 Martin Kužma1*
Martin Kužma1* Peter Vaňuga2Dušan Pávai2Zdenko Killinger1Didier Hans3Neil Binkley4
Peter Vaňuga2Dušan Pávai2Zdenko Killinger1Didier Hans3Neil Binkley4 Juraj Payer1Peter Jackuliak1
Juraj Payer1Peter Jackuliak1- 15th Department of Internal Medicine, Comenius University Faculty of Medicine, University Hospital Bratislava, Bratislava, Slovakia
- 2Department of Endocrinology, National Institute of Endocrinology and Diabetology, Lubochna, Slovakia
- 3Center of Bone Diseases, Bone and Joint Department, Lausanne University Hospital, Lausanne, Switzerland
- 4Department of Medicine, University of Wisconsin, Madison, WI, United States
Introduction: Acromegaly is associated with increased vertebral fracture (VF) risk regardless of bone mineral density (BMD). However, the vertebral trabecular compartment is still low; a possible contributor to this may be impaired glucose metabolism (GM) which frequently complicates acromegaly. Additionally, soft tissue thickness may confound bone imaging in acromegaly patients.
Objective: This study aims to assess the association of GM with BMD, trabecular bone score adjusted for BMI (TBSBMI), and trabecular bone score adjusted for tissue thickness (TBSTT) among acromegaly subjects.
Patients and methods: A cross-sectional study was performed among 70 consecutive acromegaly patients (24 male/46 female, aged 55.1 years) divided in two subgroups: abnormal GM (n = 35) and normal GM (n = 35). Using DXA, BMD, TBSBMI, TBSTT, and VF screening were performed.
Results: In all subjects, TBSTT was higher (mean 9.5%) than TBSBMI. Abnormal GM subjects had lower TBSBMI (1.166 ± 0.15) than normal GM subjects (1.232 ± 0.12; p < 0.05). No between-group difference in TBSTT or BMD was observed. In a multiple regression model, the best predictor of TBSTT was HbA1c (p = 0.002). None of the DXA measures or GM parameters was a significant predictor of VF (n = 7).
Conclusion: The abnormal GM acromegaly subjects had lower TBSBMI than those with normal GM. TBSTT was higher than TBSBMI, and no between-group difference based on GM status was observed. TBSTT was significantly associated with GM parameters, notably HbA1c. The relationship of TBSTT with GM parameters may imply an effect of GM on trabecular bone microstructure in patients with acromegaly; a further study is indicated.
Introduction
In those with acromegaly, chronic GH hypersecretion leads to increased fasting plasma glucose (FPG), impaired insulin tolerance, and diabetes similar to type 2 diabetes (T2DM). T2DM adversely affects the skeleton with low bone turnover, accumulation of advanced glycation end products, and micro- and macro-architecture alterations that lead to impaired strength (1). Despite this, many studies find the bone mineral density (BMD) in T2DM patients to be ~5%–10% higher than those of age-matched non-diabetic populations (2). This BMD elevation is more pronounced in those with high BMI and, perhaps surprisingly, high HbA1c levels. This enhancement in BMD is predominantly a feature of the weight-bearing skeleton but not of non-weight-bearing bone such as the forearm. However, some caveats exist regarding the greater spine BMD in patients with T2DM, as diffuse idiopathic skeletal hyperostosis is common (3) and elevates DXA-measured BMD. By contrast, the lumbar spine trabecular bone score (TBS) is somewhat lower in patients with T2DM (4–6). A meta-analysis of 2,018 patients with T2DM found a lower TBS in diabetic than non-diabetic individuals, suggesting that TBS can be a useful measurement for fracture risk assessment in diabetic patients (7). Previously, it was thought that acromegaly patients have low BMD (8). More recently, it has been revealed that GH hypersecretion is associated with normal or even higher BMD (9), which is partly explained by larger bone size and differing effects on cortical and trabecular bone (10–13). However, several quantitative computed tomography studies in acromegaly patients found poor trabecular bone parameters, such as higher trabecular separation, lower trabecular number, and lower bone volume to tissue volume, in comparison with healthy controls (12). It is plausible that adverse trabecular bone status among acromegalic patients is related to glucose status, as a negative association of TBS with GM was indicated in the sub-analysis of a recent case–control study (14). However, there is a lack of studies that comprehensively evaluate the effect of GM status on bone parameters as assessed by DXA in acromegaly patients.
Acromegaly subjects have greater soft tissue due to the effect of GH on soft tissues such as muscle, cartilage, and visceral fat (15, 16). Thus, the potential effects of soft tissue thickness on bone measurements provided by DXA should be considered. Importantly, TBS may be lowered by greater soft tissue thickness and, as such, is currently adjusted by BMI, denoted as TBSBMI (17). Moreover, greater soft tissue thickness is associated with higher fracture risk (18). Forthcoming TBS software (TBSTT) directly adjusts TBS for densitometer-measured tissue thickness. While not currently available for clinical use, TBSTT is increasingly being reported in research studies (20–24). However, TBSTT results have not been reported in those with acromegaly.
Thus, the aim of this study was to comprehensively analyze DXA-measured BMD, TBSBMI, and TBSTT and evaluate their association with GM in patients with acromegaly.
Patients and methods
This single-center cross-sectional study of acromegaly patients was conducted at the National Institute of Endocrinology and Diabetology, Lubochna, Slovakia. Acromegaly patients evaluated from June 2016 to February 2020 were included. The regional medical ethics committee approved this study; signed informed consent was obtained prior to the conduct of any study procedure.
The inclusion criteria were as follows:
- Diagnosis of acromegaly, i.e., GH hypersecretion defined as failure to suppress GH concentration to below 1 ug/L following documented hyperglycemia during oral glucose load and increased IGF-1 (25).
- All patients regardless of age, sex, disease activity, or acromegaly-associated treatments were included in this study.
Hypopituitarism was defined as having at least one pituitary axis insufficiency and was diagnosed and treated according to the Endocrine Society (ES) guidelines (26). Central hypothyroidism was defined as free thyroxine (fT4) level below the reference range in conjunction with low or normal thyroid-stimulating hormone (TSH). Central adrenal insufficiency was defined as 8–9 a.m. serum cortisol values below 80 nmol/L or failure to increase the cortisol levels to more than 500 nmol/L at 60 min during corticotropin (ACTH) stimulation test. Male hypogonadism was defined as serum testosterone (TST) concentration and/or sperm count below the lower limit of normal with serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations not being elevated. In female patients, central hypogonadism was diagnosed by the presence of oligomenorrhea or amenorrhea, no history of uterine instrumentation or pregnancy, and normal or decreased FSH and/or LH in the absence of hyperprolactinemia (27). Diabetes insipidus was diagnosed by the presence of polyuria plus high serum osmolarity (more than 295 mOsm/L) and urine osmolality/plasma osmolality ratio ≥2.
Exclusion criteria
- Active pharmacologic osteoporosis treatment: Supplementation with vitamin D and calcium in the dose recommended by ESCEO/IOF was allowed (28).
- Patients with BMI outside of the TBSBMI recommended range (15–37 kg/m2).
The following parameters were examined in all of the patients:
1. Anthropometric parameters: weight (kg), height (cm), and body mass index (BMI; kg/m2).
2. Disease activity: According to the ES guidelines (25), active disease was defined by an IGF-1 level above the upper limit of normal for age regardless of treatment modality and a GH level >1 g/L with failure to suppress GH to <1 g/L after oral glucose load. Otherwise, the disease was considered controlled. The IGF-1 levels were measured using IMMULITE® 2500 assay, a solid phase, enzyme-labeled chemiluminescent immunometric method (ECLIA) with inter-assay variability CV of 2.4%–4.7%. The GH levels were measured with an immunoassay ECLIA having a sensitivity of 0.05 μg/L.
3. Hormonal status: Pituitary and their target hormone (TST, LH, FSH, PRL, morning serum cortisol, ACTH, TSH, and fT4) levels were measured in a routine clinical manner. All blood samples were obtained between 7:00 and 8:00 following at least an 8-h fast.
4. Bone measurements: Each subject had BMD and TBS measurement performed ±7 days from blood sampling. BMD measurements at the L1-4 spine, femoral neck (FN), and total hip (TH) were performed using a Hologic Horizon device with APEX software version 13.3:7. L1-4 TBS was performed initially using TBS iNsight® software (Medimaps SASU, Pessac, France), version 3.0.2.0. Subsequently, blinded TBSTT analysis was performed using TBS iNsight software 4.0. centrally in Geneva, Switzerland. Briefly, the TBSTT algorithm was derived through experimental work, where scans of dry ex vivo human vertebrae with different thicknesses of soft tissue equivalent material were acquired. Then, the relationship between TBS and soft tissue thickness was estimated and a specific model was defined and further applied to in vivo data (19). Vertebra were excluded from BMD and TBS analysis when there was more than one SD difference in BMD T-score from the immediately adjacent vertebral body and if vertebral fracture or cementoplasty were present.
5. GM parameters: Fasting blood glucose, HBA1c (DCCT; Diabetes Control and Complication Trial), C-peptide, and insulin resistance index (IRI) were assessed in a routine clinical manner.
6. VF assessment was performed on lateral spine images obtained using a Hologic Horizon® A densitometer (Hologic Inc., Marlborough, MA, USA) in supine position. VF was defined using the Genant VSQ approach (29) by Professor Harry Genant with vertebral height reduction of 20%–25% defining grade I, 26%–40% grade II, and ≥40% grade III. A subject was considered “fractured” if a fracture was observed regardless of unreadable levels elsewhere. VFA obtained at baseline defined prevalent fractures; new VFs at the end of the follow-up were considered incident VFs.
The subjects included in this analysis were divided into two groups based on the American Diabetes Association (ADA) 2016 guidelines (30):
1. patients with abnormal GM.
2. patients with normal GM.
Abnormal GM was defined as overt DM or prediabetes where we included those with borderline fasting blood glucose (5.6–6.9 mmol/L or 140–200 mg/dL) or impaired glucose tolerance (7.8–11.1 mmol/L at hour 2 of oGTT) or increased HBA1c (5.7%–6.4%).
Statistics
Statistical analysis was performed using the software JASP (University of Amsterdam, Netherlands, v.0.18.3). The obtained data were expressed as mean ± standard deviations (SD). Kolmogorov normality test was used to test the normality of the data. Comparisons between normal GM and abnormal GM cohorts were derived from Student’s t-test for continuous variables with normal distribution, Wilcoxon–Mann–Whitney test for continuous variables with not normal distribution, and chi-square test for categorical variables. Correlations between the investigated continuous parameters were calculated using Pearson correlation coefficient. Linear regression analysis and logistic regression were used to calculate possible relationships between significant parameters and TBS TT or vertebral fractures, respectively. The threshold for statistical significance (p-value) was set at 5%.
Results
Study group’s characteristics
A total of 70 patients—24 male (34%) and 46 female (66%)—were included in this analysis. Their mean ± SD age was 55.1 ± 11.6 years. A total of 35 (50%; 14 M/21 F) had abnormal GM, and 35 (50%; 10 M/25 F) had normal GM. At the time of diagnosis, acromegaly was treated surgically in most patients (71%), followed by medical treatment with somatostatin receptor ligands (SRLs) in 55 subjects (78%). SRL treatment was used in 34 (97%) of subjects in the abnormal GM group and 21 (60%) in the normal GM group. Out of 35 patients with abnormal GM, eight patients (22%) were treated with antidiabetic medication: five patients had oral antidiabetic therapy (metformin average dose = 1,500 mg/day), two patients had insulin, and one patient was on combined treatment with insulin + oral antidiabetic (metformin 2,000 mg/day). In the group with abnormal GM, 15 (42.8%) subjects had active disease, 23 (65.7%) had undergone pituitary surgery, eight (22.8%) were treated with SRLs pre-operatively, and 26 (74.2%) were treated with SRLs post-operatively. Among the normal GM group, 11 (31.4%) had active disease, 27 (77%) had pituitary surgery, 10 (28.5%) were treated with SRLs pre-operatively, and 14 (40%) were treated with SRLs post-operatively. A greater number of subjects within the abnormal GM group (N = 26) were treated with SRLs post-operatively than in those with normal GM (N = 14) (p < 0.001). The subjects within the abnormal GM group had a longer duration of SRL treatment pre- and post-operatively (both p < 0.05) (see also Table 1). The subjects with abnormal GM had greater weight (92.8 ± 18.9 vs. 82.7 ± 19.1 kg; p < 0.05) and BMI (33.1 ± 12.6 vs. 28.2 ± 5.5 kg/m2; p < 0.05) than subjects with normal GM. A longer duration of treatment with SRLs among subjects with abnormal GM was observed (see Table 1). The subjects with abnormal GM had significantly higher values of HGBA1c (6.25% ± 1.13% vs. 5.5% ± 0.41%) and fasting blood glucose (6.46 ± 1.36 vs. 5.1 ± 0.26 mmol/L) than the patients with normal GM (both p < 0.05, see Table 1). There was no difference in C-peptide IRI or IGF1 levels between groups.
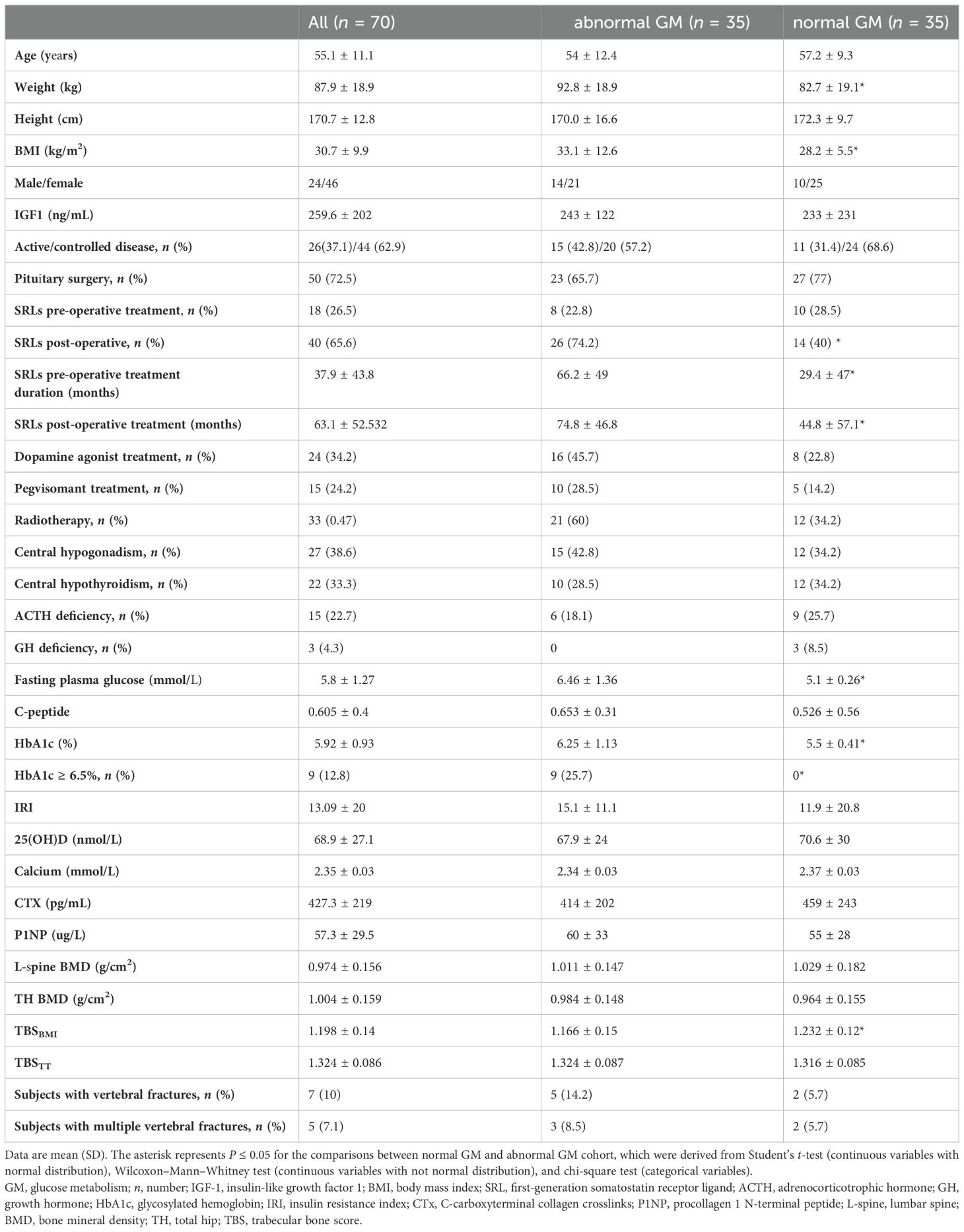
Table 1. Baseline characteristics of the study groups—comparison of subjects with impaired vs. normal GM.
Bone measurements
In all subjects, regardless of GM status, TBSTT (mean 1.324 ± 0.09) was higher by ~10% than TBSBMI (mean 1.198 ± 0.14) (p < 0.001). Patients with abnormal GM had a significantly lower mean TBSBMI than those with normal GM (1.166 ± 0.15 vs. 1.232 ± 0.12; p < 0.05). TBSTT did not differ by GM status; TBSTT = 1.324 ± 0.087 in the abnormal GM group vs. 1.316 ± 0.085 in the normal GM group (Figure 1). No difference in BMD or in bone turnover markers between patients with and without GM was observed.
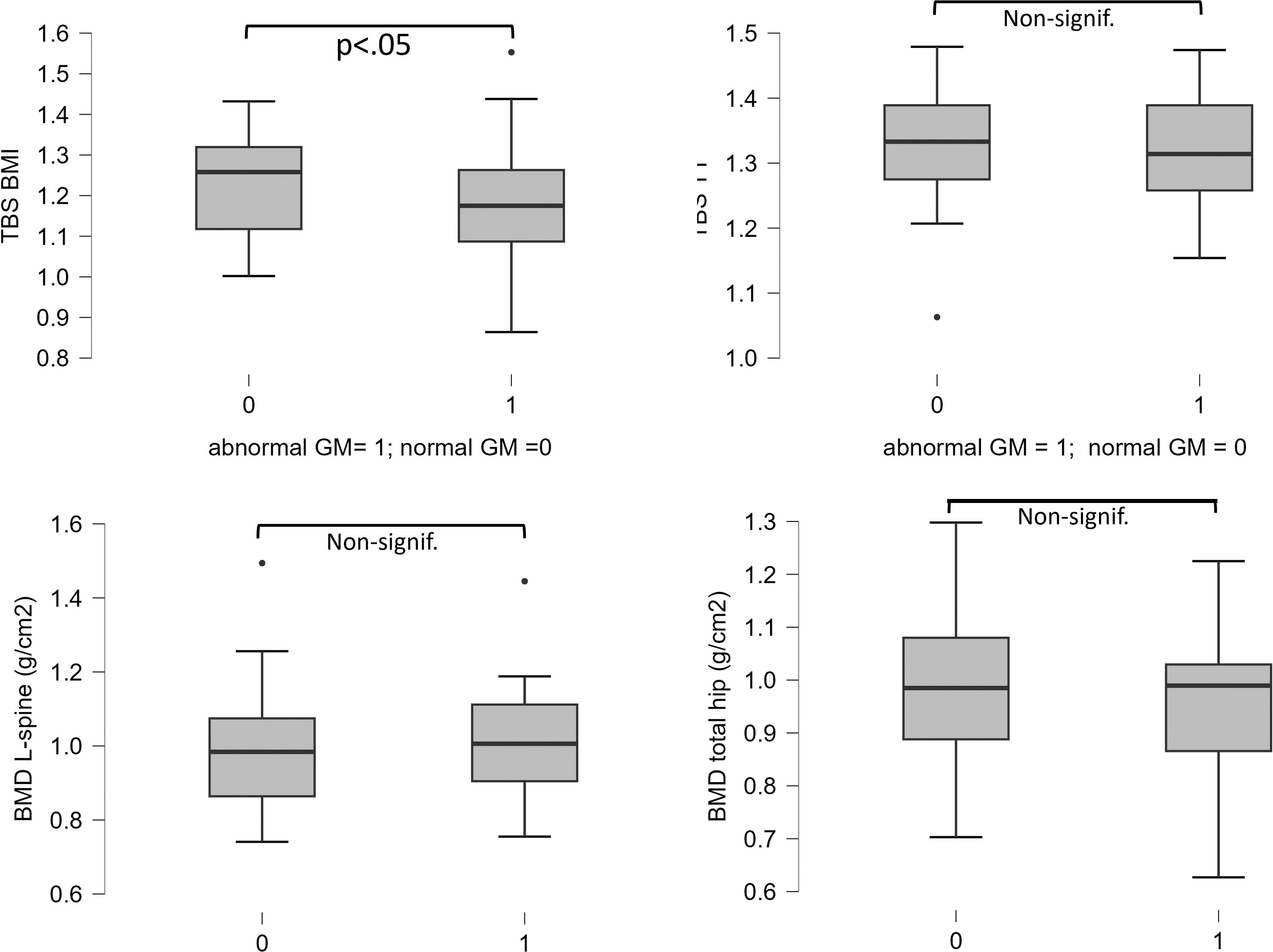
Figure 1. Differences of TBSBMI, TBSTT, L-spine BMD, and total hip BMD between subgroups with abnormal and normal glucose metabolism. A significant difference of TBSBMI was observed.
IGF-1, FPG, HBA1c, C-peptide, duration of SRL pre- and post-operatively, TBSTT, and TBSBMI were correlated in a simple regression model (see Table 2). A significant correlation of IGF-1 with C-peptide (R = 0.293; p = 0.02), but not with other parameters, was observed. HBA1c (R = 0.802; p < 0.001) and FPG (R = 0.572; p = 0.01) were significantly associated with pre-operative SRL treatment duration. FPG (R = - 0.402; p < 0.001), HbA1c (R = -0.474; p < 0.001), and C-peptide (R = -0.341; p = 0.007) were negatively associated with TBSBMI. A weaker correlation of FPG (-0.244; p = 0.05) and HBA1c (R = -0.331; p < 0.007) with TBSTT was observed (see Table 2).
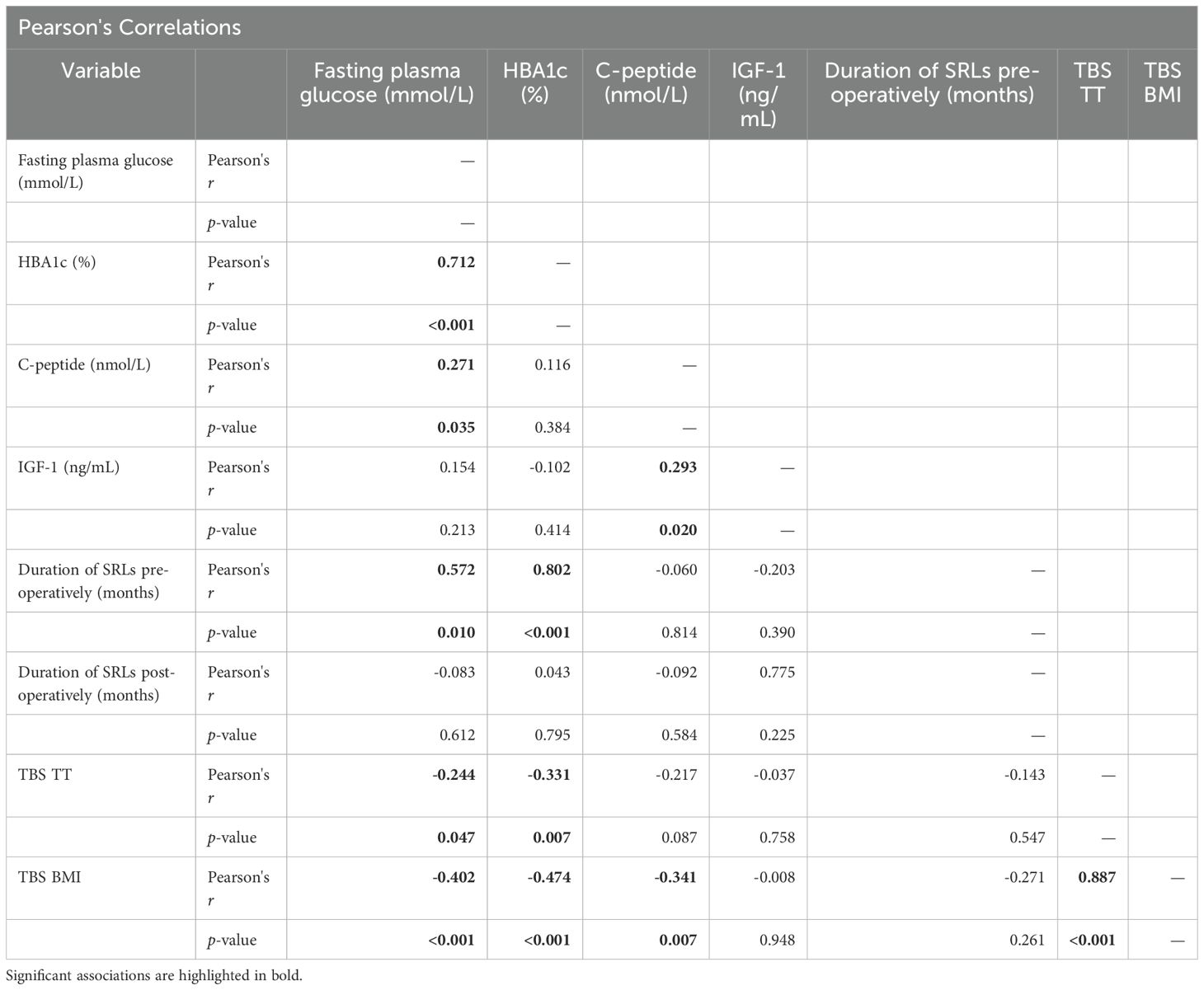
Table 2. Correlation matrix for simple regression models between significant parameters—FPG, HbA1c, C-peptide, IGF-1, duration of SRL pre- and post-operative treatments, TBSBMI, and TBSTT.
According to a linear regression model including all parameters (FPG, HbA1c, C-peptide, preoperative duration of SRL treatment, and weight), the best predictors for TBSTT was HbA1c (p = 0.002) and duration of SRL treatment preoperatively (p = 0.03) (see Table 3).
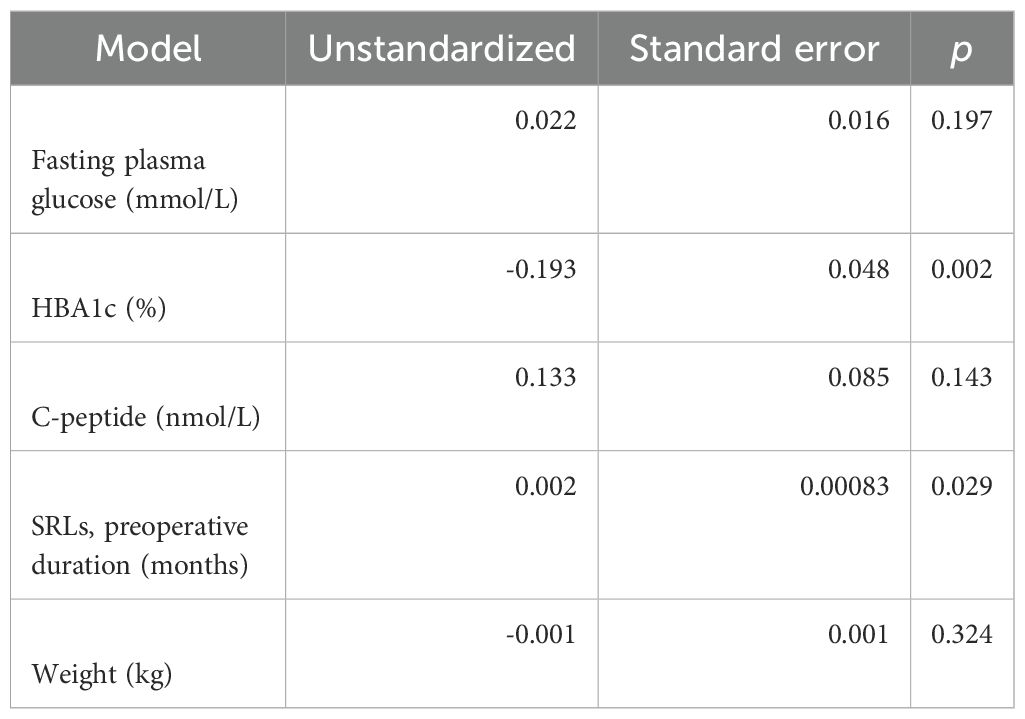
Table 3. Multiple regression model. According to a linear regression model with all of the parameters included (FPG, HbA1c, C-peptide, preoperative duration of SRL treatment, and weight), the best predictor for TBSTT was HbA1c.
Vertebral fractures
There were seven subjects with asymptomatic vertebral fracture (VF) in the entire cohort, of which five were in the abnormal GM group. There were five subjects with multiple VFs. No difference in the prevalence of VFs or multiple VFs between groups with abnormal and normal GM was observed (see Table 1). Total hip BMD was significantly lower in those with VF (0.874 ± 0.19 g/cm2) than in those without VF (0.985 ± 0.15 g/cm2; p < 0.05). No difference in TBSTT, TBSBMI, or L-spine BMD between the VF and non-VF groups was observed (see Figure 2). Among all GM or lumbar spine DXA parameters, none was a significant predictor of VF as assessed by logistic regression (see Table 4).
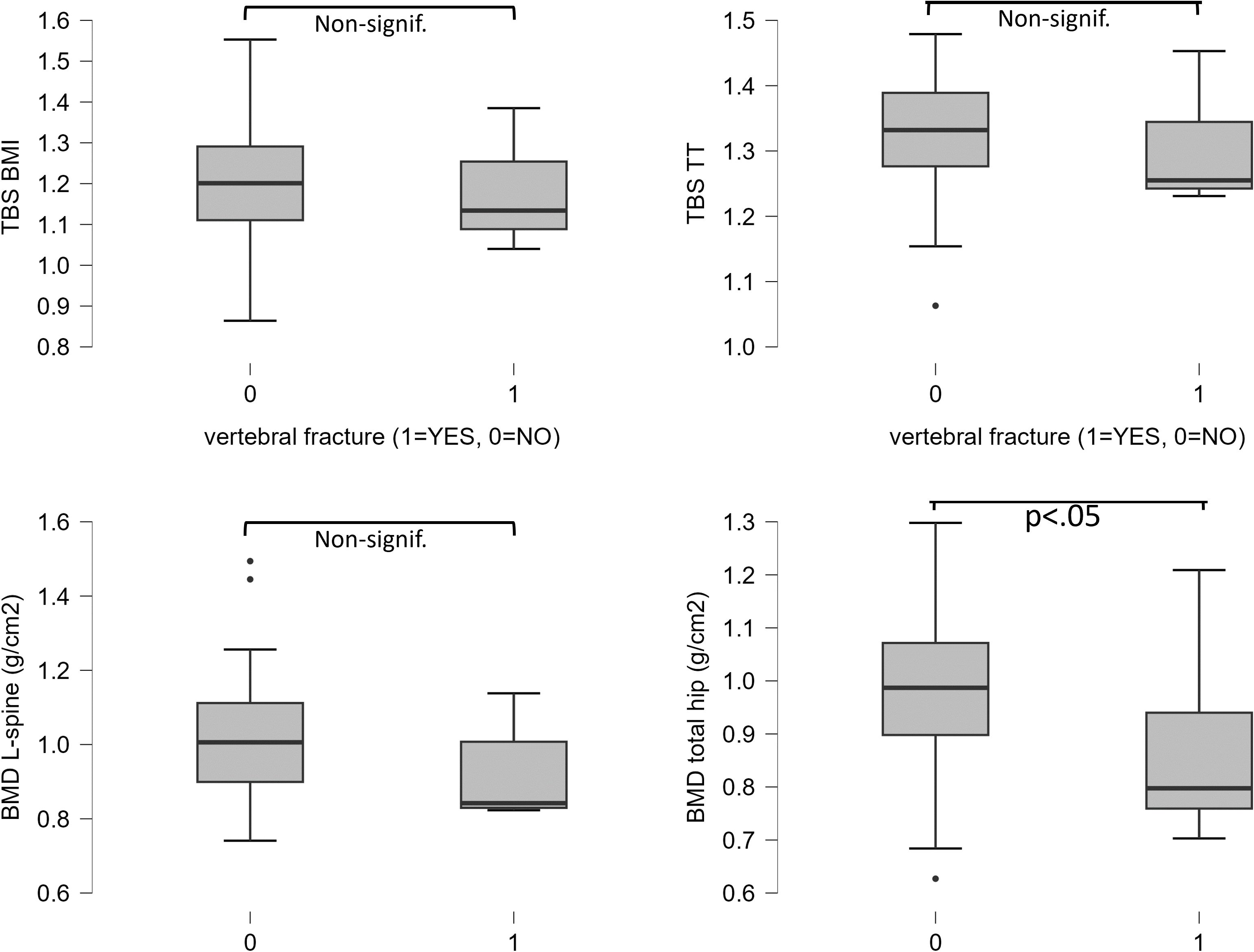
Figure 2. Differences of TBSBMI, TBSTT, L-spine BMD, and total hip BMD between subgroups with vertebral fracture (VF) and without VF. A significant difference of total hip BMD was observed.
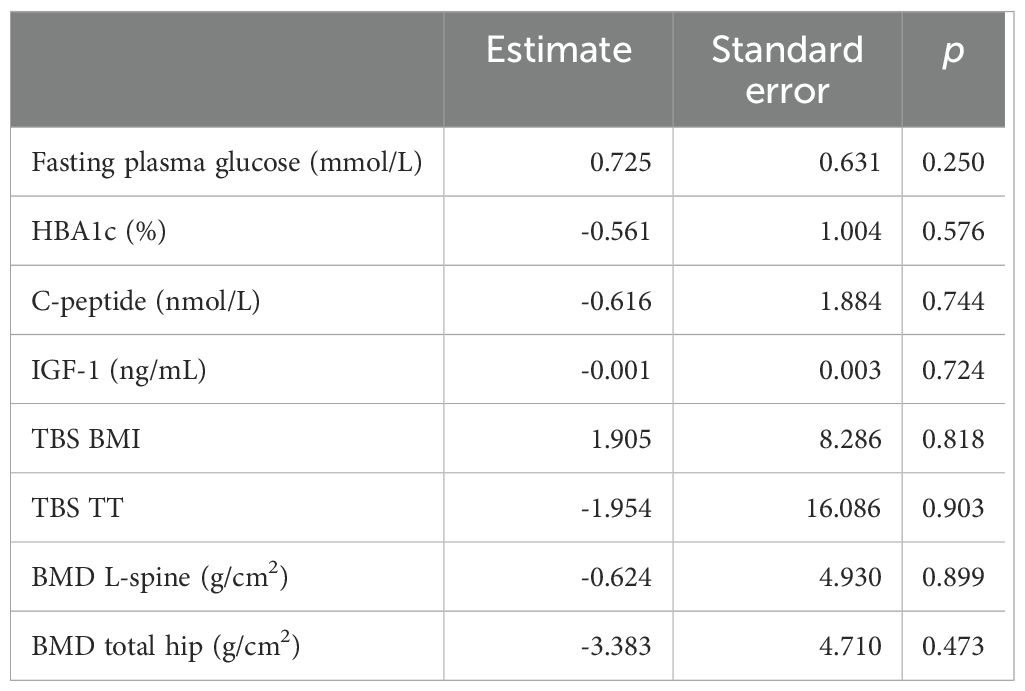
Table 4. Logistic regression model. From all glucose metabolism parameters, TBSBMI, TBSTT, and BMD, none was a significant estimate for vertebral fracture.
Discussion
In this study, acromegaly patients with abnormal GM have lower TBSBMI than those with normal GM. Correction of TBS for tissue thickness (TBSTT) increased the TBS values by ~10% compared to TBSBMI, and no difference in TBSTT according to GM status was observed. TBSTT was still negatively associated with fasting plasma glucose and HBA1c. Several significant associations between GM, IGF-1, duration of SRL treatment, TBSBMI, and TBSTT were observed. From all of these parameters, multiple regression analysis found HbA1c to be the most significant predictor of TBSTT. In addition, there was a relationship between GM and duration of SRL treatment, which is possibly one of the risk factors for impaired glucose metabolism. The relationship of TBSTT with the parameters of GM status suggests that trabecular bone microstructure in acromegaly might be affected by abnormal GM, not simply GH hypersecretion itself. VF prevalence did not differ between groups according to GM status, which was likely due to the small number of fractures. Finally, this study demonstrates that TBS correction for soft tissue thickness significantly affects the result; this should be considered in conditions with higher amounts of soft tissue, such as acromegaly, diabetes, obesity, etc.
Diabetes mellitus occurs in about 20%–40% of patients with acromegaly (31); the clinical picture resembles type 2 diabetes mellitus (32). In this study, we confirmed a high prevalence of GM impairment among subjects with acromegaly. Patients with acromegaly and abnormal GM have lower TBSBMI, but not TBSTT, than those with normal GM. Despite the differences in BMD, the risk of fractures in patients with diabetes mellitus type 1 and type 2 is increased (33). Normal or slightly increased BMD in patients with type 2 diabetes mellitus does not “protect” them from osteoporotic fractures, suggesting that BMD alone underestimates fracture risk in such individuals. As with other forms of secondary osteoporosis (34–37), the bone quality in acromegaly does not correspond to BMD. Although we confirmed a difference in TBSBMI, but not BMD, in the observed groups, the prevalence of VF in our cohort did not differ significantly based on the occurrence of GM disorder. In a simple regression model, we confirmed a positive correlation between IGF-1 and C-peptide, which indicates a link between GM and GH hypersecretion. At the same time, a significant negative association between TBSTT and GM parameters was confirmed. In a study of 105 postmenopausal women with type 2 diabetes mellitus, the analysis showed that HBA1c below 7.0% had no effect on BMD in patients with type 2 diabetes mellitus, but at the same time, patients with HBA1c <7.0% had better TBSBMI than patients with HBA1c above 7.0%. In the group of 14 patients with a low traumatic clinical fracture in different locations, higher HBA1c and lower TBSBMI compared to patients without clinical fracture were observed (38). However, there was no difference between TBSTT in this study according to GM impairment. Thus, other factors that could influence both glucose metabolism and soft tissue also come into consideration. Because we saw a strong correlation of SRL treatment duration pre-operatively, we must admit that SRLs have a significant impact on GM. In addition, in the group with abnormal GM, a greater number of subjects were treated with SRLs post-surgery. It is well known that SRLs act on pancreatic alpha‐ and beta‐cells, impairing both insulin and glucagon secretion. Despite many studies demonstrating that SRL administration leads to impairment of glucose homeostasis, there are some studies proving that the effect on glucose metabolism is not statistically significant (39–41). Based on our analysis, SRLs likely play a certain role in worsening glucose metabolism and thus indirectly lead to a decline in TBSBMI or tissue thickness. However, this should be analyzed by longitudinal studies aimed specifically to assess the effect of SRLs on bone microarchitecture.
Overall, the relationship between GM and its effect on bone in patients with acromegaly is addressed only by a minimum of studies (42). To our knowledge, this study is the only available publication that discusses the influence of GM parameters on bone parameters among subjects with acromegaly.
This study has several strengths, such as a relatively large sample size considering that acromegaly is a rare diagnosis. Multiple DXA parameters were evaluated, and vertebral fractures were identified by Dr. Harry Genant†. All DXA parameters evaluated are potentially available in routine clinical practice. Additionally, TBS correction for soft tissue thickness (TBSTT) was used. Undoubtedly, TBSTT brings new light to the issue of fracture risk assessment and must be considered in subjects with greater abdominal soft tissue. Study limitations include the absence of a control group; a comparison of acromegaly diabetic subjects with the general diabetic population could also improve this study. Finally, we were unable to clarify the relationship between the onset of GM impairment and bone status.
In conclusion, this study showed that acromegaly subjects with abnormal GM have lower TBSBMI compared to those with normal GM, and after correction of TBSBMI for soft tissue thickness, this difference was lost and, importantly, TBSTT increased significantly. However, TBSTT remained significantly associated with GM, mostly HbA1c. This study suggests, for the first time, that trabecular bone microstructure, as indirectly assessed by TBSTT, might be affected by abnormal GM, not GH hypersecretion itself. In addition, SRL treatment likely plays a role. However, further studies with a greater number of subjects and with comparison between healthy controls and subjects with diabetes among the general population are needed to better understand this issue.
Data availability statement
The datasets presented in this article are not readily available because it contains personal data. Requests to access the datasets should be directed to a3V6bWFAcnUudW5iLnNr.
Ethics statement
The studies involving humans were approved by ethics committee of the National Institute of Diabetology and Endocrinology. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MK: Conceptualization, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing, Data curation, Supervision, Validation. PV: Conceptualization, Data curation, Investigation, Supervision, Writing – review & editing, Writing – original draft, Project administration. DP: Data curation, Investigation, Project administration, Writing – original draft, Writing – review & editing. ZK: Conceptualization, Investigation, Methodology, Software, Validation, Writing – review & editing, Writing – original draft. DH: Conceptualization, Formal Analysis, Software, Writing – review & editing, Writing – original draft. NB: Conceptualization, Formal Analysis, Supervision, Writing – review & editing, Writing – original draft, Methodology. JP: Conceptualization, Supervision, Writing – original draft, Writing – review & editing, Formal Analysis, Validation. PJ: Conceptualization, Methodology, Validation, Writing – review & editing, Writing – original draft, Software.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We thank the Scientific Grant Agency of the Ministry of Education, Research, Development, and Youth of the Slovak Republic and the Slovak Academy of Sciences (VEGA) for funding this project (no. 1/0378/21).
Conflict of interest
DH is co-founder and CEO of Med-Imaps.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Napoli N, Chandran M, Pierroz DD, Abrahamsen B, Schwartz AV, Ferrari SL, et al. Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinology. (2017) 13:208–19. doi: 10.1038/nrendo.2016.153
2. Bonds DE, Larson JC, Schwartz AV, Strotmeyer ES, Robbins J, Rodriguez BL, et al. Risk of fracture in women with type 2 diabetes: the Women’s Health Initiative Observational Study. J Clin Endocrinol Metab. (2006) 91:3404–10. doi: 10.1210/jc.2006-0614
3. Weinfeld RM, Olson PN, Maki DD, Griffiths HJ. The prevalence of diffuse idiopathic skeletal hyperostosis (DISH) in two large American Midwest metropolitan hospital populations. Skeletal radiology. (1997) 26:222–5. doi: 10.1007/s002560050225
4. Dhaliwal R, Cibula D, Ghosh C, Weinstock RS, Moses AM. Bone quality assessment in type 2 diabetes mellitus. Osteoporosis Int. (2014) 25:1969–73. doi: 10.1007/s00198-014-2704-7
5. Leslie WD, Aubry-Rozier B, Lamy O, Hans D. TBS (trabecular bone score) and diabetes-related fracture risk. J Clin Endocrinol Metab. (2013) 98:602–9. doi: 10.1210/jc.2012-3118
6. Rubin MR, Patsch JM. Assessment of bone turnover and bone quality in type 2 diabetic bone disease: current concepts and future directions. Bone Res. (2016) 4:16001. doi: 10.1038/boneres.2016.1
7. Ho-Pham LT, Nguyen TV. Association between trabecular bone score and type 2 diabetes: a quantitative update of evidence. Osteoporosis Int. (2019) 30:2079–85. doi: 10.1007/s00198-019-05053-z
8. Scillitani A, Chiodini I, Carnevale V, Giannatempo GM, Frusciante V, Villella M, et al. Skeletal involvement in female acromegalic subjects: the effects of growth hormone excess in amenorrheal and menstruating patients. J Bone mineral Res. (1997) 12:1729–36. doi: 10.1359/jbmr.1997.12.10.1729
9. Mazziotti G, Biagioli E, Maffezzoni F, Spinello M, Serra V, Maroldi R, et al. Bone turnover, bone mineral density, and fracture risk in acromegaly: a meta-analysis. J Clin Endocrinol Metab. (2015) 100:384–94. doi: 10.1210/jc.2014-2937
10. Diamond T, Nery L, Posen S. Spinal and peripheral bone mineral densities in acromegaly: the effects of excess growth hormone and hypogonadism. Ann Internal Med. (1989) 111:567–73. doi: 10.7326/0003-4819-111-7-567
11. Carbonare LD, Micheletti V, Cosaro E, Valenti MT, Mottes M, Francia G, et al. Bone histomorphometry in acromegaly patients with fragility vertebral fractures. Pituitary. (2018) 21:56–64. doi: 10.1007/s11102-017-0847-1
12. Maffezzoni F, Maddalo M, Mezzone M, Zorza I, Baruffaldi F, Baruffaldi F, et al. High-resolution-cone beam tomography analysis of bone microarchitecture in patients with acromegaly and radiological vertebral fractures. Endocrine. (2016) 54:532–42. doi: 10.1007/s12020-016-1078-3
13. Madeira M, Neto LV, de Paula Paranhos Neto F, Barbosa Lima IC, Carvalho de Mendonca LM, Gadelha MR, et al. Acromegaly has a negative influence on trabecular bone, but not on cortical bone, as assessed by high-resolution peripheral quantitative computed tomography. J Clin Endocrinol Metab. (2013) 98:1734–41. doi: 10.1210/jc.2012-4073
14. Ságová I, Mokáň M, Tonhajzerová I, Rončáková M, Vaňuga P. Age, body composition parameters and glycaemic control contribute to trabecular bone score deterioration in acromegaly more than disease activity. Front Endocrinol. (2023) 14. doi: 10.3389/fendo.2023.1197725
15. Aulinas A, Crespo I, Viladés D, Leta R, Urgell E, Biagetti B, et al. Cystatin-C and epicardial adipose tissue as noninvasive predictors of cardiovascular risk in acromegaly. Clin endocrinology. (2017) 86:214–22. doi: 10.1111/cen.2017.86.issue-2
16. Dequeker J, Geussens P, De Proft G, Bouillon R. Radiogrammetry of the soft tissue at the index finger in acromegaly. Clin Radiology. (1979) 30:517–9. doi: 10.1016/S0009-9260(79)80184-1
17. Palomo T, Dreyer P, Muszkat P, Weiler FG, Bonansea TCP, Domingues FC, et al. Effect of soft tissue noise on trabecular bone score in postmenopausal women with diabetes: A cross sectional study. Bone. (2022) 157:116339. doi: 10.1016/j.bone.2022.116339
18. Leslie WD, Goel H, Binkley N, McCloskey EV, Hans D. Contributions of clinical and technical factors to longitudinal change in trabecular bone score and bone density: A registry-based individual-level analysis. J Bone Mineral Res. (2023) 38:512–21. doi: 10.1002/jbmr.4774
19. Shevroja E, Aubry-Rozier B. Clinical performance of the updated trabecular bone score (TBS) algorithm. Which Accounts Soft Tissue Thickness: OsteoLaus Study. (2019) 34:2229–37. doi: 10.1002/jbmr.3851
20. Hans D, Messina C. Increasing soft tissue thickness does not affect trabecular bone score reproducibility: a phantom study. J Bone mineral Res. (2018) 61:336–42. doi: 10.1007/s12020-018-1647-8
21. Hans D, Shevroja E. Updated trabecular bone score accounting for the soft tissue thickness (TBS(TT)) demonstrated significantly improved bone microstructure with denosumab in the FREEDOM TBS post hoc analysis. Osteoporosis Int. (2022) 33(12):2517–25. doi: 10.1007/s00198-022-06549-x
22. Poloni A, Chianca V, Albano D, Piodi LP, Ulivieri FM, Sconfienza LM, et al. Simulated increased soft tissue thickness artefactually decreases trabecular bone score: a phantom study. Endocrine. (2016) 17:17. doi: 10.1007/s12020-018-1647-8
23. Shevroja E. Clinical performance of the updated trabecular bone score (TBS) algorithm, which accounts for the soft tissue thickness: the osteoLaus study. J Bone mineral Res. (2019) 34:2229–37. doi: 10.1002/jbmr.3851
24. Valenzuela Riveros LF. Trabecular bone score (TBS) varies with correction for tissue thickness versus body mass index: implications when using pediatric reference norms. Osteoporosis Int. (2023) 38:493–8. doi: 10.1002/jbmr.4786
25. Katznelson L, Laws ER Jr., Melmed S, Molitch ME, Murad MH, Utz A, et al. Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2014) 99:3933–51. doi: 10.1210/jc.2014-2700
26. Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, et al. Hormonal replacement in hypopituitarism in adults: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2016) 101:3888–921. doi: 10.1210/jc.2016-2118
27. Kužma M, Hans D, Koller T, Némethová E, Jackuliak P, Killinger Z, et al. Less strict intervention thresholds for the FRAX and TBS-adjusted FRAX predict clinical fractures in osteopenic postmenopausal women with no prior fractures. J Bone mineral Metab. (2018) 36:580–8. doi: 10.1007/s00774-017-0864-1
28. Available online at: https://www.osteoporosis.foundation/health-professionals/prevention/nutrition/calcium (Accessed March 7, 2024).
29. Genant HK, Jergas M, Palermo L, Nevitt M, Valentin RS, Black D, et al. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone mineral Res. (1996) 11:984–96. doi: 10.1002/jbmr.5650110716
30. Association AD. 2. Classification and diagnosis of diabetes. Diabetes Care. (2015) 39:S13–22. doi: 10.2337/dc16-S005
31. Giustina A, Casanueva FF, Cavagnini F, Chanson P, Clemmons D, Frohman LA, et al. Diagnosis and treatment of acromegaly complications. J endocrinological Invest. (2003) 26:1242–7. doi: 10.1007/BF03349164
32. Räkel A, Sheehy O, Rahme E, LeLorier J. Osteoporosis among patients with type 1 and type 2 diabetes. Diabetes Metab. (2008) 34:193–205. doi: 10.1016/j.diabet.2007.10.008
33. Ma L, Oei L, Jiang L, Estrada K, Chen H, Wang Z, et al. Association between bone mineral density and type 2 diabetes mellitus: a meta-analysis of observational studies. Eur J Epidemiol. (2012) 27:319–32. doi: 10.1007/s10654-012-9674-x
34. Mazziotti G, Canalis E, Giustina A. Drug-induced osteoporosis: mechanisms and clinical implications. Am J Med. (2010) 123:877–84. doi: 10.1016/j.amjmed.2010.02.028
35. Mazziotti G, Porcelli T, Mormando M, De Menis E, Bianchi A, Mejia C, et al. Vertebral fractures in males with prolactinoma. Endocrine. (2011) 39:288–93. doi: 10.1007/s12020-011-9462-5
36. Angeli A, Guglielmi G, Dovio A, Capelli G, de Feo D, Giannini S, et al. High prevalence of asymptomatic vertebral fractures in post-menopausal women receiving chronic glucocorticoid therapy: a cross-sectional outpatient study. Bone. (2006) 39:253–9. doi: 10.1016/j.bone.2006.02.005
37. Mazziotti G, Delgado A, Maffezzoni F, Formenti A, Giustina A. Skeletal fragility in endogenous hypercortisolism. Front hormone Res. (2016) 46:66–73. doi: 10.1159/000443866
38. Jackuliak P, Kužma M, Killinger Z, Payer J. Good long-term glycemic compensation is associated with better trabecular bone score in postmenopausal women with type 2 diabetes. Physiol Res. (2019) 68:S149–S56. doi: 10.33549/physiolres
39. Ho KK, Jenkins AB, Furler SM, Borkman M, Chisholm DJ. Impact of octreotide, a long-acting somatostatin analogue, on glucose tolerance and insulin sensitivity in acromegaly. Clin endocrinology. (1992) 36:271–9. doi: 10.1111/j.1365-2265.1992.tb01443.x
40. Ronchi CL, Varca V, Beck-Peccoz P, Orsi E, Donadio F, Baccarelli A, et al. Comparison between six-year therapy with long-acting somatostatin analogs and successful surgery in acromegaly: effects on cardiovascular risk factors. J Clin Endocrinol Metab. (2006) 91:121–8. doi: 10.1210/jc.2005-1704
41. Baldelli R, Battista C, Leonetti F, Ghiggi MR, Ribaudo MC, Paoloni A, et al. Glucose homeostasis in acromegaly: effects of long-acting somatostatin analogues treatment. Clin endocrinology. (2003) 59:492–9. doi: 10.1046/j.1365-2265.2003.01876.x
Keywords: acromegaly, glucose metabolism, trabecular bone score, tissue thickness, bone mineral density
Citation: Kužma M, Vaňuga P, Pávai D, Killinger Z, Hans D, Binkley N, Payer J and Jackuliak P (2024) Association of trabecular bone score corrected for tissue thickness with glucose metabolism in acromegaly. Front. Endocrinol. 15:1448566. doi: 10.3389/fendo.2024.1448566
Received: 13 June 2024; Accepted: 05 November 2024;
Published: 12 December 2024.
Edited by:
Ali Ghasem-Zadeh, University of Melbourne, AustraliaReviewed by:
Grzegorz Tatoń, Jagiellonian University, PolandCatalina Poiana, Carol Davila University of Medicine and Pharmacy, Romania
Copyright © 2024 Kužma, Vaňuga, Pávai, Killinger, Hans, Binkley, Payer and Jackuliak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Kužma, a3V6bWE0QHVuaWJhLnNr