau. However, there was a gap in the implementation of COVID-19 prevention measures with an unknown magnitude or level.
Study Population
All adult residents of Harari Regional State who are above the age of 18 and live in selected kebeles (Smallest administrative unit in Ethiopia). The study included residents living in selected households as heads or any other household members over the age of 18 who were available during data collection. People who left the house for any reason and became seriously ill during data collection were barred from participating in the study.
Sample Size Determination and Sampling Procedures
The sample size was determined using the single population proportion formula by considering the expected margin of error (d) of 0.04, with a confidence interval level of 95% and a design effect of 2. The acceptance rate of preventive measures taken from a similar study was 48.96% (11). The number of households to be included in this study was calculated based on the following formula.
= 1200. Then, the final sample size required for the current study was 1,320, including 10% non-response rate.
The study participants were sampled using a multi-stage sampling technique. The simple random sampling (lottery) method was used to select 13 kebeles from 9 districts. One thousand and three hundred and twenty households were allocated proportionally from the selected kebeles. A systematic random sampling method was used to select each study participant (HH). Then, a total of 1,320 eligible individuals were chosen from the included households, with 1,255 completing the survey.
Data Collection Methods and Techniques
A face-to-face interview was used to collect data using a pre-tested, semi-structured questionnaire (with three sections that include socio-demographic characteristics, preventive behaviors, and self-efficacy to practice COVID-19). Investigators used an online survey portal to create the questionnaires, and Google form was used to collect the data.
Thirty data collectors (BSc holders) and 8 supervisors (MSc. holders) were trained on the ways of data collection, principles, and ethics before data collection. The questionnaire was adapted from the WHO and UNICEF documents of COVID-19 preparedness and response (12), and similar literature (3, 11, 13).
Measurement
Adherence to COVID-19 prevention methods was measured using 10 questions. The respondents rated how often they were following the preventive methods recommended by WHO on five scales: none (1), rarely (2), sometimes (3), frequently (4), and always (5). Finally, the cumulative practice score was computed (range 10–50). Finally, a higher score presents good adherence to preventive against COVID-19 (above mean score), whereas the inverse represents poor adherence (14).
Perceived self-efficacy to practice prevention measures was measured using four items which responded on five scales: certainly not (1), probably not (2), not perhaps yes (3), probably yes (4), and most certainly (5). The items were stated in a way that the higher value indicates more perceived self-efficacy to practice the measures. The sum and mean scores were computed. Finally, those who had a higher score presented high self-efficacy to practice COVID-19 prevention measures based on the mean score (above mean score), whereas the inverse represent low self-efficacy (3).
Data Quality Control
Prior to data collection, the questionnaire was pretested in Haramaya Town, Eastern Ethiopia, outside the study area, to ensure the clarity, sequence, and applicability of questions, as well as to estimate the time required to collect data. For three days, all data collectors and supervisors were thoroughly trained on the principles, ethics, procedures, and questionnaire. All completed questionnaires were reviewed for consistency and completeness.
Statistical Processing and Analysis
The data were checked for consistency and completeness. The data were analyzed using STATA version 16 software. Descriptive statistical tests were used to provide a clear distribution of the data. Numerical variables were measured as mean and standard deviations, while categorical variables were expressed as frequencies and percentages. Finally, binary logistic regression was applied to examine the effects of independent variables on adherence toward COVID-19 preventive measures and it was expressed as an odds ratio (OR) and 95% confidence interval (CI). A P-value of 0.05 was considered as a cut-off point for statistical significance.
Results
Socio-Demographic Characteristics
The survey was completed by 1,255 people out of a total of 1,320 sample sizes, yielding a 95.1% response rate. The average age of respondents was 34.4 (SD 10.9) years old, with nearly one-fourth being between the ages of 18 and 25.0 (Table 1).
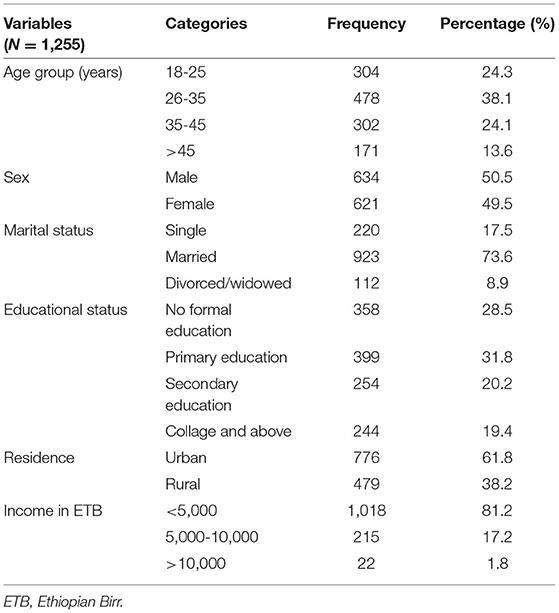
Table 1. Socio-demographic characteristics of study participants in Harari Regional State, Eastern Ethiopia 2021 (N = 1,255).
Adherence to COVID-19 Preventive Measures
About one-fourth (24.4%) of the study participants were never maintaining physical distance, whereas only 3.9% keep their distance always. About one-fourth (24.4%) of study participants were never maintained physical distance, whereas only 3.9% always maintained physical distance.
Eleven percent (11%) of the respondents never wear face masks outside the home and around 12% of participants always wash their hands with water and soap. The study found the mean cumulative score of adherences to COVID-19 preventative measure that was 29.8 (SD ± 7.8. Six hundred eight, 608 (48.5%) had good adherence to COVID 19 preventive measures while 647 (51.5%) had a poor adherence (Table 2).
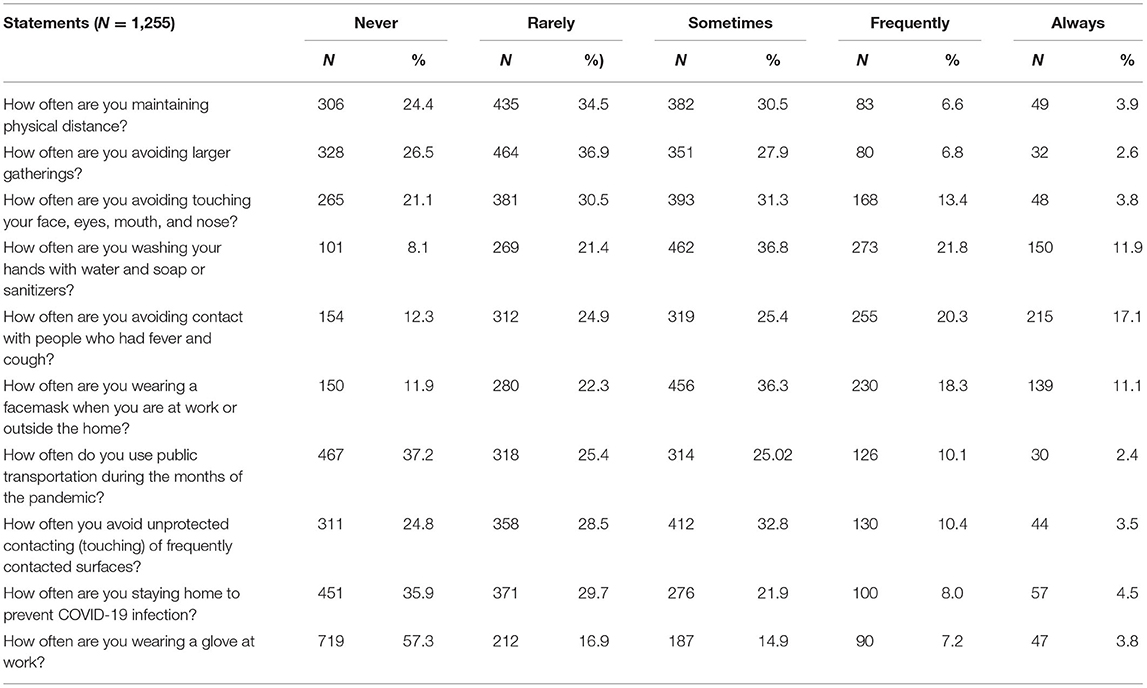
Table 2. Adherence to COVID 19 preventive measures among adult population in Harari Regional State, Eastern Ethiopia, 2021.
Risk Perception Regarding COVID-19
One-third (33.6%) of the study participants agreed that getting sick with the coronavirus can be dangerous. Regarding preventive measures, about 81.0% of respondents believe that they will contract coronavirus if they do not take any preventive measures. The mean cumulative score of risk perception was 29.8 (SD 6.9). Five hundred eighty-eight, 588(46.9%) of the participants had a high-risk perception toward COVID-19, whereas 667(53.2%) had a low-risk perception (Table 3).

Table 3. Risk perception toward COVID-19 pandemic among adult population in Harari Regional State, Eastern Ethiopia, 2021 (N = 1,255).
Perceived Self-Efficacy to Implement COVID-19 Prevention Measures
Among 1,255 respondents, only 15.6% were certain that they could wash their hands with water and soap or with sanitizers frequently. Furthermore, about 17.2% of the study participants reported that they certainly did not manage to use facemasks outside the home. According to the current study, the average cumulative score of adherences to COVID-19 preventative measures was 29.8 (SD = 7.8).
The mean cumulative score of self-efficacy items was 11.9 (SD ± 3.9). Five hundred eighty (46.2%) of the participants had high self-efficacy to practice COVID-19 preventive methods, while the remaining 675 (53.78%) had a low self-efficacy to practice COVID-19 preventive methods (Table 4).
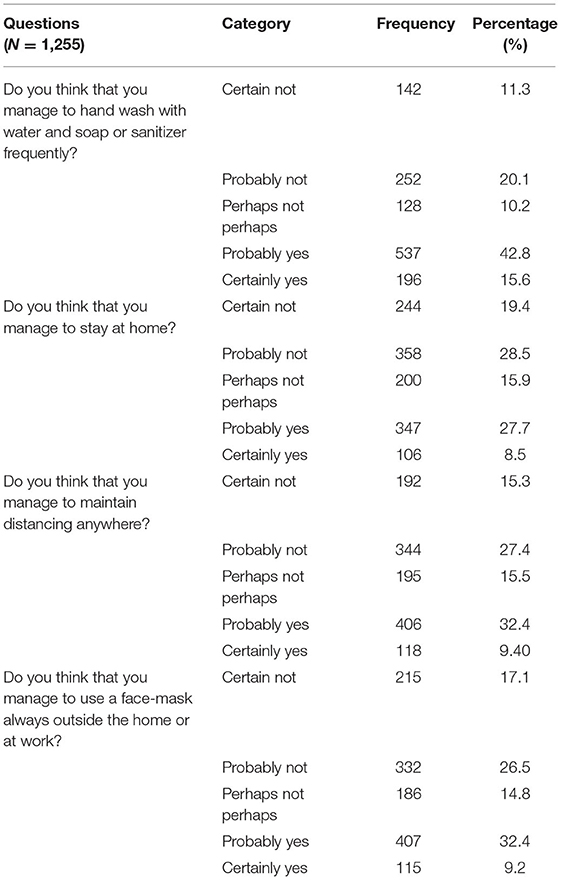
Table 4. Self-efficacy to practice COVID-19 prevention methods among adults in Harari region, East Ethiopia, 2021, (N = 1,255).
Factors Associated With the Adherence of Adults Toward COVID-19 Safety Measures
The multivariate analysis shows that participants residing in rural areas were 0.71 times less likely to have poor adherence to COVID-19 preventive measures than their counterparts (AOR: 0.71, 95%CI: 0.52-0.98). The odds of poor adherence to safety measures of COVID-19 were 0.39 times less likely among adults who had primary education than respondents who did not attend formal education (AOR: 0.61, 95%CI: 0.43-0.87). Similarly, participants with a monthly income of 5,000-10,000 ETB were 0.59 times less likely to adhere poorly to the preventive measures (AOR: 0.41, 95%CI: 0.28-0.59) compared with those who had an income of <5,000 ETB. The odds of poor COVID-19 preventive behavior among respondents who had low perceived self-efficacy was almost four times higher than those who had high self-efficacy to practice COVID-19 prevention methods (AOR: 3.8, 95%CI: 3.01-4.97) (Table 5).
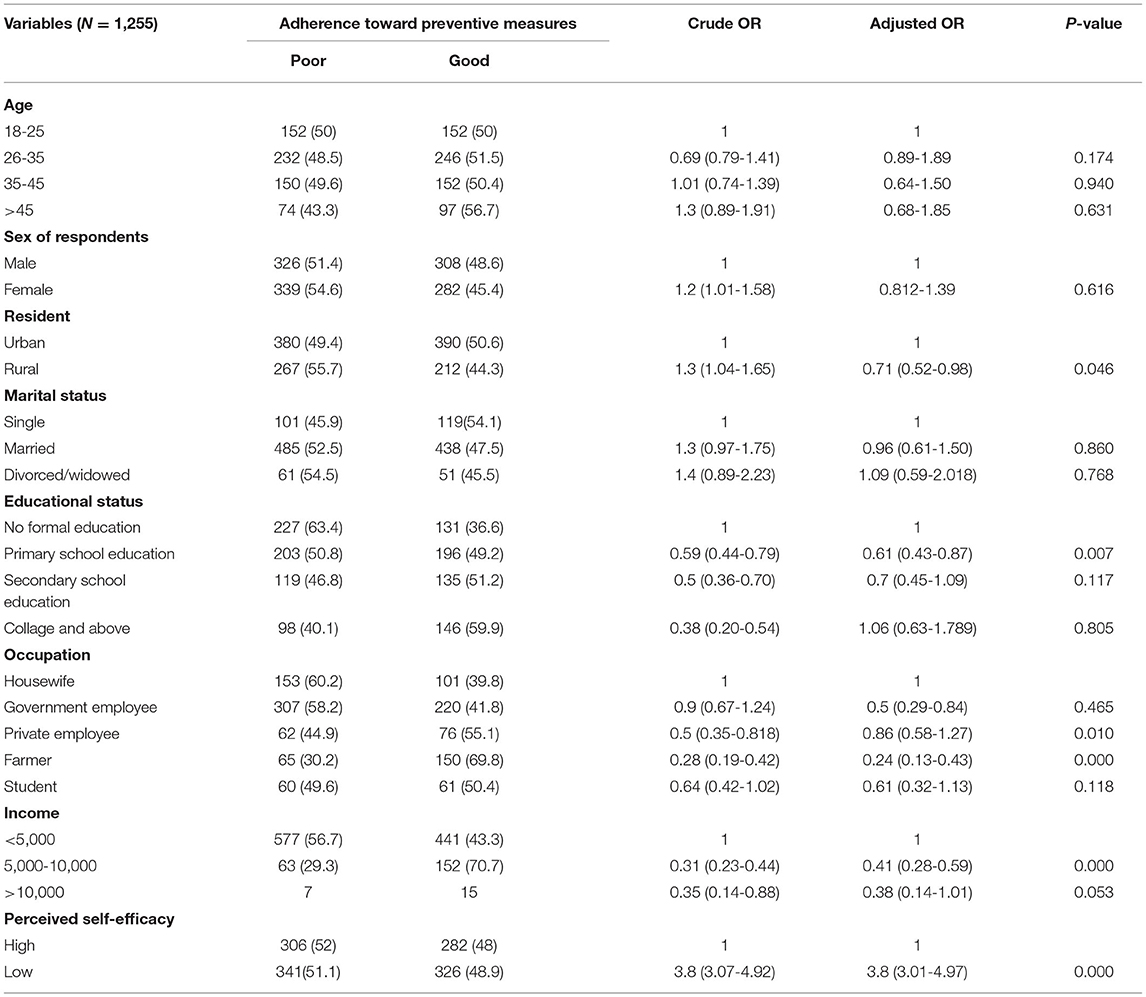
Table 5. Factors associated with poor adherence to COVID-19 preventive measures among adults in Harari Region, East Ethiopia, 2021 (N = 1,255).
Discussion
Preventive measures play an essential role in reducing infection rates and controlling the spread of various diseases. There has been no definitive treatment found since the emergence of the COVID-19 pandemic. As a result, adhering to the recommended preventive measures is the best option for limiting the spread of the COVID-19 pandemic (11). The current study sought to investigate the community's adherence to COVID-19 prevention measures in Harari Regional State, Ethiopia. In the current study, 1,255 adults provided complete responses. According to the current study, overall poor adherence to COVID-19 preventive measures accounted for 51.5%, which was higher than the finding of another study conducted in Ethiopia, which reported a community adherence level of 44.1% to the recommended COVID-19 safety measures (15). But higher than the finding of another study conducted in Ethiopia, which found only 12.3% of the study participants adhered to the recommended COVID-19 preventive measures (16).
The current study identified various factors related to COVID-19 adherence among the study participants. For example, an educational status: primary school [AOR = 0.61 (0.43-0.87)] was associated with poor adherence to COVID-19 preventive measures that were in line with the findings reported by another study conducted in Ethiopia (15). Other factors associated with poor adherence to COVID-19 preventive measures were occupational status, monthly income, and perceived self-efficacy. The current study found that being a governmental employee [AOR = 0.5 (0.29-0.84] and formal occupations [AOR = 0.24 (0.13-0.43)] were significantly associated with poor adherence to the COVID-19 preventive measures. Another study conducted in Congo also reported that being both a private and public employee was associated with poor adherence to COVID-19 preventive measures (6). Even though the two studies' findings sound discrepant, they are almost identical in their findings except their interpretations.
The current study has also found that a monthly income of more than 5,000 ETB [AOR = 0.41 (0.28-0.59)] was significantly associated with poor adherence to the COVID-19 preventive measures. This finding was in line with the finding of another study conducted in Saudi Arabia and Mexico (16, 17).
Furthermore, the current study found a statistically significant association between perceived self-efficacy [AOR = 0.25 (0.20-0.32)] and poor adherence to COVID-19 preventive measures among the study participants. Another similar study conducted in Ethiopia reported that having no perceived efficacy was significantly associated with poor adherence to COVID-19 preventive measures (15). The discrepancy may be due to the socio-cultural differences between the two areas of communities.
Overall, the current study found more than half of the study participants had poor adherence to COVID-19 preventive measures. Therefore, to reduce these gaps and to increase the implementation of COVID-19 preventive measures, and manage the COVID-19 pandemic, the local and federal governments should design the appropriate intervention strategies based on the level of community understanding.
Conclusion
Appropriate implementation of COVID-19 preventive measures among community members is required to manage or control COVID-19 pandemics and reduce health-related consequences associated with COVID-19 pandemics. The current study, on the other hand, discovered that less than half of the study participants had poor adherence. As a result, in order to manage this pandemic, the relevant organizations, including the government and non-governmental organizations, must take appropriate and timely measures.
Limitations of the Study
A community-based cross-sectional study design was used, and data was collected at predetermined time intervals. As a result, cause and effect relationships could not be investigated.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical clearance was taken from Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University. In addition, permission letters were obtained from all the concerned organization/bodies and from participants. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AE conceived the idea and had major roles in the data review, drafting, and editing the manuscript. All authors contributed to data analysis, drafting and revising the manuscript, and have read and approved the final version of the manuscript to be published and agreed on all aspects of this work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to extend their deepest thank to Haramaya University, College of Health and Medical Science Community Based Education (CBE) office and staff for providing their constructive support.
Abbreviations
CDC, Center for Disease Control and Prevention; COVID-19, Coronavirus disease, 2019; CSA, Center of Statistical Agency; ETB, Ethiopian Birr; HH, Household; MERS, Middle Eastern Respiratory Syndrome; SD, Standard Deviation; UNICEF, United Nations Children's Fund; WHO, World Health Organization.
References
1. Lango MN. How did we get here? Short history of COVID-19 and other coronavirus-related epidemics. Head Neck. (2020) 42:1535–8. doi: 10.1002/hed.26275
2. Adela N, Nkengazong L, Ambe LA, Ebogo JT, Medou Mba F, Goni HO, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. (2020) 14:e0008700. doi: 10.1371/journal.pntd.0008700
3. Asefa A, Qanche Q, Hailemariam S, Dhuguma T, Nigussie T. Risk perception towards COVID-19 and its associated factors among waiters in selected towns of southwest Ethiopia. Risk Manag Healthc Policy. (2020) 13:2601. doi: 10.2147/RMHP.S276257
4. Grant MC, Geoghegan L, Arbyn M, Mohammed Z, McGuinness L, Clarke EL, et al. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): a systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE. (2020) 15:e0234765. doi: 10.1371/journal.pone.0234765
5. Omemo P, Wasonga J. Determinants of adherence to the recommended COVID-19 Prevention and Control Guidelines by Small Scale Retail Shop Operators in Rural Parts of Siaya County, Kenya. J Epidemiol Public Health Rev. (2020) 5. doi: 10.16966/2471-8211.198
6. Ditekemena JD, Nkamba DM, Muhindo HM, Fodjo Siewe JN, Luhata C, Van den Bergh R, et al. Factors associated with adherence to COVID-19 prevention measures in the Democratic Republic of the Congo (DRC): results of an online survey. BMJ Open. (2021) 11:e043356. doi: 10.1136/bmjopen-2020-043356
7. Breevoort A, Carosso GA, Mostajo-Radji MA. High-altitude populations need special considerations for COVID-19. Nat Commun. (2020) 11:1–3. doi: 10.1038/s41467-020-17131-6
8. Deressa W, Worku A, Abebe W, Getachew S, Amogne W. Social distancing and preventive practices of government employees in response to COVID-19 in Ethiopia. PLoS ONE. (2020) 16:e0257112. doi: 10.1371/journal.pone.0257112
9. Bante A, Mersha A, Tesfaye A, Tsegaye B, Shibiru S, Ayele G, et al. Adherence with COVID-19 preventive measures and associated factors among residents of Dirashe District, Southern Ethiopia. Patient Prefer Adher. (2021) 15:237. doi: 10.2147/PPA.S293647
10. Weiss BD, Paasche-Orlow MK. Disparities in adherence to COVID-19 public health recommendations. Health Lit Res Pract. (2020) 4:e171–3. doi: 10.3928/24748307-20200723-01
11. Azene ZN, Merid MW, Muluneh AG, Geberu DM, Kassa GM, Yenit MK, et al. Adherence towards COVID-19 mitigation measures and its associated factors among Gondar City residents: a community-based cross-sectional study in Northwest Ethiopia. PLoS ONE. (2020) 15:e0244265. doi: 10.1371/journal.pone.0244265
12. UNICEF. RCCE Action Plan Guidance COVID-19 Preparedness and Response. Gonder city: UNICEF (2019).
13. Asnakew Z, Asrese K, Andualem M. Community risk perception and compliance with preventive measures for COVID-19 pandemic in Ethiopia. Risk Manag Healthc Policy. (2020) 13:2887–97. doi: 10.2147/RMHP.S279907
14. Wolff K, Larsen S, Øgaard T. How to define and measure risk perceptions. Annals Tour Res. (2019) 79:102759. doi: 10.1016/j.annals.2019.102759
15. Qanche Q, Asefa A, Nigussie T, Hailemariam S, Duguma T. Knowledge of COVID-19 and preventive behaviors among waiters working in food and drinking establishments in Southwest Ethiopia. PLoS ONE. (2021) 16:e0245753. doi: 10.1371/journal.pone.0245753
16. Al-Hanawi MK, Angawi K, Alshareef N, Qattan AMN, Helmy HZ, Abudawood Y, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. (2020) 8:217. doi: 10.3389/fpubh.2020.00217
17. Irigoyen-Camacho ME, Velazquez-Alva MC, Zepeda-Zepeda MA, Cabrer-Rosales MF, Lazarevich I, Castaño-Seiquer A. Effect of income level and perception of susceptibility and severity of COVID-19 on stay-at-home preventive behavior in a group of older adults in Mexico City. Int J Environ Res Public Health. (2020) 17:7418. doi: 10.3390/ijerph17207418
Keywords: community, COVID-19, preventive measure, novel coronavirus, Ethiopia
Citation: Eyeberu A, Debella A, Mengistu DA, Arkew M, Hailu S, Oljira A, Yusuf Kebira J, Getachew T, Nigussie S, Bekele D, Belete R, Abate D, Bekele H, Tefera T, Alemu A and Dessie Y (2022) Perceived Self Efficacy in Implementing COVID-19 Preventive Measures Among Residents of Harari Regional State, Eastern Ethiopia: A Community-Based Cross-Sectional Study. Front. Epidemiol. 2:849015. doi: 10.3389/fepid.2022.849015
Received: 05 January 2022; Accepted: 22 March 2022;
Published: 25 April 2022.
Edited by:
Shengjie Lai, University of Southampton, United KingdomReviewed by:
Yijun Lou, Hong Kong Polytechnic University, Hong Kong SAR, ChinaJuanjuan Zhang, Fudan University, China
Copyright © 2022 Eyeberu, Debella, Mengistu, Arkew, Hailu, Oljira, Yusuf Kebira, Getachew, Nigussie, Bekele, Belete, Abate, Bekele, Tefera, Alemu and Dessie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adera Debella, YWtzYW5hZGVyYTYyQGdtYWlsLmNvbQ==; orcid.org/0000-0002-8060-0027