 Yan Zhao
Yan Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Environ. Sci., 12 October 2022
Sec. Land Use Dynamics
Volume 10 - 2022 | https://doi.org/10.3389/fenvs.2022.1021522
This article is part of the Research TopicLand Use Management and Carbon Abatement in a Sustainable Development PerspectiveView all 12 articles
The problem of elderly service supply is a important issue that must be solved for the development of an aging society. This study uses microdata from the China Health and Retirement Longitudinal Study that were published in 2017 and from a regression analysis using a dichotomous logistic model. Finally, the article examines the factors that affect the supply of elderly services and land use in rural China. The results show that 1) the health level is the most direct influencing factor on whether rural elderly people in rural land can obtain elderly services; 2) the family characteristics that affects the supply of elderly services in rural land is the relationship of living with children rather than the number of children; 3) socio-economic status has an impact on the supply of elderly services, but this impact is limited; and 4) the factors affecting the supply of family elderly services and social elderly services for the rural elderly are basically the same, with the fundamental difference between the two being that the service targets are different, which reflects typological characteristics.
China is a developing country that has entered the aging society earlier than many peer countries and has seen an urban-rural inversion of population aging (Xue et al., 2022; Zhu et al., 2021). The latest data from the its census shows that by the end of 2020, China’s population aged 60 and above reached 260 million, accounting for 18.7% of the total population, with nearly 200 million people aged 65 and above, accounting for 13.5% of the total population. The proportion of people aged 60 and 65 and above in China’s rural areas is 23.81% and 17.72% respectively, values that are 5.11 and 4.22 percentage points higher than the general national level and 7.99 and 6.61 percentage points higher than that in urban areas1. As the economy and social progress develop, elderly services need to emphasize accessibility, satisfaction, and quality (Zhu et al., 2021; Hong et al., 2020). Likewise, pensions need to emphasize the accessibility, satisfaction, and dignity of old age. How to scientifically address the problem of rural elderly service supply has become an important theoretical and practical problem for the government and society to solve (Zheng et al., 2020; Wu et al., 2021).
Why is it that some people have access to senior care and others do not if they have the same mobility issues and need care equally? Why is there a difference in the providers or the manner of access to senior care? International research on the supply of elderly services has begun earlier than in China and has tended to focus on supply subjects, such as families, communities, social organizations, and the state, as well as their relationships of responsibility (Shanas et al., 1969; Cicirelli, 1981; Tennsted et al., 1989). There are three main types of senior care facilities in the United States, namely, general elder care facilities, intermediate elder care facilities, and skilled elder care facilities (Eskildsen and Price, 2009; Carlsen, 2021).
Different types of elderly care facilities provide different specialized services according to the needs of the elderly, such as oral care, medical services, and so on (Daaleman et al., 2009; Dharamsi et al., 2009; Jensen et al., 2009). Previous studies indicate that the longer that older people are sick, the more likely they are to use elderly services (John A. Krout, 1984); those with poor self-care, older people, and “empty nesters” tend to use elderly services more (Calsyn et al., 1999; Murphy et al., 2009). Individual factors of the elderly, such as personal situation, family situation, economic status, and physical condition have an impact on the demand for institutional elderly services, and some key sociodemographic characteristics beyond health and physical functioning characteristics can positively affect the demand for and supply of elderly care (Kraus et al., 1976; Shapiro and Tate, 1985). At the same time, the main body of elderly institutions, management level, occupancy rate, size, and wage level also have an impact on the quality of elderly institutions (Rosko et al., 1995; Bjorkgren et al., 2001). In addition to this, the health care policies and health care costs of nursing facilities also have an impact on the supply of nursing facilities (Newcomer et al., 2016; Hao et al., 2022).
Rural older adults choose to call upon family first when they are ill or require care. This may be related to factors such as the lack of specialized rural services, monetary factors, and the perception that older adults are more self-reliant and do not want to be seen as vulnerable (Coburn, 2002; Morgan et al., 2002). In addition to the primary care provided by the family, informal care provided by other relatives, church networks, and friends and neighbors play a complementary role for daily help for older adults (Kivett, 1985; Mahmoud et al., 2021). Rural seniors, on the other hand, tend to show a lower use of market-based, specialized care services (Rowles et al., 1996). This study analyzes the relevant factors affecting the supply of rural elderly services in China relative to the specific characteristics of micro-individuals.
This study uses data from the China Health and Retirement Longitudinal Study (CHARLS). These data are provided by the National Development Institute of Peking University and form a set of high-quality microdata representative of Chinese middle-aged households and individuals aged 45 and above. The rate of the access response and data quality have been among the highest in the world among similar projects, and it is widely used and recognized for academic studies. The CHARLS survey used a multi-stage sampling method to conduct survey interviews in 150 counties and 450 communities (villages) in 28 provinces (autonomous regions and municipalities of China), such that the conclusions drawn from the sample analysis can have application to the entire elderly population in China.
In this study, we selected 3385 rural people aged 60 and above who are indicated to need care from the total sample of 21,095 in the latest CHARLS (2015) survey data, released to the public in November 2017. The questionnaire included the question “Is there someone to help you when you have difficulties in moving and doing things?” The availability of elderly care services was analyzed. A new analysis sample was formed from 2067 rural elderly people who had access to elderly care services. Does the supply of elderly care services for the urban elderly show the same characteristics and influencing factors as the supply of elderly care services in rural areas? The author compiled a sample of 951 urban elderly with care needs and a sample of 563 urban elderly who received senior care services and then further examined the urban-rural differences in the influencing factors of senior care service provision from an individual micro perspective.
Because the responses in the questionnaire were limited to yes or no, a binary logistic model is suitable for regression analysis. Therefore, this study takes the basic personal characteristics of individuals as the basis; takes health characteristics, socioeconomic status, and family characteristics into consideration; and then constructs a logistic model as follows.
The explained variable in this study is the supply of rural elderly service (YC). The supply status is divided into two cases: ① whether the elderly are provided with elderly services (YC1). The questionnaire asks the elderly whether “someone helps you” in case of difficulty, and if the answer is yes, the elderly are considered supplied with elderly services, recorded as 1 (receive = 1). Otherwise, it is recorded as 0, which means no elderly services are supplied; ② whether they are supplied with specific elderly services. In the study, the types of elderly service providers are divided into two main types: family elderly service (YC2) and social elderly service (YC3), such that the elderly service provided by the corresponding elderly service provider are recorded as 1 (receive = 1); otherwise 0 is recorded. The questionnaire investigates the specific providers of elderly service received by the elderly and lists ten specific ways: 1–5 are relatives, including spouse, parents, children, siblings, and other relatives, 6 are employed persons, 7 are volunteers, 8 are nursing homes, 9 are provided by the community, and 10 are others. In this study, 1–5 are referred to as family elderly service supply, which refers to the elderly service provided by family members and relatives as the main provider, and 6–10 are social elderly service supply, which includes all elderly service provided by non-family members and relatives.
Health variable (health_c). The factors related to basic health are grouped into health variables and measured with three variables: the ADL index and the IADL index, as well as chronic disease (chronic). The ADL index reflects the mobility of the elderly. The ADL scale consists of six items: dressing, bathing, eating on one’s own, getting in and out of bed, going to the toilet, and controlling urination. An elderly person is considered to have lost the ability to care for himself/herself if he/she is unable to perform any of these activities independently and needs assistance for them. The IADL scale investigates whether the respondent has the ability to live independently and consists of six items: difficulty in doing household chores, cooking, shopping, making phone calls, taking medication, and managing money. An elderly person who is unable to do any of these items independently and needs help is considered to have insufficient ability to live independently. ADL and IADL are scored using three levels of measurement: 2 points for “no difficulty” or “difficulty, but can still be completed,” 1 point for “difficulty, need help,” and 0 points for “unable to complete.” Instead of using the self-rated health of the test subjects, a more objective chronic disease (chron) prevalence was used in this study. The questionnaire details 14 chronic diseases: hypertension, hyperlipidemia, blood sugar, malignancy and tumors, lung, liver, heart disease, stroke, kidney, stomach, mental illness, memory-related disorders, joints and rheumatism, and asthma. The elderly may suffer from several chronic diseases at the same time, so the health status of the elderly is evaluated with the chronic disease score, which is calculated with one point per each chronic disease (van der Jadt et al., 2021).
Socioeconomic status variable (soec_c). In this study, four variables are used to capture socioeconomic status: personal income (inc_i), household income (inc_h), medical insurance (ins_m), and pension insurance (ins_p). The income of the rural elderly includes agricultural income, wage income, business income, transfer income, and low-income income, while urban elderly people have the same categories with the exception of agricultural income. Medical insurance and pension insurance are important elements of the social security system and reflect the status of social members. According to the questionnaire for the Health Care and Insurance Database, the options for whether the respondent has medical insurance, 1–5 report urban employees’ medical insurance, urban residents’ medical insurance, new cooperative medical insurance, urban and rural residents’ medical insurance, and public medical insurance, respectively. Respondents who report participating in any of them are recorded as 1, indicating that they had health insurance. Otherwise, they are recorded as 0. According to the Work Retirement and Pension Database questionnaire, “Do you participate in the basic pension insurance for employees of government agencies, institutions or enterprises” and “Do you participate in/receive the following pension insurance: new rural insurance, residents’ pension insurance, or urban residents pension insurance?” The responses were all marked as 1 if they participated in or were receiving any pension insurance; otherwise they were marked as 0.
Family characteristics variable (family_c). Du et al. (2016) argued that even with an adequate supply of social care services, it is still difficult to replace the needs of elder people for their own family members in terms of financial, care, or spiritual needs. Therefore, this study includes the number of living children (child_a) and whether they lived with their children (child_p) among the household characteristics.
Control variables (control), including gender (gen_c), age (age_c), marriage (marri_c), and education level (edu_c).
α0 is a constant term, α1-9 are the coefficients of the corresponding variables, and μ is a random disturbance term for other unobserved factors that have an impact on the supply of elderly services.
From the total sample of 3385 (see Table 1), 61.1% were receiving appropriate senior care services for difficulties in self-care and mobility impairments and were unable to successfully complete activities of daily living items. The average ADL index was 11.328, and the average IADL index was 9.243. The severity of loss of self-care ability was lower than the ability to care for oneself, and on average, each rural elderly person had about two chronic diseases. The health statistics are in line with the practical experience that the elderly who cannot take care of themselves in life are still a minority, and most of them belong to the category of partially declining or lost living ability. The disparity in household incomes among the rural elderly are greater than the personal incomes, and 77.3% of rural elderly had medical insurance, compared to 69.6% who have pension insurance. The average number of surviving children of the surveyed seniors reached 3.683, while only 55 seniors had no surviving children, but only 34% of the seniors lived with their children. There are far more women than men in the sample, with an average age of 70.44. Nearly 70% of the elderly have spouses and live with them, but the education level of the rural elderly is low, with half of them being illiterate or not having graduated from elementary school.
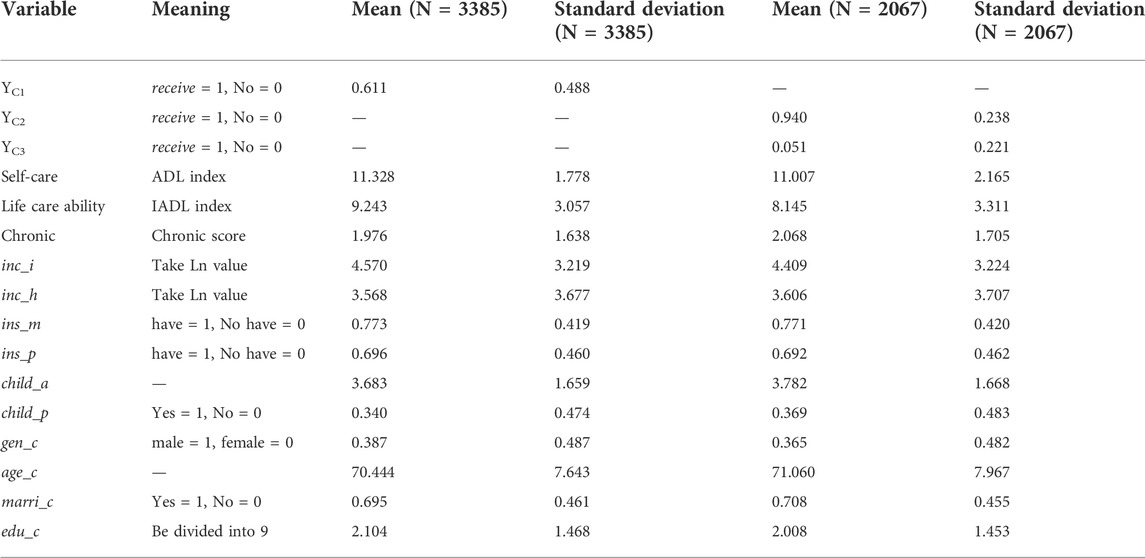
TABLE 1. Primary descriptive statistics.
As can be seen from the rural sample of 2067 that were receiving elderly care services in Table 1, 94% of the elderly received family elderly care services (YC2), and only 5.1% received social elderly care services (YC3). Rural older adults with access to senior care services had lower scores for self-care ability, life care ability, and higher scores for chronic diseases, indicating poorer health. The average personal income of rural elderly was lower than the total sample, and household income was higher. Rural seniors with medical insurance were about the same as the overall level, and those with pension insurance exceeded the overall level by 0.4%. The proportion living with children is 2.9% higher than the overall level, while the number of surviving children had changed little. Overall, more rural seniors who received various types of elderly care services were female (1.86% more), older (0.7 years), had a spouse (1.4% more), and were better educated (about 1% higher).
To avoid possible multicollinearity where there are more explanatory variables and to test the robustness of the model estimation results, this study uses a stepwise logistic regression method. Analytical software was used to progressively regress the health variable (health_c), the socioeconomic status variable (soes_c), and both together, followed by all variables. Therefore, the regression results produce outputs corresponding to model 1–4 (the last of which is the total model).
Model 1,
Model 2,
Model 3,
Model 4, i.e. total model
The regression results are shown in Table 2, and the model fit results have a large LR statistic with a p-value of 0, showing that the models fit well.
1) Influence of health factors on the supply of elderly services
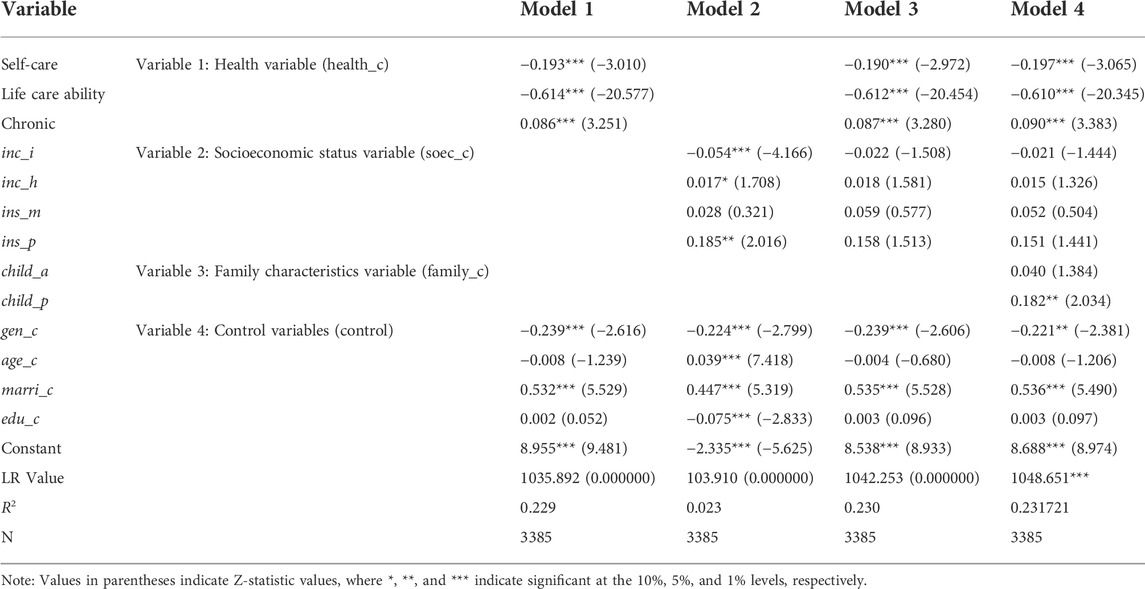
TABLE 2. Regression results for whether the rural elderly can obtain the supply of old-age care services. Explained variable: supply of elderly services (Yc1).
Models 1, 3, and 4 contain health variables, and from the regression results, the health variables show a strong correlation in each model, all of which are significant at the 1% confidence level. The lower the ability of the elderly to take care of themselves (ADL) and their ability to care for themselves (IADL), the more likely they are to receive elderly care services, as shown by the sign of the coefficient (Ren et al., 2022; Wu et al., 2022). The more types of chronic diseases an individual has (chron), the more dependent on elderly services. The results are consistent with practical observations: the health or lack of health of the elderly is the direct reason for receiving elderly care services, with the most services being received based on life care needs, with a regression coefficient value of -0.61, the smallest of all variables regression coefficients, indicating that the elderly will receive more care than other factors. In models 1, 3, and 4, the coefficients of the three health variables have small values and little variation, which implies that health factors are always the most important factor in the elderly’s access to elderly services.
2) Influence of socioeconomic status factors on the supply of elderly services
Model 2 has a low statistical value, although the LR value passes the test. Personal income (inc_i) and household income (inc_h) of the rural elderly were associated with the availability of elderly care services. Personal income has a significant but a negative effect on access to senior care services. That is to say, the lower the personal income of the elderly, the more likely they are to access senior care services. By contrast, household income is positively correlated with access to elderly care services, indicating that the higher the household income, the easier it is to access elderly care services. The reason for this discrepancy may be related to the statistics in the text about the sources of personal and household income. The data in this article include items such as wage income and various types of allowances that may have been available in the past 12 months when counting personal income. Older adults who also have wage income often indicate relative good health and the ability to work, and if the subsidized income is high, this indicates that older adults belong to special groups, such as the elderly, disabled, or orphaned and poor, which are precisely the manifestations of socially vulnerable groups. Household income in statistics mainly includes agricultural and forestry income, low income, and transfer income, which is actually a reflection of the real socio-economic status of the rural elderly. The higher the household income, the greater the help received by the elderly, indicating that the rural elderly have a higher socioeconomic status and receive more elderly care services. Thus, Model 2 can be explained by the fact that non-special (i.e., non-vulnerable) groups tend to receive more elderly care services.
Two social security factors, namely, health insurance (ins_m) and pension insurance (ins_p), have different effects on the availability of elderly services. The health insurance variable did not pass the significance test, while the old-age insurance variable was significant for access to elderly services, and the elderly who were participating in the old-age insurance system were more likely to be cared for. A reasonable interpretation is that Medicare is a cost-sharing mechanism only when there is inpatient care, and that routine medical care and other services are not provided or reimbursed by Medicare. In contrast, the pension insurance system reflects certain income effects, as the pension will directly increase the income of the elderly and can be used as they wish, thus enhancing their socio-economic status (Kumar, 2021). However, in model 3, the effects of both income and social insurance are nonsignificant after including health and socioeconomic status variables together in the model, but the overall goodness of fit of the model is still better than that in model 1. This indicates the limited influence of socioeconomic status factors in China.
3) Influence of household characteristics on the supply of elderly services
From model 4, the number of living children (child_a) is not significant in relation to the availability of elderly care services. In other words, it does not support the traditional equation of “‘more children” with “more happiness,” and parents do not receive more elderly care services because of the number of their children. The relationship between the number of children and the availability of elderly services was not significant. The living with children (child_p) variable passed the test and was significant at the p<5% level, indicating that regardless of the number of children. The elderly receive more senior care whenever they live with their children, meaning that living with children is a favorable condition for intergenerational caregiving behavior to occur. The inclusion of household characteristics variables also led to an increase in the degree of influence of self-care ability and chronic diseases, and a further decrease in the degree of influence of personal income, household income, health insurance, and pension insurance. A possible explanation is that the worse health that the elderly people are in, the likely it is that their children choose to live with them for caregiving reasons.
4) Influence of basic personal characteristics on the supply of elderly services
Among control variables (control), access to elderly care services for rural elderly was significantly associated with gender (gen_c) and marriage (marri_c) in any of the models. Women and elderly people in normal marriages (with spouses) receive more elderly care; 61.3% of the sample were women, who lived longer but were in worse health and thus received more care and received it for longer. The higher z-statistic value of the marriage variable indicates that older adults with normal marriages have more service care from their spouses. Age (age_c), and education level (edu_c) were only significantly correlated in model 2. The reason for this is that age is an important parameter in the design of all kinds of subsidies and social insurance systems in China, and the conditions of participation and benefits are often linked to age. For example, senior citizen benefits are granted to those aged 80 and above, and pensions can only be received when they reach the age of 60. A lower level of education can easily result in people being at the bottom of the social ladder. And their level of awareness often determines whether they are willing to participate in the social insurance system. Therefore the education level is significant in model 2. It is worth noting that in models 1, 3, and 4, the coefficients of the age variables are all negative, indicating that the older you are the less senior care you receive. A possible explanation is that the elderly are a vulnerable group in rural areas and the needs for elderly services are not being met in reality.
Why do some rural elders receive a home care service supply while others receive a social care service supply? What factors are associated with this? Are there common influencing factors? In this study, we construct models 5 and 6 to perform further analysis based on the regression results (see Table 3).
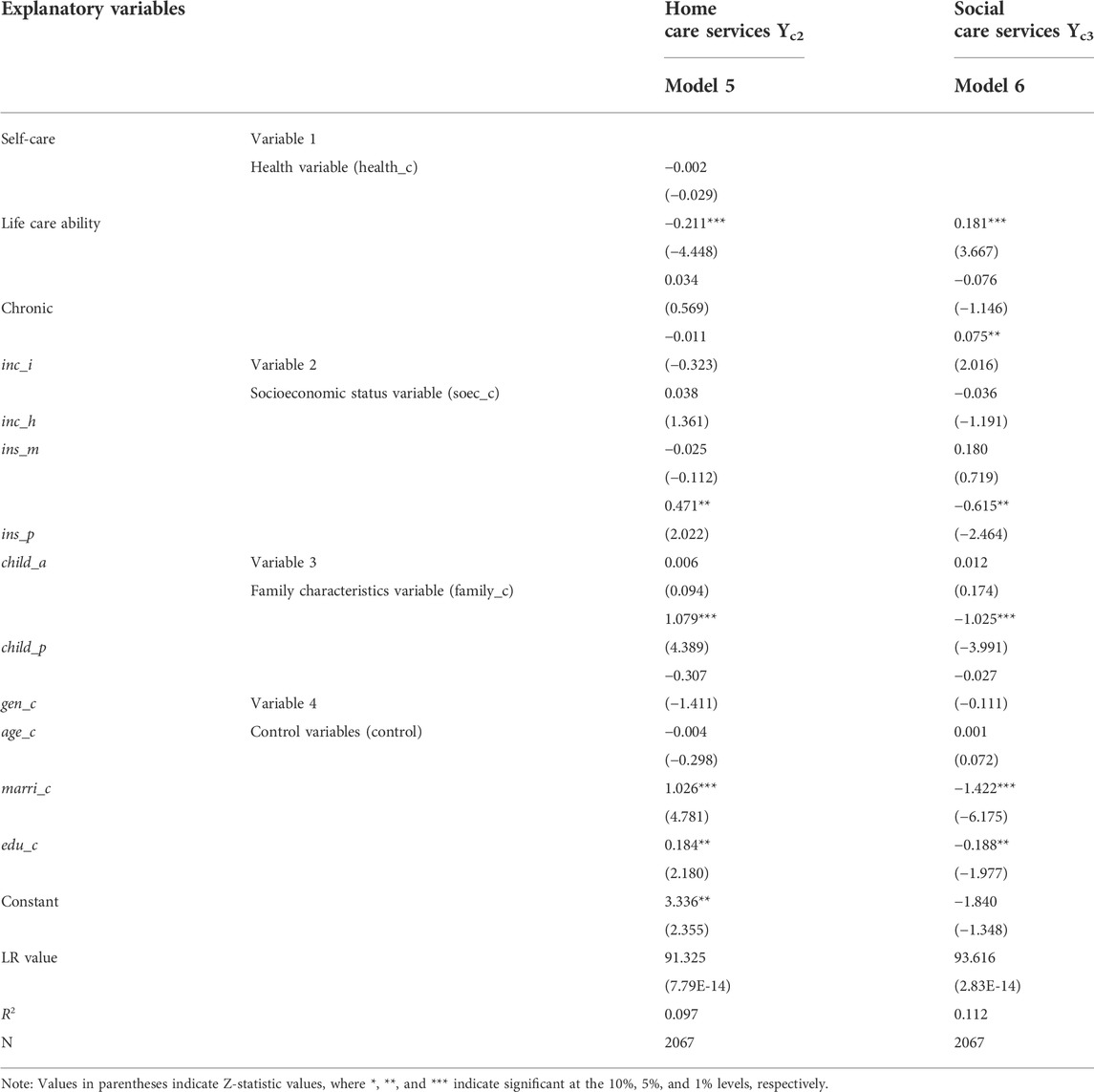
TABLE 3. Regression results of the rural elderly get the main types of old-age service supply.
Model 5,
Model 6,
1) Factors affecting rural elders to obtain home care service provision
In model 5, it can be seen that the ability of rural elderly to care for themselves (IADL) significantly affects the availability of home care service. The less able the older person is to care for themselves, the more home care services they receive. The pension insurance (ins_p) variable is significant at the p<0.05% level and has a positive sign of the coefficient, indicating that rural elders who can receive insurance benefits have an improved socioeconomic status and are more likely to be cared for by their families. The variables for living with children (child_a) and marriage (marri_c) remained significant at the p<0.01% level, indicating that harmonious family and marital relationships contribute to older adults’ obtain in-home elderly care. The education level (edu_c) variable was significant, with the more educated elderly being more likely to receive help from family members. Possible explanations are that the more educated elderly are more reasonable, communicate more easily with their children and spouses, and are better at maintaining harmonious relationships.
2) Factors affecting rural elders to obtain social elderly service supply
The significant influencing variables in the social elderly service supply are also the ability for self-care, living with children, marital status, pension insurance, and education level, showing consistency with the influencing factors of family elderly service provision. However, in contrast to family elderly care services, rural elderly who are better able to take care of themselves, live separately from their children, have abnormal marriages, have no pension insurance, and have low education level receive more social elderly care services. This demonstrates the mutual substitutability between family and social care services for the elderly. This is in line with the findings of Liu (2011), who demonstrated that social elderly care replaces family elderly care to some extent. The individual income variable in model 6 is significant at the p<0.5% level. That is to say, the rural elderly who receive more subsidies of various kinds and assistance funds receive more social elderly services, indicating that the group receiving social elderly services is predominantly a vulnerable group.
To further validate the results and test the robustness of the model, this study conducts a comparative urban-rural analysis of the factors affecting the supply of elderly services.
1) Descriptive statistical analysis
Table 4 shows that 59.2% of urban elderly were provided with elderly care services, a rate that is 1.9% lower than rural elderly. Urban elderly have lower self-care ability than rural elderly, but better life care ability than rural elderly and slightly higher chronic disease score. Urban seniors have higher personal income than rural seniors, but lower household income. Urban seniors have 2.5% less health insurance coverage than rural seniors, and 28.1% less pension insurance than rural seniors. Urban seniors have fewer living children (0.48 fewer children per senior on average) and a higher proportion of children living with them (5.2% higher), they are 1.6% more male than rural, are older (0.678 years more), they and are more educated (urban seniors are close to elementary school graduation, while rural seniors on average have not completed elementary school). However, the percentage of normal marriages is lower than in rural areas (2.4% lower).
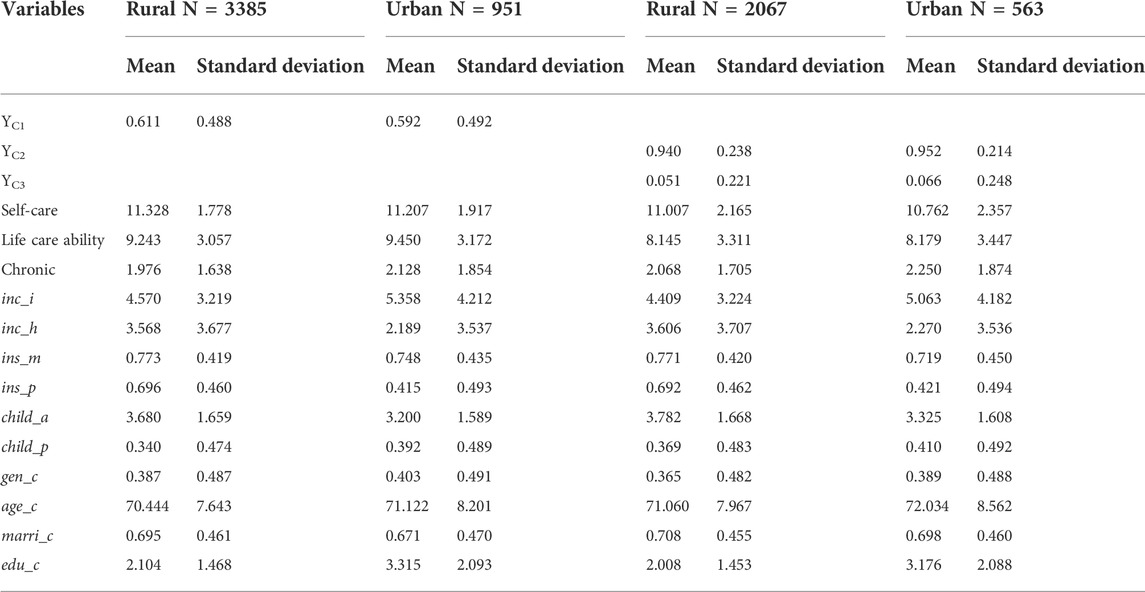
TABLE 4. Statistics of main variables of urban and rural samples 1.
The proportion of both family elderly service and social elderly service received by the urban elderly is higher than that received in rural areas. The 94% of rural seniors were provided with family elderly care services, compared to 95.2% of urban seniors, and 5.1% of rural seniors were provided with social elderly care services, compared to 6.6% of urban seniors, 1.2% and 1.7% higher respectively. Urban seniors are less able to take care of themselves and have higher chronic disease scores, but they have slightly better life care than rural seniors. The average personal income of the urban elderly is higher than that of the rural elderly, and the household income of the urban elderly is lower than that of the rural elderly. The participation rate of medical insurance is 5.2% lower than that of the rural elderly, and the participation rate of pension insurance is 27.1% lower than that of the rural elderly. The number of able-bodied children is still lower than that of the rural elderly, and the proportion of those living together with their children is 4.1% higher than that of the rural elderly. The proportion of urban seniors with access to elderly services rose by 2.4% for men compared to rural seniors, and they were older (about 1 year), more educated (regarding the gap between those who did not finish elementary school and private school graduation), and 1% more were married abnormally. Among urban seniors with access to senior care, the proportion of men rose by 2.4% compared to rural seniors. They were also older (by about 1 year), more educated (the difference between not finishing elementary school and graduating from private school). Marriage had a 1% higher rate.
2) Analysis of regression results
From the regression results (Table 5), the factors affecting the access of urban and rural elderly to elderly services in Model 4 are basically the same, and the significance also shows a high degree of similarity. The differences were in the health factors, with greater z-values for the self-care ability variable for the urban elderly, indicating a greater impact than rural elderly in terms of access to elderly care services. However, the elderly care services obtained due to their ability to care for the duration of life were obtained less often than among the rural elderly, and the significant degree of chronic diseases decreased and was significant at the p<0.1% level. This indicates that although there were differences in the health status of urban and rural elderly, both received the supply of elderly services for health reasons. From the perspective of socioeconomic status, the personal income variable was significant for the urban elderly, which is directly related to the fact that the income and subsidy standards are significantly higher in urban than in rural areas in China. Household income, health insurance, and pension insurance were nonsignificant. It is worth noting that health insurance for the urban elderly was negatively correlated, which may be explained by the difference between urban and rural health care resources, with the urban elderly taking up health care resources in disguise by “hanging on to their beds” (referring to people who occupy hospital beds and refuse to leave the hospital).
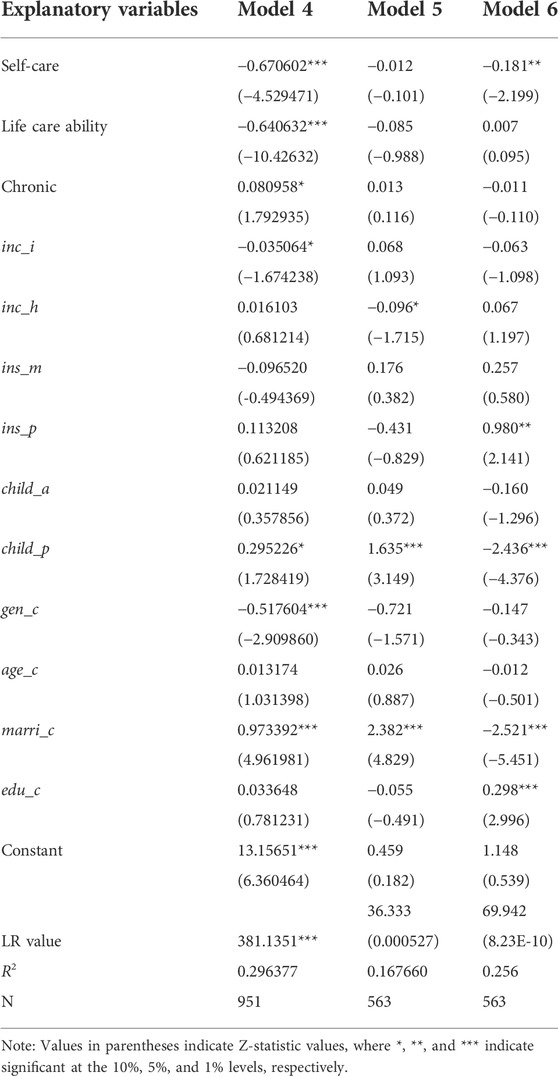
TABLE 5. Regression results of elderly care service supply in urban.
It remains true that the number of living children variable was not significant and that living with children was the only way to get more help. In terms of control variables, the gender factor increased in significance, women received more elderly services, having a spouse significantly affected the availability of elderly services, and the age and education variables were still not significant. However, while urban seniors received more help as they aged, the same was not true for rural seniors.
3) Comparative analysis of urban-rural regression results for the types of elderly service providers
The urban elderly and the rural elderly in Model 5 showed significant differences in the supply of home care services. The urban elderly sample did not have any significant health factors, but the rural elderly life care capacity variable was significant. This suggests that the ability of rural elderly to receive care from family members was directly related to their impaired ability to care for themselves. Among the factors in socioeconomic status, the household income of urban seniors had some effect on the availability of senior care, but it was negatively correlated, with urban seniors with lower incomes receiving more family care. Possible explanations are that urban elderly people lack income from agriculture and forestry, as well as from reforestation and agricultural subsidies, etc. Household income came more from low income and special hardship assistance, relief money, and other sources. The low household income indicates that the elderly in that city were not a vulnerable group and therefore received more services for aging in place. Urban seniors without pension insurance received more family care, unlike rural seniors. This suggests that the income effects of the pension insurance system were different for urban and rural seniors. The urban and rural areas performed exactly the same in the household characteristics variable. Among personal characteristics, only marriage was a significant influencing factor for urban elderly. Unlike the rural elderly, urban elderly with higher education levels received significantly more elderly services supply. In general, among the factors affecting the supply of family care services, urban and rural areas had more differences than commonalities.
In the social elderly service supply (Model 6), urban and rural elderly still show significant differences between urban and rural areas, except for the factors of children living together and marriage. Among the health factors, the self-care ability variable was significant at the p<0.5% level for the urban elderly, and the life care ability variable was significant and more significant for the rural elderly. In terms of socioeconomic status, urban seniors had fewer significant impact variables than rural seniors, the personal income variable was not significant, and only the pension insurance variable was significant. In contrast to rural seniors, the elders with pension insurance made more use of social pension services. Among possible explanations are that socialized retirement resources are more abundant in urban areas than in rural areas, and that the income effect of urban elderly pension insurance allows for market-based purchase of retirement services. Among personal characteristics, the urban elderly with higher education level receive more social elderly care services. Rural elderly are the ones with lower education level are more likely to obtain social elderly services. The reason may be that social welfare homes are mainly for special groups in rural social care services. There were more hired, community, and volunteer forms of support in urban social care services than in rural areas, which are more easily accepted and used by the urban elderly with their higher levels of education.
1) Health level is the most direct factor that affects the availability of elderly services in rural areas
Health variables were consistently significant and had the highest explanatory power for every model. The supply of elderly care services is necessary when the elderly are less able to take care of themselves and are unable to perform basic behaviors such as dressing, eating, getting up, and going to the toilet by themselves. Older people in rural areas receive mainly life care services, most of which are received when they are unable to take care of their daily lives such as cooking, cleaning up after themselves, shopping, taking medicine, and managing money due to their inability to do so. Rural elders in poorer health receive a greater supply of senior services. Once again, research proves that health is a basic human need and that the supply of elderly services is a necessary form of meeting such basic needs of the elderly.
2) Household characteristics that affect the supply of senior care services are the relationship with children living together rather than the number of children
Traditionally, it is believed that the more children you have, the more care you will receive in your old age. The average number of children of elders in the sample was more than three. The truth is that the only “useful” children were re the ones who lived with the elderly, and they were the real providers of senior care services. Parent-child relationships with separation with them, greatly reduced the occurrence of intergenerational mutual aid behaviors. This can affect people’s perceptions of aging and the residential relationship between parents and children. The ability of children to supply elderly care was the most important factor. In terms of accessibility of senior care services, living with children is the best living relationship.
3) Socioeconomic status has an impact on the supply of senior care services, but the impact is limited
Level of personal income (excluding retirement income) was an indication of vulnerability. However, in rural areas this vulnerable group received fewer elderly services, indicating that social security system has not established a corresponding system of elderly services for special groups in China. More security systems are supplied in the form of funds, with more opportunities to issue money and fewer services. The increased economic strength and economic status of rural elderly, as marked by household income, was conducive to an increase in the supply of elderly services. The rural health insurance system is a direct service for health. However, medical care from health insurance is not a substitute for the health care nursing act in elderly services, and China does not currently have a long-term care insurance system. Pensions can enhance the economic and social status of seniors and allow for greater access to senior care. However, China’s current rural pension insurance system is not perfect and does not achieve full coverage; crucially, the pension level is too low, and the effect of the system is limited. Thus, the socioeconomic status of the rural elderly, as determined by income and social insurance factors, has some influence on the availability of elderly services, but it is currently limited.
The salient factors that affected the availability of elderly services supply were the same in rural and urban areas. Elders’ own poor health, family characteristics of living with children, and gender and marital status affected the supply of elderly services. The difference between urban and rural elderly service supply was reflected in the socioeconomic status factor. In rural areas, where the sample size was large, none of the variables indicating economic and social status, which were mainly characterized by the social security system, had no explanatory power. However in urban areas, where the sample size was small, the influence of the individual income variable increased. That is, the availability of elderly services was significant for socially vulnerability. This study argues that the main reason is the difference in the level of urban and rural social security systems.
4) The factors that affected the supply of family elderly care services for rural elderly people were basically the same as the factors for social elderly care services. The main body of rural elderly service supply reflected the type of characteristics.
Health level, socioeconomic status, family characteristics, marital status, and educational attainment determined the type of rural elderly service providers. The supply of family elderly care services and the supply of social elderly care services showed obvious substitution, and the characteristics of the groups that received family elderly care services and social elderly care services were opposite. The effects of living with children and marital status on the types of urban and rural elderly service providers reflected the same characteristics of urban and rural areas. In other words, the elderly people who lived with their children and had normal marriages received more family elderly care services, and those who did not live with their children and had abnormal marriages received more social elderly care services. On the other hand, the rural elderly who obtained social pension services reflected the characteristics of a distinct socially disadvantaged group, with few having pension insurance and most of them not living with their children (most were childless), without spouses, and with even lower education levels. Therefore, the elderly had different types of service needs, and elderly services should \be provided by multiple entities.
Both urban and rural areas showed the characteristics of mainly family elderly service supply and insufficient social elderly service supply. The supply rate of both home care services and socialized care services was higher for urban seniors than for rural seniors. The results of the study prove that there are fundamental differences between family elderly care services and social elderly care services in terms of different service recipients, reflecting typological characteristics. The services provided by the community and volunteers were mostly for the special difficulty groups, often the “three no’s” (no stable source of income, no ability to work, no dependents) elderly who were mainly characterized by economic difficulties, and the elderly services were survival-type services. Market-based purchase of senior care services (hiring others) is minimal, and enjoyable and developmental senior care services are largely non-existent. These differences fully illustrate the differences in the types of elderly service providers due to the different urban and rural identities of the elderly under the dual economic structure of urban and rural areas in China. The main body of rural elderly service provision is single, the market-based supply is not as good as urban areas, and the main body of elderly service supply was not diversified.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
YZ: writing—review and editing, writing—original draft, conceptualization, methodology, funding acquisition, supervision.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1Data from major figures on 2020 population census of China, National Bureau of Statistics of China, 1 July 2021.
Bjorkgren, M. A., Hakkinen, U., and Linna, M. (2001). Measuring efficiency of long-term care units in Finland. Health Care Manag. Sci. 4 (3), 193–200. doi:10.1023/a:1011444815466
Calsyn, R. J., Morse, G. A., and &Allen, G. (1999). Predicting the helping alliance with people with a psychiatric disability. Psychiatric Rehabilitation J. 22 (3), 283–287. doi:10.1037/h0095232
Carlsen, L. (2021). Decent work and economic growth in the European union. A partial order analysis of eurostat SDG 8 data. Green Finance 3 (4), 483–494. doi:10.3934/gf.2021022
Coburn, A. F. (2002). Rural long-term care: What do we need to know to improve policy and programs? J. Rural. Health 5, 256–269. doi:10.1111/j.1748-0361.2002.tb00935.x
Daaleman, T. P., Williams, C. S., Preisser, J. S., Sloane, P. D., Biola, H., and Zimmerman, S. (2009). Advance care planning in nursing homes and assisted living communities. J. Am. Med. Dir. Assoc. 10 (4), 243–251. doi:10.1016/j.jamda.2008.10.015
Dharamsi, S., Jivani, K., Charmaine, D., and Wyatt, C. (2009). Oral care for frail elders:knowledge, attitudes, and practices of long-term care staff. J. Dent. Educ. 73 (5), 581–588. doi:10.1002/j.0022-0337.2009.73.5.tb04733.x
Du, P., Sun, J., Zhang, W., and Wang, X. (2016). The demands of old-age care and the family and social resources for the Chinese elderly: A study based on 2014 China longitudinal aging social survey. Popul. Res. 6, 49–61.
Eskildsen, M., and Price, T. (2009). Nursing home care in the USA. Geriatr. Gerontol. Int. 9 (1), 1–6. doi:10.1111/j.1447-0594.2008.00513.x
Hao, Y., Li, Y., Guo, Y., Chai, J., Yang, C., and Wu, H. (2022). Digitalization and electricity consumption: Does internet development contribute to the reduction in electricity intensity in China? Energy Policy 164, 112912. doi:10.1016/j.enpol.2022.112912
Hong, M., Drakeford, B., and Zhang, K. (2020). The impact of mandatory CSR disclosure on green innovation: evidence from China. Green Finance 2 (3), 302–322. doi:10.3934/gf.2020017
Jensen, P. M., Fraser, F., Shankardass, K., Epstein, R., and Khera, J. (2009). Are long-term care residents referred appropriately to hospital emergency departments. Can. Fam. Physician 55 (5), 500–505.
Kivett, V. R. (1985). “Aging in rural society:non-kin community relations and participation,” in The elderly in rural society. Editors R. T. Coward, and G. R. Lee (New York: Springer Publishing Company), 171–191.
Kraus, A. S., Spasoff, R. A., Beattie, E. J., Holden, D. E. W., Lawson, J. S., Rodenburg, M., et al. (1976). Elderly applicants to long-term care institutions. L their characteristics, health problems and state of mind*. J. Am. Geriatrics Soc. 24 (3), 117–125. doi:10.1111/j.1532-5415.1976.tb04282.x
Krout, J. A. (1984). The organizational characteristics of senior centers in America. J. Appl. Gerontol. 3, 192–205. doi:10.1177/073346488400300209
Kumar, P. (2021). Climate change and cities: challenges ahead. Front. Sustain. Cities 3, 645613. doi:10.3389/frsc.2021.645613
Mahmoud, I. H., Morello, E., Ludlow, D., and Salvia, G. (2021). Co-creation pathways to inform shared governance of urban living labs in practice: lessons from three European projects. Front. Sustain. Cities 3, 690458. doi:10.3389/frsc.2021.690458
Morgan, D. G., Semchuk, K. M., Stewart, N. J., and D’Arcy, C. (2002). Rural families caring for a relative with dementia:barriers to use of formal services. Soc. Sci. Med. 7, 1129–1142. doi:10.1016/s0277-9536(01)00255-6
Murphy, A., Lasky-Su, J., Tantisira, K., Litonjua, A., Lange, C., and Weiss, S. (2009). Genome-wide association studies of family data in pharmacogenetics: A case study. Curr. Pharm. Des. 15, 3764–3772. doi:10.2174/138161209789649493
Newcomer, R. J., Ko, M., Kang, T., Harrington, C., Hulett, D., and Bindman, A. B. (2016). Health care expenditures after initiating long-term services and supports in the community versus in a nursing facility. Med. Care 54 (3), 221–228. doi:10.1097/mlr.0000000000000491
Ren, S., Li, L., Han, Y., Hao, Y., and Wu, H. (2022). The emerging driving force of inclusive green growth: Does digital economy agglomeration work? Bus. Strategy Environ. 31 (4), 1656–1678. doi:10.1002/bse.2975
Rosko, M. D., Chilingerian, J. A., Zinn, J. S., and Aaronson, W. E. (1995). The effects of ownership, operating environment, and strategic choices on nursing home efficiency. Med. Care 33 (10), 1001–1021. doi:10.1097/00005650-199510000-00003
Rowles, G. D., Beaulieu, J. E., and Myers, W. W. (1996). Long-term care for the rural elderly: New directions in research, services and policy. New York: Springer Publishing.
Shanas, E., Townsend, P., Wedderburn, D., Henning, F., Milhof, F. P., Stethouwer, J., et al. (1969). Old people in three industrial social. Soc. Serv. Rev. 2, 470.
Shapiro, E., and Tate, R. (1985). Predictors of long term care facility use among the elderly. Can. J. Aging 4 (1), 11–19. doi:10.1017/S0714980800015798
Tennsted, S. L., Mckinlay, J. B., and Sullivan, L. M. (1989). Informal care for frail elders: The role of secondary caregives. Gerontologist 5, 677–683.
van der Jagt, A. P., Kiss, B., Hirose, S., and Takahashi, W. (2021). Nature-based solutions or debacles? The politics of reflexive governance for sustainable and just cities. Front. Sustain. Cities 2, 583833. doi:10.3389/frsc.2020.583833
Wu, H., Ba, N., Ren, S., Xu, L., Chai, J., Irfan, M., et al. (2022). The impact of internet development on the health of Chinese residents: Transmission mechanisms and empirical tests. Socio-Economic Plan. Sci. 81, 101178. doi:10.1016/j.seps.2021.101178
Wu, H., Xue, Y., Hao, Y., and Ren, S. (2021). How does internet development affect energy-saving and emission reduction? Evidence from China. Energy Econ. 103, 105577. doi:10.1016/j.eneco.2021.105577
Xue, Y., Jiang, C., Guo, Y., Liu, J., Wu, H., and Hao, Y. (2022). Corporate social responsibility and high-quality development: Do green innovation, environmental investment and corporate governance matter? Emerg. Mark. Finance Trade 58, 3191–3214. doi:10.1080/1540496x.2022.2034616
Zheng, Y., Chen, S., and Wang, N. (2020). Does financial agglomeration enhance regional green economy development? Evidence from China. Green Finance 2 (2), 173–196. doi:10.3934/gf.2020010
Keywords: elderly services, elderly service supply, socioeconomic status, rural land use, China
Citation: Zhao Y (2022) The factors influencing the supply of rural elderly services in China based on CHARLS data: Evidence from rural land use and management. Front. Environ. Sci. 10:1021522. doi: 10.3389/fenvs.2022.1021522
Received: 17 August 2022; Accepted: 20 September 2022;
Published: 12 October 2022.
Edited by:
Haitao Wu, Beijing Institute of Technology, ChinaReviewed by:
Xiaowei Song, Ocean University of China, ChinaCopyright © 2022 Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan Zhao, emhhb3lhbkBpbW51LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.