 Dongli Huang
Dongli Huang Hang Wu
Hang Wu Yanhua Huang
Yanhua Huang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 03 March 2025
Sec. Reproduction
Volume 16 - 2025 | https://doi.org/10.3389/fendo.2025.1527506
Purpose: This study explored the association between the C-reactive protein-albumin-lymphocyte (CALLY) index and erectile dysfunction (ED).
Patients and methods: Data from 2,128 participants in the 2001–2004 National Health and Nutrition Examination Survey (NHANES) were analyzed and classified into ED and non-ED groups.Additionally, a separate analysis of complete erectile dysfunction was conducted.A weighted multiple logistic regression model was used to assess the association between CALLY and ED, while smooth curve fitting was applied to explore their linear relationship.ROC analysis was conducted to compare the predictive accuracy (AUC) of CALLY, Systemic Inflammation Response Index (SIRI), Systemic Immune-Inflammation Index (SII), Aggregate Index of Systemic Inflammation (AISI), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and the product of platelet count and neutrophil count (PPN) for ED.
Results: After adjustment, Ln-CALLY was negatively associated with ED (OR = 0.77, 95% CI: 0.69–0.85, p < 0.0001) and complete ED (OR = 0.88, 95% CI: 0.78–1.00, p = 0.0450).The highest Ln-CALLY tertile (Q3) was associated with a significantly lower risk of ED compared to Q1 (OR = 0.40, 95% CI: 0.30–0.55, p < 0.0001).A similar trend was observed for complete ED (OR = 0.57, 95% CI: 0.38–0.85, p = 0.006).Curve fitting revealed a negative correlation between CALLY and both types of ED.Subgroup analysis confirmed the consistent and independent association.CALLY exhibited superior predictive performance for ED (AUC = 0.6512) and complete ED (AUC = 0.6237) compared to other markers.
Conclusion: Higher CALLY levels were linked to a reduced ED risk and proved a superior predictor compared to other inflammatory markers.
Erectile dysfunction is a common disease of the male reproductive system that seriously affects the quality of life of both the patient and their partner, which has a prevalence of 19-52% in the world and increases with age (1). ED is a multifactorial disease associated with various factors, including injury, endothelial dysfunction, smooth muscle issues, infection, and oxidative stress (2). Evidence indicates systemic inflammation contributes to endothelial dysfunction, which is linked to various vascular diseases (3, 4). Penile arteries are small and sensitive; therefore, ED may significantly indicate systemic endothelial dysfunction. Consequently, considerable research has been directed toward exploring the relationship between inflammation and ED.
In clinical and previous studies, hematological indicators are frequently used to reflect patients’ inflammatory levels, nutritional status, and immune function. C-reactive protein (CRP) is a common clinical marker used to reflect the inflammatory status of patients with ED (5). Serum albumin has long been used as a marker of clinical nutritional status, with low albumin serving as an independent risk factor for ED. Lymphocyte count is a conventional biomarker that reflects immune function (6, 7). The C-reactive protein-albumin-lymphocyte (CALLY) index, developed by Hiroya Iida et al., is a novel immunity and nutrition scoring system calculated by multiplying the albumin level by the lymphocyte count and dividing by the C-reactive protein level (8). Previous studies have investigated the relationship between CALLY and the prognosis of patients with colorectal cancer, hepatocellular carcinoma, and myocardial infarction (8–11). Similarly, a cross-sectional study showed that the CALLY index was negatively correlated with cardiocirculatory syndrome (12). These studies show that, compared with traditional immune indicators, the CALLY index has excellent predictive power for various diseases. However, studies on the correlation between the CALLY index and ED are still limited. Using data from the National Health and Nutrition Examination Survey (NHANES), we investigated the potential independent association between the CALLY index and ED to address gaps in understanding ED risk factors and predictors and to guide the development of effective preventive measures.
We performed a cross-sectional analysis using NHANES data from 2001 to 2004. This comprehensive program, administered by the National Center for Health Statistics, is a vital resource for assessing the health and nutritional status of the US population.NHANES includes detailed interviews covering demographic characteristics, socioeconomic status, dietary practices, and various health aspects, supplemented by thorough examinations conducted by qualified healthcare professionals, including medical tests and blood marker assessments. All participants in the NHANES study program provided informed consent, and the NCHS Research Ethics Review Board approved the program. Detailed information about the NHANES survey is publicly available.
The National Health and Nutrition Examination Survey (NHANES) is a major initiative of the Centers for Disease Control and Prevention (CDC) designed to assess the health and nutritional status of the U.S. population. NHANES uses a multistage probability sampling design to collect a representative sample of the noninstitutionalized civilian population in the United States. All participants in the NHANES study protocol provided informed consent, and the protocol was approved by the NCHS Research Ethics Review Board. Further details about the NHANES survey can be found on the official website: https://www.cdc.gov/nchs/nhanes/index.htm.
For our study, we utilised data from two NHANES cycles (2001-2002 and 2003-2004) as ED information was only available for these years. The initial sample consisted of 21,161 participants. We then applied the following inclusion and exclusion criteria:(1) Participants with incomplete ED assessments, as assessed through the “Body Measures” and “Prostate Conditions” questionnaires, were excluded (n=17,045). (2) Participants lacking the necessary data for calculating the C-reactive protein-albumin-lymphocyte (CALLY) index, specifically CRP, albumin, and lymphocyte data, were excluded (n=1,988). (3) Participants under the age of 18 years were excluded (n=0). As a result, the final study population consisted of 2,128 participants. The detailed selection process, including all exclusions, is shown in Figure 1.

Figure 1. Flowchart of participant selection. NHANES, National Health and Nutrition Examination Survey; CALLY, C-reactive protein-albumin-lymphocyte; ED, erectile dysfunctioncholesterol ratio.
The blood cell count analysis results, including neutrophils, platelets, monocytes, and lymphocytes, obtained using the Kurt HMX blood analyzer, are reported in standardized units per microliter × 10³ cells. Our primary focus is the CALLY index, a novel indicator derived from albumin levels, lymphocyte counts, and CRP values. The CALLY index is calculated explicitly as [(albumin in g/L) × (lymphocyte count in 1000 cells/μL)]/(CRP in mg/dL), offering a comprehensive assessment of inflammation and nutritional status.
Interviews were conducted in private rooms at the MEC using the Audio Computer-Assisted Self-Interview (ACASI) method.ED self-assessment, used as the dependent variable, was measured with a question from the Massachusetts Male Aging Study (13): ‘How would you describe your ability to get and maintain an erection sufficient for satisfactory sexual intercourse?’Response options included ‘always or almost always can,’ ‘usually can,’ ‘sometimes can,’ and ‘never can.’For this analysis, ED was defined as participants who answered ‘sometimes able’ or ‘never able’ to maintain an erection. Respondents who answered ‘always or almost always able’ or ‘usually able’ to maintain an erection were classified as not having ED. In this study, complete erectile dysfunction was defined as participants who answered ‘never able’ to maintain an erection.
In this study, the covariates of interest included age, race, education level, marital status, family poverty income ratio (PIR), BMI, physical activity (vigorous/moderate), smoking status, alcohol consumption, diabetes, hypertension, hypercholesterolemia, and cardiovascular disease(CVD). Physical activity was categorized as vigorous (yes/no) or moderate (yes/no). Participants who reported smoking at least 100 cigarettes in their lifetime and were smoking at the time of the survey were classified as current smokers. Former smokers were defined as those who had smoked at least 100 cigarettes in their lifetime but were not smoking at the time of the survey. Additionally, men who had smoked fewer than 100 cigarettes in their lifetime were classified as non-smokers. A non-drinker was a participant who answered ‘no’ to having consumed at least 12 alcoholic beverages in their lifetime or any single year. In this study, men who answered ‘yes’ to having consumed 12 alcoholic drinks in their lifetime or any single year but had not consumed any in the past 12 months were classified as former drinkers. Participants who answered ‘yes’ to consuming 12 alcoholic beverages in their lifetime or any single year and had consumed at least one in the past 12 months were classified as current drinkers. Participants were considered diabetic if they had a physician’s diagnosis of diabetes, a fasting blood glucose level ≥ 7.0 mmol/L, glycated hemoglobin (HbA1c) ≥ 6.5%, or were using glucose-lowering medication or insulin, according to the American Diabetes Association (ADA) criteria. Participants were classified as hypertensive if they had a history of hypertension, were taking antihypertensive medications, or had a systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 80 mmHg, according to the 2017 American College of Cardiology (ACC) and American Heart Association (AHA) guidelines. Participants were considered hypercholesterolemic if their total cholesterol level was > 5.2 mmol/L or their low-density lipoprotein cholesterol (LDL-C) level was > 3.4 mmol/L, according to the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) guidelines.CVD was defined as participants with a prior diagnosis of congestive heart failure, coronary heart disease, angina pectoris, stroke, or heart attack.
In this study, the multistage design of NHANES was accounted for in all statistical analyses by selecting appropriate sampling weights, strata, and primary sampling units.Continuous variables were expressed as weighted means and standard errors (SE), and categorical variables were expressed as weighted proportions in the baseline characteristics table. We observed that the CALLY data exhibited skewness, necessitating the application of the natural logarithm (Ln) to the values prior to statistical analysis (Supplementary Figures 1, 2). The Kruskal Wallis rank sum test was used for continuous variables and the chi-square test for categorical variables to assess differences between participants with different CALLY tertiles. The relationship between CALLY and ED prevalence was analyzed using multivariate logistic regression. Three models were used: Model 1 was unadjusted; Model 2 was adjusted for age and race; and Model 3 was adjusted for age, race, BMI, education level, marital status, family PIR, smoking status, alcohol consumption, vigorous and moderate activity, diabetes, hypertension, high cholesterol, and CVD. Subgroup analyses explored the association between CALLY and ED across various subgroups. Smooth curve fitting was applied to examine the nonlinear relationship between CALLY and ED. The Receiver Operating Characteristic (ROC) curve and the area under the curve (AUC) were used to evaluate the predictive ability of CALLY and other inflammatory markers (SIRI, SII, AISI, NLR, PLR, and PPN) for ED. A p-value < 0.05 was considered statistically significant. All statistical analyses were conducted using EmpowerStats (http://www.empowerstats.com, X&Y Solutions, Inc.) and the R statistical software package (http://www.R-project.org; The R Foundation).
A total of 2,128 participants were included in our study, with 709 in T1, 709 in T2, and 710 in T3 of the three CALLY groups Table 1 shows the baseline demographic and clinical characteristics of the participants. Of the participants, 648 (30.45%) were diagnosed with ED, and 268 (12.59%) had complete ED. No statistically significant differences in education level were observed between groups (P > 0.05). At the same time, all other baseline covariates showed statistically significant differences between CALLY groups (P < 0.05).
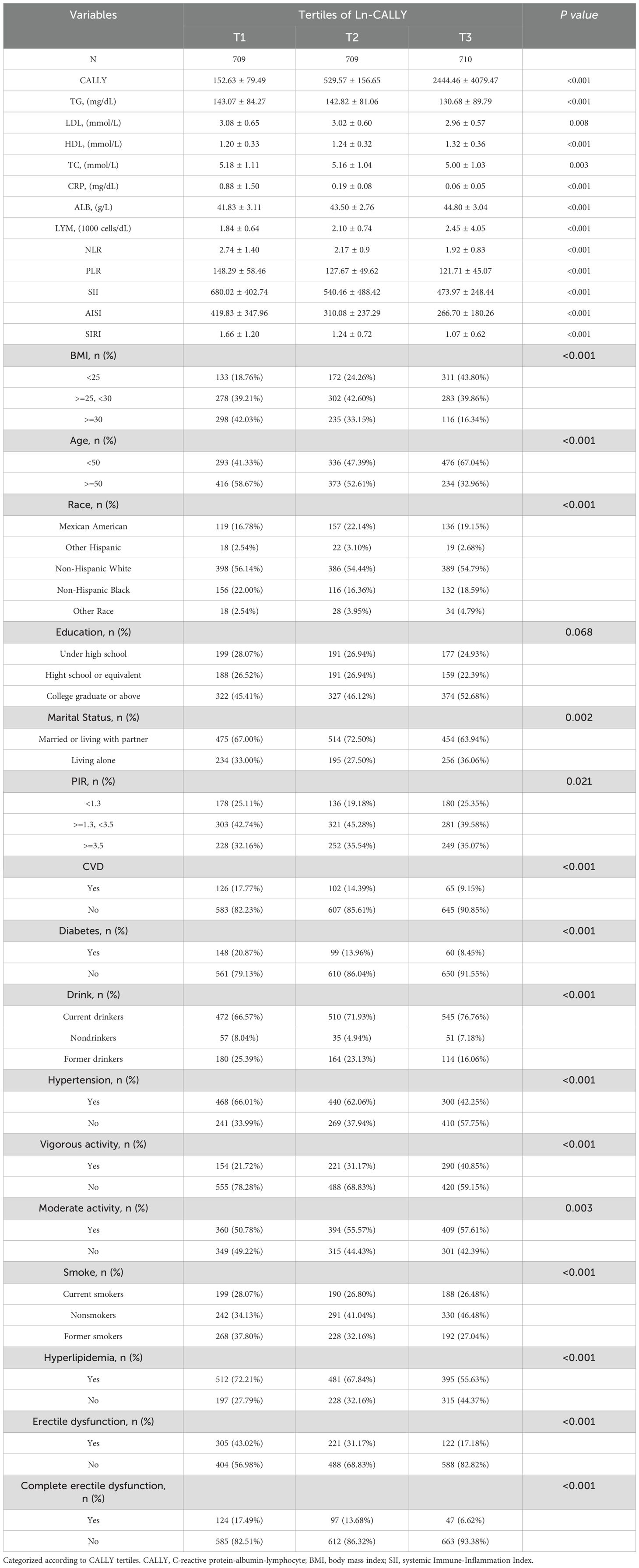
Table 1. Baseline characteristics of NHANES participants, 2001–2004.
Weighted multivariate logistic regression was used to examine the relationship between CALLY and ED in the crude model, Model 1, and the fully adjusted model. Details are presented in Table 2, which showed a significant negative correlation between Ln-CALLY and ED and complete ED across all models. In the fully adjusted model (Model 3), each one-unit increase in Ln-CALLY was associated with a 23% reduction in the risk of ED (OR = 0.77, 95% CI: 0.69–0.85, p < 0.0001). The risk of complete ED decreased by 12% (OR = 0.88, 95% CI: 0.78–1.00, p = 0.0450). The continuous Ln-CALLY variable was converted into a categorical variable by dividing it into three tertiles. In Model 3, individuals in the highest tertile (T3) had a 60% lower risk of ED compared to those in the lowest tertile (T1) (OR = 0.40, 95% CI: 0.30–0.55, p < 0.0001). This trend was consistent for complete ED, with an OR of 0.57 (95% CI: 0.38–0.85, p = 0.0066). Smooth curve fitting analysis revealed a negative linear correlation between CALLY and both ED and complete ED (Figure 2).
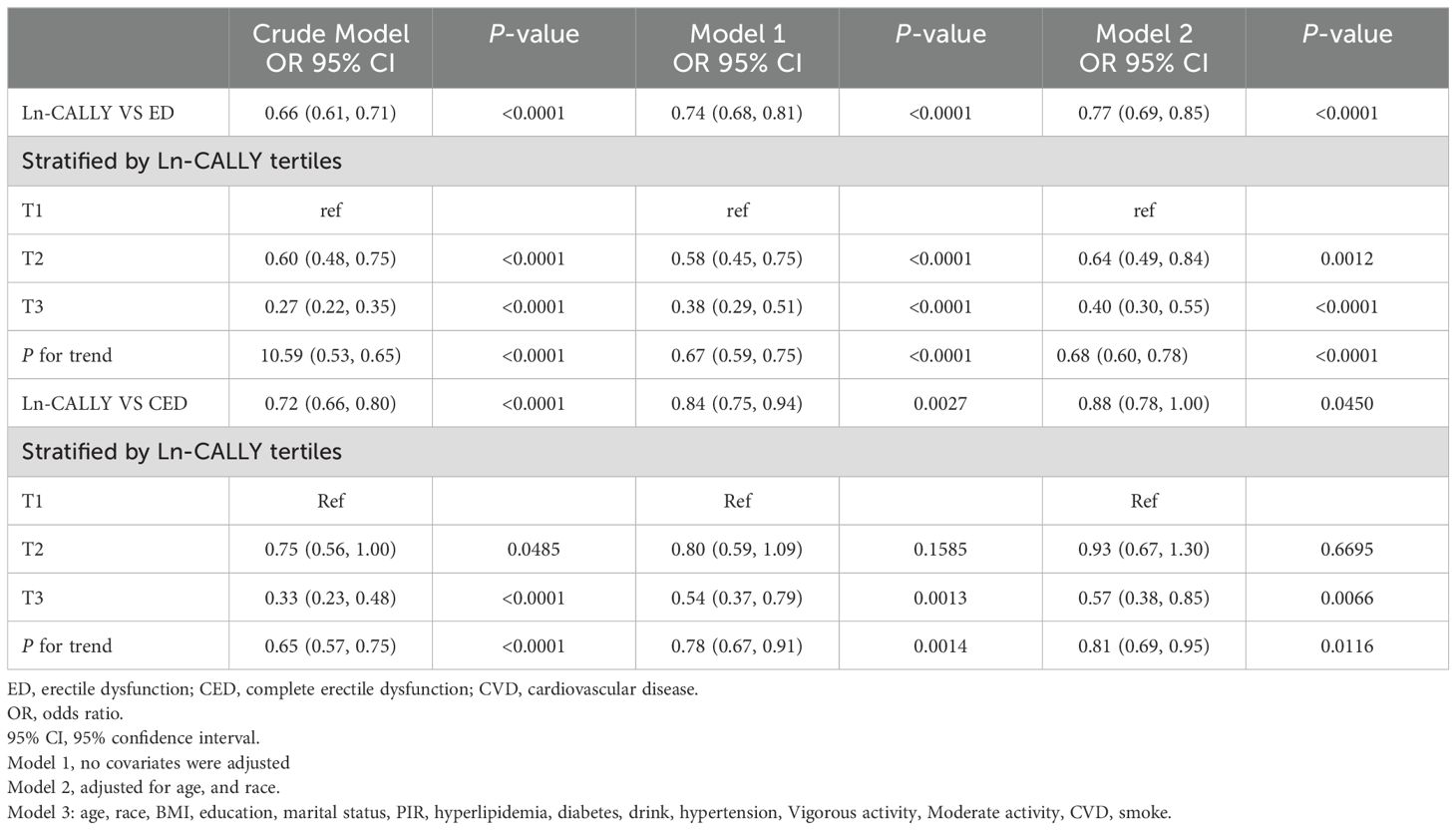
Table 2. Multiple logistic regression analysis Ln-CALLY vs erectile dysfunction.

Figure 2. (A) Smooth curve fitting diagram of Ln-AISI and erectile dysfunction in fully adjusted models; (B) Smooth curve fitting diagram of Ln-AISI and complete erectile dysfunction in fully adjusted models.
Subgroup analyses were conducted to determine whether the association between Ln-CALLY and ED and complete ED was consistent across different strata. As shown in Table 3, all subgroups, including age, BMI, hypertension, diabetes mellitus, high cholesterol, vigorous activity, moderate activity, and CVD, did not affect the negative correlation between CALLY and ED or complete ED (p > 0.05 for all interactions).In certain strata, the negative correlations were statistically significant and stable. For instance, among participants over 50 years of age, each unit increase in Ln-CALLY was associated with a 27% reduction in the likelihood of developing ED (OR = 0.73, 95% CI: 0.65–0.83, p = 0.029) and a 12% reduction in the possibility of creating complete ED (OR = 0.88, 95% CI: 0.77–1.00, p = 0.0431). Detailed results of this analysis are presented in Table 3.
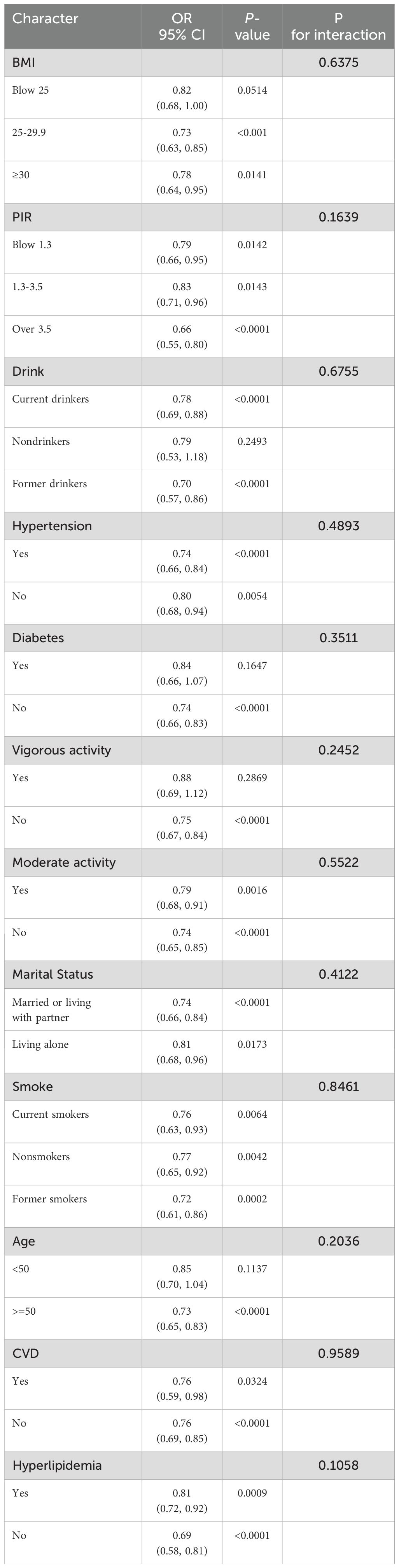
Table 3.1. Subgroup analysis for the association between CALLY and ED.
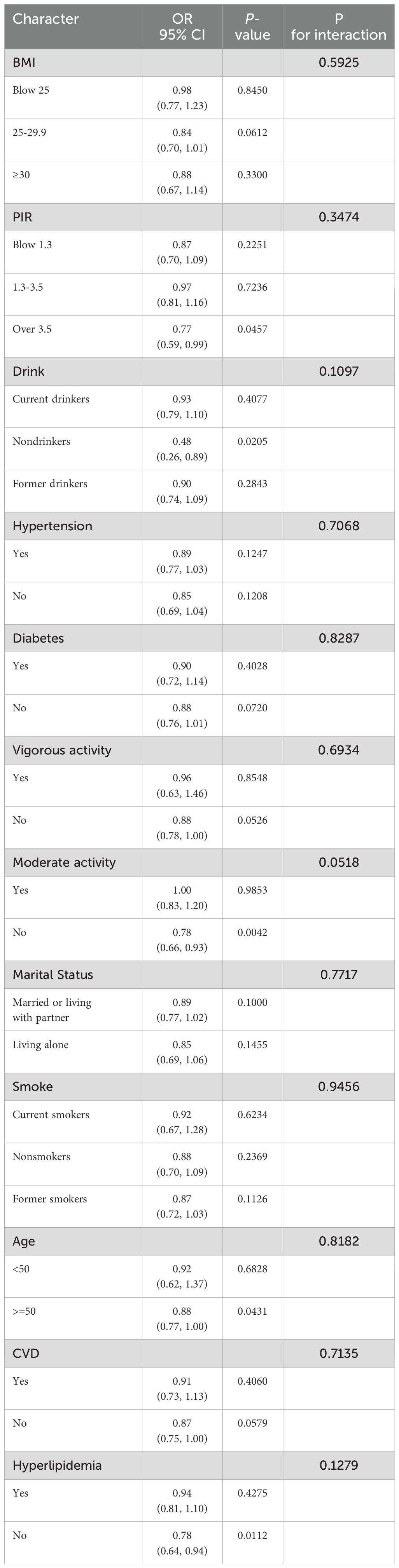
Table 3.2. Subgroup analysis for the association between CALLY and complete ED.
The area under the curve (AUC) was calculated to compare the predictive accuracy of CALLY with other inflammatory indicators (NLR, PLR, PPN, SII, AISI, SIRI) for ED and complete ED. Figure 3 shows the ROC curve used to evaluate the predictive performance of CALLY and other inflammatory markers for ED and complete ED. Table 4 presents the AUC value (95% CI) for diagnosing ED: CALLY: 0.6512 (0.6263–0.6762).CALLY demonstrated the highest AUC compared to other inflammatory markers, with a statistically significant difference (p < 0.05). The AUC of CALLY was also the highest for diagnosing complete ED. Table 4 includes additional details, such as cut-off values, sensitivity, and specificity. For instance, the optimal cut-off value for CALLY in predicting ED was 556.79 (specificity: 0.5405, sensitivity: 0.6867). These results suggest that CALLY may be a superior predictor of ED and complete ED compared to other inflammatory markers.

Figure 3. ROC curve and AUC value of seven inflammatory indicators(CALLY, SIRI, NLR, AISI, SII, PLR, PPN) for dignosing erectile dysfunction and complete erectile dysfunction. (A) seven inflammatory indicators are assessed to identify erectile dysfunction. (B) seven inflammatory indicators are assessed to identify complete erectile dysfunction.
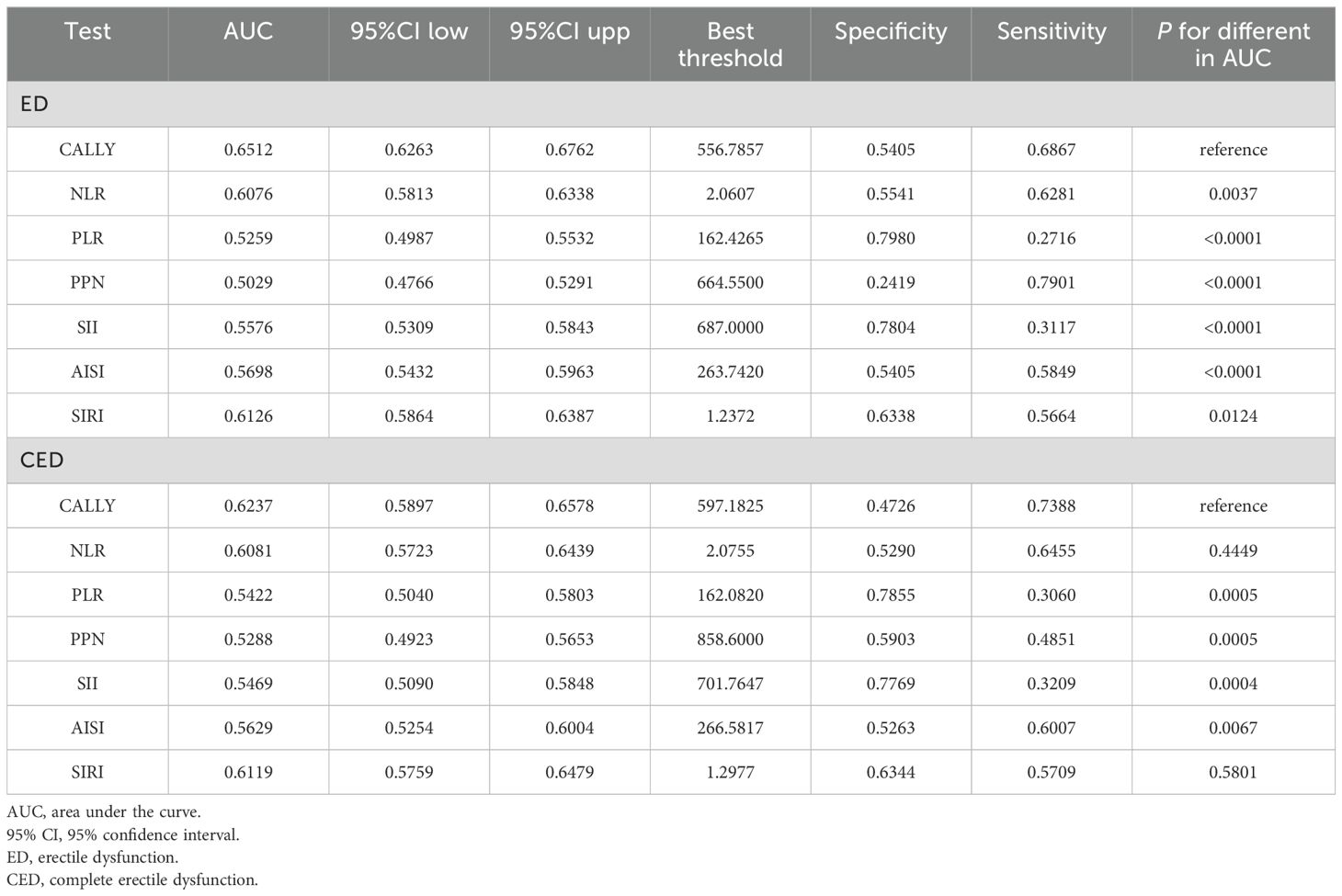
Table 4. Comparison of AUC values between CALLY and other Inflammation marks.
Ultimately, the study included 2,128 participants from the 2001–2004 NHANES cohort, of whom 648 (30.45%) had ED. Of the patients with ED, 268 (12.59%) were diagnosed with complete ED. Our findings indicate a negative association between CALLY and ED prevalence, with this association remaining stable in patients with complete ED. The negative correlation persists when CALLY is divided into tertiles (Q1–Q3). Furthermore, subgroup analysis demonstrated that the relationship between CALLY and ED was consistent across all stratifying variables, with a stable negative correlation. Finally, ROC analysis indicated that CALLY may be a superior predictor of ED and complete ED compared to other inflammatory markers. Our study supports previous findings suggesting that inflammation may be a potential mechanism underlying ED. Therefore, incorporating CALLY into clinical practice may help identify individuals at higher risk of ED in the general population.
This is the first study to report CALLY levels in ED patients and controls from the NHANES database. The CALLY index, a novel inflammatory marker, comprises albumin levels, lymphocyte count, and CRP (14). Unlike more straightforward inflammatory indicators like NLR or SII, the CALLY index integrates nutritional, inflammatory, and immune factors to assess inflammation’s impact on erectile dysfunction comprehensively. Albumin, a key indicator of nutritional status, has been implicated in the pathogenesis of ED due to its association with malnutrition (15, 16). Lymphocytes and C-reactive protein (CRP) indicate the body’s immune and inflammatory status. Numerous studies have supported the association between inflammation and ED. Zhong’s analysis revealed that ED patients exhibited higher systemic immune-inflammatory indices(SII) (17). Feng et al. identified a significant positive association between a novel inflammatory marker, the neutrophil-to-lymphocyte ratio (NLR) exceeding 1.52, and ED (18). A study among dialysis patients demonstrated a significant association between C-reactive protein (CRP)/albumin ratio (CAR) and severe ED (19).
However, the mechanisms underlying this association are still not well understood. The most plausible mechanism involves endothelial dysfunction, which ultimately results in arteriosclerosis. Normal vascular endothelium regulates hemostasis, inflammation, and local injury responses, maintaining steady blood flow to mitigate inflammation (20). However, disrupted homeostasis, marked by increased oxidative stress and inflammation, can precipitate endothelial dysfunction (21). Albumin possesses antioxidant properties that can mitigate cell damage caused by free radicals, thereby potentially inhibiting the progression of atherosclerosis. By mitigating the inflammatory response, albumin may help slow the formation of arterial plaques (22). Studies have demonstrated that the presence and severity of endothelial dysfunction correlate with inflammatory markers and mediators like C-reactive protein (23, 24). CRP levels, assessed via penile Doppler ultrasound, significantly correlate with the severity of penile arterial disease (25). Arteriosclerosis uniformly affects blood vessels, and given the smaller diameter of penile arteries (1-2 mm), similar degrees of endothelial dysfunction and arteriosclerosis likely result in substantial reductions in penile tissue blood flow, leading to erectile dysfunction. The pathogenesis of immune cells in erectile dysfunction (ED) is highly complex. Several studies have demonstrated that regulatory B cells expressing CD20 are crucial in suppressing excessive immune activation and inflammation. Regulatory T cells (Tregs) are pivotal in maintaining immune homeostasis and controlling excessive inflammatory responses, thereby safeguarding vascular health—particularly in conditions closely related to vascular function, such as ED (26).
Our study boasts several strengths, including extensive, representative NHANES sample data, fully accounting for sample design and weighting. Additionally, we adjusted for relevant covariates in our multivariate logistic regression analysis to isolate the independent effect of CALLY on erectile dysfunction (ED). Furthermore, subgroup analyses were conducted to examine the stability of these effects. However, our study is not without limitations. For instance, being a cross-sectional study, it cannot establish causality. In addition, due to the limitations of the NHANES database, reliance on self-reported ED history may introduce bias, potentially underestimating the true prevalence of ED. Incorporating objective measures, such as the International Index of Erectile Function (IIEF) or colour Doppler ultrasound, could help mitigate this bias and provide a more accurate assessment.Additionally, while we made efforts to adjust for as many covariates as possible, there remain uncontrolled factors, such as sex hormones, that may still influence the results. Finally, the NHANES database solely represents the United States population. The applicability of the CALLY-ED relationship in other countries or regions requires further verification through additional research. Therefore, future large-scale prospective studies are essential to elucidate the longitudinal relationship between the CALLY index and ED, and clinical data-based studies are needed to assess its predictive and practical value fully.
This study underscores a significant negative correlation between the CALLY index and the risk of erectile dysfunction (ED). The CALLY index has proven to be a robust and independent predictor of ED, surpassing many other inflammatory markers in performance. This finding emphasizes the potential utility of the CALLY index as a clinical tool for identifying individuals at risk of ED.
Publicly available datasets were analyzed in this study. This data can be found here: The data used in this study is publicly available from the National Health and Nutrition Examination Survey (NHANES). The dataset can be accessed directly through the following link: https://wwwn.cdc.gov/nchs/nhanes/default.aspx.
This study is based on data from the National Health and Nutrition Examination Survey (NHANES), a publicly available dataset, and therefore did not require specific ethics approval.
DH: Data curation, Software, Writing – original draft. HW: Validation, Visualization, Writing – original draft. YH: Methodology, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that Generative AI was used in the creation of this manuscript. The author(s) verify and take full responsibility for the use of generative AI in the preparation of this manuscript. Generative AI was used specifically for language polishing and grammar correction during the final revision stages of the manuscript. All intellectual and conceptual content, data analysis, and interpretations presented in the manuscript were conducted independently by the author(s), and the AI was only employed to enhance readability and clarity without altering the scientific content.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1527506/full#supplementary-material
1. Sambel M, Kilic M, Demirbas M, Onen E, Oner S, Erdogan A, et al. Relationship between erectile dysfunction and the neutrophil to lymphocyte and platelet to lymphocyte ratios. Int J Impot Res. (2018) 30:27–35. doi: 10.1038/s41443-017-0007-1
2. Zhu B, Niu Y, Guo H, Jin X, Liu F. Pyroptosis and inflammation−mediated endothelial dysfunction may act as key factors in the development of erectile dysfunction (Review). Mol Med Rep. (2023) 28(3):165. doi: 10.3892/mmr.2023.13052
3. Wang L, Cheng CK, Yi M, Lui KO, Huang Y. Targeting endothelial dysfunction and inflammation. J Mol Cell Cardiol. (2022) 168:58–67. doi: 10.1016/j.yjmcc.2022.04.011
4. Chen D, Chen F, Luo Q, Fan W, Chen C, Liu G. Association between the systemic immune-inflammation index and erectile dysfunction: A cross-sectional study. Immun Inflammation Dis. (2024) 12:e1363. doi: 10.1002/iid3.v12.8
5. Liu G, Zhang Y, Zhang W, Wu X, Jiang H, Huang H, et al. Novel predictive risk factor for erectile dysfunction: Serum high-sensitivity C-reactive protein. Andrology. (2022) 10:1096–106. doi: 10.1111/andr.13206
6. Bullock AF, Greenley SL, McKenzie GAG, Paton LW, Johnson MJ. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: systematic review, narrative synthesis and meta-analysis. Eur J Clin Nutr. (2020) 74:1519–35. doi: 10.1038/s41430-020-0629-0
7. Zinellu A, Mangoni AA. A systematic review and meta-analysis of the association between the neutrophil, lymphocyte, and platelet count, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio and COVID-19 progression and mortality. Expert Rev Clin Immunol. (2022) 18:1187–202. doi: 10.1080/1744666X.2022.2120472
8. Yang M, Lin SQ, Liu XY, Tang M, Hu CL, Wang ZW, et al. Association between C-reactive protein-albumin-lymphocyte (CALLY) index and overall survival in patients with colorectal cancer: From the investigation on nutrition status and clinical outcome of common cancers study. Front Immunol. (2023) 14:1131496. doi: 10.3389/fimmu.2023.1131496
9. Ji H, Luo Z, Ye L, He Y, Hao M, Yang Y, et al. Prognostic significance of C-reactive protein-albumin-lymphocyte (CALLY) index after primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. Int Immunopharmacol. (2024) 141:112860. doi: 10.1016/j.intimp.2024.112860
10. Pan Y, Wu TT, Deng CJ, Jiang ZH, Yang Y, Hou XG, et al. Association between the C-Reactive Protein-Albumin-Lymphocyte (CALLY) Index and Adverse Clinical Outcomes in CAD Patients after PCI: Findings of a Real-World Study. Rev Cardiovasc Med. (2024) 25:111. doi: 10.31083/j.rcm2504111
11. Furukawa K, Tsunematsu M, Tanji Y, Ishizaki S, Akaoka M, Haruki K, et al. Impact of C-reactive protein-albumin-lymphocyte (CALLY) index on prognosis after hepatectomy for colorectal liver metastasis. Surg Oncol. (2023) 47:101911. doi: 10.1016/j.suronc.2023.101911
12. Xu Z, Tang J, Xin C, Jin Y, Zhang H, Liang R. Associations of C-reactive protein-albumin-lymphocyte (CALLY) index with cardiorenal syndrome: Insights from a population-based study. Heliyon. (2024) 10:e37197. doi: 10.1016/j.heliyon.2024.e37197
13. Derby CA, Araujo AB, Johannes CB, Feldman HA, McKinlay JB. Measurement of erectile dysfunction in population-based studies: the use of a single question self-assessment in the Massachusetts Male Aging Study. Int J Impot Res. (2000) 12:197–204. doi: 10.1038/sj.ijir.3900542
14. Iida H, Tani M, Komeda K, Nomi T, Matsushima H, Tanaka S, et al. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB (Oxford). (2022) 24:101–15. doi: 10.1016/j.hpb.2021.06.414
15. Toda K, Miwa Y, Kuriyama S, Fukushima H, Shiraki M, Murakami N, et al. Erectile dysfunction in patients with chronic viral liver disease: its relevance to protein malnutrition. J Gastroenterol. (2005) 40:894–900. doi: 10.1007/s00535-005-1634-8
16. Triantos CK, Tsintoni A, Karaivazoglou K, Grigoropoulou X, Tsolias C, Diamantopoulou G, et al. Male hepatitis C patients’ sexual functioning and its determinants. Eur J Gastroenterol Hepatol. (2017) 29:1241–6. doi: 10.1097/MEG.0000000000000971
17. Zhong L, Zhan X, Luo X. Higher systemic immune-inflammation index is associated with increased risk of erectile dysfunction: Result from NHANES 2001-2004. Med (Baltimore). (2023) 102:e35724. doi: 10.1097/MD.0000000000035724
18. Feng X, Mei Y, Wang X, Cui L, Xu R. Association between neutrophil to lymphocyte ratio and erectile dysfunction among US males: a population-based cross-sectional study. Front Endocrinol (Lausanne). (2023) 14:1192113. doi: 10.3389/fendo.2023.1192113
19. Fujita N, Hatakeyama S, Momota M, Hamaya T, Tobisawa Y, Yoneyama T, et al. Relationships of low-grade systemic inflammation and nutritional status with erectile dysfunction severity in men on dialysis. Andrology. (2022) 10:1548–55. doi: 10.1111/andr.13259
20. Xu S, Ilyas I, Little PJ, Li H, Kamato D, Zheng X, et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and Beyond: From Mechanism to Pharmacotherapies. Pharmacol Rev. (2021) 73:924–67. doi: 10.1124/pharmrev.120.000096
21. Higashi Y. Roles of oxidative stress and inflammation in vascular endothelial dysfunction-related disease. Antioxidants (Basel). (2022) 11(10):1958. doi: 10.3390/antiox11101958
22. Piarulli F, Banfi C, Brioschi M, Altomare A, Ragazzi E, Cosma C, et al. The burden of impaired serum albumin antioxidant properties and glyco-oxidation in coronary heart disease patients with and without type 2 diabetes mellitus. Antioxidants (Basel). (2022) 11(8):1501. doi: 10.3390/antiox11081501
23. Hessler JR, Robertson AL Jr., Chisolm GM 3rd. LDL-induced cytotoxicity and its inhibition by HDL in human vascular smooth muscle and endothelial cells in culture. Atherosclerosis. (1979) 32:213–29. doi: 10.1016/0021-9150(79)90166-7
24. Yasunari K, Maeda K, Nakamura M, Yoshikawa J. Oxidative stress in leukocytes is a possible link between blood pressure, blood glucose, and C-reacting protein. Hypertension. (2002) 39:777–80. doi: 10.1161/hy0302.104670
25. Billups KL, Kaiser DR, Kelly AS, Wetterling RA, Tsai MY, Hanson N, et al. Relation of C-reactive protein and other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. Int J Impot Res. (2003) 15:231–6. doi: 10.1038/sj.ijir.3901012
Keywords: the C-reactive protein-albumin-lymphocyte, erectile dysfunction, national health and nutrition examination survey, cross-sectional study, inflammation marker
Citation: Huang D, Wu H and Huang Y (2025) Novel indicator for erectile dysfunction: the CALLY index, evidence from data of NHANES 2001-2004. Front. Endocrinol. 16:1527506. doi: 10.3389/fendo.2025.1527506
Received: 18 November 2024; Accepted: 12 February 2025;
Published: 03 March 2025.
Edited by:
Murat Dursun, Istanbul University, TürkiyeReviewed by:
Mustafa Ozan Horsanali, İzmir Bakırçay University, TürkiyeCopyright © 2025 Huang, Wu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanhua Huang, aHVhbmd5YW5odWEyNTY3QDE2My5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.