 Ling Guo
Ling Guo Xiao Li1†
Xiao Li1† Yufeng Wang
Yufeng Wang Yan Li
Yan Li Hong Lv
Hong Lv- 1Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, Shandong, China
- 2Medical Integration and Practice Center, Shandong University, Jinan, Shandong, China
- 3State Key Laboratory of Reproductive Medicine and Offspring Health, Center for Reproductive Medicine, Institute of Women, Children and Reproductive Health, Shandong University, Jinan, Shandong, China
- 4Department of Otolaryngology, Qilu Hospital of Shandong University, Jinan, Shandong, China
The safety and clinical effectiveness of preimplantation genetic testing for aneuploidy (PGT-A) in improving pregnancy outcomes for sub-fertile patients remains controversial. Potential sex-based differences in the relationship between PGT-A and pregnancy complications have not been investigated, which could guide the appropriate clinical application of PGT-A. In this secondary analysis of data from a multicenter, randomized, controlled, non-inferiority trial (NCT03118141), 940 women who achieved singleton live birth during the trial were included to estimate the between-group differences in pregnancy complications following PGT-A versus conventional in vitro fertilization (IVF) vary with fetal sex. Logistic regression analysis was used to adjust for possible confounders, and subgroup analysis was also performed. Among male fetuses, the risk of maternal preeclampsia was significantly lower after PGT-A compared to conventional IVF treatment (3.37% vs. 7.88%; adjusted OR, 0.40; 95% CI, 0.17-0.92; P = 0.032). However, this protective effect was not observed in pregnancies with female fetuses (3.63% vs. 3.38%; adjusted OR, 1.04; 95% CI, 0.36-3.00; P = 0.937). In addition, no significant sex-dependent differences in the risks of other pregnancy complications or neonatal outcomes were detected between PGT-A and conventional IVF groups (P > 0.05). In summary, PGT-A was associated with a decreased risk of maternal preeclampsia in singleton pregnancies with male fetuses, highlighting its potential utility in preeclampsia prevention in addition to spontaneous abortion rate reduction.
Introduction
Preimplantation genetic testing for aneuploidy (PGT-A), a derivative technology of in vitro fertilization and embryo transfer (IVF-ET), has become increasingly utilized to improve outcomes in the field of assisted reproduction (1). The goal of PGT-A is to identify euploid embryos that are suitable for transfer, thereby increasing the live birth rates and reducing the risk of adverse pregnancy outcomes, such as spontaneous abortion (2). Some studies have shown that PGT-A can significantly improve pregnancy outcomes compared to conventional IVF, especially in women of advanced maternal age (3, 4). However, our recent randomized controlled study indicates that despite a perceived reduction in the frequency of pregnancy loss among clinical pregnancies for the PGT-A group, it does not positively affect cumulative live birth rates following embryo transfer in patients with a good prognosis, nor does it impact other obstetric pregnancy or neonatal outcomes (5). This provokes debates regarding whether the purported clinical effectiveness and benefits of PGT-A justify the risks intrinsic to the testing process. Despite controversy surrounding the invasiveness of this procedure for transferred embryos, PGT-A is currently utilized in approximately half of all IVF cycles in the USA, with its application steadily increasing worldwide (6). Thus, evidence regarding the effectiveness and safety of PGT-A is urgently needed for guiding the correct indications and optimal utilization.
Preeclampsia, a common pregnancy complication characterized by de novo development of high blood pressure (≥140/90 mm Hg) concurrent with proteinuria (≥300 mg/L per 24 hours) after 20 weeks of gestation, remains a leading cause of maternal and perinatal mortality and morbidity worldwide (7) and is associated with a substantial long-term risk for cardiovascular disease (8). One previous report showed a higher risk of preeclampsia associated with frozen single blastocyst transfer compared to fresh single blastocyst transfer (9). It is now broadly accepted that placental dysfunction, originating from the trophectoderm of the embryo, contributes to preeclampsia pathogenesis (7). Given that PGT-A necessitates biopsy of embryonic trophectoderm cells for genetic examination, it could provide valuable insights into preventing diseases related to embryonic trophectoderm abnormalities, such as preeclampsia. However, the accuracy and reliability of PGT-A results should be carefully validated due to potential confounding factors.
Furthermore, emerging evidence indicates that selecting euploid embryos via PGT-A may be misleading, as the genetic features of the trophectoderm do not fully represent the chromosomal status of the inner cell mass, which eventually develops into the fetus. Given the self-correction ability of aneuploid cells in the embryo and the presence of mosaic cells in the placenta of healthy pregnancies, as revealed in recent studies (6, 10, 11), PGT-A could potentially produce high false-positive rates for aneuploidy, resulting in a waste of transferrable embryos. Moreover, an increasing number of studies highlight that placenta formation and function during pregnancy are sex-dependent, and that male fetuses carry a higher risk of pregnancy complications, including gestational diabetes, gestational hypertension, preeclampsia, and eclampsia (12–14). However, studies investigating the effects of PGT-A on pregnancy complications, particularly those related to placental dysfunction, have generally disregarded differences in fetal sex (15).
Our group conducted a multicenter, randomized, controlled, non-inferiority trial and observed no improvement in the cumulative live birth rate by PGT-A compared to IVF in women with a good prognosis (5). In this study, we further performed a post hoc exploratory secondary analysis among women who achieved a singleton live birth during this trial and assessed the differences in pregnancy complications between male and female fetuses in PGT-A versus conventional IVF.
Materials and methods
Design and participants
The original multicenter, randomized, controlled clinical trial (registration number: NCT03118141) was conducted sequentially from July 2017 through June 2018, and the primary outcomes and protocols of the trial are published (5). Briefly, 1212 women who planned to undergo their first IVF cycle with a good prognosis for live birth were enrolled. A good prognosis was defined by patient age of 20 to 37 years and the availability of three or more high-quality blastocysts. All participants were randomized and then assigned to either the PGT-A group or the conventional IVF group (each group included 606 women). In the present analyses, the subjects without a live birth or with a multiple pregnancy were excluded, resulting in a total cohort of 940 women who achieved singleton live birth for further evaluation (Figure 1).
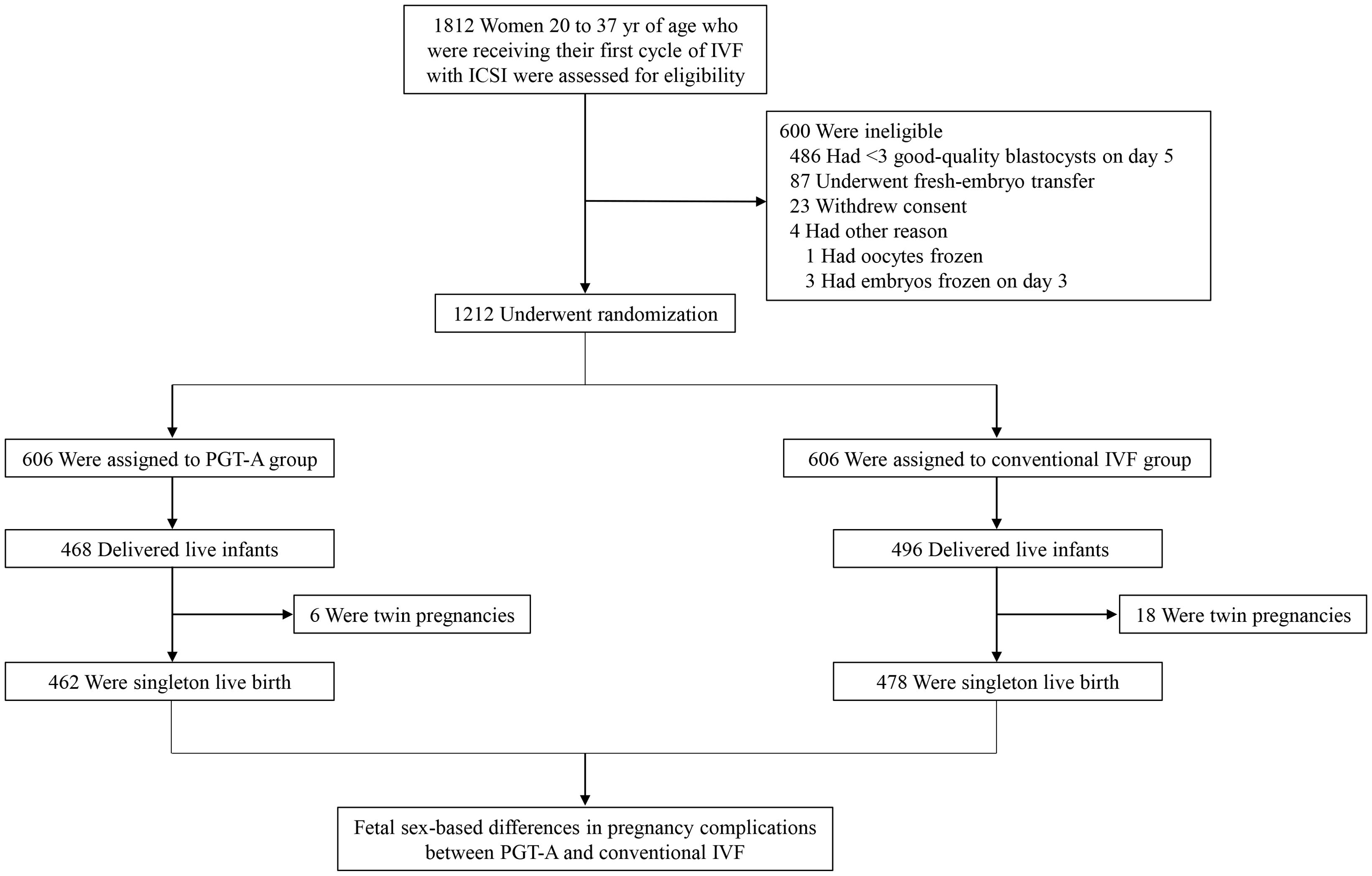
Figure 1. Flow chart of participants screening and enrollment. IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; PGT-A, preimplantation genetic testing for aneuploidy.
Study procedure
Ovarian stimulation was performed through long or short regimens of gonadotropin-releasing hormone (GnRH) agonist or with a GnRH antagonist. The detailed schedule for controlled ovarian hyperstimulation has been previously described (5, 16). Human chorionic gonadotropin (hCG), GnRH agonist, or both were administered to trigger oocyte maturation when at least two follicles were ≥18 mm. All oocytes were inseminated by intracytoplasmic sperm injection (ICSI), and viable embryos were cultured to the blastocyst stage. According to the trial design, three high-quality blastocysts selected by means of morphological criteria (17) in the PGT-A group underwent trophectoderm biopsy. In each cycle, a euploid blastocyst in the PGT-A group or a high-quality blastocyst in the conventional IVF group was chosen for transfer. Endometrial preparation before frozen embryo transfer was performed with either a natural ovulation cycle, an artificial regimen, or an ovulation induction cycle. Luteal-phase support was administered in both groups. These techniques have been previously described in detail (16, 18). In this trial, up to three blastocyst-stage embryos were transferred either in the PGT-A group or conventional IVF group within 1 year after randomization until live birth or pregnancy termination. All pregnancy and neonatal outcomes were recorded in detail. Only singleton live births were included in the present study.
Study outcomes
The primary outcomes were pregnancy complications, principally including the incidence of preeclampsia in subjects with singleton live births following PGT-A or conventional IVF. Secondary outcomes were neonatal outcomes, mainly including mean birth weight, as well as the incidence of small for gestational age (SGA) and large for gestational age (LGA) of singleton fetuses. The parameters of controlled ovarian hyperstimulation and other pregnancy complications were also analyzed. Preeclampsia was defined as hypertension appearing after 20 weeks of gestation with proteinuria (≥ 0.3 mg urinary protein per 24 h) (19, 20). SGA and LGA were defined as smaller than the 10th percentile or larger than the 90th percentile of birth weight at the corresponding gestational week, respectively, with consideration of fetal sex (21).
Statistical analysis
Statistical analyses were performed using SPSS 26.0 for Windows (IBM, Armonk, NY, USA). The Kolmogorov–Smirnov test, in conjunction with histogram and Q-Q plot, was used to test for normality in the distribution of data. Continuous variables with normal distributions are presented as the mean ± standard deviation (SD) and were analyzed by independent t test. The median with interquartile range is used to show data with a non-normal distribution and compared by the Mann–Whitney U test. Categorical variables are presented as counts (percentages) and were compared using either the chi-square or Fisher’s exact test. Multivariable logistic regression analysis was performed to adjust for baseline characteristics. Multivariable linear regression or logistic regression analysis was used to investigate potential associations between PGT-A and pregnancy complications, adjusting for maternal age, body mass index (BMI), serum anti-Müllerian hormone (AMH) level, number of oocytes retrieved, number of high-quality embryos on day 5 or 6, endometrial thickness before embryo transfer, PGT-A vs. conventional IVF, fetal sex, and interaction between PGT-A vs. conventional IVF and fetal sex. Values of P < 0.05 were considered statistically significant.
Results
Baseline characteristics
This study included a total of 940 women who achieved singleton live birth after PGT-A or conventional IVF during the trial. Among them, 462 women were randomly assigned to the PGT-A group, and 478 women were assigned to the conventional IVF group. As shown in Table 1, there were no significant differences in baseline characteristics between the two groups (P > 0.05), including maternal age, BMI, duration of infertility, type of infertility, indications for IVF, antral follicle count, serum thyroid stimulating hormone (TSH), AMH, follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol, progesterone, testosterone and prolactin levels. Additionally, the results indicated that the proportion of male fetuses in the PGT-A group was slightly higher than in the conventional IVF group. This difference may be due to the limitations of sample size or could suggest that PGT-A may have some influence on sex ratios, warranting further investigation.
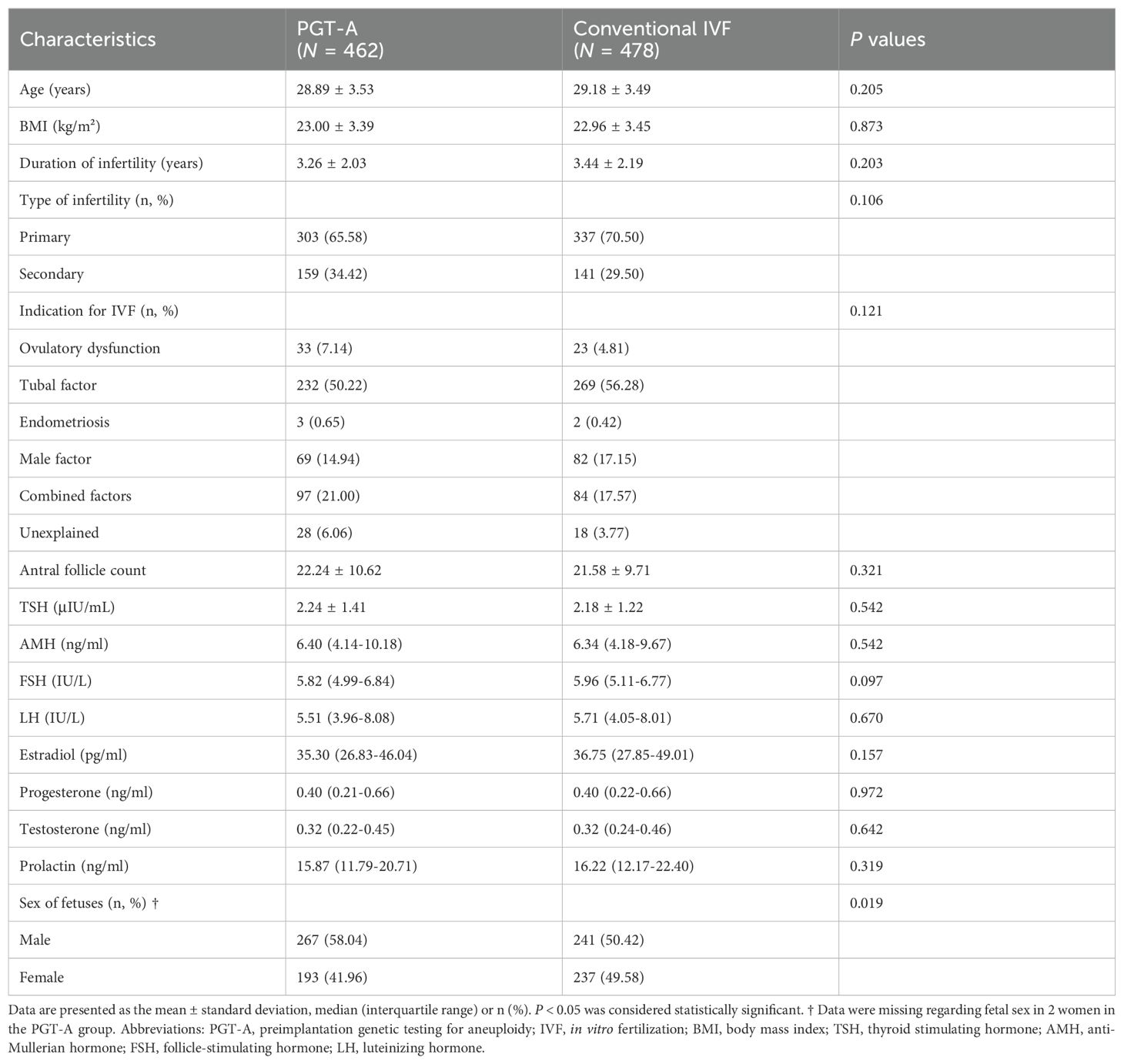
Table 1. Baseline characteristics of the participants who achieved singleton live birth after PGT-A vs. conventional IVF.
Ovarian response and embryo quality
The outcomes of controlled ovarian hyperstimulation in the two groups are compared in Table 2. No significant differences were observed in the duration of ovarian stimulation, gonadotropin dose, serum estradiol, LH and progesterone levels on the hCG trigger day, endometrial thickness on the hCG trigger day, number of oocytes with diameters ≥ 14 mm and ≥ 18 mm on the hCG trigger day, number of retrieved, metaphase II (MII), and two pronuclei (2PN) oocytes, number of high-quality embryos on day 3 and number of high-quality embryos on day 5 or 6 (P > 0.05). This indicates that ovarian response and embryo quality were equivalent between the two groups.
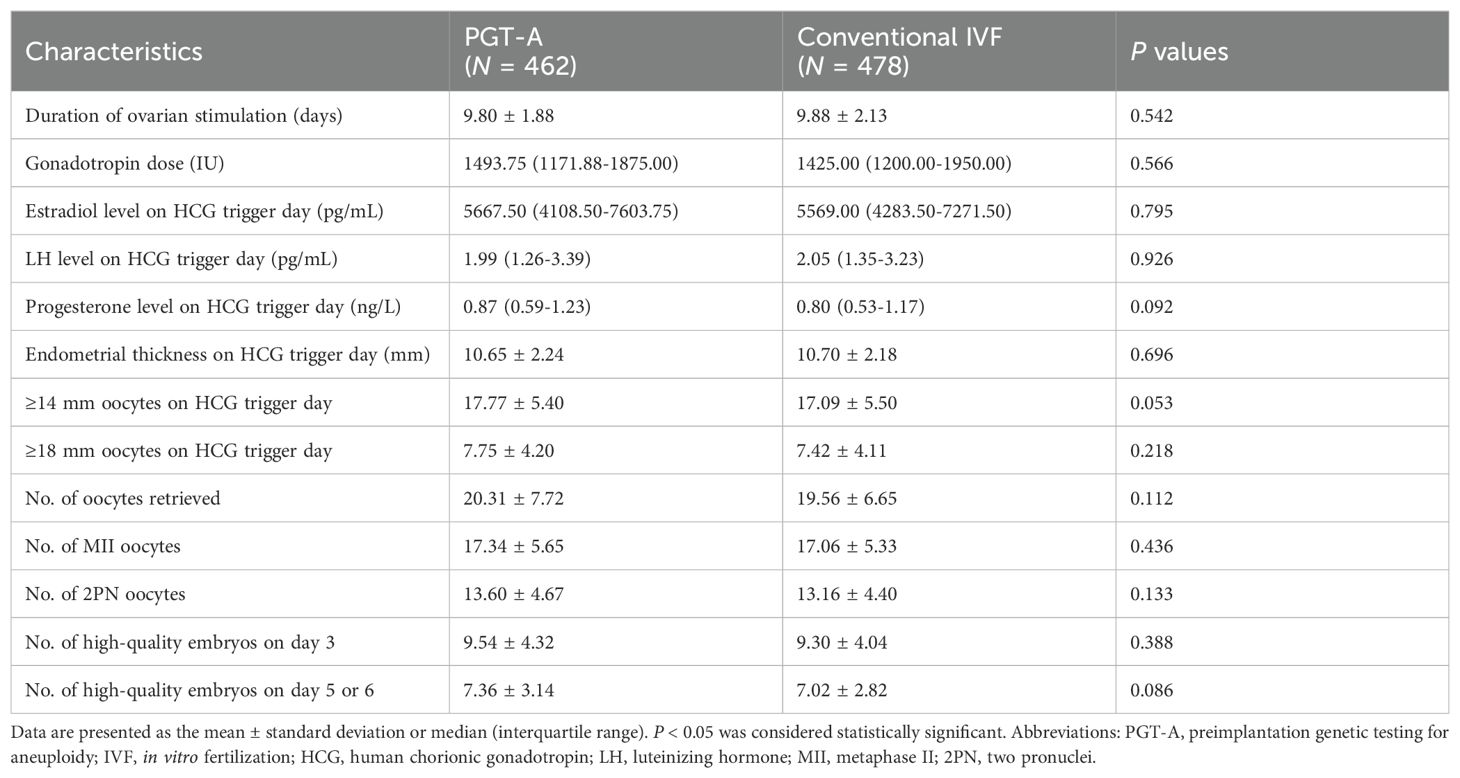
Table 2. Comparison of COH outcomes of singleton pregnancy after PGT-A vs. conventional IVF.
Pregnancy complications
Multivariable regression analyses showed no significant differences (P > 0.05) in the interaction between fetal sex and PGT-A vs. conventional IVF regarding risks of pregnancy complications, including gestational age at delivery, incidence of cesarean section, pre-term delivery, gestational diabetes, gestational hypertension, preeclampsia, placenta previa, or pre-term rupture of the membrane (Table 3). However, subgroup analysis based on fetal sex demonstrated a significantly lower risk of preeclampsia following PGT-A compared to conventional IVF in male fetuses (3.37% vs. 7.88%; adjusted OR, 0.40; 95% CI, 0.17-0.92; P = 0.032) (Figure 2A and Supplementary Tables 1, 2). This protective effect was not observed in pregnancies with female fetuses (3.63% vs. 3.38%; adjusted OR, 1.04; 95% CI, 0.36-3.00; P = 0.937) (Figure 2B, Supplementary Table 3), suggesting that the impacts of PGT-A on preeclampsia incidence is dependent on fetal sex.
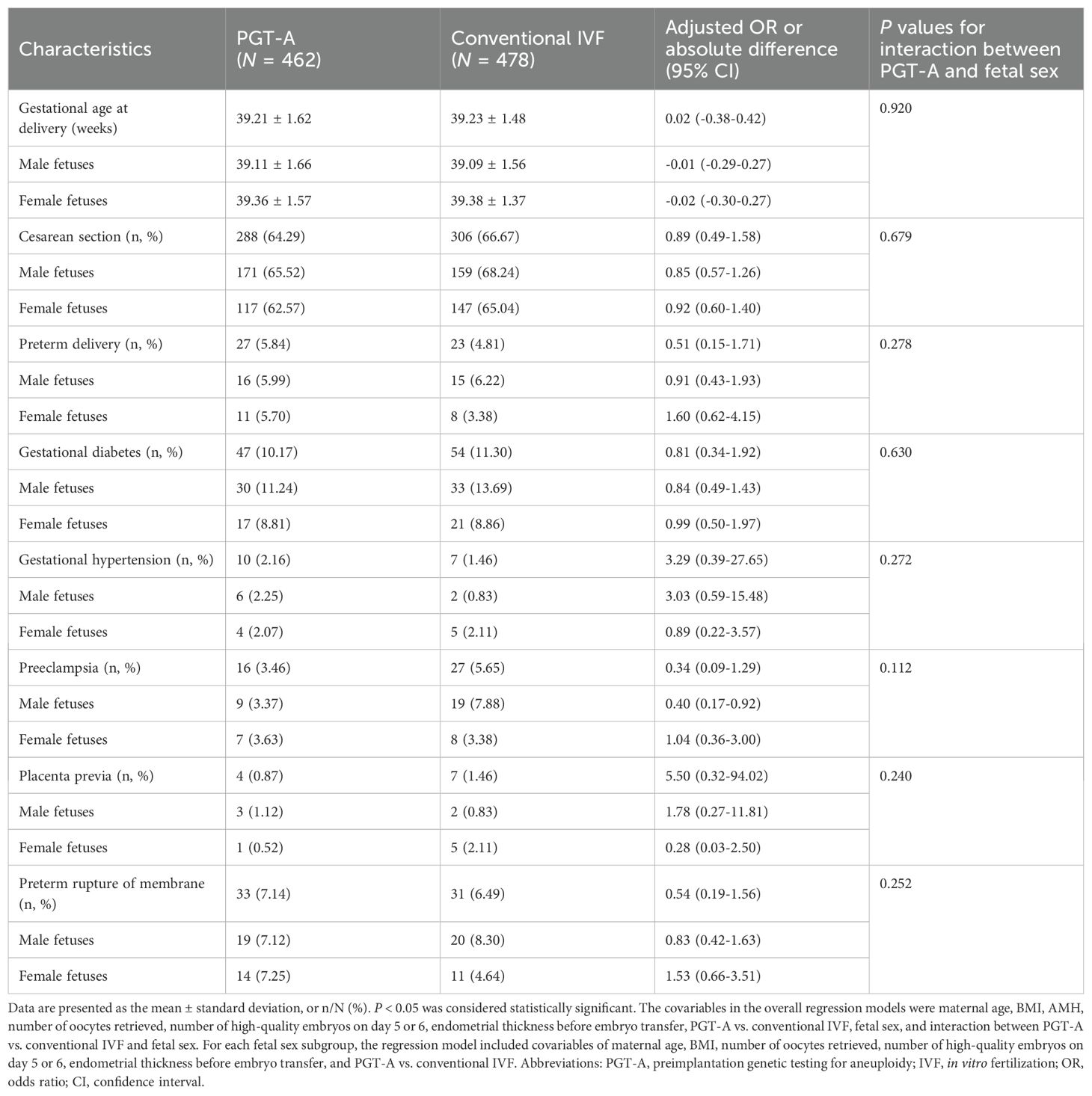
Table 3. Comparison of pregnancy complications of singleton pregnancy after PGT-A vs. conventional IVF.
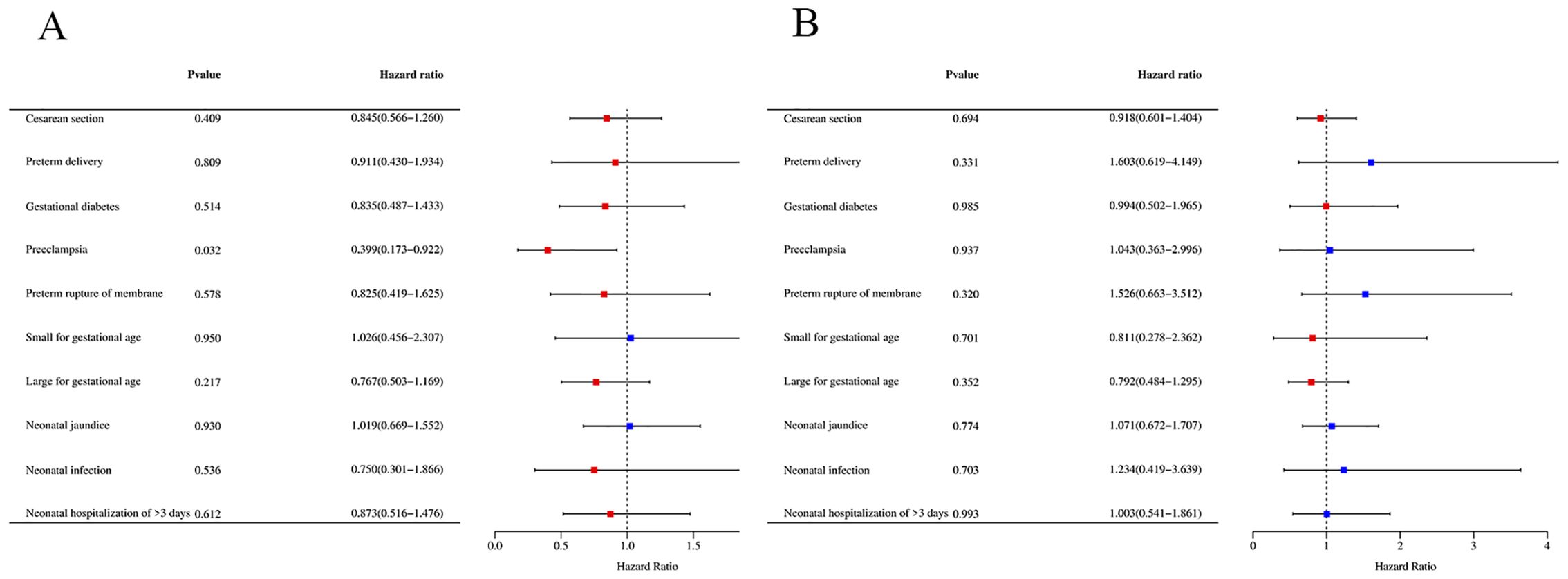
Figure 2. The risk of pregnancy complications based on fetal sex. (A) The risk of pregnancy complications in male fetuses. (B) The risk of pregnancy complications in female fetuses. OR > 1 indicates a risk factor, and OR < 1 indicates a protective factor.
Neonatal outcomes
As shown in Table 4, no significant differences were found in neonatal outcomes attributable to the interaction between fetal sex and PGT-A vs. conventional IVF (P > 0.05), including mean birth weight, incidence of SGA, LGA, neonatal respiratory distress syndrome (RDS), neonatal jaundice, neonatal infection and neonatal hospitalization of >3 days. For each fetal sex subgroup analysis, no significant difference in neonatal outcomes was detected between the PGT-A group and the conventional IVF group.
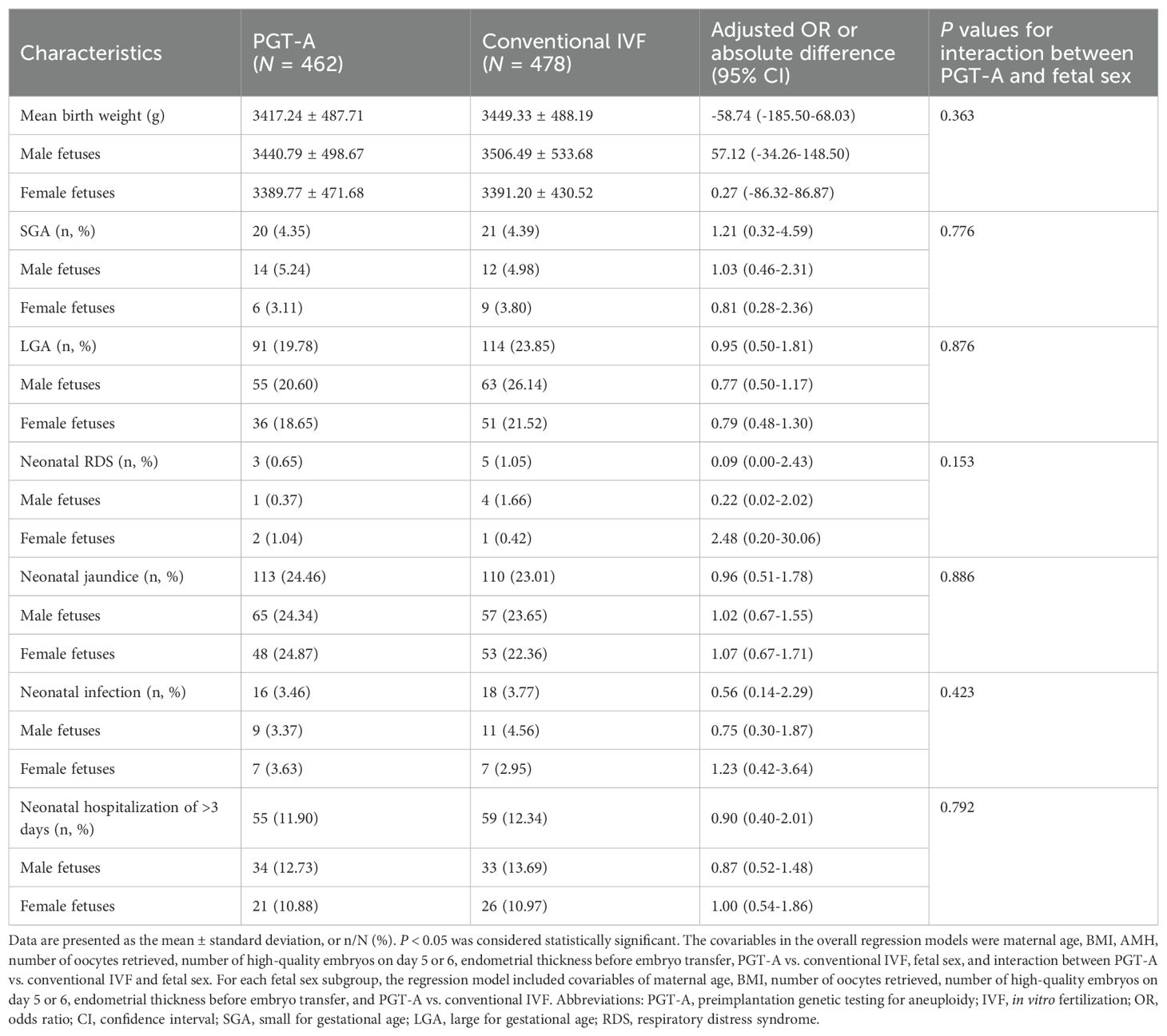
Table 4. Comparison of neonatal outcomes and birth weight of singleton pregnancy after PGT-A vs. conventional IVF.
Discussion
To our knowledge, no previous studies have examined the potential relationships between PGT-A and fetal sex in relation to the risk of pregnancy complications. In this post hoc exploratory secondary analysis of data from a multicenter randomized controlled trial, we provided evidence that PGT-A treatment may decrease the risk of preeclampsia in women carrying singleton male fetuses compared with those pregnant women who underwent conventional IVF treatment. Notably, this potential benefit of PGT-A treatment was not observed in mothers who delivered female fetuses. In addition, no obvious relationship between PGT-A and fetal sex in other pregnancy complications or neonatal outcomes, such as the mean birth weight, SGA, or LGA, was observed.
Given the unavoidable invasive nature of embryo biopsy during PGT-A, the choice of embryonic stage for biopsyis usually with cautious to minimize potential adverse impacts on embryo development. Current methods of PGT-A involve polar body biopsy (22), cleavage-stage biopsy (23), and blastocyst-stage biopsy (24). Among these, blastocyst-stage biopsy is most common due to its improved genetic testing accuracy and lesser impact on the inner cell mass. As the prevalence recognition of mosaic embryos which refer to the embryos possess two or more genetically different sets of cells, it has been realized that the biopsy and test of 5-10 trophectoderm cells cannot accurately reflect aneuploidy throughout the embryo and for the inner cell mass, let alone predicting pregnancy outcomes after embryo transfer (11, 25). Several studies have found that PGT-A can improve rates of clinical (3) and ongoing pregnancies (26), as well as effectively reduce the occurrence of adverse pregnancy outcomes such as pre-term birth and low birth weight (27). However, more recent randomized controlled studies have suggested that PGT-A does not improve ongoing pregnancy or live birth rates after frozen embryo transfer compared with conventional IVF treatment (28, 29). Our original randomized controlled trial also found that PGT-A does not improve the cumulative live birth rates after embryo transfer in patients with a good prognosis, except for the rate of first-trimester pregnancy loss, nor does it affect other pregnancy complications or neonatal outcomes (5). These inconsistent findings might be partially attributed to the self-correction ability of aneuploidy cells and the recognition of mosaic embryos as a normal stage in embryo development (30, 31).
While PGT-A may not accurately depict the chromosomal status of the inner cell mass, it could still theoretically aid in the prevention of diseases related to placental development, considering its ability to identify aneuploidy in the trophectoderm, which forms the placenta. Studies have demonstrated the presence of aneuploid cells in placentas of otherwise chromosomally normal pregnancies (32). It has been established that the placenta serves as a repository for unrepaired aneuploid cells, which can rectify embryonic endoderm aneuploidy, protect the fetus from aneuploidy, and promote implantation (10, 31). Notably, sex-based differences in disease risk, pathophysiology, clinical manifestations, and responses to clinical interventions have gained significant research attention recently (33). It has been indicated that the formation and function of the placenta are sex-dependent, with male fetuses having smaller placentas than female fetuses, suggesting an increased risk of adverse pregnancy events for male fetuses (12–14, 34). Recent studies suggests that the underlying mechanism of this observed phenomenon may be that the female placenta is more sensitive to abnormal intrauterine stress signals. This sensitivity could confer adaptive benefits through the inactivation of one X chromosome during preimplantation (35).
Abnormalities in the embryonic trophectoderm are known to be associated with the occurrence of pregnancy complications such as preeclampsia, which arises from impaired placental development (7). Given that the PGT-A during the trophectoderm development stage could potentially eliminate aneuploid cells that are resistant to self-correction later on, we hypothesize PGT-A could provide protective benefits against placental dysfunction-related pregnancy complications such as preeclampsia. Based on a secondary analysis of a large randomized controlled trial, our study provides evidence supporting the notion that PGT-A reduces the risk of maternal preeclampsia in singleton pregnancies carrying male fetuses compared to conventional IVF. It is important to note the differences in fetal sex between the PGT-A and conventional IVF groups, as these differences could influence the observed outcomes. While our findings suggest a potential protective effect of PGT-A, the mechanisms remain unclear, possibly relating to the timing or self-correction of mosaic cells in male versus female fetuses.
Ethical considerations surrounding sex selection in reproductive technologies, especially PGT-A, must be carefully examined. Choosing embryos based on sex can raise significant concerns about societal preferences for male or female offspring, potentially exacerbating gender imbalances. Additionally, while IVF is associated with an increased risk of preeclampsia, factors such as maternal age, underlying health conditions, and multiple gestations also play crucial roles (36). Currently, the proportion of male births during normal pregnancies in our country is relatively high (37), which may further influence these ethical dynamics, including the complex interplay of societal norms, reproductive choices, and potential long-term effects on gender ratios within the population. Further research is essential to disentangle these variables and comprehend the broader implications of our findings.
This study has several strengths, including the use of data from a prospective multicenter randomized controlled trial, which greatly minimizes potential bias compared to retrospective observational studies. We also have access to comprehensive data regarding baseline characteristics, as well as obstetric and neonatal outcomes. However, the robustness of our analysis was restricted by a relatively small sample size (N=940 singleton births), necessitating further larger studies. Furthermore, given that the original randomized controlled trial only enrolled women predicted to have a good prognosis for a live birth, whether our findings can be extended to patients with a predicted poor prognosis, such as those with chromosomal abnormalities that are indications for PGT-A treatment, needs further evaluation. Additionally, as the original study focused on cumulative live birth rates, the available information on pregnancy complications, particularly preeclampsia, is quite limited. Future research could explore detailed clinical characteristics related to preeclampsia for a more comprehensive understanding.
In conclusion, our study demonstrates that the sex of the fetus significantly influences the maternal risk of preeclampsia in singleton pregnancies following PGT-A treatment as compared to conventional IVF treatment. Specifically, pregnant women carrying male fetuses are likely to experience a decreased risk of preeclampsia after undergoing PGT-A treatment compared to those who received conventional IVF treatment. In this sense, our findings suggest a potential value in considering the sex-dependent influence of PGT-A treatment on the pathogenesis of preeclampsia, beyond its known protective role in reducing the rate of spontaneous abortion. In the future, additional large cohort studies are needed to not only reaffirm our findings but also to uncover the possible underlying mechanisms for these observed correlations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethics committees of the Reproductive Medical Center of Shandong University (reference number 2021140). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LG: Writing – review & editing, Writing – original draft, Visualization, Validation, Software, Methodology, Formal analysis, Data curation. XL: Writing – original draft, Methodology. AG: Writing – review & editing, Software, Formal analysis. YW: Writing – original draft, Formal analysis. YLiang: Writing – original draft, Formal analysis. YLi: Conceptualization, Writing – review & editing. XX: Writing – review & editing, Conceptualization. HL: Project administration, Funding acquisition, Writing – review & editing, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants from the National Key Research and Development Program of China (2022YFC2702400).
Acknowledgments
We are grateful to all the participants included in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1453083/full#supplementary-material
References
1. Sciorio R, Tramontano L, Catt J. Preimplantation genetic diagnosis (PGD) and genetic testing for aneuploidy (PGT-A): status and future challenges. Gynecol Endocrinol. (2020) 36:6–11. doi: 10.1080/09513590.2019.1641194
2. Gleicher N, Patrizio P, Brivanlou A. Preimplantation genetic testing for aneuploidy - a castle built on sand. Trends Mol Med. (2021) 27:731–42. doi: 10.1016/j.molmed.2020.11.009
3. Yang Z, Liu J, Collins GS, Salem SA, Liu X, Lyle SS, et al. Selection of single blastocysts for fresh transfer via standard morphology assessment alone and with array CGH for good prognosis IVF patients: results from a randomized pilot study. Mol Cytogenet. (2012) 5:24. doi: 10.1186/1755-8166-5-24
4. Rubio C, Bellver J, Rodrigo L, Castillon G, Guillen A, Vidal C, et al. In vitro fertilization with preimplantation genetic diagnosis for aneuploidies in advanced maternal age: a randomized, controlled study. Fertil Steril. (2017) 107:1122–9. doi: 10.1016/j.fertnstert.2017.03.011
5. Yan J, Qin Y, Zhao H, Sun Y, Gong F, Li R, et al. Live birth with or without preimplantation genetic testing for aneuploidy. N Engl J Med. (2021) 385:2047–58. doi: 10.1056/NEJMoa2103613
6. Gleicher N, Barad DH, Patrizio P, Orvieto R. We have reached a dead end for preimplantation genetic testing for aneuploidy. Hum Reprod. (2022) 37:2730–4. doi: 10.1093/humrep/deac052
7. Chappell LC, Cluver CA, Kingdom J, Tong S. Pre-eclampsia. Lancet. (2021) 398:341–54. doi: 10.1016/S0140-6736(20)32335-7
8. Tooher J, Thornton C, Makris A, Ogle R, Korda A, Hennessy A. All hypertensive disorders of pregnancy increase the risk of future cardiovascular disease. Hypertension. (2017) 70:798–803. doi: 10.1161/HYPERTENSIONAHA.117.09246
9. Wei D, Liu JY, Sun Y, Shi Y, Zhang B, Liu JQ, et al. Frozen versus fresh single blastocyst transfer in ovulatory women: a multicentre, randomised controlled trial. Lancet. (2019) 393:1310–8. doi: 10.1016/S0140-6736(18)32843-5
10. Gleicher N, Albertini DF, Patrizio P, Orvieto R, Adashi EY. The uncertain science of preimplantation and prenatal genetic testing. Nat Med. (2022) 28:442–4. doi: 10.1038/s41591-022-01712-7
11. Barad DH, Albertini DF, Molinari E, Gleicher N. IVF outcomes of embryos with abnormal PGT-A biopsy previously refused transfer: a prospective cohort study. Hum Reprod. (2022) 37:1194–206. doi: 10.1093/humrep/deac063
12. Broere-Brown ZA, Adank MC, Benschop L, Tielemans M, Muka T, Goncalves R, et al. Fetal sex and maternal pregnancy outcomes: a systematic review and meta-analysis. Biol Sex Differ. (2020) 11:26. doi: 10.1186/s13293-020-00299-3
13. Jaskolka D, Retnakaran R, Zinman B, Kramer CK. Fetal sex and maternal risk of pre-eclampsia/eclampsia: a systematic review and meta-analysis. BJOG. (2017) 124:553–60. doi: 10.1111/bjo.2017.124.issue-4
14. Aliyu MH, Salihu HM, Lynch O, Alio AP, Marty PJ. Fetal sex and differential survival in preeclampsia and eclampsia. Arch Gynecol Obstet. (2012) 285:361–5. doi: 10.1007/s00404-011-1984-9
15. Woitowich NC, Beery A, Woodruff T. A 10-year follow-up study of sex inclusion in the biological sciences. Elife. (2020) 9:e56344. doi: 10.7554/eLife.56344
16. Shi Y, Sun Y, Hao C, Zhang H, Wei D, Zhang Y, et al. Transfer of fresh versus frozen embryos in ovulatory women. N Engl J Med. (2018) 378:126–36. doi: 10.1056/NEJMoa1705334
17. Gardner DK, Schoolcraft WB. Culture and transfer of human blastocysts. Curr Opin Obstet Gynecol. (1999) 11:307–11. doi: 10.1097/00001703-199906000-00013
18. Ghobara T, Gelbaya TA, Ayeleke RO. Cycle regimens for frozen-thawed embryo transfer. Cochrane Database Syst Rev. (2017) 7:CD003414. doi: 10.1002/14651858.CD003414.pub3
19. A.C.o.O. Practice, ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. (2002) 77:67–75.
20. Hypertension in pregnancy. Report of the American college of obstetricians and gynecologists' Task force on hypertension in pregnancy. Obstet Gynecol. (2013) 122:1122–31. doi: 10.1097/01.AOG.0000437382.03963.88
21. Dai L, Deng C, Li Y, Zhu J, Mu Y, Deng Y, et al. Birth weight reference percentiles for Chinese. PLoS One. (2014) 9:e104779. doi: 10.1371/journal.pone.0104779
22. Montag M, van der Ven K, Rosing B, van der Ven H. Polar body biopsy: a viable alternative to preimplantation genetic diagnosis and screening. Reprod BioMed Online. (2009) 18 Suppl 1:6–11. doi: 10.1016/s1472-6483(10)60109-5
23. De Vos A, Staessen C, De Rycke M, Verpoest W, Haentjens P, Devroey P, et al. Impact of cleavage-stage embryo biopsy in view of PGD on human blastocyst implantation: a prospective cohort of single embryo transfers. Hum Reprod. (2009) 24:2988–96. doi: 10.1093/humrep/dep251
24. Dolan SM, Goldwaser TH, Jindal SK. Preimplantation genetic diagnosis for mendelian conditions. JAMA. (2017) 318:859–60. doi: 10.1001/jama.2017.10892
25. Gleicher N, Metzger J, Croft G, Kushnir VA, Albertini DF, Barad DH. A single trophectoderm biopsy at blastocyst stage is mathematically unable to determine embryo ploidy accurately enough for clinical use. Reprod Biol Endocrinol. (2017) 15:33. doi: 10.1186/s12958-017-0251-8
26. Scott RT Jr., Upham KM, Forman EJ, Hong KH, Scott KL, Taylor D, et al. Blastocyst biopsy with comprehensive chromosome screening and fresh embryo transfer significantly increases in vitro fertilization implantation and delivery rates: a randomized controlled trial. Fertil Steril. (2013) 100:697–703. doi: 10.1016/j.fertnstert.2013.04.035
27. Forman EJ, Hong KH, Franasiak JM, Scott RT Jr. Obstetrical and neonatal outcomes from the BEST Trial: single embryo transfer with aneuploidy screening improves outcomes after in vitro fertilization without compromising delivery rates. Am J Obstet Gynecol. (2014) 210:157.e1–6. doi: 10.1016/j.ajog.2013.10.016
28. Munne S, Kaplan B, Frattarelli JL, Child T, Nakhuda G, Shamma FN, et al. Preimplantation genetic testing for aneuploidy versus morphology as selection criteria for single frozen-thawed embryo transfer in good-prognosis patients: a multicenter randomized clinical trial. Fertil Steril. (2019) 112:1071–9.e7. doi: 10.1016/j.fertnstert.2019.07.1346
29. Ozgur K, Berkkanoglu M, Bulut H, Yoruk GDA, Candurmaz NN, Coetzee K. Single best euploid versus single best unknown-ploidy blastocyst frozen embryo transfers: a randomized controlled trial. J Assist Reprod Genet. (2019) 36:629–36. doi: 10.1007/s10815-018-01399-1
30. Coticchio G, Barrie A, Lagalla C, Borini A, Fishel S, Griffin D, et al. Plasticity of the human preimplantation embryo: developmental dogmas, variations on themes and self-correction. Hum Reprod Update. (2021) 27:848–65. doi: 10.1093/humupd/dmab016
31. Yang M, Rito T, Metzger J, Naftaly J, Soman R, Hu J, et al. Depletion of aneuploid cells in human embryos and gastruloids. Nat Cell Biol. (2021) 23:314–21. doi: 10.1038/s41556-021-00660-7
32. Eggenhuizen GM, Go A, Koster MPH, Baart EB, Galjaard RJ. Confined placental mosaicism and the association with pregnancy outcome and fetal growth: a review of the literature. Hum Reprod Update. (2021) 27:885–903. doi: 10.1093/humupd/dmab009
33. Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, Brinton RD, Carrero JJ, DeMeo DL, et al. Sex and gender: modifiers of health, disease, and medicine. Lancet. (2020) 396:565–82. doi: 10.1016/S0140-6736(20)31561-0
34. Vari R, Scazzocchio B, Filardi T, Citarella A, Bellenghi M, Masella R, et al. Significance of sex differences in ncRNAs expression and function in pregnancy and related complications. Biomedicines. (2021) 9:1509. doi: 10.3390/biomedicines9111509
35. Petropoulos S, Edsgard D, Reinius B, Deng Q, Panula SP, Codeluppi S, et al. Single-cell RNA-seq reveals lineage and X chromosome dynamics in human preimplantation embryos. Cell. (2016) 165:1012–26. doi: 10.1016/j.cell.2016.03.023
36. Chih HJ, Elias FTS, Gaudet L, Velez MP. Assisted reproductive technology and hypertensive disorders of pregnancy: systematic review and meta-analyses. BMC Pregnancy Childbirth. (2021) 21:449. doi: 10.1186/s12884-021-03938-8
Keywords: preimplantation genetic testing for aneuploidy, in vitro fertilization and embryo transfer, singleton pregnancy, fetal sex, preeclampsia
Citation: Guo L, Li X, Guo A, Wang Y, Liang Y, Li Y, Xu X and Lv H (2024) Comparative study on pregnancy complications: PGT-A vs. IVF-ET with gender-specific outcomes. Front. Endocrinol. 15:1453083. doi: 10.3389/fendo.2024.1453083
Received: 22 June 2024; Accepted: 17 October 2024;
Published: 06 November 2024.
Edited by:
Mariana Farina, CONICET Centro de Estudios Farmacológicos y Botánicos (CEFYBO), ArgentinaReviewed by:
Reggie García-Robles, Pontifical Javeriana University, ColombiaFelipe Vadillo-Ortega, National Autonomous University of Mexico, Mexico
Copyright © 2024 Guo, Li, Guo, Wang, Liang, Li, Xu and Lv. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinbo Xu, eHV4aW5ib0BzZHUuZWR1LmNu; Hong Lv, bHZob25nemhpZmVpQDE2My5jb20=
†These authors have contributed equally to this work and share first authorship