
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol., 18 March 2025
Sec. Thyroid Endocrinology
Volume 16 - 2025 | https://doi.org/10.3389/fendo.2025.1445977
 Glòria Tena Vivó1*
Glòria Tena Vivó1* Oriol Cunillera Puértolas2*
Oriol Cunillera Puértolas2* Mercè Albareda Riera3Neus Parellada Esquius4Mònica Isidro Albaladejo5Gemma Rodríguez Palomar6Silvia Palmero Aliste5Lluís Vila3
Mercè Albareda Riera3Neus Parellada Esquius4Mònica Isidro Albaladejo5Gemma Rodríguez Palomar6Silvia Palmero Aliste5Lluís Vila3Objective: This study aims to describe hypothyroidism monitoring and control during the first trimester of pregnancy in women with known hypothyroidism in Catalonia.
Materials and methods: Pregnancies registered in primary care in Catalonia between 2014 and 2016 were retrospectively studied. Women with hypothyroidism were selected for the study. Hypothyroidism was defined if, on the date of the last menstrual period (LMP), there was an updated thyroid hormone prescription (code ATC H03AA -levothyroxine) or any of the following active diagnostic codes: ICD-10: E02, E03, E89.0. To evaluate hypothyroidism monitoring and control, thyrotropin (TSH) tests during the first trimester of pregnancy were considered and categorized according to the reference values of each laboratory.
Results: Out of 111,811 pregnancies, 5,574 had known hypothyroidism. TSH was evaluated in 3,158 (56.65%) of them. The TSH values were within the recommended ranges in 1,146 (36.3%) of the cases, being low abnormal in 53 of them (1.7%) and high abnormal in 1,959 (62%).
Conclusion: TSH testing was not evaluated in almost half of the pregnant women with known hypothyroidism in primary care services in Catalonia during the pregnancy first trimester. Among those tested, more than two-thirds had TSH levels outside the target range. This means that it is essential to improve the management of hypothyroidism during the first trimester of pregnancy in Catalonia.
Thyroid normal function is essential during pregnancy to avoid complications and ensure a healthy offspring (1–3). Thyroid dysfunction during gestation is the second most common endocrinopathy after diabetes (4), with more than 3% of pregnancies affected (5).
Pregnancy implies important hormonal changes involving a significant thyroid requirement, which depends on adequate iodine intake and normal thyroid gland function (1, 6). Pregnancy thyroid overloading could lead to new thyroid dysfunctions and worsen the previously known ones (1, 4).
Therefore, to manage thyroid dysfunctions effectively during pregnancy, it is essential to prioritize early detection and implement appropriate treatment for pre-existing conditions (7).
Pregnancy thyroid dysfunction prevalence is estimated for clinical hypothyroidism in 0.3%–1.5% and for subclinical hypothyroidism in 3.5%–18% (1, 7–11). Such variations in findings, especially in the case of subclinical hypothyroidism, are largely influenced by the methodologies applied, TSH evaluation techniques used, and reference values considered (9, 10).
Previous and current clinical guidelines recommend that hypothyroid women who are treated with levothyroxine should have a ≤2.5 mIU/L TSH value during the first trimester of pregnancy (5, 12–14).
There are few clinical practice studies dealing with thyroid dysfunction management during pregnancy (15–18). They report poor control for pregnant people following hypothyroidism treatment, which may affect up to 50% of the cases (15, 16). Studies reporting the control degree of these women in primary healthcare in Catalonia have not been published so far. However, data exist confirming that TSH high levels during the first trimester imply a major risk for adverse obstetrical outcomes in Catalan women (19).
The main objective of the present study is to evaluate hypothyroidism monitoring during the first trimester of gestation in women with previously known hypothyroidism, that is to say, what the adherence to guidelines is by primary healthcare professionals in Catalonia and also to verify if hypothyroidism control reached adequate TSH levels in the tested ones.
A descriptive study of pregnancies in hypothyroid women between 2014 and 2016 was performed. It was based on secondary data from the computerized register of the Primary Health Care Research Information and Development System (SIDIAP, Sistema d’Informació per al Desenvolupament de la Investigació en Atenció Primària) (www.sidiap.org). The pregnancies occurred in Catalonia.
SIDIAP generates a comprehensive amount of medical data providing access to reliable information for primary healthcare research. The data originate mainly from ICS (Institut Català de la Salut) electronic health records and other sources. ICS is the governmental institution that manages the public health system in Catalonia.
The SIDIAP database covers about 80% of the Catalan population with over 7 million inhabitants. SIDIAP includes diagnostic and prescription data from both primary care and hospitals (with the exception of propyl-thyouracil, which is dispensed in hospitals only). The laboratory data are from primary healthcare, not from specialized or private centers.
The analytical results come from 33 laboratories which provide service to primary health centers in Catalonia. A total of 15 different laboratory techniques were used, mainly enzyme-chemiluminescence, electro-chemiluminescence, and immuno-chemiluminescence. The general population reference values (GPRV) for TSH ranged between 0.2–4.2 and 0.34–5.6 mIU/L, and for FT4 they ranged between 0.54–1.24 and 0.78-2.02 ng/dL. During the studied period, three laboratories out of the 33 had reference values adjusted for pregnant people.
The population under study included pregnancies that started between 2014 and 2016 in women with known hypothyroidism and who had at least one follow-up visit to the Sexual and Reproductive Health Programme at the primary healthcare. This program is responsible for antenatal care in Catalonia.
Hypothyroidism was defined if there was an active prescription of thyroid hormones (code ATC H03AA -levothyroxine) or any of the following active diagnoses [ICD-10: E02 subclinical iodine-deficiency hypothyroidism, E03 other hypothyroidism, and E89.0 post-procedural hypothyroidism (total thyroidectomy and post I-131 ablation)] recorded on the date of the last menstrual period (LMP) in the computerized medical records in primary healthcare.
Any hyperthyroidism diagnostic or treatment on the date of the LMP posterior to hypothyroidism evidence was excluded. Multiple pregnancies or pregnancies in women under 16 or above 49 years old were also rejected.
Pregnant populations with hypothyroidism under levothyroxine treatment have shown TSH testing frequencies between 75.9% and 91.4% (15, 16). No publications studying pregnant women with hypothyroidism disregarding treatment have been found. We could therefore expect lower testing rates in our samples. Conservatively, considering the most demanding 50% percentage, assuming 5% alpha risk and 2% accuracy, 2,396 hypothyroid pregnant people are needed to answer the main goal of the present study.
IDESCAT (Institut d’Estadística de Catalunya) reported 210,943 births between 2014 and 2016 (http://www.idescat.cat/pub/?id=aec,n=259,t=2015). In the SIDIAP database, 134,860 births were registered in the same period. Considering 5% hypothyroidism prevalence (1, 6, 8, 9), around 6,743 cases of hypothyroidism were expected.
According to TSH values during the first trimester of pregnancy, the study main outcomes were defined as follows:
TSH evaluation (yes/no): TSH evaluation undertaken during the first trimester of pregnancy.
Hypothyroidism control (normal: when TSH values are higher or equal to 0.1 mIU/L and lower or equal to 2.5 mIU/L; low abnormal: when TSH values are lower than 0.1 mIU/L; high abnormal according to obstetric guidelines: when TSH values are higher than 2.5 mIU/L; high abnormal according to general population reference values: when TSH values are higher than the GPRV (5, 14).
The following study independent variables were evaluated on the date of the LMP as they are very important health risk factors, especially during pregnancy: age, hypertension (I10, I15), diabetes (E11, E12, E13; E14), obesity (BMI ≥40 kg/m2) (E66.8), ischemic heart disease (I20, I21, I22, I23, I24, I25), and hormone therapy (code ATC H03AA -levothyroxine).
All continuous numerical variables were categorized. Study variables were described using absolute and relative frequencies. Chi-square test was used to compare frequencies of TSH evaluation according to independent variables. Distribution homogeneity of TSH levels according to hormonal treatment was tested with chi-square test as well.
A multivariate logistic regression model was fit for TSH evaluation using age, hypertension, diabetes, obesity, morbid obesity, and hormone therapy—interacting with the other factors—as predictors. From this initial model and through a stepwise backward variable selection process based on Akaike Information Criteria, a final reduced model was obtained with those factors which contribute plausibly enough to the model.
For the multivariate logistic regression model, odds ratios are shown. To facilitate interpretation, probabilities of having a TSH evaluation are calculated for all possible profiles according to the regression model.
The R-4.0.3 statistical package for Windows was used.
Confidentiality was ensured since all of the cases in the SIDIAP database are pseudo-anonymous and the established protocol was followed. Therefore, informed consent is not needed.
Study ethical protocol was approved by the Ethical Committee for Clinical Research (Comité Ético de Investigación Clínica CEIC) from IDIAP (Institut Universitari d’Investigació en Atenció Primària) Jordi Gol (P17/113).
During 2014–2016, 111,811 pregnancies fulfilled the inclusion criteria. From these, 5,574 (4.98%) were pregnant women with known hypothyroidism, with their average age being 32.49 years old (5.52 standard deviation). On the date of the LMP, 31.29% of these women were 35 years old or above, and their prevalence rates for hypertension, diabetes, obesity, morbid obesity, and ischemic heart disease were 1.72%, 1.40%, 14.57%, 0.72%, and 0.02%, respectively. Levothyroxine treatment was followed by 45.96% of them (Table 1).
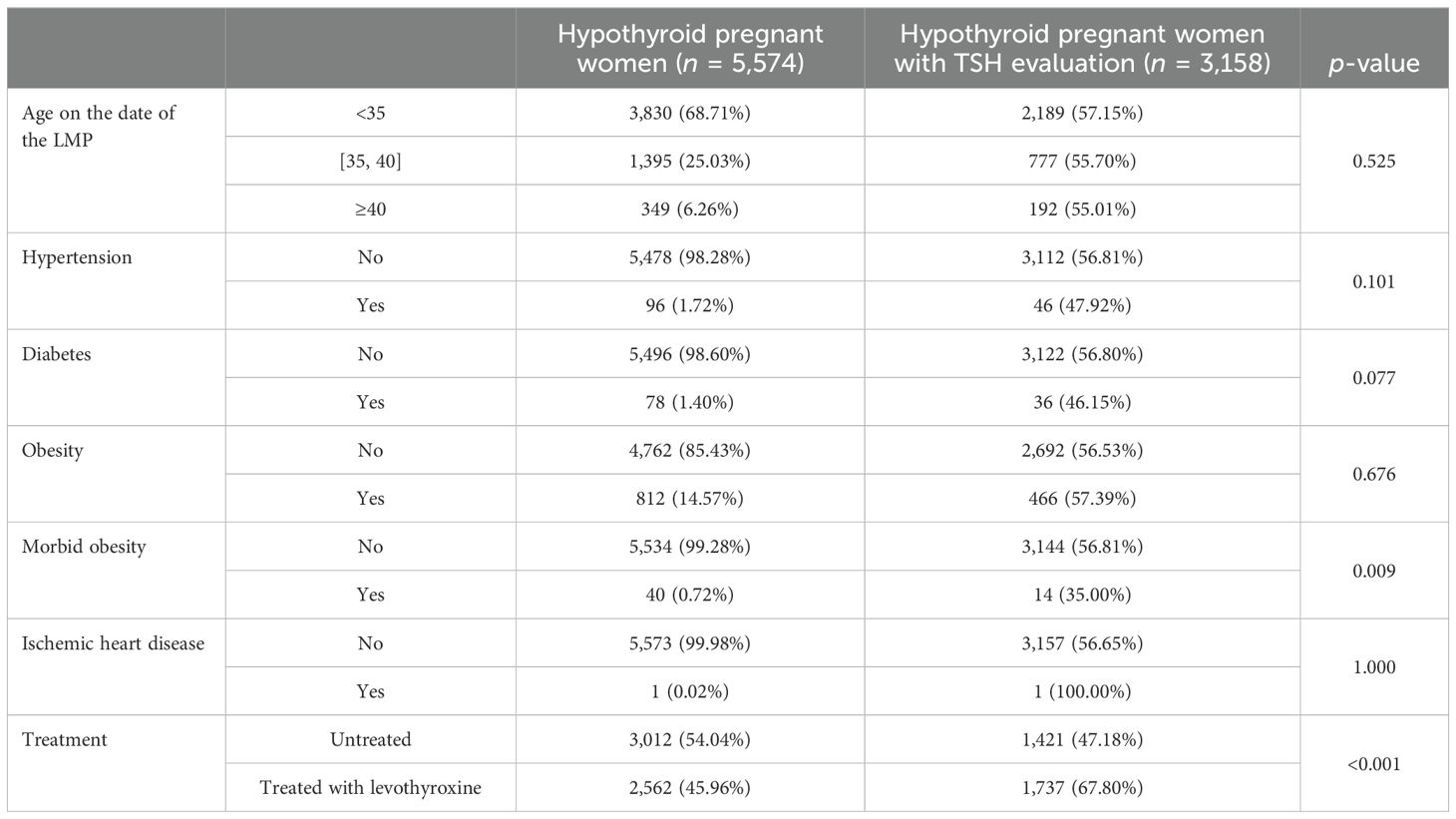
Table 1. Characteristics of pregnant women with previously known hypothyroidism and TSH evaluations in the first trimester in accordance with these characteristics.
TSH was evaluated in 3,158 (56.65%) of the cases. The median [IQR] TSH values in the subgroup of women who underwent this evaluation was 63 [40, 71], and the mean gestational age at the time of the TSH test was 9 weeks. Bivariate association between age and TSH evaluation was not detected. TSH evaluation was lower among morbid obese women compared to the ones without obesity (35% versus 56.81%; p = 0.023). TSH evaluation was also lower in diabetic patients (46.15%) compared to the ones without diabetes (56.80%; p = 0.08).
TSH was more frequently evaluated in hypothyroid women under treatment (67.80% vs. 47.18%; p < 0.001) (Table 1).
The TSH figures showed hypothyroidism normal control in 1,146 (36.3%), low abnormal control in 53 (1.7%), and high abnormal control in 1,959 (62%) of the cases. The TSH figures for hypothyroidism control in untreated women were more frequently higher than 2.5 mIU/L (66.3%) compared to the figures obtained in women treated with levothyroxine (58.5%) (Table 2).
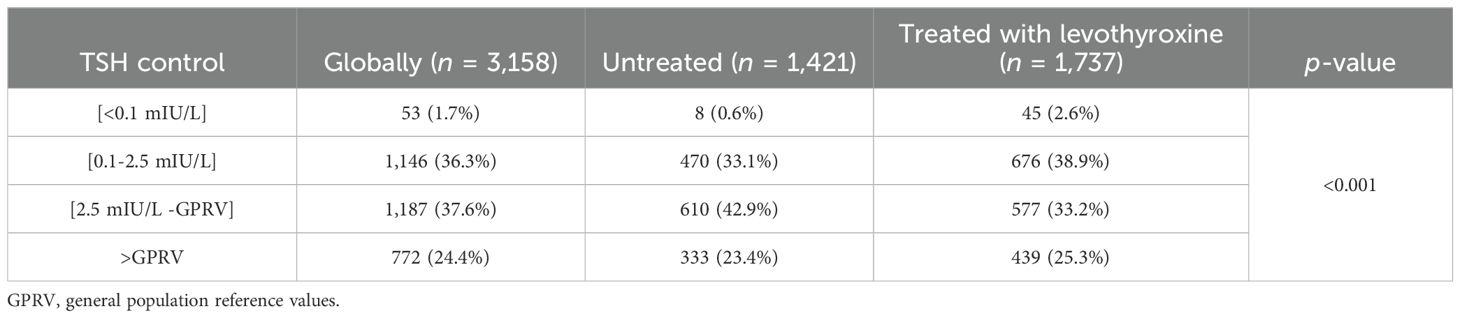
Table 2. TSH control during the first trimester of gestation in hypothyroid pregnant women, globally and according to treatment, on the date of the LMP.
No differences were observed between treated and untreated women in terms of frequency of abnormal TSH control according to GPRV.
Obesity and the interaction of diabetes with levothyroxine treatment were excluded during the variable selection process, as they did not provide enough likelihood to the model when other co-variables were present. In the final multivariate model, TSH evaluation in untreated women was inferior compared to women under treatment [OR = 0.37 (0.32, 0.42)]. It was also lower in women over 35 or with any of the covariates included in the model (diabetes, hypertension, and morbid obesity) (Table 3). The interaction between these co-variables with levothyroxine treatment showed a dilution of the effect of these co-variables in the probability of recording TSH for untreated patients, except for diabetes. Diabetes kept its OR of 0.55 (0.35, 0.87) both in treated and untreated patients. The estimated probabilities for the different profiles are presented in Supplementary Material 2.
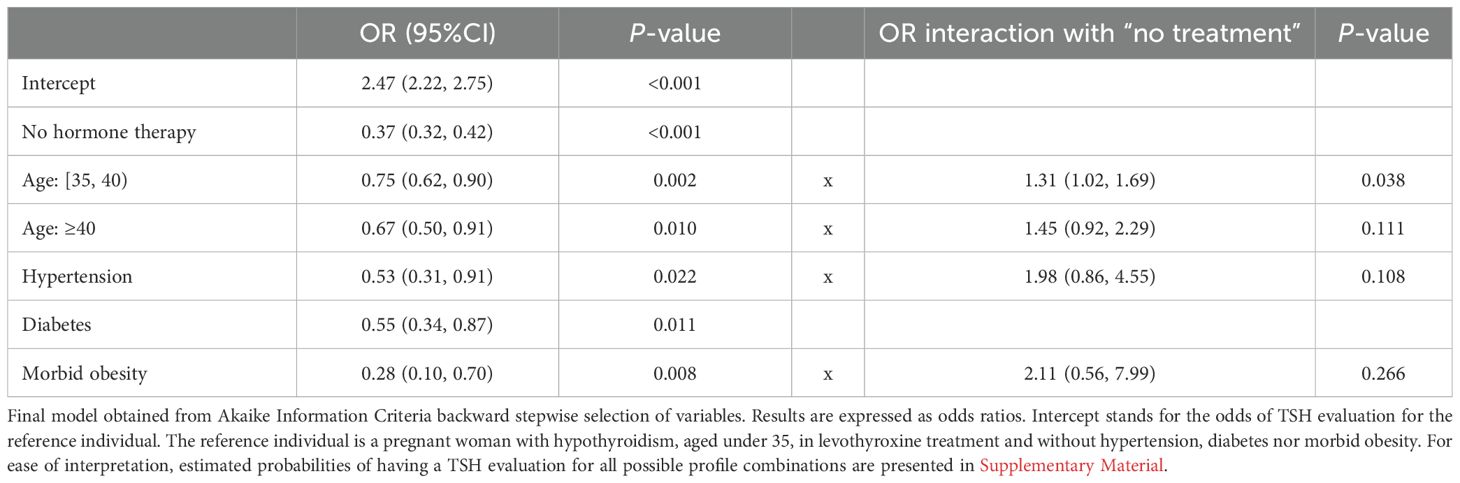
Table 3. Results from the multivariate logistic regression model explaining TSH evaluations.
This study reveals inadequate control in pregnant women with known hypothyroidism in a high percentage of pregnant women in Catalonia since 43.35% of them did not have a TSH evaluation in primary care. Moreover, among the tested ones, more than 60% were out of the recommended control ranges during gestation.
The prevalence of hypothyroidism in pregnant women observed in this study (4.98%) is lower than that reported in previous papers based on the Spanish general population ((9.1% (20)), but similar to the data published about the European general population by Taylor et al. (21) (0.2%–5.3%). Besides, it is higher than the one mentioned for the USA general population by Chaker et al. with rates between 0.3% and 3.7% (22).
The reported prevalence of hypothyroidism in pregnant women varies across different papers. This prevalence ranges from 0.3% to 1.5% for overt hypothyroidism and from 0.2% to 18% for subclinical hypothyroidism (1, 4, 7). The epidemiology of thyroid disorders is variable because it depends on multiple factors, such as illness definition, different methodology used to measure thyroid hormones, different reference ranges applied, iodine nutritional intake, thyroid autoimmunity, or the target population under study (10).
TSH was evaluated in 56.65% of the 5,574 hypothyroid pregnant women. This means that no TSH test was evaluated for almost half of the hypothyroid pregnant women during their first trimester in primary healthcare. Out of the total, 45.82% were under treatment with levothyroxine. In this group, TSH evaluation was 67.80%. This figure is significantly higher compared to the group without treatment, but it is far below the one recommended in the guidelines. ATA 2011 recommended a TSH test every 4 weeks for all hypothyroid pregnant women under levothyroxine treatment, so this figure is really alarming (5). In other papers, these rates were 57.68% (23), 75.9% (16), and 91.4% (15) for hypothyroid pregnant women under treatment.
It is not possible to compare the current study to that of Taylor et al. with almost 76% TSH evaluation, as the population in Taylor’s study (16) started hypothyroidism treatment just 6 months before pregnancy, nor to that of Granfors et al. (15) where just 163 hypothyroid pregnant women were included in the study. Moreover, in the Swedish (15) study, all TSH tests were available, hospital and primary care ones. In the present study, hospital data are not available, which could explain the difference, since pregnant women with comorbidities are monitored in hospitals in Catalonia. Nonetheless, just 1,030 hypothyroid women out of the total (18.4%) have one comorbidity including obesity, which implies that those pregnancies require hospital control.
Bivariate association between age on the date of the LMP and TSH test evaluation has not been found. Despite that ATA 2011 and 2017 recommend one TSH test in all pregnant women aged over 30 (5, 12), whether or not they have thyroid problems, just 56.66% of the cases with hypothyroidism have a TSH evaluation. If we realized that 66% of the participants were over 30 years old, a TSH test should have been ordered in all of these cases regardless of the diagnosis.
It must be acknowledged that the older the maternal age is, the more risk factors associated with pregnancy could appear, which implies an increasing need for pregnancy hospital controls. This fact could explain why pregnant women with morbid obesity have less TSH evaluations than the ones without morbid obesity (35% vs. 56.81%; p = 0.023) and the same occurs for diabetic women, with regard to the non-diabetic ones (46.15% vs. 56.80%; p = 0.08). Probably these women have been monitored in hospitals. Data from hospitals are not available in the present study.
TSH evaluation was higher in the treated group compared to the untreated one (55% vs. 44%; p < 0.001). It could be speculated that health professionals consider that untreated women have a lower risk, and for this reason, less controls are needed. Nevertheless, untreated women significantly have an out-of-range TSH percentage (p < 0.001) (TSH >2.5 mIU/L, 66.3%) with regard to the ones under treatment with levothyroxine (TSH >2.5 mIU/L, 58.5%), which implies an increased risk for these pregnancies (19).
TSH values >2.5 mIU/L were found in 62% in hypothyroid pregnant women. Such a figure is very high but similar to the ones reported in other papers (67%–69.41%) (16, 17). Moreover, in the present study, TSH values >2.5 mIU/L have been found in 58.5% pregnant women under levothyroxine treatment. This figure is slightly higher than the ones reported in other studies [50.9%–55% (15, 17)], although it is worth noting that the above mentioned reports have much lower sample sizes than the one in this study.
All of these data reveal that the recommendations in the guidelines have not been implemented. Clinical guidelines recommend to plan pregnancies and begin or increase levothyroxine treatment depending on previous TSH values when pregnancy starts (5, 12, 14). That is to say, there is a significant discrepancy between the clinical guidelines’ recommendations and daily clinical practice (16).
Even without taking into account the TSH cutoff point of 2.5 mIU/L, as recommended by ATA 2011, a large percentage of pregnant women is above the GPRV. TSH values above the GPRV are very prevalent in pregnant women, regardless of being under treatment or not. Good monitoring must be emphasized since a large number of research has proved a greater risk for pregnancies when the TSH levels are out of the recommended ranges (1–4, 6, 19).
TSH was found to be <0.1 mIU/L in 53 hypothyroid pregnant women during the first trimester (1.7%). Among the ones under levothyroxine treatment, such percentage was 2.6%. All of these women were over-treated, but this figure is lower than the one in the study of Taylor et al. (5.11%) (16). Taylor shows that TSH suppression due to overtreatment for a short period does not lead to worse perinatal results. Despite this, Lemieux et al. (23) report an increased risk of prematurity in over-treated pregnant women.
This study has some limitations. The data used come from registers that are not intended for research. Complete information on thyroid autoimmunity was not available for the whole population studied, consequently limiting the analysis of the results. There is also no direct information about the studied population’s diet, although the last study carried out in Catalonia in the pregnant population showed an adequate iodine intake (24). Some codes might not have been used properly due to human errors or difficulties in selecting the proper ICD-10 code in some cases. In addition, some codes could still be active after the illness’ resolution.
This may explain why 33.05% of women diagnosed with untreated hypothyroidism had a TSH <2.5 mIU/L. Several studies have described spontaneous remissions of subclinical hypothyroidism. The study by Rosario et al. (25), conducted in a group of 142 women between 20 and 70 years of age with subclinical hypothyroidism, shows that after 5 years of follow-up, 36% and 60% had normalized TSH, depending on whether they had positive or negative thyroid autoimmunity. Diez et al. (26) also observed regression of subclinical hypothyroidism in 52% of patients after 32 months of follow-up. Furthermore, the high percentage of women diagnosed with hypothyroidism who have a normal TSH without treatment could also be explained by the criteria used for the diagnosis (9, 10).
ESCA (Enquesta de Salut de Catalunya) (Catalan Health Survey) reveals that 25.4% of Catalan women aged between 15 and 44 had private and public health care coverage in 2014. This figure increased up to 29% during 2015 and 2016. It is not possible to know if some participants had TSH tests in private healthcare.
The relevant strengths in this study are the large sample size and the database used, which covers more than 80% of the Catalan population with more than 7 million inhabitants.
A TSH test was not evaluated in almost half of pregnant women with previously known hypothyroidism in a primary healthcare in Catalonia during the first trimester of gestation. Besides, among the tested ones, more than 60% had TSH levels out of the recommended ranges.
This study shows that it is essential to improve the management of hypothyroidism during the first trimester of pregnancy in Catalonia. It is crucial that healthcare professionals and pregnant women raise awareness that the controls have to be done earlier and regularly.
It can be concluded that there is an urgent need to improve hypothyroidism monitoring and control during the first trimester in hypothyroid pregnant women in Catalonia.
Publicly available datasets were analyzed in this study. The data that support the findings of this study are not publicly available on legal or ethical grounds, as they contain information that could compromise the privacy of research participants, but are available from Oriol Cunillera Puértolas upon reasonable request.
Study ethical protocol was approved by the Ethical Committee for Clinical Research (Comité Ético de Investigación Clínica CEIC) from IDIAP (Institut Universitari d’Investigació en Atenció Primària) Jordi Gol (P17/113). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by-product of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
GT: Writing – original draft, Writing – review & editing. OC: Data curation, Formal analysis, Methodology, Supervision, Writing – review & editing, Writing – original draft. MA: Writing – original draft, Writing – review & editing. NP: Writing – original draft, Writing – review & editing, Methodology, Supervision. MI: Writing – original draft, Writing – review & editing. GR: Writing – original draft, Writing – review & editing. SP: Writing – original draft, Writing – review & editing. LV: Writing – original draft, Writing – review & editing, Conceptualization.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the 6a Convocatòria d’Ajut SIDIAP Finançament per obtenció de dades SIDIAP (Grant number 4R17/019). This research did not receive any other specific grant from any funding agency in the public, commercial or not-for-profit sector.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1445977/full#supplementary-material
1. Delitala AP, Capobianco G, Cherchi PL, Dessole S, Delitala G. Thyroid function and thyroid disorders during pregnancy: a review and care pathway. Arch Gynecology Obstetrics. (2018) 299:327–338. doi: 10.1007/s00404-018-5018-8
2. Lee SY, Cabral HJ, Aschengrau A, Pearce EN. Associations between maternal thyroid function in pregnancy and obstetrics and perinatal outcomes. The Journal of Clinical Endocrinology & Metabolism. (2019) 105(5):2015–2023. doi: 10.1210/clinem/dgz275
3. Ge GM, Leung MTY, Man KKC, Leung WC, Ip P, Li GHY, et al. Maternal thyroid dysfunction during pregnancy and the risk of adverse outcomes in the offspring: a systematic review and meta-analysis. The Journal of Clinical Endocrinology & Metabolism. (2020) 105(12):3821–3841. doi: 10.1210/clinem/dgaa555
4. Tingi E, Syed A, Kyriacou A, Mastorakos G, Kyriacou A. Benign Thyroid disease in pregnancy: A state of the art review. J Clin Trans Endocrinol. (2016) 6:37–49. doi: 10.1016/j.jcte.2016.11.001
5. Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, et al. Guidelines of the american thyroid association for the di of thyroid disease during pregnancy and postpartum. Thyroid. (2011) 21:1081–125. doi: 10.1089/thy.2011.0087
6. Krassas G, Karras SN, Pontikides N. Thyroid diseases during pregnancy: A number of important issues. Hormones. (2015) 14:59–69. doi: 10.1007/BF03401381
7. Stagnaro-Green A, Dong A, Stephenson M. Universal Screening for thyroid disease during pregnancy should be performed. Best Pract Res Clin Endocrinol Metab. (2020) 34(4). doi: 10.1016/j.beem.2019.101320
8. López-Muñoz E, Mateos-Sánchez L, Mejía-Terrazas GE, Bedwell-Cordero SE. Hypothyroidism and isolated hypothyroxinemia in pregnancy, from physiology to the clinic. Taiwanese J Obstetrics Gynecology. (2019) 58:757–63. doi: 10.1016/j.tjog.2019.09.005
9. Springer D, Jiskra J, Limanova Z, Zima T, Potlukova E. Thyroid in pregnancy: From physiology to screening. Crit Rev Clin Lab Sci. (2017) 54(2):102–116. doi: 10.1080/10408363.2016.1269309
10. Dong AC, Stagnaro-Green A. Differences in diagnostic criteria mask the true prevalence of thyroid disease in pregnancy: A systematic review and meta-analysis. Thyroid. (2019) 29:278–89. doi: 10.1089/thy.2018.0475
11. Lee SY. Pearce EN.Assessment and treatment of thyroid disorders in pregnancy and the postpartum period. Nat Rev Endocrinol. (2022) 18:158–71. doi: 10.1038/s41574-021-00604-z
12. Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, et al. 2017 guidelines of the american thyroid association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. (2017) 27:315–89. doi: 10.1089/thy.2016.0457
13. Velasco I, Vila L, Goya M, Oleaga A, de la Calle M, Santamaria F. Documento de consenso sobre el manejo de la disfunción tiroidea durante el embarazo (SEGO/SEEN). Endocrinología Diabetes y Nutrición. (2022) 70(1):38–50. doi: 10.1016/j.endinu.2022.03.003
14. Sociedad Española de Ginecología y Obstetricia. Enfermedad tiroidea y gestación (actualizado julio 2013). Progresos Obstetricia y Ginecología. (2015) 2(58):101–11. doi: 10.1016/j.pog.2014.11.003.2015
15. Granfors M, Akerud H, Berglund A, Skogö J, Sundström-Poromaa I, Wikström AK. Thyroid testing and management of hypothyroidism during pregnancy; A population based study. J Clin Endocrinology Metab. (2013) 98(7):2687–2692. doi: 10.1210/jc.2013-1312
16. Taylor PN, Minassian C, Rehman A, Iqbal A, Draman MS, Hamilton W, et al. TSH levels and risk of miscarriage in women on long-term levothyroxine: A community-based study. J Clin Endocrinology Metab. (2014) 99:3895–902. doi: 10.1210/jc.2014-1954
17. Donnay S, Fajardo C, Fernández-García J, Torres T, Badrés O, Domínguez J, et al. Diagnosis, treatment and management of gestational hypothyroidism. The TIROGEST study. Endocrinología Diabetes y Nutrición. (2019) 67(1):36–42. doi: 10.1016/j.endinu.2029.03.008
18. Yamamoto J, Metcalfe A, Nerenberg KA, Khurana R, Chin A, Donovan LE. Thyroid function testing and management during and after pregnancy among women without thyroid disease before pregnancy. Can Med Assoc J. (2020) 192:596–602. doi: 10.1503/cmaj.191664
19. Soldevila B, Hernández M, López C, Cecenarro L, Martínez-Barahona M, Palomera E, et al. Impact of TSH during the first Trimester of pregnancy on obstetric and fetal complications: Usefulness of 2.5 mIU/L cut-off value. Clin Endocrinol. (2018) 88(5):728–734. doi: 10.1111/cen.13575
20. Valdés S, Maldonado-Araque C, Lago-Sampedro A, Lillo J, García-Fuentes E, Perez-Valero V, et al. Population-based national prevalence of thyroid dysfunction in Spain and associated factors:RGlAYmV0LmVzstudy. Thyroid. (2016) 27(2):156–66. doi: 10.1089/thy.2016.0353
21. Taylor PN, Albrecht D, Scholz A, Gutíerrez-Buey G, Lazarus JH, Dayan CM, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Reviews/Endocrinology. (2018) 14:301–3016. doi: 10.1038/nrendo.2018.18
22. Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. (2017) 390:1550–62. doi: 10.1016/S0140-6736(17)30703-1
23. Lemieux P, Yamamoto JM, Nerenberg KA, Metcalfe A, Chin A, Khurana R, et al. Thyroid laboratory testing and management in women on thyroid replacement before pregnancy and associated pregnancy outcomes. Thyroid. (2020) 31(5):1–9. doi: 10.1089/thy.2020.0609
24. Torres MT, Francés L, Vila L, Manresa JM, Falguera G, Prieto G, et al. Iodine nutritional status of women in their first trimester of pregnancy in Catalonia. BMC Pregnancy Childbirth. (2017) 17:249. doi: 10.1186/s12884-017-1423-4
25. Rosário PW, Carvalho M, Calsolari MR. Natural history of subclinical hypothyroidism with TSH ≤10 mIU/l: a prospective study. Clin Endocrinol (Oxf). (2016) 84:878–81. doi: 10.1111/cen.12939
Keywords: hypothyroidism, pregnancy, prevalence, hypothyroidism monitoring, hypothyroidism control
Citation: Tena Vivó G, Cunillera Puértolas O, Albareda Riera M, Parellada Esquius N, Isidro Albaladejo M, Rodríguez Palomar G, Palmero Aliste S and Vila L (2025) Hypothyroidism monitoring and control during the first trimester of pregnancy in Catalonia. Front. Endocrinol. 16:1445977. doi: 10.3389/fendo.2025.1445977
Received: 08 June 2024; Accepted: 17 February 2025;
Published: 18 March 2025.
Edited by:
Terry Francis Davies, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Mariacarla Moleti, University of Messina, ItalyCopyright © 2025 Tena Vivó, Cunillera Puértolas, Albareda Riera, Parellada Esquius, Isidro Albaladejo, Rodríguez Palomar, Palmero Aliste and Vila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oriol Cunillera Puértolas, b2N1bmlsbGVyYS5pZGlhcEBnbWFpbC5jb20=; Glòria Tena Vivó, Z3RlbmFAZ2VuY2F0LmNhdA==; Z2xvcmlhdGVuYXZpdm9AZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.