 Meron Asmamaw Alemayehu1*
Meron Asmamaw Alemayehu1* Sewnet Getaye Workie2
Sewnet Getaye Workie2 Makida Abate Belew3
Makida Abate Belew3 Muluken Chanie Agimas1
Muluken Chanie Agimas1 Nebiyu Mekonnen Derseh1
Nebiyu Mekonnen Derseh1 Habtamu Wagnew Abuhay1Redeat Berihanu4Fasika Terefe Kinfe4Haymanot Assefa Abebe4Sophiya zemene4
Habtamu Wagnew Abuhay1Redeat Berihanu4Fasika Terefe Kinfe4Haymanot Assefa Abebe4Sophiya zemene4 Astewil Moges Bazezew5
Astewil Moges Bazezew5
- 1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 2Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, Debre Berhan University, Debre Berhan, Ethiopia
- 3Department of Nursing, School of Nursing and Midwifery, College of Medicine and Health Sciences, Debre Berhan University, Debre Berhan, Ethiopia
- 4Department of Nursing, GAMBY Medical and Business College, Bahir Dar, Ethiopia
- 5Department of Adult Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: Increased knowledge about the health impacts of climate change would motivate health students and health professionals to adopt sustainable healthcare practices, design climate-centered health programs, help build climate-resilient health systems, and ultimately contribute to the global effort of mitigating climate change.
Method: An Institution-based cross-sectional study was conducted among Universities in the Amhara region. A total of 616 undergraduate health science students were included from three Universities. A validated, self-administered structured questionnaire was used. Data were analyzed using STATA™ version 14.0. A Logistic regression model was used to identify the factors associated with the health impacts of climate change. A P-value less than 0.05 was considered to be statistically significant.
Result: Only 48.5% (95% CI: 44.6, 52.4) of students had good knowledge regarding the health impacts of climate change. Sex of the student—male (AOR = 1.44, 95% CI: 1.032, 2.023), University (AOR = 0.534, 95% CI: 0.360, 0.792), and Department—comprehensive Nursing, (AOR = 0.264, 95% CI: 0.117, 0.592), Midwifery (AOR = 0.201, 95% CI: 0.085, 0.476), and Medical Laboratory (AOR = 0.151, 95% CI: 0.055, 0.413) were significantly associated factors.
Conclusion: The knowledge of the health impacts of climate change among health science students was low. Sex, University, and Department were the associated factors. Hence, undergraduate health science programs should incorporate at least the fundamental details of climate change. Universities should also develop and use a harmonized curriculum.
Introduction
Carbon emissions from the crop, livestock, and industrial sectors are contributing to the rising Earth temperature (1–3). The increase in the earth's average temperature and the consequences that might be related to this temperature rise is called climate change. There are numerous direct and indirect mechanisms through which Climate Change can affect health. On the one hand, extreme weather events like draughts, flooding, and heat waves cause a direct increase in mortality. On the other hand, inconsistent rainfall pattern results in a lack of safe and adequate water supply and leads to a rise in diseases related to poor personal hygiene and environmental sanitation. Respiratory and cardiovascular diseases and death can also be stimulated and aggravated by higher temperatures. Likewise, the distribution of disease reservoirs such as mosquitoes can be affected by small changes in rainfall patterns and/or temperature, which can then affect the magnitude and distribution of vector-borne diseases (4, 5).
Even though all people are at risk of being negatively affected by climate change, some groups of people are more vulnerable than others. Low-income countries and urban areas could be affected to a greater extent mostly because their weak health system and infrastructure are least prepared to respond and adapt to the changes in climate and subsequent changes in health and disease patterns. Globally, children and the elderly are the most vulnerable to the diseases that climate change is likely to cause and influence (6).
Climate change is also considered a significant threat to the fight to improve the health, particularly of poor people in developing countries. According to World Health Organization (WHO) estimates, “climate change will cause an additional 250,000 deaths per year between 2030 and 2050 (7). More specifically, WHO has estimated that climate change will lead to approximately 38,000 additional deaths due to heat exposure in elderly people, 48,000 deaths due to diarrhea 60,000 deaths due to malaria, and 95,000 deaths due to childhood undernutrition”. Apart from a high number of expected deaths, climate change is estimated that by 2030, the damage to health will cost us between $2–4 billion per year (4, 8).
The United Nations adopted the Sustainable Development Goals (SDGs) in 2015 as a global call to action to end poverty, protect the planet, and guarantee that by 2030 everyone will live in peace and prosperity. It has 17 goals with goal number 13 being Climate Action. It advocates that the world can make the necessary changes to protect the planet through urgent and collective action that links education, innovation, and adherence to our climate commitments. Hence, an up-to-date and validated knowledge of Climate Change is a necessary precursor for people to adapt appropriately and be able to play one's role in a very productive way. Graduating health science students (particularly students to become public health professionals), as they have been assimilating cutting-edge evidence regarding the health impacts of climate change as well as are at the forefront of community service, possess an undeniable capacity and responsibility to disseminate health information and education regarding the devastating direct and indirect health impacts of climate change (9). Even though there are a reasonable number of studies in developed countries, the knowledge of the health impacts of climate change among health science students in most sub-Saharan African countries was not studied at all (10).
The World Health Organization has called for health professionals to act as leaders in establishing climate-informed health systems by engaging in health and climate research, adopting sustainable healthcare practices, and designing climate-centered health programs. A study conducted in 2017 suggests that increased knowledge about climate change and its health impacts would motivate health students and/or health professionals to adopt sustainable practices such as efficient waste management in the clinical environment, to help build climate-resilient health systems, and educate patients and visitors regarding the potential threats, health impacts, and mitigation strategies of climate change (11).
Furthermore, educational curriculums that focus on the health impacts of climate change and sustainability to health care in undergraduate health programs will drive health science students to challenge unsustainable clinical practices that might increase the greenhouse gases emitted during, for example, the combustion of large volumes of clinical wastes. Hence, assessing the knowledge of health students who soon will be joining the healthcare system will play a critical role in combating the impacts of climate change (5). In Ethiopia, although a few prior researches have studied the knowledge of the health impacts of climate change among the general public, none of them were conducted among University students of health sciences. A single and outdated study done nine years ago (12) existed and it is not a multi-centered study. Considering these facts, the current multi-centered research aimed at assessing the knowledge of the health impacts of climate change and associated factors among health science students in the Universities of Amhara region.
Methods
Study setting
There are 13 Regions in Ethiopia and Amhara Region is one of the largest region in the Country. It is located in northern Ethiopia. The Regional Government of Amhara has its seat in Bahir Dar, the region's capital. The largest inland body of water in Ethiopia (i.e., Lake Tana), and Semien Mountains National Park, home to Ethiopia's highest point, Ras Dashan, are all located in the. The region is bordered by the Tigray region to the north, the Benishangul-Gumuz to the west and southwest, the Oromia region to the south, and Sudan to the west and northwest.
Universities in Ethiopia are classified by the Ethiopian Ministry of Education (EMoE), according to their excellence. According to the EMoE, there are a total of 8 Universities that are categorized as research institutions, 17 Universities classified as applied institutions, and 21 Universities categorized under general institutions. The difference in the classification of Universities strictly determines their quality, capacity, and international reputation. Research Universities/Institutions generally have more capacity (in terms of the number of student and programs the University can handle), more quality (in terms of educational quality as well as the composition and number of academicians and researchers), and consequently, retain better international reputation than applied, and general Universities in the country (13).
In the Amhara region, there are 10 Government Universities and the study was conducted in the three randomly selected (using lottery method) universities namely University of Gondar, Debre Berhan University, and Bahir Dar University. The University of Gondar and Bahir Dar University are among research institutions while Debre Berhan University is among the applied institution. The former two are found 734 Km and 557 Km far from Addis Ababa, respectively. Debre Berhan University is found only 131 Km far from the Addis Ababa. The study was conducted among undergraduate health science students who are in their final semester of study.
Study design and period
An institution based cross-sectional study was conducted among undergraduate health science students in government Universities found in the Amhara region from 15 February, 2023 to 15 March, 2023.
Population
Source population of this study were all undergraduate health science students who are in their final semester of studies and enrolled in the Universities of Amhara region, whereas, the study population were the undergraduate health science students who are in their final semester of their study and enrolled in the three sampled Universities of Amhara region.
Sample size determinations
The sample size was determined using a single population proportion formula. Since there is no recent published study, the extent of knowledge of the health impact of climate change among study participants was taken as 50%. The confidence level was fixed to be 95% and 10% non-response rate with a design effect of 1.5 was used.
Where, n = sample size
Z = 1.96 at confidence level of 95%
P = The proportion of knowledge towards the health impacts of Climate Change (50%)
W = The margin of error to be tolerated as 5%
D = The design effect to be taken as 1.5, since multi stage cluster sampling technique was used.
Then,
Sampling method and procedure
Multi-stage cluster sampling technique was used. In the first stage, three Universities namely Debre Berhan University, Bahir Dar University, and University of Gondar were randomly selected from the 10 Universities in the region. In the second stage, the number of students to be taken from each University was determined by dividing the total number of students within a selected University by the total number of health science students in all of the three Universities and multiplying by the calculated sample size (635). Accordingly, 251, 206, and 178 students were recruited from the University of Gondar, Debre Berhan University, and Bahir Dar University respectively (Figure 1).
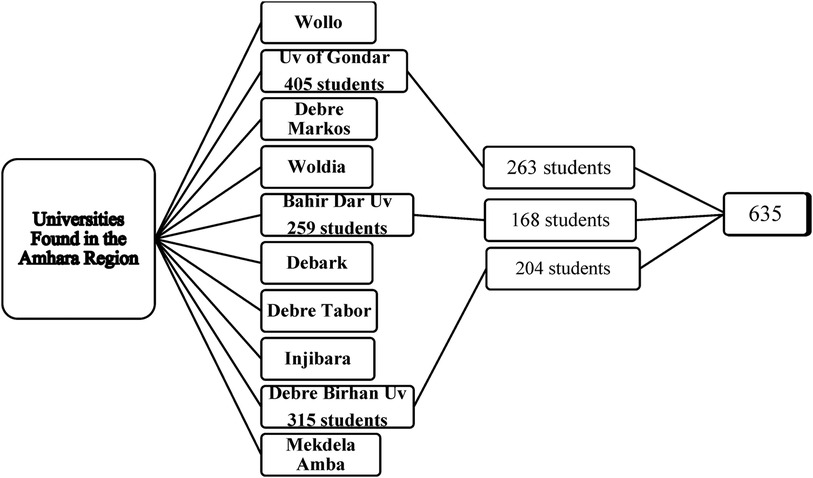
Figure 1 Sampling procedure of the knowledge towards the health impacts of climate change among undergraduate health science students in universities of Amhara region (N = 618).
To representatively and proportionally select participant students from their respective departments, the number of students from each department in each University was calculated by dividing the number of students within each department by the total number of health science students in that particular University and multiplying it by the total sample size to be taken from that University (calculated by previous calculation for each University) (Annex 1). Sampling frame was prepared by taking the list of all undergraduate students from their respective departments. Finally, in order to recruit students who participated in the study, the students’ identity (ID) numbers were entered into an online random number generator software. The students whose ID numbers were selected by the computer were approached with the help of class-representative students and invited to participate in the study. The students id number were then deleted immediately before the analysis, to keep anonymity and confidentiality.
Eligibility criteria
This study included Students who are in their final semester of undergraduate study, students of both sex, and students from departments that are being delivered in at least two of the study Universities. Whereas, students who were not available and who were unable to communicate during the data collection period were excluded from the study.
Study variables
The response variable of the study was “knowledge” of the health impacts of Climate Change, a variable with two outcomes (Good Knowledge and Poor Knowledge). It was measured by using 26 closed-ended questions that were designed to measure students’ knowledge of the causes/reasons of climate change, effects of climate change, and health impacts of climate change. Every question had a “Yes”, “No”, and “I do not Know” answers. A correct answers were scored as “one” and incorrect answers (including both “No” and “I do not Know”) were scored as “zero”. Then, the response of each student was computed by a statistical software (Stata) and the mean value of students’ score (which was 13) was used as a cut-off point to separate students with “Good” and “Poor” knowledge towards the health impacts of climate change. After a thorough and careful review of similar literatures, Age of the student, Sex of the student, University of the students, Department of the student, and the usual information source of the student were included as an independent variables in the study.
Data collection tool and procedure
The design and development of the questionnaire was done in four phases. In the first phase, we conducted a thorough literature review to synthesize and adapt the questionnaire from available relevant literatures. Twenty-Five closed-ended questions were developed in English during this phase. In the second phase, we tried to manually validate the contents of the questionnaire by requesting the professional comment of two experts in the field (i.e., an environmental health and global health experts) from the University of Gondar. The experts provided their professional judgment about the semantics and content of the scale addition, evaluation of the structure of the questionnaire, understanding of the items, and analysis of the format and presentation of the questionnaires as well. In this evaluation process, the experts recommended the addition of 1 item and removal of unnecessary details from a couple of questions with a remark of “might give un unnecessary hints for the students towards the correct answers”.
Accepting the provided suggestions, In the third phase, the tool was pre-tested among 5% of the calculated sample size (32 students) at the Debre Markos University, a University other than those sampled to the study. This pilot study was intended to make sure that the respondents would understand the questions easily and clearly. Finally, we proceeded to the statistical validation of the questionnaire with the analysis of internal reliability (Cronbach's alpha). The Cronbach's alpha coefficient reached a value of 0.884, which makes the knowledge towards the health impacts of climate change assessment questionnaire a reliable instrument (Annex 2).
The data were collected by paper-based self-administered structured questionnaire. Once the data collection process was ended, data completeness was checked. Data entry was performed using the EpiData v.7 data manager software and finally was exported to Stata software for the final analysis. Academicians with a position of Graduate Assistant II (two for each Universities) collected the data. Students of the selected IDs were approached with the help of students’ representatives in each departments of each Universities. The Data collection process was supervised by the principal investigator either through phone calls or physical visits, when and where it is possible.
Data processing and analysis
After the completeness of the data was checked, it was entered into EpiData v.7 data manager software and finally was exported to Stata ™ (V. 14.0) for the final analysis. Descriptive analysis for categorical variables was done using frequency and proportion while for continuous variables, mean with SD were computed. Prior to the final analysis, the dependent variable of greatest interest (Good Knowledge) was coded as 1 and the other class (Poor Knowledge) was coded as 0. Bivariable logistic regression was used to select candidate variables for multivariable logistic regression. Considering the limited number of explanatory variables, a p-value less than 0.25 was used as a cutoff point in the bivariable logistic regression analysis.
Multivariable logistic regression analysis was used to identify independent predictors of Knowledge towards the health impacts of Climate Change and to control confounding variables. The adjusted odds ratios (AOR) with its corresponding 95% confidence interval was presented. Adjusted odds ratio and confidence interval (CI) were used respectively to measure the association between knowledge of the health impact of climate change and predictor variables and their statistical significance in the final model. We used confidence interval to declare a statistical significance in the final model. Hosmer and Lameshow test was used to check the goodness of model.
Ethical approval and consent
The study was conducted based on the Helsinki Declaration of Ethical Principles for Medical Research Involving Human Subjects. Ethical clearance was obtained from the Ethical Review Committee (ERC) of the University of Gondar, College of Medicine and Health Sciences, school of public health. Permission was obtained from the study Universities. Participant students were assured of anonymity regarding the collected data. The identification number of all participant students were deleted immediately before the analyses. All processes and relevant details were conducted in accordance with relevant and approved University guidelines. Prior to administering the questionnaire, the purpose of the study was briefly explained to and oral informed consent was obtained from study participants.
Result
Students’ characteristics
In this work, 18 students of the 635 who were selected to participate did not complete the questionnaire, making the response rate of the study 97.16%. Majority of students 329 (53.2%) were within the age group greater than 25 years. The mean age was 24.6 years with minimum of 22 years and maximum of 28 years old. Out of total study participants, 318 (51.5%) were male students. In this study, students recruited from the University of Gondar were 262 (42.4%), while 195 (31.6%) were from the Debre Berhan University. Relatively large number of students were enrolled from the department of Medicine (24.4%), pharmacy (16%), and comprehensive Nursing (13.9%). In contrast, Anesthesia and Medical lab were departments that contributed relatively small number of students to this study. The widely mentioned (64.7%) information sources regarding climate change was social media and electronic mass media (Table 1).
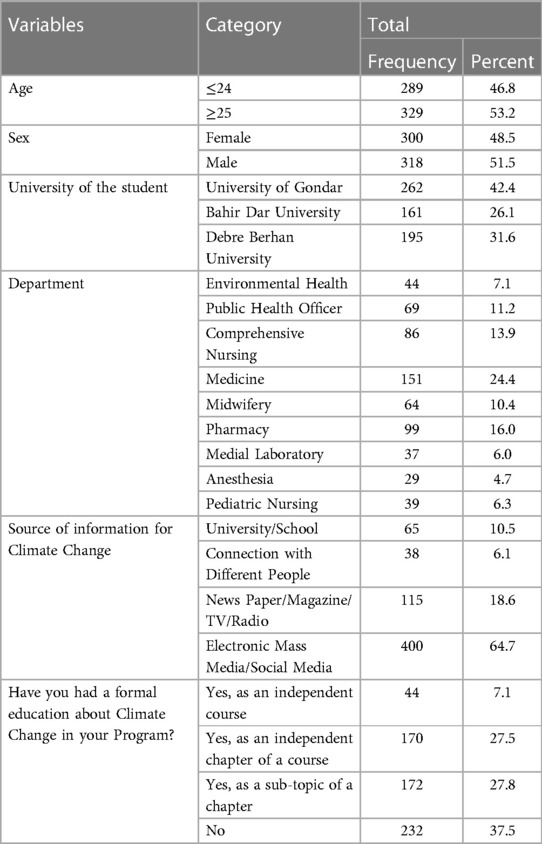
Table 1 Characteristics of study participants in knowledge towards the health impacts of climate change among undergraduate health science students in universities of Amhara region (N = 618).
Climate change and the health impacts of climate change
In this study, 100% of participant students reported that they have heard of climate change and are aware of it. However, only 57% of students think that climate change is a threat to human health. Among those students who think it is a health threat, only 7.1% perceives it as a serious health threat. About 16.3% as somewhat serious health threat, and 30.6% as not a serious threat to health at all (Figure 2). What's more, deforestation was the most frequently identified cause/reason of climate change, about 495 (80.1%) of students recognized it. Excessive carbon emission by developed countries 407 (65.9%) and black smoke of vehicles 335 (54.2%) were the next commonly identified reasons of climate change. In contrast, only 268 (43.4%) and 234 (37.9%) of students recognized rapid urbanization and changes in life style, as well as population growth as reasons of climate change, respectively. Furthermore, excessive hot temperature 510 (82.5%) and the melting of glaciers 529 (85.6%) were the widely recognized effects of climate change. Surprisingly, excessive cold weather, change of the pattern of rain fall, and draught were recognized by less than 50% of students.
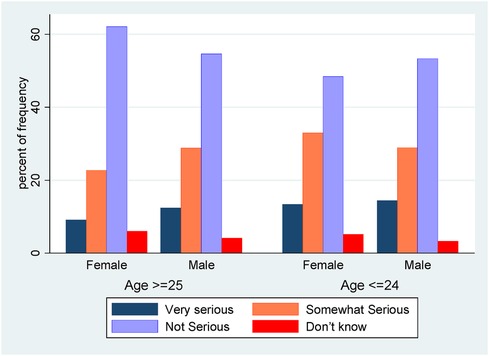
Figure 2 The perception regarding the health threat of climate change among those who believe it indeed is a health threat.
Skin cancer and Injuries from extreme weather conditions such as flooding were the two highly identified health impacts of climate change, with 495 (80.1%) and 521 (84.3%) of correct answers. Scabies and trachoma, and Pneumonia, were the less frequently recognized health impacts of climate change (Table 2).
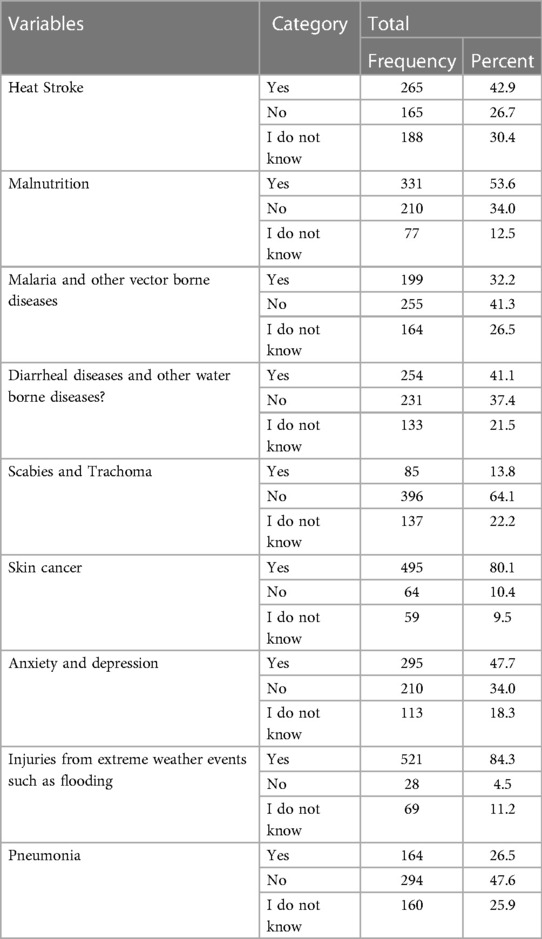
Table 2 The direct and indirect health impacts of climate change in knowledge towards the health impacts of climate change among undergraduate health science students in universities of Amhara region (N = 618).
Knowledge of the health impacts of climate change
The knowledge of the health impacts of climate change was assessed by a validated questionnaire of 26 closed ended questions. According to our finding, only 48.5% (95% CI: 44.6, 52.4) of students had good knowledge regarding the health impacts of climate change. Among students who reported to never taught the topic as an independent course in their program, only 40.9% had good knowledge level. Nearly 318 (51.5%) of students with good knowledge of the health impacts of climate change were males. About 32 (72.7%) and 38 (55.1%) of the environmental health and health officer students had good knowledge respectively, while only 27% and 33.3% of Medical laboratory and Anesthesia students had good knowledge level. About 237 (79%) of students who think that climate change is a threat to human health had a good knowledge level.
Factors associated with knowledge towards the health impacts of climate change
Before multivariable regression was run, all independent variables were tested for crude association with knowledge status by binary logistic regression analysis. In the crude analysis, sex of the student, university of the student, and department of the student had a p-value <0.25 and were included in the multivariable analysis.
In the multivariable analysis, the odds of having good knowledge regarding the health impacts of climate change was 1.44 times higher among male students (AOR = 1.44, 95% CI: 1.032, 2.023) than female students. Holding other variables constant, students studying at the University of Gondar were 1.872 times more likely (AOR = 0.534, 95% CI: 0.360, 0.792) to be knowledgeable than those who studied at the Debre Berhan University (Table 3).
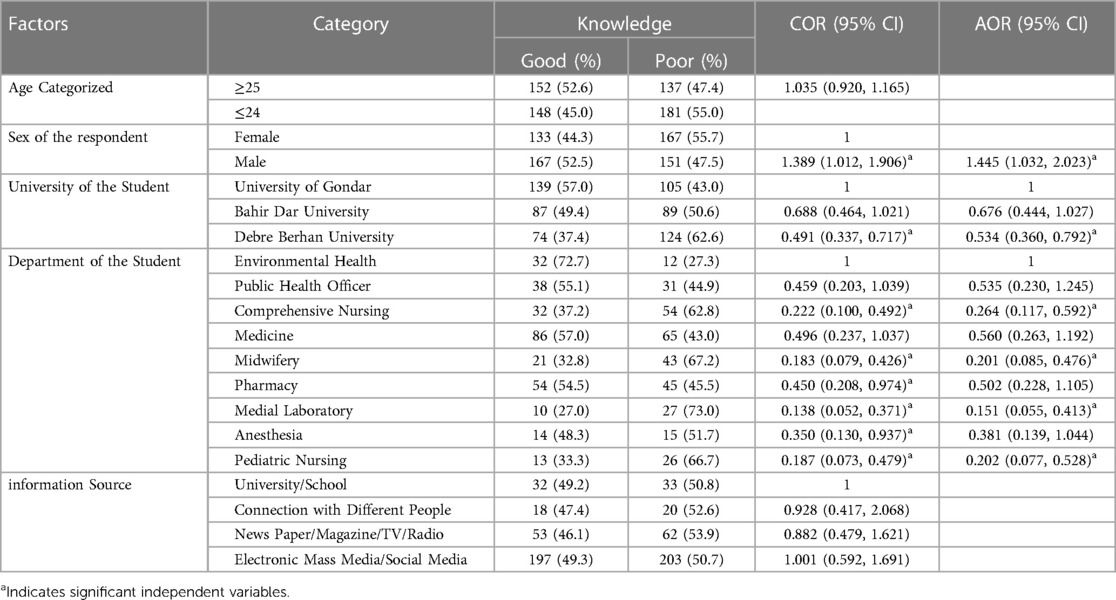
Table 3 Factors associated with the knowledge towards the health impacts of climate change among undergraduate health science students in universities of Amhara region (N = 618).
Department of the students is one of the most important variables where differences in knowledge regarding the health impacts of Climate Change was observed. While being a Health Officer, Medicine, pharmacy, and Anesthesia student did not revealed a significant association, comprehensive Nursing students were 0.26 times less likely to be knowledgeable than environmental health students (AOR = 0.264, 95% CI: 0.117, 0.592). Midwifery students were 79.8% less likely to have good knowledge (AOR = 0.201, 95% CI: 0.085, 0.476) than environmental health students. Medical Laboratory students were 0.15 times (AOR = 0.151, 95% CI: 0.055, 0.413) less likely to have good knowledge towards the health impacts of climate change than environmental health students (Table 3).
The Hosmer and Lemeshow goodness of fit test of the study revealed that the model is a good fit for the data (X2 = 7.36, P-value = 0.498).
Discussion
The World Health Organization has called for health professionals to act as leaders in establishing climate-informed health systems by engaging in health and climate research, adopting sustainable healthcare practices, and designing climate-centered health programs. Increased knowledge about climate change and its health impacts will motivate health students and/or health professionals to help build climate-resilient health systems, to educate patients and visitors regarding the potential threats and health impacts of climate change, and adopt sustainable practices such as efficient waste management in the clinical environment. In addition, educational curriculums that focus on climate change and sustainability to health care in undergraduate health programs will drive health science students to challenge unsustainable clinical practices that might increase the greenhouse gases emitted during, for example, the combustion of large volumes of healthcare wastes (5, 11, 14). In this regard, this study was aimed at assessing knowledge towards the health impacts of climate change and associated factors among undergraduate health science students in universities found in the Amhara Region.
Poor knowledge regarding the health impacts of climate change discourages sustainable behaviors and maintainable healthcare practices that support climate change mitigation strategies. In hospitals, schools, workplaces, and communities, good knowledge promotes eco-friendly practices such as reducing high energy consumption, minimizing clinical waste, and adopting sustainable transportation options within and beyond the hospital environment. By instilling these habits in health science students even before their graduation, good knowledge has the potential to create health professionals and a healthcare system of environmentally conscious (15, 16). In this study, only 48.5% of students had a good knowledge of the health impacts of climate change. This is in line with a study conducted among Italian students, which then concluded that health science students are less prepared and less aware of the consequences and causes of Climate Change than other faculties (17). Contrary to our finding, a study conducted in 2014 in Harar Ethiopia reported a greater knowledge level. This might be due to variations in the knowledge measurement tools and more importantly, differences in study participants. Unlike our study, the study from Harar Ethiopia included postgraduate public health students as well. As graduate programs in public health are designed to equip students with pressing local and global health problems, students are more knowledgeable about global health concerns, like climate change, than any undergraduate health science students (8, 12).
After adjusting for other variables, this study revealed that students in Debre Berhan University were less likely to be knowledgeable than those who studied at the University of Gondar. Primarily, this is most likely because the Environmental health program is not being delivered at the Debre Berhan University and thus, no student from that department at the Debre Berhan University was included in the study. As a result, the magnitude of students with good knowledge level from that University are probably underestimated. Secondly, variations in the program curriculum of the two Universities can explain the discrepancy that is left.
The department/program of students is another important factor that affects the knowledge of the health impacts of climate change. In this study, students from the Department of Nursing, Midwifery, and Medical Lab were less likely to have good knowledge status than the environmental health students. This finding concurs well with a study conducted in Ethiopia where being an environmental health student was strongly associated with good knowledge towards the health impacts of climate change (12). The curriculums of most undergraduate health programs are designed to solely equip students in the specific health profession that they are pursuing. As a result, departments like environmental health and public health officer were programs that incorporated climate change as an independent course or as a chapter of a course in their curriculum. All other health programs’ curricula incorporated climate change only as a sub-topic of a chapter or never incorporated it at all (18). Hence, a more detailed inclusion of content on climate change in every undergraduate health program would have an irreplaceable role in helping the global effort to mitigate the issue of climate change and its health impacts.
Male students, in this study, were more knowledgeable regarding the health impacts of climate change than female students. While this finding is similar to a study conducted in Kenya (19) and Switzerland (20), it differs from the study conducted in Ethiopia (12) and the USA (21). This discrepancy could be explained by the relatively higher tendency of male students to join undergraduate programs such as Environmental health and public health officers that have relatively rich climate change contents in their curriculum. In contrast, female students have a keen inclination towards departments like Nursing and Midwifery. Since the program curriculum of the later departments is aimed to particularly equip students with the necessary clinical skills, students would gain a lesser exposure to the topic of Climate Change than male students. As a result, it is reasonable to expect the knowledge status of female students to be relatively lower than males (18).
In conclusion, climate education and improved knowledge regarding the health impacts of climate change have the capacity to support global and national plans set to build climate-resilient health systems and environment. The Government of Ethiopia has set its climate priorities in The Paris Agreement held in December 2015. The government announced ambitious commitments and emissions cuts such as: reducing emissions by 68 percent by 2030, reforesting and restoring up to 15 million hectares, and 40 adaptation interventions across agriculture, water, forestry, transport, urban, health, and more. National climate change commitments and strategies like this can benefit from increased awareness regarding the health impacts of climate change since it can twist the behavior of people towards eco-friendly day-to-day practices and ultimately hold the lion's share in achieving SDG-13 (22).
Limitations and strengths of the study
This study did not include the variable “residence of the student (part of the country where the student originally came from)”. Due to the fierce racial conflict and tension that has been going on in the country, the ethical review board and we thought that this question would cause a sort of discomfort in the students’ psychology and decided to remove it from the questionnaire. In addition, since the items in the study are close-ended, it might have compromised the participant students’ decision in trying to decide on their right answer. The geographical locations of the three study Universities are classified as urban and this should be considered when interpreting the findings of the study. On the other hand, one of the noticeable strengths of this study is its multicenter-ness, which would increase its generalizability.
Conclusion and recommendation
The proportion of good knowledge towards the health impacts of climate change among health science students was low. Sex, University, and Department of the student were significant factors associated with knowledge towards the health impacts of climate change. Accordingly, all undergraduate health science programs should at least incorporate a comprehensive chapter or a topic that contains details of concerns and impacts of climate change on public health and the implementation of adaptation and mitigation strategies that the health care system can contribute to. One way to do this is the inclusion of the “Climate Change and Public Health” chapter in their environmental health course (environmental health course is incorporated in every health science program curriculum). In addition, onsite environmental assessment of healthcare facilities to identify clinical and environmental practices that contribute to greenhouse gas emissions (for example through the use of greater resources and higher energy consumption during patient care processes) should be considered to be performed by health students as an independent environmental demonstration or as part of their Team Training Program (TTP) and/or Community-Based Training Program (CBTP). This could cement the theoretical aspect of climate change they assimilated into a practical one. Furthermore, Universities should develop and use one, harmonized curriculum for all undergraduate health science programs. This would help them to ascertain their students are competent with the appropriate and up-to-date health issues and advancements that the healthcare sphere is dealing with every day. Lastly, this study recommends further research using longitudinal design to track changes over time with or without qualitative studies to understand the depth of students’ knowledge and attitudes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Gondar, Ethical Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because Because the study involves in adult participants and does not involve any medical interventions.
Author contributions
MA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SW: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Writing – review & editing. MB: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Writing – review & editing. MA: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – review & editing. ND: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – review & editing. HA: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – review & editing. RB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft. FK: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft. HA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft. Sz: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft. AB: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank the staff of Debre Berhan University, Bahir Dar University, and University of Gondar as well as the data collectors, the Amhara Media Corporation (AMECO), and participants for their valuable contribution to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvh.2024.1363395/full#supplementary-material
Abbreviations
AOR, adjusted odds ratio; BDU, Bahir Dar University; CI, confidence interval; COR, crude odds ratio; CBTP, community based training program; DBU, Debre Berhan University; ERC, ethical review committee; ID, identification number; SDGs, sustainable development goals; TTP, team training program; UoG, University of Gondar; WHO, World Health Organization; PHO, Public Health Officer.
References
1. Abbas A, Zhao C, Waseem M, Ahmed khan K, Ahmad R. Analysis of energy input–output of farms and assessment of greenhouse gas emissions: a case study of cotton growers. Front. Environ. Sci. (2022) 9:826838. doi: 10.3389/fenvs.2021.826838
2. Elahi E, Li G, Han X, Zhu W, Liu Y, Cheng A, et al. Decoupling livestock and poultry pollution emissions from industrial development: a step towards reducing environmental emissions. J Environ Manag. (2024) 350:119654. doi: 10.1016/j.jenvman.2023.119654
3. Abbas A, Waseem M, Ahmad R, khan KA, Zhao C, Zhu J. Sensitivity analysis of greenhouse gas emissions at farm level: case study of grain and cash crops. Environ Sci Pollut Res. (2022) 29(54):82559–73. doi: 10.1007/s11356-022-21560-9
4. Skolnik R. In: Lindsey Mawhiney NA, editor. Global Health One Hundred and One. 3rd ed United States of America: Michael Brown (2016). p. 45–6.
5. Rocque RJ, Beaudoin C, Ndjaboue R, Cameron L, Poirier-Bergeron L, Poulin-Rheault RA, et al. Health effects of climate change: an overview of systematic reviews. BMJ Open. (2021) 11(6):e046333. doi: 10.1136/bmjopen-2020-046333
6. Ehsan S, Begum RA, Abdul Maulud KN, Yaseen ZM. Households’ perceptions and socio-economic determinants of climate change awareness: evidence from Selangor coast Malaysia. J Environ Manage. (2022) 316:115261. doi: 10.1016/j.jenvman.2022.115261
7. World Health Organization. COP24 Special Report: Health and Climate Change. Geneva, Switzerland: World Health Organization (2018).
8. World Health Organization. Global Climate Change and Child Health. Geneva, Switzerland: World Health Organization (2019).
9. Elder M, Bartalini A. Assessment of the g20 Countries’ Concrete SDG Implementation Efforts: Policies and Budgets Reported in Their 2016–2018 Voluntary National Reviews: Institute for Global Environmental Strategies. Hayama, Kanagawa, Japan: Institute for Global Environmental Strategies (2019).
10. Sanni O, Salami B, Oluwasina F, Ojo F, Kennedy M. Climate change and African migrant health. Int J Environ Res Public Health. (2022) 19(24):3–4. doi: 10.3390/ijerph192416867
11. Müller L, Kühl M, Kühl SJ. Climate change and health: changes in student environmental knowledge and awareness due to the implementation of a mandatory elective at the medical faculty of Ulm? GMS J Med Educ. (2023) 40(3):Doc32. doi: 10.3205/zma001614
12. Nigatu AS, Asamoah BO, Kloos H. Knowledge and perceptions about the health impact of climate change among health sciences students in Ethiopia: a cross-sectional study. BMC Public Health. (2014) 14(1):1–10. doi: 10.1186/1471-2458-14-587
13. Federal Democratic Republic of Ethiopia, Ministry of Education. Online Fact Sheets about Ethiopian Higher Education Universities. Addis Ababa, Ethiopia: Ministry of Health Ethiopia (2023). Available online at: https://moe.gov.et/fact-sheets (accessed on May 21, 2024)
14. Huang A, Cooke SM, Garsden C, Behne C, Borkoles E. Transitioning to sustainable, climate-resilient healthcare: insights from a health service staff survey in Australia. BMC Health Serv Res. (2024) 24(1):475. doi: 10.1186/s12913-024-10882-8
15. Anderson A. Climate change education for mitigation and adaptation. J Educ Sustain Dev. (2012) 6(2):191–206. doi: 10.1177/0973408212475199
16. Feinstein N, Mach K. Three roles for education in climate change adaptation. Clim Pol. (2020) 20(3):317–22. doi: 10.1080/14693062.2019.1701975
17. Mazzalai E, Chiappetta M, La Torre G. Knowledge on causes and consequences of climate change in a cohort of Italian students. Clin Ter. (2022) 173(5):443–52. doi: 10.7417/CT.2022.2461
18. Aronsson J, Nichols A, Warwick P, Elf M. Awareness and attitudes towards sustainability and climate change amongst students and educators in nursing: a systematic integrative review protocol. Nurs Open. (2022) 9(1):839–44. doi: 10.1002/nop2.1134
19. Ajuang CO, Abuom PO, Bosire EK, Dida GO, Anyona DN. Determinants of climate change awareness level in upper Nyakach division, Kisumu County, Kenya. SpringerPlus. (2016) 5(1):1015. doi: 10.1186/s40064-016-2699-y
20. André H, Gonzalez Holguera J, Depoux A, Pasquier J, Haller DM, Rodondi PY, et al. Talking about climate change and environmental degradation with patients in primary care: a cross-sectional survey on knowledge, potential domains of action and points of view of general practitioners. Int J Environ Res Public Health. (2022) 19(8):7–8. doi: 10.3390/ijerph19084901
21. McCright A. The effects of gender on climate change knowledge and concern in the American public. Popul Environ. (2010) 32(1):1–104. doi: 10.1007/s11111-010-0113-1
Keywords: climate change, health impacts, Amhara region, health science, undergraduate, University, students
Citation: Alemayehu MA, Workie SG, Belew MA, Agimas MC, Derseh NM, Abuhay HW, Berihanu R, Kinfe FT, Abebe HA, zemene S and Bazezew AM (2024) Knowledge towards the health impacts of climate change and associated factors among undergraduate health sciences students in Amhara region: a multi-centered study. Front. Environ. Health 3: 1363395. doi: 10.3389/fenvh.2024.1363395
Received: 30 December 2023; Accepted: 3 July 2024;
Published: 15 July 2024.
Edited by:
Vinoth Kumar Ponnusamy, Kaohsiung Medical University, TaiwanReviewed by:
Michael Schmeltz, California State University, United StatesAdnan Abbas, Nanjing University of Information Science and Technology, China
© 2024 Alemayehu, Workie, Belew, Agimas, Derseh, Abuhay, Berihanu, Kinfe, Abebe, zemene and Bazezew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meron Asmamaw Alemayehu, bWVycnlhbGVtMTAxQGdtYWlsLmNvbQ==; bWVyb24uYXNtYW1hd0B1b2cuZWR1LmV0