 Hong Yi1†
Hong Yi1† Lin Chen
Lin Chen Xiaoyan Chen
Xiaoyan Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Endocrinol. , 18 March 2025
Sec. Reproduction
Volume 16 - 2025 | https://doi.org/10.3389/fendo.2025.1560981
Resistant ovary syndrome is a rare endocrinological disorder characterized by elevated serum gonadotropins and normal ovarian reserves. The leading causes of this condition include FSHR mutations, and autoimmune disorders. Due to follicle maturation defects and anovulation, these patients have menstrual disturbances and infertility. Endocrinological disorders can be treated by regular hormone replacement therapy. However, there is no consensus regarding the infertility issues and current treatment remains experimental with controlled ovarian stimulation (COS) and in vitro maturation. Herein, we conducted a review of the current literature, which concludes that: 1) patients with FSHR mutations had very poor COS outcomes; 2) follicle-stimulating hormone and luteinizing hormone levels poorly predict COS outcomes; 3) both recombinant and urinary gonadotropins may be effective in COS; 4) the dosage of exogenous gonadotropins is not the key to successful COS; 5) in vitro maturation is a feasible option for patients carrying FSHR mutations or unsuccessful COS cycles.
Resistant ovary syndrome (ROS), originally described by Jones et al. in 1969 (1), is also known as ovarian insensitive syndrome and Savage syndrome. It is a rare reproductive disorder characterized by a seemingly conflicting picture of hypergonadotropic hypogonadism and normal ovarian reserves. Women with ROS generally have anovulation disorders because of ovarian hyposensitivity to endogenous gonadotropins (2), which further cause endocrinological disturbance, primary or secondary amenorrhea, and infertility. With normal ovarian reserves, ROS differs from premature ovarian insufficiency, which represents the loss of ovarian functions before the age of 40 due to the depletion of primordial follicles. However, ovarian follicle maturation is impaired due to various etiologies. Regular hormone replacement therapy can treat endocrinological and menstrual disorders, but parenthood planning remains a tricky problem. The core of fertility management is to resume follicle maturation and the current strategies include controlled ovarian stimulation (COS) (3–6), in vitro maturation (IVM) (7), and using donor oocytes (8). Yet, fertility management in ROS is still experimental due to its heterogenous etiology and low incidence. This review focuses on the pathogenesis and fertility management of ROS and aims to summarize the common rules of fertility management based on available evidence.
The etiology of ROS remains largely unclear to date. In the initial report, Jones et al. (1) proposed two hypotheses: 1) there were biologically inactive follicle-stimulating hormone (FSH) molecules in serum; and 2) the follicle apparatus itself was defective and resistant to FSH stimulation. Current studies on the pathogenesis of ROS include follicle-stimulating hormone receptor (FSHR) mutations and autoimmune disorders.
An FSHR-inactivating mutation is the most studied mechanism in ROS. In 1995, Aittomaki et al. discovered the first FSHR mutation (c.556C>T, p.Ala189Val) in hypergonadotropic ovarian dysgenesis families (9). The mutation was located at the 7th exon of FSHR and caused a substitution of Ala by Val at the extracellular domain of the FSH receptor, which disrupted the cell surface targeting of the receptor and abolished cAMP production upon FSH stimulation despite the affinity with FSH remaining unaltered (9, 10). Thereafter, more than 200 mutations in FSHR have been discovered according to the CliniVar database, however, the clinical information was not documented in most cases. In total, 30 mutations were reported with detailed phenotypes.
These mutations involved multiple domains of the FSH receptor, and most mutations have been confirmed to impair the functions of the receptor in in vitro assays. In Fshr knock-out mouse models, preantral follicles were present in the ovaries, indicating that preantral follicle development does depend not on FSH receptors. However, no follicle progressed to the antral stages, suggesting an FSH receptor-dependent mechanism in follicle maturation (11). Similarly, equivalent small follicles were observed in ovary sections between patients with and without FSHR mutations, however, no follicles beyond the antral stages were observed in patients with FSHR mutations.
In 1982, Chiauzzi et al. identified circulating immunoglobulins that inhibited FSH binding to its receptor in two patients with hypergonadotropic amenorrhea who were complicated with myasthenia gravis (12). This discovery was subsequently validated in a larger cohort consisting of 23 patients who were previously diagnosed with ROS, whereas the immunoglobulins were negative in the control group (13). Rogenhofer and colleagues reported a patient with ROS whose serum showed strong reactivity against human menopausal gonadotropins (hMG) but no reactivity to recombinant FSH (rFSH). Interestingly, the patient achieved pregnancy after controlled ovarian stimulation with a daily injection of hMG (225 IU/d) and rFSH (75IU/d) (5). Li et al. detected circulating autoimmune antibodies against FSH receptors in a patient with ROS who was successfully managed with exogenous gonadotropins and dexamethasone (4). In addition, Chitnis et al. isolated and purified an oligopeptide from human ovarian follicular fluid, which was demonstrated to inhibit the binding of FSH to ovarian granulosa cells in vitro and to induce atresia in developing follicles in rodent models (14). This oligopeptide may represent a potential contributing factor to gonadotropin resistance and ovarian resistance syndrome, highlighting its relevance in the pathophysiology of these conditions.
ROS shares similar clinical manifestations with premature ovarian insufficiency (POI), including menstrual disturbance (oligomenorrhea or amenorrhea), hypergonadotropinemia, decreased circulating estradiol levels, and fertility issues. However, they differ in ovarian reserves as POI represents the absolute depletion of ovarian primordial follicles at early ages whereas ROS is characterized by normal ovarian reserves, which can be distinguished by serum anti-mullerian hormone (AMH) levels and antral follicle count under transvaginal ultrasound scans. In 1972, Van Campenhout et al. (2) proposed that the diagnosis of ROS must satisfy the following three criteria: 1) endogenous hypergonadotropinemia; 2) presence of normal ovarian follicles; and 3) hyposensitivity of the ovaries to excessive stimulation of exogenous human gonadotropins. However, there were many cases that satisfied the first two criteria but showed normal ovarian responsiveness to exogenous human gonadotropins (3–5). Currently, there is no consensus regarding the diagnosis criteria of ROS but all cases to date satisfied the first two criteria.
Patients with ROS are primarily affected by anovulation disorder-associated menstrual disturbances, endocrinological disorders, and infertility. The first two symptoms are successfully managed with hormonal replacement therapy, whereas fertility management has been a tricky issue. Currently, there is no systematic strategy for ROS-related infertility due to heterogeneous etiology and low incidence. Potential strategies include controlled ovarian hyperstimulation (5), in vitro maturation (7), and using donor oocytes (8). However, these methods were attempted in separate cases with varying clinical outcomes. ROS patients who have undergone fertility management are summarized in Table 1, including 16 cases with FSHR mutations. COS and IVM were the leading strategies, and the common themes (or outcomes) of these reports are presented below.
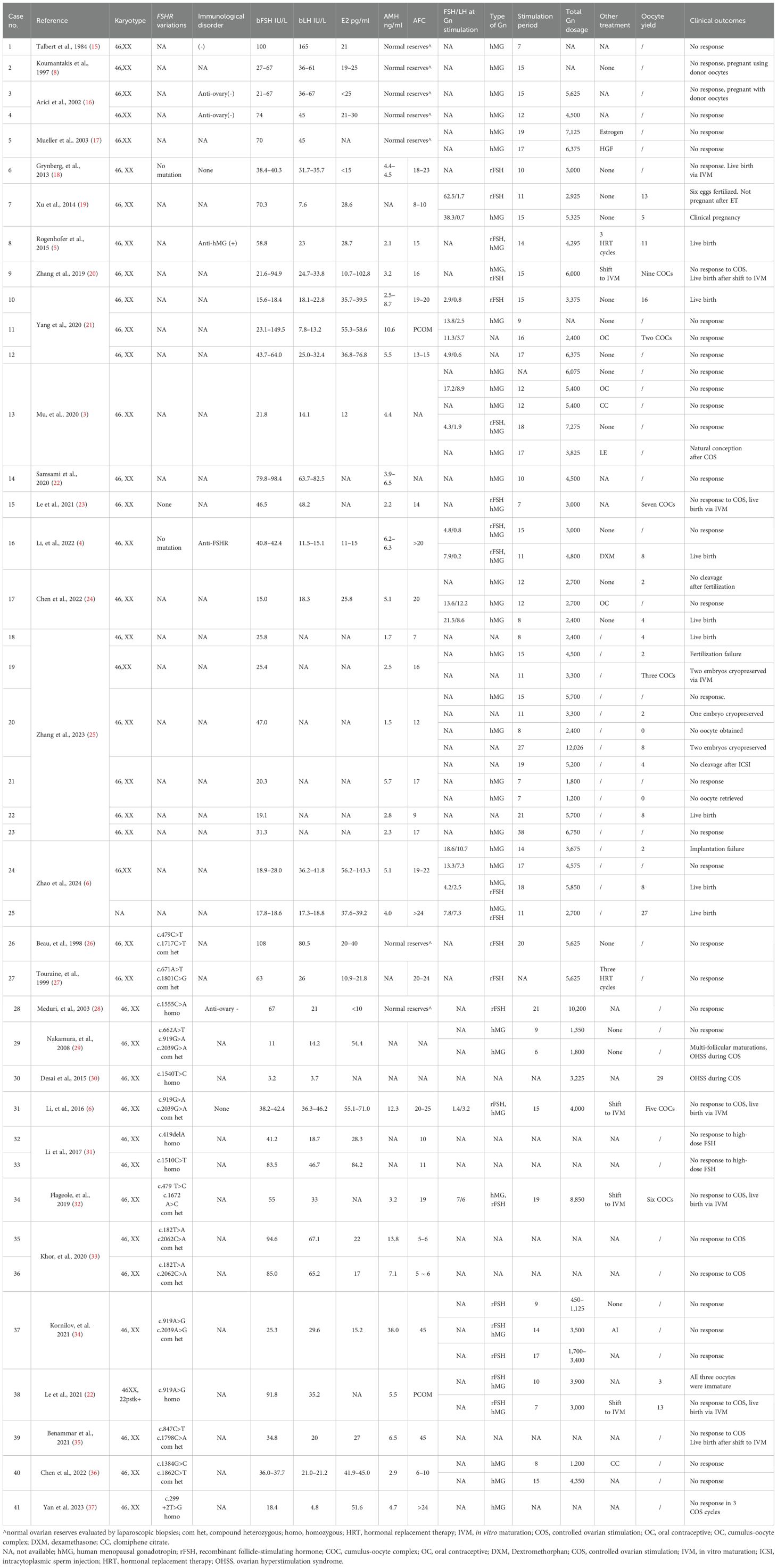
Table 1. Summary of the application of controlled ovarian stimulation in resistant ovary syndrome.
To date, more than 30 inactivating mutations of FSHR with demonstrated phenotypes in women have been discovered (38, 39), most of which have been confirmed to undermine FSH receptor functions by in vitro assays, and there were 16 cases (cases 26–41) who received COS (Table 1) for infertility management. Excessive exogenous gonadotropins were administrated but dominant follicles were observed in only two patients (cases 30 and 38) (23, 30). Case 30 had a homozygous c.1540 T>C mutation of the FSHR and she developed ovarian hyperstimulation syndrome during ovarian stimulation. However, in vitro assays confirmed that the mutation enhanced the function of FSH receptors, indicating that it is an activating mutation. In addition, she sought assisted reproductive technology (ART) treatment due to tubal and male factors rather than ovulatory disorders (30). Similar findings were also observed in case 29, a patient with compound heterozygous c.662A>T, c.919G>A, and c.2039G>A mutations in FSHR who also developed ovarian hyperstimulation syndrome during ovarian stimulation (29), but no experimental evidence regarding the impact of these mutations on receptor functions was available. Interestingly, in case 38, a patient with a homozygous c.919A>G mutation in FSHR was unresponsive to exogenous FSH in a 7-day stimulation according to follicle size under transvaginal ultrasound scans and serum estradiol levels, but four mature eggs, along with four metaphase I (MI) oocytes and five germinal vesicles (GV), were retrieved after being triggered with hCG for IVM purposes (23). This result may be explained by residual FSHR function despite its mutations; however, no experimental evidence was available.
Furthermore, there were many patients with FHSR mutations for whom ovarian stimulation was not performed because of their younger age or lack of pregnancy desire despite clinical and experimental evidence showing that mutations compromise FSHR functions (30, 33, 40–46). Among the cases where ovarian stimulation with exogeneous gonadotropins was effective, genetic tests regarding FSHR were negative (4, 18) or were not performed (5, 6, 25). It is worth noting the obviously divided ovarian responsiveness to endogenous and exogenous gonadotropins in some cases (cases 7, 8, 10, 16, 24, and 25; Table 1). These cases were normal or high ovarian responders when exogenous gonadotropin was administrated despite high endogenous gonadotropin levels (4–6, 19, 21). Therefore, abnormalities of the endogenous gonadotropins may be the cause, as proposed by Jones and Moraes in the initial report (1). In conclusion, for patients with homozygous and compound heterozygous FSHR inactivating mutations, a trial of controlled ovarian stimulation is of limited value.
For those without an FHSR mutation or where genetic tests are not available, ovarian stimulation is still worth trying for pregnancy management. Many women have achieved pregnancies and live births with the use of appropriate ovarian stimulation. According to Huang et al., basal FSH levels were negatively associated with COS outcomes. The higher the FSH levels, the poorer the outcomes (47). However, the conclusion was limited by its sample size, which included only six patients, five of whom were carrying FSHR mutations.
A downregulation protocol was the most popular protocol in patients with ROS, intended to improve ovarian responsiveness to FSH stimulation by inhibiting serum gonadotropin levels (48), and similar strategies included pretreatment with oral contraceptives (OC). However, it seems that FSH and luteinizing hormone (LH) levels (after pretreatment) were not correlated with COS outcomes in previous studies. In case 7 (Table 1), for example, FSH/LH levels before and after downregulation were as high as 70.3/7.6 IU/L, 62.5/1.7 IU/L, and 38.3/0.7 IU/L, respectively. However, 13 and 5 oocytes were obtained after ovarian stimulation with exogenous gonadotropins (19). Similar results were also observed in other cases (cases 17 and 24; Table 1) (6, 24). However, successful inhibition of serum gonadotropins does not necessarily lead to improved ovarian sensitivity to FSH stimulation and favorable oocyte yields, such as in cases 12, 13, and 16 (Table 1) (3, 4, 21). There were also successful COS cycles after successful FSH/LH inhibition and failed COS cycles after failed FSH/LH inhibition (Table 1). Unfortunately, the serum gonadotropin levels at the time of exogenous FSH stimulation were not documented in most cases, leading to a lack of data for further analysis. Given the complexities of the pathogenesis of ROS and insufficient etiology investigations (e.g. FSHR mutations), downregulation may be attempted when considering COS, whereas the failure to inhibit serum FSH and LH levels can then lead to ovarian stimulation.
Among the cases successfully managed by COS, hMG (cases 7 and 17; Table 1), rFSH (cases 6 and 10; Table 1) and the combination of both (cases 8, 16, 24, and 25; Table 1) have been attempted, leading to a median (P25, P75) yield of 4.0 (2.0, 12.0) oocytes. In addition, hMG and rFSH were used in two individual cycles in case 7, and mature oocytes were obtained in both cycles (19). Interestingly, Rogenhofer et al. detected serum antibodies against hMG but not rFSH in a patient with ROS. Nevertheless, 11 oocytes were retrieved after stimulation with hMG (225 IU/d) and recombinant FSH (75 IU/d) (5). Given the complex mixture of hMG (49), the antibodies concerned may target other ingredients rather than FSH. Meanwhile, both recombinant hCG and urinary hCG had been proven to be effective if dominant follicles were observed after FSH stimulation. Therefore, both recombinant and urinary gonadotropins are effective in patients with resistant ovary syndrome.
Excessive gonadotropins were prescribed in several cases (cases 3–5, 9, 12–14, 20, 23, 26-28, 31, 34, and 40; Table 1) (7, 16, 17, 21, 22, 25–28, 32, 36), but in vain. There were 19 successful COS cycles (defined by the retrieval of mature oocytes) and 33 failed COS cycles (Table 1), respectively. The median (P25, P75) stimulating duration was 13.00 (10.25, 15.50) vs. 15.00 (10.00, 17.00) (p = 0.529, by Mann Whitney test) days, respectively. Furthermore, the total gonadotropin (FSH) dosage per cycle was 3,375 (2,700, 4,800) vs. 4,500(3,000, 6,038) (p = 0.190, by Mann Whitney test) IU, respectively. The total dosages of FSH prescribed in the failed cycles were surprisingly higher than the successful cycles, though not statistically significant. In addition, several cycles were canceled due to a lack of follicle growth after a short period of ovarian stimulation, which led to the underestimation of the actual dosage of gonadotropins in this group. Therefore, simply increasing the dosage of gonadotropins does not necessarily improve COS outcomes, while investigations into etiologies may provide more clues for further management (e.g., genetic evaluations). For example, similar dosages of exogenous FSH [3,500 (1 700, 5 625)] were prescribed to those patients with FSHR mutations1 when compared with those successful cycles, but seldomly did it work. Given the complexities of ROS, simply increasing the dosage of gonadotropins in COS is not recommended.
In vitro maturation, as a method that supports immature GV-stage cumulus-oocyte complexes (COCs) from antral follicles to grow into the metaphase II (MII) stage, may serve as a final resort for fertility management in ROS (50). Several live births have been reported in patients with this condition who showed no response to conventional ovarian stimulation (7, 18, 21, 25, 32, 51). Currently, 12 patients have achieved live births via IVM, including 10 who were resistant to exogenous gonadotropin stimulation (Table 2). On average, 10 COCs were retrieved per IVM cycle, yielding an overall maturation rate of 41.51% per cycle and a live birth rate of 54.54% per patient (Table 2). In addition, there were serval patients who still had their embryos cryopreserved, and it is likely that the number of live births will increase (25). Eftekhar et al. also reported a series of cases managed with IVM, however, these patients seemed unlikely to have resistant ovary syndrome as their FSH levels were within the normal range (52). Overall, IVM is a feasible option for patients with FSHR mutations or unsuccessful COS cycles.
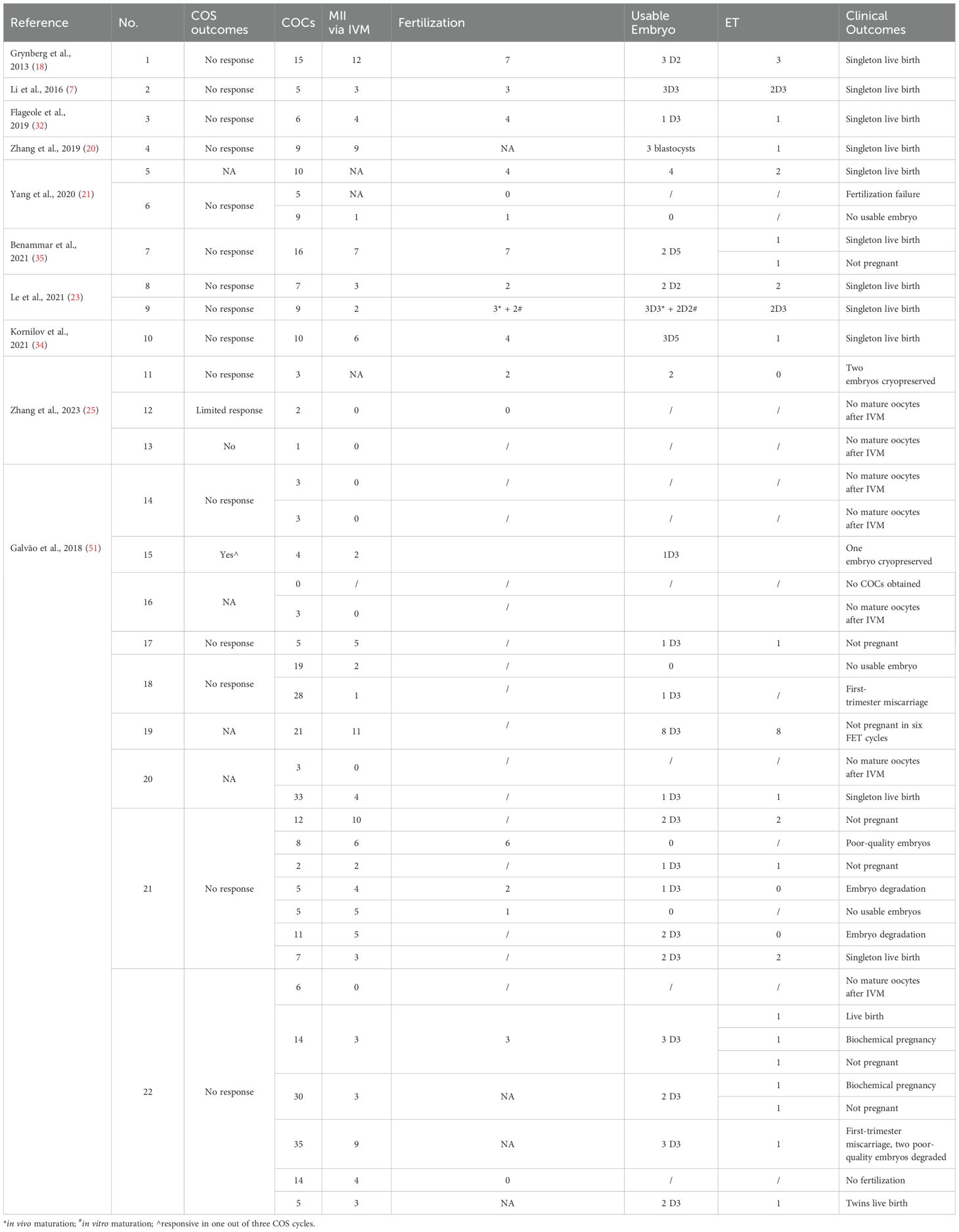
Table 2. In vitro maturation for patients with resistant ovary syndrome.
Patients with FSHR mutations had very poor COS outcomes, making it not worthy of a trial. For those without an FSHR mutation, COS is worth trying, with either recombinant or urinary gonadotropins at approximate dosages, whereas FSH and LH levels poorly predict COS outcomes. Furthermore, IVM is a feasible option for patients carrying FSHR mutations or with unsuccessful COS cycles.
HY: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. LC: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. JZ: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. YW: Data curation, Formal analysis, Supervision, Writing – original draft, Writing – review & editing. XZ: Data curation, Writing – original draft, Writing – review & editing. XC: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Shenzhen Key Medical Discipline Construction Fund (Grant no. SZXK028), the Shenzhen Science and Technology Program (Grant no. JCYJ20210324141403009 and RCYX20210609104608036), and the Natural Science Funding of China (Grant no. 82201851).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jones GS, De-Moraes-Ruehsen M. A new syndrome of amenorrhae in association with hypergonadotropism and apparently normal ovarian follicular apparatus. Am J Obstet Gynecol. (1969) 104:597–600. doi: 10.1016/S0002-9378(16)34255-7
2. Van Campenhout J, Vauclair R, Maraghi K. Gonadotropin–resistant ovaries in primary amenorrhea. Obstet Gynecol. (1972) 40:6–12.
3. Mu Z, Song J, Yu Y, Sun Z. Successful live birth in a woman with resistant ovary syndrome treated with letrozole and HMG: A case report. Med (Baltimore). (2020) 99:e20199. doi: 10.1097/MD.0000000000020199
4. Li H, Chang T, Mu H, Xiang W. Case report: Birth achieved after effective ovarian stimulation combined with dexamethasone in a patient with resistant ovary syndrome. J Ovarian Res. (2022) 15:42. doi: 10.1186/s13048-022-00976-4
5. Rogenhofer N, Pavlik R, Jeschke U, Wypior G, Ochsenkühn R, Thaler CJ. Effective ovarian stimulation in a patient with resistant ovary syndrome and antigonadotrophin antibodies. Am J Reprod Immunol. (2015) 73:185–91. doi: 10.1111/aji.2015.73.issue-2
6. Zhao S, Zheng W, Gu X, Liang G, Long G. Resistant ovary syndrome: Two case reports and a literature review of effective controlled ovarian stimulation in IVF. Med (Baltimore). (2024) 103:e37886. doi: 10.1097/MD.0000000000037886
7. Li Y, Pan P, Yuan P, Qiu Q, Yang D. Successful live birth in a woman with resistant ovary syndrome following in vitro maturation of oocytes. J Ovarian Res. (2016) 9:54. doi: 10.1186/s13048-016-0263-6
8. Koumantakis E, Matalliotakis I, Livas V, Neonaki M, Papavasiliou E. Gonadotrophin-resistant ovary syndrome (Savage syndrome). J Obstet Gynaecol. (1997) 17:208. doi: 10.1080/01443619750113924
9. Aittomäki K, Lucena JL, Pakarinen P, Sistonen P, Tapanainen J, Gromoll J, et al. Mutation in the follicle-stimulating hormone receptor gene causes hereditary hypergonadotropic ovarian failure. Cell. (1995) 82:959–68. doi: 10.1016/0092-8674(95)90275-9
10. Rannikko A, Pakarinen P, Manna PR, Beau I, Misrahi M, Aittomäki K, et al. Functional characterization of the human FSH receptor with an inactivating Ala189Val mutation. Mol Hum Reprod. (2002) 8:311–7. doi: 10.1093/molehr/8.4.311
11. Abel MH, Wootton AN, Wilkins V, Huhtaniemi I, Knight PG, Charlton HM. The effect of a null mutation in the follicle-stimulating hormone receptor gene on mouse reproduction. Endocrinology. (2000) 141:1795–803. doi: 10.1210/endo.141.5.7456
12. Chiauzzi V, Cigorraga S, Escobar ME, Rivarola MA, Charreau EH. Inhibition of follicle-stimulating hormone receptor binding by circulating immunoglobulins. J Clin Endocrinol Metab. (1982) 54:1221–8. doi: 10.1210/jcem-54-6-1221
13. Chiauzzi VA, Bussmann L, Calvo JC, Sundblad V, Charreau EH. Circulating immunoglobulins that inhibit the binding of follicle-stimulating hormone to its receptor: a putative diagnostic role in resistant ovary syndrome? Clin Endocrinol (Oxf). (2004) 61:46–54. doi: 10.1111/j.1365-2265.2004.02054.x
14. Chitnis SS, Selvaakumar C, Jagtap DD, Barnwal RP, Chary KV, Mahale SD, et al. Interaction of follicle-stimulating hormone (FSH) receptor binding inhibitor-8: a novel FSH-binding inhibitor, with FSH and its receptor. Chem Biol Drug Des. (2009) 73(6):637–43. doi: 10.1111/j.1747-0285.2009.00810.x
15. Talbert LM, Raj MH, Hammond MG, Greer T. Endocrine and immunologic studies in a patient with resistant ovary syndrome. Fertil Steril. (1984) 42:741–4. doi: 10.1016/S0015-0282(16)48200-2
16. Arici A, Matalliotakis IM, Koumantakis GE, Goumenou AG, Neonaki MA, Koumantakis EE. Diagnostic role of inhibin B in resistant ovary syndrome associated with secondary amenorrhea. Fertil Steril. (2002) 78:1324–6. doi: 10.1016/S0015-0282(02)04239-5
17. Mueller A, Berkholz A, Dittrich R, Wildt L. Spontaneous normalization of ovarian function and pregnancy in a patient with resistant ovary syndrome. Eur J Obstet Gynecol Reprod Biol. (2003) 111:210–3. doi: 10.1016/S0301-2115(03)00211-2
18. Grynberg M, Peltoketo H, Christin-Maître S, Poulain M, Bouchard P, Fanchin R. First birth achieved after in vitro maturation of oocytes from a woman endowed with multiple antral follicles unresponsive to follicle-stimulating hormone. J Clin Endocrinol Metab. (2013) 98:4493–8. doi: 10.1210/jc.2013-1967
19. Xu DF, Wu QF. A Case report: Clinical Pregnancy Achieved by IVF-ET Using Long−Acting GnRH Agonist Long Protocol in a patient with Persistently Elevated FSH levels. Jiangxi Med J. (2014) 49:1489–91. doi: 10.3969/j.issn.1006-2238.2014.12.065
20. Zhang ZZ, Han T, Li J, Shi YH. A Case report: Live birth obtained via in vitro maturation followed by frozen-thawed embryo transfer in a patient with resistant ovary syndrome. J Shandong Univ (Health Sci). (2019) 57:117–9. doi: 10.6040/j.issn.1671-7554.0.2018.824
21. Yang R, Wang Y, Zhang CM, Li R, Liu P, Qiao J. Case analysis and literature review of resistant ovary syndrome infertility. Chin J Reprod Contracep. (2020) 40:45–9. doi: 10.3760/cma.j.issn.2096-2916.2020.0003
22. Samsami A, Davoodi S, Ghasmpour L, Moradi Alamdarloo S, Rahmati J, Karimian A. Gonadotropin-resistant ovary syndrome presented with secondary amenorrhea and infertility: A case report. Iran J Med Sci. (2020) 45:140–2. doi: 10.30476/ijms.2019.81965
23. Le HL, Ho VNA, Le TTN, Tran VTT, Ma MPQ, Le AH, et al. Live birth after in vitro maturation in women with gonadotropin resistance ovary syndrome: report of two cases. J Assist Reprod Genet. (2021) 38:3243–9. doi: 10.1007/s10815-021-02355-2
24. Chen YL, Guo JL, Li ZW, Yang AJ. A case of successful delivery in an infertile patient with ovarian resistance syndrome: treated with antagonist protocol and fresh-embryo transfer. J Int Reprod Health/Fam Plan. (2022) 41:294–7. doi: 10.12280/gjszjk.20210634
25. Zhang F, Zhang H, Du H, Li X, Jin H, Li G. Application value of Early-Follicular Phase Long-Acting Gonadotropin-Releasing Hormone Agonist Long Protocol in patients with resistant ovary syndrome. BMC Pregnancy Childbirth. (2023) 23:178. doi: 10.1186/s12884-023-05477-w
26. Beau I, Touraine P, Meduri G, Gougeon A, Desroches A, Matuchansky C, et al. A novel phenotype related to partial loss of function mutations of the follicle stimulating hormone receptor. J Clin Invest. (1998) 102:1352–9. doi: 10.1172/JCI3795
27. Touraine P, Beau I, Gougeon A, Meduri G, Desroches A, Pichard C, et al. New natural inactivating mutations of the follicle-stimulating hormone receptor: correlations between receptor function and phenotype. Mol Endocrinol. (1999) 13:1844–54. doi: 10.1210/mend.13.11.0370
28. Meduri G, Touraine P, Beau I, Lahuna O, Desroches A, Vacher-Lavenu MC, et al. Delayed puberty and primary amenorrhea associated with a novel mutation of the human follicle-stimulating hormone receptor: clinical, histological, and molecular studies. J Clin Endocrinol Metab. (2003) 88:3491–8. doi: 10.1210/jc.2003-030217
29. Nakamura Y, Maekawa R, Yamagata Y, Tamura I, Sugino N. A novel mutation in exon8 of the follicle-stimulating hormone receptor in a woman with primary amenorrhea. Gynecol Endocrinol. (2008) 24:708–12. doi: 10.1080/09513590802454927
30. Desai SS, Achrekar SK, Sahasrabuddhe KA, Meharji PK, Desai SK, Mangoli VS, et al. Functional characterization of two naturally occurring mutations (Val514Ala and Ala575Val) in follicle-stimulating hormone receptor. J Clin Endocrinol Metab. (2015) 100:E638–45. doi: 10.1210/jc.2014-3662
31. Li W, He WB, Zhou LH, Hu X, Li SF, G F, et al. Study of two Chinese families affected with resistant ovarian syndrome resulted from novel mutations of FSHR gene. Chin J Med Genet. (2017) 34:196–9. doi: 10.3760/cma.j.issn.1003-9406.2017.02.009
32. Flageole C, Toufaily C, Bernard DJ, Ates S, Blais V, Chénier S, et al. Successful in vitro maturation of oocytes in a woman with gonadotropin-resistant ovary syndrome associated with a novel combination of FSH receptor gene variants: a case report. J Assist Reprod Genet. (2019) 36:425–32. doi: 10.1007/s10815-018-1394-z
33. Khor S, Lyu Q, Kuang Y, Lu X. Novel FSHR variants causing female resistant ovary syndrome. Mol Genet Genomic Med. (2020) 8:e1082. doi: 10.1002/mgg3.1082
34. Kornilov NV, Pavlova MN, Yakovlev PP. The live birth in a woman with resistant ovary syndrome after in vitro oocyte maturation and preimplantation genetic testing for aneuploidy. J Assist Reprod Genet. (2021) 38:1303–9. doi: 10.1007/s10815-021-02085-5
35. Benammar A, Fanchin R, Filali-Baba M, Vialard F, Fossard C, Vandame J, et al. Utilization of in vitro maturation in cases with a FSH receptor mutation. J Assist Reprod Genet. (2021) 38:1311–21. doi: 10.1007/s10815-021-02249-3
36. Chen X, Chen L, Wang Y, Shu C, Zhou Y, Wu R, et al. Identification and characterization of novel compound heterozygous variants in FSHR causing primary ovarian insufficiency with resistant ovary syndrome. Front Endocrinol (Lausanne). (2022) 13:1013894. doi: 10.3389/fendo.2022.1013894
37. Yan H, Huang L, Ma XH, Ha LX, Zhao JL, Zhang Q, et al. Identification of a novel splice variant c 299 + 2T>G of FSHR in a pedigree affected with resistant ovary syndrome. J Reprod Med. (2023) 32:245–51. doi: 10.3969/j.issn.1004-3845.2023.02.013
38. He WB, Du J, Yang XW, Li W, Tang WL, Dai C, et al. Novel inactivating mutations in the FSH receptor cause premature ovarian insufficiency with resistant ovary syndrome. Reprod BioMed Online. (2019) 38:397–406. doi: 10.1016/j.rbmo.2018.11.011
39. Mu Z, Shen S, Lei L. Resistant ovary syndrome: Pathogenesis and management strategies. Front Med (Lausanne). (2022) 9:1030004. doi: 10.3389/fmed.2022.1030004
40. Allen LA, Achermann JC, Pakarinen P, Kotlar TJ, Huhtaniemi IT, Jameson JL, et al. A novel loss of function mutation in exon 10 of the FSH receptor gene causing hypergonadotrophic hypogonadism: clinical and molecular characteristics. Hum Reprod. (2003) 18:251–6. doi: 10.1093/humrep/deg046
41. Bramble MS, Goldstein EH, Lipson A, Ngun T, Eskin A, Gosschalk JE, et al. A novel follicle-stimulating hormone receptor mutation causing primary ovarian failure: a fertility application of whole exome sequencing. Hum Reprod. (2016) 31:905–14. doi: 10.1093/humrep/dew025
42. Katari S, Wood-Trageser MA, Jiang H, Kalynchuk E, Muzumdar R, Yatsenko SA, et al. Novel inactivating mutation of the FSH receptor in two siblings of Indian origin with premature ovarian failure. J Clin Endocrinol Metab. (2015) 100:2154–7. doi: 10.1210/jc.2015-1401
43. Doherty E, Pakarinen P, Tiitinen A, Kiilavuori A, Huhtaniemi I, Forrest S, et al. A Novel mutation in the FSH receptor inhibiting signal transduction and causing primary ovarian failure. J Clin Endocrinol Metab. (2002) 87:1151–5. doi: 10.1210/jcem.87.3.8319
44. França MM, Lerario AM, Funari MFA, Nishi MY, Narcizo AM, de Mello MP, et al. A novel homozygous missense FSHR variant associated with hypergonadotropic hypogonadism in two siblings from a Brazilian family. Sex Dev. (2017) 11:137–42. doi: 10.1159/000477193
45. Liu H, Xu X, Han T, Yan L, Cheng L, Qin Y, et al. A novel homozygous mutation in the FSHR gene is causative for primary ovarian insufficiency. Fertil Steril. (2017) 108:1050–5.e2. doi: 10.1016/j.fertnstert.2017.09.010
46. Kuechler A, Hauffa BP, Köninger A, Kleinau G, Albrecht B, Horsthemke B, et al. An unbalanced translocation unmasks a recessive mutation in the follicle-stimulating hormone receptor (FSHR) gene and causes FSH resistance. Eur J Hum Genet. (2010) 18:656–61. doi: 10.1038/ejhg.2009.244
47. Huang BY, Xu P, Liu MT, Fu Y, Xu JH, Zeng YT, et al. Grading and etiology of ovarian resistant syndrome. Chin J Pract Gynecol Obstetrics. (2017) 33:963–6. doi: 10.19538/j.fk2017090120
48. Jayaprakasan K, Campbell BK, Hopkisson JF, Clewes JS, Johnson IR, Raine-Fenning NJ. Effect of pituitary desensitization on the early growing follicular cohort estimated using anti-Mullerian hormone. Hum Reprod. (2008) 23:2577–83. doi: 10.1093/humrep/den282
49. Deeks ED. Highly purified human menopausal gonadotropin (Menopur(®)): A profile of its use in infertility. Clin Drug Investig. (2018) 38:1077–84. doi: 10.1007/s40261-018-0703-8
50. Gilchrist RB, Smitz J. Oocyte in vitro maturation: physiological basis and application to clinical practice. Fertil Steril. (2023) 119:524–39. doi: 10.1016/j.fertnstert.2023.02.010
51. Galvão A, Segers I, Smitz J, Tournaye H, De Vos M. In vitro maturation (IVM) of oocytes in patients with resistant ovary syndrome and in patients with repeated deficient oocyte maturation. J Assist Reprod Genet. (2018) 35:2161–71. doi: 10.1007/s10815-018-1317-z
Keywords: resistant ovary syndrome, follicle-stimulating hormone receptor, gene mutation, controlled ovarian stimulation, in vitro maturation
Citation: Yi H, Chen L, Zhang J, Wen Y, Zheng X and Chen X (2025) Infertility management in resistant ovary syndrome: a review. Front. Endocrinol. 16:1560981. doi: 10.3389/fendo.2025.1560981
Received: 15 January 2025; Accepted: 21 February 2025;
Published: 18 March 2025.
Edited by:
Duan Xing, Southeast University, ChinaReviewed by:
Jeremy Egbert, UCONN Health, United StatesCopyright © 2025 Yi, Chen, Zhang, Wen, Zheng and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyan Chen, Y2hlbnhpYW95YW5AY3Voay5lZHUuaGs=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.