 Yan Ma†
Yan Ma† Linlin Jia
Linlin Jia- School of International Pharmaceutical Business, China Pharmaceutical University, Nanjing, China
Medical waste has a high environmental risk, economic development and medical policies can affect medical waste generation. Per capita gross domestic product (GDP) is an important indicator to measure the macroeconomic development status, and the tiered medical policy plays an important role in the process of China’s medical reform. The study considered the Environmental Kuznets Curve (EKC) of medical waste generation (MWG) in eight cities in China from 2013 to 2019, using economic indicator (GDP per capita) and policy indicator (tiered medical policy) to reveal the impact of economic development and medical policy on MWG. Furthermore, residents, especially the elderly, are the main consumers of medical resources, and medical institutions are the main places where medical waste is generated. Education level can affect waste management practices. Therefore, the research introduced population size, number of medical institutions, aging degree and education level as control variables. The results confirmed the validity of the N-shaped EKC curve between medical waste and GDP per capita. The amount of medical waste would continue to increase with economic growth, but the growth rate was not fixed. Implementing the tiered medical policy had shown a trend towards reducing medical waste. Population size and aging degree positively affected the generation of medical waste. The number of medical institutions negatively affected the generation of medical waste. The effect of education level on MWG could be ignored. Based on the empirical analysis results, this research put forward relevant policy suggestions in the light of medical waste management practice in China.
1 Introduction
Medical waste is a unique pollutant with infectious, polluting and toxicity produced by medical institutions in diagnosis, treatment, prevention and care (Lee et al., 1991). Because it carries a large number of pathogenic microorganisms, harmful chemicals and even radioactive substances (Chaerul et al., 2008), medical waste has a high risk of environmental pollution. It releases large quantities of harmful gases when stored in the open air (Hossain et al., 2011), releases carcinogens when burned (Windfeld and Brooks, 2015), and causes serious health threats for health technicians, garbage cleaners, patients and their families when disposed randomly (Mohammed and Elias, 2017). In addition, the scouring of pathogenic bacteria and heavy metals carried by medical waste into the soil will affect the survival of animals and plants (Mavakala et al., 2016). Improper disposal of medical waste during the COVID-19 epidemic may also be a new source of infection. As a solid line of defense for public health safety, medical waste management has always received widespread attention from the international community (Cao et al., 2021). Since the promulgation and implementation of the Regulations on the Administration of Medical Wastes (State Council of the People’s Republic of China, 2003), China has also formed a standardized medical waste management system, which has gradually been supplemented and improved under the new requirements of policy standards. After the outbreak of the COVID-19 epidemic, General Secretary Xi Jinping put forward higher demands on the collection and disposal of medical waste, the management of medical waste and environmental risks have once again attracted significant great attention from the state and widely concerned by the public (You et al., 2020).
In recent years, the medical waste generation (MWG) in China is growing. According to the Ministry of Ecology and Environment statistics, there were 547,500 tons of medical waste in 261 large and medium-sized cities in China in 2013 (Ministry of Ecology and Environment of the People’s Republic of China, 2019). By 2019, the number of medical waste in 196 large and medium-sized cities increased to 843,000 tons (Ministry of Ecology and Environment of the People’s Republic of China, 2020). As of the end of 2019, a total of 442 hazardous waste licenses were issued nationwide for the disposal of medical waste, and the actual amount of medical waste handled by licensees was 1.18 million tons (Ministry of Ecology and Environment of the People’s Republic of China, 2020). Since the beginning of 2020, the COVID-19 epidemic has greatly affected the quality and quantity of waste generated, including municipal solid waste and medical waste (Hantoko et al., 2021). The amount of medical waste has increased sharply in responding to the COVID-19 outbreak and the national production of medical waste was expected to increase by more than 25% in 2020 compared to 2019 (Silva et al., 2020). At the same time, China’s medical waste disposal capacity has increased by 27% compared with that before the epidemic, from 4,903 tons per day to 6,227 tons per day, and the medical waste disposal rate has basically reached 100% (Hbzhan, 2021). Although the basic medical waste disposal system in China has been established, with the ever-increasing amount of medical waste, the expanding medical waste disposal market needs to be further standardized. In order to curb environmental pollution and health threats of medical waste, we must increase our attention and understanding of the issue of medical waste, carrying out proper and targeted planning for the control and management of waste generation (Aldieri et al., 2019). This study explores the factors affecting the generation of medical waste, which is of great significance to medical waste management.
The relationship between the economic system and the environmental system has always been the focus and hotspot of many scholars in the field of environmental economics. Studies showed that the amount of waste was related to economic development level of a country or region (Marinković et al., 2005). With the rapid development of the economy, the continuous progress of medical technology and the significant improvement of medical level, the multi-purpose medical equipment has been transformed into safer, single-purpose medical equipment, leading to a rapid increase in MWG (Mbongew et al., 2008). At the same time, economic growth is accompanied by the gradual improvement of people’s living standards, more and more people can afford modern medical services. The increase in the number of doctor visits further leads to an increase in MWG (Yu et al., 2018). It can be seen that there is also a significant relationship between MWG and economic development (Windfeld and Brooks, 2015). Generally, the Environmental Kuznets Curve (EKC) model was considered to be an important model for evaluating the relationship between municipal solid waste (MSW) generation and economic factors, and per capita gross domestic product (GDP) was an important economic indicator in the model (Fu et al., 2015; Chen, 2018; Khandelwal et al., 2019). Although medical waste is a kind of MSW, few articles had studied the relationship between economic growth and medical waste based on the EKC model. Therefore, it is valuable to study the relationship between economic growth and MWG based on the EKC model with GDP per capita as an economic indicator.
Studies have found that government policies can significantly affect waste generation (Shams et al., 2017) and that government regulations, taxes and support programs play an important role in waste management (Malinauskaite et al., 2017). Many countries implement waste policies to control waste generation. Marti and Puertas (2021) determined the effectiveness of policies by analyzing the status of waste management in 41 OECD and EU member States and found that countries with high levels of participation in environmental treaties have made significant progress in waste management and can reduce waste generation to some extent. More specifically, Caniato et al. (2015) proposed that medical policy has an important impact on the management structure of medical waste, and thus on the amount of medical waste produced. Since the implementation of the new medical reform in China, tiered medical policy has always been promoted as the core content, the purpose of which is to reshape the order of residents’ medical treatment, improve the efficiency of medical services and save medical resources through the implementation of measures such as primary consultation, up-and-down collaboration, two-way referral and rapid and slow separation. In 2015, the General Office of the State Council issued the Guiding Opinions on Propelling the Building of a Hierarchical Diagnosis and Treatment System (General Office of the State Council of the People’s Republic of China, 2015). It proposed that by 2017, the policy system for tiered medical should be gradually improved, and that by 2020, the capacity of tiered medical services should be comprehensively improved. Some scholars have verified the effectiveness of tiered medical policy for saving medical resources based on the Andersen model and difference-in-difference method (Gong and Sun, 2021), but the effect of the implementation of tiered medical policy on the MWG need to be further studied.
Based on the above analysis, the impact of economic growth and tiered medical policy on medical waste is a matter of concern. At the same time, population size (Ansari et al., 2019), the number of beds in medical institutions (Su and Chen, 2018), the number of medical institutions (Wei et al., 2020), age structure data (Çetinkaya et al., 2020), education level (Mattar et al., 2018), healthcare spending per capita (Windfeld and Brooks, 2015) and so on could also affect the generation of medical waste. In addition, previous studies on the influencing factors of medical waste were mostly based on multiple linear regression models (Windfeld and Brooks, 2015; Korkut, 2018), stochastic impact by regression on population, affluence and technology (STIRPAT) models (Cheng et al., 2020; Wei et al., 2020) and correlation analysis (Minoglou and Komilis, 2018; Ansari et al., 2019), few used the EKC model (Su and Chen, 2018).
This research established the EKC model with panel data of eight cities in China, and the main research objectives were as follows. First, descriptively analyzed the time trend of the amount of medical waste in China. Second, verified the relationship between the per capita GDP and MWG of each city. Third, investigated the impact of implementing the tiered medical policy on MWG in each region. Finally, comprehensively analyzed the influence of other factors on MWG. This study can fill the vacancy of related research on the EKC hypothesis in the field of medical waste in China, and can also evaluate the implementation effectiveness of the tiered medical policy from an environmental perspective.
This study consists of five parts: introduction, literature review, data and methods, results and discussions, and the last part of conclusions and policy recommendations.
2 Literature Review
The literature review firstly sorted out the theoretical basis and related research of the EKC hypothesis, and then reviewed the relevant empirical research on economic development, policy and medical waste generation.
2.1 Related Research on the Environmental Kuznets Curve Model
The Kuznets curve hypothesis originated from Kuznets’ original research in 1955, which revealed an inverted U-shaped relationship between per capita income and income inequality. As per capita income increased, income inequality exhibited the same increasing trend in the initial period, but began to decline after reaching a turning point. Therefore, the initial stage of income growth was characterized by an unequal distribution of income, but as the economy grew, the distribution of income gradually became more equal (Kuznets, 1955). Subsequently, Grossman and Krueger, 1995 proposed the environmental Kuznets curve (EKC) to describe the inverted U-shaped relationship between economic development and environmental quality, arguing that economic growth leads to environmental degradation, but that when economic income reaches a certain level, the environmental degradation degree decreases with economic development. The EKC hypothesis attracted a lot of attention in the 1990s. However, influenced by other factors, the environmental Kuznets curve is not necessarily an inverted U-shaped and may be positive U-shaped, positive N-shaped, inverted N-shaped, monotonically increasing, monotonically decreasing, or even irregular shapes. At present, environmental degradation and environmental quality decline have been issues of global concern. Many scholars used the EKC hypothesis to study the relationship between economic development and environmental quality. Table 1 lists the relevant studies based on the EKC model in the past 5 years.
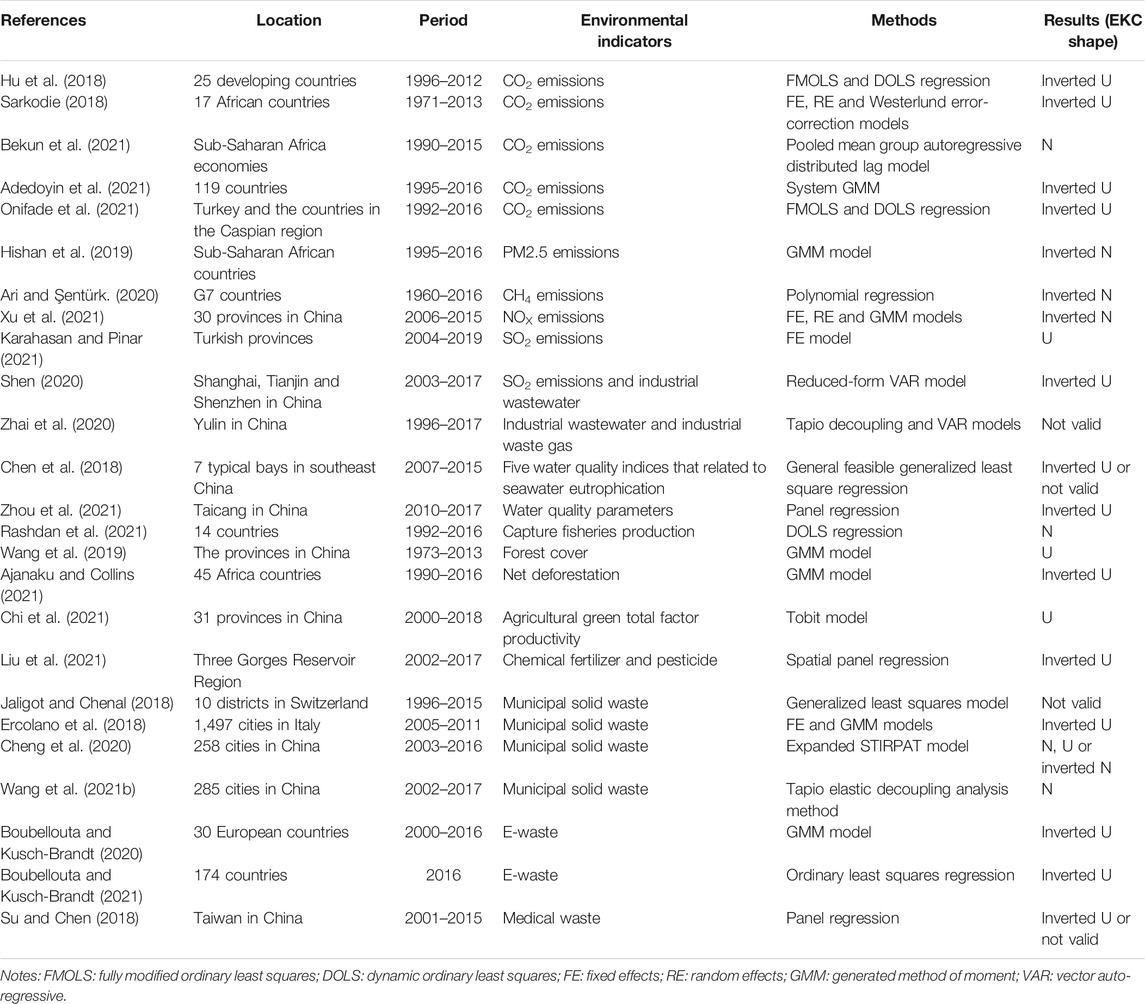
TABLE 1. Compilation of studies on the EKC hypothesis in the past 5 years.
Due to the wide application range of the EKC model, the environmental indicators of related research involved a variety of environmental issues. Table 1 shows that most of the research focused on air pollutant emission, water quality, industrial wastewater emission, land resource quality, solid waste and so on, especially carbon emission was a hot topic in EKC hypothesis research (Bashir et al., 2021). Few studies involved the field of medical waste. Chinese contributed the largest number of EKC research (Bashir et al., 2021), but in the field of medical waste, only Su and Chen (2018) verified the existence of an inverted U-shaped EKC in illegal disposal of medical waste in Taiwan, finding the linear relationship between MWG and economic growth. No studies had yet investigated the validity of the EKC hypothesis in medical waste in mainland China. Furthermore, Table 1 shows that, even for the same topic, differences in research methods and data still make the EKC shape uncertain. Therefore, the validity of the EKC hypothesis in medical waste in mainland China and the shape of the EKC curve are issues worth exploring. Although there are many literatures related to the EKC hypothesis, this study is still innovative and valuable.
2.2 Empirical Research on Economic Development, Policy and Medical Waste Generation
In previous studies, Windfeld and Brooks (2015) found a linear relationship between per capita GDP and MWG by regression analysis based on data from 14 countries. Minoglou and Komilis (2018) selected 16 economic, social, health and environmental indicators from 41 countries, finding a significant positive correlation between GDP and waste generation by regression models and principal component analysis. Based on the STIRPAT model to quantify the impact of socio-economic factors on medical waste in China since the outbreak of SARS, Wei et al. (2020) also found significant positive correlation between medical waste production and GDP. Ansari et al. (2019) conducted a correlation analysis on the economic indices and environmental performance indices of hospital solid waste in developing countries, finding that per capita GDP in developing countries was significantly correlated with hospital solid waste generation rate. It can be seen that the previous research mainly focused on the correlation and linear relationship between MWG and economic growth, and few studied the relationship between economic growth and medical waste generation based on the EKC model.
The EKC hypothesis states that environmental quality will only improve after reaching a certain economic threshold. If the EKC hypotheses are correct, achieving economic growth will be accompanied by environmental degradation, and failure to implement policy measures to prevent environmental damage could lead to severe ecological consequences (Usman et al., 2019). Therefore, many countries implement waste policies to control the increase in waste.
In recent years, many studies have investigated the impact of policy implementation on MSW generation. Cheng et al. (2020) verified that implementing waste charging policy can effectively reduce the generation of MSW based on panel data of 258 cities in China. Jaligot and Chenal (2018) used time-series data on policy implementation in ten regions of the Swiss canton’s Vaud, finding that the waste bag tax policy was significantly associated with a reduction in MSW production. Zhao et al. (2020) analyzed the effectiveness of the second MSW source classification plan based on the consideration of urban spatial interactions in China, finding that the policy significantly reduced MSW production. Medical waste belongs to a category of municipal solid waste, and the impact of policy implementation on medical waste is also worthy of attention. Based on empirical research, Su and Chen (2018) found that implementing the disease diagnosis-related group (DRG) policy can effectively reduce the generation and illegal disposal of medical waste, which means that medical policy implementation may have an important impact on medical waste. The tiered medical policy is the core of China’s new medical reform, and its impact on MWG is worth exploring.
In conclusion, there was no research based on panel data in mainland China to verify the existence of the EKC phenomenon and the effectiveness of the tiered medical policy from the perspective of medical waste. Therefore, this study used the panel data of eight cities in China from 2013 to 2019 to establish an environmental Kuznets curve model to study the relationship between economic growth and MWG, analyzing the impact of implementing tiered medical policy on MWG.
3 Data and Methods
3.1 Summary of Selected Variables
3.1.1 Dependent Variable
Medical waste generation. Medical waste is direct or indirect hazardous waste produced by medical and health institutions in diagnosis and treatment, nursing and other related activities, mainly including infectious waste, pathological waste, damaging waste, pharmaceutical waste, chemical waste. With the development of the economy, the expansion of the medical system and the epidemic of the COVID-19 in 2019, the demand and consumption of medical equipment and medical supplies have increased significantly (Bloom et al., 2018), and MWG is also gradually increasing. The generation of large amounts of medical waste poses a direct threat to the environment and public health, and the generation of medical waste needs to be safely and properly controlled and managed (Peng et al., 2020). Therefore, MWG was selected as the dependent variable in this research.
3.1.2 Independent Variables
GDP per capita. GDP per capita is an important index to reflect the economic development, and an effective tool to understand and grasp the macroeconomic operation of a country or region. Many studies have confirmed a significant positive correlation between per capita GDP and MWG (Minoglou and Komilis, 2018; Wei et al., 2020), arguing that the faster the economy develops, the more medical products and services are consumed, the more medical waste is generated. However, other studies have found that when the economy reaches a certain stage, the growth of GDP per capita is associated with the reduction of waste (Ercolano et al., 2018; Cheng et al., 2020). There is no consensus on the relationship between GDP per capita and MWG. Therefore, GDP per capita was selected as the core independent variable to study the EKC relationship between economic growth and MWG.
Tiered medical policy. The purpose of implementing tiered medical policy is to reshape the structure of the medical service system and allocate medical resources rationally, which can fundamentally reduce the double waste of medical resources in primary medical institutions and large hospitals. Based on empirical analysis, Gong and Sun (2021) found that implementing tiered medical policy has significantly saved diagnosis and treatment service resources and improved the utilization efficiency of medical resources. However, no research has paid attention to whether tiered medical policy can further reduce MWG while reducing the waste of medical resources. Although the time for exploring tiered medical varied from place to place, the first list of pilot cities was officially finalized at the national level in August 2016 to promote the pilot work of tiered medical on a large scale (National Health Commission of the People’s Republic of China, 2016). This research used 2017 as the node to study the impact of the implementation of the tiered medical policy on MWG.
3.1.3 Control Variables
3.1.3.1 Population Size
The population is considered to be a major factor affecting waste emissions (Sin et al., 2005) and is also a direct cause leading to medical waste generation (Wei et al., 2020). Ansari et al. (2019) found that in the past 2 decades, the amount of medical waste in developing countries has been increasing as the population has grown. China is the most populous country in the world. The larger the population, the more medical resources are consumed and the more medical waste is generated. Wei et al. (2020) used an environmental stress model (STIRPAT) and a time series model (Autoregressive Integrated Moving Average, ARIMA) to predict the trend of medical waste generation in China, finding that by 2030, even without the COVID-19 pandemic, based on China’s population size, MWG would still be more than 50% higher than in 2018. Therefore, it is necessary to consider the effect of population size on MWG.
3.1.3.2 Number of Medical Institutions
Medical institutions are the main places where medical behaviors occur and medical resources are consumed. Health technicians generate a large amount of medical waste when performing diagnostic, treatment and nursing activities. From 2013 to 2019, the number of medical institutions in China increased by about 30,000 (National Health Commission of the People’s Republic of China, 2020; 2019). Research showed that as the number of medical institutions increases, so will medical waste and pollutants (Kalogiannidou et al., 2018). However, since 2009, China has launched the “Medical Waste Management Project for Medical Institutions”, which promotes medical institutions to replace disposable medical supplies with repetitive medical supplies as much as possible, and recycle part of the recyclable materials in medical waste to reduce the generation of medical waste from the source. Therefore, the relationship between the number of medical institutions and the MWG needs to be further verified.
3.1.3.3 Ageing Degree
The ability of people to save health capital will decrease with the increase of age, and the depreciation rate of the elderly health capital is higher, which increases the elderly demand for medical care services (Hao et al., 2020), in turn leading to an increase in medical waste. Based on empirical analysis, Brownlee et al. (2017) found that in developed countries, rapid population aging is the main reason for the increase in hospital usage, and this growing usage has resulted in a corresponding increase in the hospital solid waste generation rate. With aging population in China increasing, many studies also showed that areas with a deeper aging degree have greater medical needs and higher utilization of medical services and medical resources (Li and Yang, 2017; Zhan and Zhang, 2017), generating more medical waste. Therefore, age structure data especially aging degree is an important determinant of the generation of medical waste.
3.1.3.4 Education level
MWG is generally related to the consumption of medical resources or medical services and the environmental knowledge and waste management practices of medical personnel and staff. Wang (2011) and Lu et al. (2017) indicated that education level has a significant impact on the public’s demand for medical services, which in turn affects the consumption of medical resources and the generation of medical waste. Education level is also critical for medical staff to effectively manage medical waste (Windfeld and Brooks, 2015), and improving the education level of staff in healthcare facilities may help improve medical waste management practices, thereby reducing the amount of medical waste. Furthermore, highly educated people are more concerned about environmental issues and have more environmentally conscious behavioral intentions (Torgler and García-Valinas, 2007). Therefore, the effect of education on MWG is inconclusive.
3.2 Variable Descriptions and Data Sources
The study selected panel data from eight cities in China from 2013 to 2019 for empirical research, including Shanghai, Beijing, Guangzhou, Chengdu, Hangzhou, Chongqing, Wuhan, and Zhengzhou. The specific variables are shown in Table 2. The data on MWG were derived from the Annual Reports on the Prevention and Control of Environmental Pollution by Municipal Solid Waste (2014–2020) and due to the availability of data, the study could only obtain the specific values of the top 10 cities in the annual amount of MWG. In addition, this study used 2017 as the key time node for advancing tiered medical policy. The data of each city’s GDP per capita, permanent population, number of medical institutions, the proportion of the elderly population over 65, and the proportion of university students in the population aged six and over were derived from the statistical yearbooks of each city (2014–2020) and National Statistics Yearbook (2014–2020). Among them, some urban statistical yearbooks lacked the proportion of the elderly population over 65 and the proportion of university students aged six and over, replaced by provincial data. The summary statistics for each variable are shown in Table 3.
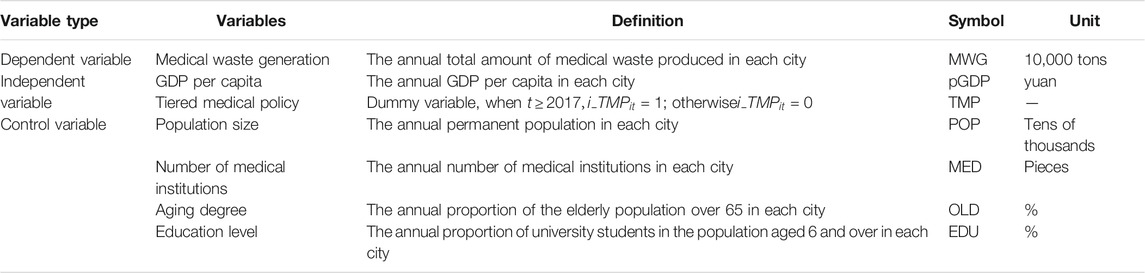
TABLE 2. Descriptions of variables.
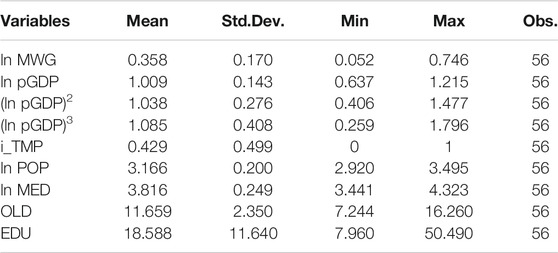
TABLE 3. Summary statistics of variables.
3.3 Research Models
The study used the panel data of eight cities from 2013 to 2019. In order to capture the heterogeneity among individuals, the estimation strategy for panel data usually adopts the individual effect model:
Among them,
Based on the individual effect model, this study constructed the EKC models 1, 2, and 3 of MWG.
3.3.1 Environmental Kuznets Curve Model of Economic Growth and Medical Waste Generation
Considering the complexity of the relationship between economic variables and environmental variables, we introduced the linear, square, cubic terms of GDP per capita as independent variables to construct a simple EKC model 1 between economic growth and MWG:
Among them, the environmental variable
Depending on the estimated coefficients, there will be a different EKC relationship between GDP per capita and MWG (Table 4).
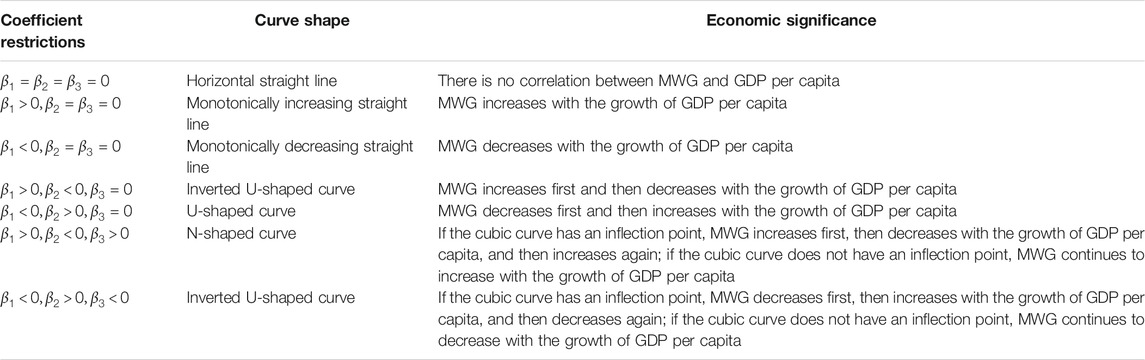
TABLE 4. The estimated coefficients, curve shape and economic significance of EKC model.
3.3.2 Environmental Kuznets Curve Model of Economic Growth, Tiered Medical Policy and Medical Waste Generation
The implementation of the tiered medical policy can promote the rational allocation of medical resources and reduce the waste of medical resources. From the perspective of medical waste, we examined the effectiveness of the tiered medical policy, introduced policy dummy variable into the simple EKC model, and constructed model 2:
Among them,
3.3.3 Robustness Test of Environmental Kuznets Curve Model
The research mainly focuses on the impact of economic growth and medical policy on the amount of medical waste, but the population size, number of medical institutions, aging degree and education level also affect the generation of medical waste. Therefore, the control variables were added to the model to test the robustness of the research results, and constructed model 3:
Among them,
3.3.4 Estimation Strategy
The individual effect model includes two estimation strategies, the fixed effect model and the random effect model, the differences of which depends on whether the individual effect is related to other independent variables. The Hausman test can be introduced to determine which estimator is more effective (Hausman, 1978). The results of the Hausman test in this study showed that using the individual fixed effect model is more effective, and the estimation process are as follows:
Given an individual
Eq. 1 minus Eq. 5, and get the dispersion form of the original model:
Define
It can be seen that the individual fixed effects can obtain a consistent estimator by performing dispersion transformation on the model and eliminating
4 Results and Discussions
4.1 Analysis of the Total Amount of Medical Waste Generation
According to statistics from the Ministry of Ecology and Environment, in recent years, the number of large and medium-sized cities that published medical waste statistics in China has been on the decline overall, but the total amount of medical waste counted has been on the rise (Figure 1). Among them, the amount of MWG in the top 10 cities has increased year by year, accounting for the proportion of total medical waste statistics that has gradually stabilized after 2014 (Figure 2).
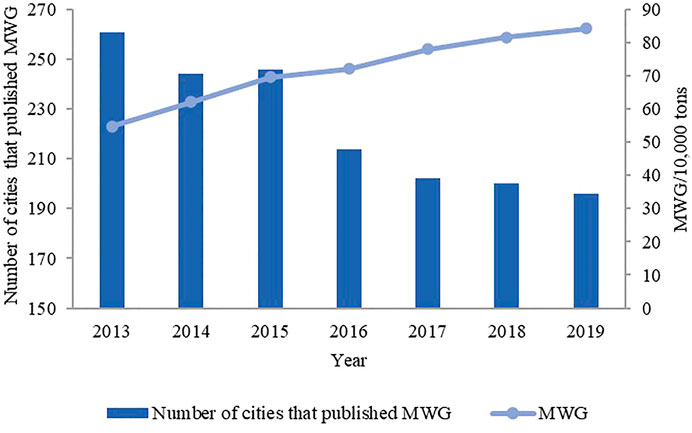
FIGURE 1. Number of cities that published medical waste statistics each year and annual MWG.
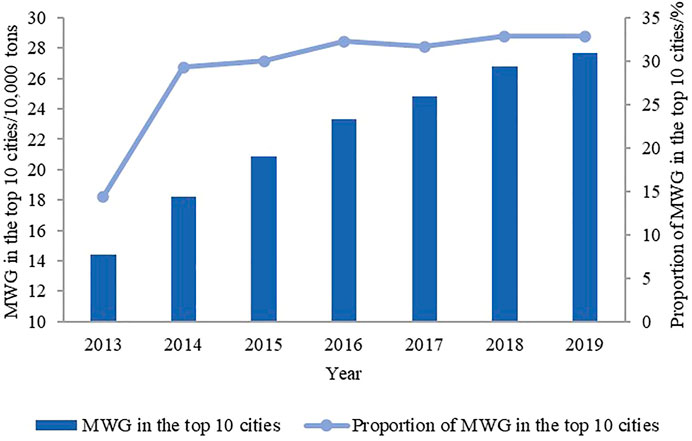
FIGURE 2. The amount and proportion of MWG in the top 10 cities.
Figure 3 shows the amount of MWG in eight cities from 2013 to 2019. Among them, Shanghai and Beijing produced the most medical waste, far exceeding other cities, due to they are the most economically developed regions in China, with a large population, advanced medical technology and abundant medical resources. It can be found from the figure that there are significant differences in the time trends of MWG in eight regions. Waste production in Beijing has been growing steadily, while Shanghai’s waste production has been growing relatively fast in the early stage, showing a slowdown in 2019. In addition, the waste production in Chengdu shows a trend of first increasing, then decreasing and finally increasing. The waste production in Hangzhou shows a negative growth in 2019, and the waste production in Wuhan shows a trend of first decreasing and then increasing. However, the GDP per capita of each region is increasing year by year. It indicates that there is a nonlinear relationship between economic growth and MWG.
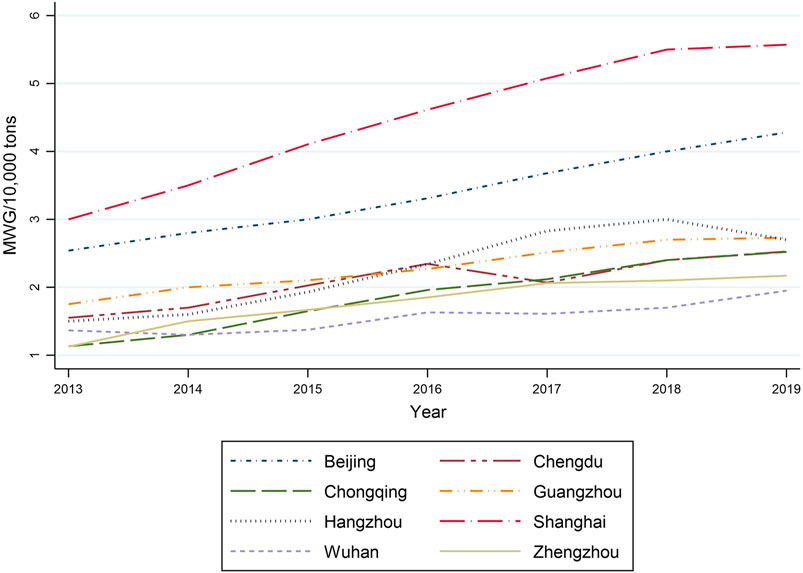
FIGURE 3. The amount of MWG in eight cities from 2013 to 2019.
4.2 Model Regression Results and Discussions
We regressed the simple EKC model 1 which contained only economic variable and the EKC model 2 which introduced the policy dummy variable, respectively, to study the impact of GDP per capita and tiered medical policy on MWG. Then we regressed the EKC model 3 that introduced the control variables to study the effect of the control variables on MWG and test the robustness of the regression results of the models 1 and 2. The results are shown in Table 5.
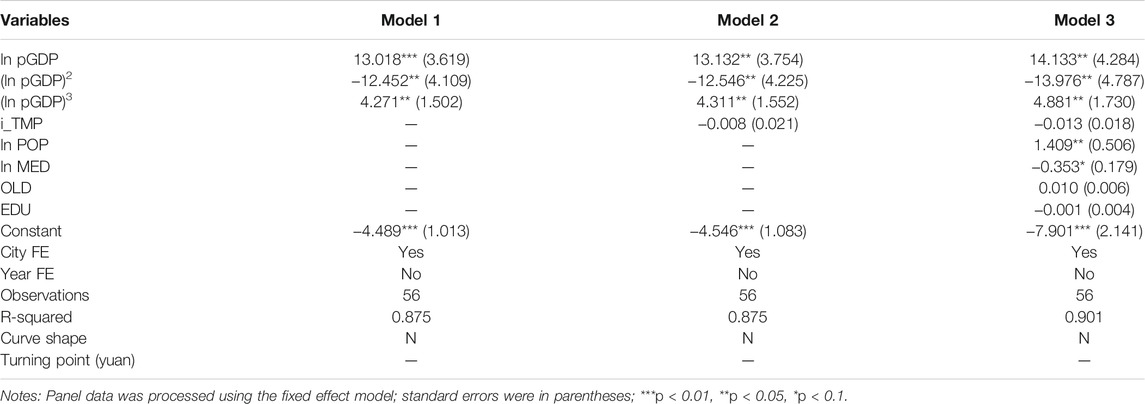
TABLE 5. Regression results of the EKC models of MWG.
The results showed that the EKC curve between GDP per capita and MWG was N-shaped. The coefficients of linear, square and cubic terms were positive, negative, and positive, respectively, and were all significant at the level of 5%. The introduction of other variables in models 2 and 3 did not affect the sign and significance of the coefficient of GDP per capita. The EKC curve diagram shows no inflection point in the cubic curve, which means that MWG increases with the growth of GDP per capita, showing a monotonous increasing trend (Figure 4). However, the growth rate of MWG slowed down and then accelerated with the growth of GDP per capita. As Figure 4 shows, waste production growth slows significantly when the GDP per capita level is within a certain range. It was calculated that when GDP per capita was around 93,700 yuan, the growth rate of medical waste was the slowest. Among the eight cities, Chongqing’s GDP per capita in 2019 was 75,800 yuan, and the impact of economic growth on MWG was still at a gradual weakening stage. GDP per capita in other regions has exceeded 93,700 yuan, and the growth rate of medical waste has gradually accelerated with economic growth.
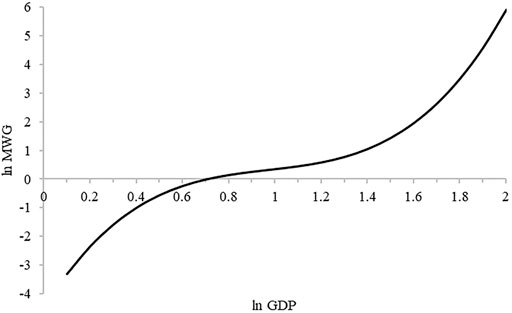
FIGURE 4. EKC curve between GDP per capita and MWG.
There was a significant N-shaped relationship between GDP per capita and MWG. However, the curve had no inflection point, showing a monotonous increasing trend, which confirms the conclusion that hospital solid waste in developing countries was significantly related to GDP per capita (Ansari et al., 2019). Nevertheless, it was different from Karagiannidis et al. (2010), Windfeld and Brooks (2015), Su and Chen (2018) and others’ research results, which observing a linear incremental relationship between economic growth and MWG. The study holds that the two rapid growth stages of MWG with GDP per capita growth are due to the change of public health care needs at different stages of economic development. Traditional economic theories indicate that the most important factor influencing the satisfaction of individual needs is the individual income level. When the economic development level is relatively low and medical resources are less accessible, to meet the basic medical services and health needs of the public, various regions continue to improve the level of medical and health technology. The continuous expansion of the scale of medical production factors and the widespread use of disposable medical consumables lead to a rapid increase in medical waste (Khan et al., 2019). With further GDP per capita improvement, public health awareness deepens, and personalized, diversified and high-level health care needs are further stimulated (Han et al., 2017). Studies have shown a significant positive correlation between health care expenditure and GDP per capita, and health care expenditures tend to grow faster than GDP per capita in the long run (Hensher et al., 2020). Therefore, rapid economic growth will stimulate public demand for health care and increase medical services (Russo et al., 2016), thereby contributing to the high generation of medical waste.
The regression results of models 2 and 3 showed that the implementation of the tiered medical policy reduced the generation of medical waste, with regression coefficients of −0.008 and −0.013, but the impact was not significant (p > 0.1). The purpose of implementing the tiered medical policy is to classify the disease according to the severity and urgency, and to reshape the order of medical treatment through primary consultation, up-and-down collaboration and rigorous referral (Sepulveda et al., 2008), so that patients can make full use of medical resources while receiving reasonable diversion, reducing the waste of medical resources and the generation of medical waste. Previous empirical research results have proved that the implementation of the tiered medical policy can significantly reduce emergency visits and the average length of hospital stay (Gong and Sun, 2021). However, the effect of this policy has not yet been reflected in the reduction of medical waste. It may be because the comprehensive promotion and implementation of the policy is not long, coupled with the policy lag period, the effect of the policy has not yet been significantly manifested. It may also be due to the lack of depth of implementation of the tiered medical policy and the improvement of policy effectiveness is mainly driven by the number of policies, rather than the quality of the policies (Wu et al., 2021). The policy has only a short-term effect on the correction of medical treatment orders and the reasonable allocation of medical resources (Wang et al., 2021a), which will not have a major impact on MWG with the long-term policy effect disappearing. It may also be because the implementation of the tiered medical policy is not yet in place, and some problems in the implementation process have not been resolved. At present, in the implementation of tiered medical, the proportion of primary consultations at the grassroots level is between 50 and 60%, which is still far from the target of 70%. The proportion of primary medical institutions in the total number of visits has dropped from 61.82% in 2009 to 53.04% in 2018, with no upward trend (Zhang, 2020). The medical treatment structure cannot achieve a reasonable balance, the waste of medical resources still cannot be improved, and the generation of medical waste will not decrease.
Population size was significantly positively correlated with the increase in MWG, with a coefficient of 1.409, which was significant at the statistical level of 5%, indicating a 1.41% increase in MWG for every 1% increase in population size. It is consistent with the empirical research results of Wei et al. (2020) on medical waste, that for every 1% increases in population size, MWG increased by 2.47%. It can be seen that the population size is still the main influencing factor of MWG in China. In addition, some scholars directly used the fitting equation between the MWG rate and the population to estimate Istanbul’s future medical waste volume (Korkut, 2018). Medical waste is a direct product of people in the process of medical treatment. The increase in population size will inevitably lead to an increase in the demand for medical and health services and the utilization of medical resources, thereby leading to an increase in MWG.
The number of medical institutions significantly affected MWG at the statistical level of 10%. For every 1% increase in the number of medical institutions, the production of medical waste decreased by 0.35%, contrary to the results of previous studies. Wei et al. (2020) found that for every 1% increase in the number of medical institutions, medical waste increased by 0.40%. Medical institutions are the main places where medical waste is generated. In order to reduce the adverse environmental impact of persistent organic pollutants in the process of medical waste disposal, the source reduction of medical waste has been listed as one of the key tasks in the world (Mohammed and Elias, 2017). The Medical Waste Management Project for Medical Institutions organized and implemented by the Hospital Management Institute of the Ministry of Health in China from 2009 to 2017 also focused on promoting the reduction, harmlessness, and recycling of medical waste at the source (Li et al., 2020). In the process of implementation, many medical institutions used the PDCA concept to manage medical waste reduction, which not only improved the staff’s awareness of classified collection and recyclability, but also achieved the actual effect of medical waste reduction (Zhang et al., 2011; Liang et al., 2016; Zhang et al., 2019). Therefore, even if the number of medical institutions continues to increase, the in-depth advancement of medical waste reduction work may still be able to control the amount of MWG effectively.
Increased aging degree contributed to an increase in the production of medical waste. For every 1% increase in the degree of aging, the amount of medical waste would increase by 0.01%, although the impact was not significant enough at present (p > 0.1). Many scholars have found that age is an important factor affecting medical expenses (Colombier and Weber, 2011; Breyer et al., 2015). Compared with the population under 65, the medical expenses of the elderly have increased more rapidly (Fuchs, 1984). With the continuous growth of the elderly population, the demand for health and medical treatment is increasing, and the increase in the utilization of medical resources will lead to more medical wastes. According to calculations, the average life expectancy in China increases from 76.3 years in 2015 to 77.3 years in 2019 (National Health Commission of the People’s Republic of China, 2020); the total fertility rate in 2020 reduced to 1.3 extremely low fertility levels (Wang and Li, 2021); the aging rate in China is expected to reach 21% in 2035, entering the stage of a super-aging society (Li and Du, 2021). Although the impact of aging on medical waste is currently slight, in the future, as the aging problem increases, medical demand and medical pressure further deepen, the amount of medical waste generated will inevitably increase.
The regression coefficient of education level was -0.001, and the significance level was greater than 10%, which indicated that the impact of education on MWG was weak. Su and Chen (2018) also confirmed that education level had no significant effect on medical waste generation. On the one hand, education helps to raising environmental protection awareness of medical personnel and public (Gaeta et al., 2017) and the willingness to contribute to the environment (Ercolano et al., 2014). Education can also promote medical waste management practices of health care technicians to some extent (Williams, 2014). So the improvement of educational level may negatively affect the generation of medical waste. On the other hand, since people with higher levels of education are more aware of health and may consume more medical services to minimize the risk of disease, an increase in the level of education will increase the utilization rate of public health services (Rhodes et al., 2008), which in turn will positively affect the generation of medical waste. In summary, the negative and positive effects cancel each other out, and the impact of education on the amount of medical waste becomes slight.
5 Conclusion and Policy Recommendations
The generation and disposal of medical waste have a high environmental risk. In order to prevent and control its serious threats to human health and the ecological environment, reducing the generation of medical waste from the source has become an important task. Using the panel data of eight cities from 2013 to 2019, the research discussed the impact of GDP per capita, tiered medical policy and other factors on medical waste, which provides a theoretical basis for medical waste management practice in China and has some reference significance to other developing countries.
The conclusions of the research are as follows:
First, the EKC curve between medical waste and GDP per capita was N-shaped, economic growth was a key factor affecting the amount of MWG. Since the curve had not inflection point, the amount of MWG gradually increased with economic growth, but the growth rate changed from fast to slow with economic growth, and then from slow to faster.
Second, the implementation of the tiered medical policy could reduce the generation of medical waste, but the impact was not significant enough, which confirmed the effectiveness of the policy to some extent, and also showed that the policy effect was still limited.
Third, population size was an important factor influencing MWG and the increasing aging degree promoted the generation of medical waste. Although the impact was not significant, the medical and environmental pressures with the aging trend cannot be ignored. The increase in the number of medical institutions negatively affected the generation of medical waste, benefitting from the in-depth advancement of medical waste reduction work in medical institutions. Education level had no significant effect on the amount of MWG.
Based on the research conclusions and the background of the COVID-19 epidemic, we put forward the following suggestions:
First, improve medical waste capacity of collection, transfer and disposal. Although the amount of MWG was monotonically increasing with economic development, the growth rate of waste generation varied in different periods of development. The economic development level of various regions in China is not balanced. Different regions should arrange the construction of medical waste disposal facilities in advance according to the law of development to improve the capacity of medical waste disposal. In addition, the size of the population and the degree of aging could affect the generation of medical waste. For areas with denser populations and serious aging, it is necessary to increase the number of medical waste disposal institutions and facilities to relieve the pressure on waste disposal in a timely manner. At the national level, a modern medical waste collection, transportation and disposal system and governance system that combines centralized disposal and self-disposal, territorial responsibility and regional coordination should be established to improve the modern level of medical waste collection, transportation and disposal. At the same time, it is necessary to put forward practical key link management technical points to guide grass-roots supervisors and front-line collection and transfer staff, quickly improve the efficiency of medical waste disposal and supervision, and reduce environmental pollution and health risks in key processes.
Second, actively promote the landing of tiered medical policy. The implementation of the policy of tiered medical has shown a negative impact on medical waste, but at present, the effectiveness of the policy is not significant enough, and the reform measures are not yet in place. As patients pay more attention to the quality and effectiveness of diagnosis and treatment, economic incentives have little effect on guiding the public’s medical behavior, and the siphoning effect of public hospitals is still significant. Therefore, in response to the shortage of high-quality medical resources at the grass-roots level, it is urgent to actively introduce excellent doctors and high-quality resources to the primary medical institutions. It is not only necessary to increase the introduction of talents in traditional Chinese medicine, rehabilitation, and nursing to improve the management of chronic diseases at the grass-roots level, but also to expand the drug catalogue of primary medical institutions to meet patient needs. Furthermore, government decision-making departments should increase the motivation for reform, realize coordinated comprehensive management and policy compatibility between different departments, pay more attention to the implementation of policies, actively promote the landing of tiered medical, and improve the effectiveness of reforms.
Third, continue to promote the reduction of medical waste. The most important step in medical waste management is to minimize the generation of waste. With the core purpose of reducing the generation of medical waste, we should clarify the classification of medical waste according to the disposal technology, encourage recycling, and plan from the source to avoid waste. With economic growth, increased health awareness, and aging problems, the increasing demand for medical and health in the future will lead to a large amount of medical waste, which also puts forward higher requirements on the waste management capabilities of medical institutions. Medical institutions, especially primary medical institutions, should further strengthen policy advocacy and practical training of medical waste management, improve the awareness of medical personnel in the classification and collection of recyclable waste, and reduce the use of disposable medical consumables, thereby reducing the generation of medical waste from the source. At the same time, medical waste management should be incorporated into the overall hospital management system, an effective medical waste management responsibility system and performance appraisal system should be established, and the reduction of medical waste should be continuously promoted. The management department should implement information-based supervision, keep abreast of the changes and problems in the progress of reduction work, promoting the scientific development of medical waste management.
Fourth, improve the emergency management system of medical waste. In the context of the epidemic and normalization of the COVID-19, along with the increase in infection cases, MWG is also increasing accordingly. In order to avoid secondary disasters caused by the COVID-19 epidemic and secondary pollution caused by medical waste, it is critical to establish a sound emergency management system for medical waste. First of all, medical waste should be classified reasonably, and biosafety control technology should be integrated into waste classification facilities. Highly infectious medical waste, general medical waste and general domestic waste shall be managed by source classification and diversion. Secondly, promote the standardization of emergency disposal of medical waste, formulate technical specifications and unified technical requirements in combination with the level of epidemic prevention and control of infectious diseases. Finally, it is necessary to establish daily joint prevention and control mechanism and coordinated emergency response mechanism during major epidemics involving multiple departments. Based on the daily supervision of medical waste, the interaction between the departments of health, ecological environment, transportation, and housing and urban-rural construction should be strengthened, and a long-term mechanism for emergency disposal of medical waste should be established.
This study investigated the EKC phenomenon in the field of medical waste, and also examined the implementation effect of the tiered medical policy from the perspective of medical waste. Since the study was based on analysis of macro data released by the Chinese government, the findings were general but not targeted. Due to the limited literature currently available on the EKC phenomenon in medical waste, a comparison of the EKC shapes cannot be made. In the future, more micro-data are needed to support the relevant empirical research on the EKC phenomenon of medical waste, and the research perspective can also be extended to other countries.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Author Contributions
YM (Co-first author) collected the latest literature and information, made major revisions and improvements to the manuscript. LJ (Co-first author) conceptualized the study, analyzed the data and led drafting the manuscript. YH led data collection and contributed to drafting. XW (Corresponding author) directed the revision and arrangement of the entire manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors sincerely thank the editor and the reviewers of this paper.
Abbreviations
ARIMA, Autoregressive Integrated Moving Average; Covid-19, Corona Virus Disease 2019; DOLS, Dynamic Ordinary Least Squares; DRG, Diagnosis-related Group; EKC, Environmental Kuznets curve; FE, Fixed Effects; FMOLS, Fully Modified Ordinary Least Squares; GDP, Gross Domestic Product; GMM, Generated Method of Moment; MSW, Municipal Solid Waste; MWG, Medical Waste Generation; RE, Random Effects; STIRPAT, Stochastic Impact by Regression on Population, Affluence and Technology; VAR, Vector Auto-regressive.
References
Adedoyin, F. F., Nwulu, N., and Bekun, F. V. (2021). Environmental Degradation, Energy Consumption and Sustainable Development: Accounting for the Role of Economic Complexities with Evidence from World Bank Income Clusters. Bus Strat Env 30 (5), 2727–2740. doi:10.1002/bse.2774
Ajanaku, B. A., and Collins, A. R. (2021). Economic Growth and Deforestation in African Countries: Is the Environmental Kuznets Curve Hypothesis Applicable? For. Pol. Econ. 129, 102488. doi:10.1016/j.forpol.2021.102488
Aldieri, L., Ioppolo, G., Vinci, C. P., and Yigitcanlar, T. (2019). Waste Recycling Patents and Environmental Innovations: an Economic Analysis of Policy Instruments in the USA, Japan and Europe. Waste Manag. 95, 612–619. doi:10.1016/j.wasman.2019.06.045
Ansari, M., Ehrampoush, M. H., Farzadkia, M., and Ahmadi, E. (2019). Dynamic Assessment of Economic and Environmental Performance index and Generation, Composition, Environmental and Human Health Risks of Hospital Solid Waste in Developing Countries; A State of the Art of Review. Environ. Int. 132, 105073. doi:10.1016/j.envint.2019.105073
Ari, I., and Şentürk, H. (2020). The Relationship between GDP and Methane Emissions from Solid Waste: a Panel Data Analysis for the G7. Sustainable Prod. Consumption 23, 282–290. doi:10.1016/j.spc.2020.06.004
Bashir, M. F., Ma, B., Bashir, M. A., Bilal,, , and Shahzad, L. (2021). Scientific Data-Driven Evaluation of Academic Publications on Environmental Kuznets Curve. Environ. Sci. Pollut. Res. 28 (14), 16982–16999. doi:10.1007/s11356-021-13110-6
Bekun, F. V., Alola, A. A., Gyamfi, B. A., and Ampomah, A. B. (2021). The Environmental Aspects of Conventional and Clean Energy Policy in Sub-saharan Africa: Is N-Shaped Hypothesis Valid? Environ. Sci. Pollut. Res. 28, 66695–66708. doi:10.1007/s11356-021-14758-w
Bloom, D. E., Khoury, A., and Subbaraman, R. (2018). The Promise and Peril of Universal Health Care. Science 361 (6404), eaat9644. doi:10.1126/science.aat9644
Boubellouta, B., and Kusch-Brandt, S. (2021). Cross-country Evidence on Environmental Kuznets Curve in Waste Electrical and Electronic Equipment for 174 Countries. Sust. Prod. Consumption 25, 136–151. doi:10.1016/j.spc.2020.08.006
Boubellouta, B., and Kusch-Brandt, S. (2020). Testing the Environmental Kuznets Curve Hypothesis for E-Waste in the EU28+2 Countries. J. Clean. Prod. 277, 123371. doi:10.1016/j.jclepro.2020.123371
Breyer, F., Lorenz, N., and Niebel, T. (2015). Health Care Expenditures and Longevity: Is There a Eubie Blake Effect? Eur. J. Health Econ. 16 (1), 95–112. doi:10.1007/s10198-014-0564-x
Brownlee, S., Chalkidou, K., Doust, J., Elshaug, A. G., Glasziou, P., Heath, I., et al. (2017). Evidence for Overuse of Medical Services Around the World. The Lancet 390 (10090), 156–168. doi:10.1016/S0140-6736(16)32585-5
Caniato, M., Tudor, T., and Vaccari, M. (2015). International Governance Structures for Health-Care Waste Management: a Systematic Review of Scientific Literature. J. Environ. Manage. 153, 93–107. doi:10.1016/j.jenvman.2015.01.039
Cao, Y. X., Yu, X. D., Shan, S. J., Wang, L., Chen, G., Zhang, Z. A., et al. (2021). Pollution Prevention Policy on Medical Waste Treatment and Disposal in China: Evolvement, Problem Analysis and Suggestions. Chin. J. Environ. Eng. 15 (2), 389–400.
Çetinkaya, A. Y., Kuzu, S. L., and Demir, A. (2020). Medical Waste Management in a Mid-populated Turkish City and Development of Medical Waste Prediction Model. Environ. Dev. Sustain. 22, 6233–6244. doi:10.1007/s10668-019-00474-6
Chaerul, M., Tanaka, M., and Shekdar, A. V. (2008). A System Dynamics Approach for Hospital Waste Management. Waste Manag. 28 (2), 442–449. doi:10.1016/j.wasman.2007.01.007
Chen, K., Liu, Y., Huang, D., Ke, H., ChenZhang, H. S. B., Zhang, S., et al. (2018). Anthropogenic Activities and Coastal Environmental Quality: a Regional Quantitative Analysis in Southeast China with Management Implications. Environ. Sci. Pollut. Res. 25, 3093–3107. doi:10.1007/s11356-017-9147-6
Chen, Y.-C. (2018). Effects of Urbanization on Municipal Solid Waste Composition. Waste Manag. 79, 828–836. doi:10.1016/j.wasman.2018.04.017
Cheng, J., Shi, F., Yi, J., and Fu, H. (2020). Analysis of the Factors that Affect the Production of Municipal Solid Waste in China. J. Clean. Prod. 259, 120808. doi:10.1016/j.jclepro.2020.120808
Chi, Y., Xu, Y., Wang, X., Jin, F., and Li, J. (2021). A Win-Win Scenario for Agricultural Green Development and Farmers' Agricultural Income: An Empirical Analysis Based on the EKC Hypothesis. Sustainability 13 (15), 8278. doi:10.3390/su13158278
Colombier, C., and Weber, W. (2011). Projecting Health-Care Expenditure for Switzerland: Further Evidence against the 'red-Herring' Hypothesis. Int. J. Health Plann. Mgmt 26 (3), 246–263. doi:10.1002/hpm.1068
Ercolano, S., Gaeta, G. L., and Romano, O. (2014). Environmental Tax Reform and Individual Preferences: an Empirical Analysis on European Micro Data. J. Behav. Exp. Econ. 51, 1–11. doi:10.1016/j.socec.2014.02.008
Ercolano, S., Lucio Gaeta, G. L., Ghinoi, S., and Silvestri, F. (2018). Kuznets Curve in Municipal Solid Waste Production: an Empirical Analysis Based on Municipal-Level Panel Data from the Lombardy Region (Italy). Ecol. Indicators 93, 397–403. doi:10.1016/j.ecolind.2018.05.021
Fu, H.-z., Li, Z.-s., and Wang, R.-h. (2015). Estimating Municipal Solid Waste Generation by Different Activities and Various Resident Groups in Five Provinces of China. Waste Manag. 41, 3–11. doi:10.1016/j.wasman.2015.03.029
Fuchs, V. (1984). "Though Much Is Taken" -- Reflections on Aging, Health, and Medical Care. Milbank. Mem. Fund. Q. Health Soc. 62 (2), 143–166. doi:10.3386/w1269
Gaeta, G. L., Ghinoi, S., and Silvestri, F. (2017). Municipal Performance in Waste Recycling: an Empirical Analysis Based on Data from the Lombardy Region (Italy). Lett. Spat. Resour. Sci. 10, 337–352. doi:10.1007/s12076-017-0188-8
General Office of the State Council of the People’s Republic of China (GPSC) (2015). Guiding Opinions of the General Office of the State council on Propelling the Building of a Hierarchical Diagnosis and Treatment System. Available at: http://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm (Accessed August 2, 2021).
Gong, X. Q., and Sun, C. H. (2021). Can Tiered Medical Service System in China Save Medical Resources? South. China. J. Econ. 5, 34. doi:10.19592/j.cnki.scje.381477
Grossman, G. M., and Krueger, A. B. (1995). Economic Growth and the Environment. Q. J. Econ. 110 (2), 353–377. doi:10.2307/2118443
Han, D. M., Lu, J. X., Li, X. M., and Li, J. (2017). A Development Strategy for China’s Healthcare Industry. Strateg. Study CAE. 19 (2), 21. doi:10.15302/J-SSCAE-2017.02.004
Hantoko, D., Li, X., Pariatamby, A., Yoshikawa, K., Horttanainen, M., and Yan, M. (2021). Challenges and Practices on Waste Management and Disposal during COVID-19 Pandemic. J. Environ. Manage. 286, 112140. doi:10.1016/j.jenvman.2021.112140
Hao, F., Zhang, Y., and Li, X. H. (2020). Estimation of Endogenous Depreciation Rate of Health Capital and Relative Analysis in China. Popul. Dev. 26 (02), 36–48.
Hausman, J. A. (1978). Specification Tests in Econometrics. Econometrica 46 (6), 1251–1271. doi:10.2307/1913827
Hbzhan, (2021). The Second Solid Waste Disposal and Recycling Summit Forum (Medical Waste Special) Ended Successfully. Available at: https://www.hbzhan.com/news/detail/142052.html (Accessed March 1, 2022).
Hensher, M., Tisdell, J., Canny, B., and Zimitat, C. (2020). Health Care and the Future of Economic Growth: Exploring Alternative Perspectives. Hepl 15 (4), 419–439. doi:10.1017/S1744133119000276
Hishan, S. S., Sasmoko,, , Khan, A., Ahmad, J., Hassan, Z. B., Zaman, K., et al. (2019). Access to Clean Technologies, Energy, Finance, and Food: Environmental Sustainability Agenda and its Implications on Sub-saharan African Countries. Environ. Sci. Pollut. Res. 26 (16), 16503–16518. doi:10.1007/s11356-019-05056-7
Hossain, M. S., Santhanam, A., Nik Norulaini, N. A., and Omar, A. K. M. (2011). Clinical Solid Waste Management Practices and its Impact on Human Health and Environment - A Review. Waste Manag. 31 (4), 754–766. doi:10.1016/j.wasman.2010.11.008
Hu, H., Xie, N., Fang, D., and Zhang, X. (2018). The Role of Renewable Energy Consumption and Commercial Services Trade in Carbon Dioxide Reduction: Evidence from 25 Developing Countries. Appl. Energ. 211, 1229–1244. doi:10.1016/j.apenergy.2017.12.019
Jaligot, R., and Chenal, J. (2018). Decoupling Municipal Solid Waste Generation and Economic Growth in the canton of Vaud, Switzerland. Resour. Conservation Recycling 130, 260–266. doi:10.1016/j.resconrec.2017.12.014
Kalogiannidou, K., Nikolakopoulou, E., and Komilis, D. (2018). Generation and Composition of Waste from Medical Histopathology Laboratories. Waste Manag. 79, 435–442. doi:10.1016/j.wasman.2018.08.012
Karagiannidis, A., Papageorgiou, A., Perkoulidis, G., Sanida, G., and Samaras, P. (2010). A Multi-Criteria Assessment of Scenarios on thermal Processing of Infectious Hospital Wastes: a Case Study for Central Macedonia. Waste Manag. 30 (2), 251–262. doi:10.1016/j.wasman.2009.08.015
Karahasan, B. C., and Pinar, M. (2021). The Environmental Kuznets Curve for Turkish Provinces: a Spatial Panel Data Approach. Environ. Sci. Pollut. Res. doi:10.1007/s11356-021-17706-w
Khan, B. A., Cheng, L., Khan, A. A., and Ahmed, H. (2019). Healthcare Waste Management in Asian Developing Countries: a Mini Review. Waste. Manag. Res. 37 (9), 863–875. doi:10.1177/0734242X19857470
Khandelwal, H., Dhar, H., Thalla, A. K., and Kumar, S. (2019). Application of Life Cycle Assessment in Municipal Solid Waste Management: a Worldwide Critical Review. J. Clean. Prod. 209, 630–654. doi:10.1016/j.jclepro.2018.10.233
Korkut, E. N. (2018). Estimations and Analysis of Medical Waste Amounts in the City of Istanbul and Proposing a New Approach for the Estimation of Future Medical Waste Amounts. Waste Manag. 81, 168–176. doi:10.1016/j.wasman.2018.10.004
Lee, C., Huffman, G., and Nalesnik, R. (1991). Medical Waste Management. Environ. Sci. Technol. 25 (3), 360–363. doi:10.1021/es00015a607
Li, L. L., and Du, T. T. (2021). The Effect of Age and Health Care Needs on the Growth of Medical Expenditures: Based on the Empirical Research on Medical Insurance Settlement Data. Contemp. Econ. Manag. 43 (4), 72. doi:10.13253/j.cnki.ddjjgl.2021.04.010
Li, L. L., and Yang, Y. S. (2017). The Impact of Population Aging to the Growth of Health Care Cost. Soc. Secur. Stud. 3, 27.
Li, N., Miao, F. Y., Zhao, S., Yang, L., Zhou, B., Zhang, Y., et al. (2020). To Standardize Management and Realize Harmlessness, Reducing and Recycling of Medical Waste. Chin. Hosp. Archit. Equip. 21 (3), 26. doi:10.3969/j.issn.1671-9174.2020.03.003
Liang, X. L., Huang, J. H., Xu, Y. Q., Shi, J., Chen, F. Y., and Zhou, X. F. (2016). Application Effect of PDCA Circulation Method in Classified Management of Medical Wastes Reduction. China. Med. Pharm. 6 (21), 169. 2095-0616(2016)21-169-04.
Liu, Y., Cheng, X., and Li, W. (2021). Agricultural Chemicals and Sustainable Development: the Agricultural Environment Kuznets Curve Based on Spatial Panel Model. Environ. Sci. Pollut. Res. 28, 51453–51470. doi:10.1007/s11356-021-14294-7
Lu, Z.-N., Chen, H., Hao, Y., Wang, J., Song, X., and Mok, T. M. (2017). The Dynamic Relationship between Environmental Pollution, Economic Development and Public Health: Evidence from China. J. Clean. Prod. 166, 134–147. doi:10.1016/j.jclepro.2017.08.010
Malinauskaite, J., Jouhara, H., Czajczyńska, D., Stanchev, P., Katsou, E., Rostkowski, P., et al. (2017). Municipal Solid Waste Management and Waste-To-Energy in the Context of a Circular Economy and Energy Recycling in Europe. Energy 141, 2013–2044. doi:10.1016/j.energy.2017.11.128
Marinković, N., Vitale, K., Afrić, I., and Janev Holcer, N. (2005). Hazardous Medical Waste Management as a Public Health Issue. Arh. Hig. Rada. Toksikol. 56 (1), 21.
Marti, L., and Puertas, R. (2021). Influence of Environmental Policies on Waste Treatment. Waste Manag. 126, 191–200. doi:10.1016/j.wasman.2021.03.009
Mattar, L., Abiad, M. G., Chalak, A., Diab, M., and Hassan, H. (2018). Attitudes and Behaviors Shaping Household Food Waste Generation: Lessons from Lebanon. J. Clean. Prod. 198, 1219–1223. doi:10.1016/j.jclepro.2018.07.085
Mavakala, B. K., Le Faucheur, S., Mulaji, C. K., Laffite, A., Devarajan, N., Biey, E. M., et al. (2016). Leachates Draining from Controlled Municipal Solid Waste Landfill: Detailed Geochemical Characterization and Toxicity Tests. Waste Manag. 55, 238–248. doi:10.1016/j.wasman.2016.04.028
Mbongwe, B., Mmereki, B. T., and Magashula, A. (2008). Healthcare Waste Management: Current Practices in Selected Healthcare Facilities, Botswana. Waste Manag. 28 (1), 226–233. doi:10.1016/j.wasman.2006.12.019
Ministry of Ecology and Environment of the People's Republic of China (MEE) (2019). Annual Reports on the Prevention and Control of Environmental Pollution by Municipal Solid Waste (2014-2019). Available at: https://www.mee.gov.cn/hjzl/sthjzk/gtfwwrfz/(Accessed August 2, 2021).
Ministry of Ecology and Environment of the People's Republic of China (MEE) (2020). Annual Reports on the Prevention and Control of Environmental Pollution by Municipal Solid Waste. Available at: https://www.mee.gov.cn/hjzl/sthjzk/gtfwwrfz/(Accessed August 2, 2021).
Minoglou, M., and Komilis, D. (2018). Describing Health Care Waste Generation Rates Using Regression Modeling and Principal Component Analysis. Waste Manag. 78, 811–818. doi:10.1016/j.wasman.2018.06.053
Mohammed, A., and Elias, E. (2017). Domestic Solid Waste Management and its Environmental Impacts in Addis Ababa City. J. Environ. Waste. Manag. 4 (1), 194.
National Health Commission of the People’s Republic of China (NHC) (2020). Annual Statistical Bulletin on the Development of Health Services. Available at: http://www.nhc.gov.cn/yzygj/s3593g/201608/eba4b53f5b5745f0a4e51ffd8de802b3.shtml (Accessed August 2, 2021).
National Health Commission of the People’s Republic of China (NHC) (2016). Notice on Promoting the Pilot Work of Hierarchical Diagnosis and Treatment. Available at: http://www.nhc.gov.cn/yzygj/s3593g/201608/eba4b53f5b5745f0a4e51ffd8de802b3.shtml (Accessed August 2, 2021).
National Health Commission of the People’s Republic of China (NHC) (2019). Statistical Bulletin of China's Health Development. Available at: http://www.gov.cn/guoqing/2021-04/09/content_5598657.htm (Accessed February 21, 2022).
Onifade, S. T., Erdoğan, S., Alagöz, M., and Bekun, F. V. (2021). Renewables as a Pathway to Environmental Sustainability Targets in the Era of Trade Liberalization: Empirical Evidence from Turkey and the Caspian Countries. Environ. Sci. Pollut. Res. 28, 41663–41674. doi:10.1007/s11356-021-13684-1
Patrício Silva, A. L., Prata, J. C., Walker, T. R., Campos, D., Duarte, A. C., Soares, A. M. V. M., et al. (2020). Rethinking and Optimising Plastic Waste Management under COVID-19 Pandemic: Policy Solutions Based on Redesign and Reduction of Single-Use Plastics and Personal Protective Equipment. Sci. Total Environ. 742, 140565. doi:10.1016/j.scitotenv.2020.140565
Peng, J., Wu, X., Wang, R., Li, C., Zhang, Q., and Wei, D. (2020). Medical Waste Management Practice during the 2019-2020 Novel Coronavirus Pandemic: Experience in a General Hospital. Am. J. Infect. Control. 48 (8), 918–921. doi:10.1016/j.ajic.2020.05.035
Rashdan, M. O. J., Faisal, F., Tursoy, T., and Pervaiz, R. (2021). Investigating the N-Shape EKC Using Capture Fisheries as a Biodiversity Indicator: Empirical Evidence from Selected 14 Emerging Countries. Environ. Sci. Pollut. Res. 28, 36344–36353. doi:10.1007/s11356-021-13156-6
Rhodes, S. D., Hergenrather, K. C., Zometa, C., Lindstrom, K., and Montaño, J. (2008). Characteristics of Immigrant Latino Men Who Utilize Formal Healthcare Services: Baseline Findings from the HoMBReS Study. J. Natl. Med. Assoc. 100 (10), 1177–1185. doi:10.1016/s0027-9684(15)31476-0
Russo, G., Rego, I., Perelman, J., and Barros, P. P. (2016). A Tale of Loss of Privilege, Resilience and Change: the Impact of the Economic Crisis on Physicians and Medical Services in Portugal. Health Pol. 120 (9), 1079–1086. doi:10.1016/j.healthpol.2016.07.015
Sarkodie, S. A. (2018). The Invisible Hand and EKC Hypothesis: what Are the Drivers of Environmental Degradation and Pollution in Africa? Environ. Sci. Pollut. Res. 25, 21993–22022. doi:10.1007/s11356-018-2347-x
Sepulveda, M.-J., Bodenheimer, T., and Grundy, P. (2008). Primary Care: Can it Solve Employers' Health Care Dilemma? Health Aff. 27 (1), 151–158. doi:10.1377/hlthaff.27.1.151
Shams, S., Sahu, J. N., Rahman, S. M. S., and Ahsan, A. (2017). Sustainable Waste Management Policy in Bangladesh for Reduction of Greenhouse Gases. Sust. Cities Soc. 33, 18–26. doi:10.1016/j.scs.2017.05.008
Shen, Z. (2020). Coordinated Environment and Economy in Coastal Development Based on Industrial Wastewater and SO2 Emissions. J. Coastal Res. 109, 13–18. doi:10.2112/JCR-SI109-003.1
Sin, J., Hee, S., and Lee, A. (2005). Effect of Population Change on Waste Emission: the Case of Busan City. J. Korean Assoc. Reg. Geogr. 11 (6), 559.
State Council of the People’s Republic of China (SC) (2003). Regulations on the Administration of Medical Wastes. Available at: http://www.gov.cn/gongbao/content/2003/content_62236.htm (Accessed August 2, 2021).
Su, E. C.-Y., and Chen, Y.-T. (2018). Policy or Income to Affect the Generation of Medical Wastes: An Application of Environmental Kuznets Curve by Using Taiwan as an Example. J. Clean. Prod. 188, 489–496. doi:10.1016/j.jclepro.2018.04.011
Torgler, B., and García-Valiñas, M. A. (2007). The Determinants of Individuals' Attitudes towards Preventing Environmental Damage. Ecol. Econ. 63, 536–552. doi:10.1016/j.ecolecon.2006.12.013
Usman, O., Iorember, P. T., and Olanipekun, I. O. (2019). Revisiting the Environmental Kuznets Curve (EKC) Hypothesis in India: the Effects of Energy Consumption and Democracy. Environ. Sci. Pollut. Res. 26 (13), 13390–13400. doi:10.1007/s11356-019-04696-z
Wang, J., and Li, X. M. (2021). The Situation of Low Fertility, the Dilemma of Population Policy and the Way Out under the Three-Child Policy in China. Youth. Explor. 4, 50.
Wang, J., Xin, L., and Wang, Y. (2019). Economic Growth, Government Policies, and forest Transition in China. Reg. Environ. Change 19, 1023–1033. doi:10.1007/s10113-018-1450-3
Wang, K.-M. (2011). Health Care Expenditure and Economic Growth: Quantile Panel-type Analysis. Econ. Model. 28 (4), 1536–1549. doi:10.1016/j.econmod.2011.02.008
Wang, C. C., Li, X. W., Wu, R. Y., and Lu, X. (2021a). Evaluation of the Corrective Effect of Hierarchical on “Inverted Triangle” Order of Medical Visits: a Quasi-Natural Experimental Research on Progressive Pilots. Chin. J. Health Pol. 14 (3), 13. doi:10.3969/j.issn.1674-2982.2021.03.003
Wang, K. K., Zhu, Y., and Zhang, J. (2021b). Decoupling Economic Development from Municipal Solid Waste Generation in China's Cities: Assessment and Prediction Based on Tapio Method and EKC Models. Waste Manag. 133, 37–48. doi:10.1016/j.wasman.2021.07.034
Wei, Y., Cui, M., Ye, Z., and Guo, Q. (2021). Environmental Challenges from the Increasing Medical Waste since SARS Outbreak. J. Clean. Prod. 291, 125246. doi:10.1016/j.jclepro.2020.125246
Williams, I. D. (2014). The Importance of Education to Waste (Resource) Management. Waste Manag. 34 (11), 1909–1910. doi:10.1016/j.wasman.2014.08.003
Windfeld, E. S., and Brooks, M. S.-L. (2015). Medical Waste Management - A Review. J. Environ. Manage. 163, 98–108. doi:10.1016/j.jenvman.2015.08.013
Wu, Q. D., Xie, X. Y., Wu, Y., Chen, C. B., Deng, W. W., and Wu, S. Y. (2021). Force and Effect of Policies Associated with the Implementation of Hierarchical Diagnosis and Treatment in China. Chin. Gen. Pract. 34, 4293. doi:10.12114/j.issn.1007-9572.2021.00.253
Xu, B., Zhong, R., Liu, D., and Liu, Y. (2021). Investigating the Impact of Energy Consumption and Nitrogen Fertilizer on NOx Emissions in China Based on the Environmental Kuznets Curve. Environ. Dev. Sustain. 23, 17590–17605. doi:10.1007/s10668-021-01401-4
You, S., Sonne, C., and Ok, Y. S. (2020). COVID-19's Unsustainable Waste Management. Science 368, 1438. doi:10.1126/science.abc7778
Yu, K., Gong, R., Qiu, X., Wang, X., and Luo, Y. (2018). Discussing the Effect of Urban Economic Development on Medical Environment with Lisrel Model. Ekoloji 27 (106), 697.
Zhai, X., Cheng, Z., Ai, K., and Shang, B. (2020). Research on Environmental Sustainability of Coal Cities: a Case Study of Yulin, China. Energies 13 (10), 2470. doi:10.3390/en13102470
Zhan, G. H., and Zhang, X. W. (2017). The Measurement of Test the Correlation Relationship between Aging of Population and Basic Medical Expenditure. J. Shanghai. Adm. Inst. 18 (06), 68.
Zhang, L. F. (2020). A Study on the Effective Strategies of Urban Hierarchical Medical System in the post-epidemic Era. Nanjing. J. Soc. Sci. 4, 7–13.
Zhang, L. W., Feng, C. Y., Liu, T., Jiang, S. F., Li, X. M., Dai, Y. F., et al. (2019). Effect of Quality Control circle on Medical Waste Reduction and Standardized Management. Chin. J. Nosocomiology. 29 (16), 2555.
Zhang, Z. P., Zheng, Y. H., and Chen, R. M. (2011). Role of PDCA Cycle in Improving Quality of Medical Waste Management. Chin. J. Nosocomiology. 21 (17), 3682.
Keywords: medical waste management, environmental kuznets curve, tiered medical policy, aging degree, education level
Citation: Ma Y, Jia L, Hou Y and Wu X (2022) The Impact of Economic Growth and Tiered Medical Policy on the Medical Waste Generation: An Empirical Analysis Based on the Environmental Kuznets Curve Model. Front. Environ. Sci. 10:824435. doi: 10.3389/fenvs.2022.824435
Received: 30 November 2021; Accepted: 02 March 2022;
Published: 24 March 2022.
Edited by:
Jinhui Li, Tsinghua University, ChinaReviewed by:
Festus Victor Bekun, Gelişim Üniversitesi, TurkeyEmrah Bese, Texas A&M University Corpus Christi, United States
Mi Yan, Zhejiang University of Technology, China
Copyright © 2022 Ma, Jia, Hou and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoming Wu, eG13dUBjcHUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship