 Henrik Olstrup1*
Henrik Olstrup1* Hani A. S. Mohamed2Julie Honoré2Jörg Schullehner2,3
Hani A. S. Mohamed2Julie Honoré2Jörg Schullehner2,3 Torben Sigsgaard2,3Bertil Forsberg1
Torben Sigsgaard2,3Bertil Forsberg1 Anna Oudin1,4
Anna Oudin1,4
- 1Sustainable Health, Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden
- 2Department of Public Health, Aarhus University, Aarhus, Denmark
- 3The Danish Big Data Centre for Environment and Health (BERTHA), Aarhus University, Aarhus, Denmark
- 4Division of Occupational and Environmental Medicine, Department of Laboratory Medicine, Lund University, Lund, Sweden
This systematic literature review investigates the relationship between air pollution exposure and inflammatory bowel disease (IBD), encompassing Crohn's disease (CD) and ulcerative colitis (UC). Despite the growing concern over air pollution's impact on various health outcomes, studies specifically addressing effects on the digestive system, particularly IBD, are relatively rare. This review aims to synthesize the current knowledge on this topic, focusing on the mechanisms underlying these associations and the role of different air pollutants. Following PRISMA guidelines, a systematic literature search of PubMed and Web of Science databases was conducted, yielding 13 epidemiological studies and six mechanistic (toxicological) studies meeting the inclusion criteria. The epidemiological studies examined associations between IBD and various air pollutants, including PM2.5 (particles with an aerodynamic diameter smaller than, or equal to, 2.5 µm), PM10 (particles with an aerodynamic diameter smaller than, or equal to, 10 µm), PM2.5–10 (coarse particles with an aerodynamic diameter in the range of 2.5–10 µm), BC (black carbon), NO2 (nitrogen dioxide), NO (nitrogen monoxide), NOx (nitrogen oxides), N2O (nitrous oxide), CO (carbon monoxide), SO2 (sulfur dioxide), VOC (volatile organic compounds), O3 (ozone), Ox (oxidant capacity), and traffic load. Study methodologies varied among these 13 epidemiological studies, including four cohort studies, two ecological studies, three case-control studies, two studies using two-sample Mendelian randomization, and two longitudinal time-series studies. Eight studies investigated associations with Crohn's disease and ulcerative colitis separately, while five studies analyzed IBD as a whole without distinguishing between CD and UC. Eleven studies found statistically significant associations between air pollution exposure and IBD, although inconsistent results were found in several of these studies. A total number of six mechanistic (toxicological) studies were retrieved. Among these six studies, five were using particulate matter as exposure metric, and one was based on NO2 and O3 as exposure metrics. With a combination of animal, human, and in vitro studies, the results in terms of biological mechanisms indicate that air pollution exposure influences the composition of the gut microbiome, altering metabolic functions within the gut, and creates immunological reactions with inflammation contributing to the development of IBD. Consequently, the results suggest a link between air pollution exposure and both the onset and exacerbation of IBD. However, differences in study design, exposure assessment, and pollutant types make it challenging to draw any firm conclusions. Moreover, the lack of multi-pollutant models in most epidemiological studies makes it difficult to estimate the individual effect of specific air pollutants. This review highlights the need for further research utilizing robust study designs and standardized exposure assessment methods to better understand the impact of air pollution on IBD. By elucidating these associations, policymakers and healthcare professionals can develop effective strategies to mitigate the adverse effects of air pollution on digestive health.
1 Introduction
Exposure to air pollution has, in a wide range of studies, been shown to have detrimental health effects. According to the World Health Organization, ambient (outdoor) air pollution is estimated to have caused around 4.2 million premature deaths worldwide in 2019 (1). Moreover, ambient PM2.5 was the fifth-ranking risk factor of preterm mortality in 2015 (2). In epidemiological studies focusing on health outcomes associated with air pollution exposure, increased mortality has often been used as a metric. Harmful health effects in terms of increased mortality associated with exposure to air pollution have been shown in several studies focusing on both short- and long-term relationships. Long-term mortality effects associated with air pollution have been shown for both NO2 (3–6) particulate matter (7), and O3 (6, 8) although the results for O3 are less clear and consistent. Likewise, associations between short-term exposure to air pollutants and mortality have been shown for NO2 by Wang et al. (9), for O3 by Vicedo-Cabrera et al. (10), and for PM10 and PM2.5 by Orrelano et al. (11). Moreover, cardiovascular and respiratory outcomes as well as cancer can be captured by calculating cause-specific mortality. Associations between air pollution exposure and cardiovascular mortality and respiratory mortality (less clear for respiratory mortality though) have been shown in a systematic review by Hoek et al. (12), and for cancer mortality in a meta-analysis of cohort studies by Kim et al. (13). However, many other health outcomes associated with air pollution exposure are more difficult to capture using mortality as a metric (14).
Neurodegenerative and psychiatric disorders as well as immune-mediated disorders have been shown to be associated with air pollution exposure, but are less well captured by mortality. When considering neurodegenerative disorders, associations between air pollution have been shown for both dementia (15–17), Parkinson's disease (18–21), and multiple sclerosis (22–24). Regarding psychiatric disorder, an association between air pollution exposure and depression has been shown by Borroni et al. (25). Moreover, a potential link between particulate matter and depression, anxiety, and suicide was suggested in a systematic review and meta-analysis by Braithwaite et al. (26).
Other immune-mediated diseases, including autoimmune diseases, have also been shown to be influenced by air pollution exposure (27). Regarding rheumatic diseases, effects from air pollution exposure were demonstrated for both systemic autoimmune rheumatic diseases (SARD) by Celen et al. (28) and Sun et al. (29), and for rheumatic arthritis (RA) by Di et al. (30) and by Essouma and Noubiap (31). Associations between air pollution exposure and RA are also supported by both toxicological, clinical, in vitro and in vivo studies (32–35).
Studies on the effects of air pollution exposure on the digestive system are not as abundant as many of the outcomes mentioned above. Inflammatory bowel disease (IBD) constitutes an umbrella term for some different types of inflammatory conditions in the gut. The two main types of IBD referred to are Crohn's disease (CD) and ulcerative colitis (UC). Both these conditions affect the bowel, but they manifest differently with different mechanisms of emergence (36), and exhibit clear differences in terms of bacterial composition in the gut (37). Ulcerative colitis is an inflammatory disorder of the colonic mucosa, which generally manifests in a continuous manner through part of, or the entire large intestine (38). Crohn's disease (Morbus Crohn) constitutes a relapsing systemic inflammatory disease, which can potentially manifest in parts of the whole gastrointestinal tract, and with extraintestinal manifestations and associated immune disorders (39). The prevalence of IBD has increased worldwide during the last decades (40), and this increase has been particularly marked in the Western world (41, 42), however, newly industrialized countries whose societies have become more westernized also show a sharp increase in the incidence of IBD (43). The burden and costs related to IBD are significant. In Europe during 2020, the direct health care costs associated with IBD per patient and year are estimated to be approximately €3,500 in CD and €2,000 in UC, and with indirect costs of approximately €1,900 per patient yearly related to work productivity loss (44). A total number of 2.5‒3 million people in Europe are estimated to be affected by IBD, with a direct healthcare cost of €4.6‒€5.6 billion Euros per year (45). In the U.S., the total annual health care expenditures for gastrointestinal diseases during the year 2015 were $135.9 billion, of which the costs for IBD were estimated to be $7.2 billion (46).
The associations between environmental factors, including air pollution exposure, and IBD have been addressed in a number of review studies (47–59). Although the mechanisms behind IBD are not fully understood, the current opinion on the mechanisms behind IBD suggests that environmental factors, a dysregulated gut microbiota, and certain genes interact in terms of disease onset (47–49, 52, 54, 56–58, 60–65). A dramatic increase in the incidence of IBD has been observed during the past few decades, suggesting that environmental factors constitute an increasingly critical role in the development of these disorders (48, 57, 66, 67).
When focusing more specifically on the effects of air pollution exposure on IBD, several studies suggest that there is a relationship (47, 48, 53). Plausible mechanisms mediating the effects of air pollution exposure on the gastrointestinal tract could include direct effects on epithelial cells, systemic inflammation and immune activation, and modulation of the intestinal microbiota (48). The gut is exposed to particles in the inhaled air as most of these inhaled particles are removed from the lungs to the gastrointestinal tract via mucociliary clearance (50), alternatively from swallowing of air or from foods coated with airborne particles (68). It has also become evident that there exists a “crosstalk” between the respiratory and gastrointestinal tracts, which is commonly referred to as the gut-lung axis (51). Alterations in the gut microbiota as a result of exposure to NO2 and O3 have been demonstrated on humans by using whole-genome sequence analysis (69). Other than IBD, there are also associations between air pollution exposure and other disorders of the gastrointestinal tract. Associations between air pollution exposure and IBS (irritable bowel syndrome) have been shown (70–72). Short-term air pollution exposure may trigger non-specific abdominal pain in young individuals (73), peptic ulcers (74–76), appendicitis (77–79), and finally, acute effects of air pollution on enteritis were shown by Xu et al. (80).
The goal of this review was to update the current state of knowledge regarding the effects of air pollution exposure on IBD including the intestinal mechanisms that may underlie these associations, and the importance of various kinds of air pollutants.
2 Materials and methods
2.1 Literature search and selection criteria
The elaboration of this systematic review was based on the guidelines presented in PRISMA (Preferred Reporting System for Systematic Reviews and Meta-Analysis) (81–83). The main issue was to find out if exposure to air pollution is associated with an increased risk of inducing and/or exacerbating IBD. A systematic literature search was conducted using PubMed and Web of Science. The search terms “air pollution”, “environmental factors”, “environment” “inflammatory bowel disease”, “IBD”, “exposomes”, “Crohn's disease”, and “ulcerative colitis” were used to identify and select relevant studies. In addition, the reference lists of the retrieved studies were searched to identify additional relevant articles on air pollution as a risk factor for IBD.
Boolean operators were generated based on different search terms related to “IBD” and “air pollution” in “title” and “abstract” with the following main search string:
“((inflammatory bowel disease[Title/Abstract] OR IBD[Title/Abstract] OR crohns disease[Title/Abstract] OR morbus crohn[Title/Abstract] OR ulcerative colitis[Title/Abstract] OR colitis[Title/Abstract]) AND (exposure[Title/Abstract] OR exposome[Title/Abstract] OR environmental factors[Title/Abstract] OR environment[Title/Abstract] OR environmental pollution[Title/Abstract])) AND (air pollution[Title/Abstract] OR nitrogen dioxide[Title/Abstract] OR nitrogen oxide[Title/Abstract] OR carbon monoxide[Title/Abstract] OR sulfur dioxide[Title/Abstract] OR volatile organic compounds[Title/Abstract] OR particulate matter[Title/Abstract] OR black carbon[Title/Abstract] OR elemental carbon[Title/Abstract] OR ozone[Title/Abstract])”.
Two researchers (H.A.S.M. and H.O.) independently screened the studies generated with this search string for potential relevance for further analysis. In a first step, each record's title and abstract underwent a screening process. If the reviewers disagreed during this initial stage, the study went on to a full-text screening phase. During the full-text screening, only those studies that passed the initial review were evaluated in detail.
The following inclusion criteria:
1. Epidemiological studies using prospective and retrospective cohort study designs, longitudinal study designs, case-control and nested case-control study designs, and ecological study designs;
2. Apart from epidemiological studies, other relevant studies including toxicological, clinical, in vitro and in vivo studies analyzing the relationships between air pollution and IBD, and the potential underlying mechanisms behind these relationships;
3. Studies assessing the impact of ambient air pollution on any of the different population groups;
4. A description of the method for assigning exposure had to be present;
5. Studies on associations between short- and long-term exposure to outdoor air pollution and incidence of IBD (Crohn's disease and ulcerative colitis separately or altogether);
6. Providing information on population characteristics;
7. Epidemiological studies reporting the effect estimates in terms of relative risks (RR), odds ratios (OR), incidence rate ratios (IRR), or hazard ratios (HR) with 95% confidence intervals (CI);
8. Studies written in English language.
The following exclusion criteria:
1. Review studies, meta-analyses, and other studies not reporting original research results;
2. Studies investigating the associations between IBD and pollutants other than ambient air like smoking (both passive and active) and pollutants originating indoors;
3. Health outcome was ascertained by self-diagnosis;
4. Not peer reviewed studies like conference abstracts, theses, and preprints;
5. Studies written in other than English language.
2.2 Selected studies and synthesis
All epidemiological studies selected based on the above mentioned criteria were further evaluated based on their quality. The factors that were used to evaluate the quality consist of exposure assessment, magnitude of effect, consistency of results, adjustments of confounders, and the study design. A quality score from 1 to 4 was used in order to create an average value based on these factors. The few toxicological studies that were selected were not evaluated in the same way as the epidemiological studies, but rather presented to clarify the biological mechanisms behind air pollution exposure and IBD.
Although the focus of this literature review is on air pollution exposure and IBD, other environmental factors as well as genetic factors have been addressed in the Discussion section. The reason for that is to also have a certain focus on the complex interplay between several environmental factors and genes where air pollution is one of many important factors regarding the onset and exacerbation of IBD.
3 Results
3.1 Literature search procedure
This literature search was conducted according to a complete “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA) checklist (83). “Title” and “abstract” were screened using different search terms related to “IBD” and “air pollution”. The search procedure is presented in Figure 1.
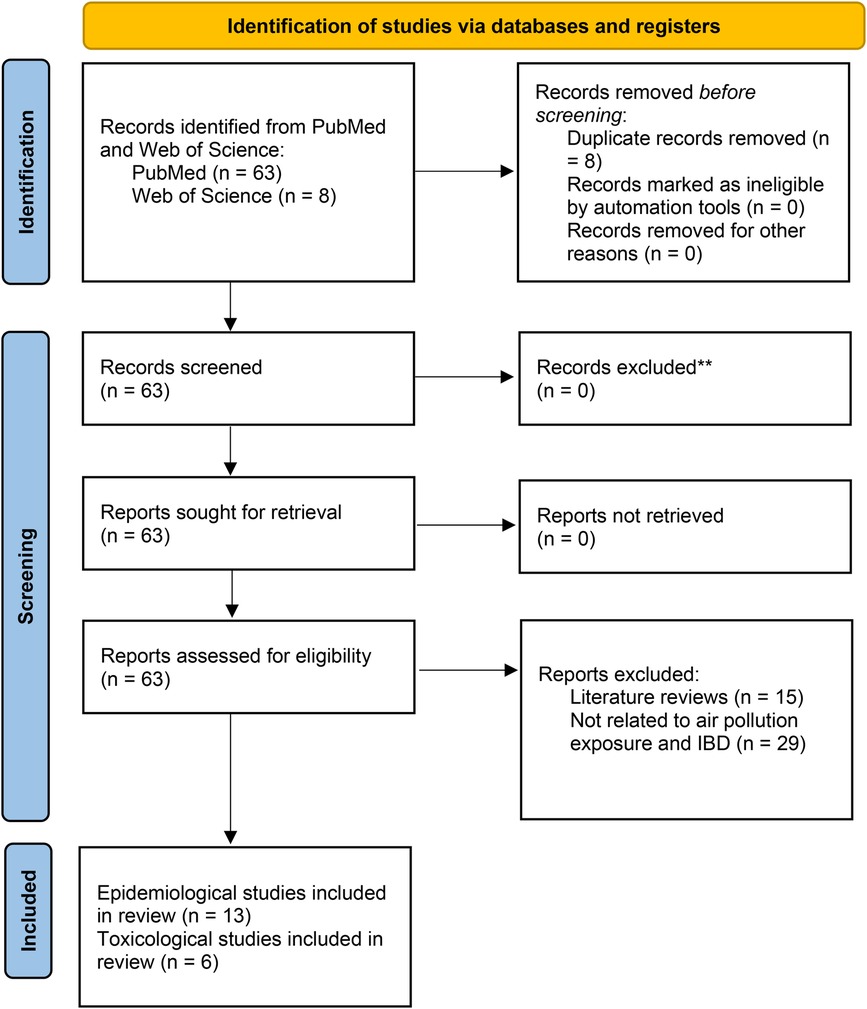
Figure 1. The search and selection procedure performed in PubMed and Web of Science.
3.2 Summary of studies retrieved from PubMed and web of science divided into epidemiological studies and toxicological (mechanistic) studies
Table 1 summarizes the epidemiological studies selected for this systematic literature review, and Table 2 presents the corresponding toxicological studies. In order to make a fair synthesis of the epidemiological studies, the quality of evidence for a potential causal link between air pollution exposure and IBD was evaluated based on a number of factors (101) (see Table A2 in Appendix A). A quality score from 1‒4, presented in Table A1 (Appendix A), was used in order to create an average value based on the factors presented in Table A2. Factors that increase the score include consistent results, a large magnitude of the effect, and detailed adjustments of confounders. Factors lowering the grade include limitations in study design or execution (risk of bias) and inconsistency of results. The evaluation from very low (1) to high (4), with a description of the assessment criteria, is presented in a Table A1, Appendix A.
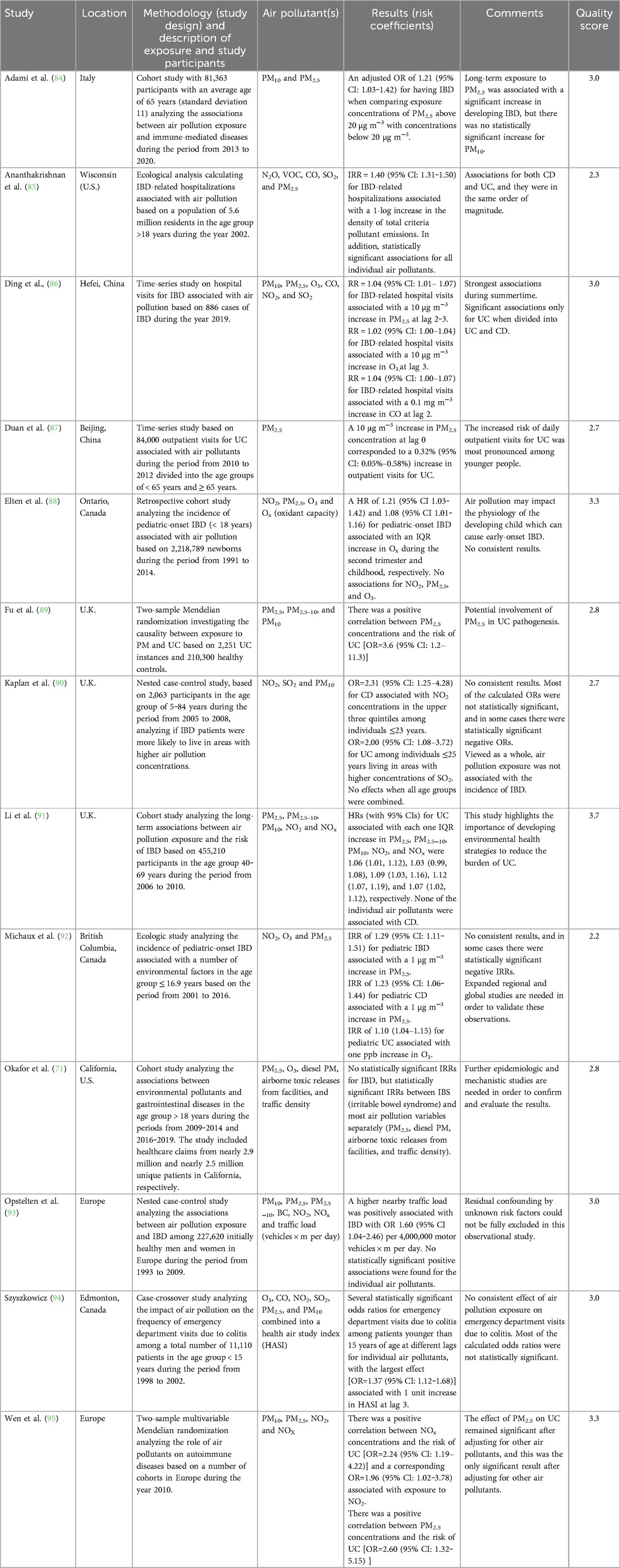
Table 1. Summary of epidemiological studies analyzing the associations between air pollution exposure and IBD.
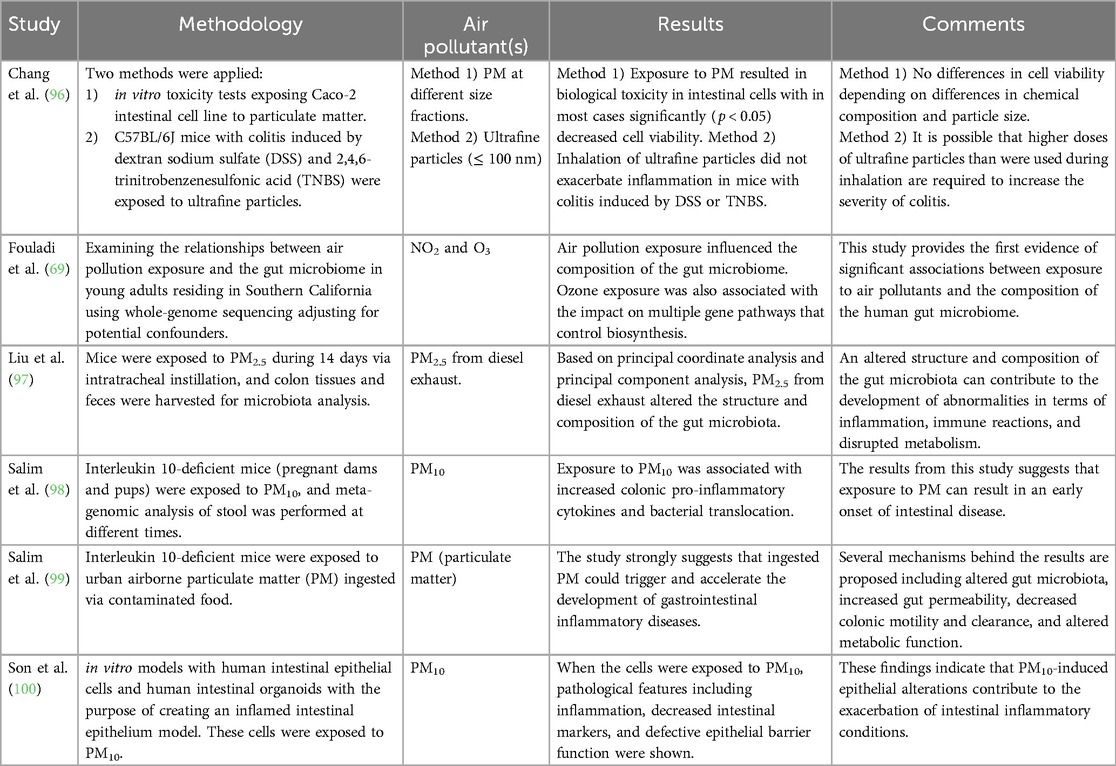
Table 2. Summary of the toxicological studies analyzing the biological mechanisms behind air pollution exposure and the intestinal physiology including IBD.
3.3 Interpretation of the results
Based on both the epidemiological and the toxicological studies, the findings from this systematic literature review suggest that air pollution exposure could influence the onset and worsening of IBD. The quality score of the epidemiological studies in the range of 2.2–3.7 indicates a relatively high quality level of the included studies. However, variations in study design across the included epidemiological studies pose challenges in drawing definitive conclusions. Despite this, the analysis reveals both short- and long-term impacts on IBD associated with various air pollutants, affecting both Crohn's disease and ulcerative colitis, and plausible biological mechanisms are supported by the toxicological studies. However, the lack of multi-pollutant models in most of the epidemiological studies makes it difficult to distinguish the individual effect of specific air pollutants.
4 Discussion
4.1 The link between environmental factors and IBD
4.1.1 Air pollution and IBD based on study design and pollutants
This comprehensive literature review encompassed 13 epidemiological studies, each examining distinct air pollutants in relation to IBD. Among these, PM2.5 was the focus of twelve studies, followed by NO2 in eight studies, and PM10 in eight studies, among others. Eight studies investigated associations with Crohn's disease and ulcerative colitis separately, while five studies analyzed IBD as a whole without distinguishing between CD and UC. Study methodologies varied, including four cohort studies, two ecological studies, three case-control studies, two studies using two-sample Mendelian randomization, and two longitudinal time-series studies. Despite methodological differences, a number of consistent associations between air pollution exposure and IBD were observed. For example, one cohort study linked IBD to PM2.5 exposure (84), while another associated ulcerative colitis with exposure to multiple pollutants such as PM10, PM2.5, PM2.5–10, NO2, and NOx (91). Ecological studies also identified associations between PM2.5 and a combination of pollutants including N2O, NO2, VOC, CO, SO2, O3, and PM2.5 (85, 92). The six toxicological studies (69, 96–100) do not have as much variation in terms of air pollutants; five studies have focused on particles (96–100), and one study is based on NO2 and O3 (69). However, with a combination of animal, human, and in vitro studies, the results in terms of biological mechanisms indicate that air pollution exposure influences the composition of the gut microbiome, altering metabolic functions within the gut, and creates immunological reactions with inflammation contributing to the development of IBD.
4.1.2 Genes, air pollutants, and other environmental factors affecting IBD
During the past few decades, the incidence and prevalence of IBD has increased rapidly in the industrialized countries (41, 102–106), which cannot be explained through genetic mechanisms (103, 107–110). This increase in IBD has been particularly noticeable in many developing countries where IBD has previously been relatively uncommon (111). Additionally, when immigrants from countries with little occurrence of IBD move to countries with a higher occurrence, the risk of developing IBD levels with the country they have moved to rather than the country they have moved from (112–115). However, a complex interplay between epigenetic mechanisms in terms of DNA methylation, histone modification, and alterations in the expressions of microRNAs could explain the link between genetic and environmental factors regarding the onset of IBD (54). Nevertheless, certain genes are involved in the pathogenesis of IBD, with more than 200 risk genes being identified (116, 117). Possible genetic mechanisms involve dysregulation of innate immune response to the microbiome, increased permeability across the intestinal mucosa, and dysregulation of the adaptive immune system (118–120). However, these risk genes explain less than 30% of the susceptibility to the development of IBD, suggesting environmental factors as the key in the pathogenesis of IBD (117, 121), and where a large proportion of the cases of IBD may be preventable through lifestyle modifications (122, 123).
The impact of environmental factors on IBD are reflected by geographical variations, with a higher incidence of IBD among people living in urban environments compared to those living in rural environments (124–126), as well as a higher incidence of IBD among those living in densely populated areas (127). Living in green and blue spaces as well as in natural environments may also constitute protective factors regarding the development of IBD (128). However, a higher incidence of IBD in rural agricultural areas has been shown for northern France by Declercq et al. (129). Urbanization including changes in diet, use of antibiotics, hygiene status, microbial exposures, and pollution have all been suggested as potential environmental risk factors for IBD (130). In addition to air pollution, water pollution has been shown to have some impact on the development of IBD, with increased risks associated with drinking water containing certain metals and disinfectants (131).
The use of some pharmaceuticals, most commonly used in the industrialized world, may have an impact on the IBD incidence. Non-steroidal anti-inflammatory drugs (NSAIDs) have, despite their anti-inflammatory effects, been shown to be able to contribute to the exacerbation of IBD (132), and effects in terms of gastrointestinal toxicity (dyspepsia, gastroduodenal ulcers, and gastrointestinal bleeding and perforation) have been shown in association with the use of NSAIDs (133). An increased risk of developing IBD associated with antibiotic consumption has also been shown (134), with the highest risk increase linked to the antibiotics affecting the gut microbiota (135). Moreover, exposure to oral contraceptives has been shown to increase the risk of developing IBD (136, 137), where estrogen can potentially affect the gut microbiota, the intestinal wall barrier function, and possibly cause micro-ischaemia within the vasculature of the gut (138).
When considering dietary intake and the risk of IBD, there is a general pattern with a decreased risk associated with high fruit, vegetable, fiber, and omega-3 fatty acid intake, and an increased risk associated with total fat, animal fat, polyunsaturated fatty acid, omega-6 fatty acid, and refined sugar intake (139–145). Vitamin D has also been shown to constitute an important risk factor, with higher plasma concentrations of vitamin D linked to a reduced risk of developing IBD (146). High prevalence of vitamin D deficiency among people with IBD has also been shown, with some evidence of a latitude-dependent effect, and with higher incidence at northern latitudes, possibly reflecting the role of sun exposure (147, 148).
Stress and high mental load are also well-known risk factors for the development and exacerbation of IBD (149–153). More specifically, stress is defined as an acute threat to the body's homeostasis, which can give rise to a number of physiological changes in the intestine including changes in gastrointestinal secretion, increased intestinal permeability, decreased mucosal blood flow, and negative effects on the microbiota, of which all affect the risk of IBD (152–154).
When considering IBD incidence and educational level, the associations point in different directions. A Swedish study by Li et al. (155) found a decreased risk of IBD-related hospitalizations among higher educated groups, while a Norwegian study by Aamodt et al. (124) found a higher incidence rate of IBD in the municipalities with the highest level of education when compared to the municipalities with the lowest level of education. When comparing IBD diagnoses between men and women based on two cohorts, there were some differences in the age of onset and disease location, but there were no large sex-related differences regarding therapeutic management or IBD-specific healthcare costs (156).
When considering air pollution exposure and IBD, it is only one of many interacting environmental factors mentioned above that can influence the onset and exacerbation of IBD. Despite air pollution being an important risk factor in the development and pathogenesis of IBD, its interaction with other environmental factors also needs to be addressed in terms of their impact and how the burden of IBD can be reduced.
4.1.3 The biological mechanisms behind air pollution exposure and induction or exacerbation of IBD
According to the toxicological studies presented in Table 2, it was found that exposure to air pollution affected both the gut microbiota and the metabolic processes in the intestine. However, the mechanisms of how air pollution exposure affect the intestinal physiology and pathology are not fully understood. Nevertheless, there are several potential mechanisms of how air pollution exerts its effects on IBD. In general, air pollution and its components can alter the host's mucosal defenses and trigger immune responses (47). Inhaled air pollutants reach the gut via mucociliary clearance from the lungs. Potential mechanisms of how air pollution exposure affects the gut physiology include direct effects on epithelial cells, systemic inflammation and immune activation, and modulation of the intestinal microbiome (48). An increased thrombotic tendency and imbalances in prostaglandin synthesis have also been proposed as possible mechanisms (55). Impact on the intestinal microbiome associated with air pollution exposure has been suggested as a very conceivable mechanism. The lipid metabolism within the intestine is controlled by the gut microbiota, and intestinal redox lipids might be important in terms of both systemic and intestinal inflammation (50). A crosstalk between the respiratory and gastrointestinal tracts occurs via the bloodstream and the lymphatic system, commonly referred to as the gut-lung axis, where these two organs communicate via microbial secretions, metabolites, immune mediators, and lipid profiles (51).
In comparison with healthy individuals, a less diverse microbiome and imbalances between different bacterial strains has been shown in those diagnosed with IBD (157), and different epigenetic profiles between inflamed and non-inflamed colonic segments have also been shown (158). Accordingly, an association between air pollution exposure and changes in the composition of the gut microbiota has been shown in several studies, although the pattern is not completely clear, and the mechanisms behind it are not fully understood (59, 159). Alterations in the gut microbiome as a result of exposure to air pollution have been shown for particulate matter in both epidemiological and experimental studies (97–100, 160–165), for NOx and O3 in one experimental study by Fouladi et al. (69), and for traffic-related air pollution (NOx) in one epidemiological study by Alderete et al. (166). Alterations and dysfunctions of the microbiome have been shown among people with IBD, and this in turn results in shifts in oxidative stress pathways with decreased carbohydrate metabolism and amino acid biosynthesis during tissue damage (167).
Although the etiology of IBD is multifactorial, involving both environmental, genetic, epigenetic, and immunological factors, oxidative stress constitutes an inherent part of any one of them. Air pollution entering the gastrointestinal tract can have a direct effect on the intestinal epithelium by oxidizing intestinal lipids (50). Consequently, redox equilibrium is crucial in order to maintain cell homeostasis within the gastrointestinal tract (168, 169), and increased levels of reactive oxygen species in combination with decreased levels of antioxidants contribute to the disease pathogenesis of IBD (170). Oxidative stress causes damages to the mucosal layer of the gastrointestinal tract with subsequent bacterial invasion, which in turn causes immune responses and initiates IBD (169). Particulate matter has been shown to induce oxidative stress in human cells, with subsequent chronic inflammation (171). Exposure to PM2.5 has also been shown to increase the concentrations of oxidized low density lipoproteins, as shown in a clinical study in China by Qin et al. (172). Consequently, and with respect to the close relationship between the gut microbiota and lipid metabolism, air pollution exposure can cause an increase in oxidized lipids with subsequent pathological systemic effects (50).
Changes in the intestinal barrier function have been associated with IBD (173). Exposures to particulate matter and ozone have been shown to change the intestinal permeability by breaking the intercellular barriers (68, 99, 174). The intestinal mucosal barrier maintains a delicate balance between absorbing important and essential nutrients, but also has the function of preventing the influx of harmful substances and form a defense against them. IBD is incidentally associated with disruptions of essential elements of the intestinal barrier, which creates dysfunctions of gut permeability (175).
To sum up, the mechanisms behind air pollution exposure and the onset or exacerbation of IBD are very complex, and all details are not fully understood. The mechanisms constitute a combination of several interrelated and interacting factors where microbial composition, oxidative stress, lipid metabolism, and gut permeability play significant roles (Figure 2). Altered composition and decreased diversity of bacterial species can cause changes in the gut metabolism with changes in fatty acid production, and with the creation of toxic and inflammatory substances. Increased oxidative stress can be caused by air pollution exposure itself, or secondarily to that followed by altered metabolism caused by changes in the composition of the gut microbiota. Increased production of radicals and oxidative stress can cause increased gut permeability, which in turn promotes the influx of toxic substances with inflammatory responses from macrophages and the release of cytokines (99).
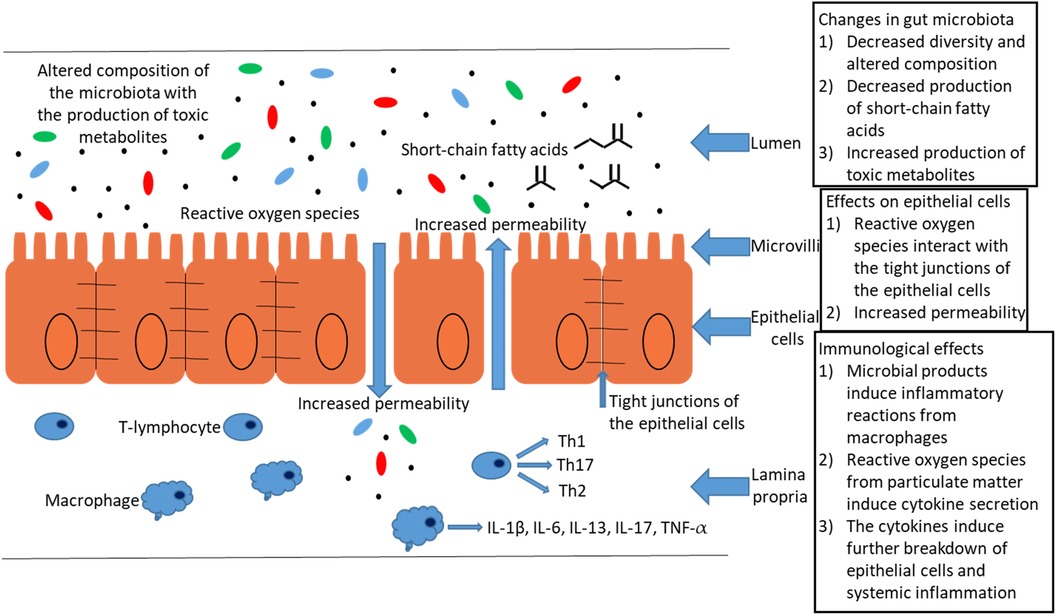
Figure 2. An illustration describing the biological mechanisms behind exposure to particulate matter and the accompanying pathophysiological mechanisms of the gut [adapted from Salim et al. (99)]. The development of IBD as a result of exposure to particulate matter is caused by several factors: (1) Changes in the composition of the microbiome, with a decrease in beneficial short-chained fatty acids and an increase in toxic metabolites, when particles are metabolized by the gut microbiota. (2) Reactive oxygen species interact with the tight junctions of the epithelial cells resulting in increased permeability and leaky gut syndrome. (3) Immunological effects in terms of production of pro-inflammatory cytokines with further breakdown of epithelial cells and systemic inflammation.
4.1.4 The effects of smoking on IBD in relation to the effects of ambient air pollution
Although there are clear indications that outdoor air pollution is associated with the induction and exacerbation of both CD and UC, the impact of tobacco smoke on IBD is complex. Smoking may be able to impact the pathogenesis of IBD through several direct and indirect effects including oxidative stress, impairment of intestinal barrier and immune cell function, epigenetic changes, and dysregulation of the microbiota (176). In general, smoking is unfavorable for CD, but beneficial for UC (108, 177–181). Current smoking is associated with an increased risk of CD, but former smoking is associated with an increased risk of UC (182, 183). Current smoking is furthermore protective against the development of UC (183). However, passive smoking during childhood has not been shown to increase the risk of developing either CD or UC in adulthood (184).
The role of smoking in the pathogenesis of IBD is complex. Nicotine is considered to play an important role. Tobacco smoke modulates nicotinic acetylcholine receptors by activating a cholinergic anti-inflammatory pathway among smokers who have UC. Contrarily, with regard to CD, nicotine can exacerbate the condition as nicotine will increase the inflammatory response of macrophages infected with certain types of bacteria, and with a reduced cellular apoptosis in macrophages exposed to nicotine (185).
The potential role of carbon monoxide exposure as beneficial on the pathogenesis of IBD could also explain the positive effect of smoking on UC. Carbon monoxide (CO) is produced as a result of incomplete combustion of tobacco, and smokers usually have a significant proportion of carbon monoxide bound to the hemoglobin (186). Apart from being inhaled from tobacco smoke, CO is endogenously and physiologically produced in cells during the degradation of heme (a ring-shaped iron-containing component of hemoglobin) under the influence of the enzyme heme oxygenase (187, 188). Heme oxygenase is generated by the enteric microbiota, and the pathway involving heme oxygenase and CO can affect the balance between pro-inflammatory and anti-inflammatory cytokine expressions. The heme oxygenase and CO-pathway also includes antimicrobial effects regulating the intestinal immune homeostasis (189). The action of CO involves the activating of heme-containing proteins resulting in the promotion of autophagy, a decreased generation of reactive oxygen species, and the promotion of adaptive responses and cell survival (190). Besides, tangible therapeutic effects of CO on both inflammation and arthritis have been shown by Takagi et al. (191). In summary, CO has the potential to exert anti-inflammatory and tissue-protective effects (190).
Regarding IBD and ambient air pollution exposure, no protective effects have been demonstrated in the epidemiological studies reviewed. Unlike tobacco smoke, outdoor air pollution does not contain nicotine, and CO is emitted along with a variety of other air pollutants, which makes it unlikely that CO in ambient air could exert any notable anti-inflammatory effects.
4.1.5 Environmental factors including air pollution and pediatric IBD
The effects of air pollution on pediatric IBD need to be addressed separately. The incidence of IBD is rising worldwide, with a particularly prominent increase among children (53, 192–199). Even though the incidence of IBD varies around the world, there is an increasing trend of pediatric IBD (particularly evident for CD) in both developed and developing countries (194). However, Northern Europe and North America have the highest incidence and prevalence of pediatric-onset IBD, while Southern Europe, Asia, and the Middle East have the lowest incidence and prevalence (200). Despite an increasing trend of pediatric IBD in developed countries, the corresponding trend for adult IBD in developed countries seems to have stabilized in recent times according to some studies (105). However, the genetic risk factors associated with pediatric IBD are largely similar to those associated with adult-onset IBD (201). Nevertheless, childhood-onset IBD might be etiologically different from adult-onset IBD. When comparing the phenotypic characteristics between those two, childhood-onset IBD was shown to be characterized by more extensive intestinal involvement and rapid early progression in comparison with adult-onset IBD (202). When comparing the vulnerability to environmental pollutants among children and adults, several factors are important to take into account: their relatively much smaller body volume, the way they interact with the environment, and their dynamic developmental physiology are decisive in terms of differences in susceptibility between adults and children (203). Moreover, the fetal gut is generally thought to be sterile, but starts to develop during the neonatal period during the influence of early-life exposures (204). Since the initial colonization of the gut microbiome is determined early in life, early-life environmental exposures can cause various pathological changes (193). Observational studies have also shown that there are associations between the living conditions during childhood and the risk of developing IBD later in life (205).
Apart from an increased risk for a child to develop IBD later in life if the mother was diagnosed with IBD, or having different types of illnesses during the first year of life (206, 207), or being hospitalized for gastrointestinal infections during childhood (208), the importance of several environmental factors regarding pediatric IBD is confirmed through several studies (193). The use of antibiotics in early age is a well-known risk factor developing IBD (209–212). An increased risk of pediatric IBD has also been shown in association with the use of antibiotics during pregnancy (213). The “hygiene hypothesis” means that growing up in cleaner environments can alter the balance of the immune system, with an increased risk of developing immunological conditions including IBD. The “hygiene hypothesis” is based on the assumption that exposure to harmless microorganisms decreases the risk of developing immune-mediated diseases, possibly leading to less induction of dendritic cell maturation and the regulation of T lymphocytes (58). The impact of exposure to microorganisms is supported by the fact the H. pylori infection in early childhood has been shown to decrease the risk of developing IBD (214). Additionally, the impact of childhood hygiene on the risk of developing IBD is supported by studies on several markers of hygiene, with an increased risk associated with fewer family members (215, 216), an increased risk of CD associated with living in households with hot-water tap and separate bathrooms (217), and a decreased risk of IBD associated with growing up with pets and having contact with farm animals (215, 218–220). However, the use of agricultural pesticides has been shown to increase the risk of developing pediatric IBD (92).
Other identified risk factors for pediatric IBD include low fruit intake, low physical activity, birth by caesarean section, exposure to antibiotics, appendectomy, age above 10 years, and frequent gastroenteritis admissions according to a multicenter case-control study in Saudi Arabia (221). Moreover, gluten introduction in early age (222), as well as high sugar intake and stressful life events (208) have been shown to increase the risk of developing pediatric IBD. Finally, when comparing the incidence and phenotypic expression of IBD in the South Asian pediatric population with the domestic pediatric population, a significantly higher incidence and different phenotypic expression was shown in Canada by Pinsk et al. (223), and in New Zealand by Rajasekaran et al. (224), suggesting potential effects of migration, environment, and lifestyle factors.
In contrast to risk factors, there are also a number of identified factors that are protective regarding the development of pediatric IBD. Based on studies performed in Canada, protective factors regarding the development of IBD with respect to childhood exposure include living in rural households (225). A decreased risk of developing CD among children living in relatively more deprived areas has been shown in Scotland (192). Breastfeeding is another protective factor regarding the development of both pediatric-onset and adult-onset IBD, as shown by systematic reviews (226–228), possibly reflecting the role of breast milk on the process of colonization of the gut microbiota and pathological imprinting early in life (229). Vitamin D supplementation may also have a beneficial effect on pediatric IBD, with significantly decreased markers of inflammation, which was shown when two groups of children with IBD were compared, one of which received vitamin D supplementation (230). Moreover, appendectomy has been shown to reduce the risk of developing UC according to a meta-analysis by Koutroubakis et al. (231). Finally, when measuring exposure to residential greenspace among children using a normalized difference vegetation index, an increase in residential greenspace during childhood was associated with a decreased risk of developing pediatric-onset IBD (232).
When addressing the relationship between air pollution exposure and pediatric IBD, it is important to consider the dynamic developmental physiology of a child. In general, exposure to air pollutants during fetal development and early postnatal life is associated with a number of negative health effects including abnormal development, decreased lung growth, increasing rates of respiratory tract infections, childhood asthma, behavioral problems, and neurocognitive decrements (233). Among the epidemiological studies included in this literature review, presented in Table 1, three studies have focused on pediatric IBD. In the retrospective cohort study by Elten et al. (88), analyzing the incidence of pediatric-onset IBD associated with maternal and early-life exposure to NO2, PM2.5, O3 and Ox (oxidant capacity), statistically significant associations were found only for Ox, indicating that oxidative stress plays an important role in the disease onset. Ozone constitutes a powerful oxidizing agent where the effects resulting from exposure may differ between children and adults due to differences in antioxidant defense responses and vulnerabilities to cellular injury. It is also possible that exposure to O3 during the postnatal period may constitute a priming event that increases the toxicity of other pollutants or allergens, as proposed by a study focusing on O3 and the development of asthma during the postnatal period (234).
When considering air pollution in rural and urban environments, and the potential differences in terms of being a risk factor for IBD, it is important to take into account differences in the composition of air pollutants in rural and urban environments. A higher incidence of IBD in urban environments compared to rural environments has been shown for both children and the general population (124, 126, 225). Apart from the hygiene hypothesis previously described, differences in the composition of air pollutants could also be a contributing factor. Air pollutants in the urban environment are in general dominated by emissions originating from traffic, while agriculture, and in some cases industries, are in general more significant sources in the rural environment (235). Additionally, airborne particles can contain a variety of bacterial strains depending on its source (236), and certain bacterial strains including phylum Firmitus and Proteobacteria phylum have been shown to be decreased and increased, respectively, among IBD patients (237). Both phylum Firmitus and Proteobacteria phylum are present in aerosols near cows at dairy farms (238), and similar to the hygiene hypothesis, exposure to different bacterial contents in particles, with respect to urban and rural conditions, could also have some impact on the development of IBD.
To sum up, air pollution probably acts synergistically together with a number of other environmental factors mentioned above when it comes to the onset and exacerbation of pediatric IBD. According to Elten et al. (88), the oxidant capacity (the redox-weighted oxidant capacity based on both O3 and NO2) has been shown to be important when it comes to the onset of pediatric IBD. That is in line with the study suggesting O3 as especially important regarding asthma during the postnatal development (234). Besides oxidant capacity as a potentially important factor regarding pediatric-onset IBD, the dynamic developmental physiology of a child needs to be considered when air pollution and IBD is addressed in terms of prevention measures.
4.2 Opportunities to alleviate IBD associated with air pollutants
This review underscores the imperative for further research employing robust study designs and standardized exposure assessment methods to deepen our understanding of the impact of air pollution on IBD. By elucidating these associations, policymakers and healthcare professionals can develop effective strategies to mitigate the adverse effects of air pollution on the digestive health. However, the multifactorial nature of IBD, with several environmental factors acting together in its development, necessitates exploring various approaches to mitigate and limit the disease.
On an individual level, mitigating the effects of air pollution exposure on IBD and digestive health can be challenging. However, strengthening mucosal and epithelial barriers can help mitigate air pollution-induced systemic inflammation and oxidative stress. Probiotics and prebiotics, collectively known as synbiotics, are well-known gut health stimulators that optimize the composition of the gut microbiome and microbial metabolites (51). Additionally, natural antioxidants have shown effectiveness in relieving IBD by combating oxidative stress, as indicated by research conducted by Sahoo et al. (170). Furthermore, maintaining adequate plasma concentrations of vitamin D has been demonstrated to have a protective effect against the development of IBD (146).
These interventions offer promising avenues for both individual and population-level strategies to mitigate the impact of air pollution on IBD and promote digestive health.
4.3 Policy implications and future research needs
The presence of IBD entails both great costs for society and personal suffering for those affected. The societal costs attributed to IBD can be divided into several factors including healthcare, sick leave, disability pension, and medications (239). The costs related to IBD are also increasing in high-income settings (240), and based on the total costs related to gastrointestinal diseases in U.S., IBD is estimated to make up roughly five percent of this total cost (46). Therefore, identifying and mitigating environmental risk factors are of significant importance to reduce unnecessary suffering and alleviate the burden on healthcare systems. Reallocation of resources can enhance the care provided to individuals living with IBD.
Moreover, when considering air pollution as a risk factor for the onset or exacerbation of IBD, the societal costs attributed to air pollution would likely be underestimated, as IBD is not usually included in terms of costs associated with air pollution. Thus, there is an urgent need for expanded research efforts, employing robust study designs and standardized exposure assessment techniques, to deepen our understanding of the intricate relationship between air pollution and IBD. By uncovering these associations, policymakers and healthcare practitioners can develop targeted interventions to reduce exposure to specific pollutants, raise public awareness about the risks associated with air pollution, and integrate pollution control measures into broader public health initiatives. Additionally, further research can inform the development of tailored interventions and treatments to mitigate the worsening of IBD symptoms in individuals exposed to air pollution. Ultimately, a multifaceted approach that integrates scientific findings with policy and practice is essential to safeguarding digestive health in the face of environmental challenges posed by air pollution.
5 Conclusions
An overall conclusion of this systematic literature review is that there is a link between air pollution exposure and the onset and exacerbation of IBD, and where air pollution exposure constitutes one of many environmental factors which probably act synergistically in the development of IBD. The mechanisms behind air pollution exposure and the onset or exacerbation of IBD are very complex, and all details are not fully understood. These mechanisms constitute a combination of several interrelated and interacting factors where microbial composition, oxidative stress, lipid metabolism, and gut permeability play significant roles. Due to the lack of multi-pollutant models in the epidemiological studies included in this literature review, the role of specific air pollutants is difficult to determine. Thus, there is an urgent need for expanded research efforts, employing robust study designs and standardized exposure assessment techniques, to deepen our understanding of the intricate relationship between air pollution exposure and IBD.
Author contributions
HO: Conceptualization, Data curation, Formal Analysis, Writing – original draft. HM: Conceptualization, Data curation, Writing – review & editing. JH: Writing – review & editing. JS: Writing – review & editing. TS: Writing – review & editing. BF: Writing – review & editing. AO: Conceptualization, Formal Analysis, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Funded by the European Union (Horizon Europe project MARCHES: Methodologies for Assessing the Real Costs to Health of Environmental Stressors, grant no. 101095430). Views and opinions expressed are however those of the authors only and do not necessarily reflect those of the European Union. Neither the European Union nor the granting authority can be held responsible for them.
Acknowledgments
Great thanks to Joy Sandberg, librarian at the Medical Library at Umeå University, for the help in finding relevant literature through appropriate search paths.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the global burden of diseases study 2015. Lancet. (2017) 389(10082):1907–18. doi: 10.1016/S0140-6736(17)30505-6
3. Huang S, Li H, Wang M, Qian Y, Steenland K, Caudle WM, et al. Long-term exposure to nitrogen dioxide and mortality: a systematic review and meta-analysis. Sci Total Environ. (2021) 776:145968. doi: 10.1016/j.scitotenv.2021.145968
4. Atkinson RW, Butland BK, Anderson HR, Maynard RL. Long-term concentrations of nitrogen dioxide and mortality: a meta-analysis of cohort studies. Epidemiology. (2018) 29(4):460–72. doi: 10.1097/EDE.0000000000000847
5. Stieb DM, Berjawi R, Emode M, Zheng C, Salama D, Hocking R, et al. Systematic review and meta-analysis of cohort studies of long term outdoor nitrogen dioxide exposure and mortality. PLoS One. (2021) 16(2):e0246451. doi: 10.1371/journal.pone.0246451
6. Huangfu P, Atkinson R. Long-term exposure to NO(2) and O(3) and all-cause and respiratory mortality: a systematic review and meta-analysis. Environ Int. (2020) 144:105998. doi: 10.1016/j.envint.2020.105998
7. Chen J, Hoek G. Long-term exposure to PM and all-cause and cause-specific mortality: a systematic review and meta-analysis. Environ Int. (2020) 143:105974. doi: 10.1016/j.envint.2020.105974
8. Atkinson RW, Butland BK, Dimitroulopoulou C, Heal MR, Stedman JR, Carslaw N, et al. Long-term exposure to ambient ozone and mortality: a quantitative systematic review and meta-analysis of evidence from cohort studies. BMJ Open. (2016) 6(2):e009493. doi: 10.1136/bmjopen-2015-009493
9. Wang M, Li H, Huang S, Qian Y, Steenland K, Xie Y, et al. Short-term exposure to nitrogen dioxide and mortality: a systematic review and meta-analysis. Environ Res. (2021) 202:111766. doi: 10.1016/j.envres.2021.111766
10. Vicedo-Cabrera AM, Sera F, Liu C, Armstrong B, Milojevic A, Guo Y, et al. Short term association between ozone and mortality: global two stage time series study in 406 locations in 20 countries. Br Med J. (2020) 368:m108. doi: 10.1136/bmj.m108
11. Orellano P, Reynoso J, Quaranta N, Bardach A, Ciapponi A. Short-term exposure to particulate matter (PM(10) and PM(2.5)), nitrogen dioxide (NO(2)), and ozone (O(3)) and all-cause and cause-specific mortality: systematic review and meta-analysis. Environ Int. (2020) 142:105876. doi: 10.1016/j.envint.2020.105876
12. Hoek G, Krishnan RM, Beelen R, Peters A, Ostro B, Brunekreef B, et al. Long-term air pollution exposure and cardio- respiratory mortality: a review. Environ Health. (2013) 12(1):43. doi: 10.1186/1476-069X-12-43
13. Kim HB, Shim JY, Park B, Lee YJ. Long-term exposure to air pollutants and cancer mortality: a meta-analysis of cohort studies. Int J Environ Res Public Health. (2018) 15(11):2608. doi: 10.3390/ijerph15112608
14. Sigsgaard T, Hoffmann B. Assessing the health burden from air pollution. Science. (2024) 384(6691):33–4. doi: 10.1126/science.abo3801
15. Abolhasani E, Hachinski V, Ghazaleh N, Azarpazhooh MR, Mokhber N, Martin J. Air pollution and incidence of dementia: a systematic review and meta-analysis. Neurology. (2023) 100(2):e242–e54. doi: 10.1212/WNL.0000000000201419
16. Tang J, Chen A, He F, Shipley M, Nevill A, Coe H, et al. Association of air pollution with dementia: a systematic review with meta-analysis including new cohort data from China. Environ Res. (2023) 223:115048. doi: 10.1016/j.envres.2022.115048
17. Wilker EH, Osman M, Weisskopf MG. Ambient air pollution and clinical dementia: systematic review and meta-analysis. Br Med J. (2023) 381:e071620. doi: 10.1136/bmj-2022-071620
18. Han C, Lu Y, Cheng H, Wang C, Chan P. The impact of long-term exposure to ambient air pollution and second-hand smoke on the onset of Parkinson disease: a review and meta-analysis. Public Health. (2020) 179:100–10. doi: 10.1016/j.puhe.2019.09.020
19. Hu CY, Fang Y, Li FL, Dong B, Hua XG, Jiang W, et al. Association between ambient air pollution and Parkinson’s disease: systematic review and meta-analysis. Environ Res. (2019) 168:448–59. doi: 10.1016/j.envres.2018.10.008
20. Kasdagli MI, Katsouyanni K, Dimakopoulou K, Samoli E. Air pollution and Parkinson’s disease: a systematic review and meta-analysis up to 2018. Int J Hyg Environ Health. (2019) 222(3):402–9. doi: 10.1016/j.ijheh.2018.12.006
21. Murata H, Barnhill LM, Bronstein JM. Air pollution and the risk of Parkinson’s disease: a review. Mov Disord. (2022) 37(5):894–904. doi: 10.1002/mds.28922
22. Abbaszadeh S, Tabary M, Aryannejad A, Abolhasani R, Araghi F, Khaheshi I, et al. Air pollution and multiple sclerosis: a comprehensive review. Neurol Sci. (2021) 42(10):4063–72. doi: 10.1007/s10072-021-05508-4
23. Farahmandfard MA, Naghibzadeh-Tahami A, Khanjani N. Ambient air pollution and multiple sclerosis: a systematic review. Rev Environ Health. (2021) 36(4):535–44. doi: 10.1515/reveh-2020-0079
24. Noorimotlagh Z, Azizi M, Pan HF, Mami S, Mirzaee SA. Association between air pollution and multiple sclerosis: a systematic review. Environ Res. (2021) 196(110386):110386. doi: 10.1016/j.envres.2020.110386
25. Borroni E, Pesatori AC, Bollati V, Buoli M, Carugno M. Air pollution exposure and depression: a comprehensive updated systematic review and meta-analysis. Environ Pollut. (2022) 292(Pt A):118245. doi: 10.1016/j.envpol.2021.118245
26. Braithwaite I, Zhang S, Kirkbride JB, Osborn DPJ, Hayes JF. Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: a systematic review and meta-analysis. Environ Health Perspect. (2019) 127(12):126002. doi: 10.1289/EHP4595
27. Ritz SA. Air pollution as a potential contributor to the ‘epidemic’ of autoimmune disease. Med Hypotheses. (2010) 74(1):110–7. doi: 10.1016/j.mehy.2009.07.033
28. Celen H, Dens AC, Ronsmans S, Michiels S, De Langhe E. Airborne pollutants as potential triggers of systemic autoimmune rheumatic diseases: a narrative review. Acta Clin Belg. (2022) 77(5):874–82. doi: 10.1080/17843286.2021.1992582
29. Sun G, Hazlewood G, Bernatsky S, Kaplan GG, Eksteen B, Barnabe C. Association between air pollution and the development of rheumatic disease: a systematic review. Int J Rheumatol. (2016) 2016:5356307. doi: 10.1155/2016/5356307
30. Di D, Zhang L, Wu X, Leng R. Long-term exposure to outdoor air pollution and the risk of development of rheumatoid arthritis: a systematic review and meta-analysis. Semin Arthritis Rheum. (2020) 50(2):266–75. doi: 10.1016/j.semarthrit.2019.10.005
31. Essouma M, Noubiap JJ. Is air pollution a risk factor for rheumatoid arthritis? J Inflamm (Lond). (2015) 12:48. doi: 10.1186/s12950-015-0092-1
32. Gumtorntip W, Kasitanon N, Louthrenoo W, Chattipakorn N, Chattipakorn SC. Potential roles of air pollutants on the induction and aggravation of rheumatoid arthritis: from cell to bedside studies. Environ Pollut. (2023) 334:122181. doi: 10.1016/j.envpol.2023.122181
33. McDermott GC, Sparks JA. Invited perspective: air pollutants, genetics, and the mucosal paradigm for rheumatoid arthritis risk. Environ Health Perspect. (2023) 131(3):31303. doi: 10.1289/EHP12167
34. Sigaux J, Biton J, Andre E, Semerano L, Boissier MC. Air pollution as a determinant of rheumatoid arthritis. Joint Bone Spine. (2019) 86(1):37–42. doi: 10.1016/j.jbspin.2018.03.001
35. Zhang RD, Chen C, Wang P, Fang Y, Jiang LQ, Fang X, et al. Air pollution exposure and auto-inflammatory and autoimmune diseases of the musculoskeletal system: a review of epidemiologic and mechanistic evidence. Environ Geochem Health. (2023) 45(7):4087–105. doi: 10.1007/s10653-023-01495-x
36. Sawyerr AM, Ferguson A. Ulcerative colitis and crohn’s disease: similarities and distinctions. J R Coll Physicians Lond. (1994) 28(3):197–9.7932315
37. Bibiloni R, Mangold M, Madsen KL, Fedorak RN, Tannock GW. The bacteriology of biopsies differs between newly diagnosed, untreated, crohn’s disease and ulcerative colitis patients. J Med Microbiol. (2006) 55(Pt 8):1141–9. doi: 10.1099/jmm.0.46498-0
38. Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet. (2012) 380(9853):1606–19. doi: 10.1016/S0140-6736(12)60150-0
39. Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet. (2012) 380(9853):1590–605. doi: 10.1016/S0140-6736(12)60026-9
40. Collaborators GBDIBD. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. (2020) 5(1):17–30. doi: 10.1016/S2468-1253(19)30333-4
41. Cosnes J, Gower-Rousseau C, Seksik P, Cortot A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology. (2011) 140(6):1785–94. doi: 10.1053/j.gastro.2011.01.055
42. Kaplan GG, Ng SC. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology. (2017) 152(2):313–21 e2. doi: 10.1053/j.gastro.2016.10.020
43. Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. (2017) 390(10114):2769–78. doi: 10.1016/S0140-6736(17)32448-0
44. Zhao M, Gonczi L, Lakatos PL, Burisch J. The burden of inflammatory bowel disease in Europe in 2020. J Crohns Colitis. (2021) 15(9):1573–87. doi: 10.1093/ecco-jcc/jjab029
45. Burisch J, Jess T, Martinato M, Lakatos PL, EpiCom E. The burden of inflammatory bowel disease in Europe. J Crohns Colitis. (2013) 7(4):322–37. doi: 10.1016/j.crohns.2013.01.010
46. Peery AF, Crockett SD, Murphy CC, Lund JL, Dellon ES, Williams JL, et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2018. Gastroenterology. (2019) 156(1):254–72 e11. doi: 10.1053/j.gastro.2018.08.063
47. Ananthakrishnan AN, Bernstein CN, Iliopoulos D, Macpherson A, Neurath MF, Ali RAR, et al. Environmental triggers in IBD: a review of progress and evidence. Nat Rev Gastroenterol Hepatol. (2018) 15(1):39–49. doi: 10.1038/nrgastro.2017.136
48. Beamish LA, Osornio-Vargas AR, Wine E. Air pollution: an environmental factor contributing to intestinal disease. J Crohns Colitis. (2011) 5(4):279–86. doi: 10.1016/j.crohns.2011.02.017
49. Dam AN, Berg AM, Farraye FA. Environmental influences on the onset and clinical course of Crohn’s disease-part 1: an overview of external risk factors. Gastroenterol Hepatol (N Y. (2013) 9(11):711–7.24764788
50. Feng J, Cavallero S, Hsiai T, Li R. Impact of air pollution on intestinal redox lipidome and microbiome. Free Radic Biol Med. (2020) 151:99–110. doi: 10.1016/j.freeradbiomed.2019.12.044
51. Keulers L, Dehghani A, Knippels L, Garssen J, Papadopoulos N, Folkerts G, et al. Probiotics, prebiotics, and synbiotics to prevent or combat air pollution consequences: the gut-lung axis. Environ Pollut. (2022) 302:119066. doi: 10.1016/j.envpol.2022.119066
52. Khan R, Kuenzig ME, Benchimol EI. Epidemiology of pediatric inflammatory bowel disease. Gastroenterol Clin North Am. (2023) 52(3):483–96. doi: 10.1016/j.gtc.2023.05.001
53. Kuenzig ME, Benchimol EI. The role of the urban exposome in the increasing global rates of pediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr. (2022) 75(2):116–9. doi: 10.1097/MPG.0000000000003500
54. Legaki E, Gazouli M. Influence of environmental factors in the development of inflammatory bowel diseases. World J Gastrointest Pharmacol Ther. (2016) 7(1):112–25. doi: 10.4292/wjgpt.v7.i1.112
55. Martin TD, Chan SS, Hart AR. Environmental factors in the relapse and recurrence of inflammatory bowel disease: a review of the literature. Dig Dis Sci. (2015) 60(5):1396–405. doi: 10.1007/s10620-014-3437-3
56. Rogler G, Vavricka S. Exposome in IBD: recent insights in environmental factors that influence the onset and course of IBD. Inflamm Bowel Dis. (2015) 21(2):400–8. doi: 10.1097/MIB.0000000000000229
57. Shouval DS, Rufo PA. The role of environmental factors in the pathogenesis of inflammatory bowel diseases: a review. JAMA Pediatr. (2017) 171(10):999–1005. doi: 10.1001/jamapediatrics.2017.2571
58. van der Sloot KWJ, Amini M, Peters V, Dijkstra G, Alizadeh BZ. Inflammatory bowel diseases: review of known environmental protective and risk factors involved. Inflamm Bowel Dis. (2017) 23(9):1499–509. doi: 10.1097/MIB.0000000000001217
59. Vignal C, Guilloteau E, Gower-Rousseau C, Body-Malapel M. Review article: epidemiological and animal evidence for the role of air pollution in intestinal diseases. Sci Total Environ. (2021) 757(143718):143718. doi: 10.1016/j.scitotenv.2020.143718
60. Abegunde AT, Muhammad BH, Bhatti O, Ali T. Environmental risk factors for inflammatory bowel diseases: evidence based literature review. World J Gastroenterol. (2016) 22(27):6296–317. doi: 10.3748/wjg.v22.i27.6296
61. Ananthakrishnan AN. Environmental risk factors for inflammatory bowel diseases: a review. Dig Dis Sci. (2015) 60(2):290–8. doi: 10.1007/s10620-014-3350-9
62. Bilski J, Wojcik D, Danielak A, Mazur-Bialy A, Magierowski M, Tonnesen K, et al. Alternative therapy in the prevention of experimental and clinical inflammatory bowel disease. Impact of regular physical activity, intestinal alkaline phosphatase and herbal products. Curr Pharm Des. (2020) 26(25):2936–50. doi: 10.2174/1381612826666200427090127
63. Lee SH, Kwon JE, Cho ML. Immunological pathogenesis of inflammatory bowel disease. Intest Res. (2018) 16(1):26–42. doi: 10.5217/ir.2018.16.1.26
64. Santana PT, Rosas SLB, Ribeiro BE, Marinho Y, de Souza HSP. Dysbiosis in inflammatory bowel disease: pathogenic role and potential therapeutic targets. Int J Mol Sci. (2022) 23(7):3464. doi: 10.3390/ijms23073464
65. Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. (2014) 20(1):91–9. doi: 10.3748/wjg.v20.i1.91
66. Bernstein CN, Shanahan F. Disorders of a modern lifestyle: reconciling the epidemiology of inflammatory bowel diseases. Gut. (2008) 57(9):1185–91. doi: 10.1136/gut.2007.122143
67. Chen X, Wang S, Mao X, Xiang X, Ye S, Chen J, et al. Adverse health effects of emerging contaminants on inflammatory bowel disease. Front Public Health. (2023) 11:1140786. doi: 10.3389/fpubh.2023.1140786
68. Mutlu EA, Engen PA, Soberanes S, Urich D, Forsyth CB, Nigdelioglu R, et al. Particulate matter air pollution causes oxidant-mediated increase in gut permeability in mice. Part Fibre Toxicol. (2011) 8:19. doi: 10.1186/1743-8977-8-19
69. Fouladi F, Bailey MJ, Patterson WB, Sioda M, Blakley IC, Fodor AA, et al. Air pollution exposure is associated with the gut microbiome as revealed by shotgun metagenomic sequencing. Environ Int. (2020) 138:105604. doi: 10.1016/j.envint.2020.105604
70. Marynowski M, Likonska A, Zatorski H, Fichna J. Role of environmental pollution in irritable bowel syndrome. World J Gastroenterol. (2015) 21(40):11371–8. doi: 10.3748/wjg.v21.i40.11371
71. Okafor PN, Dahlen A, Youssef M, Olayode A, Sonu I, Neshatian L, et al. Environmental pollutants are associated with irritable bowel syndrome in a commercially insured cohort of California residents. Clin Gastroenterol Hepatol. (2023) 21(6):1617–26 e9. doi: 10.1016/j.cgh.2022.09.025
72. Tan TK, Saps M, Lin CL, Wei CC. Is long-term ambient air pollutant exposure a risk factor for irritable bowel syndrome in children? A 12-year longitudinal cohort study. J Neurogastroenterol Motil. (2019) 25(2):241–9. doi: 10.5056/jnm18135
73. Kaplan GG, Szyszkowicz M, Fichna J, Rowe BH, Porada E, Vincent R, et al. Non-specific abdominal pain and air pollution: a novel association. PLoS One. (2012) 7(10):e47669. doi: 10.1371/journal.pone.0047669
74. Duan R, Tian Y, Hu Y, Duan L. Exploring the association between short-term exposure to ambient fine particulate matter pollution and emergency admissions for peptic ulcer bleeding in Beijing, China. Atmos Environ. (2019) 213:485–90. doi: 10.1016/j.atmosenv.2019.06.037
75. Tsai SS, Chiu HF, Yang CY. Ambient air pollution and hospital admissions for peptic ulcers in Taipei: a time-stratified case-crossover study. Int J Environ Res Public Health. (2019) 16(11):1916. doi: 10.3390/ijerph16111916
76. Tian L, Qiu H, Sun S, Tsang H, Chan KP, Leung WK. Association between emergency admission for peptic ulcer bleeding and air pollution: a case-crossover analysis in Hong Kong’s elderly population. Lancet Planet Health. (2017) 1(2):e74–81. doi: 10.1016/S2542-5196(17)30021-9
77. Chen CC, Yang CY. Effects of ambient air pollution exposure on frequency of hospital admissions for appendicitis in Taipei, Taiwan. J Toxicol Environ Health A. (2018) 81(17):854–60. doi: 10.1080/15287394.2018.1498276
78. Kaplan GG, Dixon E, Panaccione R, Fong A, Chen L, Szyszkowicz M, et al. Effect of ambient air pollution on the incidence of appendicitis. CMAJ. (2009) 181(9):591–7. doi: 10.1503/cmaj.082068
79. Kaplan GG, Tanyingoh D, Dixon E, Johnson M, Wheeler AJ, Myers RP, et al. Ambient ozone concentrations and the risk of perforated and nonperforated appendicitis: a multicity case-crossover study. Environ Health Perspect. (2013) 121(8):939–43. doi: 10.1289/ehp.1206085
80. Xu C, Kan HD, Fan YN, Chen RJ, Liu JH, Li YF, et al. Acute effects of air pollution on enteritis admissions in Xi'an, China. J Toxicol Environ Health A. (2016) 79(24):1183–9. doi: 10.1080/15287394.2016.1227006
81. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
82. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
83. PRISMA. PRISMA (prisma-statement.org (2020).
84. Adami G, Pontalti M, Cattani G, Rossini M, Viapiana O, Orsolini G, et al. Association between long-term exposure to air pollution and immune-mediated diseases: a population-based cohort study. RMD Open. (2022) 8(1):e002055. doi: 10.1136/rmdopen-2021-002055
85. Ananthakrishnan AN, McGinley EL, Binion DG, Saeian K. Ambient air pollution correlates with hospitalizations for inflammatory bowel disease: an ecologic analysis. Inflamm Bowel Dis. (2011) 17(5):1138–45. doi: 10.1002/ibd.21455
86. Ding S, Sun S, Ding R, Song S, Cao Y, Zhang L. Association between exposure to air pollutants and the risk of inflammatory bowel diseases visits. Environ Sci Pollut Res Int. (2022) 29(12):17645–54. doi: 10.1007/s11356-021-17009-0
87. Duan R, Wu Y, Wang M, Wu J, Wang X, Wang Z, et al. Association between short-term exposure to fine particulate pollution and outpatient visits for ulcerative colitis in Beijing, China: a time-series study. Ecotoxicol Environ Saf. (2021) 214:112116. doi: 10.1016/j.ecoenv.2021.112116
88. Elten M, Benchimol EI, Fell DB, Kuenzig ME, Smith G, Chen H, et al. Ambient air pollution and the risk of pediatric-onset inflammatory bowel disease: a population-based cohort study. Environ Int. (2020) 138:105676. doi: 10.1016/j.envint.2020.105676
89. Fu C, Wang Q, Chen Y, Zhang Y. Exploring the causal relationship between airborne particulate matter and ulcerative colitis: a two-sample Mendelian randomization study. PLoS One. (2024) 19(3):e0300066. doi: 10.1371/journal.pone.0300066
90. Kaplan GG, Hubbard J, Korzenik J, Sands BE, Panaccione R, Ghosh S, et al. The inflammatory bowel diseases and ambient air pollution: a novel association. Am J Gastroenterol. (2010) 105(11):2412–9. doi: 10.1038/ajg.2010.252
91. Li FR, Wu KY, Fan WD, Chen GC, Tian H, Wu XB. Long-term exposure to air pollution and risk of incident inflammatory bowel disease among middle and old aged adults. Ecotoxicol Environ Saf. (2022) 242:113835. doi: 10.1016/j.ecoenv.2022.113835
92. Michaux M, Chan JM, Bergmann L, Chaves LF, Klinkenberg B, Jacobson K. Spatial cluster mapping and environmental modeling in pediatric inflammatory bowel disease. World J Gastroenterol. (2023) 29(23):3688–702. doi: 10.3748/wjg.v29.i23.3688
93. Opstelten JL, Beelen RMJ, Leenders M, Hoek G, Brunekreef B, van Schaik FDM, et al. Exposure to ambient air pollution and the risk of inflammatory bowel disease: a European nested case-control study. Dig Dis Sci. (2016) 61(10):2963–71. doi: 10.1007/s10620-016-4249-4
94. Szyszkowicz M. An approach to represent a combined exposure to air pollution. Int J Occup Med Environ Health. (2015) 28(5):823–30. doi: 10.13075/ijomeh.1896.00380
95. Wen J, Zhang J, Zhang H, Zhang N, Lei R, Deng Y, et al. Large-scale genome-wide association studies reveal the genetic causal etiology between air pollutants and autoimmune diseases. J Transl Med. (2024) 22(1):392. doi: 10.1186/s12967-024-04928-y
96. Chang C, Louie A, Zhou Y, Gupta R, Liang F, Xanthou G, et al. Ambient particulate matter induces in vitro toxicity to intestinal epithelial cells without exacerbating acute colitis induced by dextran sodium sulfate or 2,4,6-trinitrobenzenesulfonic acid. Int J Mol Sci. (2024) 25(13):7184. doi: 10.3390/ijms25137184
97. Liu Y, Wang T, Si B, Du H, Liu Y, Waqas A, et al. Intratracheally instillated diesel PM(2.5) significantly altered the structure and composition of indigenous murine gut microbiota. Ecotoxicol Environ Saf. (2021) 210:111903. doi: 10.1016/j.ecoenv.2021.111903
98. Salim SY, Jovel J, Wine E, Kaplan GG, Vincent R, Thiesen A, et al. Exposure to ingested airborne pollutant particulate matter increases mucosal exposure to bacteria and induces early onset of inflammation in neonatal IL-10-deficient mice. Inflamm Bowel Dis. (2014) 20(7):1129–38. doi: 10.1097/MIB.0000000000000066
99. Salim SY, Kaplan GG, Madsen KL. Air pollution effects on the gut microbiota: a link between exposure and inflammatory disease. Gut Microbes. (2014) 5(2):215–9. doi: 10.4161/gmic.27251
100. Son YS, Son N, Yu WD, Baek A, Park YJ, Lee MS, et al. Particulate matter 10 exposure affects intestinal functionality in both inflamed 2D intestinal epithelial cell and 3D intestinal organoid models. Front Immunol. (2023) 14:1168064. doi: 10.3389/fimmu.2023.1168064
101. Boogaard H, Patton AP, Atkinson RW, Brook JR, Chang HH, Crouse DL, et al. Long-term exposure to traffic-related air pollution and selected health outcomes: a systematic review and meta-analysis. Environ Int. (2022) 164:107262. doi: 10.1016/j.envint.2022.107262
102. Kaplan GG, Ng SC. Globalisation of inflammatory bowel disease: perspectives from the evolution of inflammatory bowel disease in the UK and China. Lancet Gastroenterol Hepatol. (2016) 1(4):307–16. doi: 10.1016/S2468-1253(16)30077-2
103. Loftus EV J, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Ulcerative colitis in Olmsted County, Minnesota, 1940–1993: incidence, prevalence, and survival. Gut. (2000) 46(3):336–43. doi: 10.1136/gut.46.3.336
104. Logan RF. Inflammatory bowel disease incidence: up, down or unchanged? Gut. (1998) 42(3):309–11. doi: 10.1136/gut.42.3.309
105. Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. (2012) 142(1):46–54 e42. quiz e30. doi: 10.1053/j.gastro.2011.10.001
106. Wang R, Li Z, Liu S, Zhang D. Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: a systematic analysis based on the global burden of disease study 2019. BMJ Open. (2023) 13(3):e065186. doi: 10.1136/bmjopen-2022-065186
107. Loftus EV J, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Crohn’s disease in Olmsted County, Minnesota, 1940–1993: incidence, prevalence, and survival. Gastroenterology. (1998) 114(6):1161–8. doi: 10.1016/S0016-5085(98)70421-4
108. Danese S, Sans M, Fiocchi C. Inflammatory bowel disease: the role of environmental factors. Autoimmun Rev. (2004) 3(5):394–400. doi: 10.1016/j.autrev.2004.03.002
109. Lakatos PL. Environmental factors affecting inflammatory bowel disease: have we made progress? Dig Dis. (2009) 27(3):215–25. doi: 10.1159/000228553
110. Koloski NA, Bret L, Radford-Smith G. Hygiene hypothesis in inflammatory bowel disease: a critical review of the literature. World J Gastroenterol. (2008) 14(2):165–73. doi: 10.3748/wjg.14.165
111. Thia KT, Loftus EV Jr, Sandborn WJ, Yang SK. An update on the epidemiology of inflammatory bowel disease in Asia. Am J Gastroenterol. (2008) 103(12):3167–82. doi: 10.1111/j.1572-0241.2008.02158.x
112. Agrawal M, Burisch J, Colombel J-F, Shah CS. Viewpoint: inflammatory bowel diseases among immigrants from low- to high-incidence countries: opportunities and considerations. J Crohns Colitis. (2020) 14(2):267–73. doi: 10.1093/ecco-jcc/jjz139
113. Agrawal M, Corn G, Shrestha S, Nielsen NM, Frisch M, Colombel JF, et al. Inflammatory bowel diseases among first-generation and second-generation immigrants in Denmark: a population-based cohort study. Gut. (2021) 70(6):1037–43. doi: 10.1136/gutjnl-2020-321798
114. Tsironi E, Feakins RM, Probert CS, Rampton DS, Phil D. Incidence of inflammatory bowel disease is rising and abdominal tuberculosis is falling in Bangladeshis in East London, United Kingdom. Am J Gastroenterol. (2004) 99(9):1749–55. doi: 10.1111/j.1572-0241.2004.30445.x
115. Williams CN. Does the incidence of IBD increase when persons move from a low- to a high-risk area? Inflamm Bowel Dis. (2008) 14(Suppl 2):S41–2. doi: 10.1097/00054725-200810001-00021
116. Hadad J E, Schreiner P, Vavricka SR, Greuter T. The genetics of inflammatory bowel disease. Mol Diagn Ther. (2024) 28(1):27–35. doi: 10.1007/s40291-023-00678-7
117. Zhao M, Burisch J. Impact of genes and the environment on the pathogenesis and disease course of inflammatory bowel disease. Dig Dis Sci. (2019) 64(7):1759–69. doi: 10.1007/s10620-019-05648-w
118. Goyette P, Labbe C, Trinh TT, Xavier RJ, Rioux JD. Molecular pathogenesis of inflammatory bowel disease: genotypes, phenotypes and personalized medicine. Ann Med. (2007) 39(3):177–99. doi: 10.1080/07853890701197615
119. Sartor RB. Mechanisms of disease: pathogenesis of Crohn’s disease and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol. (2006) 3(7):390–407. doi: 10.1038/ncpgasthep0528
120. Scharl M, Rogler G. Inflammatory bowel disease pathogenesis: what is new? Curr Opin Gastroenterol. (2012) 28(4):301–9. doi: 10.1097/MOG.0b013e328353e61e
121. Vedamurthy A, Ananthakrishnan AN. Influence of environmental factors in the development and outcomes of inflammatory bowel disease. Gastroenterol Hepatol (N Y). (2019) 15(2):72–82.31011301
122. Lopes EW, Chan SSM, Song M, Ludvigsson JF, Hakansson N, Lochhead P, et al. Lifestyle factors for the prevention of inflammatory bowel disease. Gut. (2022):328174. doi: 10.1136/gutjnl-2022-328174
123. Sun Y, Yuan S, Chen X, Sun J, Kalla R, Yu L, et al. The contribution of genetic risk and lifestyle factors in the development of adult-onset inflammatory bowel disease: a prospective cohort study. Am J Gastroenterol. (2023) 118(3):511–22. doi: 10.14309/ajg.0000000000002180
124. Aamodt G, Jahnsen J, Bengtson MB, Moum B, Vatn MH, Group IS. Geographic distribution and ecological studies of inflammatory bowel disease in southeastern Norway in 1990–1993. Inflamm Bowel Dis. (2008) 14(7):984–91. doi: 10.1002/ibd.20417
125. Green C, Elliott L, Beaudoin C, Bernstein CN. A population-based ecologic study of inflammatory bowel disease: searching for etiologic clues. Am J Epidemiol. (2006) 164(7):615–23. discussion 24-8. doi: 10.1093/aje/kwj260
126. Soon IS, Molodecky NA, Rabi DM, Ghali WA, Barkema HW, Kaplan GG. The relationship between urban environment and the inflammatory bowel diseases: a systematic review and meta-analysis. BMC Gastroenterol. (2012) 12(51):51. doi: 10.1186/1471-230X-12-51
127. Ng SC, Kaplan GG, Tang W, Banerjee R, Adigopula B, Underwood FE, et al. Population density and risk of inflammatory bowel disease: a prospective population-based study in 13 countries or regions in Asia-pacific. Am J Gastroenterol. (2019) 114(1):107–15. doi: 10.1038/s41395-018-0233-2
128. Zhang Z, Chen L, Qian ZM, Li H, Cai M, Wang X, et al. Residential green and blue space associated with lower risk of adult-onset inflammatory bowel disease: findings from a large prospective cohort study. Environ Int. (2022) 160:107084. doi: 10.1016/j.envint.2022.107084
129. Declercq C, Gower-Rousseau C, Vernier-Massouille G, Salleron J, Balde M, Poirier G, et al. Mapping of inflammatory bowel disease in northern France: spatial variations and relation to affluence. Inflamm Bowel Dis. (2010) 16(5):807–12. doi: 10.1002/ibd.21111
130. Ng SC, Bernstein CN, Vatn MH, Lakatos PL, Loftus EV Jr, Tysk C, et al. Geographical variability and environmental risk factors in inflammatory bowel disease. Gut. (2013) 62(4):630–49. doi: 10.1136/gutjnl-2012-303661
131. Zhou S, Chai P, Dong X, Liang Z, Yang Z, Li J, et al. Drinking water quality and inflammatory bowel disease: a prospective cohort study. Environ Sci Pollut Res Int. (2023) 30(27):71171–83. doi: 10.1007/s11356-023-27460-w
132. Cohen-Mekelburg S, Van T, Wallace B, Berinstein J, Yu X, Lewis J, et al. The association between nonsteroidal anti-inflammatory drug use and inflammatory bowel disease exacerbations: a true association or residual bias? Am J Gastroenterol. (2022) 117(11):1851–7. doi: 10.14309/ajg.0000000000001932
133. Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A comprehensive review of non-steroidal anti-inflammatory drug use in the elderly. Aging Dis. (2018) 9(1):143–50. doi: 10.14336/AD.2017.0306
134. Preda CM, Manuc T, Istratescu D, Louis E, Baicus C, Sandra I, et al. Environmental factors in Romanian and Belgian patients with inflammatory bowel disease - a retrospective comparative study. Maedica (Bucur). (2019) 14(3):233–9. doi: 10.26574/maedica.2019.14.3.233
135. Faye AS, Allin KH, Iversen AT, Agrawal M, Faith J, Colombel JF, et al. Antibiotic use as a risk factor for inflammatory bowel disease across the ages: a population-based cohort study. Gut. (2023) 72(4):663–70. doi: 10.1136/gutjnl-2022-327845
136. Khalili H, Higuchi LM, Ananthakrishnan AN, Richter JM, Feskanich D, Fuchs CS, et al. Oral contraceptives, reproductive factors and risk of inflammatory bowel disease. Gut. (2013) 62(8):1153–9. doi: 10.1136/gutjnl-2012-302362
137. Ortizo R, Lee SY, Nguyen ET, Jamal MM, Bechtold MM, Nguyen DL. Exposure to oral contraceptives increases the risk for development of inflammatory bowel disease: a meta-analysis of case-controlled and cohort studies. Eur J Gastroenterol Hepatol. (2017) 29(9):1064–70. doi: 10.1097/MEG.0000000000000915
138. Pasvol TJ, Bloom S, Segal AW, Rait G, Horsfall L. Use of contraceptives and risk of inflammatory bowel disease: a nested case-control study. Aliment Pharmacol Ther. (2022) 55(3):318–26. doi: 10.1111/apt.16647
139. Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature. Am J Gastroenterol. (2011) 106(4):563–73. doi: 10.1038/ajg.2011.44
140. Asakura H, Suzuki K, Kitahora T, Morizane T. Is there a link between food and intestinal microbes and the occurrence of Crohn’s disease and ulcerative colitis? J Gastroenterol Hepatol. (2008) 23(12):1794–801. doi: 10.1111/j.1440-1746.2008.05681.x
141. Reif S, Klein I, Lubin F, Farbstein M, Hallak A, Gilat T. Pre-illness dietary factors in inflammatory bowel disease. Gut. (1997) 40(6):754–60. doi: 10.1136/gut.40.6.754
142. Ananthakrishnan AN, Khalili H, Konijeti GG, Higuchi LM, de Silva P, Korzenik JR, et al. A prospective study of long-term intake of dietary fiber and risk of Crohn’s disease and ulcerative colitis. Gastroenterology. (2013) 145(5):970–7. doi: 10.1053/j.gastro.2013.07.050
143. Ananthakrishnan AN, Khalili H, Konijeti GG, Higuchi LM, de Silva P, Fuchs CS, et al. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn’s disease. Gut. (2014) 63(5):776–84. doi: 10.1136/gutjnl-2013-305304
144. Ananthakrishnan AN, Khalili H, Song M, Higuchi LM, Richter JM, Nimptsch K, et al. High school diet and risk of Crohn’s disease and ulcerative colitis. Inflamm Bowel Dis. (2015) 21(10):2311–9. doi: 10.1097/MIB.0000000000000501
145. Ajabnoor SM, Thorpe G, Abdelhamid A, Hooper L. Long-term effects of increasing omega-3, omega-6 and total polyunsaturated fats on inflammatory bowel disease and markers of inflammation: a systematic review and meta-analysis of randomized controlled trials. Eur J Nutr. (2021) 60(5):2293–316. doi: 10.1007/s00394-020-02413-y
146. Ananthakrishnan AN, Khalili H, Higuchi LM, Bao Y, Korzenik JR, Giovannucci EL, et al. Higher predicted vitamin D status is associated with reduced risk of Crohn’s disease. Gastroenterology. (2012) 142(3):482–9. doi: 10.1053/j.gastro.2011.11.040
147. Holmes EA, Rodney Harris RM, Lucas RM. Low sun exposure and vitamin D deficiency as risk factors for inflammatory bowel disease, with a focus on childhood onset. Photochem Photobiol. (2019) 95(1):105–18. doi: 10.1111/php.13007
148. Shivananda S, Lennard-Jones J, Logan R, Fear N, Price A, Carpenter L, et al. Incidence of inflammatory bowel disease across Europe: is there a difference between north and south? Results of the European collaborative study on inflammatory bowel disease (EC-IBD). Gut. (1996) 39(5):690–7. doi: 10.1136/gut.39.5.690
149. Abautret-Daly A, Dempsey E, Parra-Blanco A, Medina C, Harkin A. Gut-brain actions underlying comorbid anxiety and depression associated with inflammatory bowel disease. Acta Neuropsychiatr. (2018) 30(5):275–96. doi: 10.1017/neu.2017.3
150. Black J, Sweeney L, Yuan Y, Singh H, Norton C, Czuber-Dochan W. Systematic review: the role of psychological stress in inflammatory bowel disease. Aliment Pharmacol Ther. (2022) 56(8):1235–49. doi: 10.1111/apt.17202
151. Sidik S. Chronic stress can inflame the gut—now scientists know why. Nature. (2023) 618(7964):221–2. doi: 10.1038/d41586-023-01700-y
152. Oligschlaeger Y, Yadati T, Houben T, Condello Olivan CM, Shiri-Sverdlov R. Inflammatory bowel disease: a stressed “gut/feeling”. Cells. (2019) 8(7):659. doi: 10.3390/cells8070659
153. Konturek PC, Brzozowski T, Konturek SJ. Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options. J Physiol Pharmacol. (2011) 62(6):591–9.22314561
154. Karl JP, Hatch AM, Arcidiacono SM, Pearce SC, Pantoja-Feliciano IG, Doherty LA, et al. Effects of psychological, environmental and physical stressors on the gut microbiota. Front Microbiol. (2018) 9:2013. doi: 10.3389/fmicb.2018.02013
155. Li X, Sundquist J, Sundquist K. Educational level and occupation as risk factors for inflammatory bowel diseases: a nationwide study based on hospitalizations in Sweden. Inflamm Bowel Dis. (2009) 15(4):608–15. doi: 10.1002/ibd.20815
156. Severs M, Spekhorst LM, Mangen MJ, Dijkstra G, Lowenberg M, Hoentjen F, et al. Sex-Related differences in patients with inflammatory bowel disease: results of 2 prospective cohort studies. Inflamm Bowel Dis. (2018) 24(6):1298–306. doi: 10.1093/ibd/izy004
157. Alam MT, Amos GCA, Murphy ARJ, Murch S, Wellington EMH, Arasaradnam RP. Microbial imbalance in inflammatory bowel disease patients at different taxonomic levels. Gut Pathog. (2020) 12:1. doi: 10.1186/s13099-019-0341-6
158. Ryan FJ, Ahern AM, Fitzgerald RS, Laserna-Mendieta EJ, Power EM, Clooney AG, et al. Colonic microbiota is associated with inflammation and host epigenomic alterations in inflammatory bowel disease. Nat Commun. (2020) 11(1):1512. doi: 10.1038/s41467-020-15342-5
159. Dujardin CE, Mars RAT, Manemann SM, Kashyap PC, Clements NS, Hassett LC, et al. Impact of air quality on the gastrointestinal microbiome: a review. Environ Res. (2020) 186:109485. doi: 10.1016/j.envres.2020.109485
160. Kish L, Hotte N, Kaplan GG, Vincent R, Tso R, Ganzle M, et al. Environmental particulate matter induces murine intestinal inflammatory responses and alters the gut microbiome. PLoS One. (2013) 8(4):e62220. doi: 10.1371/journal.pone.0062220
161. Li R, Yang J, Saffari A, Jacobs J, Baek KI, Hough G, et al. Ambient ultrafine particle ingestion alters gut microbiota in association with increased atherogenic lipid metabolites. Sci Rep. (2017) 7:42906. doi: 10.1038/srep42906
162. Liu W, Zhou Y, Yong L, Qin Y, Yu L, Li R, et al. Effects of PM(2.5) exposure during gestation on maternal gut microbiota and pregnancy outcomes. Chemosphere. (2020) 247:125879. doi: 10.1016/j.chemosphere.2020.125879
163. Mutlu EA, Comba IY, Cho T, Engen PA, Yazici C, Soberanes S, et al. Inhalational exposure to particulate matter air pollution alters the composition of the gut microbiome. Environ Pollut. (2018) 240:817–30. doi: 10.1016/j.envpol.2018.04.130
164. Ran Z, An Y, Zhou J, Yang J, Zhang Y, Yang J, et al. Subchronic exposure to concentrated ambient PM2.5 perturbs gut and lung microbiota as well as metabolic profiles in mice. Environ Pollut. (2021) 272:115987. doi: 10.1016/j.envpol.2020.115987
165. Van Pee T, Nawrot TS, van Leeuwen R, Hogervorst J. Ambient particulate air pollution and the intestinal microbiome; a systematic review of epidemiological, in vivo and, in vitro studies. Sci Total Environ. (2023) 878:162769. doi: 10.1016/j.scitotenv.2023.162769
166. Alderete TL, Jones RB, Chen Z, Kim JS, Habre R, Lurmann F, et al. Exposure to traffic-related air pollution and the composition of the gut microbiota in overweight and obese adolescents. Environ Res. (2018) 161:472–8. doi: 10.1016/j.envres.2017.11.046
167. Morgan XC, Tickle TL, Sokol H, Gevers D, Devaney KL, Ward DV, et al. Dysfunction of the intestinal microbiome in inflammatory bowel disease and treatment. Genome Biol. (2012) 13(9):R79. doi: 10.1186/gb-2012-13-9-r79
168. Kloska M, Mankowska-Wierzbicka D, Czlapka-Matyasik M, Dobrowolska A, Grzymislawski M. [Oxidative stress in etiopathogenesis of inflammatory bowel diseases]. Postepy Biochem. (2020) 66(2):143–50. doi: 10.18388/pb.2020_324
169. Tian T, Wang Z, Zhang J. Pathomechanisms of oxidative stress in inflammatory bowel disease and potential antioxidant therapies. Oxid Med Cell Longev. (2017) 2017:4535194. doi: 10.1155/2017/4535194
170. Sahoo DK, Heilmann RM, Paital B, Patel A, Yadav VK, Wong D, et al. Oxidative stress, hormones, and effects of natural antioxidants on intestinal inflammation in inflammatory bowel disease. Front Endocrinol (Lausanne). (2023) 14:1217165. doi: 10.3389/fendo.2023.1217165
171. Gawda A, Majka G, Nowak B, Marcinkiewicz J. Air pollution, oxidative stress, and exacerbation of autoimmune diseases. Cent Eur J Immunol. (2017) 42(3):305–12. doi: 10.5114/ceji.2017.70975
172. Qin J, Xia W, Liang G, Xu S, Zhao X, Wang D, et al. Association of fine particulate matter with glucose and lipid metabolism: a longitudinal study in young adults. Occup Environ Med. (2021):107039. doi: 10.1136/oemed-2020-107039
173. Arrieta MC, Bistritz L, Meddings JB. Alterations in intestinal permeability. Gut. (2006) 55(10):1512–20. doi: 10.1136/gut.2005.085373
174. Rivas-Arancibia S, Miranda-Martinez A, Rodriguez-Martinez E, Hernandez-Orozco E, Valdes-Fuentes M, De la Rosa-Sierra R. Ozone environmental pollution: relationship between the intestine and neurodegenerative diseases. Antioxidants (Basel). (2023) 12(7):1323. doi: 10.3390/antiox12071323
175. Salim SY, Soderholm JD. Importance of disrupted intestinal barrier in inflammatory bowel diseases. Inflamm Bowel Dis. (2011) 17(1):362–81. doi: 10.1002/ibd.21403
176. Papoutsopoulou S, Satsangi J, Campbell BJ, Probert CS. Review article: impact of cigarette smoking on intestinal inflammation-direct and indirect mechanisms. Aliment Pharmacol Ther. (2020) 51(12):1268–85. doi: 10.1111/apt.15774
177. Breuer-Katschinski BD, Hollander N, Goebell H. Effect of cigarette smoking on the course of crohn’s disease. Eur J Gastroenterol Hepatol. (1996) 8(3):225–8. doi: 10.1097/00042737-199603000-00007
178. Danese S, Fiocchi C. Etiopathogenesis of inflammatory bowel diseases. World J Gastroenterol. (2006) 12(30):4807–12. doi: 10.3748/wjg.v12.i30.4807
179. Karczewski J, Poniedzialek B, Rzymski P, Rychlewska-Hanczewska A, Adamski Z, Wiktorowicz K. The effect of cigarette smoking on the clinical course of inflammatory bowel disease. Prz Gastroenterol. (2014) 9(3):153–9. doi: 10.5114/pg.2014.43577
180. Parkes GC, Whelan K, Lindsay JO. Smoking in inflammatory bowel disease: impact on disease course and insights into the aetiology of its effect. J Crohns Colitis. (2014) 8(8):717–25. doi: 10.1016/j.crohns.2014.02.002
181. van der Heide F, Dijkstra A, Weersma RK, Albersnagel FA, van der Logt EM, Faber KN, et al. Effects of active and passive smoking on disease course of Crohn’s disease and ulcerative colitis. Inflamm Bowel Dis. (2009) 15(8):1199–207. doi: 10.1002/ibd.20884
182. Higuchi LM, Khalili H, Chan AT, Richter JM, Bousvaros A, Fuchs CS. A prospective study of cigarette smoking and the risk of inflammatory bowel disease in women. Am J Gastroenterol. (2012) 107(9):1399–406. doi: 10.1038/ajg.2012.196
183. Mahid SS, Minor KS, Soto RE, Hornung CA, Galandiuk S. Smoking and inflammatory bowel disease: a meta-analysis. Mayo Clin Proc. (2006) 81(11):1462–71. doi: 10.4065/81.11.1462
184. Jones DT, Osterman MT, Bewtra M, Lewis JD. Passive smoking and inflammatory bowel disease: a meta-analysis. Am J Gastroenterol. (2008) 103(9):2382–93. doi: 10.1111/j.1572-0241.2008.01999.x
185. AlQasrawi D, Abdelli LS, Naser SA. Mystery solved: why smoke extract worsens disease in smokers with crohn’s disease and not ulcerative colitis? Gut MAP! Microorganisms. (2020) 8(5):666. doi: 10.3390/microorganisms8050666
186. Dorey A, Scheerlinck P, Nguyen H, Albertson T. Acute and chronic carbon monoxide toxicity from tobacco smoking. Mil Med. (2020) 185(1-2):e61–e7. doi: 10.1093/milmed/usz280
187. Maines MD. The heme oxygenase system: a regulator of second messenger gases. Annu Rev Pharmacol Toxicol. (1997) 37:517–54. doi: 10.1146/annurev.pharmtox.37.1.517
188. Naito Y, Takagi T, Yoshikawa T. Heme oxygenase-1: a new therapeutic target for inflammatory bowel disease. Aliment Pharmacol Ther. (2004) 20(Suppl 1):177–84. doi: 10.1111/j.1365-2036.2004.01992.x
189. Onyiah JC, Sheikh SZ, Maharshak N, Otterbein LE, Plevy SE. Heme oxygenase-1 and carbon monoxide regulate intestinal homeostasis and mucosal immune responses to the enteric microbiota. Gut Microbes. (2014) 5(2):220–4. doi: 10.4161/gmic.27290
190. Takagi T, Uchiyama K, Naito Y. The therapeutic potential of carbon monoxide for inflammatory bowel disease. Digestion. (2015) 91(1):13–8. doi: 10.1159/000368765
191. Takagi T, Naito Y, Inoue M, Akagiri S, Mizushima K, Handa O, et al. Inhalation of carbon monoxide ameliorates collagen-induced arthritis in mice and regulates the articular expression of IL-1beta and MCP-1. Inflammation. (2009) 32(2):83–8. doi: 10.1007/s10753-009-9106-6
192. Armitage EL, Aldhous MC, Anderson N, Drummond HE, Riemersma RA, Ghosh S, et al. Incidence of juvenile-onset crohn’s disease in Scotland: association with northern latitude and affluence. Gastroenterology. (2004) 127(4):1051–7. doi: 10.1053/j.gastro.2004.06.024
193. Aujnarain A, Mack DR, Benchimol EI. The role of the environment in the development of pediatric inflammatory bowel disease. Curr Gastroenterol Rep. (2013) 15(6):326. doi: 10.1007/s11894-013-0326-4
194. Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. (2011) 17(1):423–39. doi: 10.1002/ibd.21349
195. Benchimol EI, Guttmann A, Griffiths AM, Rabeneck L, Mack DR, Brill H, et al. Increasing incidence of paediatric inflammatory bowel disease in Ontario, Canada: evidence from health administrative data. Gut. (2009) 58(11):1490–7. doi: 10.1136/gut.2009.188383
196. Chan JM, Carroll MW, Smyth M, Hamilton Z, Evans D, McGrail K, et al. Comparing health administrative and clinical registry data: trends in incidence and prevalence of pediatric inflammatory bowel disease in British Columbia. Clin Epidemiol. (2021) 13:81–90. doi: 10.2147/CLEP.S292546
197. Huang JG, Wong YKY, Chew KS, Tanpowpong P, Calixto Mercado KS, Reodica A, et al. Epidemiological characteristics of Asian children with inflammatory bowel disease at diagnosis: insights from an Asian-pacific multi-centre registry network. World J Gastroenterol. (2022) 28(17):1830–44. doi: 10.3748/wjg.v28.i17.1830
198. Kim SH, Park Y, Kim SP, Lee SH, Oh SH, Yang SK, et al. Shift to a younger age and regional differences in inflammatory bowel disease in Korea: using healthcare administrative data. Dig Dis Sci. (2022) 67(11):5079–89. doi: 10.1007/s10620-021-07328-0
199. Nikkila A, Auvinen A, Kolho KL. Clustering of pediatric onset inflammatory bowel disease in Finland: a nationwide register-based study. BMC Gastroenterol. (2022) 22(1):512. doi: 10.1186/s12876-022-02579-1
200. Kuenzig ME, Fung SG, Marderfeld L, Mak JWY, Kaplan GG, Ng SC, et al. Twenty-first century trends in the global epidemiology of pediatric-onset inflammatory bowel disease: systematic review. Gastroenterology. (2022) 162(4):1147–59 e4. doi: 10.1053/j.gastro.2021.12.282
201. Imielinski M, Baldassano RN, Griffiths A, Russell RK, Annese V, Dubinsky M, et al. Common variants at five new loci associated with early-onset inflammatory bowel disease. Nat Genet. (2009) 41(12):1335–40. doi: 10.1038/ng.489
202. Van Limbergen J, Russell RK, Drummond HE, Aldhous MC, Round NK, Nimmo ER, et al. Definition of phenotypic characteristics of childhood-onset inflammatory bowel disease. Gastroenterology. (2008) 135(4):1114–22. doi: 10.1053/j.gastro.2008.06.081
203. Sly PD, Flack F. Susceptibility of children to environmental pollutants. Ann N Y Acad Sci. (2008) 1140:163–83. doi: 10.1196/annals.1454.017
204. Jost T, Lacroix C, Braegger CP, Chassard C. New insights in gut microbiota establishment in healthy breast fed neonates. PLoS One. (2012) 7(8):e44595. doi: 10.1371/journal.pone.0044595
205. Song C, Yang J, Ye W, Zhang Y, Tang C, Li X, et al. Urban-rural environmental exposure during childhood and subsequent risk of inflammatory bowel disease: a meta-analysis. Expert Rev Gastroenterol Hepatol. (2019) 13(6):591–602. doi: 10.1080/17474124.2018.1511425
206. Bernstein CN, Burchill C, Targownik LE, Singh H, Roos LL. Events within the first year of life, but not the neonatal period, affect risk for later development of inflammatory bowel diseases. Gastroenterology. (2019) 156(8):2190–7 e10. doi: 10.1053/j.gastro.2019.02.004
207. Sonntag B, Stolze B, Heinecke A, Luegering A, Heidemann J, Lebiedz P, et al. Preterm birth but not mode of delivery is associated with an increased risk of developing inflammatory bowel disease later in life. Inflamm Bowel Dis. (2007) 13(11):1385–90. doi: 10.1002/ibd.20206
208. Jakobsen C, Paerregaard A, Munkholm P, Wewer V. Environmental factors and risk of developing paediatric inflammatory bowel disease—a population based study 2007–2009. J Crohns Colitis. (2013) 7(1):79–88. doi: 10.1016/j.crohns.2012.05.024
209. Jawad AB, Jansson S, Wewer V, Malham M. Early life oral antibiotics are associated with pediatric-onset inflammatory bowel disease-A nationwide study. J Pediatr Gastroenterol Nutr. (2023) 77(3):366–72. doi: 10.1097/MPG.0000000000003861
210. Kronman MP, Zaoutis TE, Haynes K, Feng R, Coffin SE. Antibiotic exposure and IBD development among children: a population-based cohort study. Pediatrics. (2012) 130(4):e794–803. doi: 10.1542/peds.2011-3886
211. Shaw SY, Blanchard JF, Bernstein CN. Association between the use of antibiotics in the first year of life and pediatric inflammatory bowel disease. Am J Gastroenterol. (2010) 105(12):2687–92. doi: 10.1038/ajg.2010.398
212. Virta L, Auvinen A, Helenius H, Huovinen P, Kolho KL. Association of repeated exposure to antibiotics with the development of pediatric crohn’s disease–a nationwide, register-based Finnish case-control study. Am J Epidemiol. (2012) 175(8):775–84. doi: 10.1093/aje/kwr400
213. Ortqvist AK, Lundholm C, Halfvarson J, Ludvigsson JF, Almqvist C. Fetal and early life antibiotics exposure and very early onset inflammatory bowel disease: a population-based study. Gut. (2019) 68(2):218–25. doi: 10.1136/gutjnl-2017-314352
214. Luther J, Dave M, Higgins PD, Kao JY. Association between Helicobacter pylori infection and inflammatory bowel disease: a meta-analysis and systematic review of the literature. Inflamm Bowel Dis. (2010) 16(6):1077–84. doi: 10.1002/ibd.21116
215. Bernstein CN, Rawsthorne P, Cheang M, Blanchard JF. A population-based case control study of potential risk factors for IBD. Am J Gastroenterol. (2006) 101(5):993–1002. doi: 10.1111/j.1572-0241.2006.00381.x
216. Klement E, Lysy J, Hoshen M, Avitan M, Goldin E, Israeli E. Childhood hygiene is associated with the risk for inflammatory bowel disease: a population-based study. Am J Gastroenterol. (2008) 103(7):1775–82. doi: 10.1111/j.1572-0241.2008.01905.x
217. Gent AE, Hellier MD, Grace RH, Swarbrick ET, Coggon D. Inflammatory bowel disease and domestic hygiene in infancy. Lancet. (1994) 343(8900):766–7. doi: 10.1016/S0140-6736(94)91841-4
218. Cholapranee A, Ananthakrishnan AN. Environmental hygiene and risk of inflammatory bowel diseases: a systematic review and meta-analysis. Inflamm Bowel Dis. (2016) 22(9):2191–9. doi: 10.1097/MIB.0000000000000852
219. Radon K, Windstetter D, Poluda AL, Mueller B, von Mutius E, Koletzko S, et al. Contact with farm animals in early life and juvenile inflammatory bowel disease: a case-control study. Pediatrics. (2007) 120(2):354–61. doi: 10.1542/peds.2006-3624
220. Timm S, Svanes C, Janson C, Sigsgaard T, Johannessen A, Gislason T, et al. Place of upbringing in early childhood as related to inflammatory bowel diseases in adulthood: a population-based cohort study in Northern Europe. Eur J Epidemiol. (2014) 29(6):429–37. doi: 10.1007/s10654-014-9922-3
221. Hasosah M, Alhashmi W, Abualsaud R, Alamoudi A, Aljawad A, Tunkar M, et al. Environmental risk factors for childhood inflammatory bowel diseases: a multicenter case-control study. Children (Basel). (2022) 9(3):438. doi: 10.3390/children9030438
222. Strisciuglio C, Giugliano F, Martinelli M, Cenni S, Greco L, Staiano A, et al. Impact of environmental and familial factors in a cohort of pediatric patients with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. (2017) 64(4):569–74. doi: 10.1097/MPG.0000000000001297
223. Pinsk V, Lemberg DA, Grewal K, Barker CC, Schreiber RA, Jacobson K. Inflammatory bowel disease in the south Asian pediatric population of British Columbia. Am J Gastroenterol. (2007) 102(5):1077–83. doi: 10.1111/j.1572-0241.2007.01124.x
224. Rajasekaran V, Evans HM, Andrews A, Bishop JR, Lopez RN, Mouat S, et al. Rising incidence of inflammatory bowel disease in south Asian children in New Zealand-A retrospective population-based study. J Pediatr Gastroenterol Nutr. (2023) 76(6):749–55. doi: 10.1097/MPG.0000000000003735
225. Benchimol EI, Kaplan GG, Otley AR, Nguyen GC, Underwood FE, Guttmann A, et al. Rural and urban residence during early life is associated with risk of inflammatory bowel disease: a population-based inception and birth cohort study. Am J Gastroenterol. (2017) 112(9):1412–22. doi: 10.1038/ajg.2017.208
226. Barclay AR, Russell RK, Wilson ML, Gilmour WH, Satsangi J, Wilson DC. Systematic review: the role of breastfeeding in the development of pediatric inflammatory bowel disease. J Pediatr. (2009) 155(3):421–6. doi: 10.1016/j.jpeds.2009.03.017
227. Klement E, Cohen RV, Boxman J, Joseph A, Reif S. Breastfeeding and risk of inflammatory bowel disease: a systematic review with meta-analysis. Am J Clin Nutr. (2004) 80(5):1342–52. doi: 10.1093/ajcn/80.5.1342
228. Xu L, Lochhead P, Ko Y, Claggett B, Leong RW, Ananthakrishnan AN. Systematic review with meta-analysis: breastfeeding and the risk of Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. (2017) 46(9):780–9. doi: 10.1111/apt.14291
229. Bertin B, Foligne B, Ley D, Lesage J, Beghin L, Morcel J, et al. An overview of the influence of breastfeeding on the development of inflammatory bowel disease. Nutrients. (2023) 15(24):5103. doi: 10.3390/nu15245103
230. Amrousy D E, Ashry H E, Hodeib H, Hassan S. Vitamin D in children with inflammatory bowel disease: a randomized controlled clinical trial. J Clin Gastroenterol. (2021) 55(9):815–20. doi: 10.1097/MCG.0000000000001443
231. Koutroubakis IE, Vlachonikolis IG. Appendectomy and the development of ulcerative colitis: results of a metaanalysis of published case-control studies. Am J Gastroenterol. (2000) 95(1):171–6. doi: 10.1111/j.1572-0241.2000.01680.x
232. Elten M, Benchimol EI, Fell DB, Kuenzig ME, Smith G, Kaplan GG, et al. Residential greenspace in childhood reduces risk of pediatric inflammatory bowel disease: a population-based cohort study. Am J Gastroenterol. (2021) 116(2):347–53. doi: 10.14309/ajg.0000000000000990
233. Wang L, Pinkerton KE. Air pollutant effects on fetal and early postnatal development. Birth Defects Res C Embryo Today. (2007) 81(3):144–54. doi: 10.1002/bdrc.20097
234. Auten RL, Foster WM. Biochemical effects of ozone on asthma during postnatal development. Biochim Biophys Acta. (2011) 1810(11):1114–9. doi: 10.1016/j.bbagen.2011.01.008
235. Suarez RG, Osornio-Vargas AR, Wine E. Ambient air pollution and pediatric inflammatory bowel diseases: an updated scoping review. Dig Dis Sci. (2022) 67(9):4342–54. doi: 10.1007/s10620-022-07597-3
236. Ruiz-Gil T, Acuna JJ, Fujiyoshi S, Tanaka D, Noda J, Maruyama F, et al. Airborne bacterial communities of outdoor environments and their associated influencing factors. Environ Int. (2020) 145:106156. doi: 10.1016/j.envint.2020.106156
237. Vester-Andersen MK, Mirsepasi-Lauridsen HC, Prosberg MV, Mortensen CO, Trager C, Skovsen K, et al. Increased abundance of proteobacteria in aggressive Crohn’s disease seven years after diagnosis. Sci Rep. (2019) 9(1):13473. doi: 10.1038/s41598-019-49833-3
238. Ravva SV, Sarreal CZ, Mandrell RE. Bacterial communities in aerosols and manure samples from two different dairies in central and Sonoma valleys of California. PLoS One. (2011) 6(2):e17281. doi: 10.1371/journal.pone.0017281
239. Everhov AH, Soderling J, Befrits G, Khalili H, Broms G, Neovius M, et al. Increasing healthcare costs in inflammatory bowel disease 2007–2020 in Sweden. Aliment Pharmacol Ther. (2023) 58(7):692–703. doi: 10.1111/apt.17675
240. Burisch J, Zhao M, Odes S, De Cruz P, Vermeire S, Bernstein CN, et al. The cost of inflammatory bowel disease in high-income settings: a lancet gastroenterology & hepatology commission. Lancet Gastroenterol Hepatol. (2023) 8(5):458–92. doi: 10.1016/S2468-1253(23)00003-1
Appendix A

Table A1. The evaluation from very low to high, with a description of the assessment criteria (101).
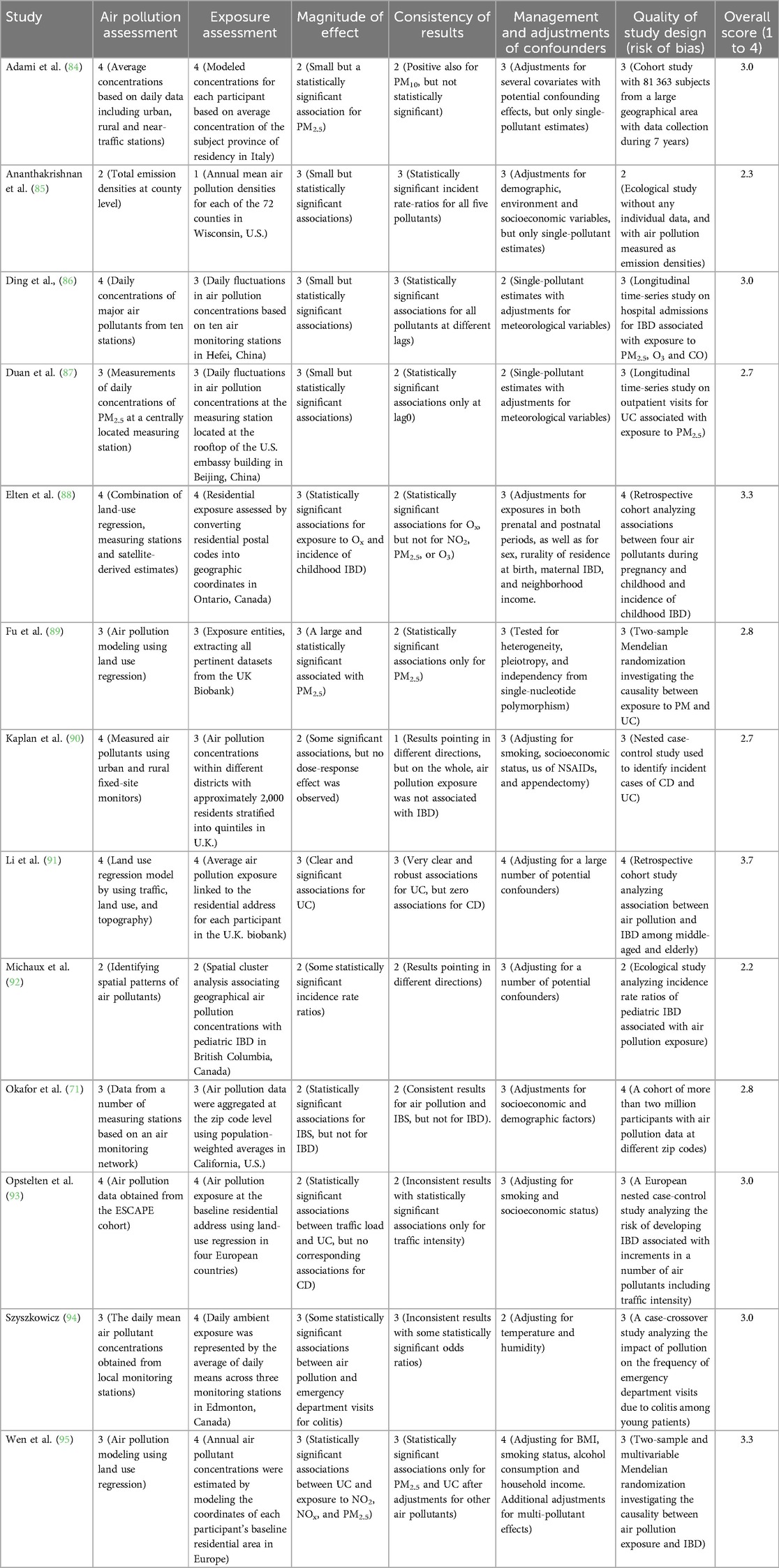
Table A2. Factors that determine the quality of evidence graded on a scale from 1 to 4 (1 = very low; 2 = low; 3 = average; and 4 = high).
Keywords: air pollutants, IBD, Crohn's disease, ulcerative colitis, disease onset, disease exacerbation, toxicology
Citation: Olstrup H, Mohamed HAS, Honoré J, Schullehner J, Sigsgaard T, Forsberg B and Oudin A (2024) Air pollution exposure and inflammatory bowel disease: a systematic literature review of epidemiological and mechanistic studies. Front. Environ. Health 3:1463016. doi: 10.3389/fenvh.2024.1463016
Received: 11 July 2024; Accepted: 6 September 2024;
Published: 20 September 2024.
Edited by:
Godfred O. Boateng, York University, CanadaReviewed by:
Yuhan Yang, Georgia Institute of Technology, United StatesGiovanni Giurdanella, Kore University of Enna, Italy
Copyright: © 2024 Olstrup, Mohamed, Honoré, Schullehner, Sigsgaard, Forsberg and Oudin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henrik Olstrup, aGVucmlrLm9sc3RydXBAdW11LnNl