
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Endocrinol., 28 February 2025
Sec. Bone Research
Volume 16 - 2025 | https://doi.org/10.3389/fendo.2025.1356831
 Jing Luo1†
Jing Luo1† Qian Wang1,2†Wenhong Liu1†Huazhi Liao1Weipeng Qing1
Qian Wang1,2†Wenhong Liu1†Huazhi Liao1Weipeng Qing1 Minyi Zhang3Deqiu Tang1Guanghua Luo1*
Minyi Zhang3Deqiu Tang1Guanghua Luo1* Heng Zhao1*
Heng Zhao1*The global trend towards longer lifespans has led to an aging population and a rise in the prevalence of diseases that predominantly affect elderly people. Coronary artery calcification (CAC) and osteoporosis (OP) are common in elderly populations. CT scans provide a reliable method to assess and monitor the progression of these diseases. In this review, the relationship between OP and CAC in terms of pathophysiological mechanism, comorbidity risk factors and clinical manifestations is reviewed, with a focus on the advancements in CT imaging, clinical applications and the possibility for “one-stop-shop” for examination.
The global trend towards longer lifespans has led to an aging population and a rise in the prevalence of diseases that predominantly affect elderly people (1). Coronary artery disease (CAD) and osteoporosis (OP) are two clinical diseases influenced by aging, and often coexisting (2). Coronary artery calcification (CAC) is a marker of coronary atherosclerosis, indicating the presence of CAD, and regardless of the presence of risk factors or symptoms, serving as a definite predictor of future cardiac events (3, 4). Cardiovascular calcification is a widespread condition that that primarily affects the elderly population. Surprisingly, it is even more prevalent in OP patients (5). Compared with the general population, individuals with reduced bone mass and OP are at a higher risk of cardiovascular diseases. In one study, Chen et al. found that OP patients had a higher risk of CAD (6). Likewise in the presence of CAD, patients with low bone mineral density may have higher incidence rate and mortality, irrespective of age or conventional cardiovascular risk factors (2). Vascular calcification (VC) is an active process similar to bone formation and it is controlled by complex enzymatic and cellular pathways (7, 8). OP and cardiovascular calcification share common risk factors, including age, sex, inflammation and unhealthy lifestyle, which may partly explain the association between OP and CAC (9). Both diseases can be prevented or slowed by alleviating or treating modifiable risk factors. With the aging of global population and the rapidly growing burden of complications, the clinical applications of computed tomography (CT) scans continues to grow. Despite this, OP remains largely underdiagnosed and undertreated, leveraging CT images acquired for diverse indications (e.g., chest, heart, coronary artery, etc.) to opportunistically screen for OP offers a promising strategy to enhance its detection rate. CAC can be easily quantified via CT and expressed as a CAC score (CACS). This means that a single CT scan could potentially be used to evaluate both OP and CAC.
In this review, the relationship between OP and CAC in terms of pathophysiological mechanism, comorbidity risk factors and clinical manifestations is reviewed, with a focus on the advancements in CT imaging, clinical applications and the possibility for “one-stop-shop” examination.
There is a growing body of studies regarding the correlation between CAC and BMD, however, there are still conflicting results regarding these two age-related disorders. A study conducted in the Copenhagen general population reported a negative correlation between BMD and CAC in both men and postmenopausal women. This suggests that reduced bone density may increase the risk of CAC, regardless of gender. Xu et al. investigated the relationship between BMD and CAC in postmenopausal women, finding that women with low BMD were at a higher risk for CAC (10). In contrast, a study from China found no direct relationship between OP and CAC in elderly men after adjusting for age and other influencing factors (11). A study in middle-aged women had shown a direct association between high CAC and BMD, but no association in adjusted group for age and shared risk factors (12). Additionally, BMD varies by anatomical site and the relationship between BMD at different measurement sites and CAC also differs. A study on postmenopausal women also suggested that BMD at the spine and femoral neck, measured by dual-energy X-ray absorptiometry (DXA), were independent markers for an increased risk of CAC (10). Similarly, a Swedish study reported that the BMD in the trabecular bone volume of the 12th thoracic vertebra vertebra, measured by quantitative computed tomography (QCT), was negatively correlated with CAC in women, but the BMD in the cortical bone volume of the right femur was directly and independently correlated with CAC (13). This opposite relationship may be explained by the differences in mineral regulation of trabecular bone and cortical bone and may indicate distinct pathophysiologic mechanisms exist for the trabecular vs cortical bone in the bone-vascular axis (Table 1).
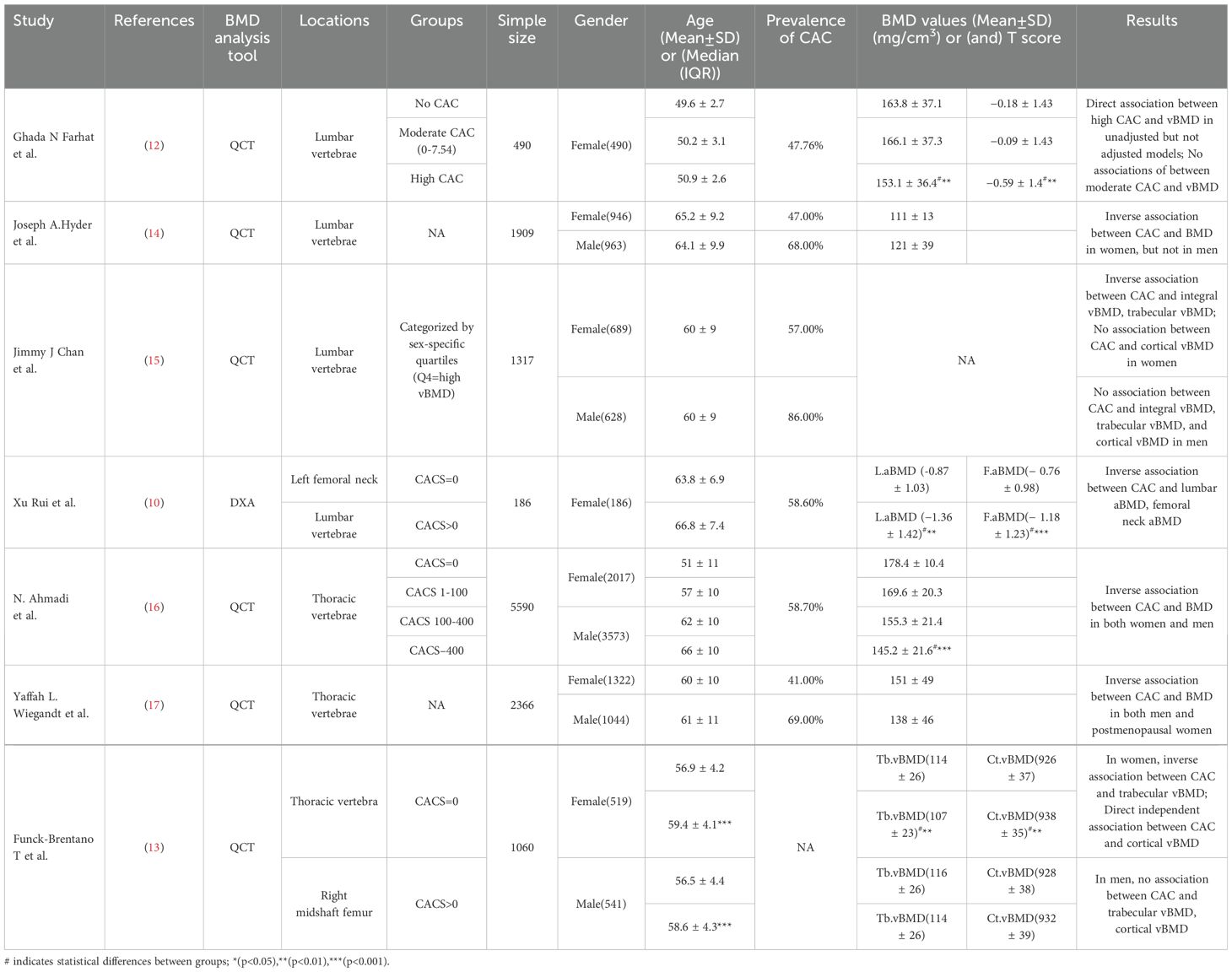
Table 1. Associations of BMD and CAC.
Biomineralization is considered as the deposition of minerals in an organized manner on a matrix (18). Apart from the skeleton, the most common structure in humans to undergo calcification is the vascular system, where VC represents an active regulatory form of tissue biomineralization (19). Mineralization is crucial for the maintenance of normal skeletal health. However, the deposition of minerals in soft tissues, especially in the vascular system, is typically pathological and linked to an increased risk of adverse cardiovascular events (20). Notably, ectopic arterial calcification is frequently accompanied by decreased BMD or disturbed of bone turnover (21). At the molecular level, the various biomarkers involved in the osteogenic processes can be discovered in calcified vascular segments (22). Cellular, endocrine and metabolic signals flow bidirectionally between the vascular system and the skeleton, which is essential for the maintenance of both bone and vascular health (19) (Figure 1).
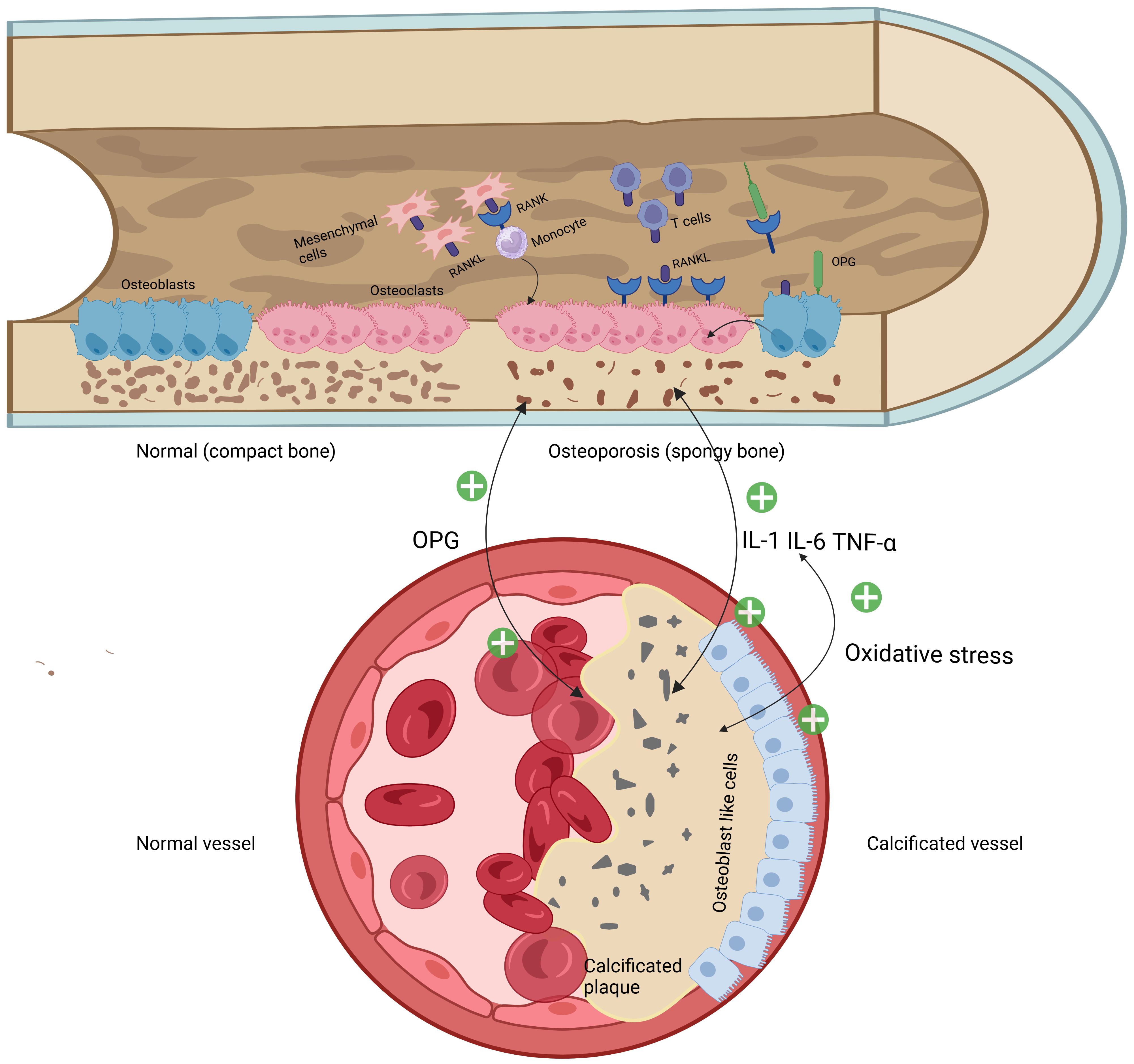
Figure 1. Mechanical diagram of bone-vascular axis regulation.
Osteogenesis is a process carried out in two steps: the secretion of extracellular matrix by osteoblasts and the subsequent mineralization of the matrix (23). This process is regulated by numerous cellular pathways and bone-related proteins, such as the RANK/RANKL/OPG pathway, osteopontin (OPN), bone morphogenetic proteins (BMP) and alkaline phosphatase (ALP). Among these, the RANK/RANKL/OPG pathway plays a critical role in maintaining bone homeostasis and is also implicated in various pathological processes, including atherosclerosis and cardiovascular diseases (24).
RANKL is a type II transmembrane protein expressed by osteoblasts, osteocytes and immune cells within bone tissues. Its receptor, RANK is a type I transmembrane protein located on osteoclast progenitor cells, mature osteoclasts and immune cells (25). Under normal physiological conditions, the interaction between RANKL and RANK plays a pivotal role in stimulating osteoclastogenesis, bone remodeling, and maintaining calcium homeostasis (24). Osteoprotegerin (OPG), a member of the TNF receptor superfamily, is secreted by osteoblasts and acts by binding to RANKL and disrupting the RANK-RANKL interaction, inhibiting osteoclast formation and bone resorption (26). The RANK/RANKL/OPG pathway has emerged as a potential connection between osteoporosis and coronary artery CAC (27). Mice with OPG gene knockout exhibit both VC and brittle fractures (28).On the contrary, OPG treatment has been shown to prevent VC induced by vitamin D and warfarin in rats, as well as inhibit the calcification of vascular smooth muscle cells (VSMCs) in vitro (29). These findings suggest that OPG may act as a molecular link between the vascular and bone systems. Paradoxically however, in human studies, serum OPG levels were increased in patients with CAD and correlated with their severity, ischemic cardiac decompensation, and future cardiovascular events (30, 31). They proposed that OPG may be passively elevated as a protective factor against vascular calcification. Therefore, it is possible that OPG could be a potential biomarker in early identification and monitoring patients with cardiovascular disease (32).
VC is an active regulatory form of extracellular matrix biomineralization. Ectopic biomineralization of the vascular walls begins with impaired endothelial function. Repeated endothelial dysfunction leads to excessive calcium transport from bones to the vascular walls, ultimately resulting in VC and OP (33). Osteopontin (OPN) is an extracellular matrix protein involved in bone metabolism and osteoclast activation. It facilitates the attachment of osteoclasts to the extracellular matrix by tightly binding to hydroxyapatite. Studies have confirmed that OPN is rarely expressed in normal arterial walls, but its expression is significantly elevated in the neointima formed after various pathological damages to the vessels, which proves that it can promote the adhesion, proliferation and migration of VSMCs and fibroblasts, and enhance the chemotaxis of macrophages (34). This eventually leads to the transformation of VSMCs from a contractile phenotype to an osteogenic phenotype. The discovery that bone morphogenetic protein (BMP) is abundantly expressed in calcified areas of atherosclerotic vessels preliminarily determines its ability to promote abnormal calcification (35–37). Subsequent research has shown that BMP ligands play a key role in the development and homeostasis of the vascular system (38). BMP-2 stands out as a cytokine with strong osteogenic activity and can induce ectopic osteogenesis (39). It can trigger cell chemotaxis, mitotic proliferation, cell differentiation and ultimately lead to ectopic bone formation, and the development of VC through mechanisms such as microRNAs, MGP, apoptosis, oxidative stress and hyperglycemia (40).
The endocrine system also participates in the regulation of calcification. An important process of VC is the transformation of VSMCs from a contractile phenotype to an osteoblastic phenotype. Among the molecules involved in this process, parathyroid hormone (PTH) plays a key role via multiple mechanisms, including the regulation of the RANK/RANKL/OPG system and the Wnt/β-catenin pathway, which are the main pathways for bone resorption and formation respectively (41). In addition, PTH also regulates the action of several VC promoters, like calcium, phosphorus and vitamin D.
Sex hormones, especially estrogen, regulate bone metabolism by acting on receptors on osteoblasts and osteoclasts, and a deficiency of sex hormones can eventually lead to OP (9). Estrogen reduces the responsiveness of osteoclast precursors to RANKL, interfering with osteoclast signaling pathways and inhibiting osteoclast differentiation. The withdrawal of estrogen after menopause affects the normal balance between RANKL and OPG, ultimately prolonging the life of osteoclasts and promoting bone resorption (42). Sex hormones are known to affect the development of atherosclerotic disease, with women experiencing a 10-15 year delay in the onset of the disease compared to men, possibly due to the protective effect of estrogen in the years prior to menopause. Increasing evidence has suggested that endogenous estrogen plays a protective role against CAD in postmenopausal women and its deprivation worsens CAD progression after menopause. The reduction in estrogen also increases the risk of OP (10, 43–45).
The mineral component of bone is hydroxyapatite (HA), with the chemical formula Ca10(PO4)6(OH)2, formed by inorganic phosphate and calcium ions (Ca2+). Calcium-phosphorus metabolism is regulated by a wide variety of local and systemic factors. The coordinated actions of these substances prevent both low and high mineralization, both of which are detrimental to bone function. For this reason, the balance between calcification inducers and calcification inhibitors in the body is crucial for maintaining biomineralization. Pyrophosphate (PPi) is a local inhibitor of mineralization. Extracellular PPi effectively inhibits the ability of Ca2+ to crystallize with Pi and form HA and it strongly binds to the surface of HAP, thereby preventing further crystal growth (46).
Alkaline phosphatase (ALP), a membrane-bound extracellular enzyme, facilitates calcification by hydrolyzing phosphodiester bonds to release phosphate (47). Tissue-nonspecific ALP (TNSALP)-knockout mice exhibit skeletal deformities, impaired bone mineralization, and premature mortality due to seizures before weaning, consistent with the vital role of ALP in bone health (48, 49). Research has shown that TNSALP expression increases in a calcification environment and this enzyme inhibition can reduce calcification in VSMCs (50, 51).
There exist some genes that contribute to the comorbidity of VC and OP. Previous study has shown that mice with OPG gene knockout exhibit VC and fragility fractures (28). As one of the OPG promoter polymorphisms (950 T→C), it is not related to OP, but is associated with vascular morphology and function (52). One study found that the proportion of OPG gene haplotypes significantly increased in CAD patients, and that serum OPG levels were also associated with the presence of the C allele at position 950, suggesting that variations in the OPG gene can increase the risk of CAD (53). The above researches indicate that defects in the OPG gene are closely related to the occurrence of OP and CAD. Moreover, a study indicated that biallelic ENPP1 deficiency can lead to systemic arterial calcification in infants, while a heterozygous ENPP1 deficiency may result in early-onset OP (54). This suggests that mutations in ENPP1 may also be a factor contributing to the co-morbidity of CAC and OP. However, there are currently few studies on the genetic links between CAC and osteoporosis, and further exploration is needed to determine whether there are other genes causing its changes.
Both OP and CAC share certain risk factors, such as ageing, sex, inflammation and unhealthy lifestyle.
Cardiovascular calcification is a common disease in the elderly population, especially affecting most people over the age of 60, and is more common in patients with OP (10). According to the latest statistics from the International Osteoporosis Foundation, in the global context, one-third of women over 50 and one-fifth of men will experience an osteoporotic fracture during their lifetime (17).
Lower BMD was associated with higher coronary calcification and coronary plaque burdens in postmenopausal women, independent of cardiovascular risk factors and age (55). Hyder et al. demonstrated an inverse association between CAC and lumbar BMD in women, but not in men (14). Similarly, Chan et al. displayed an inverse association between CAC and integral vBMD, trabecular vBMD in women, but not in men (15). This may be due to estrogen deficiency in postmenopausal women, which leads to decreased cardiovascular and bone protection.
Another potential mechanism linking CAC and OP is that both processes are tissue-specific responses to chronic inflammation. Calcification results from the impaired clearance of Ca2+ following tissue damage, particularly during inflammation (56). Within atherosclerosis, inflammatory processes are triggered by the accumulation and oxidative modification of lipids within the subendothelial region. Initial calcification manifests within the lipid-rich core of the atheroma, adjacent to infiltrating inflammatory cells within the fibrocalcific plaque (57, 58). Previous studies by Al-Aly et al (59) and Cheng (60) et al. have demonstrated that the inflammatory cytokine tumor necrosis factor-α exerts significant control over osteochondrogenic differentiation in osteoblastic and vascular cells via modulation of the Msx2 and Wnt signaling pathways.
Sedentary lifestyle is associated with both cardiovascular disease and osteoporosis (61).The health of bones depends on optimal nutrition. Fruits and vegetables contain many nutrients that are essential for maintaining bone health such as magnesium, vitamin C, potassium and carotenoids (62). Smoking has a direct impact on the physiological activity of nuclear factor kappa-B receptor activator (RANKL), osteoprotegerin and osteoblasts (63). Interestingly, quitting smoking has been reported to reverse its effects on BMD (64).
CAC is an independent risk factor of major adverse cardiovascular events (65). There are two main methods of CT to assess CAC, one is non-contrast CT to measure calcification score, and the other is coronary artery CT angiography (CCTA) to detect both calcified and non-calcified plaques and measure the resulting degree of luminal stenosis (66). CT is a non-invasive examination method commonly used in clinical practice, which with high sensitivity and specificity for detecting calcium, and is able to quantify calcification (67).
Agatston et al. in 1990 initially described a quantitative index of CAC which was later named Agatston score. They acquired coronary artery images by an electrocardiogram (ECG)-gated non-contrast CT, 20 contiguous slices were obtained below the bifurcation of the main pulmonary artery, with a 100 ms scan time, a 3 mm slice thickness, each image slice was triggered at 80% of the patient’s RR interval. A calcific lesion is defined as lesion with a CT attenuation threshold of 130 Hounsfield units (HU) and an area greater than 1mm2. A calcification score for each lesion is calculated by multiplying the lesion area and the density score that is determined based on maximal CT attenuation of measured lesion (density score: 1 = 130 to 199, 2 = 200 to 299, 3 = 300 to 399 and 4 = ≥ 400), then add the score of calcified coronary lesions at all levels to calculate total Agatston score (68).
Agatston score remains the standard reference for quantifying CAC and most widely used in clinical practice (69). With the development of high-resolution CT, the coronary artery scanning protocol has also been optimized, and the parameters are as follows: 120 kVp with variable mA according to patient body weight, slice thickness of ≤1.25 mm can be obtained, scan range from the level of the tracheal carina to the bottom of the heart. CAC provides great value for risk stratification of patients with cardiovascular disease, and is the gold standard method of assessing subclinical atherosclerosis (70). A meta-analysis by Abuzaid et al. had showed that compared with absence of CAC, CAC > 0 was associated with an increased risk of major adverse cardiovascular and all-cause mortality in both asymptomatic and symptomatic population in patients without an established diagnosis of CAD (71). A large-scale study of multiple ethnicities with a median follow-up of 11.7 years showed that the risk of total and CAD mortality increased with increasing levels of CAC (72). Moreover, A diabetes heart study demonstrated that CAC score had a higher predictive value of cardiovascular risk than the Framingham risk score (FRS) (73). Therefore, CAC has an incremental predictive value, and CT can accurately quantify and grade CAC, which is of great guiding significance for clinical diagnosis and treatment. It is worth noting that multiple studies had shown patients with higher CAC had lower BMD (16, 74), and the prevalence of CAD increased in populations with OP or osteopenia (75). This reminds us the importance of simultaneously evaluating CAC and BMD to screen for osteoporosis in patients with CAD in clinical practice.
Compared to non-contrast CT, in addition to detecting calcified plaques, CCTA can also detect mixed plaques and non-calcified plaques, and identify vascular stenosis. CCTA is an excellent non-invasive imaging modality of excluding CAD (66). Although CAC was significantly associated with adverse cardiovascular events, no CAC did not completely rule out obstructive CAD (76), and minimal CAC is also not exactly an indication of a small risk of malignant cardiovascular events. Spotty calcification is a feature of vulnerable plaques (77). Studies have proposed that spotty calcification is more likely to develop into unstable plaques and rupture abruptly leading to myocardial infarction (MI), while extensive calcification tend to develop into stable plaques and cause myocardial ischemia and angina (78, 79). A prospective cohort study revealed that compared with individuals with the absence of CAC, those with a minimal CAC were more likely to have hypertension, dyslipidemia and a family history of heart attack (80). And people with minimal CAC had a threefold higher risk of developing coronary heart disease compared with a CAC = 0 (81). Moreover, a recent study showed that patients with CAC measured by CTA have lower bone mineral density compared with those without CAC in postmenopausal women, and every 10 units of CACS increase, the risk of OP increases by 2% (82). Therefore, it is important to rule out severe coronary artery disease and screen for osteoporosis even in populations with very low CACS.
However, it is worth noting that evaluating BMD through contrast-enhanced CT scans of patients can lead to severe overestimation, and in clinical practice, relevant adjustments need to be made before implementing contrast-enhanced imaging for BMD screening (83).
OP remains largely underdiagnosed and undertreated. Clinically, BMD measured by DXA is commonly used to assess OP. Its advantages are being convenient to operate, low cost, and low radiation, while the disadvantage is that DXA can only measure area bone density, which cannot reflect the three-dimensional characteristics of the bone (84). Three-dimensional imaging by CT to assess OP can be a good way to overcome this disadvantage. Based on CT images clearly display the anatomical structure of bone, the BMD of trabecular, cortical, or integral bone, centrally or peripherally can all be quantitatively measured (85). BMD measurements by CT are less influenced by vascular calcifications, abnormal bone changes (e.g. spine degenerative diseases, scoliosis, kyphosis, etc.), patient positioning errors, and various artifacts (86). Quantitative computed tomography (QCT) is an excellent diagnostic tool for OP and equipped with those advantages.
As early as the 1980s, CT can be used to assess for OP (87). The measurement of BMD by QCT requires a special calibration phantom and professional post-processing software, on which the attenuation values on the clinical CT images can be converted to the equivalent density of hydroxyapatite (88). Compared with DXA, a projectional method for measuring BMD, QCT can measure cortical bone separately from trabecular bone, which has a larger surface area and is more metabolically active, allowing for more sensitive detection of OP (89). Traditional calibration phantoms are made with known amounts of HA or potassium phosphate and are placed under the subject’s lower back while simultaneously undergoing CT scanning, which referred to as “synchronous calibration” (86). However, calibration phantom is not convenient in clinical practice, because the vast majority of CT scans are not initially intended to assess for OP, thus the phantom is not scanned simultaneously with patients. Nowadays, there is an asynchronous calibration phantom can be scanned separately from the subject and then the CT images that have been scanned can be transferred by to specialized post-processing software for subsequent BMD assessment (90). Based on this asynchronous calibration, images taken for other purposes, such as chest, abdomen, pelvis, etc., can be retrospectively used to measure BMD, providing great convenience for clinical practice. Besides, Funck-Brentano T et al. demonstrated CAC was inversely associated with trabecular QCT volumetric BMD (QCT-vBMD) of thoracic vertebra, but was directly and independently associated with cortical QCT-vBMD of midshaft femur in women (13). This opposite connection may be due to differences in the regulation of trabecular and cortical bone, further reflecting differences in the mechanism of mineral transformation of coronary calcification to trabecular and cortical bone.
Because of the spatial resolution of clinical whole-body CT scanners is not enough, measurements of cortical BMD in the femoral neck and the vertebral body may be insufficiently accurate (91). High-resolution peripheral QCT (HR-pQCT) scanners sufficiently improve spatial resolution for evaluating distal tibia and radius (91). It is an imaging technique designed for in vivo 3D evaluation of the volumetric BMD (vBMD), geometry and microstructure of distal radius and tibia, making it a unique tool for obtaining alternative quantitative measurements of bone strength. The small isotropic voxel size achieved by HR-pQCT (82mm or 61mm) can distinguish cortical and trabecular bone compartments, visualize and quantify trabecular microstructure and cortical porosity (92–94). Thus, additional information can be obtained for osteoporosis evaluation. A Framingham Study of QCT-vBMD and VC reported that CAC was negatively associated with integral vBMD, trabecular vBMD of lumbar vertebra, but no association with cortical vBMD (15). This may indicate that the mechanisms of cortical bone and trabecular bone in the bone-vascular axis are inconsistent. Despite this, due to the insufficient spatial resolution of clinical whole-body CT scanners, the measurement of vertebral and femoral cortical bones may be inaccurate. Therefore, HR-pQCT, specialized in the assessment of cortical bone, is necessitated to further evaluate the relationship between CAC and cortical bone BMD.
Although QCT is gradually replacing DXA as the gold standard for measuring BMD, it is still limited in clinical use due to the need for specific phantom and dedicated software for assessment of osteoporosis. Efforts are underway to validate the application of opportunistic screening based on clinical CT scans—i.e., without calibration phantoms—for assessing OP (95). While Josephine et al. measured pelvic bone density using two calibration techniques (phantom-based and non-phantom-based) and found insufficient consistency to support interchangeability (96). Nevertheless, multiple studies have shown that measuring trabecular HU in routine CT scans can be an effective tool for the opportunistic evaluation and screening of OP, yielding promising results (97, 98). The vast majority of CT images in clinical practice contain skeletal composition information, from which the HU values of trabecular bone can be conveniently obtained. Therefore, CT scans of the chest, abdomen, pelvis, and spine for any clinical indications can be used to screen for OP without additional burden to the patient of radiation exposure, examination time, or image acquisition cost (86), thus OP can be extensively screened and substantially improve diagnosis in clinical practice. There was a clinical studies shown that patients with lower thoracic BMD measured by cardiac CT have a higher risk of fractures (99). A large cohort study had reported that the threshold for distinguishing OP from osteopenia was 90% sensitivity at 160 HU and more than 90% sensitivity at 110 HU (98). A recent Chinese study had revealed an excellent correlation between the average volume HU values of L1 and L2 and BMD measured by QCT (r = 0.941, P < 0.001), and the optimal thresholds of ROC for diagnosing osteopenia and OP were 154.73HU (sensibility 92.9%) and 106.52HU (sensitivity 86.6%), respectively (100). These studies have drawn similar conclusions, confirming the effectiveness of volumetric HU in predicting the occurrence of OP. Therefore, HU value can be used as a supplement method for clinical screening of OP. Moreover, studies had shown a significant inverse association between the HU value of vertebrae and CAC (101, 102), and the CT values of thoracic cancellous bone were significantly negatively correlated with the number of branches involved in coronary artery calcification and severity, which synchronously obtained coronary calcification date and thoracic cancellous bone CT measurements in one-time coronary spiral CT scan, able to achieve “one-stop-shop” targeted analysis (101).
As early as the 1980s, there were studies using dual-energy CT(DECT) to measure the bone mineral mass of human vertebrae in vitro (103, 104). Since different tissue components exhibit variable attenuation at two different rapid-switching X-ray spectral energy levels, DECT can distinguish different materials and identify diverse body contents (105, 106). Based on this material decomposition (MD) technology, DECT is superior to conventional single-energy CT in material separation, and it has been carried out in various musculoskeletal applications such as measuring bone density, analyzing bone composition, and detecting bone trauma, which provided more clinically relevant information (106–108). Studies had compared the accuracy of bone component values directly quantified by DECT MD technology with the vBMD values of vertebral bodies measured by QCT, and derived different results (109, 110). Zhou et al. further proposed an indirect quantification method through linear regression calibration, which demonstrated the indirect method was in good agreement with the QCT, while the direct method was not accurate enough (110), implying the MD technology does not directly reflect the content of human tissue. In this study, CT imaging was performed with a Revolution GSI CT scanner (GE Medical Systems, Milwaukee, WI, USA), then the raw image data were transmitted to an advanced workstation (ADW4.6; GE Medical Systems) – which is also equipped with an Agatston score analysis technique – for BMD assessment by MD technique, thus a single DECT scan can be used for simultaneous post-processing analysis of BMD and CAC.
With the continuous progress of mineral metabolism research in vivo, the view that OP and vascular calcification share common pathophysiology mechanism and interact with each other has been more and more recognized, and the bone-vascular axis has attracted increasing attention. Multiple studies had confirmed there were coexisting risk factors in both diseases, including aging, estrogen deficiency, inflammation, and unhealthy lifestyle (55, 111, 112), and there were complex relationships in age, sex and anatomical sites between these diseases (2, 56).
Many methods are able to visually and assess calcification in vivo. Due to its high contrast resolution and short examination time, CT is widely used in clinical practice and can be conveniently used to quantitative calcified components and effectively monitor their progression. Clinical whole-body CT scanners provide images for diagnostic purposes while also reflecting a variety of additional body composition information, such as the attenuation of calcification (or mineralization), with no additional increase in radiation exposure, examination time, or image acquisition costs (86). Therefore, A routine CT scan can simultaneously detect vascular calcification and OP and provide quantitative data. For example, coronary spiral CT image can be used to reflect the bone density of patients by simultaneously detecting the CT value of thoracic cancellous bone (101). Moreover, the images by routine CT involved coronary, heart or chest can be used to detect CAC and transferred to the QCT post-processing station for BMD measurement, thus we can achieve “one-stop-shop” examination for OP and CAC. In this way, the detection rate of OP may be substantially improved, the preventive measures can be actively taken in the primary care setting in patients with CAD.
Overall, numerous studies have shown that the bone-vascular axis is the common pathological basis for CAC and OP. The relationship between CAC and bone density varies across age, gender and different anatomical sites. CT provides a reliable means of synchronously evaluating CAC and vertebral BMD in single scan, and monitoring the progression and response to therapy. The “one-stop-shop” examination provides great help in the screening, prevention, and management of clinical diseases.
JL: Writing – original draft. QW: Investigation, Project administration, Writing – original draft. WL: Investigation, Project administration, Writing – original draft. HL: Investigation, Project administration, Writing – original draft. WQ: Visualization, Writing – original draft. MZ: Visualization, Writing – original draft. DT: Funding acquisition, Supervision, Writing – review & editing. GL: Funding acquisition, Supervision, Writing – review & editing. HZ: Conceptualization, Funding acquisition, Project administration, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Natural Science Foundation of Hunan Provincial of China (Grant No.2023JJ30554 (HZ), 2021JJ30621(DT)), the Scientific Research Project of Department of Education of Hunan Province (Grant No.20A437 (HZ)), the Scientific Research Project of Health Commission of Hunan Province (Grant No.202109040556 (HL), D202309019457 (HL), B202309018212(GL), 202109010099(DT)), the College Student Innovation and Entrepreneurship Training Project of the University of South China (Grant No.2022X10555118 (MZ)).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lorentzon M, Cummings SR. Osteoporosis: the evolution of a diagnosis. J Internal Med. (2015) 277:650–61. doi: 10.1111/joim.12369
2. Khandkar C, Vaidya K, Karimi Galougahi K, Patel S. Low bone mineral density and coronary artery disease: A systematic review and meta-analysis. Int J Cardiol Heart Vasculature. (2021) 37:100891. doi: 10.1016/j.ijcha.2021.100891
3. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with framingham score for risk prediction in asymptomatic individuals. JAMA. (2004) 291:210–5. doi: 10.1001/jama.291.2.210
4. Criqui MH, Denenberg JO, Ix JH, McClelland RL, Wassel CL, Rifkin DE, et al. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA. (2014) 311:271–8. doi: 10.1001/jama.2013.282535
5. Demer LL, Tintut Y. Mechanisms linking osteoporosis with cardiovascular calcification. Curr Osteoporosis Rep. (2009) 7:42–6. doi: 10.1007/s11914-009-0008-1
6. Chen S-J, Lin C-S, Lin C-L, Kao C-H. Osteoporosis is associated with high risk for coronary heart disease: A population-based cohort study. Medicine. (2015) 94:e1146. doi: 10.1097/MD.0000000000001146
7. Johnson RC, Leopold JA, Loscalzo J. Vascular calcification: pathobiological mechanisms and clinical implications. Circ Res. (2006) 99:1044–59. doi: 10.1161/01.RES.0000249379.55535.21
8. Lee SJ, Lee I-K, Jeon J-H. Vascular calcification-new insights into its mechanism. Int J Mol Sci. (2020) 21:2685. doi: 10.3390/ijms21082685
9. Azeez TA. Osteoporosis and cardiovascular disease: A review. Mol Biol Rep. (2023) 50:1753–63. doi: 10.1007/s11033-022-08088-4
10. Xu R, Yang H-N, Li Y-Q, Wang Q-F, Guo A-H, Ayiti A, et al. Association of coronary artery calcium with bone mineral density in postmenopausal women. Coronary Artery Dis. (2016) 27:586–91. doi: 10.1097/MCA.0000000000000402
11. Lin T, Liu JC, Chang LY, Shen CW. Association between coronary artery calcification using low-dose mdct coronary angiography and bone mineral density in middle-aged men and women. Osteoporosis international: J established as result cooperation between Eur Foundation Osteoporosis Natl Osteoporosis Foundation USA. (2011) 22:627–34. doi: 10.1007/s00198-010-1303-5
12. Farhat GN, Cauley JA, Matthews KA, Newman AB, Johnston J, Mackey R, et al. Volumetric bmd and vascular calcification in middle-aged women: the study of women’s health across the nation. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (2006) 21:1839–46. doi: 10.1359/jbmr.060903
13. Funck Brentano T, Grahnemo L, Hjelmgren O, Brandberg J, Bergström G, Ohlsson C, et al. Associations of trabecular and cortical volumetric bone mineral density with coronary artery calcification score: the swedish cardiopulmonary bioimage study pilot study. JAMA Cardiol. (2021) 6:238–40. doi: 10.1001/jamacardio.2020.4880
14. Hyder JA, Allison MA, Wong N, Papa A, Lang TF, Sirlin C, et al. Association of coronary artery and aortic calcium with lumbar bone density: the mesa abdominal aortic calcium study. Am J Epidemiol. (2009) 169:186–94. doi: 10.1093/aje/kwn303
15. Chan JJ, Cupples LA, Kiel DP, O’Donnell CJ, Hoffmann U, Samelson EJ. Qct volumetric bone mineral density and vascular and valvular calcification: the framingham study. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (2015) 30:1767–74. doi: 10.1002/jbmr.2530
16. Ahmadi N, Mao SS, Hajsadeghi F, Arnold B, Kiramijyan S, Gao Y, et al. The relation of low levels of bone mineral density with coronary artery calcium and mortality. Osteoporosis international: J established as result cooperation between Eur Foundation Osteoporosis Natl Osteoporosis Foundation USA. (2018) 29:1609–16. doi: 10.1007/s00198-018-4524-7
17. Wiegandt YL, Sigvardsen PE, Sørgaard MH, Knudsen AD, Rerup SA, Kühl JT, et al. The relationship between volumetric thoracic bone mineral density and coronary calcification in men and women - results from the copenhagen general population study. Bone. (2019) 121:116–20. doi: 10.1016/j.bone.2019.01.010
18. Boskey AL. Biomineralization: conflicts, challenges, and opportunities. J Cell Biochem (1998). (72) Suppl 30(31):83–91. doi: 10.1002/(SICI)1097-4644(1998)72:30/31+<83::AID-JCB12>3.0.CO;2-F
19. Thompson B, Towler DA. Arterial calcification and bone physiology: role of the bone-vascular axis. Nat Rev Endocrinol. (2012) 8:529–43. doi: 10.1038/nrendo.2012.36
20. Hutcheson JD, Blaser MC, Aikawa E. Giving calcification its due: recognition of a diverse disease: A first attempt to standardize the field. Circ Res. (2017) 120:270–3. doi: 10.1161/CIRCRESAHA.116.310060
21. Persy V, D’Haese P. Vascular calcification and bone disease: the calcification paradox. Trends Mol Med. (2009) 15:405–16. doi: 10.1016/j.molmed.2009.07.001
22. Tyson KL, Reynolds JL, McNair R, Zhang Q, Weissberg PL, Shanahan CM. Osteo/chondrocytic transcription factors and their target genes exhibit distinct patterns of expression in human arterial calcification. Arteriosclerosis Thrombosis Vasc Biol. (2003) 23:489–94. doi: 10.1161/01.ATV.0000059406.92165.31
23. Bourne LE, Wheeler-Jones CP, Orriss IR. Regulation of mineralisation in bone and vascular tissue: A comparative review. J Endocrinol. (2021) 248:R51–65. doi: 10.1530/JOE-20-0428
24. Marcadet L, Bouredji Z, Argaw A, Frenette J. The roles of rank/rankl/opg in cardiac, skeletal, and smooth muscles in health and disease. Front Cell Dev Biol. (2022) 10:903657. doi: 10.3389/fcell.2022.903657
25. Ono T, Hayashi M, Sasaki F, Nakashima T. Rankl biology: bone metabolism, the immune system, and beyond. Inflammation Regeneration. (2020) 40:2. doi: 10.1186/s41232-019-0111-3
26. Caetano-Lopes J, Canhão H, Fonseca JE. Osteoblasts and bone formation. Acta Reumatologica Portuguesa. (2007) 32:103–10.
27. Demer LL, Tintut Y. Vascular calcification: pathobiology of a multifaceted disease. Circulation. (2008) 117:2938–48. doi: 10.1161/CIRCULATIONAHA.107.743161
28. Bucay N, Sarosi I, Dunstan CR, Morony S, Tarpley J, Capparelli C, et al. Osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev. (1998) 12:1260–8. doi: 10.1101/gad.12.9.1260
29. Panizo S, Cardus A, Encinas M, Parisi E, Valcheva P, López-Ongil S, et al. Rankl increases vascular smooth muscle cell calcification through a rank-bmp4-dependent pathway. Circ Res. (2009) 104:1041–8. doi: 10.1161/CIRCRESAHA.108.189001
30. Jono S, Ikari Y, Shioi A, Mori K, Miki T, Hara K, et al. Serum osteoprotegerin levels are associated with the presence and severity of coronary artery disease. Circulation. (2002) 106:1192–4. doi: 10.1161/01.cir.0000031524.49139.29
31. Kiechl S, Schett G, Wenning G, Redlich K, Oberhollenzer M, Mayr A, et al. Osteoprotegerin is a risk factor for progressive atherosclerosis and cardiovascular disease. Circulation. (2004) 109:2175–80. doi: 10.1161/01.CIR.0000127957.43874.BB
32. Makarović S, Makarović Z, Steiner R, Mihaljević I, Milas-Ahić J. Osteoprotegerin and vascular calcification: clinical and prognostic relevance. Collegium Antropologicum. (2015) 39:461–8.
33. Xie M, Li X, Chen L, Zhang Y, Chen L, Hua H, et al. The crosstalks between vascular endothelial cells, vascular smooth muscle cells, and adventitial fibroblasts in vascular remodeling. Life Sci. (2025) 361:123319. doi: 10.1016/j.lfs.2024.123319
34. Pleskovič A, Šantl Letonja M, Cokan Vujkovac A, Makuc J, Nikolajević Starčević J, Petrovič D. Phosphoprotein 1 (Osteopontin) gene (Rs4754) affects markers of subclinical atherosclerosis in patients with type 2 diabetes mellitus. Int Angiology: A J Int Union Angiology. (2018) 37:64–70. doi: 10.23736/S0392-9590.17.03853-6
35. Boström K, Watson KE, Horn S, Wortham C, Herman IM, Demer LL. Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest. (1993) 91:1800–9. doi: 10.1172/JCI116391
36. Sampath TK, Reddi AH. Dissociative extraction and reconstitution of extracellular matrix components involved in local bone differentiation. Proc Natl Acad Sci United States America. (1981) 78:7599–603. doi: 10.1073/pnas.78.12.7599
37. Wang EA, Rosen V, D’Alessandro JS, Bauduy M, Cordes P, Harada T, et al. Recombinant human bone morphogenetic protein induces bone formation. Proc Natl Acad Sci United States America. (1990) 87:2220–4. doi: 10.1073/pnas.87.6.2220
38. Morrell NW, Bloch DB, ten Dijke P, Goumans M-JTH, Hata A, Smith J, et al. Targeting bmp signalling in cardiovascular disease and anaemia. Nat Rev Cardiol. (2016) 13:106–20. doi: 10.1038/nrcardio.2015.156
39. Ueyama H, Ohta Y, Imai Y, Suzuki A, Sugama R, Minoda Y, et al. Topical co-administration of zoledronate with recombinant human bone morphogenetic protein-2 can induce and maintain bone formation in the bone marrow environment. BMC musculoskeletal Disord. (2021) 22:94. doi: 10.1186/s12891-021-03971-w
40. Huang MS, Morony S, Lu J, Zhang Z, Bezouglaia O, Tseng W, et al. Atherogenic phospholipids attenuate osteogenic signaling by bmp-2 and parathyroid hormone in osteoblasts. J Biol Chem. (2007) 282:21237–43. doi: 10.1074/jbc.M701341200
41. Baron R, Rawadi G. Targeting the wnt/beta-catenin pathway to regulate bone formation in the adult skeleton. Endocrinology. (2007) 148:2635–43. doi: 10.1210/en.2007-0270
42. Mohamad N-V, Ima-Nirwana S, Chin K-Y. Are oxidative stress and inflammation mediators of bone loss due to estrogen deficiency? A review of current evidence. Endocrine Metab Immune Disord Drug Targets. (2020) 20:1478–87. doi: 10.2174/1871530320666200604160614
43. Knowlton AA, Lee AR. Estrogen and the cardiovascular system. Pharmacol Ther. (2012) 135:54–70. doi: 10.1016/j.pharmthera.2012.03.007
44. Mendelsohn ME. Protective effects of estrogen on the cardiovascular system. Am J Cardiol. (2002) 89:12E–7E. doi: 10.1016/s0002-9149(02)02405-0
45. Tankò LB, Bagger YZ, Christiansen C. Low bone mineral density in the hip as a marker of advanced atherosclerosis in elderly women. Calcified Tissue Int. (2003) 73:15–20. doi: 10.1007/s00223-002-2070-x
46. Johnson K, Polewski M, van Etten D, Terkeltaub R. Chondrogenesis mediated by ppi depletion promotes spontaneous aortic calcification in npp1-/- mice. Arteriosclerosis Thrombosis Vasc Biol. (2005) 25:686–91. doi: 10.1161/01.ATV.0000154774.71187.f0
47. Kosmopoulos M, Paschou SA, Grapsa J, Anagnostis P, Vryonidou A, Goulis DG, et al. The emerging role of bone markers in diagnosis and risk stratification of patients with coronary artery disease. Angiology. (2019) 70:690–700. doi: 10.1177/0003319718822625
48. Fedde KN, Blair L, Silverstein J, Coburn SP, Ryan LM, Weinstein RS, et al. Alkaline phosphatase knock-out mice recapitulate the metabolic and skeletal defects of infantile hypophosphatasia. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (1999) 14:2015–26. doi: 10.1359/jbmr.1999.14.12.2015
49. Waymire KG, Mahuren JD, Jaje JM, Guilarte TR, Coburn SP, MacGregor GR. Mice lacking tissue non-specific alkaline phosphatase die from seizures due to defective metabolism of vitamin B-6. Nat Genet. (1995) 11:45–51. doi: 10.1038/ng0995-45
50. Narisawa S, Harmey D, Yadav MC, O’Neill WC, Hoylaerts MF, Millán JL. Novel inhibitors of alkaline phosphatase suppress vascular smooth muscle cell calcification. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (2007) 22:1700–10. doi: 10.1359/jbmr.070714
51. Shioi A, Nishizawa Y, Jono S, Koyama H, Hosoi M, Morii H. Beta-glycerophosphate accelerates calcification in cultured bovine vascular smooth muscle cells. Arteriosclerosis Thrombosis Vasc Biol. (1995) 15:2003–9. doi: 10.1161/01.atv.15.11.2003
52. Montagnana M, Lippi G, Danese E, Guidi GC. The role of osteoprotegerin in cardiovascular disease. Ann Med. (2013) 45:254–64. doi: 10.3109/07853890.2012.727019
53. Soufi M, Schoppet M, Sattler AM, Herzum M, Maisch B, Hofbauer LC, et al. Osteoprotegerin gene polymorphisms in men with coronary artery disease. J Clin Endocrinol Metab. (2004) 89:3764–8. doi: 10.1210/jc.2003-032054
54. Oheim R, Zimmerman K, Maulding ND, Stürznickel J, von Kroge S, Kavanagh D, et al. Human heterozygous enpp1 deficiency is associated with early onset osteoporosis, a phenotype recapitulated in a mouse model of enpp1 deficiency. J Bone Miner Res. (2020) 35:528–39. doi: 10.1002/jbmr.3911
55. Choi SH, An JH, Lim S, Koo BK, Park SE, Chang HJ, et al. Lower bone mineral density is associated with higher coronary calcification and coronary plaque burdens by multidetector row coronary computed tomography in pre- and postmenopausal women. Clin Endocrinol. (2009) 71:644–51. doi: 10.1111/j.1365-2265.2009.03535.x
56. Zhang P, Yang L, Xu Q, Zeng Y, Yu Y, Peng Q, et al. Associations between bone mineral density and coronary artery calcification: A systematic review and meta-analysis. Ther Adv Chronic Dis. (2022) 13:20406223221086998. doi: 10.1177/20406223221086998
57. Aikawa E, Nahrendorf M, Figueiredo J-L, Swirski FK, Shtatland T, Kohler RH, et al. Osteogenesis associates with inflammation in early-stage atherosclerosis evaluated by molecular imaging in vivo. Circulation. (2007) 116:2841–50. doi: 10.1161/CIRCULATIONAHA.107.732867
58. Qin X, Corriere MA, Matrisian LM, Guzman RJ. Matrix metalloproteinase inhibition attenuates aortic calcification. Arteriosclerosis Thrombosis Vasc Biol. (2006) 26:1510–6. doi: 10.1161/01.ATV.0000225807.76419.a7
59. Al-Aly Z, Shao J-S, Lai C-F, Huang E, Cai J, Behrmann A, et al. Aortic msx2-wnt calcification cascade is regulated by tnf-alpha-dependent signals in diabetic ldlr-/- mice. Arteriosclerosis Thrombosis Vasc Biol. (2007) 27:2589–96. doi: 10.1161/ATVBAHA.107.153668
60. Cheng S-L, Shao J-S, Cai J, Sierra OL, Towler DA. Msx2 exerts bone anabolism via canonical wnt signaling. J Biol Chem. (2008) 283:20505–22. doi: 10.1074/jbc.M800851200
61. Rodríguez-Gómez I, Mañas A, Losa-Reyna J, Rodríguez-Mañas L, Chastin SFM, Alegre LM, et al. Associations between sedentary time, physical activity and bone health among older people using compositional data analysis. PloS One. (2018) 13:e0206013. doi: 10.1371/journal.pone.0206013
62. Finck H, Hart AR, Jennings A, Welch AA. Is there a role for vitamin C in preventing osteoporosis and fractures? A review of the potential underlying mechanisms and current epidemiological evidence. Nutr Res Rev. (2014) 27:268–83. doi: 10.1017/S0954422414000195
63. Tarantino U, Cariati I, Greggi C, Gasbarra E, Belluati A, Ciolli L, et al. Skeletal system biology and smoke damage: from basic science to medical clinic. Int J Mol Sci. (2021) 22:6629. doi: 10.3390/ijms22126629
64. Yoon V, Maalouf NM, Sakhaee K. The effects of smoking on bone metabolism. Osteoporosis international: J established as result cooperation between Eur Foundation Osteoporosis Natl Osteoporosis Foundation USA. (2012) 23:2081–92. doi: 10.1007/s00198-012-1940-y
65. Luo S, Qiu XM, Zeng XJ, Zhang DY, Wan B, Li X, et al. Coronary artery calcification and risk of mortality and adverse outcomes in patients with covid-19: A chinese multicenter retrospective cohort study. Chin J Acad Radiol. (2022) 5:20–8. doi: 10.1007/s42058-021-00072-4
66. Aziz MU, Singh S. Computed tomography of coronary artery atherosclerosis: A review. J Med Imaging Radiat Sci. (2021) 52:S19–39. doi: 10.1016/j.jmir.2021.08.007
67. Madhavan MV, Tarigopula M, Mintz GS, Maehara A, Stone GW, Généreux P. Coronary artery calcification: pathogenesis and prognostic implications. J Am Coll Cardiol. (2014) 63:1703–14. doi: 10.1016/j.jacc.2014.01.017
68. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. (1990) 15:827–32. doi: 10.1016/0735-1097(90)90282-t
69. Blaha MJ, Mortensen MB, Kianoush S, Tota-Maharaj R, Cainzos-Achirica M. Coronary artery calcium scoring: is it time for a change in methodology? JACC Cardiovasc Imaging. (2017) 10:923–37. doi: 10.1016/j.jcmg.2017.05.007
70. Goldsborough E, Tasdighi E, Blaha MJ. Assessment of cardiovascular disease risk: A 2023 update. Curr Opin Lipidology. (2023) 34:162–73. doi: 10.1097/MOL.0000000000000887
71. Abuzaid A, Saad M, Addoumieh A, Ha LD, Elbadawi A, Mahmoud AN, et al. Coronary artery calcium score and risk of cardiovascular events without established coronary artery disease: A systemic review and meta-analysis. Coronary Artery Dis. (2021) 32:317–28. doi: 10.1097/MCA.0000000000000974
72. Orimoloye OA, Budoff MJ, Dardari ZA, Mirbolouk M, Uddin SMI, Berman DS, et al. Race/ethnicity and the prognostic implications of coronary artery calcium for all-cause and cardiovascular disease mortality: the coronary artery calcium consortium. J Am Heart Assoc. (2018) 7:e010471. doi: 10.1161/JAHA.118.010471
73. Agarwal S, Cox AJ, Herrington DM, Jorgensen NW, Xu J, Freedman BI, et al. Coronary calcium score predicts cardiovascular mortality in diabetes: diabetes heart study. Diabetes Care. (2013) 36:972–7. doi: 10.2337/dc12-1548
74. Chuang T-L, Chuang M-H, Koo M, Lin C-H, Wang Y-F. Association of bone mineral density and trabecular bone score with cardiovascular disease. Ci Ji Yi Xue Za Zhi = Tzu-Chi Med J. (2020) 32:234–9. doi: 10.4103/tcmj.tcmj_234_19
75. Yesil Y, Ulger Z, Halil M, Halaçli B, Yavuz BB, Yeşil NK, et al. Coexistence of osteoporosis (Op) and coronary artery disease (Cad) in the elderly: it is not just a by chance event. Arch Gerontology Geriatrics. (2012) 54:473–6. doi: 10.1016/j.archger.2011.06.007
76. Sheppard JP, Lakshmanan S, Lichtenstein SJ, Budoff MJ, Roy SK. Age and the power of zero cac in cardiac risk assessment: overview of the literature and a cautionary case. Br J Cardiol. (2022) 29:23. doi: 10.5837/bjc.2022.023
77. Motoyama S, Kondo T, Sarai M, Sugiura A, Harigaya H, Sato T, et al. Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol. (2007) 50:319–26. doi: 10.1016/j.jacc.2007.03.044
78. Mori H, Torii S, Kutyna M, Sakamoto A, Finn AV, Virmani R. Coronary Artery Calcification And its progression: What Does It Really Mean? JACC Cardiovasc Imaging. (2018) 11:127–42. doi: 10.1016/j.jcmg.2017.10.012
79. Puchner SB, Liu T, Mayrhofer T, Truong QA, Lee H, Fleg JL, et al. High-risk plaque detected on coronary ct angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: results from the romicat-ii trial. J Am Coll Cardiol. (2014) 64:684–92. doi: 10.1016/j.jacc.2014.05.039
80. Osawa K, Nakanishi R, McClelland RL, Polak JF, Bishop W, Sacco RL, et al. Ischemic stroke/transient ischemic attack events and carotid artery disease in the absence of or with minimal coronary artery calcification: results from the multi-ethnic study of atherosclerosis. Atherosclerosis. (2018) 275:22–7. doi: 10.1016/j.atherosclerosis.2018.05.027
81. Alexopoulos N, Raggi P. Calcification in atherosclerosis. Nat Rev Cardiol. (2009) 6:681–8. doi: 10.1038/nrcardio.2009.165
82. Asadi M, Razi F, Fahimfar N, Shirani S, Behzad G, Salari P. The association of coronary artery calcium score and osteoporosis in postmenopausal women: A cross-sectional study. J Bone Metab. (2022) 29:245–54. doi: 10.11005/jbm.2022.29.4.245
83. Cheneymann A, Therkildsen J, Winther S, Nissen L, Thygesen J, Langdahl BL, et al. Bone mineral density derived from cardiac ct scans: using contrast enhanced scans for opportunistic screening. J Clin densitometry: Off J Int Soc Clin Densitometry. (2024) 27:101441. doi: 10.1016/j.jocd.2023.101441
84. Chen W, Mao M, Fang J, Xie Y, Rui Y. Fracture risk assessment in diabetes mellitus. Front Endocrinol. (2022) 13:961761. doi: 10.3389/fendo.2022.961761
85. Genant HK, Block JE, Steiger P, Glueer CC, Smith R. Quantitative computed tomography in assessment of osteoporosis. Semin Nucl Med. (1987) 17:316–33. doi: 10.1016/s0001-2998(87)80024-7
86. Lenchik L, Weaver AA, Ward RJ, Boone JM, Boutin RD. Opportunistic screening for osteoporosis using computed tomography: state of the art and argument for paradigm shift. Curr Rheumatol Rep. (2018) 20:74. doi: 10.1007/s11926-018-0784-7
87. Genant HK, Ettinger B, Cann CE, Reiser U, Gordan GS, Kolb FO. Osteoporosis: assessment by quantitative computed tomography. Orthopedic Clinics North America. (1985) 16:557–68. doi: 10.1016/S0030-5898(20)30459-4
88. Li X, Li X, Li J, Jiao X, Jia X, Zhang X, et al. The accuracy of bone mineral density measurement using dual-energy spectral ct and quantitative ct: A comparative phantom study. Clin Radiol. (2020) 75:320.e9–.e15. doi: 10.1016/j.crad.2019.11.008
89. Guerri S, Mercatelli D, Aparisi Gómez MP, Napoli A, Battista G, Guglielmi G, et al. Quantitative imaging techniques for the assessment of osteoporosis and sarcopenia. Quantitative Imaging Med Surg. (2018) 8:60–85. doi: 10.21037/qims.2018.01.05
90. Brett AD, Brown JK. Quantitative computed tomography and opportunistic bone density screening by dual use of computed tomography scans. J Orthopaedic Translation. (2015) 3:178–84. doi: 10.1016/j.jot.2015.08.006
91. Engelke K. Quantitative computed tomography-current status and new developments. J Clin Densitometry: Off J Int Soc Clin Densitometry. (2017) 20:309–21. doi: 10.1016/j.jocd.2017.06.017
92. Manske SL, Zhu Y, Sandino C, Boyd SK. Human trabecular bone microarchitecture can be assessed independently of density with second generation hr-pqct. Bone. (2015) 79:213–21. doi: 10.1016/j.bone.2015.06.006
93. Folkestad L, Hald JD, Hansen S, Gram J, Langdahl B, Abrahamsen B, et al. Bone geometry, density, and microarchitecture in the distal radius and tibia in adults with osteogenesis imperfecta type I assessed by high-resolution pqct. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (2012) 27:1405–12. doi: 10.1002/jbmr.1592
94. Liu XS, Zhang XH, Sekhon KK, Adams MF, McMahon DJ, Bilezikian JP, et al. High-resolution peripheral quantitative computed tomography can assess microstructural and mechanical properties of human distal tibial bone. J Bone Mineral Research: Off J Am Soc Bone Mineral Res. (2010) 25:746–56. doi: 10.1359/jbmr.090822
95. Lee DC, Hoffmann PF, Kopperdahl DL, Keaveny TM. Phantomless calibration of ct scans for measurement of bmd and bone strength-inter-operator reanalysis precision. Bone. (2017) 103:325–33. doi: 10.1016/j.bone.2017.07.029
96. Therkildsen J, Thygesen J, Winther S, Svensson M, Hauge E-M, Böttcher M, et al. Vertebral bone mineral density measured by quantitative computed tomography with and without a calibration phantom: A comparison between 2 different software solutions. J Clin densitometry: Off J Int Soc Clin Densitometry. (2018) 21:367–74. doi: 10.1016/j.jocd.2017.12.003
97. Lee SJ, Binkley N, Lubner MG, Bruce RJ, Ziemlewicz TJ, Pickhardt PJ. Opportunistic screening for osteoporosis using the sagittal reconstruction from routine abdominal ct for combined assessment of vertebral fractures and density. Osteoporosis international: J established as result cooperation between Eur Foundation Osteoporosis Natl Osteoporosis Foundation USA. (2016) 27:1131–6. doi: 10.1007/s00198-015-3318-4
98. Pickhardt PJ, Pooler BD, Lauder T, del Rio AM, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Internal Med. (2013) 158:588–95. doi: 10.7326/0003-4819-158-8-201304160-00003
99. Therkildsen J, Nissen L, Jørgensen HS, Thygesen J, Ivarsen P, Frost L, et al. Thoracic bone mineral density derived from cardiac ct is associated with greater fracture rate. Radiology. (2020) 296:499–508. doi: 10.1148/radiol.2020192706
100. Zhou F, Yan D, Wang L, Geng J, Zhang W, Liu Y, et al. Application value of lumbar spine volume CT value in the diagnosis of osteoporosis. Chin J Osteoporosis. (2023) 29:1272–7.
101. Liu W, Lu Z, Wang D, Zhu H, Song L, Cao X. Correlation between CT value of thoracic vertebrae cancellous bone andcoronary artery calcification in type 2 diabetes mellitus patients. J Jiangsu Univ (Med Edition). (2023) 33:152–5, 161. doi: 10.13312/j.issn.1671-7783.y230030
102. Nakama C, Kadowaki T, Choo J, El-Saed A, Kadota A, Willcox BJ, et al. Cross-sectional association of bone mineral density with coronary artery calcification in an international multi-ethnic population-based cohort of men aged 40-49: era jump study. Int J Cardiol Heart Vasculature. (2020) 30:100618. doi: 10.1016/j.ijcha.2020.100618
103. Glüer CC, Reiser UJ, Davis CA, Rutt BK, Genant HK. Vertebral mineral determination by quantitative computed tomography (Qct): accuracy of single and dual energy measurements. J Comput Assisted Tomography. (1988) 12:242–58. doi: 10.1097/00004728-198803000-00013
104. Vetter JR, Perman WH, Kalender WA, Mazess RB, Holden JE. Evaluation of a prototype dual-energy computed tomographic apparatus. Ii. Determination Vertebral Bone Mineral Content. Med Phys. (1986) 13:340–3. doi: 10.1118/1.595951
105. Johnson TRC, Krauss B, Sedlmair M, Grasruck M, Bruder H, Morhard D, et al. Material differentiation by dual energy ct: initial experience. Eur Radiol. (2007) 17:1510–7. doi: 10.1007/s00330-006-0517-6
106. Ren Q, Tang D, Xiong Z, Zhao H, Zhang S. Traumatic bone marrow lesions in dual-energy computed tomography. Insights into Imaging. (2022) 13:174. doi: 10.1186/s13244-022-01312-6
107. Goodsitt MM, Hoover P, Veldee MS, Hsueh SL. The composition of bone marrow for a dual-energy quantitative computed tomography technique. Comput Simulation Study. Invest Radiol. (1994) 29:695–704. doi: 10.1097/00004424-199407000-00006
108. Wesarg S, Kirschner M, Becker M, Erdt M, Kafchitsas K, Khan MF. Dual-energy ct-based assessment of the trabecular bone in vertebrae. Methods Inf Med. (2012) 51:398–405. doi: 10.3414/ME11-02-0034
109. Wang X, Li B, Tong X, Fan Y, Wang S, Liu Y, et al. Diagnostic accuracy of dual-energy ct material decomposition technique for assessing bone status compared with quantitative computed tomography. Diagnostics (Basel Switzerland). (2023) 13:1751. doi: 10.3390/diagnostics13101751
110. Zhou S, Zhu L, You T, Li P, Shen H, He Y, et al. In vivo quantification of bone mineral density of lumbar vertebrae using fast kvp switching dual-energy ct: correlation with quantitative computed tomography. Quantitative Imaging Med Surg. (2021) 11:341–50. doi: 10.21037/qims-20-367
111. Bagger YZ, Rasmussen HB, Alexandersen P, Werge T, Christiansen C, Tankó LB, et al. Links between cardiovascular disease and osteoporosis in postmenopausal women: serum lipids or atherosclerosis per se? Osteoporosis international: J established as result cooperation between Eur Foundation Osteoporosis Natl Osteoporosis Foundation USA. (2007) 18:505–12. doi: 10.1007/s00198-006-0255-2
Keywords: computed tomography, coronary artery calcification, osteoporosis, bone-vascular axis, “one-stop-shop” analysis
Citation: Luo J, Wang Q, Liu W, Liao H, Qing W, Zhang M, Tang D, Luo G and Zhao H (2025) Computed tomography provides a “one-stop-shop” targeted analysis for coronary artery calcification and osteoporosis: a review. Front. Endocrinol. 16:1356831. doi: 10.3389/fendo.2025.1356831
Received: 01 February 2024; Accepted: 05 February 2025;
Published: 28 February 2025.
Edited by:
Ting Zheng, Hospital for Special Surgery, United StatesReviewed by:
Hengyi Xu, The University of Texas at Austin, United StatesCopyright © 2025 Luo, Wang, Liu, Liao, Qing, Zhang, Tang, Luo and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heng Zhao, YW5nZXJoOUAxMjYuY29t; Guanghua Luo, bHVvZ3VhbmdodWFkZWFyQDEyNi5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.