 Ashtyn T. Areal1,2
Ashtyn T. Areal1,2 Nidhi Singh1
Nidhi Singh1 Qi Zhao1,3
Qi Zhao1,3 Dietrich Berdel4
Dietrich Berdel4 Sibylle Koletzko5,6Andrea von Berg4Monika Gappa7Joachim Heinrich8,9,10
Sibylle Koletzko5,6Andrea von Berg4Monika Gappa7Joachim Heinrich8,9,10 Marie Standl9,11
Marie Standl9,11 Tamara Schikowski1*
Tamara Schikowski1*
- 1Department of Epidemiology, IUF-Leibniz Research Institute for Environmental Medicine, Düsseldorf, Germany
- 2Department of Epidemiology, Medical Research School, Heinrich-Heine-University, Düsseldorf, Germany
- 3School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, China
- 4Research Institute, Department of Pediatrics, Marien-Hospital Wesel, Wesel, Germany
- 5Department of Pediatrics, Dr. von Hauner Children's Hospital Munich, University Hospital, LMU Munich, Munich, Germany
- 6Department of Pediatrics, Gastroenterology and Nutrition, School of Medicine, Collegium Medicum University of Warmia and Mazury, Olsztyn, Poland
- 7Department of Paediatrics, Evangelisches Krankenhaus, Düsseldorf, Germany
- 8Institute and Clinic for Occupational, Social and Environmental Medicine, University Hospital, LMU Munich, Munich, Germany
- 9German Center for Lung Research (DZL), Munich, Germany
- 10Allergy and Lung Health Unit, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, VIC, Australia
- 11Helmholtz Zentrum München—German Research Center for Environmental Health, Institute of Epidemiology, Neuherberg, Germany
Background: Relative humidity (RH) and air pollution significantly affect respiratory health. However, how RH and air pollution interact and modify each other and affect lung function in adolescence is largely unknown. This study assesses the interactive association of RH and air pollution on lung function, i.e. forced vital capacity (FVC) and forced expiratory volume in one second (FEV1), in German adolescents.
Methods: A total of 2,116 participants with available spirometry measurements (z-scores of FEV1 and FVC) were included from the 15-year follow-up of the German GINIplus and LISA birth cohort. Daily environmental exposure data included RH, ozone (O3), nitrogen dioxide (NO2), and particulate matter <2.5 µm (PM2.5). Linear models were fitted to assess the main associations of RH, air pollution, and maximum temperature (Tmax) an interaction term between one-day moving average of RH (Lag01) and a categorical air pollution term was then included to assess the modifying association of air pollution on RH and was adjusted for study location, season and chronic respiratory disease (CRD) status. Effect modification was performed for sex and CRD. The results are presented as beta coefficients (ß) and 95% confidence intervals (95% CI).
Results: A 5% increase in RH was associated with an increase in FEV1 (ß = 0.040–0.045; 95% CI: 0.008 to 0.076) and FVC (ß = 0.007–0.012; 95% CI: −0.023 to 0.045) in the main associations models. In the interaction models, there was a significant decrease in FEV1 (ß = −0.211; 95% CI: −0.361 to −0.062) and FVC (ß = −0.258; 95% CI: −0.403 to −0.0113) per 5% increase in RH on high O3 days compared to the reference category; while there was a non-significant trend towards a decrease in FEV1 on high PM2.5 and NO2 days. Female participants were more likely to experience a decrease in FEV1 than male participants on high-pollution days.
Conclusions: Air pollution interacts and modifies the association of weather on lung function in this cohort of German adolescents. An increase in RH on high air pollution exposure days was associated with a decrease in lung function in German adolescents. Female participants were more sensitive to RH and air pollution.
1. Introduction
Investigating the relationship between weather parameters and respiratory health outcomes due to the effects of climate change is a rapidly evolving field of study. Relative humidity (RH) has rarely been the focus of environmental exposure-health studies and has largely only been used as a confounding variable in multi-exposure/temperature-health studies (1, 2). However, it is known that temperature, RH, and air pollution interact in different ways while having both individual and, potentially, interactive associations with respiratory health (2). Therefore, insights into the potential associations of different weather parameters and air pollutants with lung health are important; therefore, surrogate subclinical endpoints such as lung function and biomarkers need to be investigated.
To determine a person's respiratory health, lung function tests are conducted (3). Two indicators of lung function are forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC). Both of these surrogate subclinical endpoints allow us to assess different components of lung function and to diagnose lung disease. While the short-term association of environmental factors on lung function has been described in children, young and older adults, there is limited evidence for adolescents. However, biological development occurs rapidly during adolescence, making it crucial to understand environment associations with adolescent health (4). Regarding respiratory health, adolescence is a period of rapid lung development due to accelerated physical growth; additionally, during this period, asthma becomes more common in females than in males as puberty induces physical changes that lower airway resistance in males while increasing airway resistance in females (4, 5).
Individual environmental factors are associated with lung health, and as such are associated with lung function, in different ways; low levels of RH (<40%), which indicates that the air is dry, are associated with causing dryness in the respiratory tract which then damages lung tissue, while high levels (>60%) have been associated with increased mucous production (6). High and low temperatures have both been associated with an increase in respiratory rate, exacerbation of chronic respiratory disease, and respiratory mortality (7). Air pollutants have consistently been associated with a decrease in lung function (8, 9). While there is extensive research on the individual association of air pollution on lung function, the same cannot be said of RH; additionally, air pollution, RH, and temperature interact or modify each other's associations with human health.
Climate change and it's determining environmental factors present a unique situation in that they intersect with many existing vulnerabilities (e.g., including geography, urban/rural, sex, and chronic diseases) that impact adolescent health (4). Therefore, understanding how short-term environmental exposures interact or modify each other and how they are associated with lung function during such a crucial time in human development is of the utmost importance. In this study, we aimed to assess the short-term individual and interactive associations of relative humidity and air pollution with lung function in a subset of German adolescents.
2. Methods and material
2.1. Study population
The present study utilises the data collected for two ongoing German population-based birth cohort studies which recruited healthy full-term neonates with normal birthweight. The first is the German Infant Study on the Influence of Nutrition Intervention plus Air Pollution and Genetics on Allergy Development (GINIplus), which recruited a total of 5,991 neonates in Munich and Wesel between September 1995 and July 1998. The second is the influence of Lifestyle factors on the development of the Immune System and Allergies in East and West Germany Study (LISA) (10) which recruited a total of 3,097 neonates in Bad Honnef, Leipzig, Munich and Wesel between November 1997 and January 1999. The study areas of the cohorts are shown in Supplementary Figure S1. Participant data were collected at birth and ages 6, 10, and 15, and were then due to their harmonised design, pooled for Wesel (GINIplus/LISA North: n = 3,390) and Munich (GINIplus/LISA South: n = 4,413). Parents completed questionnaires that collected data on respiratory conditions and covariates such as parental/personal smoking and socioeconomic status (parental education). Further details of recruitment and follow-up to 15 years have been presented elsewhere (11). The present analysis employs data from the 15-year follow-up assessments for both cohorts in Munich and Wesel. This analytic sample was restricted to 1,236 children from Munich and 880 children from Wesel with complete spirometry (forced vital capacity [FVC] and forced expiratory volume in one second [FEV1]) and environmental exposure data. Ethical approval was granted by the Bavarian Board of Physicians (10,090 and 12,067), Board of Physicians of North-Rhine Westphalia (20101424 and 2012446), and Board of Physicians of Saxony (EK-BR-02/13–1). The parents of participants provided written informed consent at each of the study phases with participants also providing consent at the 15-year follow-up.
2.2. Assessment of lung function
Spirometric measurements (FEV1 and FVC) during adolescence were conducted between 2011 and 2013 following the guidelines of the American Thoracic Society and European Respiratory Society (12). Detailed operation procedures for lung function measurements have been described previously (13). Any respiratory tract infections, personal smoking and anti-inflammatory medications were recorded. To adequately compare the impacts of environmental exposures on FEV1 and FVC, both measurements were converted into z-scores using LUng function NOrmal values for KIDs in Germany (LUNOKID) scale (14). The LUNOKID study was designed to provide reliable reference values of spirometry for German children and adolescents which adjusted for the non-linear associations of age, height, and sex (15–17).
2.3. Assessment of environmental exposures
Weather parameters (daily maximum [Tmax] and, minimum temperature [Tmin], mean temperature [Tmean], and RH) were obtained for Munich and Wesel from the German Weather Service's high-resolution reanalysis system COSMO-REA6 at a spatial resolution of 6 × 6 km (18). Short-term daily air pollution exposure was assessed as average concentrations of 24 h O3, NO2 and PM2.5. The air pollutant exposures at participants' residential addresses were estimated at a spatial resolution of 2 × 2 km by chemical transport models and data provided by the German Environment Agency [Umwelt Bundesamt, UBA (19)]. The warm season was defined as May to October and the cold season as November to April.
2.4. Statistical analysis
As there were minimal differences in RH between the study sites in Munich and Wesel, it was decided to pool the participants to increase the power of the statistical analysis as in previous studies (20, 21). To ensure that all potential variables were considered, we used correlation coefficients, multicollinearity tests, adjusted R-squared, Akaike information criterion (AIC) and p values <0.05 for variable selection. Due to the small number of participants diagnosed with asthma, we created a Chronic Respiratory Disease (CRD) variable that combined a history of asthma and asthma at the time of examination, with chronic respiratory symptoms and conditions associated with asthma, i.e., history of chronic bronchitis, a history of chronic wheezing, and/or, chronic bronchitis and/or wheeze at the time of assessment. We graphically assessed the association between the short-term environmental exposures and the outcomes and found that all variables showed a linear association; therefore, we used multivariable linear models to quantify the main associations of short-term exposure RH (one-day moving average; Lag01), Tmax (lowest AIC of all temperature variables) and air pollution on FEV1 and FVC; separate models were created for different air pollutants (O3, NO2 and PM2.5). All models (the main model and interactive model) were mutually adjusted for each environmental factor, CRD (Yes as the reference category), study location (Munich as the reference category), and season (warm season as the reference category). To assess the interactive associations between RH and air pollution, we used RH parameters as a continuous variable and air pollutants as a categorical variable: Low (<5th percentile), Medium (5–95th percentile), and High (>95th percentile); the cut-offs were: PM2.5 = 2.71 µg/m3 and 22.08 µg/m3, O3 = 10.15 µg/m3 and 82.60 µg/m3 and NO2 = 4.90 µg/m3 and 37.85 µg/m3. We chose “Medium” as the reference category, as it represented the most common exposure levels while “Low” represented optimum exposure and “High” represented non-optimum exposure. We did not adjust for age, sex, height, or weight in the main model as the chosen outcomes (FEV1 and FVC) were estimated following standard guidelines accounting for these variables. Effect modification was examined by sex (female/male), and history of CRD.
2.5. Sensitivity analysis
To test the robustness of the core model, several sensitivity analyses were conducted. First, we explored the possibility of lag associations for up to 5 days (Lag05). Second, we explored the change in the interaction between RH and air pollution by redefining cut-offs for air pollution categories. At first, the cutoff was set below the 10th percentile (Low) and above the 90th percentile (High), and in the second stage, it was set below the 25th percentile (Low) and above the 75th percentile (High). Third, extended models were performed by additionally adjusting for the association of age, sex, CRD, BMI, the highest parental education level (less than 10 years, 10 years, and more than 10 years), and active parental smoking (yes or no).
All the results were presented as beta coefficient (ß) with a 95% confidence interval (CI) per five percent increase in RH. All statistical analysis was conducted in R version 4.0.4 (22). Results above zero indicate improved lung function; a two-sided p-value <0.05 was considered statistically significant.
3. Results
3.1. Characteristics of study population and exposures
A total of 2,116 participants, with a mean age of 15.24 [standard deviation (SD) ± 0.31], of which approximately 51% were female, had complete spirometric measurements and environmental exposure data; 1,236 (58.41%) participants were from Munich and 880 (41.59%) participants were from Wesel (Table 1). Approximately, 42% of participants reported suffering from/or having had a CRD (e.g., diagnosed asthma, chronic wheeze, chronic bronchitis), with there being slightly more cases in Wesel than in Munich (42.84% vs. 41.59%) (Table 1). This was supported by the spirometric measurements that showed that participants in Wesel had lower FEV1 (−0.103 vs. 0.199) and FVC (−0.128 vs. 0.025) z-scores than Munich (Table 1). Approximately, 67% of participants had parents with a high educational level; this was most apparent in participants from Munich (Table 1). The majority of participants fell within the normal BMI category (69.57%), with participants from Wesel slightly more likely to be overweight (12.84% vs. 8.41%); while more participants from Munich were underweight (21.28% vs. 18.64%) (Table 1). Passive smoking exposure was reported by 16% of participants, with participants from Wesel reporting more exposure to passive smoking than Munich (Table 1).
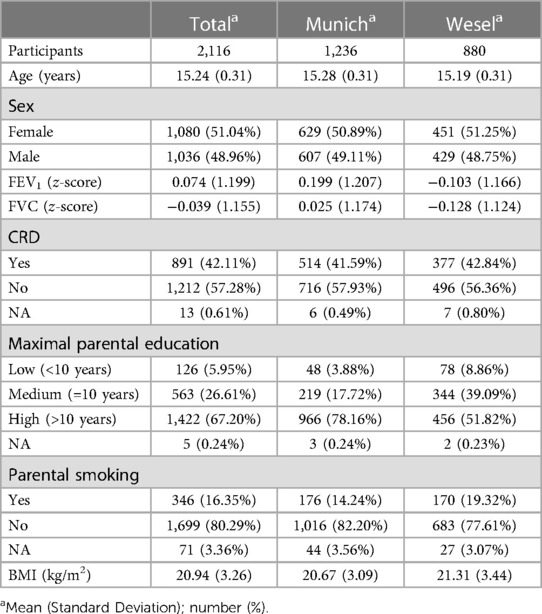
Table 1. Summary of population characteristics.
Weather parameters were similar in Munich and Wesel. The average RH was 74.92% and 75.43% in Munich and Wesel respectively (Table 2). Tmax was similar in Munich and Wesel however, Wesel was marginally warmer (Table 2). O3 and NO2 were approximately the same in both Munich and Wesel (Table 2). PM2.5 was higher in Wesel than in Munich (12.75 µg/m3 vs. 9.42 µg/m3) (Table 2). The majority of participants had their spirometry measurements taken in the warm season (63.75%) (Table 2).
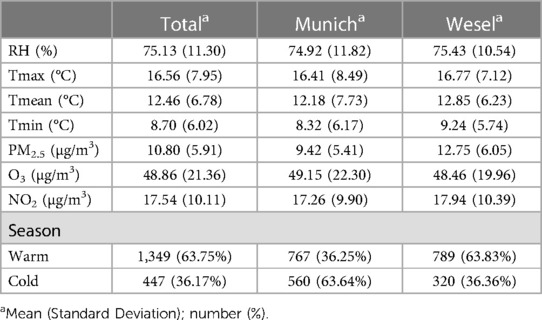
Table 2. Summary of environmental exposure on the day of examination.
3.2. Main associations of RH, Tmax, and air pollution on FEV1 and FVC
Collinearity tests showed that all included variables were not highly correlated and multicollinearity tests for the models showed that all variables were below 3, indicating no multicollinearity issue in the models. A 5% increase in RH was consistently associated with an increase in FEV1 (ß = 0.040 to 0.044; 95% CI: 0.009 to 0.076); Tmax was also consistently associated was an increase in FEV1 (ß = 0.014 to 0.015; 95% CI: 0.003 to 0.027) (Table 3). No significant associations were found for O3 (ß = −0.0003; 95% CI: −0.004 to 0.003), NO2 (ß = 0.005; 95% CI:−0.0005 to 0.011) and PM2.5 (ß = 0.006; 95% CI: −0.002 to 0.015) (Table 3). No significant associations were observed for FVC (Table 3).
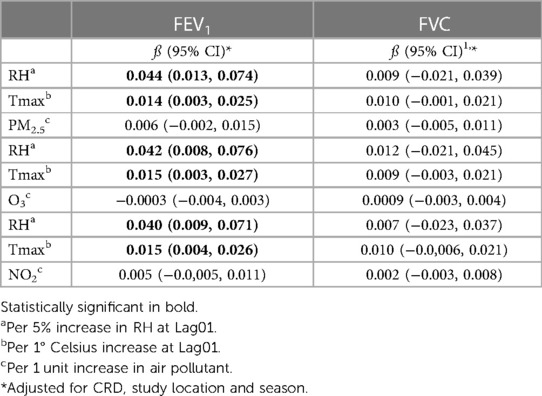
Table 3. A table showing the beta coefficient and 95% CI of the main associations of RH, Tmax, and air pollution on FEV1 and FVC in a cohort of German adolescents.
3.3. Interactive and modifying association of air pollution on RH
On days with high levels of O3, there was a decrease in FEV1 (ß = −0.211; 95% CI: −0.361 to −0.062) and FVC (ß = −0.258; 95% CI: −0.404 to −0.113) per 5% increase in RH compared to the reference category (Figures 1, 2; Supplementary Table S1); there was no significant finding for low O3 days. However, the interactive term for O3 was statistically significant for both FEV1 (p = 0.0121) and FVC (p = 0.002) (Supplementary Table S1). No significant findings were found for interactions between RH and PM2.5 or RH and NO2 on high or low air pollution days compared to the reference category (Figures 1, 2; Supplementary Table S1).
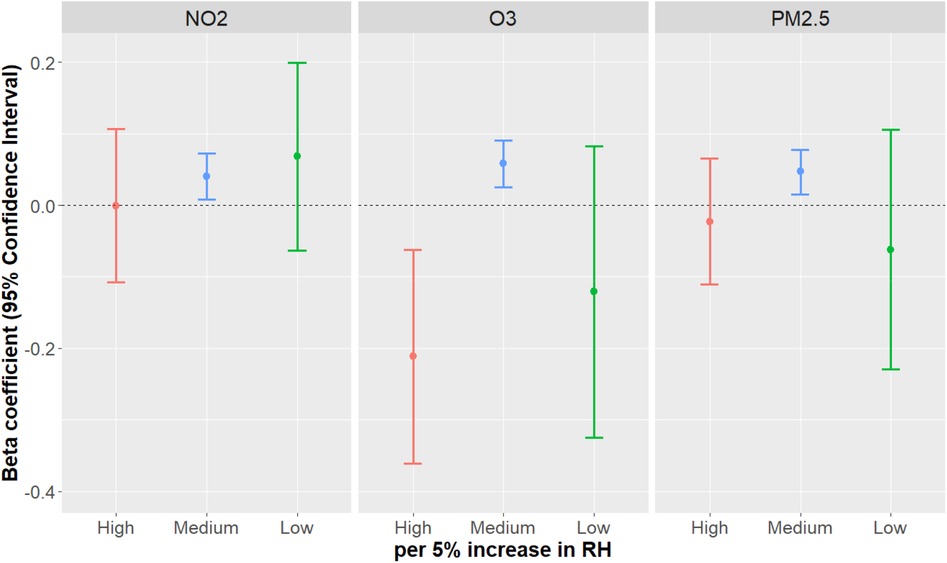
Figure 1. The association of RH when modified by categorical air pollution (reference category: medium) on FEV1.
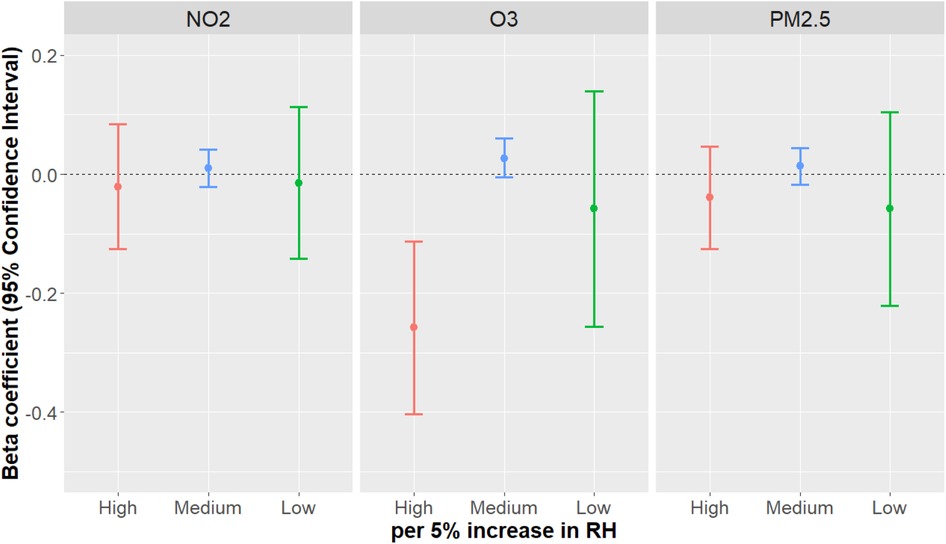
Figure 2. The association of RH when modified by categorical air pollution (reference category: medium) on FVC.
3.4. Effect modification of CRD and sex on FEV1 and FVC
RH and temperature tended to show stronger protective associations with lung function in female participants than in male participants in the stratified analysis (Supplementary Table S2). However, a contrasting result was observed in interaction models, which shows female participants, in general, were more likely to experience a decrease in FEV1 (Supplementary Table S3), yet male participants on high O3 days in particular when compared to the reference category, experienced a greater decrease in FVC than their counterparts respectively.
In both, with and without CRD, the main association model shows an increase in RH and temperature was associated with an increase in FEV1 (Supplementary Table S4), whereas, FVC did not show any significant associations. In our interaction models, we found a decrease in FEV1 and FVC per 5% increase in RH on both high and low O3 days when compared to the reference category; this association was more apparent in those without CRD than those with CRD (Supplementary Table S5). For NO2 there was a non-significant trend towards a decrease in FEV1 and FVC in those with CRD (Supplementary Table S5).
3.5. Sensitivity analysis
Results for the different lag period shows that the values were consistent across all lags for RH and temperature. Secondly, the direction of the association was consistent at different cut-offs for the air pollutants (i.e., 25th and 95th, 10th and 90th); additionally, the strength of the association was consistent (Supplementary Tables S6, S7). The results for the extended model show that the associations of RH, temperature, and air pollution with FEV1 and FVC remain unchanged after additionally adjusting for age, sex, BMI, parental education, second-hand smoking, family history of respiratory disease, and anti-inflammatory medications (data not shown).
4. Discussion
In recent years, climate change has adversely affected human health. It is known that meteorology variables and air pollution are associated with each other, with RH modifying the toxicity of air pollutants as well as stagnant meteorological conditions, i.e., high relative humidity and temperature, encouraging increased pollutant emissions and secondary particle formations (23); however, how these environmental factors modify and interact with each other concerning health is largely unknown. In this study, we assessed how air pollution modifies and interacts with weather variables and how this impacts lung function. We found that the main associations of RH and Tmax showed statistically significant protective associations on lung function, while O3, NO2, and PM2.5 failed to reach statistical significance. In the interaction models we found that exposure high levels of O3 modified the protective association of RH and that this interaction caused a decrease in lung function. Typically, O3 and RH have an inverse relationship, however, in recent years, due to the effects of climate change, this relationship is changing with O3 and RH peaks occurring concurrently along with temperature (Supplementary Figures S1–S3), as we have seen in our data set.
Additionally, female participants were more sensitive to the main associations of weather variables than male participants. Biological sex might also modify the associations of environmental factors on respiratory health. At 15 years of age, females are typically in the late- or post-stages of puberty and have reached their peak lung function, while males are typically in an earlier stage and are still experiencing an increase in lung function (24). Before puberty, females typically have higher lung function than males, however, after puberty, males have higher lung function than females. The increase in lung size, and as such the thoracic cage, can lower airway resistance, while the increase in high-fat mass in females is associated with increases in lung inflammation and airway resistance (25). Furthermore, females have slower blood flow, indicating that females are more sensitive to changes in outdoor temperature than males, as cold exposure causes their skin temperature to lower even further, especially in the extremities (26, 27). These arguments complement the findings from the present analysis which found lung function in females to be more vulnerable to temperature than in males.
With regard to CRD, typically the associations of weather and air pollution were stronger in those without CRD. However, in interaction models between RH and NO2, as well as RH and O3, we did see a decrease in lung function in those without CRD (28, 29).
According to the Köppen-Geiger climate classification, most of Germany falls into what is called a cfb climate (30). By definition, cfb climate means locations whose climates are temperate with a warm summer and cool winter that has year-round precipitation and high levels of humidity; these locations usually have an average temperature below 22°C and do not experience extreme heat or extreme cold (30, 31).
Regarding air pollution, the 95th percentile of O3 (82.60 µg/m3) in Wesel and Munich is already below that of the World Health organisations (WHO) updated 2021 air quality guidelines (100 µg/m3); while, PM2.5 (22.08 µg/m3) and NO2 (37.85 µg/m3), are above the WHO air quality guidelines (15 µg/m3 and 25 µg/m3) (32). Considering that our results showed that air pollution modifies and has an adverse association on lung function, by meeting the WHO's air quality guideline targets, there could be an improvement in lung function. However, O3, which is already below the WHO guidelines was found to decrease lung function with increasing RH even with low O3 exposure. This suggests that further reduction in O3 is needed. Reduction in air pollution emissions and secondary particle formation can occur by addressing the sources of air pollution in our study, namely traffic-related emissions and agricultural emissions (33).
This is the first study that investigates the short-term interactive association of RH and air pollution on lung function in adolescents in Germany. Due to the lack of studies on this topic, it is complex to place our study into context as (1) research primarily has looked at the long-term associations of temperature and air pollution rather than immediate short-term impacts of temperature and air pollution, (2) there is primarily a focus on children or the elderly and not on adolescents which is a stage of major biological change which is not truly comparable to either adults or children, and (3) weather parameters, RH in particular, are often only used as confounders in epidemiological analyses and as such, the association of these variables is poorly understood, and (4) modifying associations between RH and air pollution are largely unknown. A previous study by Lepeule, Litonjua (34) looked at a cohort of elderly men from the United States of America (USA) and investigated the association of short-term temperature and RH on lung function. This study found that there was a decrease in FEV1 and FVC with a 5% increase in both temperature and RH. Our results differed in that we found that an increase in temperature and RH were associated with an increase in FEV1 in male adolescents. In contrast, we found lower FVC with increasing temperatures and RH in males which is in line with the results reported for older males. The BAMSE birth cohort by Schultz, Hallberg (35) found that FEV1 was potentially more sensitive to environmental exposures than FVC which is consistent with our results. The most likely reason for differences in our results compared to those in literature can be attributed to different climates (i.e., Germany vs. the USA), the age of our participants (i.e., adolescents vs. middle-aged and elderly adults), and differences in behaviour and personal characteristics.
It is beyond the scope of this study to identify the exact biological mechanisms that may underlie the association of weather parameters and lung function. Potentially, during periods of high temperatures, e.g., heat waves, the body is unable to efficiently thermoregulate; this leads to excessive sweating and increased dehydration. which exacerbates CRD due to increased airway resistance within the lungs (10, 36, 37). During low temperatures, the veins and arteries narrow, causing an increase in cardiac and respiratory workload (38, 39).
Research on the association of environmental factors on adolescent health is limited. Future research should aim to further investigate the immediate short-term associations of weather parameters on respiratory health in adolescents as well as continue assessing the potential interactive associations between environmental factors which would allow us to consolidate research on the association of multiple environmental exposures on respiratory health.
This analysis has several strengths: The data were obtained from large, well-characterised birth cohorts. Short-term air pollution and meteorological exposures were estimated by well-validated high-resolution models. Additionally, this is one of the first studies to focus on RH and temperature associations on lung function in adolescents as well as one of the first studies to investigate the potential interactive associations of RH and air pollution on lung function. This helps to identify potential environmental impacts during a time of great biological importance due to rapid growth during adolescence.
However, we also need to acknowledge some limitations. Firstly, although the GINIplus/LISA cohort has been well described, the findings might not be generalisable to adolescents in other countries as this cohort was exposed to relatively low air pollution levels compared to adolescents in other geographical regions. Additionally, Germany typically has lower temperatures, but high RH which further limits generalisability to adolescents in other countries. Secondly, we did not have access to indoor temperature and humidity which means this is limited to outdoor exposure. Lastly, there is limited literature on the interactive association of RH and air pollution on lung function, which makes placing our results in context, complex.
5. Conclusions
This analysis of a large data set of German adolescents from two birth cohorts demonstrates that there is an interaction between climate variables and lung function which is different from that observed in other age groups. The interactive association of RH and air pollution is associated with a decline in lung function in this cohort of German adolescents. These findings may have important clinical implications as the association of short-term weather variables, which influence climate, on adolescent health is largely unknown; additionally, how RH and air pollution interact with each other and how this interaction is associated with health is poorly understood. This study fills important gaps in the evidence of climate change's effects on health. Future research should focus further not just on the potential associations of extreme climate events on health but also on the short- and long-term associations of daily weather and air pollution interactions on health in adolescents.
Data availability statement
The datasets presented in this article are not readily available because they are raw personal data from the cohort and not for public viewing. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethical approval was granted by the Bavarian Board of Physicians (10090 and 12067), Board of Physicians of North-Rhine Westphalia (20101424 and 2012446), and Board of Physicians of Saxony (EK-BR-02/13-1). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AA: Conceptualisation, Formal analysis, methodology, Visualisation, Writing – original draft, Writing – review & editing. NS: Supervision, Validation, Methodology, Writing – review & editing. QZ: Methodology, Writing – review & editing. DB: Investigation, Writing – review & editing. SK: Investigation, Writing – review & editing. Av: Investigation, Writing – review & editing. MG: Investigation, Writing – review & editing. JH: Investigation, Writing – review & editing. MS: Data curation, Investigation, Writing – review & editing. TS: Data Curation, Investigation, Conceptualisation, Supervision, Validation, Methodology, Writing – review & editing. All authors contributed to the article and approved the submitted version.
Funding
The GINIplus study was mainly supported for the first 3 years by the Federal Ministry for Education, Science, Research and Technology (interventional arm) and Helmholtz Zentrum Munich (former GSF) (observational arm). The 4-year, 6-year, 10-year and 15-year follow-up examinations of the GINIplus study were covered from the respective budgets of the 5-study centres [Helmholtz Zentrum Munich (former GSF), Research Institute at Marien-Hospital Wesel, LMU Munich, TU Munich and from 6 years onwards also from the IUF—Leibniz Research-Institute for Environmental Medicine at the University of Düsseldorf] and a grant from the Federal Ministry for Environment (IUF Düsseldorf, FKZ 20462296). Furthermore, the 15-year follow-up examination of the GINIplus study was supported by the Commission of the European Communities, the 7th Framework Program: MeDALL project, and as well by the companies Mead Johnson and Nestlé. The LISA study was mainly supported by grants from the Federal Ministry for Education, Science, Research and Technology and in addition from Helmholtz Zentrum Munich (former GSF), Helmholtz Centre for Environmental Research—UFZ, Leipzig, Research Institute at Marien-Hospital Wesel, Pediatric Practice, Bad Honnef for the first 2 years. The 4-year, 6-year, 10-year and 15-year follow-up examinations of the LISA study were covered from the respective budgets of the involved partners (Helmholtz Zentrum Munich (former GSF), Helmholtz Centre for Environmental Research—UFZ, Leipzig, Research Institute at Marien-Hospital Wesel, Pediatric Practice, Bad Honnef, IUF—Leibniz-Research Institute for Environmental Medicine at the University of Düsseldorf) and in addition by a grant from the Federal Ministry for Environment (IUF Düsseldorf, FKZ 20462296). Further, the 15-year follow-up examination of the LISA study was supported by the Commission of the European Communities, the 7th Framework Program: MeDALL project. The IUF is funded by the federal and state governments—the Ministry of Culture and Science of North Rhine-Westphalia (MKW) and the Federal Ministry of Education and Research (BMBF). Mead Johnson and Nestlé were not involved in the study design, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors would like to thank all the families for their participation in the GINIplus and LISA studies. Furthermore, we thank all members of the GINIplus and LISA Study Groups for their excellent work. The GINIplus Study group consists of the following: Institute of Epidemiology, Helmholtz Zentrum München, German Research Center for Environmental Health, Neuherberg (Heinrich J, Brüske I, Schulz H, Flexeder C, Zeller C, Standl M, Schnappinger M, Ferland M, Thiering E, Tiesler C); formerly: Department of Pediatrics, Marien-Hospital, Wesel (Berdel D, von Berg A); Ludwig-Maximilians-University of Munich, Dr von Hauner Children's Hospital (Koletzko S); Child and Adolescent Medicine, University Hospital rechts der Isar of the Technical University Munich (Bauer CP, Hoffmann U); Evangelical Hospital Düsseldorf (Gappa M, Libuda L); IUF- Environmental Health Research Institute, Düsseldorf (Schikowski T, Link E, Klümper C, Krämer U, Sugiri D). The LISA Study group consists of the following: Helmholtz Zentrum München, German Research Center for Environmental Health, Institute of Epidemiology, Munich (Heinrich J, Schnappinger M, Brüske I, Ferland M, Schulz H, Zeller C, Standl M, Thiering E, Tiesler C, Flexeder C); Department of Pediatrics, Municipal Hospital “St. Georg”, Leipzig (Borte M, Diez U, Dorn C, Braun E); Marien Hospital Wesel, Department of Pediatrics, Wesel (von Berg A, Berdel D, Stiers G, Maas B); Pediatric Practice, Bad Honnef (Schaaf B); Helmholtz Centre of Environmental Research—UFZ, Department of Environmental Immunology/Core Facility Studies, Leipzig (Lehmann I, Bauer M, Röder S, Schilde M, Nowak M, Herberth G, Müller J); Technical University Munich, Department of Pediatrics, Munich (Hoffmann U, Paschke M, Marra S); Clinical Research Group Molecular Dermatology, Department of Dermatology and Allergy, Technische Universität München (TUM), Munich (Ollert M, J. Grosch). We thank all study members, staff involved in data collection, and the respective funding bodies. During the last decades, many scientists, study nurses and laboratories were involved in conducting the studies. We are most grateful for all the individuals who participated in the study over decades. We also wish to thank the Deutsche Wetterdienst and the DeutscheUmweltbundesamt (UBA) for providing data from the COSMO-REA6 model and the UBA air pollution models. We would like to thank Dr. Kathrin Wolf for her assistance in preparing the exposure data for participants in Munich.
Conflict of interest
SK has received a speaker's fee from Danone, Jansson, Sanofi, Pfizer, and Takeda. Additionally, she has participated on the advisory board for Abbvie, Danone, Jansson, GSK, Pfizer, Sanofi, and Takeda.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors QZ and NS declared that they were editorial board members of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fenvh.2023.1250523/full#supplementary-material
References
1. Lim CC, Hayes RB, Ahn J, Shao Y, Silverman DT, Jones RR, et al. Long-term exposure to ozone and cause-specific mortality risk in the United States. Am J Respir Crit Care Med. (2019) 200(8):1022–31. doi: 10.1164/rccm.201806-1161OC
2. Wu S, Deng F, Hao Y, Wang X, Zheng C, Lv H, et al. Fine particulate matter, temperature, and lung function in healthy adults: findings from the hvnr study. Chemosphere. (2014) 108:168–74. doi: 10.1016/j.chemosphere.2014.01.032
3. Cotes JE, Chinn DJ, Miller MR. Lung function: Physiology, measurement and application in medicine. John Wiley & Sons (2009).
4. McGushin A, Graef V, Ngendahayo C, Timilsina S, Ameratunga S, Baltag V, et al. Adolescent well-being and the climate crisis. Partnership Maternal Newborn Child Health UHL. (2020).
5. Trivedi M, Denton E. Asthma in children and adults-what are the differences and what can they tell US about asthma? Front Pediatr. (2019) 7:256. doi: 10.3389/fped.2019.00256
6. Guarnieri G, Olivieri B, Senna G, Vianello A. Relative humidity and its impact on the immune system and infections. Int J Mol Sci. (2023) 24(11):9456. doi: 10.3390/ijms24119456
7. Rice MB, Li W, Wilker EH, Gold DR, Schwartz J, Zanobetti A, et al. Association of outdoor temperature with lung function in a temperate climate. Eur Respir J. (2019) 53(1). doi: 10.1183/13993003.00612-2018
8. Rice MB, Ljungman PL, Wilker EH, Gold DR, Schwartz JD, Koutrakis P, et al. Short-term exposure to air pollution and lung function in the framingham heart study. Am J Respir Crit Care Med. (2013) 188(11):1351–7. doi: 10.1164/rccm.201308-1414OC
9. Garcia E, Rice MB, Gold DR. Air pollution and lung function in children. J Allergy Clin Immunol. (2021) 148(1):1–14. doi: 10.1016/j.jaci.2021.05.006
10. Leon LR. Thermoregulatory responses to environmental toxicants: the interaction of thermal stress and toxicant exposure. Toxicol Appl Pharmacol. (2008) 233(1):146–61. doi: 10.1016/j.taap.2008.01.012
11. Heinrich J, Brüske I, Cramer C, Hoffmann U, Schnappinger M, Schaaf B, et al. Giniplus and lisaplus—design and selected results of two German birth cohorts about natural course of atopic diseases and their determinants. Allergol Select. (2017) 1(1):85–95. doi: 10.5414/alx01455e
12. American Thoracic Society. European respiratory society. Ats/ers recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005 [see comment]. Am J Respir Crit Care Med. (2005) 171(8):912–30. doi: 10.1164/rccm.200406-710ST
13. Fuertes E, Bracher J, Flexeder C, Markevych I, Klümper C, Hoffmann B, et al. Long-term air pollution exposure and lung function in 15 year-old adolescents living in an urban and rural area in Germany: the giniplus and lisaplus cohorts. Int J Hyg Environ Health. (2015) 218(7):656–65. doi: 10.1016/j.ijheh.2015.07.003
14. Zhao Q, Kress S, Markevych I, Berdel D, von Berg A, Gappa M, et al. Air pollution during infancy and lung function development into adolescence: the giniplus/lisa birth cohorts study. Environ Int. (2021) 146:106195. doi: 10.1016/j.envint.2020.106195
15. Hüls A, Krämer U, Gappa M, Müller-Brandes C, Schikowski T, von Berg A, et al. Age dependency of gli reference values compared with paediatric lung function data in two German studies (giniplus and lunokid). PLoS One. (2016) 11(7):e0159678. doi: 10.1371/journal.pone.0159678
16. Hüls A, Krämer U, Gappa M, Müller-Brandes C, Seitner-Sorge G, von Berg A, et al. New spirometric reference values for children and adolescents in Germany considering height and non-linear age effects: the lunokid-study. Pneumologie (Stuttgart Germany). (2013) 67(3):141–9. doi: 10.1055/s-0032-1326090
17. Müller-Brandes C, Krämer U, Gappa M, Seitner-Sorge G, Hüls A, von Berg A, et al. Lunokid: can numerical American thoracic society/European respiratory society quality criteria replace visual inspection of spirometry? Eur Respir J. (2014) 43(5):1347–56. doi: 10.1183/09031936.00058813
18. Bollmeyer C, Keller JD, Ohlwein C, Wahl S, Crewell S, Friederichs P, et al. Towards a high-resolution regional reanalysis for the European cordex domain. Q J R Metereol Soc. (2015) 141(686):1–15. doi: 10.1002/qj.2486
19. Minkos A, Dauert U, Feigenspan S, Kessenger S. Air quality 2016: preliminary evaluation. In: Umweltbundesamt [German environment agency]. Dessau-Roßlau: Umweltbundesamt (2017). 24.
20. Zhao T, Markevych I, Standl M, Schulte-Körne G, Schikowski T, Berdel D, et al. Ambient ozone exposure and depressive symptoms in adolescents: results of the giniplus and lisa birth cohorts. Environ Res. (2019) 170:73–81. doi: 10.1016/j.envres.2018.12.014
21. Fuertes E, Standl M, Forns J, Berdel D, Garcia-Aymerich J, Markevych I, et al. Traffic-related air pollution and hyperactivity/inattention, dyslexia and dyscalculia in adolescents of the German giniplus and lisaplus birth cohorts. Environ Int. (2016) 97:85–92. doi: 10.1016/j.envint.2016.10.017
22. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing, (2021).
23. Han B, Wang Y, Zhang R, Yang W, Ma Z, Geng W, et al. Comparative statistical models for estimating potential roles of relative humidity and temperature on the concentrations of secondary inorganic aerosol: statistical insights on air pollution episodes at Beijing during January 2013. Atmos Environ. (2019) 212:11–21. doi: 10.1016/j.atmosenv.2019.05.025
24. Best O, Ban S. Adolescence: physical changes and neurological development. Br J Nurs. (2021) 30(5):272–5. doi: 10.12968/bjon.2021.30.5.272
25. Kim JH, Kim JA, Ha EK, Jee HM, Lee SW, Jung MK, et al. Sex differences in body composition affect total airway resistance during puberty. BMC Pediatr. (2022) 22(1):143. doi: 10.1186/s12887-022-03198-1
26. Yang L, Zhao S, Gao S, Zhang H, Arens E, Zhai Y. Gender differences in metabolic rates and thermal comfort in sedentary young males and females at various temperatures. Energy Build. (2021) 251:111360. doi: 10.1016/j.enbuild.2021.111360
27. Sarlani E, Farooq N, Greenspan JD. Gender and laterality differences in thermosensation throughout the perceptible range. Pain. (2003) 106(1–2):9–18. doi: 10.1016/s0304-3959(03)00211-2
28. Cecchi L, Annesi-Maesano I, d'Amato G. News on climate change, air pollution, and allergic triggers of asthma. J Investig Allergol Clin Immunol. (2018) 28(2):91–7. doi: 10.18176/jiaci.0228
29. Sunyer J, Basagaña X, Belmonte J, Antó JM. Effect of nitrogen dioxide and ozone on the risk of dying in patients with severe asthma. Thorax. (2002) 57(8):687. doi: 10.1136/thorax.57.8.687
30. Beck HE, Zimmermann NE, McVicar TR, Vergopolan N, Berg A, Wood EF. Present and future Köppen-geiger climate classification maps at 1-km resolution. Sci Data. (2018) 5(1):180214. doi: 10.1038/sdata.2018.214
31. Pidwirny M. Physical Geography Lab Manual: the Atmosphere and Biosphere: our planet earth (2021). Available at: https://pressbooks.bccampus.ca/physgeoglabmanual1/
32. World Health Organization. Who global air quality guidelines: Particulate matter (Pm2.5 and Pm10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. Geneva: World Health Organization (2021).
33. Gehring U, Gruzieva O, Agius RM, Beelen R, Custovic A, Cyrys J, et al. Air pollution exposure and lung function in children: the escape project. Environ Health Perspect. (2013) 121(11–12):1357–64. doi: 10.1289/ehp.1306770
34. Lepeule J, Litonjua AA, Gasparrini A, Koutrakis P, Sparrow D, Vokonas PS, et al. Lung function association with outdoor temperature and relative humidity and its interaction with air pollution in the elderly. Environ Res. (2018) 165:110–7. doi: 10.1016/j.envres.2018.03.039
35. Schultz ES, Hallberg J, Andersson N, Thacher JD, Pershagen G, Bellander T, et al. Early life determinants of lung function change from childhood to adolescence. Respir Med. (2018) 139:48–54. doi: 10.1016/j.rmed.2018.04.009
36. Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Beagley J, Belesova K, et al. The 2020 report of the lancet countdown on health and climate change: responding to converging crises. Lancet. (2020) 397:129–70. doi: 10.1016/S0140-6736(20)32290-X
37. Bernstein AS, Rice MB. Lungs in a warming world: climate change and respiratory health. Chest. (2013) 143(5):1455–9. doi: 10.1378/chest.12-2384
38. Seltenrich N. Between extremes: health effects of heat and cold. Environ Health Perspect. (2015) 123(11):A275–A279. doi: 10.1289/ehp.123-A275
Keywords: relative humidity, air pollution, lung function, adolescents, cohort studies, environmental epidemiology
Citation: Areal AT, Singh N, Zhao Q, Berdel D, Koletzko S, von Berg A, Gappa M, Heinrich J, Standl M and Schikowski T (2023) The association of relative humidity and air pollution interaction on lung function in adolescents. Front. Environ. Health 2:1250523. doi: 10.3389/fenvh.2023.1250523
Received: 30 June 2023; Accepted: 8 November 2023;
Published: 23 November 2023.
Edited by:
Marie-Abele Bind, Massachusetts General Hospital and Harvard Medical School, United StatesReviewed by:
Antonis Analitis, National and Kapodistrian University of Athens, GreeceZhicheng Du, Sun Yat-sen University, China
© 2023 Areal, Singh, Zhao, Berdel, Koletzko, von Berg, Gappa, Heinrich, Standl and Schikowski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tamara Schikowski dGFtYXJhLnNjaGlrb3dza2lAaXVmLWR1ZXNzZWxkb3JmLmRl