 Wemboo Afiwa Halatoko1*
Wemboo Afiwa Halatoko1* Essozimna Sondou1Ghislain Emmanuel Sopoh2Amèwouga Kassegne1
Essozimna Sondou1Ghislain Emmanuel Sopoh2Amèwouga Kassegne1 Gnatoulma Katawa3Mounerou Salou4
Gnatoulma Katawa3Mounerou Salou4 Simplice Damintoti Karou5Edgard-Marius Ouendo2
Simplice Damintoti Karou5Edgard-Marius Ouendo2
- 1Laboratoire de Bactériologie, Institut National d’Hygiène, Lomé, Togo
- 2Département Santé et Environnement, Institut Régional de Santé Publique (IRSP), Université d’Abomey Calavi, Cotonou, Bénin
- 3Unité de Recherche en Immunologie et Immunomodulation (UR2IM), Université de Lomé, Lomé, Togo
- 4Facultés des Sciences de la Santé (FSS), Université de Lomé, Lomé, Togo
- 5Ecole Supérieure des Techniques Biologiques et Alimentaires (ESTBA), Université de Lomé, Lomé, Togo
Introduction: Faced with the emergence of pandemics and the omnipresence of gaps in the process of controlling elements likely to impact the implementation of biosafety and biosecurity measures, the evaluation of the related determinants becomes an urgent necessity.
Methods: The subject addressed in this study was primarily aimed at exploring the current situation of knowledge, attitudes and practices of biosafety and biosecurity as well as the associated factors in medical biology laboratories in Togo in 2021. A cross-sectional study with an analytical focus among laboratory professionals was conducted using a structured questionnaire. Statistical tests were performed using Epi Info 7.2.3.0 (2019) and Stata 13 (2013) software.
Results: Of the 322 participants, 49.1% had good knowledge while 62.4% and 77.6% had good attitudes and practices respectively. In 23.4% (25/107) of the laboratories, the staff surveyed ate their meals in the manipulation room, of which 80.0% (20/25) were in the public sector. Although the results showed that respondents who had received prior training in this area had higher score on the knowledge component (p = 0.03), this intervention had no direct effect on the attitude (p = 0.91) or practice (p = 0.84) scores. Trained participants were significantly more likely to have good knowledge. Regional disparity was noted on the knowledge and practice components and several gaps were identified.
Discussion: Biosafety and biosecurity remain a challenge in medical biology laboratories in Togo. Based on the gaps identified, training, substantial improvement of the working environment, and provision of resources to achieve optimal and sustainable biosafety and biosecurity practices in Togo are required.
Introduction
Mastering the knowledge, attitudes and practices of laboratory staff is becoming increasingly important given the growing interest in biosafety and biosecurity (BSS) in public health over the past few years (1–4). Laboratories, in addition to the ability to perform diagnostic activities, should operate around a cross-cutting human-centered system to articulate viable responses to the risks of intentional (biosecurity) or accidental (biosafety) release of biological agents (1, 5). In addition to the challenge of anchoring the culture in BSS (6), there is currently an acute problem of human resources capable of identifying, assessing, mitigating biological risks and communicating possible prevention measures (7, 8). Thus, it is crucial that every laboratory professional be familiar with the basic requirements and provisions to achieve better biohazard management, involving up-to-date knowledge, good attitudes and universal practices.
In low-income countries, the medical biology laboratories at the heart of public health surveys often operate with limited capacity and under-prioritization of BSS issues (2, 3, 9, 10). However, the problem of the human environment, reflecting the global trend, remains an element in common with developed countries. In this regard, a study conducted in 2020 in the Democratic Republic of Congo found that 91% of the laboratories surveyed were not applying basic BSS measures (11). Meanwhile, in Canada, another study noted that human interaction was the most cited root cause (24%) of laboratory acquired infections (12). Wurtz et al. in 2016, following an international survey, also noted that the underlying cause of 78% of laboratory acquired infections (LAI) was due to human error (13). The poor application of the BSS is a factor favoring LAI. A recent review of LAI identified 304 cases derived from 26 differents pathogens, and 34 cases were due to unknown pathogens (14). In addition, with regard to advances in biomedical technology, AI as ChatGPT, is of paramount importance, especially in countries in this field (15). In South Africa in 2017, a study of laboratory-acquired Salmonella typhi infections between 2012 and 2016 described three cases of LAI. According to the author, all three cases were most likely the result of breaches of Good Laboratory Practice (GLP) and laboratory safety (16). In 2018, a study by Sharp et al. in the USA corroborates this fact in that their case of dengue virus LAI was most likely due to poor glove removal practice by the infected laboratory technician (17).
Although several aspects of BSS including internal accountability systems, knowledge levels, skills of laboratory professionals and BSS practices have been addressed in developed countries, little data exists in Africa.
Recently, several studies have noted the immediate positive effect of training on the knowledge, practices and attitudes of laboratory professionals (6, 18, 19) or non-laboratory professionals (20). However, with the indispensable progress of biomedical technology, the major challenges posed by these biohazards are increasing, modulating the variety of BSS approaches (5, 21). The COVID-19 pandemic has posed many challenges justifying the particular mention made on laboratory staff training in the fourth edition of the World Health Organization (WHO) BSS manual (22).
In Africa as well as in Togo, knowledge, attitudes and practices appear to be insufficient. The present study was conducted to explore the current situation of knowledge, attitudes and practices of BSS in medical biology laboratories and the associated factors in Togo. The study aimed specifically at estimating the scores of knowledges, attitudes and practices among laboratory professionals and determining the factors associated with variations in these scores.
Materials and methods
Study design and period
A cross-sectional study with an analytical focus was conducted. It took place from June to November 2021 in medical biology laboratories throughout Togo. Togo is located in West Africa with an area of 56,600 km2. Its population was estimated at 7,886,000 in 2021 (23). The study population consisted of laboratory technicians, laboratory assistants and support staff (cleaning staff, administrative staff or secretaries) working in a quarter of all laboratories. The sampling was random in two stages: the first stage was the random selection of 25% of the medical biology laboratories (MBL) in Togo, and then in the second stage the random selection of five people per MBL (three biology technicians, one laboratory assistant, one support staff).
Variables of interest
Socio-demographic characteristics; staff knowledge of microorganism transmission routes, personal protective equipment (PPE), disinfection techniques, staff practices and attitudes regarding the wearing of PPE as well as decontamination and waste disposal procedures were studied.
Data collection technique and tools
A structured, pre-tested questionnaire was used, it took into account respondents' individual knowledge, practices and attitudes. Practices and attitudes were accessed by observation. A numerical scoring system was developed to evaluate the three groups of variables (knowledge, practices and attitudes).
Data analysis
The evaluation scores were presented as a percentage and allowed for the categorization of good mastery (score greater than or equal to 55%) and poor or no mastery of the requirements being evaluated (score less than 55%).
Data were consolidated in a 2016 Excel file, and analyzed with Epi Info 7.2.3.0 (2019) and Stata 13 (2013) software. We calculated proportions, 95% confidence intervals (95% CI), means, medians and interquartile ranges (IQR). The Chi-square test was used to compare proportions. Univariate logistic regression analysis was performed to test the association between the explained variables (BSS knowledge, attitudes, and practices) and the explanatory variables (demographic factors, BSS training, and involvement in quality management). The tests were considered statistically significant for a p-value less than 0.05.
Results
During this study, a quarter of the laboratories in Togo (n = 107) were visited. The majority (77.3%) were in the public sector and 58.9% were not involved in the quality approach. Figure 1 shows the map of the geographical distribution of the laboratories in which the survey was conducted.
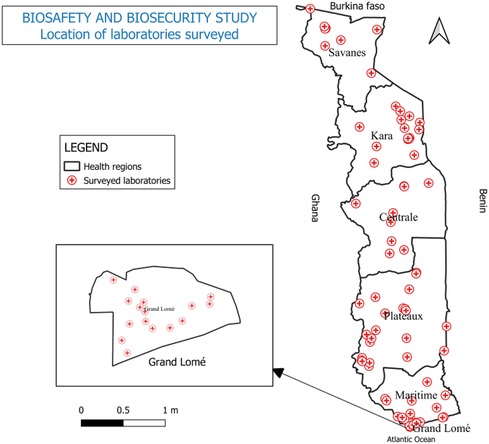
Figure 1. Map of Togo, geographical distribution of laboratories surveyed, 2021.
Socio-demographic characteristics of respondents
The response rate was 100%. A total of 322 MBL professionals participated in the survey, 75.5% of whom were biology technicians. The Grand-Lomé region and the public sector represented 72.9% (235/322) and 77.3% (249/322) respectively. A percentage of 72.9% of respondents had a higher education level (university). The male/female sex ratio was 2.93. The majority of respondents (69.9%) were between 25 and 44 years of age and 58.1% of respondents had less than 10 years of seniority (n = 187) in their job. The median age at work was 7 years (IQR = 4–13 years).
Of the 207 professionals trained in BSS, 37.7% (78) had received formal training in the classic BSS modules, i.e., 24.2% of respondents. In this group of trained staff, 78.3% (162) of respondents had received this reinforcement more than 2 years ago. Table 1 summarizes the socio-demographic information on the respondents.
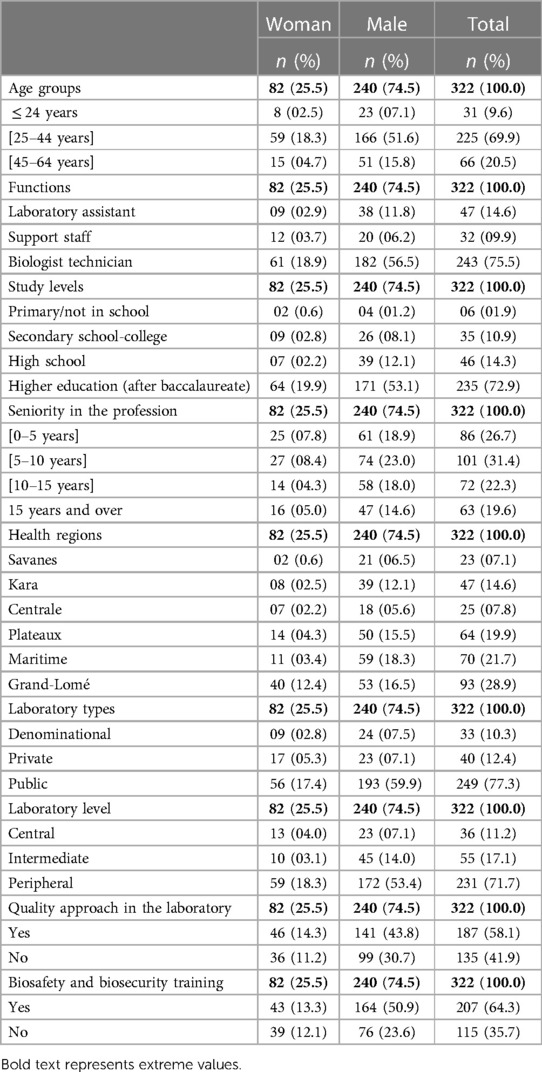
Table 1. Socio-demographic information, quality management and training in biosafety and biosecurity in laboratories, Togo, 2021.
Knowledge, attitudes and practices of laboratory staff
On the knowledge component, the scores obtained ranged from 10.0 to 95.0% with an average of 51.4% ± 16.3 (median = 50%, IQR = 40%–65%). Overall, 49.1% (158) of respondents had good knowledge (score greater than or equal to 55%). The respondents had less knowledge on the transmission routes of infectious agents, waste management and preventive measures in general.
For the attitude component, the scores ranged from 0.0% to 100.0% with an average of 68.2% ± 20.7 (median = 75%, IQR = 50%–75%). In total, 62.4% (201) of the respondents had good attitudes. The most observed bad attitude was the use of mobile phones in the manipulation room: 73.0% (235).
In terms of practice assessment, the scores ranged from 30.0 to 95.0% with an average of 63.4% ± 14.0 (median = 65%, IQR = 55%–75%). Overall, 77.6% (250) of respondents had good practices. The observation made on hand washing showed that only 3.4% (11) of responders complied with the five steps (wet, lather, scrub, rinse, dry) of hand washing with soap.
More than 41.6% (134) washed their lab coats at home and 58.1% (187) were not proficient in bleach dilution. In 23.4% (25/107) of the laboratories, the staff surveyed ate in the manipulation room, of which 80.0% (20/25) were in the public sector. Table 2 shows the frequencies of knowledge, attitude and practice scores for the items used to assess respondents.
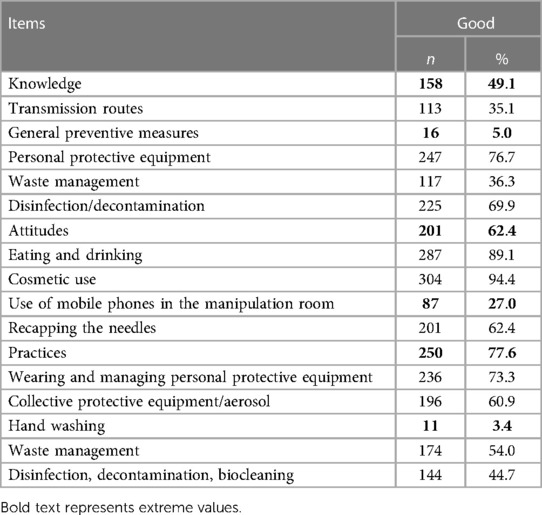
Table 2. Scores of good knowledge, attitudes and practices regarding BSS among laboratory professionals, Togo, 2021.
Scores of BSS knowledge, attitudes and practices according to selected variables among laboratory professionals
In our study, there was a significant difference in knowledge (p < 0.01) and practice (p < 0.01) scores across the regions of the country. Participants in the Central region (76.9%) had the highest scores in terms of good knowledge and Grand-Lomé, the lowest score (37.0%). In terms of good BSS practices, the Maritime region had the highest score (90.7%) and the Savanes region the lowest (47.8%).
The study also found that participants who reported having been trained in BSS had a higher good knowledge score (p = 0.03). Men who participated in the study had the highest scores on the knowledge component (p = 0.03).
Regarding good BSS practices, in addition to the variation found by regions, participants from denominational laboratories had statistically the best scores (p = 0.03) compared to public and private laboratories.
The attitude component showed no statistically significant differences in the data for the eight items, although some variations exist. In addition, it was noted that, participants with good knowledge had more mastery of good practices than those without (p = 0.03). Table 3 shows the scores of knowledge, attitudes and practices according to selected variables on BSS among laboratory professionals, Togo, 2021.
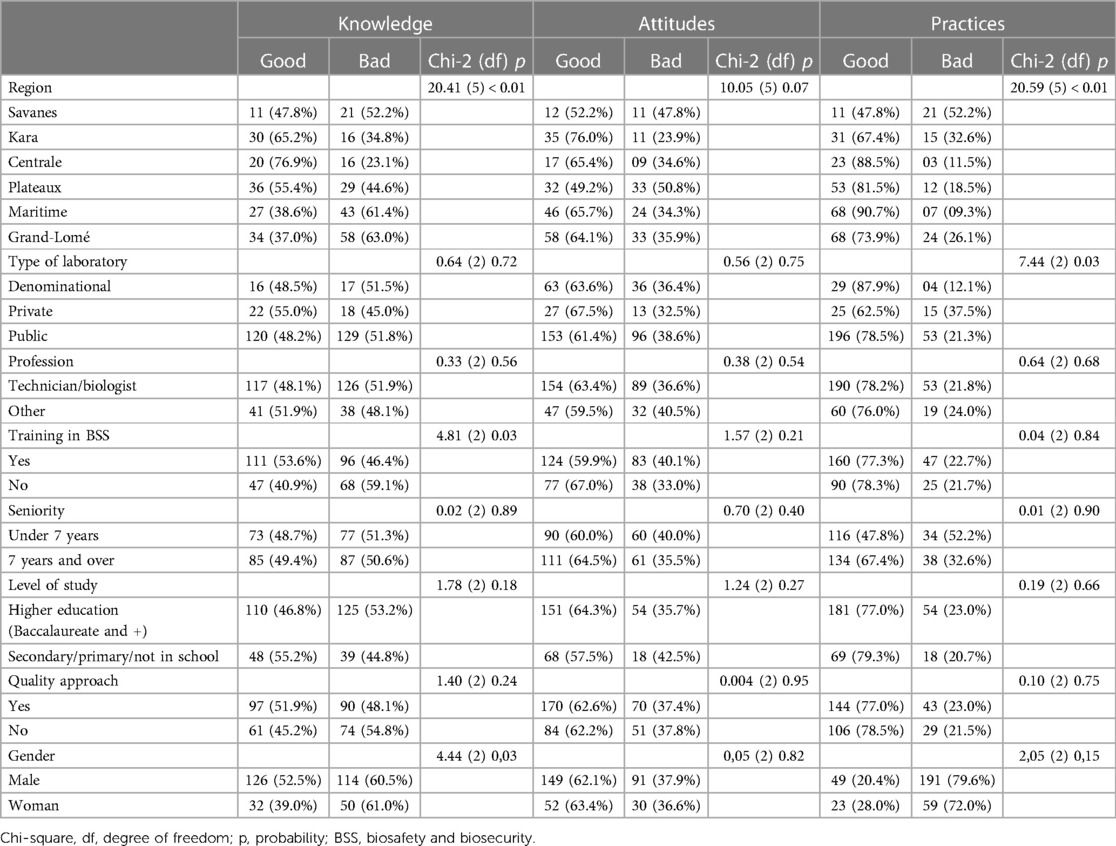
Table 3. Scores of knowledge, attitudes and practices according to selected variables on BSS among laboratory professionals, Togo, 2021.
Factors associated with good BSS knowledge, attitudes and practices in laboratories
Logistic regression in a univariate model revealed factors associated with good BSS knowledge in the laboratories. Women were less likely to have satisfactory BSS knowledge than men. PR = 0.58; CI 95% [0.35–0.96]. Laboratory professionals trained in BSS were significantly more likely to have good BSS knowledge: PR = 1.67; 95% CI [1.05–2.65]. Participants in the Grand-Lomé region were overall more likely to have lower scores in terms of BSS knowledge than the other five regions of the country with successively PR = 3.20; 95% CI [1.52–6.70] for the Kara region and PR = 5.69; 95% CI [2.08–15.55] for the Centrale region. No factor among the eight studied was associated with the right attitude. Table 4 summarizes the factors associated with good knowledge, attitudes and practice related to BSS among laboratory professionals.
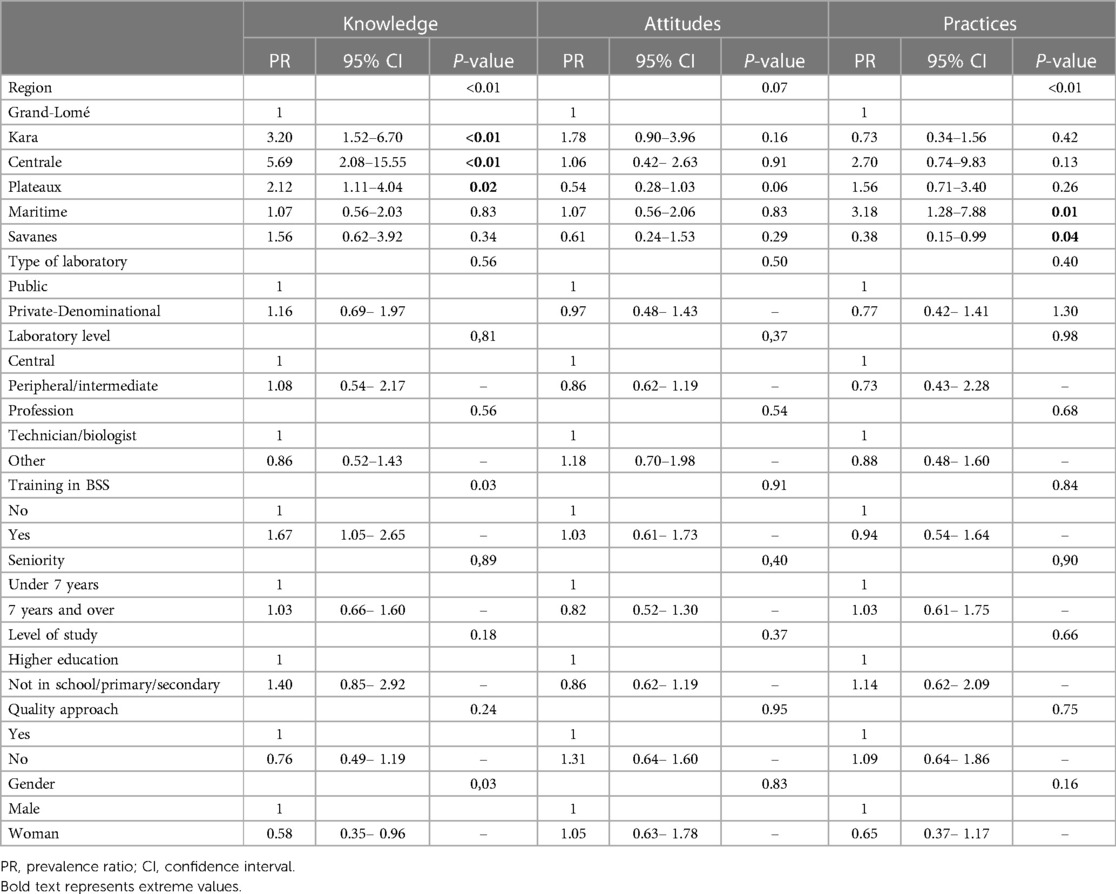
Table 4. Factors associated with knowledge, attitudes, practices related BSS among laboratory professionals, Togo, 2021.
Discussion
The study conducted aimed to assess the knowledge, attitudes and practices of BSS in laboratory at the national level in Togo in 2021 while seeking the factors associated with these three determinants.Our study, the first of its kind in Togo, covered all the country's health districts. Due to the significant variability in the composition of the staff in the laboratories, laboratory technicians were in the majority, 75% against 60% expected. Nevertheless, three important results emerge from this study. The proportion of laboratory professionals with good scores in terms of knowledge, attitudes and practices was 49.1%, 62.4% and 77.6% respectively. Some bad attitudes were identified such as the use of mobile phones (73.0%) and eating or drinking (10.9%) in the manipulating room. Respondents who had received prior training in BSS had a higher score on the knowledge component (p = 0.03). This intervention had no direct effect on the attitude (p = 0.91) or practice (p = 0.84) scores. Some associated factors were identified. Region, education and gender were associated with good knowledge. Region and type of laboratory were associated with good practice, but no factors were associated with respondents' attitudes.
Knowledge, attitudes and practices of laboratory staff
In our study 49.1% of participants had good knowledge of BSS, but Bajjou et al. (24) in Morocco in 2018 found in a similar study involving 235 participants, a higher score of 79.0% good knowledge. This difference could be explained by the study population which did not include support staff in the Moroccan study. In addition, this could be explained by the lack of updating of knowledge; 78.3% of trained respondents received this reinforcement more than 2 years ago. Ensuring the implementation of BSS when performing procedures in the laboratory depends largely on intrinsic or educational knowledge of the subject (25). Thus, in situation of poor BSS knowledge, the risks of contamination or misuse are high and the staff may be exposed to infections with inappropriate work procedures (26, 27). Several gaps were identified that affected the BSS knowledge score in our study. Essentially, these deficiencies related to issues of infectious agents’ transmission routes, waste management and infection control general measures. This would indicate a lack of initial or ongoing training for laboratory professionals.
In addition, the performance in terms of practices (77.6%) and attitudes (62.4%) in our study was acceptable even though several deficiencies were important to note. In terms of practices, biocleaning, decontamination, disinfection including hand washing and washing of lab coats at home were the main deficiencies. The proportion of laboratory professionals (58.1%) not having mastered the dilution of bleach also deserves particular attention in terms of ensuring the effectiveness of disinfection and decontamination practices in laboratories. Similarly, attitude-related deficiencies were the use of mobile phones (73.0%) including eating and drinking in the laboratory (10.9%) in 23.4% of the laboratories, most of which were in the public sector. Ngbolua in 2020 in the DRC found a rate of 58% of staff taking their meals in the laboratory (11). A progressive awareness of laboratory staff in Togo following the periodic reinforcement of skills instituted could explain this difference.
Scores of BSS knowledge, attitudes and practices according to selected variables among laboratory professionals
The infectious risk in the laboratory is ubiquitous, capacity building of laboratory professionals in BSS has been initiated in Togo since 2016. In our study, although the results noted that respondents who received prior training in BSS had a better score on the knowledge component (p = 0.03), this intervention did not have a direct effect on the attitude score (p = 0.91) nor on the practice score (p = 0.84). This could be explained by the fact that only 24.2% of respondents had received formal training, which covers many more aspects than awareness raising. Hence the importance of a comprehensive needs assessment to identify one's own gaps to be filled by training (28). This result shows that good practice in BSS depends on good knowledge, but it also depends on the organizational set-up and resources available in each laboratory.
Factors associated with good BSS knowledge, attitudes and practices in laboratories
At the national level, the study noted that participants in the Grand-Lomé region were less likely (p-value < 0.01) to have good BSS knowledge and practice scores than the other five regions of the country. No other factors were associated with practice and attitude. The variation in participants' performance from one region to another could be explained by the variability in laboratories' commitment to a quality approach associated with the proportion of participants trained in BSS. Medical laboratories are exposed to various biohazards on a daily basis. To this end, BSS is a line of defense that protects healthcare staff, the public and the environment from exposure to these biohazards. However, the perception and implementation of mitigation measures may vary from one laboratory to another (29) involving several factors. Furthermore, in our study, while no single factor among the eight studied was associated with the right attitude; some factors were associated with the right knowledge on BSS. Women were less likely to have satisfactory knowledge of BSS than men. This contrasts with Bajjou et al. in Morocco, who found no variation by gender. This could be related to the fact that the sex ratio (M/F) in the Moroccan study (0.75) was much lower than in our study (2.93) and there were more women in the laboratory assistant category.
The fact that attitude in BSS was not associated with any factor would indicate the existence of other elements that could impact on it. Some publications point out that attitude is difficult to assess by means of proficiency tests in a study participant, as his or her responses involve behavior, intention, emotion, including the cognitive aspect (6, 30). The quest for efficiency in the implementation of long-term BSS in laboratories remains an imminent need and engagement in quality programs has been noted as vital in improving safe practice (31, 32). However, in our study, participants' scores were independent of engagement in the quality process. This raises a concern about the implementation of BSS procedures that are supposed to be mastered in an established quality management system. The current health crisis that is testing the resilience of laboratories to appropriate biohazard management could be mentioned here.
Limits of the study
The study's limitation lies in the fact that the evaluation of most practices was based on questioning without observations.
Conclusion
The aim of this study which was to explore the current situation on knowledge, attitudes and practices on BSS as well as the associated factors in medical biology laboratories in 2021 in Togo was well achieved.
The study found that while lest than the half of the laboratory professionals had good knowledge of biosafety and biosecurity, overall performance in terms of attitude and practice exceeded sixty percent. In addition, gaps and barriers that negatively impacted performance were identified across the three determinants under study.
Based on these identified gaps, continuous training, substantial improvement of the working environment, and provision of the necessary resources to achieve improved or optimal biosafety and biosecurity practices in Togo are required.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
WH: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ES: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. GK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. AK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. MS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. SK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. EO: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank all the laboratory professionals, the directorate of health facilities, the laboratory division and the ministry in charge of health in Togo. We would also like to thank Ms Kpaikpai, Mr Latta and Mr Issa for their support in analyzing the data, and all the Togo regional biosafety and biosecurity referents for their active participation in the survey process.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Brizee S, Budeski K, James W, Nalabandian M, Bleijs DA, Becker SJ, et al. Accelerating action in Global Health Security: global biosecurity dialogue as a model for advancing the Global Health Security Agenda. Health Secur. (2019 ) 17(6):495–503. doi: 10.1089/hs.2019.0121
2. Berns KI. Grand challenges for biosafety and biosecurity. Front Bioeng Biotechnol. (2014) 2(35):1–3. doi: 10.3389/fbioe.2014.00035
3. Bakanidze L, Imnadze P, Perkins D. Biosafety and biosecurity as essential pillars of international health security and cross-cutting elements of biological nonproliferation. BMC Public Health. (2010) 10(Suppl 1):S12. doi: 10.1186/1471-2458-10-S1-S12
4. Munson E, Bowles EJ, Dern R, Beck E, Podzorski RP, Bateman AC, et al. Laboratory focus on improving the culture of biosafety: statewide risk assessment of clinical laboratories that process specimens for microbiologic analysis. J Clin Microbiol. (2018) 56(1):11. doi: 10.1128/JCM.01569-17
5. Li J, Zhao H, Zheng L, An W. Advances in Synthetic Biology and Biosafety Governance. Front Bioeng Biotechnol. (2021). Available online at: https://www.frontiersin.org/articles/10.3389/fbioe.2021.598087/full?utm_source=S-TWT&utm_medium=SNET&utm_campaign=ECO_FBIOE_XXXXXXXX_auto-dlvrit (cited July 21, 2021).
6. Perkins D, Danskin K, Rowe AE, Livinski AA. The culture of biosafety, biosecurity, and responsible conduct in the life sciences: a comprehensive literature review. Appl Biosaf. (2019) 24(1):34–45. doi: 10.1177/1535676018778538
7. OIT, OMS. Sécurité et santé au travail durant les crises sanitaires: Un manuel pour la protection des personnels de santé et des équipes d’intervention d’urgence. Geneva: World Health Organization (2020). p. 152.
8. Moritz RL, Berger KM, Owen BR, Gillum DR. Promoting biosecurity by professionalizing biosecurity. Science. (2020) 367(6480):856–8. doi: 10.1126/science.aba0376
9. Jacobsen KX, Mattison K, Heisz M, Fry S. Biosecurity in emerging life sciences technologies, a Canadian public health perspective. Front Public Health. (2014) 2:198. doi: 10.3389/fpubh.2014.00198
10. Heckert RA, Reed JC, Gmuender FK, Ellis M, Tonui W. International biosafety and biosecurity challenges: suggestions for developing sustainable capacity in low-resource countries. Appl Biosaf. (2011) 16(4):223–30. doi: 10.1177/153567601101600404
11. Ngbolua KTN. Connaissances et pratiques de la biosécurité dans les laboratoires cliniques de la ville de Kinshasa en République démocratique du Congo. 2020. (Editions Universitaires Européennes. ISBN: 978-620-2-53277-8.
12. Lien A, Abalos C, Atchessi N, Edjoc R, Heisz M. Surveillance des expositions en laboratoire aux agents pathogènes humains et aux toxines, Canada 2019. Relevé Mal Transm Au Can. (2020) 46(09):329–36. doi: 10.14745/ccdr.v46i09a07f
13. Wurtz N, Papa A, Hukic M, Di Caro A, Leparc-Goffart I, Leroy E, et al. Survey of laboratory-acquired infections around the world in biosafety level 3 and 4 laboratories. Eur J Clin Microbiol Infect Dis Off Publ Eur Soc Clin Microbiol. (2016) 35(8):1247–58. doi: 10.1007/s10096-016-2657-1
14. Bang E, Oh S, Chang HE, Shin IS, Park KU, Kim ES. Zika virus infection during research vaccine development: investigation of the laboratory-acquired infection via nanopore whole-genome sequencing. Front Cell Infect Microbiol. (2022) 12:819829. doi: 10.3389/fcimb.2022.819829
15. Maniaci A, Fakhry N, Chiesa-Estomba C, Lechien JR, Lavalle S. Synergizing ChatGPT and general AI for enhanced medical diagnostic processes in head and neck imaging. Eur Arch Otorhinolaryngol. (2024). doi: 10.1007/s00405-024-08511-5
16. Smith AM, Smouse SL, Tau NP, Bamford C, Moodley VM, Jacobs C, et al. Laboratory-acquired infections of Salmonella enterica serotype Typhi in South Africa: phenotypic and genotypic analysis of isolates. BMC Infect Dis. (2017) 17(1):656. doi: 10.1186/s12879-017-2757-2
17. Sharp TM, Fisher TG, Long K, Coulson G, Medina FA, Herzig C, et al. Laboratory-Acquired dengue virus infection, United States, 2018. Emerg Infect Dis. (2020) 26(7):1534. doi: 10.3201/eid2607.191598
18. Mehta A, Diwakar M. Impact of educational intervention on knowledge, attitudes, and practices of laboratory technicians regarding universal work precautions at a tertiary health care center in central India. Appl Biosaf. (2021) 26:7. doi: 10.1089/apb.21.902607
19. Muneer S, Kayani H, Ali K, Asif E, Zohra R, Kabir F. Laboratory biosafety and biosecurity related education in Pakistan: engaging students through the socratic method of learning. J Biosaf Biosecurity. (2021) 3:22–7. doi: 10.1016/j.jobb.2021.03.003
20. Emery RJ, Rios J, Patlovich SJ. Thinking outside the box: biosafety’s role in protecting non-laboratory workers from exposure to infectious disease. Appl Biosaf J Am Biol Saf Assoc. (2015) 20(3):128–9. doi: 10.1177/153567601502000301
21. Kojima K, Booth CM, Summermatter K, Bennett A, Heisz M, Blacksell SD, et al. Risk-based reboot for global lab biosafety. Science. (2018) 360(6386):260–2. doi: 10.1126/science.aar2231
22. Organization WH. Laboratory biosafety manual. World Health Organization. (2020). Available online at: https://apps.who.int/iris/handle/10665/337956 (cited June 19, 2021).
23. National Institute of Statistics, Economic Studies and Demographics of TOGO (INSEED). INSEED—Institut National de la Statistique et des Etudes Économiques et Démographiques. (2023). Available online at: https://inseed.tg/ (cited May 9, 2023).
24. Bajjou T, Sekhsokh Y, Amine IL, Gentry-Weeks C. Knowledge of biosafety among workers in private and public clinical and research laboratories in Morocco. Appl Biosaf. (2018) 24:9. doi: 10.1177/15356760187971
25. ISO 15190:2020. Medical laboratories — Requirements for safety. Available online at: https://www.iso.org/cms/render/live/fr/sites/isoorg/contents/data/standard/07/21/72191.html (cited December 22, 2020).
26. Kirunda H, Otimonapa M. Low level of awareness in biosafety and biosecurity among professionals in Uganda: a potential risk in the dual-use dilemma. J Bioterrorism Biodefense. (2014) 5(1):10. doi: 10.4172/2157-2526.1000128
27. Castriciones EV, Vijayan V. Biosecurity risk mapping and gap analysis in South East Asia. J Biosaf Biosecurity. (2020) 2(1):36–43. doi: 10.1016/j.jobb.2020.03.001
28. Rutebemberwa E, Aku FY, Zein EIKA, Bellali H. Reasons for and barriers to biosafety and biosecurity training in health-related organizations in Africa, Middle East and Central Asia: findings from GIBACHT training needs assessments 2018–2019. Pan Afr Med J. (2020) 37:64. doi: 10.11604/pamj.2020.37.64.23390
29. Li N, Hu L, Jin A, Li J. Biosafety laboratory risk assessment. J Biosaf Biosecurity. (2019) 1(2):90–2. doi: 10.1016/j.jobb.2019.01.011
30. Sanchez A, Gabrie J, Zelaya AA, Enriquez L, Canales M, Kaufman SG. Biosafety competencies in developing countries: the role of universities. J ABSA Int. (2011) 16:13. doi: 10.1177/153567601101600406
31. Giménez-Marín A, Rivas-Ruiz F, García-Raja AM, Venta-Obaya R, Fusté-Ventosa M, Caballé-Martín I, et al. Assessment of patient safety culture in clinical laboratories in the Spanish National Health System. Biochem Medica. (2015) 25(3):363–76. doi: 10.11613/BM.2015.036
Keywords: biosecurity, knowledge, attitudes, practices, associated factors, medical laboratory, biosafety
Citation: Halatoko WA, Sondou E, Sopoh GE, Kassegne A, Katawa G, Salou M, Karou SD and Ouendo E-M (2024) Knowledge, attitudes and practices in biosafety and biosecurity in medical biology laboratories in Togo, 2021. Front. Environ. Health 3:1387476. doi: 10.3389/fenvh.2024.1387476
Received: 17 February 2024; Accepted: 26 March 2024;
Published: 16 April 2024.
Edited by:
Antonino Maniaci, Kore University of Enna, ItalyReviewed by:
Salvatore Lavalle, San Raffaele Hospital (IRCCS), ItalyTiziana Nicosia, University of Catania, Italy
© 2024 Halatoko, Sondou, Sopoh, Kassegne, Katawa, Salou, Karou and Ouendo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wemboo Afiwa Halatoko aGphY2t5NzhAeWFob28uZnI=
Abbreviations BSS, biosafety and biosecurity; MBL, medical biology laboratories.