 William Brett Perkison1*
William Brett Perkison1* Ross Shegog2
Ross Shegog2 Dejian Lai3
Dejian Lai3 Saswati Upadhyay1
Saswati Upadhyay1 Geethika Yalavarthy4
Geethika Yalavarthy4 Rosalia Guerrero-Luera5
Rosalia Guerrero-Luera5 Patenne D. Mathews2
Patenne D. Mathews2 Janelle Rios1Ritesh Mehta1Jeffery McLaughlin6
Janelle Rios1Ritesh Mehta1Jeffery McLaughlin6 Ismail Nabeel7
Ismail Nabeel7
- 1Department of Environmental Health Sciences, University of Texas School of Public Health, Houston, TX, United States
- 2Department of Health Promotion, University of Texas School of Public Health, Houston, TX, United States
- 3Department of Epidemiology, Human Genetics, and Environmental Sciences, University of Texas School of Public Health, Houston, TX, United States
- 4Department of Epidemiology, University of Texas School of Public Health, Houston, TX, United States
- 5Department of Management, Policy, and Community Health, University of Texas School of Public Health, Houston, TX, United States
- 6Radiant Digital, Vienna, VA, United States
- 7Department of Environmental Medicine and Public Health, Icahn School of Medicine, New York, NY, United States
Background: The health and safety of workers who work in areas severely damaged by natural weather events (reconstruction workers) is becoming an increasingly important health problem as these disasters increase in intensity and frequency. An evidence-based, innovative e-learning tool, Pocket Ark, has been developed to meet this need.
Methods: Intervention Mapping, an iterative public health programming methodology, was used to create strategies designed to support the development and implementation of the Pocket Ark application for the health and safety of reconstruction workers before, after, and during natural disasters.
Discussion: The development of an evidence-based application, Pocket Ark, uses the concept of the Intervention Mapping planning framework. It can be an effective bridge of pre-deployment education, deployment health, and safety support for the reconstruction work in the immediate post-disaster environment.
1 Introduction
As the effects of climate change intensify, more frequent and intense meteorological events are being observed worldwide, including heat waves, drought, wildfires, and flooding events related to heavier rainfall, rising sea levels, and intensifying storm activity (1–3).
Flooding damage includes the widespread destruction of communities, including homes, commercial buildings, and public facilities (e.g., hospitals, schools), as well as infrastructure (e.g., transport facilities such as roads, railways, bridges, and ports) and water, sewage, and energy supply lines (4). In the aftermath of these events, construction workers traveling to rebuild these communities may face numerous hazards and receive the most intense exposures (5). The term reconstruction worker applies to a construction worker who is involved in the process of rebuilding structures destroyed due to extreme weather events (6, 7). There are numerous hazards associated with reconstruction, including waterborne infectious diseases (8, 9), respiratory irritants (removing sheetrock) and allergens (excessive mold growth) (10, 11), and mental health exacerbations (12).
Disaster response reconstruction workers are typically given little to no relevant safety education or adequate protective barriers (13). In one study, 85% of reconstruction workers working in the post-Hurricane Harvey Houston, TX, community reported that they had not received any safety training prior to beginning work (13). Furthermore, workers are often composed largely of immigrant populations, some are undocumented with only minimal English proficiency (14–16). As a result, this population is highly vulnerable to wage theft and job site abandonment, as well as working in unsafe worksites with few supplies, logistical coordination, and poor means of remote communication with supervisors (17–19).
Various governmental organizations have set guidelines for worker safety during natural disaster events. The National Institute for Occupational Safety and Health (NIOSH) has information on helping employers and workers to prepare in advance for anticipated response activities and to prevent work-related injuries and illnesses in the field once rescue, recovery, and clean-up begin (20). Occupational Safety and Health Administration (OSHA) has a matrix e-tool to help with worker safety (21). However, these guidelines often do not reach workers, who often do not know that they exist due to a lack of dissemination to both employers and employees. Moreover, these tools are useful but are not specific to the local hazards workers encounter, are often at too high a literacy level for some workers, and do not include worker security. They are also only useful in the pre-deployment setting, as there is no dynamic input of logistical information related to the post-flood environment.
e-Health tools have been used to successfully promote health guidelines in a variety of fields, including healthcare (22, 23), food, service, and a variety of manufacturing fields (24), including assisting reconstruction worker populations (25). These digital tools hold promise in facilitating training, decision support, and reach for these populations. Although OSHA has published a small number of e-learning tools on their website, there is still a need for tools that reach workers on a large scale (21). The e-learning platform Pocket Ark (PA) was developed to meet the ever-growing needs of the vulnerable population of construction workers who specialize in helping to repair buildings in communities that have been extensively damaged by flooding and storms. This study's purpose was to describe the development of PA, a decision support and training tool informed by stakeholder feedback and pilot tested with reconstruction workers for acceptability and feasibility. Professional reconstruction workers in this context refer to those who regularly conduct reconstruction work as their primary source of income. Reconstruction work refers to the initial stages of clean-up and repair of structures in the aftermath of a natural or manmade disaster for a large area. For this pilot study, day laborers of varying skill levels are the category of interest, and skilled craftspeople, including carpenters and electricians, were not specifically recruited for pilot testing (26).
2 Methods
2.1 Intervention Mapping
Intervention Mapping (IM) is a systematic approach to planning theory- and evidence-based health promotion interventions (27). A recent systematic review demonstrated a significant increase in the uptake of disease prevention behaviors associated with IM-based interventions when compared to placebo control groups (28). IM has been used to develop interventions for preventing cancer, including skin (29), lung (30), breast (31), and cervical (31–34) cancers. However, few applications of IM have been reported in the context of developing an e-health systems-based intervention targeting construction workers who work in areas affected by disasters and their coordinating organizations for greater efficiency and precision in disaster relief. The six steps of IM (Table 1) are to (1) assess needs and develop a logic model of the problem; (2) develop matrices of behavioral change objectives for the program; (3) identify theory-based methods and practical applications to be applied in the program; (4) produce program components and materials; (5) plan for program adoption, implementation, and sustainability; and (6) plan for evaluation (27). This project was approved by The University of Texas Health Science Center at Houston Institutional Review Board (HSC-SPH-19-0571).
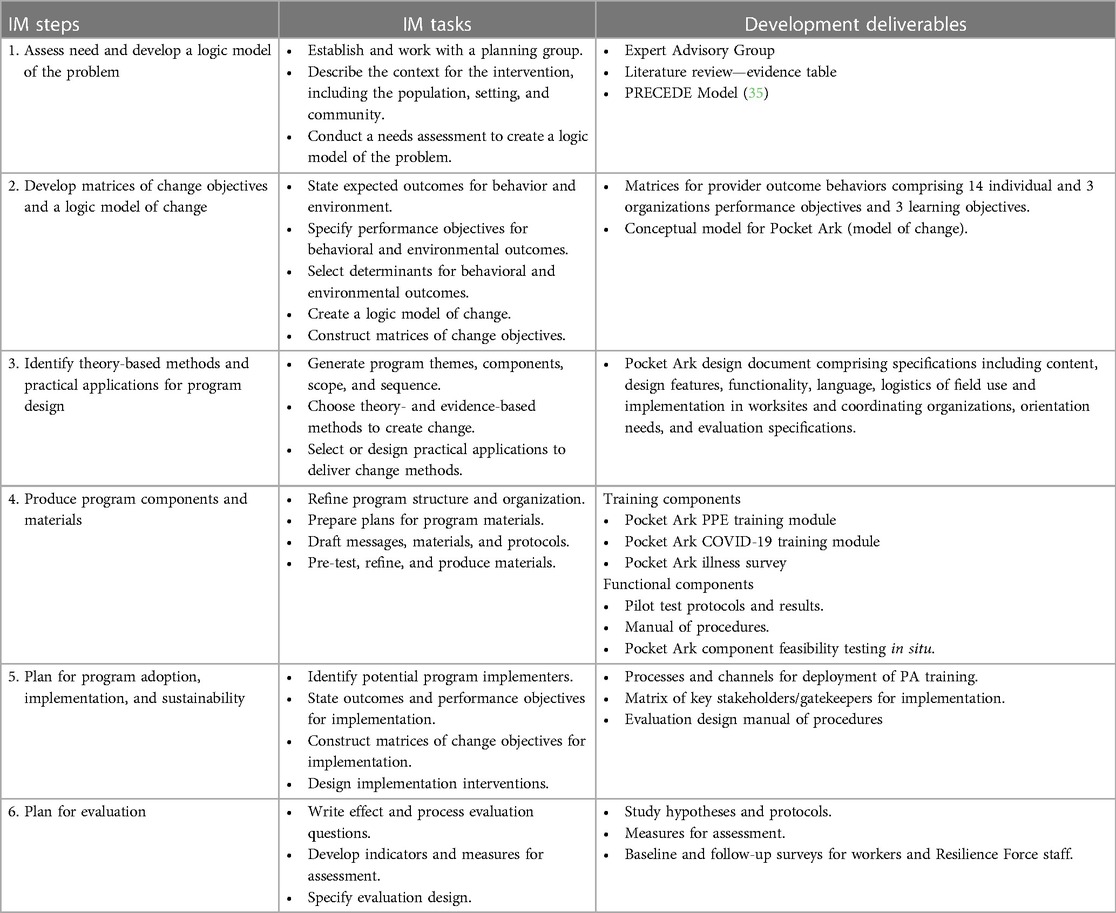
Table 1. IM steps with associated tasks and deliverables.
2.2 The development timeline
Completing the IM development process encompassed 2 years of activities (Table 1). Year 1 involved the development of the logic model of the problem (IM Step 1), defining program outcomes and objectives and matrices of change (IM Step 2), and developing the PA design document (IM Step 3). Year 2 involved completing the full program prototype, including development cycles for each component, followed by a formative evaluation with pilot testing of the components (IM step 4). Plans for implementation and evaluation (IM Steps 5 and 6) were consolidated during PA formative testing.
3 IM Step 1: logic model of the problem
Step 1 comprised the following: establishing a planning group; conducting a needs assessment informed by the PRECEDE (Predisposing, Reinforcing and Enabling Constructs in Educational Diagnosis and Evaluation) planning model that outlines the factors associated with the problem (35); defining the context of the intervention in terms of population, setting, and community; and starting to implement program goals (27).
3.1 Task 1.1: establish and work with a planning group
3.1.1 Priority population and setting
3.1.1.1 Organization description
The PA development involved close collaboration with multiple worker advocacy (WA) groups. The primary partners were Fe y Justicia and Resilience Force (RF). Fe y Justicia has seven full-time staff members and is based in Houston, TX. They provide reconstruction worker advocacy for the day laborers in over 40 different day laborer pickup sites in the Harris County area, distributing health and safety information, legal assistance, and worker advocacy leadership (WAL) training. RF has 11 full-time staff based out of New Orleans, LA. They have a similar mission as Fey y Justicia but are national in scope and focus specifically on those workers who go to work in areas affected by natural disasters, including fire and flooding.
3.1.1.2 Day laborer description
Reconstruction workers are typically also day laborers. These day laborers are the intended users of PA. Their demographic profile and the organizational structure in which they operate differ depending on the geographic location within the United States (US). A recent survey of day laborers in Texas found that these workers were predominantly male, had a mean age of 43 years, and that more recent immigrants to the US from Central and South America have lower literacy levels and were often more unskilled in the construction trade (36). Based on numerous interviews with day laborers in the Houston and New Orleans areas, it was found that more recent arrivals to the US are more susceptible to wage theft and poor treatment, such as being dropped off at remote worksites without adequate food, water, shelter, or transportation. There are many day laborers in the Houston area and many informal pickup sites for them. Given this availability, reconstruction contractors have an advantage in dictating the terms of the labor contract and determining the conditions of health and safety while still recruiting the required number of workers they need. In other urban areas with smaller populations, such as New Orleans, LA, discussions with workers indicated there are few workers in the area with fewer pickup sites. Workers in these locations are less in number, have been in the area longer, are more skilled, and can negotiate better terms with employers, such as being paid on a regular basis and working in safer conditions. Workers in these environments are also more organized in informal hierarchies, where experienced workers can advise younger workers on the validity and hazards of a particular job or location (36, 37).
Day laborers in Houston were recruited to participate in needs assessment interviews and prototype testing. These individuals were all male, all day laborers, and all of Central and South American origin. Specific demographic information was not collected with this first pilot test. This was primarily due to the fact that we recruited directly from an informal job hiring site where historically many of the workers are reluctant to relay personal information to any previously unknown organization gathering data. Future usability and utility studies using PA will help workers feel more secure as we have developed a close alliance with trusted worker advocacy organizations.
3.1.2 Stakeholder advisory committee
The IM process recommends the identification of key stakeholders, including experts, community members, potential implementers, leaders, and members of the population of interest to form a planning group that guides the intervention development (27). The PA stakeholder advisory committee (SAC) was comprised of subject matter experts from universities, individuals from the NIOSH, local county disaster preparedness groups, and worker advocacy groups. The project team held regular weekly in-person meetings through the entire IM process to plan and design components (including reviewing content, assessing functionality, flow, and the “look and feel” of PA components), develop plans for seamless implementation (rollout) without disruption to standard operating procedures, and plan for evaluation activities. Representatives from organizations vested in worker safety, including the Texas A&M Department of Construction Science, the National Institute of Occupational Safety and Health Department of Construction Safety, the National Institute of Health Prevention, Preparedness and Response Consortium, the Harris County Health Department, and the Worker's Defense Project, provided formative expert opinions in a series of stakeholder interviews (Appendix I).
3.2 Task 1.2: conduct a needs assessment to create a logic model of the problem
Previous work by this research team extensively involved an outreach project to assist residents and professional reconstruction workers in the immediate aftermath of Hurricane Harvey. Rescue kits, which included gloves, masks, and education sheets, were passed out at numerous distribution sites throughout the Houston metroplex. Six months afterward, recipients of these kits were surveyed regarding their current health, the usefulness of the kits, and the state of repair of their flood-damaged homes. Details of these results can be reviewed in previously published literature (19). Based on this experience, the research team was able to develop a needs assessment that identified (1) health and safety problems associated with construction work in recently flooded areas; (2) reconstruction worker barriers to education and training to prevent these problems from occurring to inform a logic model for health education; (3) perceived barriers, attitudes, beliefs, and needs regarding health and safety problems in the post-flood environment; and (4) current national best practices regarding health and safety strategies for creating a safe environment for post-flood reconstruction work.
3.2.1 Literature review
Conducted from 2017 to 2019, the literature review provided background on (1) health effects common to construction workers in post-flood environments, (2) current rates of injury and morbidity burden on construction workers in these environments, and (3) evidence-based strategies to increase risk reduction behaviors and organizational, behavioral, and psychosocial factors associated with their implementation. The term “reconstruction worker” has been introduced recently in the disaster recovery industry; hence, most literature reviews mention construction workers. Inclusion criteria comprised articles published in peer-reviewed journals, including review articles and surveys, and practice guidelines. Abstracts, poster presentations, and editorial publications were excluded. Electronic publication databases comprised PubMed, EMBASE, and MEDLINE.
OSHA and FEMA (Federal Emergency Management Agency) worker safety guidelines provided a systematic review of the effectiveness of health promotion strategies foundational for this study. The literature review provided information on national worker safety recommendations to prevent worksite injury and organizational factors in worksites that facilitate the operationalization of guidelines. Other actors that affect worker decision-making and motivation to adopt safety recommendations were also identified. Critical findings that informed PA are provided in Table 2.
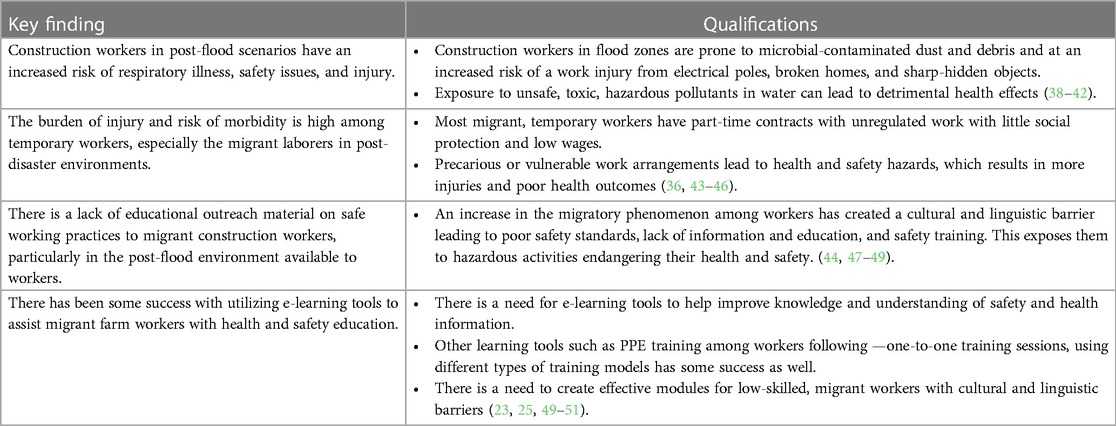
Table 2. Literature review key findings.
The literature review further informed the theoretical foundation for PA. The Conceptual Framework for Organizational Innovation Adoption (CFOIA) integrates research on innovation and technology acceptance (52). It provides a framework to understand factors that influence the adoption and implementation of innovations such as PA at individual (personal disposition, attitudes, and social usage) and organizational (supplier, network, environmental, adopter characteristic) levels. The CFOIA informs the critical determinants of adoption and implementation used to design a PA prototype with an eye to seamless adoption and implementation (Figure 1). This figure illustrates both the organizational (RF) and the individual (reconstruction worker) factors that affect the adoption of PA and how the two relate to each other. In this model, the initial adoption is driven initially at the organizational level. RF currently has a developed informal infrastructure in place to disseminate health and safety information to reconstruction workers. For PA to be adopted by this organization and synergize current protocols, the organization needs to be made aware of how the program can be integrated into existing networks of communication (social networks), meet the increasing demand for skilled reconstruction workers (environmental influences), and meet the demands of the growing organization of RF (adopted characteristics). These characteristics, along with the supplier marketing efforts are unique to this specialized subset of worker advocacy organizations. These factors can increase the potential benefits that RF will obtain from adopting the PA. The adoption and promotion of PA by RF, in turn, plays a significant role in the adoption by the individual worker, due to an extensive prior history of the build-up of trust that the worker has for the organization over the years. However, it is also important to customize the features of PA to the needs of workers regarding literacy level, cultural resonance with the largely Hispanic immigrant population, and, most importantly, how useful the e-learning tool is to the worker over existing tools such as WhatsApp. All these factors are important for the widespread adoption of PA by the reconstruction worker community.

Figure 1. Individual and organizational component diagram for the conceptual framework for organizational innovation adoption.
3.2.2 Interviews with stakeholders in partnering organizations
For additional information about the needs assessment, a series of interviews were conducted with site leaders, managers, and representatives from worker health and safety organizations, the partnering organizations previously described. Information was obtained on current best practices and protocols, suggested strategies to impact worker safety preparedness, the acceptability and utility of the PA concept, facilitators and barriers to implementing PA in the field, and consideration of critical factors to consider in PA development in terms of design and implementation.
3.2.3 Review of PA concept
The PA concept was vetted in interviews and review meetings in numerous private, federal, and academic organizations. One of the collaborating partners for the project, Fe y Justicia, provided an initial review of the PA concept, including concepts for (1) user login interface, (2) demographic information, (3) a health and safety course on personal protective equipment (PPE), and (4) post-course testing. PA staff met with this organization's field staff, managers, and executive director to review the initial prototype. This PA concept was well received with recommendations for design, including (1) educational material needed to be available in both Spanish and English, (2) material needed to be written at a third-grade education level, and (3) security information regarding work location and agreed on wages needed to be included as a key feature of the program. These barriers to a safe working environment that informed PA development are provided in Table 3.
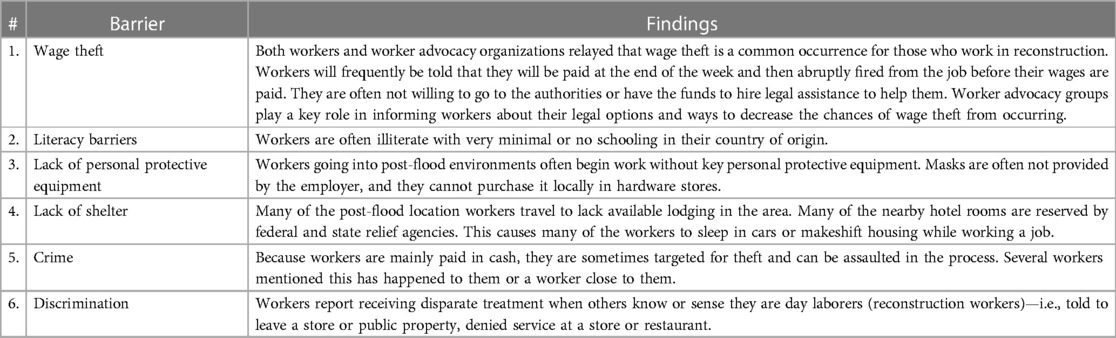
Table 3. Interview key findings.
3.3 Task 1.3: describe the context for the intervention, including the population, setting, and community
PA was developed for implementation in organizations that coordinate the initial group of construction workers that help repair a community damaged by natural disasters. The partner organization provided an ideal representation of this type of organization in terms of size, location, experience, and participant demographics. The worker population (demographics, insurance status) provided an excellent testbed for development. The priority environmental focus was the reconstruction worker advocacy organization. Federal guidelines regarding worker safety provided authority documents that informed the organization's training operations. While federal representatives were interviewed in the early stages of the design, the application of PA in a broader community context was outside the scope of the project.
3.4 Task 1.4: state program goals
The goal of the PA was to apply digital decision support to enable reconstruction workers and their coordinating organizations to meet national metrics for efficacy in worker safety training to minimize worker risk during disaster response. Respective individual worker and coordinating organization goals for PA included the following:
(a) Reconstruction workers exposed to PA training will show much greater declarative and procedural knowledge about worker safety practices.
(b) Reconstruction workers exposed to PA training will demonstrate significantly greater behavioral capability to perform work safely.
(c) Reconstruction workers will be able to access food, lodging, and personal and work-related supplies more easily while working in a recent natural disaster site.
(d) Field staff for worker advocacy groups for reconstruction workers that adopt and implement PA will rate PA as providing relative advantage over current practice (i.e., more acceptable, utilitarian, efficacious, and feasible) in worker safety training and management of workers.
The first goal was measured in the initial pilot, and subsequent testing is planned to include measuring outcomes of the additional goals.
4 IM Step 2: program outcomes and objectives—logic model of change
Step 2 comprised the following: identification of expected outcomes, performance objectives, and determinants of the behavior and environment; the development of matrices of change objectives; and the construction of a logic model of change for PA (53). This step enabled the triangulation of data obtained in Step 1 (from theory, empirical findings, and participant involvement) to inform a logic model of change. Specific technical information regarding worker's personal protective equipment, wage protection, and safety features were produced for PA's educational modules based on the identified needs derived from these from these tables. This technical information will be discussed in detail in subsequent publications.
4.1 Task 2.1: state expected outcomes for behavior and environment
4.1.1 Expected individual behavioral outcomes
Expected individual outcomes included the worker's ability to select the proper PPE for a given health hazard (OE.1); being able to properly don, wear, and replace PPE at work (OE.2); being able to practice safe respiratory-borne infectious disease practices at work (OE.3–7); improved ability to be able to contact information to a WA group (OE.8); ability to provide medical screening information to PA (OE.9); improved ability to contact the WA group for advice (OE.10); ability to use PA to successfully procure resources (OE.11); and ability to successfully negotiate a predetermined wage according to schedule (Table 4).
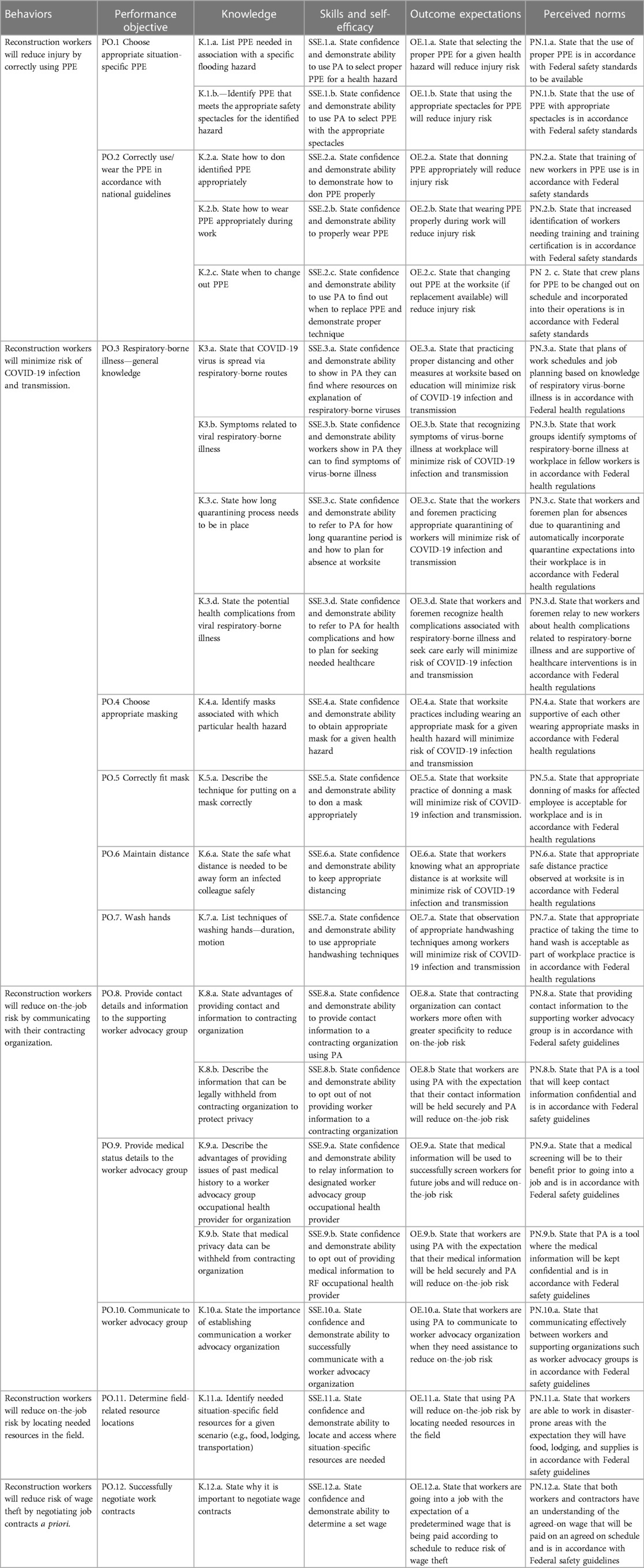
Table 4. Individual performance objectives and matrices of change objectives.
4.1.2 Expected environmental outcomes
Expected environmental outcomes included the WA group use PA to communicate most of their educational information to workers (OE.1a–b), an improvement in pre- and post-scores after completing the education section (OE.1c), and a reduction in worksite injury and illness rates (OE.1d). Outcomes also include WA group adopting evidence-based worker safety guidelines and training as usual practice. Expected behavioral outcomes include the ability of the (WA) group to use PA to communicate their logistical-related deployment information to workers (OE.2a–c). Finally, the WA group will also use PA as a tool for organizing their field staff during a disaster (OE3a–c) (Table 5).

Table 5. Organizational performance objective.
4.2 Task 2.2: specify performance objectives for health-promoting behavior and environmental outcomes
Individual performance objectives related to two domains of pre-deployment education and deployment logistical worker support. For pre-deployment information, the reconstruction worker was expected to choose situation-specific PPE (PO.1), correctly use/wear PPE in accordance with national guidelines (PO.2), have general knowledge of respiratory-borne illness prevention (PO.3), choosing appropriate masking to protect against a specific health hazard (PO.4), correctly fitting masks when wearing (PO.5), maintain distance to prevent respiratory-borne illness (PO.6), and appropriately washing hands to prevent infectious disease (PO.7). For deployment logistics, the reconstruction worker was expected to provide contact details to the WA group (PO.8), provide medical status details to the WA group (PO.9), use PA to help communicate with the WA group (PO.10), determine field-related resource location (PO.11), and successfully negotiate work contracts (PO.13) (Table 4).
Organizational performance objectives included the ability of the WA group to communicate disaster pre-deployment knowledge to workers (PO1), the ability of WA group to communicate disaster deployment logistics (locations of food, lodging, supplies) to workers in the field (PO2), and the ability of the WA group to aggregate and analyze worker input to better refine their logistical coordination and prepare for future deployments (PO3) (Table 5).
4.3 Task 2.3: select determinants for behavioral and environmental outcomes
The IM process asks researchers to consult the literature on the target behavior to identify ideas and constructs that closely align with health promotion theory constructs to devise determinants of the target behavior (54). Findings from the empirical literature, relevant theory [i.e., CFOIA, Social Cognitive Theory (SCT), Theory of Reasoned Action (TRA), Health Belief Model (HBM)], and prior formative research (Task 1.2 above) informed the selection of behavioral determinants (52, 55–58). These comprised declarative and procedural knowledge, self-efficacy, outcome expectations, skills, and normative beliefs as important and changeable for workers to perform PA-related performance objectives (Tables 4, 5). Additional determinants for organizational managers to adopt PA included perceptions of PA as providing relative advantage across usability, feasibility, and efficacy parameters. Table 7 concretely ties the theoretical constructs (RA, SCT, and HBM) to specific tasks of workers.
Reasoned Action—takes into consideration behavioral capability and normative perceptions in intention to act. Comparison to opinions and practices of significant others (peer workers, exemplary workers), organizational norms and expectations, national guidelines can provide this type of comparison (57).
Social Cognitive Theory—skills and self-efficacy are necessary to successfully perform. Drill and practice and reinforcing successive approximations to the goal behavior, goal-based behavior, and assessment of behavioral accountability emanate from SCT (56).
Health Belief Model—perceived susceptibility to risk and perceived severity of the risk motivate health/risk reduction behavior (58).
CFOIA—important for considering the adoption and implementation of technology from organizational and employer perspectives (52).
This was used to inform the elements of adoption. It comes into play in assessing usability and feasibility, which makes the PA innovation appealing (52).
4.4 Task 2.4: construct matrices of change objectives
Matrices were developed that cross-referenced behavioral performance objectives with psychosocial determinants to produce change objectives (Tables 4, 5). The resulting cells of each matrix contained change objectives. Objectives were divided into knowledge, skills and self-efficacy, outcome expectations, and perceived norms. Change objectives describe the criteria for which a specific determinant (e.g., self-efficacy) could positively influence a specific performance objective.
4.5 Task 2.5: create a logic model of change
The resultant logic model provided an encapsulated understanding of the functional components required by the PA to impact worker behaviors (Figure 2).
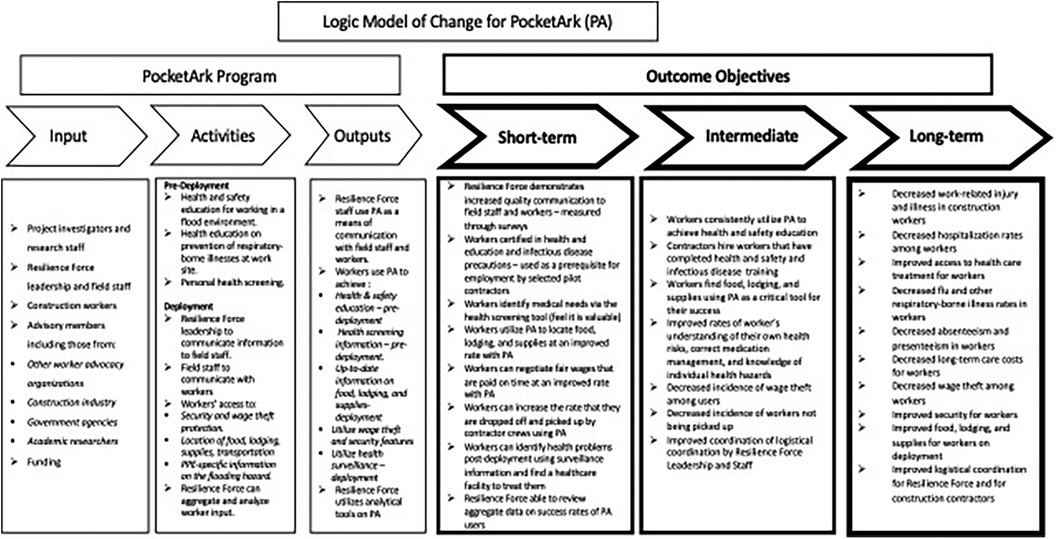
Figure 2. Logic model of change for Pocket Ark (PA).
5 IM Step 3: program plan
Step 3 comprised the following: the generation of the PA's scope and sequence, the choice of theory- and evidence-based methods, and the design of practical applications to deliver change methods. Step 3 tasks were informed by evidence tables constructed in Step 1 and from the research team's collective academic and field experience. Regular planning group meetings and brainstorming informed the PA plan.
5.1 Task 3.1: generate program themes, components, scope, and sequence
The theoretical framework for the PA is based on the Social Cognitive Theory (56), the Theory of Reasoned Action (57), the Health Belief Model (58), clinical guidelines for workers and COVID-19 safety (59), and the empirical evidence drawn from the review of literature on evidence-based strategies to increase worker safety. The development challenge was to meet both the contracting agency management and reconstruction worker needs in a format for easy institutionalization within the organizational context. At the time of program planning and pilot testing, COVID-19 was a Centers for Disease Control and Prevention (CDC) Public Health Emergency, so aspects of COVID-19 prevention were planned and included to accommodate the pandemic. These guidelines are applicable to any respiratory-borne infectious disease and could be modified to prevent outbreaks of other novel and common viruses.
5.1.1 Components
Intervention components comprised the following: worker profile and contact record, medical screening, post-flood health and safety training, COVID-19 health training, e-learning modules, and security features (Figure 2). Design documents and schematics were produced by the project team, reviewed by stakeholders, and piloted with reconstruction workers prior to implementation (detailed in Task 4.4 below).
5.1.2 Scope
PA scope was defined by evidence-based strategies shown to be efficacious in increasing worker safety training and protocols in worksites. Expert and end-user interviews (described previously) and observation of contractor organizational workflow suggested the scope and sequence of the PA functions and rollout (Figure 2) and are described in detail in Step 4 below.
5.1.3 Theme
PA was designed to complement the existing training and coordination protocols. The title, “Pocket Ark,” encompasses the underlying tenet of a safety resource in the event of a flood and carrying that safety resource (that expertise) “in your pocket.”
5.2 Task 3.2: choose theory- and evidence-based change methods
5.2.1 Individual behaviors
Theoretically and empirically based methods varied for each PA component. Methods included self-evaluation and assessment of medical history, information transfer on PPE and COVID-19 protocols, feedback and reinforcement on procedural knowledge simulation, advance organizers and real-time cues for in-field application, simulation to assess skills for selection of context-specific PPE and optimal use, role modeling, resource linkage using geolocation in the field, and social support through communication and technical support with the coordinating contracting agency (Table 6). The project team selected methods based on empirical evidence for their use to impact the target determinants (53) (Tables 1 and 2).
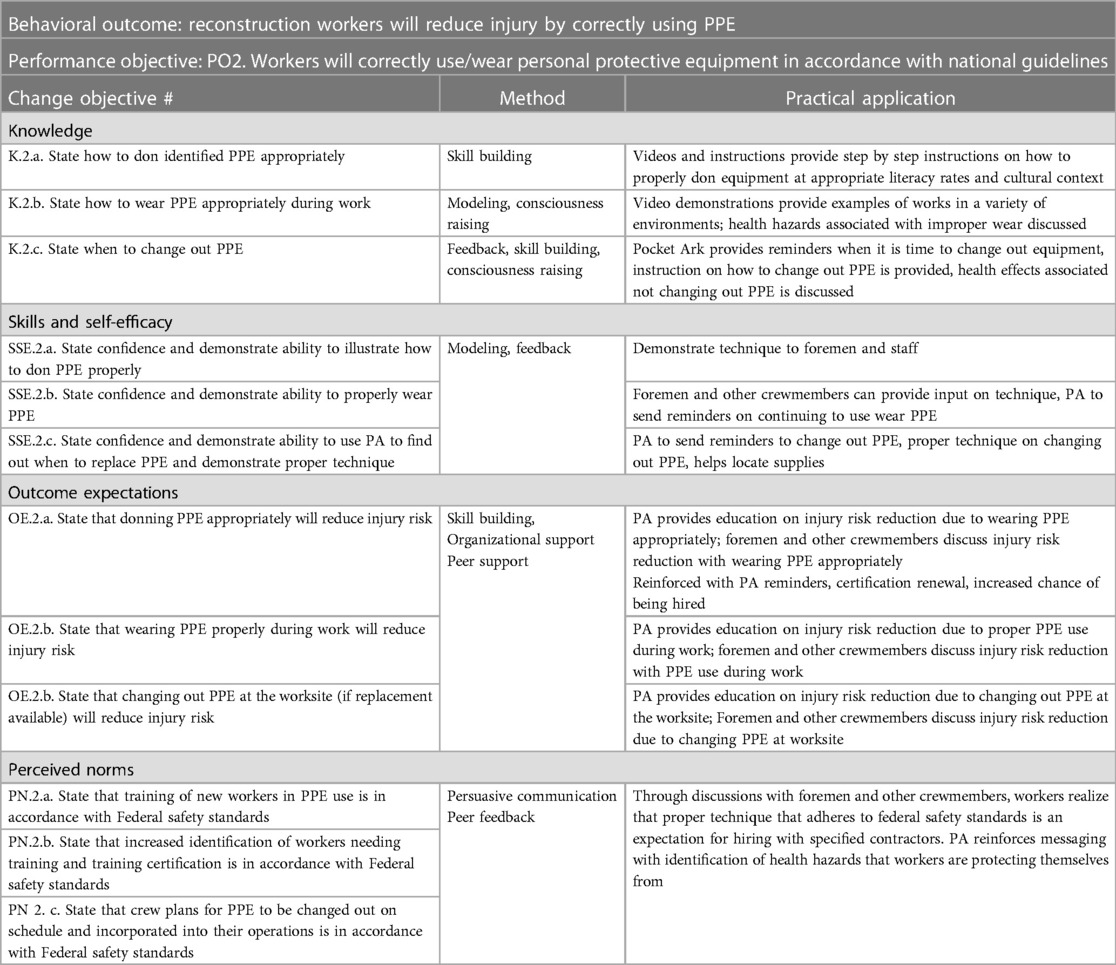
Table 6. Example of methods and practical applications used in pocket Ark.
5.2.2 Reconstruction worker organization environment
5.2.2.1 Worker safety guidelines
Published worker safety guidelines and best practices were consulted to determine the context of use for the PA. The PA was aligned with the OSHA/Healthy People 2020/Federal Guideline, which represents best-practice standards for US worksite health and wellbeing (60).
5.2.2.2 Organizational task analysis
Task analysis was conducted in the participating organizations to examine data flow within the organization, manager decision-making, interaction points between managers and workers, worker accreditation/certification training, and worker field protocols. The task analysis was based on how RF disseminates information. Briefly, the RF has a national training director who has had extensive training in construction health and safety. The training coordinator assembles information on best training practices and designs this information in a format that is appropriate for the literacy, language, and level of skill levels of the spectrum of reconstruction workers the material is targeted for. This information is currently distributed as printed material. With the coordinating assistance of the director of workforce engagement, this material is given to the field staff for distribution directly to the workers by the training staff. The training staff is composed largely of former reconstruction workers with direct experience of the health and safety hazards that workers will be encountering. Material is disseminated to the workers based on need and focus at the time. This enabled the identification of logical opportunities for the adoption and implementation of PA for training and coordination (61) (Figure 3).
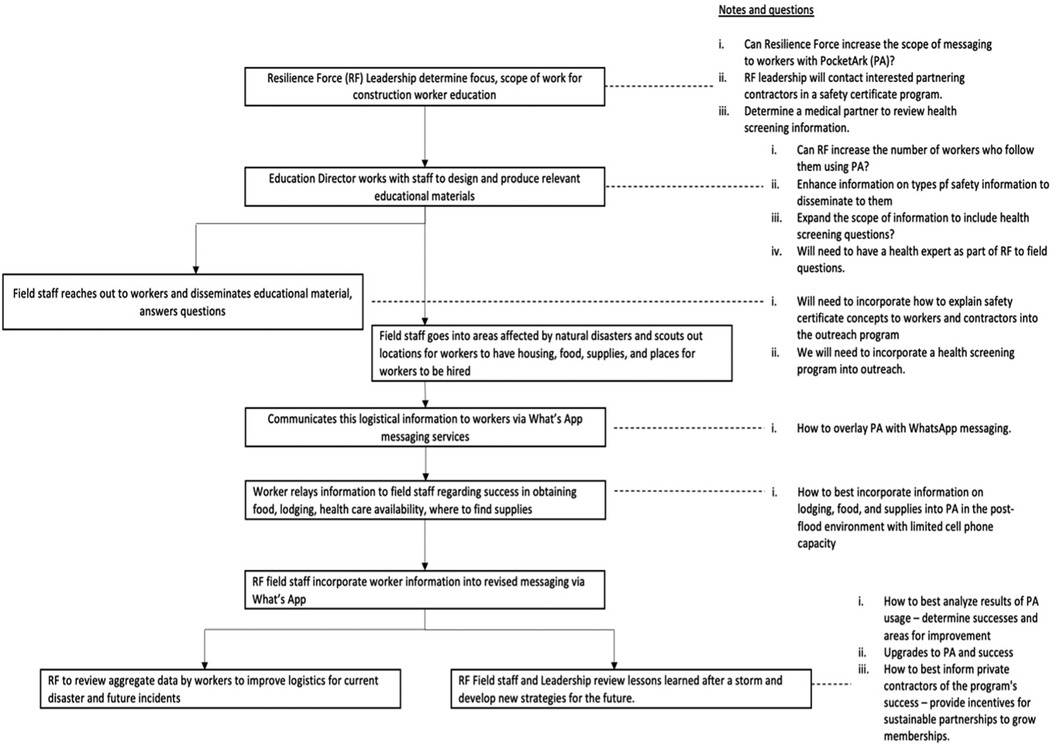
Figure 3. Resilience force worker education task analysis flow.
5.3 Task 3.3: select or design practical applications to deliver change methods
Practical applications were selected to operationalize the theory-based change methods in ways that fit the population and setting. PA was designed for easy adoption by organizations that currently incorporate computer-based methods for record keeping and tracking of workers. The digital platform provided an innovative solution to provide standardized training to the workers on a platform that could be readily accessed on personal devices and in a mixed-mode graphic/text application that could be readily understood at a reduced reading level.
6 IM Step 4: program production
Step 4 comprised refinement of the PA's structure and organization; planning for program materials; drafting of messages and materials; and pretesting, refinement, and production of materials.
Technology stack: Pocket Ark is constructed on a stable, scalable, maintainable, and extensible technology platform. Major components include (1) a cross-platform hybrid mobile application (authored in Typescript using the Ionic framework); (2) a backend management application (developed on Node.js via the Strapi framework); (3) a relational data persistence layer (Postgres); and (4) third-party services (e.g., Twilio SMS) to facilitate communication and coordination. The mobile app component of the system is deployed via standard iOS and Android app store channels, while the application backend is deployed on Azure Cloud.
System sustainability: Pocket Ark was designed with sustainability as a primary consideration. For example, the database schema can be updated by a super-user directly in the Strapi interface, allowing system maintainers to evolve the design to meet changing user and organizational needs. Program content and educational media can be updated, again in a web interface, directly by coordinating organizations, allowing them to deliver the most critical content they require for their worker population.
Commercial model: Pocket Ark is a proprietary system intended that may be offered under multiple commercialization models: as a subscription service, as a blanket organizational license, or as an underwritten program funded by a Federal or commercial agency.
6.1 Task 4.1: refine program structure and organization
Evidence-based provider-level strategies, previously described in the empirical literature (Step 1), informed the development and adaptation of PA component strategies. PA assists the coordinating center in collecting information and coordinating the training and support of reconstruction workers while providing hands-on decision support directly to the workers within three deployment phases: pre-deployment, deployment, and post-deployment.
6.2 Task 4.2: prepare plans for program materials
PA design documents provided a blueprint of the functional specifications of the prototype. Project team conference calls and face-to-face meetings provided iterative review and feedback on the design. Design documents described content, design features, functionality, language, logistics of use and worksite implementation, orientation needs, and evaluation specifications. Pocket Ark components are described below.
6.3 Task 4.3: draft messages, materials, and protocols
Pocket Ark programming followed a stepped sequence. Each component draft is built upon the iterative review of previous developmental drafts, allowing multiple reviews.
PA coordinating center deployment dashboard (Figure 4): The PA dashboard allows the coordinating center (e.g., advocacy groups, contractors) to recruit workers via SMS, evaluate and enhance their readiness for deployment, and manage the status of deployments across sites. Worker deployment can be in multiple states and for varied durations. The organization dashboard provides coordination within each deployment phase, designed to mitigate the risk faced by the flood zone workers in hazardous environments in the post-hurricane recovery and rebuilding operations. Pre-deployment phase functions incorporate (1) worker profile and contract record entry, (2) health status assessment, (3) COVID-19 prevention training, (4) disaster response behavior and safety training, and (5) scenario-based assessment (Figure 5). Deployment phase functions incorporate (5) communication, (6) job contracting, (7) security and safety, and (8) resource linkage. Post-deployment functions incorporate assessment and evaluation of health parameters, incidents, and challenges. A description of each function is provided below.
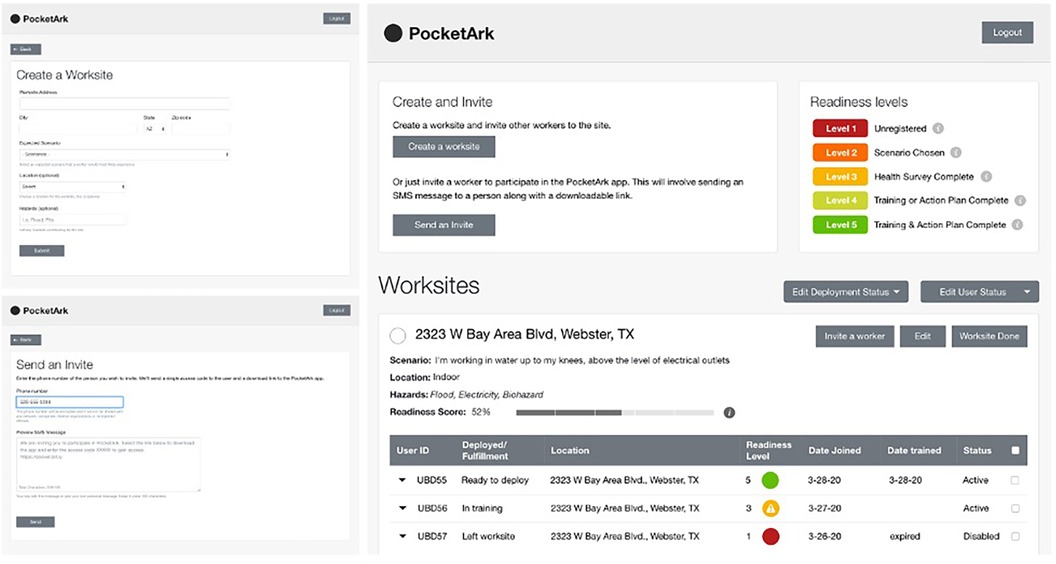
Figure 4. Coordinating center deployment dashboard.
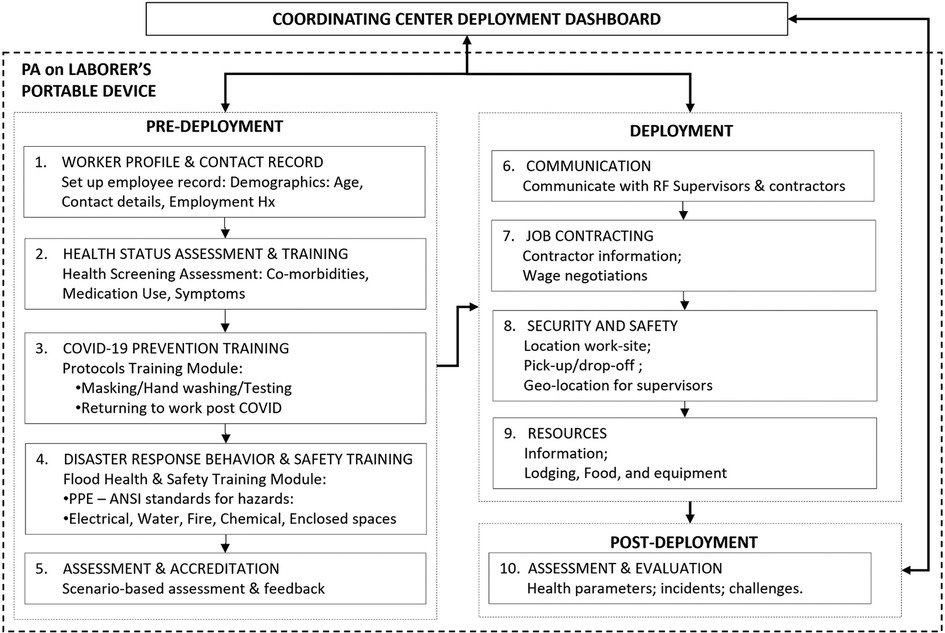
Figure 5. Pocket Ark function by deployment phase.
Pocket Ark component strategies for construction workers (Figure 5, #1–10): The PA prototype has an interface for workers to engage in pre-deployment, deployment, and post-deployment activities (previously listed and described in greater detail below).
6.3.1 Pre-deployment
Pocket Ark pre-deployment activities comprise building a worker profile, health status monitoring, COVID-19 training, disaster response behavior, and safety training, and skills assessment and accreditation (Figure 5, #1–5). The pre-deployment phase updates a database to maintain worker contact details, medical history, and accreditation status (skills training and COVID-19 protocols) and cues the contracting agency to assist workers to obtain needed skill sets.
Worker profile and contact record (Figure 5, #1): The reconstruction worker sets up a personal profile that comprises age, home address, email, and telephone callback number. This information is used by the coordinating center to help identify and locate workers who are working in an affected flooded area. Phone contact information is used to rapidly contact and communicate with workers in the post-flood environment. The worker profile section is optional. Workers can elect to opt out if they are concerned about confidentiality. This does not impact access to other PA functionality.
Health status assessment and training (Figure 5 #2 and Figure 6A): The reconstruction worker sets up a medical history profile by providing responses to a series of basic medical screening questions drawn from surveys of history of chronic disease (including cardiovascular disease), heat illness, daily medications, dietary needs). Health domains comprise physical fitness (e.g., ability to walk up two flights of stairs, ability to run two blocks) and respiratory and cardiovascular-related health and symptoms (e.g., cough, shortness of breath, chest pain, difficulty breathing). Questions include “Do you have any history of heart or breathing problems?” and enquire about currently used medications. The medical history data enable PA to cross-reference reported hazards in the field with worker medical history data to enable tailored advice to be provided in real time to the worker in the field. This also provides the contracting agency with medical information available in an emergency. These questions are intentionally designed with low readability scores, aiding reconstruction workers with limited health literacy in effectively comprehending them. In addition, the application will offer Spanish language support along with flexibility to use help from supervisors and worker advocacy staff (WAS), benefiting a predominantly Hispanic worker population and enhancing their understanding of the questions.
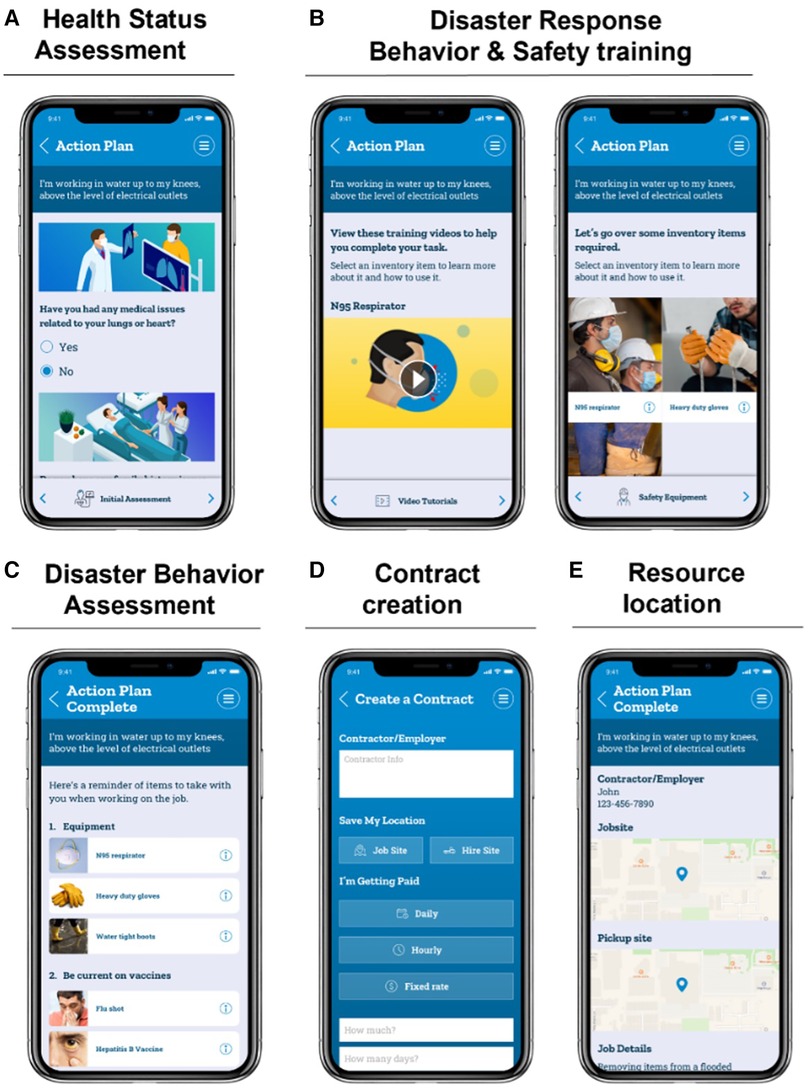
Figure 6. Pocket Ark prototype screen captures.
COVID-19 health training (Figure 5, #3): The COVID-19 training module discusses precautionary behaviors to mitigate COVID-19 risk. Worker training comprises (1) infographic representation of different types of face masks, their application, and their ability to reduce viral spread; (2) pictograms of proper hand washing techniques and use of different hand cleaners; (3) guidelines on different types of COVID-19 testing (lab and home testing) including pictographic instructions for home testing kits; and (4) video of return-to-work protocols for those testing positive based on recent OSHA guidelines. Case-based surveys are provided for self-assessment and feedback on the knowledge obtained. PA provides managers of the contracting agency with training and resources on managing COVID-19 from a supervisor's perspective and how to set up an onsite screening system at the worksite to prevent COVID-19 spread.
Disaster response behavior and safety training (Figure 5 #4 and Figure 6B): Disaster response behavior and safety training comprise skills training on (1) recognizing types of hazards and (2) PPE use. Types of hazards include the presence of water (type, depth, and flow), electrical hazards (e.g., live wiring), fire, physical debris (e.g., submerged material), biohazards (e.g., mold, chemicals, irritants, toxins), biological hazards (e.g., fire ants, snakes), and enclosed spaces. Training modules apply strategies of case studies, pictograms, and infographics to increase knowledge and skills for working in flooded environments. Training modules are provided on PPE that is needed to safely enter flooded buildings and begin demolition and reconstruction work. Details are provided regarding the appropriate protective equipment for the head, eyes, hands, and feet to wear in the post-flood environment. This content is delivered by text with accompanying visual graphics. Training is based on the American National Standards Institute (ANSI) standards and labeling that indicates approved equipment (62). The meaning of the ANSI standards and labeling is demonstrated for different hazards that workers are likely to confront in the post-flood environment, including electrical, water, fire, chemical, and enclosed spaces.
Disaster behavior assessment and accreditation (Figure 5 #5 and Figure 6C): Assessment employs a quiz-based drill and practice quiz format to assess workers on control methods when encountering an array of different types of hazards. Scenarios are provided, and the worker is prompted to correctly identify hazards, appropriate equipment required, and recommended protocols for use. An assessment and feedback report on the worker's readiness is also made available for review by the supporting worker advocacy organization.
6.3.2 Deployment
Deployment activities comprise real-time field use of PA to ensure consistent bidirectional communication, negotiate contracts, ensure safety, and locate and access resources.
Communication (Figure 5 #6): PA enables bidirectional communication between reconstruction workers with the contracting organization that operates as the communication hub to convey updates to all workers on the changing parameters in the field. This information is consistently updated from status reports from workers on the ground. Workers and the coordinating center will therefore have the latest information on changing conditions and resources. This fulfills the evolving need on the ground based on the information about the location/event at the time of the deployment into the flood zone areas.
Job contracting (Figure 5 #7 and Figure 6D) PA provides workers with a standard form to record employer details and agreed dates, times, tasks, location, and agreed wages (weekly, daily, hourly). This electronic document can be uploaded to the contracting organization as validation of an agreement in the field. The feature provides some documented evidence of worker contracts should there be reneging of negotiated contracts by employers.
Worker geolocation (Figure 5 #8): PA enables workers to send their worksite location to the contracting organization database for employee monitoring. This is useful if the employer does not provide them with transportation back home at the end of their workday.
Resource monitoring and access (Figure 5 #9 and Figure 6E): PA can enable GIS location of types of resources (accommodation, equipment, food distribution) to support the reconstruction worker in the field. Through menu options, the worker can geolocate the needed supplies. The PA application programming interface (API) enables seamless integration with ArcGIS maps.
6.3.3 Post-deployment
PA post-deployment takes the form of a debrief assessment of health parameters (e.g., symptoms experienced), incidents (injuries), and challenges (i.e., problems associated with contract negotiations, resource access, and PA functionality) (Figure 5). Continuing education is also available to workers after an incident to increase their employability and safety.
6.4 Task 4.4: pre-test, refine, and produce materials
A formative single-group pre-post usability field test was conducted with a sample of self-identified day laborer construction workers to assess usability parameters and short-term efficacy relating to program goals A (knowledge) and B (behavioral capability). Prior to the field test, in-house alpha testing was conducted to ensure the Phase 1 prototype was free of programming bugs and logical errors. Construction worker recruitment: 12 self-identified construction workers were recruited to participate in the study from an urban site where day laborers meet each day to be hired for construction work. This group was selected for pilot testing as workers who specifically identified as only working in reconstruction were not readily available at the time of the pilot. These day laborers were chosen as most identified reconstruction workers begin their careers as day laborers and often work in this capacity when not working at reconstruction sites. The construction workers are very similar to reconstruction workers in terms of skill sets and knowledge base. All workers were adult males with Spanish as their primary language, and all information was provided to them in Spanish. Participants received a brief verbal and written description of Pocket Ark and the goal of the 1-h session, which were read to each participant individually in Spanish. Individual demographic data were not obtained in response to participant requests to maintain their confidentiality.
6.4.1 Assessment protocols
Pre-test assessment: Each participant completed a written and practical assessment of declarative and procedural knowledge and behavioral capability prior to using the training component of PA. A research volunteer was available to answer questions or to read test questions for workers who had questions or low literacy. Knowledge was assessed using a 13-item multiple choice questionnaire covering the PA training module content on protective equipment, interpreting ANSI codes, and when to wear proper equipment. Modules were conducted at a level of having no prior knowledge of PPE or ANSI codes. Behavioral capability was assessed using a practical discrimination test in which participants selected the safest personal protective equipment (i.e., hard hats and protective eyewear) from a selection of four options by correctly interpreting the appropriate NIOSH safety labels. Pocket Ark training module use: Participants were then provided with a cell phone with the PA Safety App, worked through the educational module, and then one case scenario. Participants could proceed unaided at their own pace. The research field team was available for questions or to individually read each screen of the app and given assistance with forwarding to the next screen if this was necessary. Post-test assessment: Following module completion, participants repeated the written and practical assessments. Participants received a cash incentive payment of $25 for participating. Procedures and forms were reviewed and approved by the Committee for the Protection of Human Subjects (CPHS) of the University of Texas Health Science Center at Houston with the Protocol Number: HSC-SPH-19-0571. Analysis: Differences in written and practical pre- and post-test assessments were determined using paired T-tests.
6.4.2 Results
Five participants completed the knowledge testing, and 11 participants completed the practicum testing. Seven participants did not complete the PA assessments due to early job placement pick-ups (n = 3) and incorrect data entry on phones (n = 4). For the knowledge test, the range of duration for participants to complete the PA ranged from 20 to 60 min, depending on literacy level and comfort with technology. Participant’s safety knowledge significantly increased after exposure to PA. The mean difference score between the knowledge pre- and post-tests was 3.20 (±1.30), with a paired T-test statistic of 5.49, df = 4, p = 0.0054, 95% CI (1.58–4.82) (Figure 7). Individual changes in pre- and post-test scores are shown in Figure 7. Practicum test scores did not change significantly (Wilcoxon signed rank = 22, p = 0.1875) though the 11 participants demonstrated a positive net increase in scores. In post-test debrief interviews, the reconstruction workers confirmed their appreciation for the Pocket Ark project, the importance of the PA content, their lack of access to existing salient health and safety information, and the lack of support from employers in providing personal protective equipment. Many also voiced concerns about feeling vulnerable to wage theft and the unwillingness of employers to listen to health and safety concerns. The main barriers to using PA were low literacy (four participants required that the entire content of the pre- and post-tests and the PA content be read to them) and limitations on time to thoroughly review the PA material.
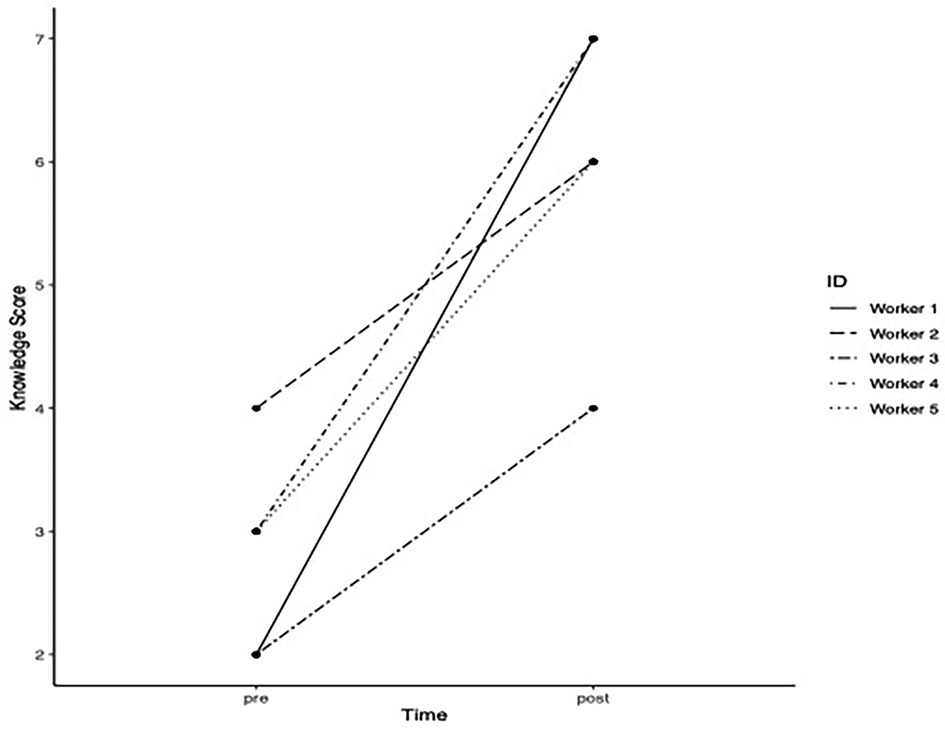
Figure 7. Pre- and post-Pocket Ark written test scores.
The PA research team is currently revising the program based on these initial results. PA is being changed to accommodate low literacy levels by making all modules incorporate audio features, which do not require reading. In addition, modules are being redesigned for workers with minimal reading skills to more easily navigate from module to module by having simplified screens with more identifiable images on each selection.
7 IM Step 5: implementation plan
Step 5 describes the future steps that we will initiate to make PA a usable product. This includes further refining who will be the program implementers, defining the outcomes and performance objectives for implementation, constructing matrices of change objectives for implementation, and designing implementation interventions (27).
7.1 Task 5.1: identify potential program implementers
The PA is specifically designed for use by the field staff of worker advocacy groups for reconstruction workers responding to disasters and the reconstruction workers themselves. Potential adopters included workers in reconstruction for flooding, wildfire, and other natural disaster areas. From an organizational standpoint, worker advocacy groups, private construction contractors, non-profit disaster relief agencies, and both federal and state government disaster relief agencies are all potential adopters.
7.2 Task 5.2: state outcomes and performance objectives for implementation
Performance objectives for adoption were brainstormed by the project team with consideration of the decision-makers in the network and informed by the IM framework and characteristics for the diffusion of the innovation (63). Outcomes included that (1) implementers (both individual workers and employers) would recognize a need for PA and its relative advantage and make a formal commitment to utilizing information technology. Steps for implementation included that the employer would assess the need for a program to provide health and safety information as well as logistical support to workers, review the program and its components and note objectives and relative advantages for its adoption, obtain feedback from workers on potential barriers to/advantages of adopting the program, and agree to trial the components.
7.3 Task 5.3: construct matrices of change objectives for implementation and Task 5.4: design implementation interventions
Critical opportunities for PA implementation in worker communities were identified using task analysis (previously described). This also helped identify existing information technology channels by which to deploy the needed strategies. Matrices categorized objectives for PA to implement performance objectives at the construction site and for champions among the workers to lead implementation efforts. The WAS were differentiated into two different groups: WAL and worker advocacy field staff (WAFS). WAL includes those members of the worker advocacy group that represent the disaster response's central coordinators, and the field staff are those at the disaster area itself, identifying worker needs and locating available resources. Champions from the WAFS and workers were identified as important parts of the program's implementation. Advantages of PA include easy access to health and safety information and a requirement of only a single investment of resources (learning to use PA). This upfront commitment is offset by significant increases in safe construction behaviors, improved ability to identify preexisting health conditions that require medical screening, and improved ability to negotiate fair wages (Table 7).
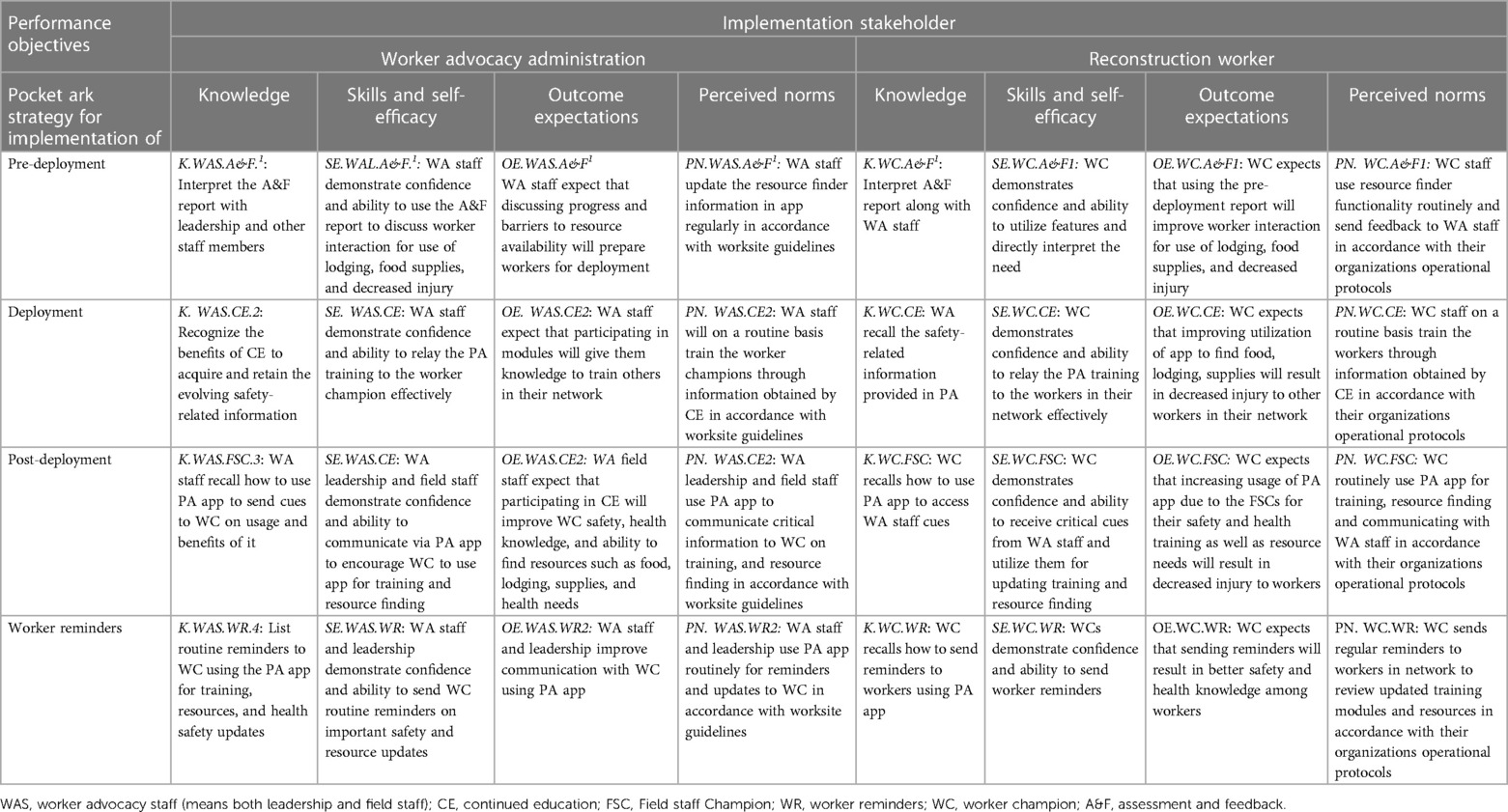
Table 7. Matrix of determinants for PA implementation for coordinating agency and reconstruction workers.
8 IM Step 6: evaluation plan
Step 6 comprises developing effect and process evaluation questions, indicators and measures of assessment, and specifying an evaluation design to measure outcomes.
8.1 Task 6.1: write effect and process evaluation questions
The main question to be addressed in the evaluation of PA is: Does the program's use improve the health of the reconstruction worker? Stated as an alternative testable empirical hypothesis: A network of reconstruction workers who use PA in the context of their usual work in the aftermath of flooding disasters will demonstrate significantly decreased rates of on-the-job illness and injuries, respiratory-borne illnesses, episodes of not being picked up from work successfully, and wage theft when compared with reconstruction workers who use conventional methods of working. Process evaluation will include the assessment of mediators for successful use of PA by the reconstruction worker and the organization.
8.2 Task 6.2: develop indicators and measures for assessment
Evaluation of PA will focus on the collection of centralized data. Worker measurements include the completion of educational modules and utilization of the program for logistical information, geolocation, and wage theft features. Organizational measurements will include the ability to utilize PA to communicate logistical information to workers, identify resources that workers will use, and analyze outcomes to further improve the effectiveness of PA for both current deployments and planning for future events. Planned process measures to assess implementation fidelity will be specified for each strategy. These measurements can be ascertained from backend PA data obtained from users.
8.3 Task 6.3: specify evaluation design
The pilot test for using PA's features for workers will be tested using a high-fidelity simulated response scenario. We will recruit 64 construction workers by working with our worker advocacy program partner's staff, utilizing their existing network of employees. The test will be administered remotely, online, via the participant's cell phone app. Interested candidates will be asked to complete an online consent form. Enrolled participants will then be asked to (1) provide demographic and health information, (2) complete a simulated wage contract, (3) complete specified training health modules, and (4) complete a pre-behavioral capability test (Table 8).
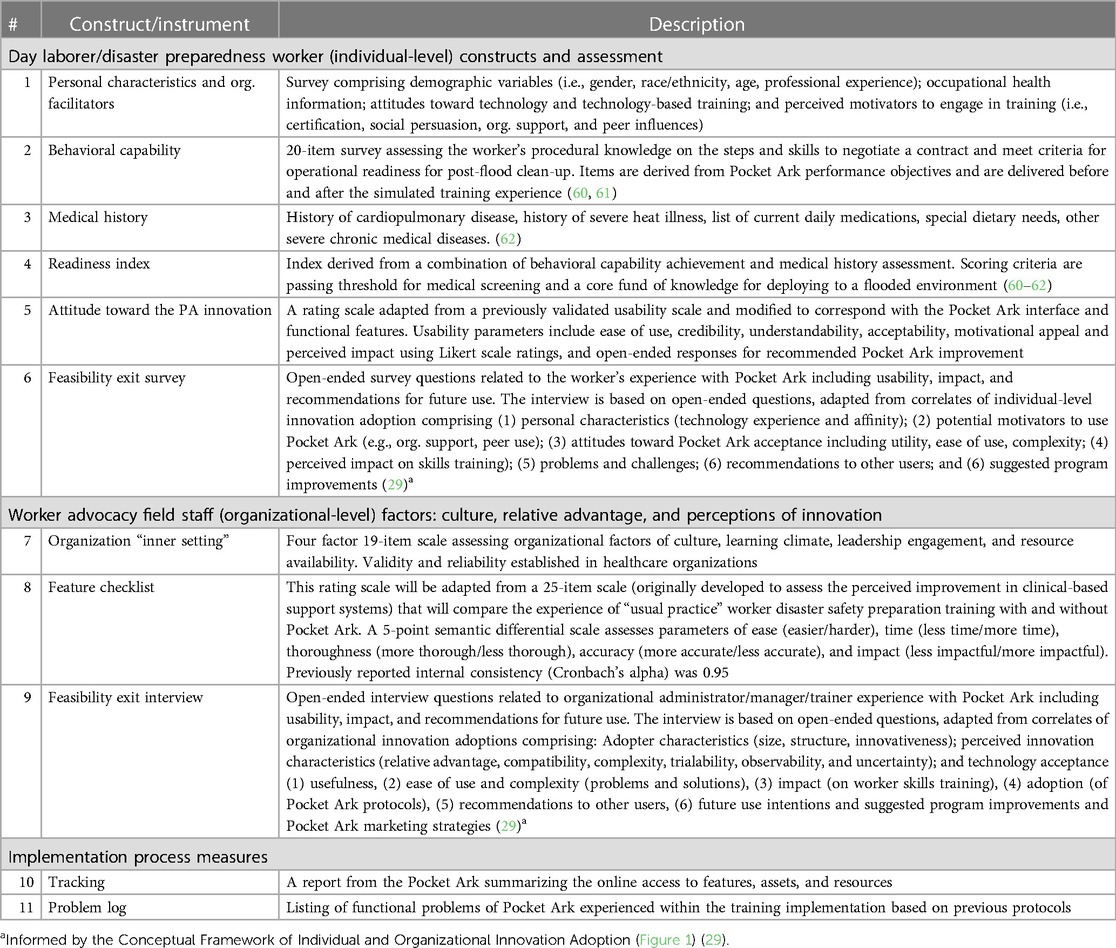
Table 8. Implementation of outcome measures: usability, feasibility, impact, and process.
A post-flood disaster scenario which is based on an actual flooding event that has occurred will then be given via phone messaging to the participants. Participants will be asked questions regarding their response to the different challenges he/she might encounter in a post-flood construction event and asked to respond appropriately. Information will be largely graphical, and workers can take the module over several days. The testing score results will be available to the participants along with explanations. A brief acceptability assessment and exit interview survey will be completed by the participants that will assess the program's usefulness, evaluate for technical glitches encountered, request suggestions for future implementation, and derive ratings on PA perceived impact.
Organizational readiness will similarly be tested for WA field staff. Ten field staff members will be asked to go through the simulated training from their perspective including evaluating worker readiness, identifying worker reconstruction sites, arranging logistical resources, and screening for deployment and post-deployment health issues in workers. They will then be asked to complete a survey on the organizational culture, a features checklist assessing relative advantage of Pocket Ark compared to usual training protocols, and a brief exit interview assessing the Pocket Ark training experience in terms of adopter characteristics, perceptions of innovation parameters, and parameters of technology acceptance (Table 8).
Improvements in health and safety using PA will be obtained by self-reported questionnaire of a cohort of reconstruction workers using PA compared with a control group after our partnering WA has begun utilizing it. The research arm of reconstruction workers using PA will be questioned regarding wearing PPE during deployment; symptoms attributable to workplace hazards; incidences of being left at work; having an infectious respiratory-borne illness; wage theft; and having a lack of adequate food, water, lodging, and supplies to safety work. These evaluations will be compared for significance on these variables with a cohort of reconstruction workers who are not using the PA and tested for significance.
9 Discussion
Due to the increase in the number and intensity of flooding events, it has become increasingly critical to educate reconstruction workers about the numerous hazards they will encounter in the immediate post-flood environment and provide them with real-time assistance during deployment at the worksite. PA has been designed as an e-learning tool specifically for reconstruction workers, which can address these pre-deployment, deployment, and post-deployment needs. Utilizing Intervention Mapping, we have been able to design a comprehensive e-learning tool to provide critical health and safety education to reconstruction workers in the pre-deployment phase at the beginning of the job in affected areas. The findings of this pilot study add to the literature on Intervention Mapping indicating the utility of e-Health tools with a theoretical and empirical basis (54). The steps of IM allow researchers to consider theory, individual factors, and environmental contexts to create targeted interventions with multiple components that address multiple levels.
The prototype's initial small pilot testing program shows encouraging results that indicate that the educational approach can be an effective means of learning and training in this population. Based on our initial pilot, in which 50% of our participants needed to have a staff member read the entire project to them, it was learned that literacy rates vary greatly in the day laborer populations. Some versions of our educational program need to be available to the groups with lower literacy quartiles, potentially providing training and education through pictorial options only. Also, the field testing showed that even in the pre-deployment phase of learning, educational modules need to be brief and able to be completed in a few minutes to accommodate the sometimes unpredictable and varied schedule of these reconstruction workers. The modest increase in the participants’ pre- and post-practicum test scores indicates the need to elaborate more on identifying appropriate NIOSH safety labels for the job. Many times, these labels on equipment are small and difficult to identify. Language barriers and literacy rates are also considered an additional challenge for these individuals to understand the hazards clearly. Increasing the number of visual cues in the e-learning modules may help improve learning. It was also recognized that the number of participants was small, and hence we are currently evaluating the effect of the PA education module on a larger cohort of participants.
Positive feedback was received from the workers involved in the field testing and the numerous stakeholders in both the public and private sectors that have vetted the features of PA. Based on their extensive feedback, the PA application is posed for further development of the project during the pending Phase II development: (1) enhanced security features, (2) customized literacy learning, (3) improved ease of completing learning modules, and (4) incorporation of employer/worker advocacy interface are all features that will be emphasized.
9.1 Limitations
Study limitations include that the initial pilot was small and testing only limited PA aspects designed for the individual reconstruction workers. The initial test was for only day laborer construction workers rather than those who specialize in reconstruction work, and their skill level was not assessed as part of interviews and pilot testing. Also, the study population of reconstruction workers is mobile and, at the time, difficult to reach, making long-term follow-up challenging. During the initial pilot, many of our workers had to leave abruptly and were initially reluctant to participate. Working more closely with the WA group Resilient Force in future testing will help improve our ability to conduct testing with a large cohort in a more controlled setting.
9.2 Next steps
As outlined in Task 6.3, our next steps in PA's development will be to evaluate its full capability more fully with both individual reconstruction workers and the WA group on an organizational level. Completing this step will subsequently develop PA to the point that it can be released for use as a product, and efficacy testing of its use in actual deployments can ensue.
10 Conclusion
PA can be an effective bridge of pre-deployment education and deployment health and safety support for reconstruction work in the immediate post-flood environment. In a time of rapidly increasing natural disasters from a variety of causes, tools like PA have the potential to greatly improve the safety of those working to help affected communities.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
WP: Writing – original draft, Writing – review & editing. RS: Writing – original draft, Writing – review & editing. DL: Writing – original draft, Writing – review & editing. SU: Writing – original draft, Writing – review & editing. GY: Writing – original draft, Writing – review & editing. RG-L: Writing – original draft, Writing – review & editing. PM: Writing – original draft, Writing – review & editing. JR: Writing – original draft, Writing – review & editing. RM: Writing – original draft, Writing – review & editing. JM: Writing – original draft, Writing – review & editing. IN: Writing – original draft, Writing – review & editing.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article.
This research was partially funded by the Centers for Disease Control and Prevention/National Institute of Occupational Safety and Health (Award #T42OH008421) through the Southwest Center for Occupational and Environmental Health (SWCOEH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Centers for Disease Control and Prevention/National Institute of Occupational Safety and Health. Research was also partially funded by NIEHS (grant #R44ES040580).
Conflict of interest
JL was employed by Radian Digital.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. USGCRP. Climate Science Special Report: Fourth National Climate Assessment, Volume I. Washington, DC: U.S. Global Change Research Program (2017). p. 470. doi: 10.7930/J0J964J6
2. Trenberth KE. Framing the way to relate climate extremes to climate change. Clim Change. (2012) 115(2):283–90. doi: 10.1007/s10584-012-0441-5
3. Perkison WB, Kearney GD, Saberi P, Guidotti T, McCarthy R, Cook-Shimanek M, et al. Responsibilities of the occupational and environmental medicine provider in the treatment and prevention of climate change-related health problems. J Occup Environ Med. (2018) 60(2):e76–81. doi: 10.1097/jom.0000000000001251
4. Kundzewicz ZW, Kanae S, Seneviratne SI, Handmer J, Nicholls N, Peduzzi P, et al. Flood risk and climate change: global and regional perspectives. Hydrol Sci J. (2014) 59(1):1–28. doi: 10.1080/02626667.2013.857411
5. Waddell SL, Jayaweera DT, Mirsaeidi M, Beier JC, Kumar N. Perspectives on the health effects of hurricanes: a review and challenges. Int J Environ Res Public Health. (2021) 18(5):2756. (in English). doi: 10.3390/ijerph18052756
6. Pamidimukkala A, Kermanshachi S, Nipa TJ. Safety risks of reconstruction workers in clean-up and recovery phase due to natural hazards. Construction Research Congress 2022. (2022). p. 520–30.
7. Sakuma A, Takahashi Y, Ueda I, Sato H, Katsura M, Abe M, et al. Post-traumatic stress disorder and depression prevalence and associated risk factors among local disaster relief and reconstruction workers fourteen months after the Great East Japan Earthquake: a cross-sectional study. BMC Psychiatry. (2015) 15:58. doi: 10.1186/s12888-015-0440-y
8. Liang SY, Messenger N. Infectious diseases after hydrologic disasters. Emerg Med Clin North Am. (2018) 36(4):835–51 (in English). doi: 10.1016/j.emc.2018.07.002
9. Kouadio IK, Aljunid S, Kamigaki T, Hammad K, Oshitani H. Infectious diseases following natural disasters: prevention and control measures. Expert Rev Anti Infect Ther. (2012) 10(1):95–104. doi: 10.1586/eri.11.155
10. Barbeau DN, Grimsley LF, White LE, El-Dahr JM, Lichtveld M. Mold exposure and health effects following hurricanes Katrina and Rita. Annu Rev Public Health. (2010) 31:165–78. doi: 10.1146/annurev.publhealth.012809.103643
11. Gunnbjörnsdóttir MI, Franklin KA, Norbäck D, Björnsson E, Gislason D, Lindberg E, et al. Prevalence and incidence of respiratory symptoms in relation to indoor dampness: the RHINE study. Thorax. (2006) 61(3):221–5 (in English). doi: 10.1136/thx.2005.057430
12. Lane JA. The ethical implication of bartering for mental health services: examining interdisciplinary ethical standards. Mich J Counsel. (2013) 39(2):4–12. doi: 10.22237/mijoc/1356998460
13. Fayard GM. Fatal work injuries involving natural disasters, 1992–2006. Disaster Med Public Health Prep. (2009) 3(4):201–9. doi: 10.1097/DMP.0b013e3181b65895
14. Vinck P, Pham PN, Fletcher LE, Stover E. Inequalities and prospects: ethnicity and legal status in the construction labor force after hurricane Katrina. Organ Environ. (2009) 22(4):470–8. doi: 10.1177/1086026609347192
15. Fussell E. Constructing New Orleans, constructing race: a population history of New Orleans. J Am Hist. (2007) 94(3):846–55. doi: 10.2307/25095147
16. Fletcher D, Hanton S, Mellalieu S. Chapter 10. An organizational stress review: conceptual and theoretical issues in competitive sport. In: Hanton S, Mellalieu SD, editors. Literature Reviews in Sport Psychology. New York: Nova Science Publishers, Inc (2006). p. 321–74.
17. Hamid AR A, Majid MZ A, Singh B. Causes of accidents at construction sites. Malays J Civil Eng. (2008) 20:242–59. doi: 10.11113/mjce.v20.15769
18. Chandran Achutan BK. Hurricane Katrina Response. CDC.gov; 2007. Report No.: HETA-2005-0369-3034. HETA-2005-0369-3034. National Institute for Occupational Safety and Health (NIOSH).
19. Li Y, Bakos-Block C, Rammah A, Magal R, Adekanye J, Esquenazi S, et al. The post hurricane Harvey respiratory protection training program. J Occup Environ Med. (2020) 62(10):842–6 (in English). doi: 10.1097/jom.0000000000001976
20. NIOSH. Emergency Response Resources. CDC; February 22. Available online at: https://www.cdc.gov/niosh/topics/emres/sitemgt.html (November 30, 2018).
21. OSHA. Hurricane eMatrix Tool. OSHA (2016). Available online at: https://www.osha.gov/etools/hurricane. (Accessed January 29, 2023)
22. Blake H, Bermingham F, Johnson G, Tabner A. Mitigating the psychological impact of COVID-19 on healthcare workers: a digital learning package. Int J Environ Res Public Health. (2020) 17(9):2997 (in English). doi: 10.3390/ijerph17092997
23. Suppan L, Abbas M, Stuby L, Cottet P, Larribau R, Golay E, et al. Effect of an E-learning module on personal protective equipment proficiency among prehospital personnel: web-based randomized controlled trial. J Med Internet Res. (2020) 22(8):e21265 (in English). doi: 10.2196/21265
24. Li D-C, Tsai C-Y. An empirical study on the learning outcomes of E-learning measures in Taiwanese small and medium-sized enterprises (SMEs) based on the perspective of goal orientation theory. Sustainability. (2020) 12(12):5054. doi: 10.3390/su12125054
25. Lee YJ, Lee D. Factors influencing learning satisfaction of migrant workers in Korea with E-learning-based occupational safety and health education. Saf Health Work. (2015) 6(3):211–7 (in English). doi: 10.1016/j.shaw.2015.05.002
26. Buchanan S. Day labor and occupational health: time to take a closer look. New Solut. (2004) 14(3):253–60. doi: 10.2190/0FAT-LRGY-AM4D-CD2P
27. Bartholomew Eldredge LK, Markham CM, Ruiter RAC, Fernández ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. 4th ed. San Francisco, CA: Jossey-Bass Inc (2016).
28. Garba RM, Gadanya MA. The role of intervention mapping in designing disease prevention interventions: a systematic review of the literature. PLoS One. (2017) 12(3):e0174438 (in English). doi: 10.1371/journal.pone.0174438
29. Tripp MK, Herrmann NB, Parcel GS, Chamberlain RM, Gritz ER. Sun protection is fun! A skin cancer prevention program for preschools. J Sch Health. (2000) 70(10):395–401 (in English). doi: 10.1111/j.1746-1561.2000.tb07226.x
30. Dalum P, Schaalma H, Kok G. The development of an adolescent smoking cessation intervention—an intervention mapping approach to planning. Health Educ Res. (2012) 27(1):172–81 (in English). doi: 10.1093/her/cyr044
31. Fernández ME, Gonzales A, Tortolero-Luna G, Partida S, Bartholomew LK. Using intervention mapping to develop a breast and cervical cancer screening program for Hispanic farmworkers: Cultivando La Salud. Health Promot Pract. (2005) 6(4):394–404 (in English). doi: 10.1177/1524839905278810
32. Byrd TL, Wilson KM, Smith JL, Heckert A, Orians CE, Vernon SW, et al. Using intervention mapping as a participatory strategy: development of a cervical cancer screening intervention for Hispanic women. Health Educ Behav. (2012) 39(5):603–11 (in English). doi: 10.1177/1090198111426452
33. Byrd TL, Wilson KM, Smith JL, Coronado G, Vernon SW, Fernandez-Esquer ME, et al. AMIGAS: a multicity, multicomponent cervical cancer prevention trial among Mexican American women. Cancer. (2013) 119(7):1365–72 (in English). doi: 10.1002/cncr.27926
34. Hou SI, Fernandez ME, Parcel GS. Development of a cervical cancer educational program for Chinese women using intervention mapping. Health Promot Pract. (2004) 5(1):80–7. doi: 10.1177/1524839903257311
35. Crosby R, Noar SM. What is a planning model? An introduction to PRECEDE-PROCEED. J Public Health Dent. (2011) 71(Suppl 1):S7–15 (in English). doi: 10.1111/j.1752-7325.2011.00235.x
36. Fernández-Esquer ME, Ibekwe LN, Guerrero-Luera R, King YA, Durand CP, Atkinson JS. Structural racism and immigrant health: exploring the association between wage theft, mental health, and injury among Latino day laborers. Ethn Dis. (2021) 31(Suppl 1):345–56 (in English). doi: 10.18865/ed.31.S1.345
37. Valdez Z, Plankey-Videla N, Murga AL, Menchaca AC, Barahona C. Precarious entrepreneurship: day laborers in the U.S. Southwest. Am Behav Scientist. (2019) 63(2):225–43. doi: 10.1177/0002764218794232
38. Moda HM, Filho WL, Minhas A. Impacts of climate change on outdoor workers and their safety: some research priorities. Int J Environ Res Public Health. (2019) 16(18):3458 (in English). doi: 10.3390/ijerph16183458
39. Rando RJ, Lefante JJ, Freyder LM, Jones RN. Respiratory health effects associated with restoration work in post-hurricane Katrina New Orleans. J Environ Public Health. (2012) 2012:462478 (in English). doi: 10.1155/2012/462478
40. Centers for Disease Control and Prevention. Floodwater After a Disaster or Emergency. Centers for Disease Control and Prevention (CDC) (2022). Available online at: https://www.cdc.gov/disasters/floods/floodsafety.html.
41. Cummings KJ, Cox-Ganser J, Riggs MA, Edwards N, Hobbs GR, Kreiss K. Health effects of exposure to water-damaged New Orleans homes six months after hurricanes Katrina and Rita. Am J Public Health. (2008) 98(5):869–75 (in English). doi: 10.2105/ajph.2007.118398
42. de Man H, van den Berg HH, Leenen EJ, Schijven JF, Schets FM, van der Vliet JC, et al. Quantitative assessment of infection risk from exposure to waterborne pathogens in urban floodwater. Water Res. (2014) 48:90–9 (in English). doi: 10.1016/j.watres.2013.09.022
43. Abdalla S, Apramian SS, Cantley LF, Cullen MR. Chapter 6. Occupation and risk for injuries. In: Mock CN, Nugent R, Kobusingye O, Smith KR, editors. Injury Prevention and Environmental Health. 3rd ed. Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2017). p. 97–133. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK525209/ doi: 10.1596/978-1-4648-0522-6_ch6.
44. Porru S, Baldo M. Occupational health and safety and migrant workers: has something changed in the last few years? Int J Environ Res Public Health. (2022) 19(15):9535 (in English). doi: 10.3390/ijerph19159535
45. Negi NJ, Siegel J, Calderon M, Thomas E, Valdez A. “They dumped me like trash”: the social and psychological toll of victimization on Latino day laborers’ lives. Am J Community Psychol. (2020) 65(3–4):369–80 (in English). doi: 10.1002/ajcp.12406
46. Díaz Fuentes CM, Martinez Pantoja L, Tarver M, Geschwind SA, Lara M. Latino immigrant day laborer perceptions of occupational safety and health information preferences. Am J Ind Med. (2016) 59(6):476–85. doi: 10.1002/ajim.22575
47. Ripoll Gallardo A, Djalali A, Foletti M, Ragazzoni L, Della Corte F, Lupescu O, et al. Core competencies in disaster management and humanitarian assistance: a systematic review. Disaster Med Public Health Prep. (2015) 9(4):430–9 (in English). doi: 10.1017/dmp.2015.24
48. Schyve PM. Language differences as a barrier to quality and safety in health care: the joint commission perspective. J Gen Intern Med. (2007) 22(Suppl 2):360–1 (in English). doi: 10.1007/s11606-007-0365-3
49. Luong Thanh BY, Laopaiboon M, Koh D, Sakunkoo P, Moe H. Behavioural interventions to promote workers’ use of respiratory protective equipment. Cochrane Database Syst Rev. (2016) 12(12):Cd010157 (in English). doi: 10.1002/14651858.CD010157.pub2
50. Hussain R, Pedro A, Lee DY, Pham HC, Park CS. Impact of safety training and interventions on training-transfer: targeting migrant construction workers. Int J Occup Saf Ergon. (2020) 26(2):272–84 (in English). doi: 10.1080/10803548.2018.1465671
51. Peiró JM, Nielsen K, Latorre F, Shepherd R, Vignoli M. Safety training for migrant workers in the construction industry: a systematic review and future research agenda. J Occup Health Psychol. (2020) 25(4):275–95 (in English). doi: 10.1037/ocp0000178
52. Frambach RT, Schillewaert N. Organizational innovation adoption: a multi-level framework of determinants and opportunities for future research. J Bus Res. (2002) 55(2):163–76. doi: 10.1016/S0148-2963(00)00152-1
53. Becker P, Morawetz J. Impacts of health and safety education: comparison of worker activities before and after training. Am J Ind Med. (2004) 46(1):63–70 (in English). doi: 10.1002/ajim.20034
54. Fernandez ME, Ruiter RAC, Markham CM, Kok G. Intervention mapping: theory- and evidence-based health promotion program planning: perspective and examples. Front Public Health. (2019) 7:209. doi: 10.3389/fpubh.2019.00209
55. Merrill MD. First principles of instruction. Educ Technol Res Dev. (2002) 50:43–59. doi: 10.1007/BF02505024
56. Bandura A. Human agency in social cognitive theory. Am Psychol. (1989) 44(9):1175. doi: 10.1037/0003-066X.44.9.1175
57. Hale J, Householder B, Greene K. The theory of reasoned action, in the persuasion handbook: developments in theory and practice. (2002). p. 259–88. doi: 10.4135/9781412976046.n14
58. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. (1984) 11(1):1–47. doi: 10.1177/109019818401100101
59. (OSHA) OSaHA. COVID-19—Control and Prevention: Healthcare Workers and Employers. Available online at: https://www.osha.gov/coronavirus/control-prevention/healthcare-workers (Accessed January 29, 2023).
60. Administration OSaH. Personal Protective Equipment—Construction. United States Department of Labor: United States Department of Labor; March 30. Available online at: https://www.osha.gov/personal-protective-equipment/construction. (Accessed January 29, 2023).
61. Chun AHW. The Agile Teaching/Learning Methodology and Its e-Learning Platform. Advances in Web-Based Learning—iCWL 2004. Berlin: Springer (2004). p. 11–8.
62. American National Standards Institute. American National Standard for Bibliographic References. New York: The Institute (1977).
63. Dearing JW, Cox JG. Diffusion of innovations theory, principles, and practice. Health Aff. (2018) 37(2):183–90. doi: 10.1377/hlthaff.2017.1104
Appendix I
Pocket Ark Research Group
Dr. Edelmiro Escamilla Jr.
Dr. Scott Earnest
Dr. Janelle Rios
Sasha Legette
Keywords: reconstruction worker, flooding, post-disaster deployment, health and safety, security, worker education, climate change, Intervention Mapping
Citation: Perkison WB, Shegog R, Lai D, Upadhyay S, Yalavarthy G, Guerrero-Luera R, Mathews PD, Rios J, Mehta R, McLaughlin J and Nabeel I (2024) Development of system-based digital decision support (“Pocket Ark”) for post-flood enhanced response coordination and worker safety: an Intervention Mapping approach. Front. Environ. Health 3:1368077. doi: 10.3389/fenvh.2024.1368077
Received: 9 January 2024; Accepted: 6 May 2024;
Published: 5 June 2024.
Edited by:
Justin Yang, Boston University, United StatesReviewed by:
Salvatore Lavalle, San Raffaele Hospital (IRCCS), ItalyPhilip Harber, University of Arizona, United States
© 2024 Perkison, Shegog, Lai, Upadhyay, Yalavarthy, Guerrero-Luera, Mathews, Rios, Mehta, McLaughlin and Nabeel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: William Brett Perkison, d2lsbGlhbS5iLnBlcmtpc29uQHV0aC50bWMuZWR1