 Lili Ma
Lili Ma Jing Wang
Jing Wang Li Ma
Li Ma Xian Min Wang
Xian Min Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Endocrinol., 07 February 2025
Sec. Systems Endocrinology
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1441503
This article is part of the Research TopicMechanistic, Machine Learning and Hybrid Models of the 'Other' Endocrine Regulatory Systems in Health and Disease: Volume IIView all 3 articles
Background: Hyperuricemia (HUA) is a significant public health issue, ranking second only to diabetes in prevalence. While existing research demonstrates a robust correlation between these two conditions, the precise etiological mechanisms remain inadequately elucidated. This study utilized scientometric analysis to investigate the global association between HUA and diabetes.
Methods: Data on HUA and diabetes were retrieved from the Web of Science Core Collection database, encompassing the period from its inception until September 30, 2024. Collaboration networks were examined using VOSviewer, cluster analysis was executed with CiteSpace, and systematic mapping was conducted using Bibliometrix.
Results: By September 30, 2024, 1,464 studies indicated a consistent yearly increase in publications connecting HUA and diabetes despite some fluctuations. The lead authors were Richard J. Johnson, Miguel A. Lanaspa, and Masanari Kuwabara, with most contributors from China, the United States, and Japan. Key institutions include China Medical University, Shanghai Jiao Tong University, and Capital Medical University. The most published journal was Nutrition, Metabolism and Cardiovascular Diseases (CVDs), whereas the most cited journal was Diabetes Care. The reference network from 1987 to September 30, 2024, identified 19 clusters highlighting key research areas in HUA and diabetes, such as metabolic syndrome, uropathology, chronic kidney disease (CKD), and CVD. Exploring pathological mechanisms and pharmacological interventions linked to diabetes concomitant with HUA has emerged as a focal point of research and a burgeoning trend within the field.
Conclusion: This study is the first scientometric analysis to synthesize research trends on HUA and diabetes, revealing molecular mechanisms and treatment strategies and providing theoretical insights for future clinical use.
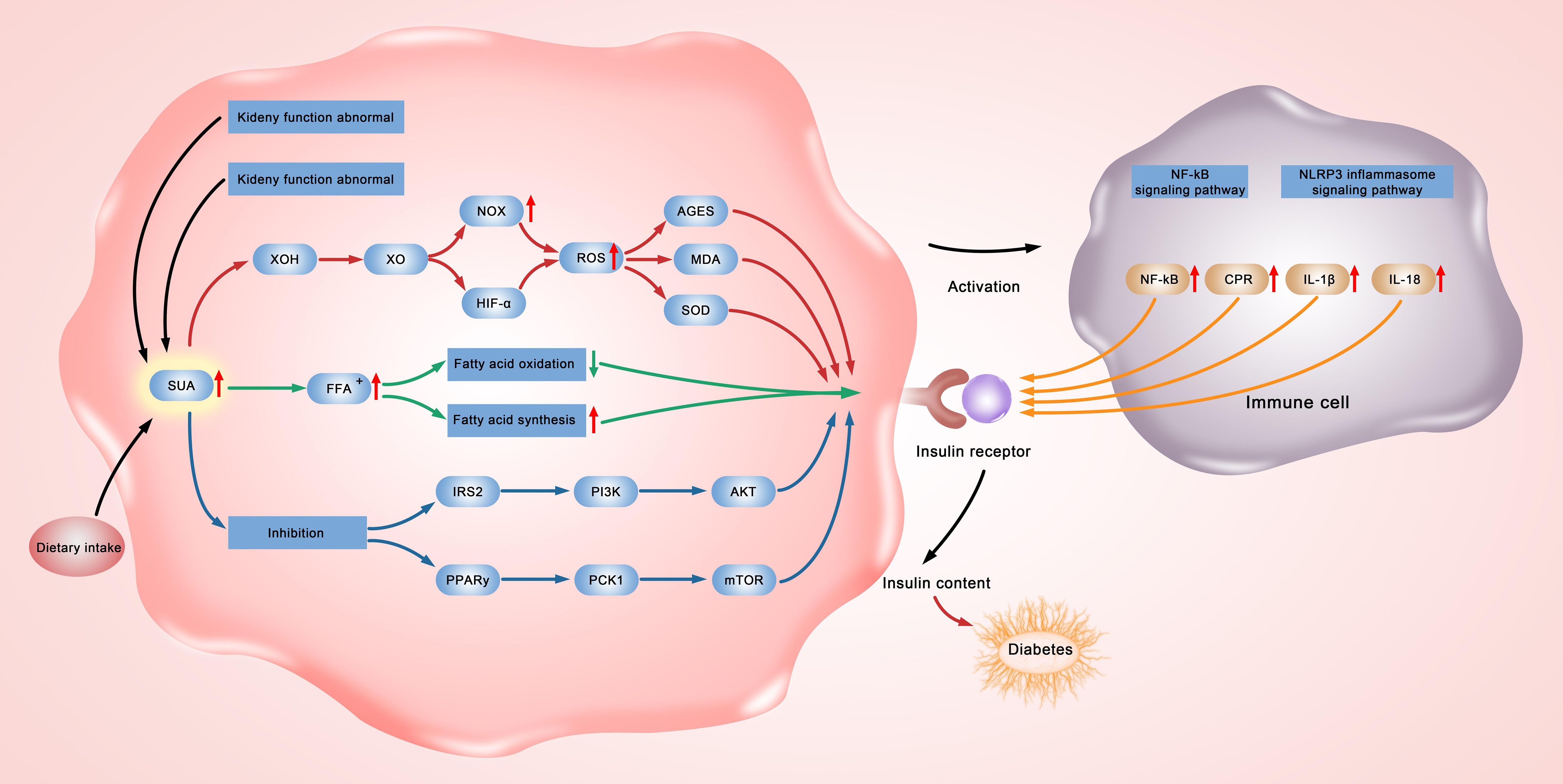
Graphical Abstract.
Hyperuricemia (HUA) is a metabolic disorder marked by high uric acid levels due to increased production or decreased excretion during purine metabolism. In adult populations, HUA is typically diagnosed when serum uric acid concentrations exceed 6.0 mg/dL in females and 7.0 mg/dL in males (1). This condition is a significant public health issue, ranking second only to diabetes in prevalence. Research has indicated that HUA prevalence in Italy increased from 8.5% to 11.9% between 2005 and 2009 (2). Additionally, HUA incidence in China was reported to be 35.4% (3), while the international prevalence was noted to be 3.3% (4). A recent cohort study observed a strong link between high serum uric acid levels and type 2 diabetes (5). HUA prevalence among diabetic patients has been reported to be 21.24% in China (6) and 20.70% in North America (7). HUA might increase the risk of developing type 2 diabetes (8), leading to a higher incidence of diabetic nephropathy (9). Serum uric acid is the only diagnostic marker for HUA, acting as a key antioxidant and playing a role in obesity-related insulin resistance (10).
Recently, there has been a substantial increase in significant research concerning HUA and diabetes, leading some scholars to conduct thorough reviews and analyses of the relevant findings. Research on male urate oxidase knockout mice indicates that glucose metabolism issues lead to reduced insulin secretion and a higher risk of streptozotocin-induced diabetes (11). Zhao et al. (12) found that HUA in mice with metabolic disorders and insulin resistance increased inflammation, impaired glucose uptake, disrupted insulin signaling, and sped up diabetes progression. Yanai et al. (13) found that elevated urate transporter 1 and glucose transporter 9 (GLUT9) levels, combined with impaired glycolysis from insulin resistance, can lead to HUA. Lu et al. (14) further revealed that uric acid contributes to diabetes progression by hindering islet beta cell survival rather than directly triggering the disease. Yu W et al. (15) found that thioredoxin-interacting protein reduces oxidative stress and counters HUA-induced insulin resistance, suggesting it as a potential treatment target. Besides, Huang et al. (16) developed a HUA risk model for diabetic nephropathy patients, enhancing early detection and prevention in those with chronic nephropathy.
While past studies have explored the pathogenesis and treatment targets of HUA and diabetes, the exact link between them remains unknown, and quantitative analysis of literature in this field is lacking. Recently, bibliometrics has been used to bridge informatics and science (17). Progress in data visualization, text mining, and web analytics has created a new framework for synthesizing research evidence and impact (18). This framework used visual analysis and scientometrics to explore a field’s growth, knowledge structure, and academic exchange, helping identify key topics and development contexts essential for theoretical and practical advancements (19). Therefore, we conducted a scientometric study on HUA and literature on diabetes to analyze trends, networks, and authors, aiming to offer fresh insights and directions for research on their relationship.
Computer searches were performed in the Web of Science Core Collection using a Topic Search for terms related to “High uric acid” and “diabetes mellitus (DM),” including variations such as “type 2 DM” and “type 1 diabetes.” The search targeted English articles and reviews published until September 30, 2024. Figure 1 depicts the retrieval process.
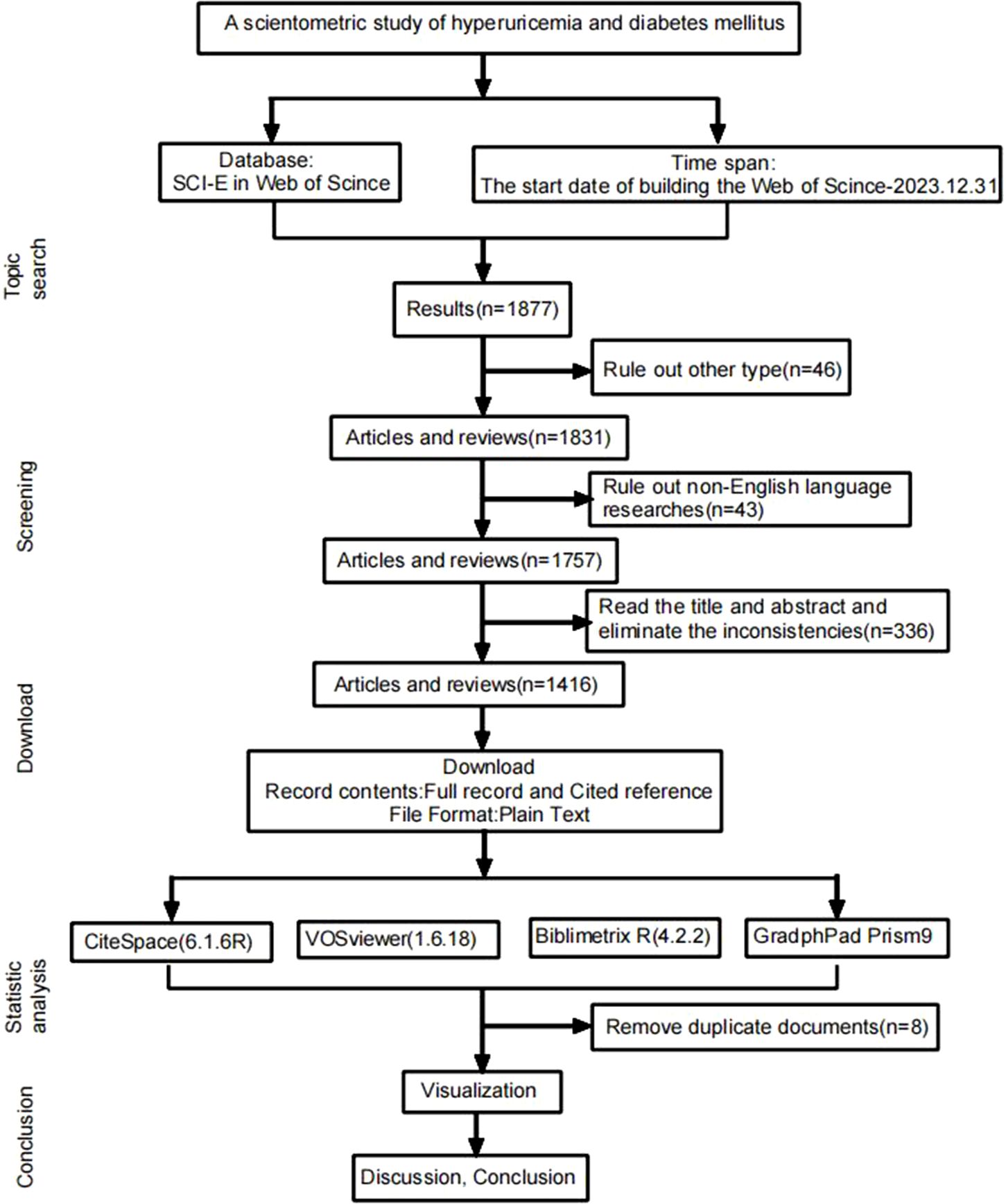
Figure 1. Document retrieval diagram.
This study utilized the Biblimetrix R package (version 4.2.2) to gather essential data on national publishing networks and trending subjects. VOSviewer (version 1.6.18) facilitated the analysis of authors, research institutions, and national cooperative networks. CiteSpace (version 6.3.R1) analyzed word frequency, co-occurrence, and clusters for keywords, as well as co-citation for highly cited studies. Cluster analysis was weighted by the Log-likelihood rate algorithm. The time slice was set to one year, cosine measures correlation strength, and Top N = 50 was the selection threshold. Key nodes have centrality (C) greater than 0.1. Module value Q and network profile value S are essential parameters for measuring clustering structure rationality, with Q > 0.3 indicating significance. Each cluster was reviewed, and the automated labels were modified by the author if needed.
Figure 2 illustrates the annual publication trend, indicating a steady increase despite some fluctuations. The peak was in 2021, with 170 publications, underscoring the increasing global interest in research related to HUA and diabetes.
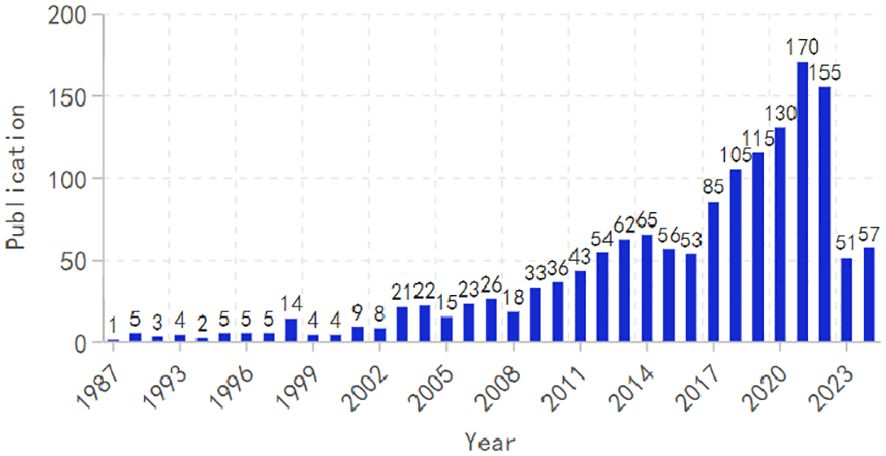
Figure 2. Annual publication trend chart.
The study’s lead authors were Johnson, Richare J (41 publications), Lanaspa, Miguel A (19), and Kuwabara, Masanari (18). Bjornstad, Krishnan, and Kanbay, with 11 publications, have similar citation levels, highlighting their significant impact (Table 1). Visual analysis reveals extensive collaboration among authors (Figure 3).
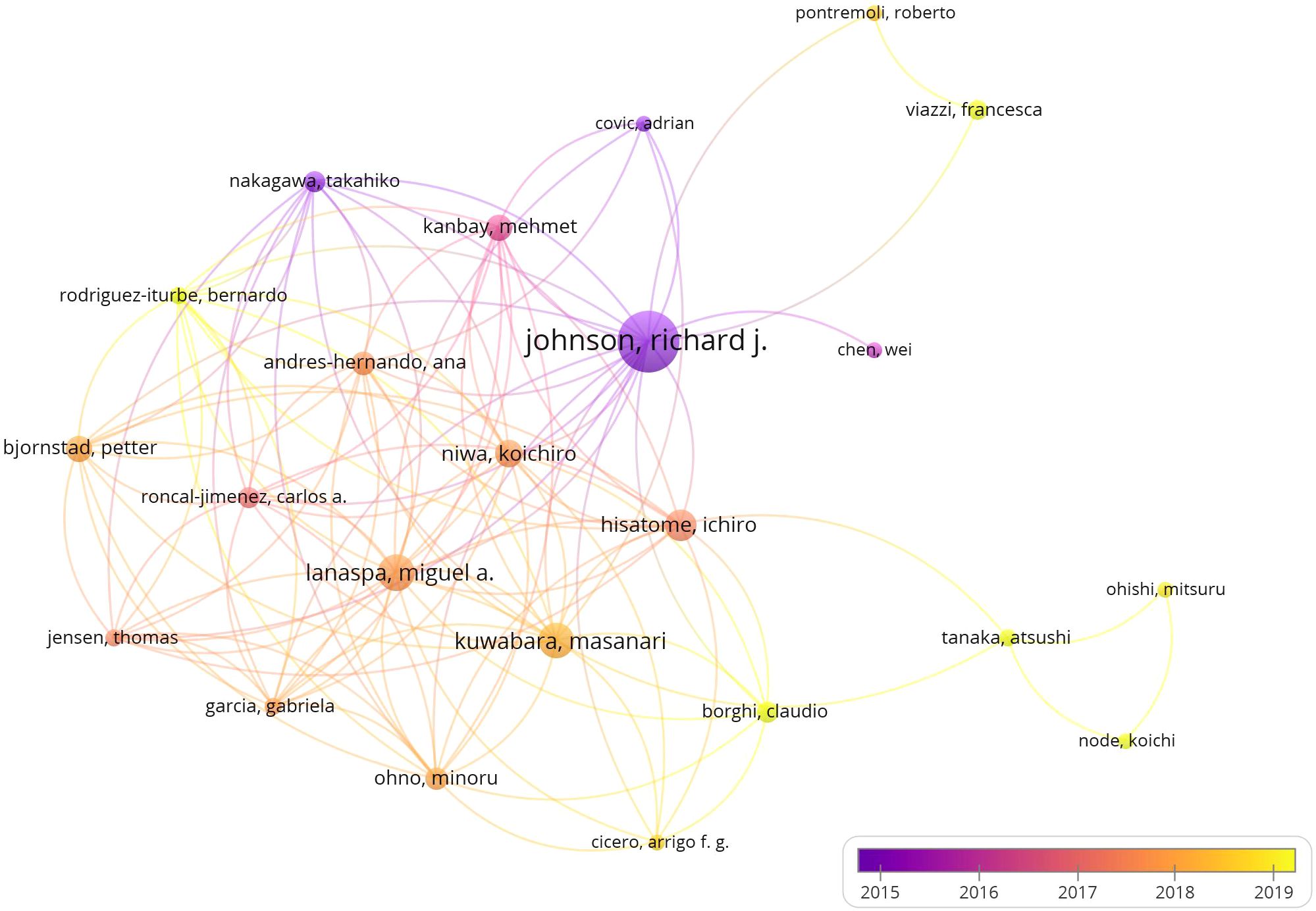
Figure 3. Author cooperation network diagram.
The study found that China (n = 433), the United States (US) (n = 259), and Japan (n = 202) led in article publications. Although the US published fewer articles than China, it exhibits higher citation counts, suggesting superior research quality (Table 2). Visual analysis indicated active international cooperation, except for Egypt, Saudi Arabia, South Africa, and Malaysia (Figures 4A, B).
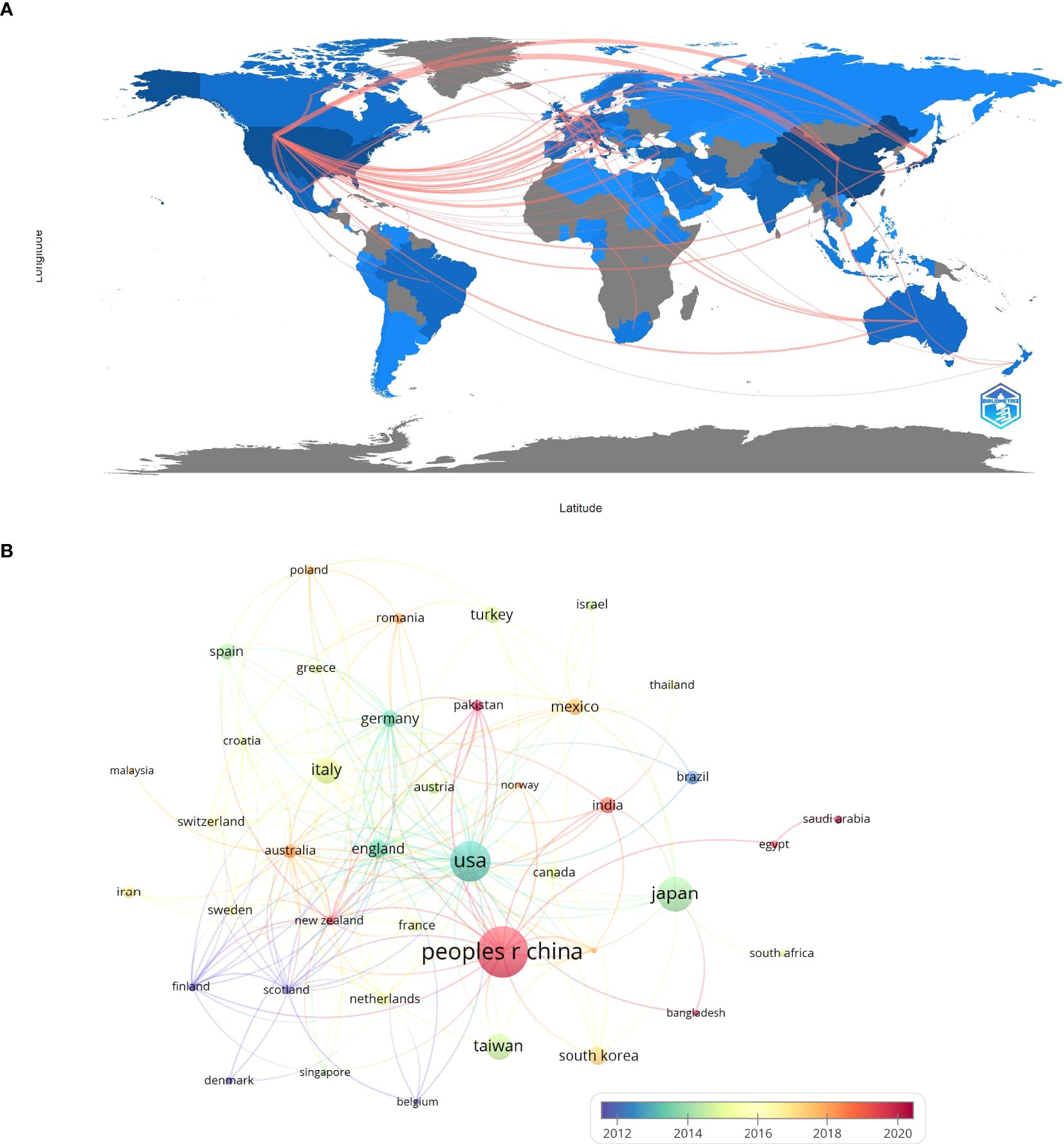
Figure 4. (A) Country collaboration map. (B) National cooperation network diagram.
The study revealed that China Medical University (n = 36), Shanghai Jiao Tong University (n = 33), and Capital Medical University (n = 31) were top in article publications. The University of Colorado excelled with 2,225 citations indicating robust research activity (Table 3), while visual analysis indicated significant organizational collaboration (Figure 5).
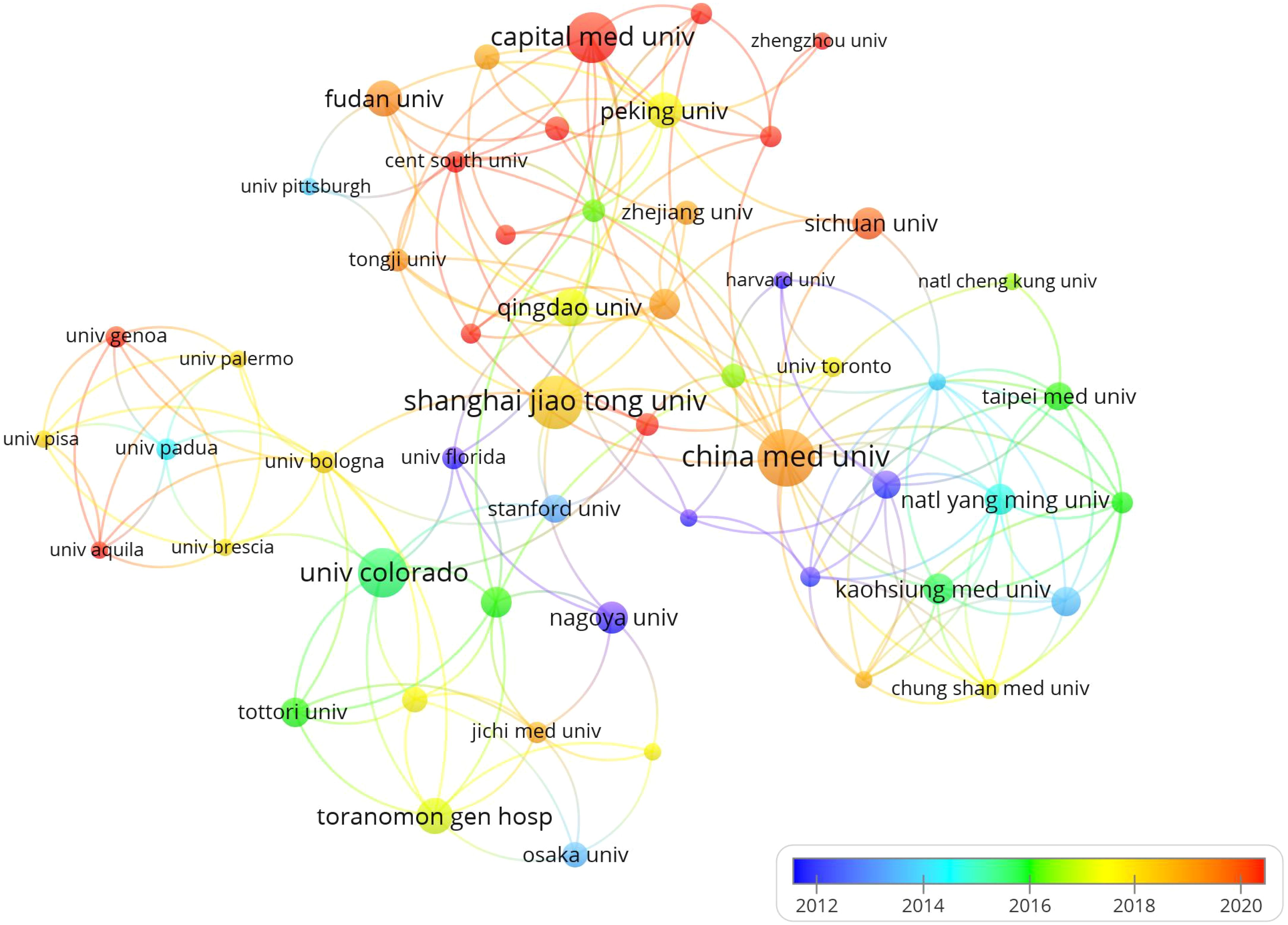
Figure 5. Organizational cooperation network diagram.
Table 1 reveals that the highest publication volumes were from Nutrition Metabolism and Cardiovascular Diseases (CVDs), PLOS One, and Scientific Reports. Supplementary Figure 1 highlights collaborative solid relationships among these journals. The most cited journals were Diabetes Care, Hypertension, and the New England Journal of Medicine (Table 2), with visual analysis indicating a strong co-citation correlation (Supplementary Figure 2). The journal’s dual map demonstrated citation links with co-citation journals, forming clusters on both sides. The green path highlighted the main reference route, indicating that Medlane, Medical, and Clinical journals mainly cite Molecular Biology, Genetics, Health, and Nursing (Figure 6).
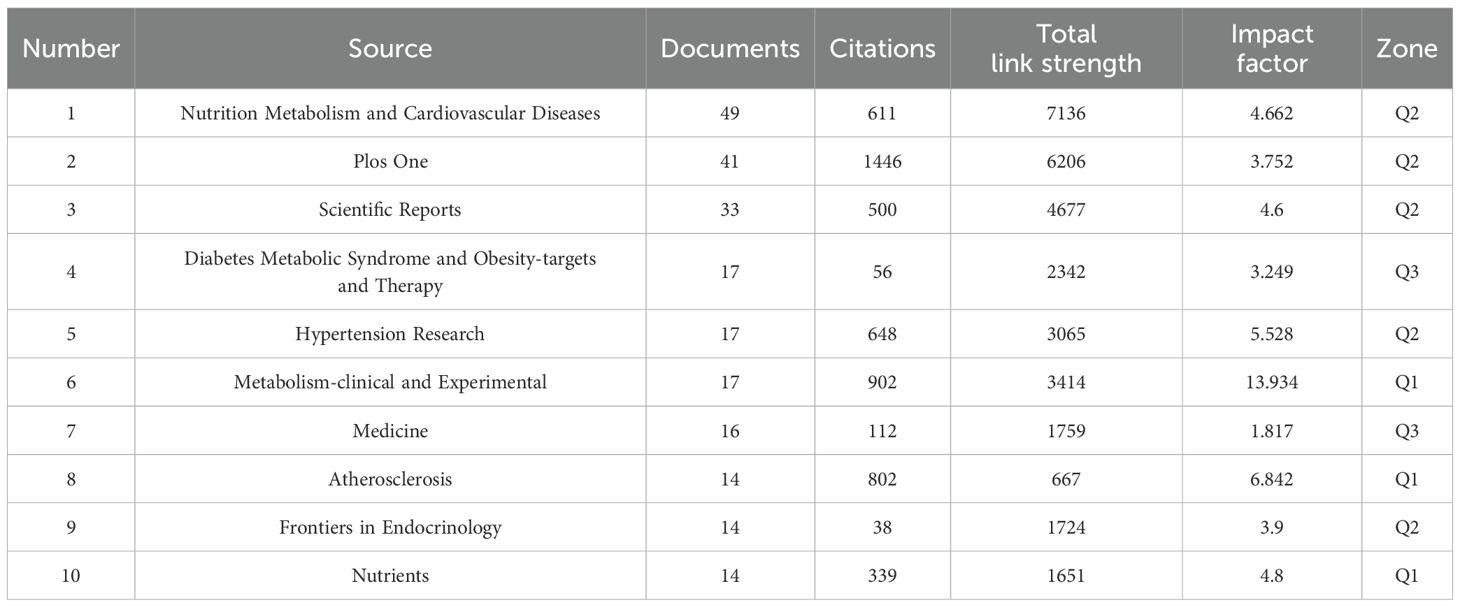
Table 1. Top 10 journals by publication volume.
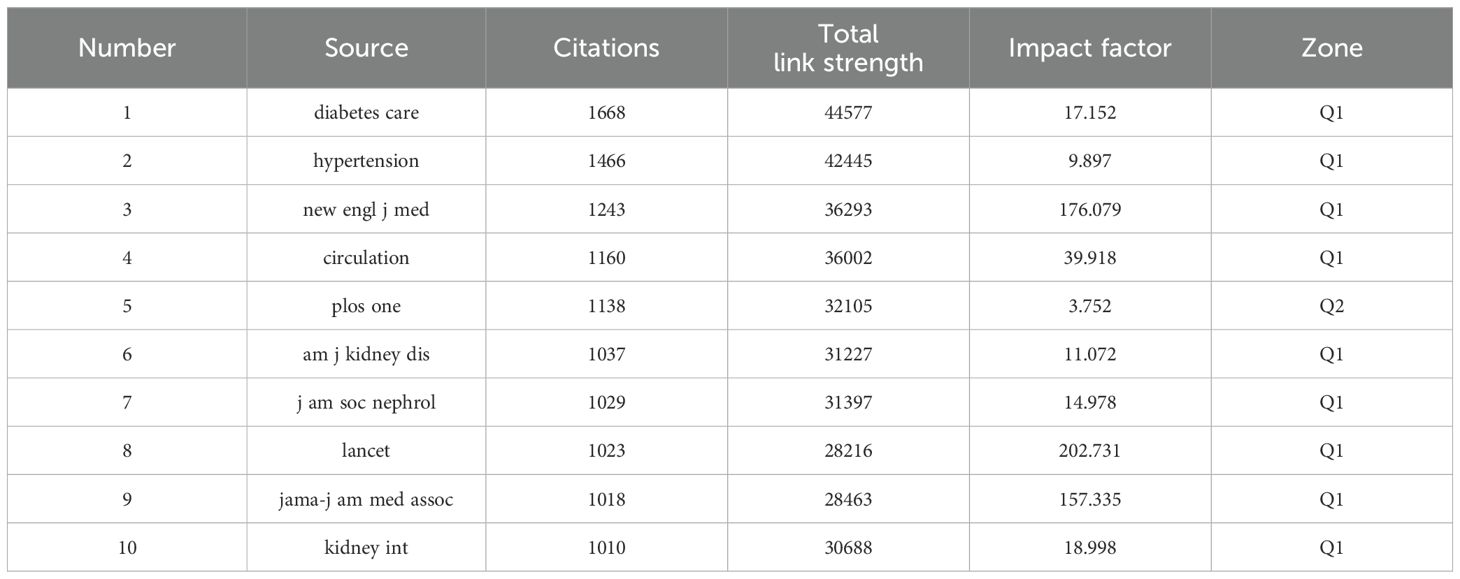
Table 2. The 10 most cited journals.
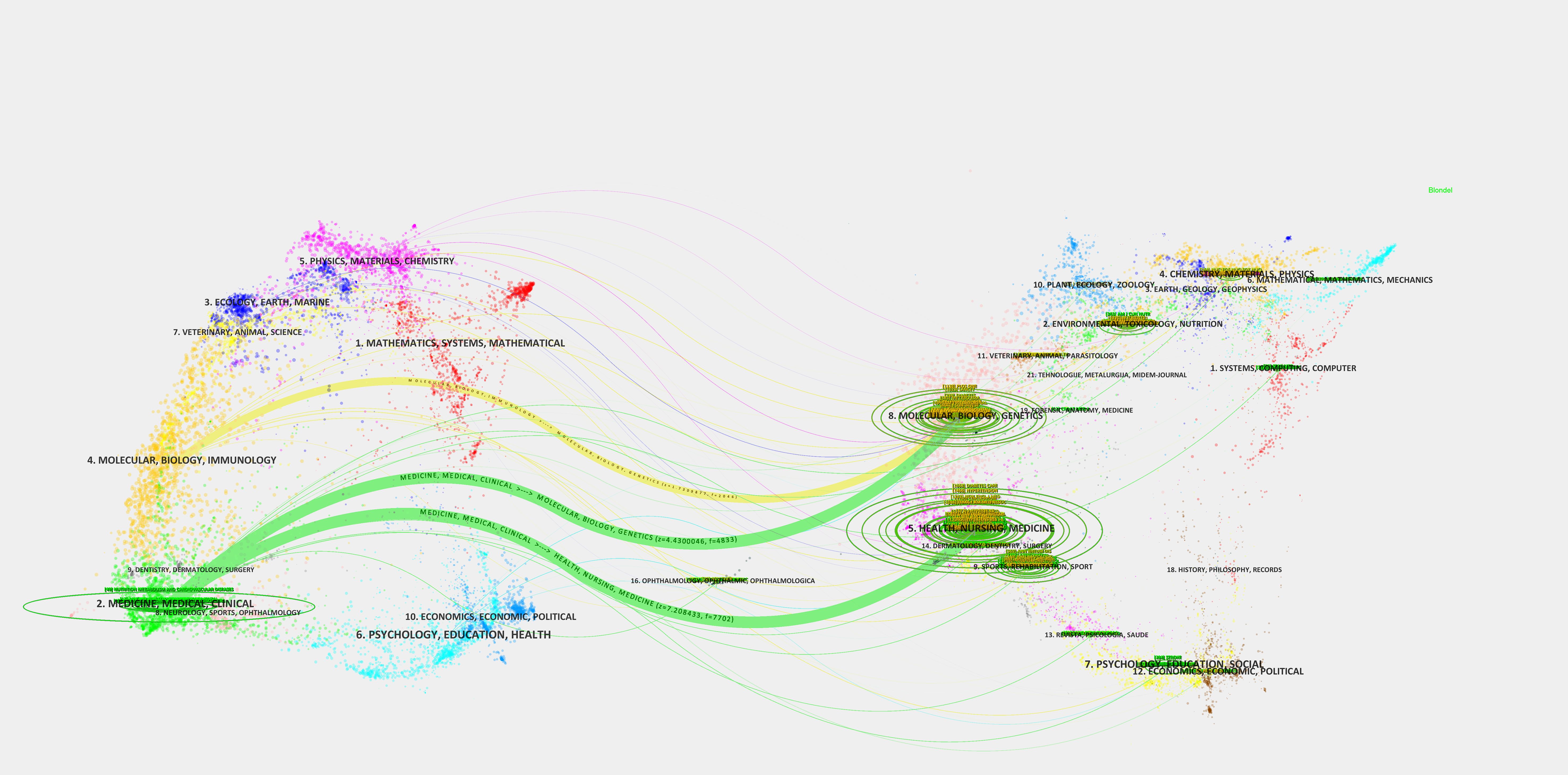
Figure 6. Journal’s dual map.
Figures 7, 8 display 19 clusters emphasizing key research domains in HUA and diabetes, including metabolic syndrome, hypertension, CVD, and chronic kidney disease (CKD) (Q = 0.8152, S = 0.9042). Each cluster included a profile score, size, average publication year, and key references.
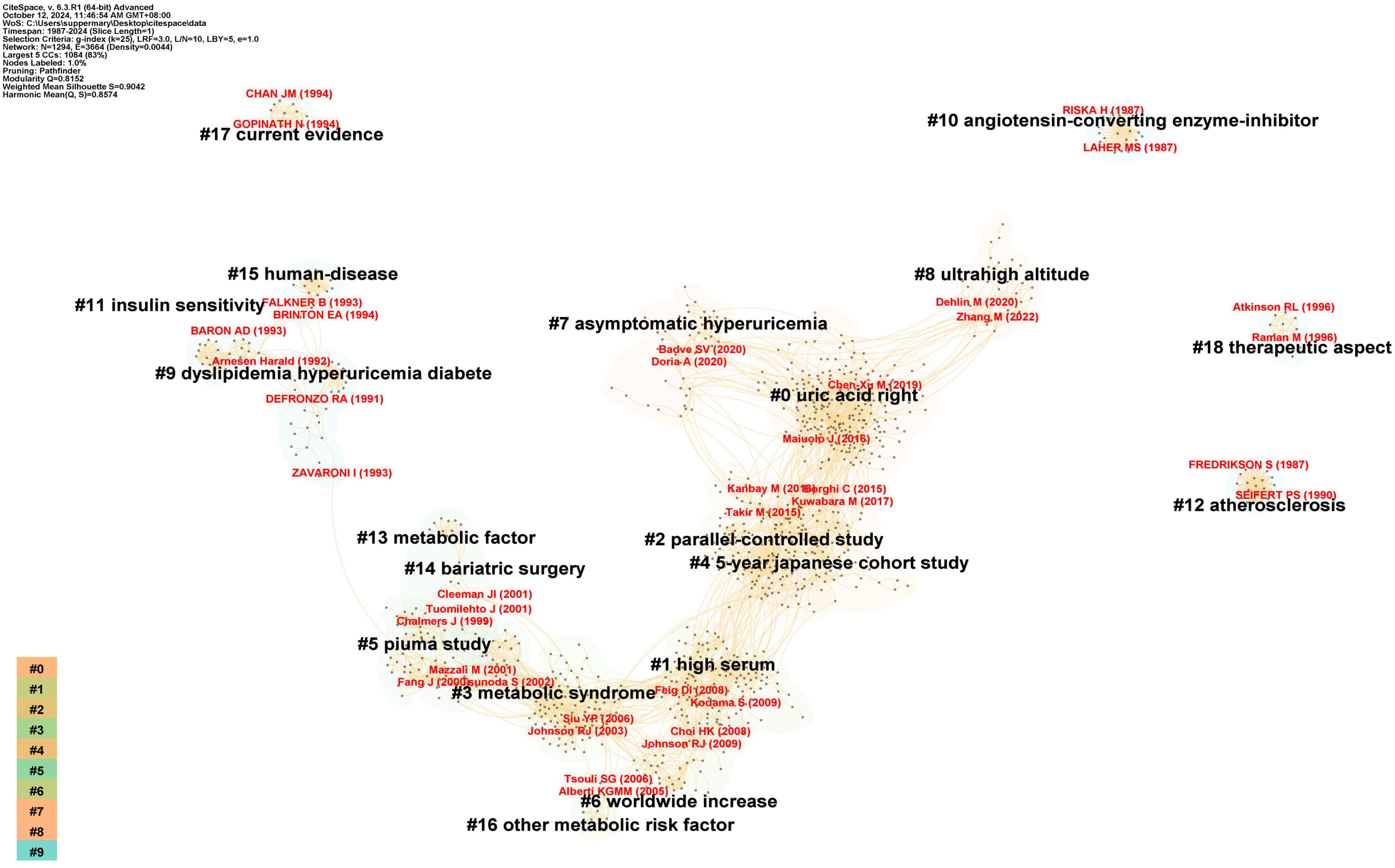
Figure 7. Co-citation references cluster analysis diagram.
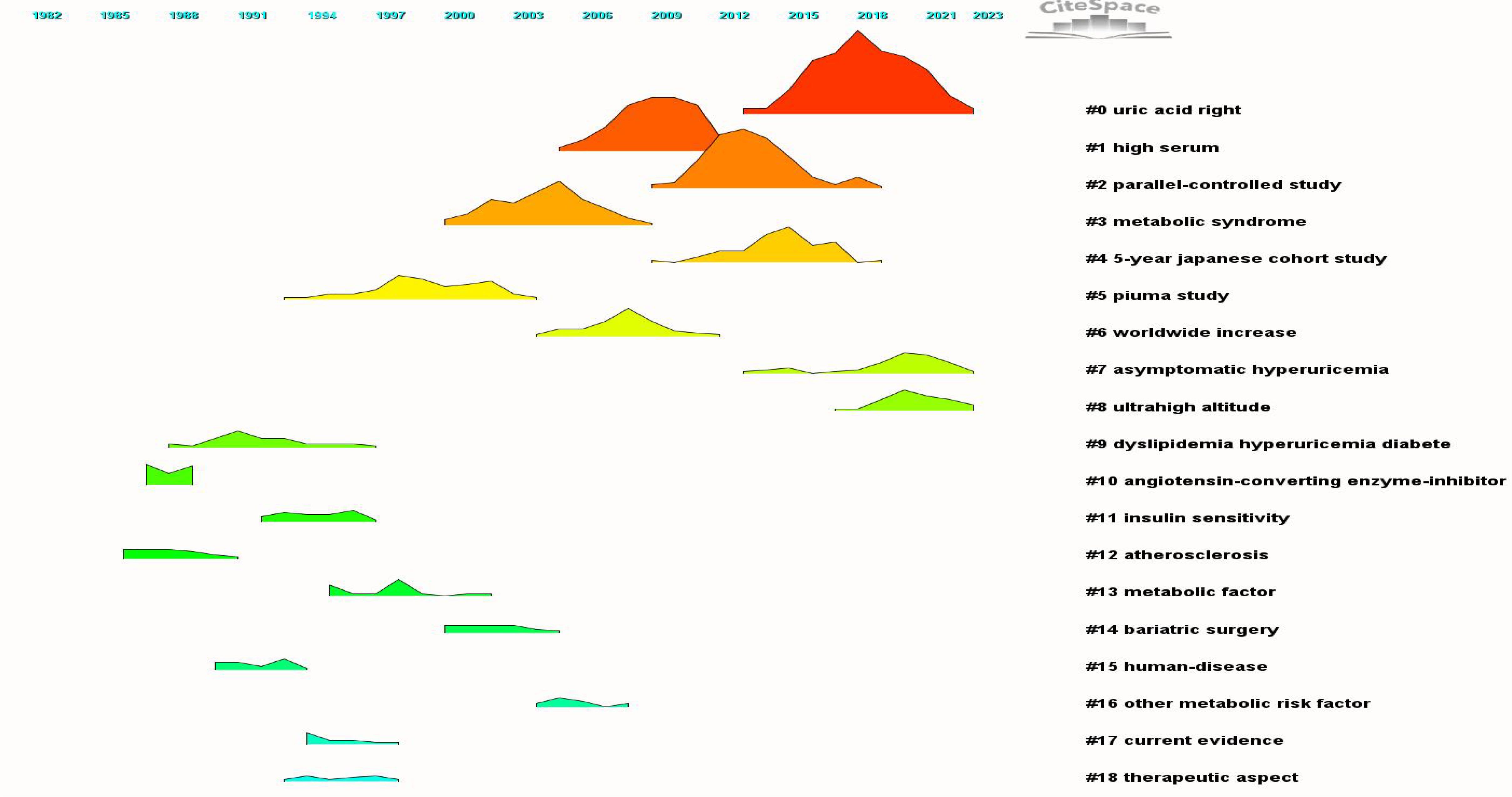
Figure 8. Co-citation references clustering peaks map.
Between 1991 and 1994, pioneering research on “metabolic syndrome” delineated three distinct clusters: cluster #9, designated as “Dyslipidemia, HUA, and DM” (S = 0.918; 34; 1991) (20), cluster #11, labeled “Insulin sensitivity” (S = 0.995; 23; 1994) (21), and cluster #15, termed “Human Diseases” (S = 0.976; 17; 1991) (22). Over time, this research trajectory has progressed, culminating in the identification of additional clusters, including “metabolic factors” in cluster #13 (S = 0.991; 20; 1997) (23), “Other metabolic risk factors” in cluster #16 (S = 0.984; 12; 2005) (24), “Metabolic syndrome” in cluster #3 (S = 0.894; 105; 2004) (25), and ongoing developments such as cluster #6 “worldwide increase” (S = 0.944; 46; 2007) (26).
In 2001, research pertaining to the pathology of uric acid gained significant prominence, as evidenced by the evolution of cluster #5, designated as the “PIUMA Study” (S = 0.948; 66; 1999) (27), into cluster #1, referred to as “High Serum” (S = 0.893; 143; 2009) (28). This progression ultimately culminated in establishing cluster #0, which emerged as the most significant cluster within the network dedicated to the study of uric acid (S = 0.802; 228; 2018) (29).
A third research area emerged from cluster #12, “Atherosclerosis” (S = 1; 22; 1997) (30), and evolved into cluster #4, “5-YEAR JAPANESE COHORT STUDY” (S = 0.897; 140; 2014) (31), which includes chronic kidney and CVDs.
Additionally, we conducted an emergent analysis of co-cited references from 1987 to September 30, 2024 (Figure 9). The analysis revealed that the three most recent and significant references on flare-ups were Chen-Xu M et al.’s cohort study on gout and HUA prevalence in the US (2007–2016) (32), White, W. B et al.’s study on cardiovascular safety of febuxostat or allopurinol in patients with gout (33), and Maiuolo J et al.’s review on uric acid metabolism regulation (1).
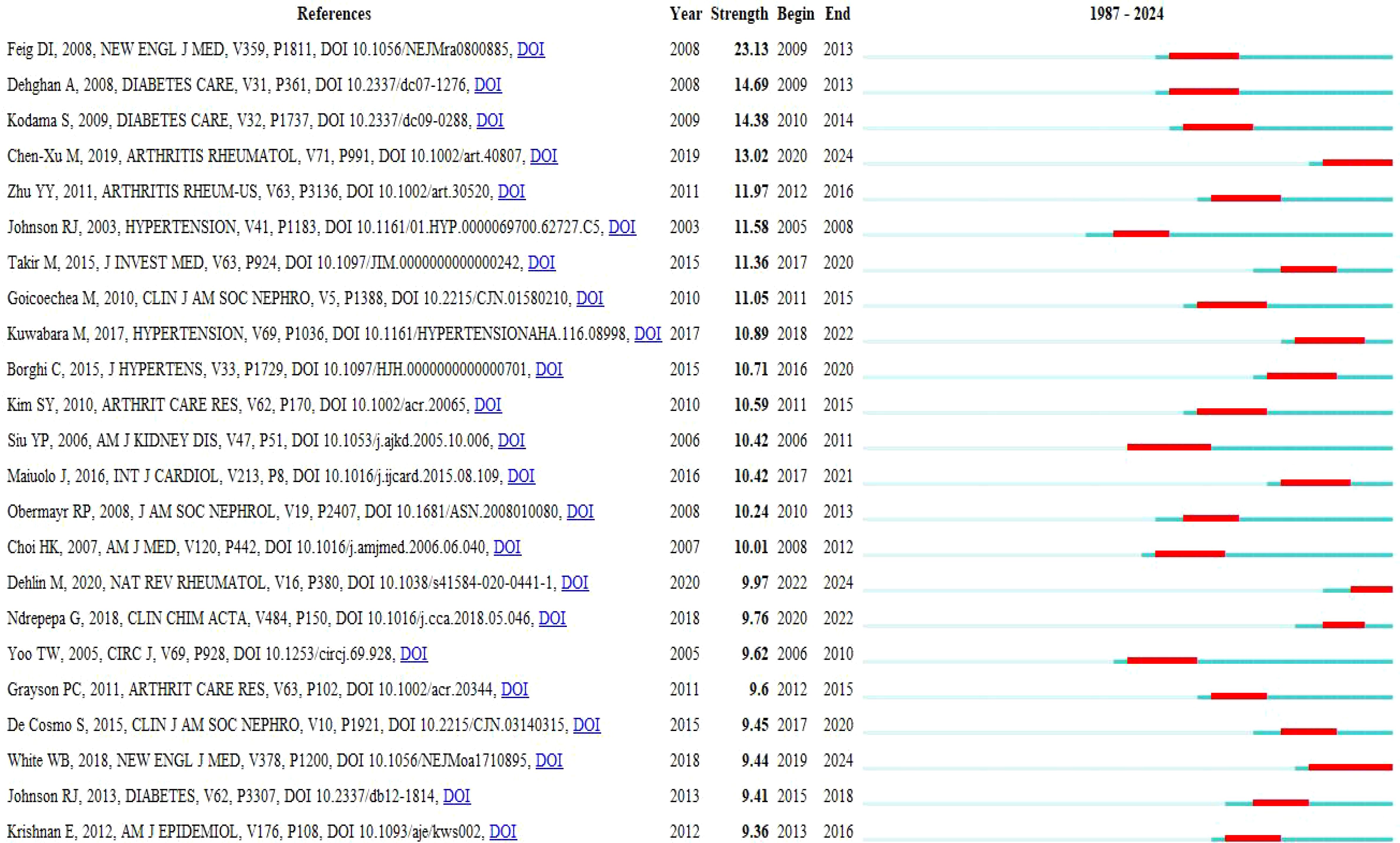
Figure 9. Top 25 references with the strongest citation bursts diagram.
Inter-cluster link detection using network burst dynamics from 1987 to September 30, 2024 (Annex 1).
Table 3 indicates that the 10 most cited references included Feig DI et al.’s comprehensive analysis of the biological function of uric acid and the specific mechanism of metabolic syndrome induced by HUA (34). Chen-Xu M et al.’s cohort study on gout and HUA prevalence in the US (2007–2016) (32), and Kuwabara M et al.’s cohort study examined the association between asymptomatic HUA and cardiometabolic diseases (35).
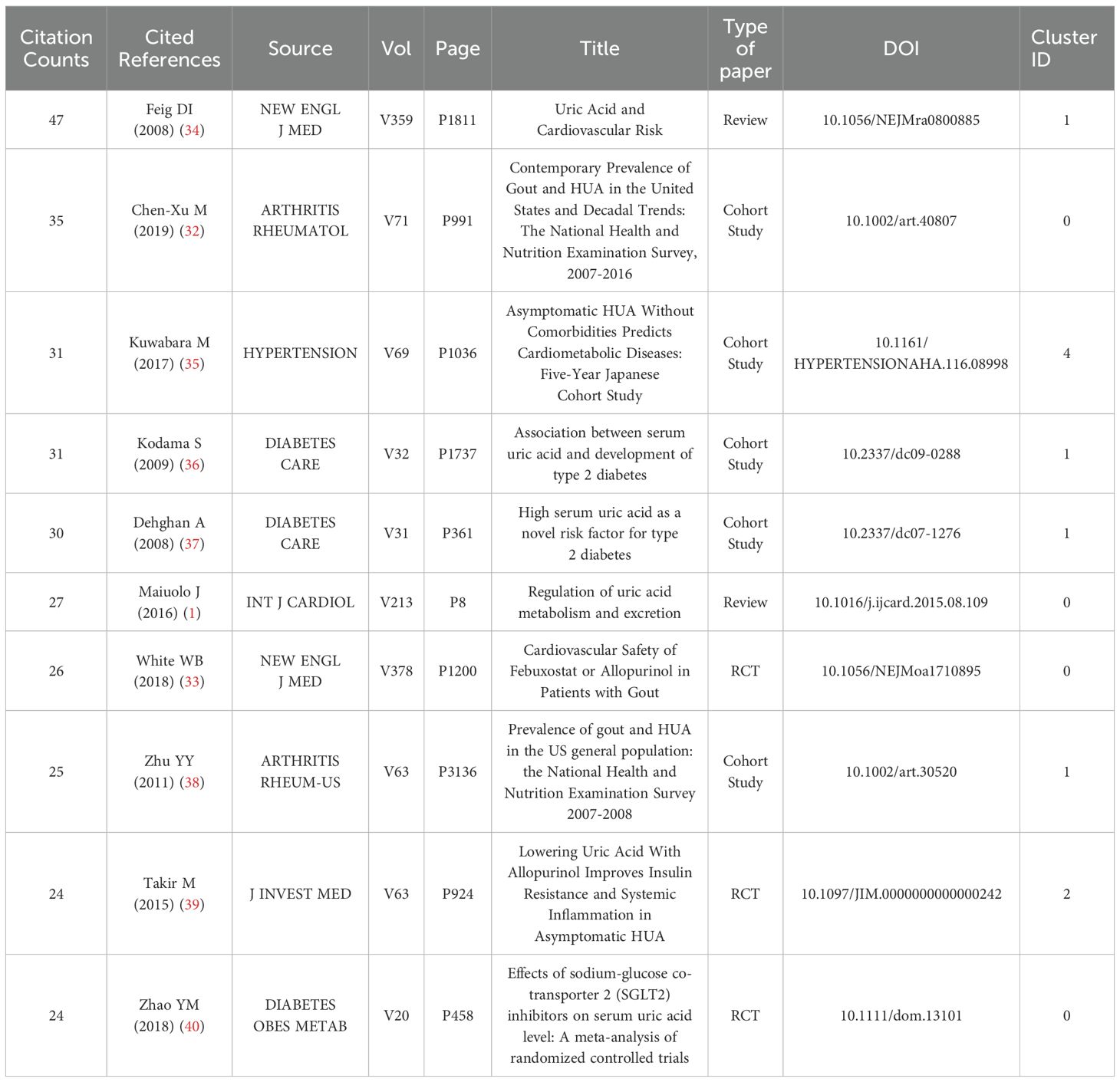
Table 3. The 10 most cited references.
Keyword frequency was crucial for identifying research trends and choosing search terms for literature reviews. The network diagram indicated that apart from “HUA,” “serum uric acid,” and “diabetes,” the most common terms were metabolic syndrome, hypertension, insulin resistance, CVD, and CKD (Figure 10).
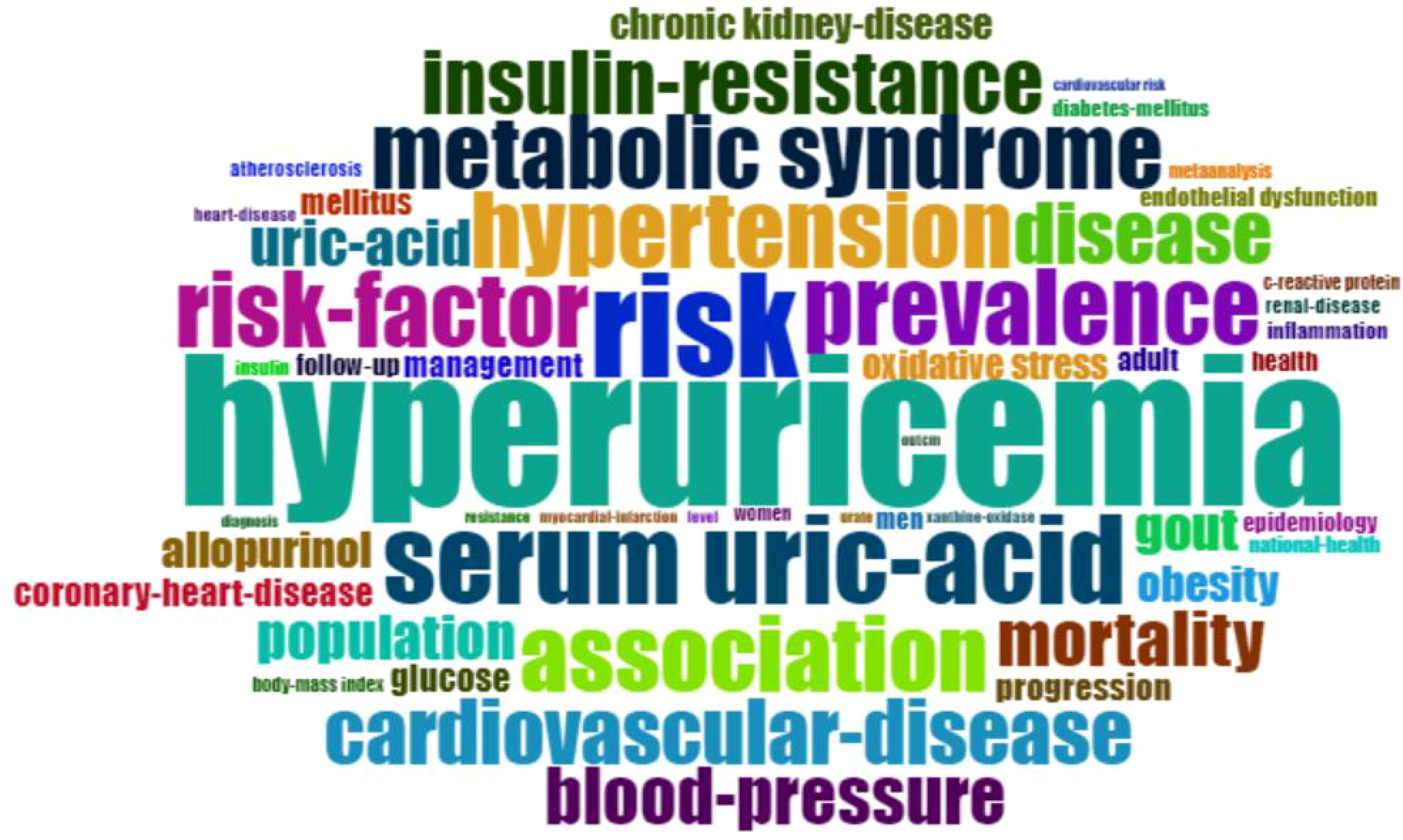
Figure 10. Keywords word cloud diagram.
The peak map identifies nine distinct clusters after re-labeling the automatic labels from the keyword cluster analysis: “ Sodium-dependent glucose transporter 2 (SGLT-2) inhibition,” “C-reactive protein (CRP),” “CKD,” “inhibition,” “antioxidant activity,” “febuxostat,” “insulin resistance,” “glucagon-like peptide-1 receptor agonists,” “inflammation,” and “endothelial dysfunction.” The network exhibits strong clustering and modularity (Q = 0.4258, S = 0.711; Figure 11). An analysis of trending topics over the past five years revealed research focus on the pathogenesis of HUA, DM, and associated conditions such as triglyceride-glucose index, diabetic nephropathy, inflammation, and heart failure (Figure 12). The top 25 co-cited keywords were identified through emergent analysis, with recent citation bursts highlighting terms such as “nutrition examination survey,” “impact,” “genome-wide association,” and “mechanism” (Figure 13).
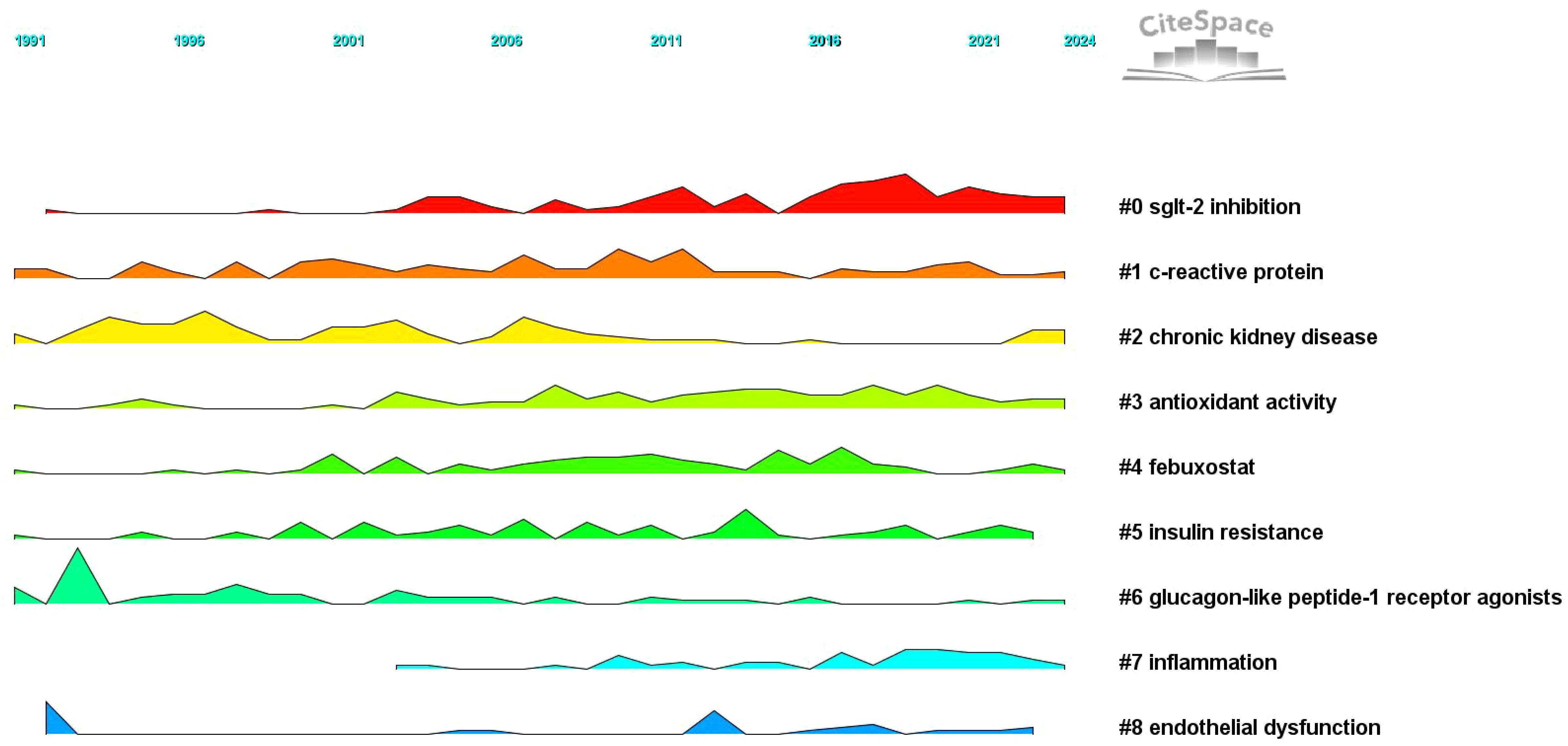
Figure 11. Keyword clustering peaks map.
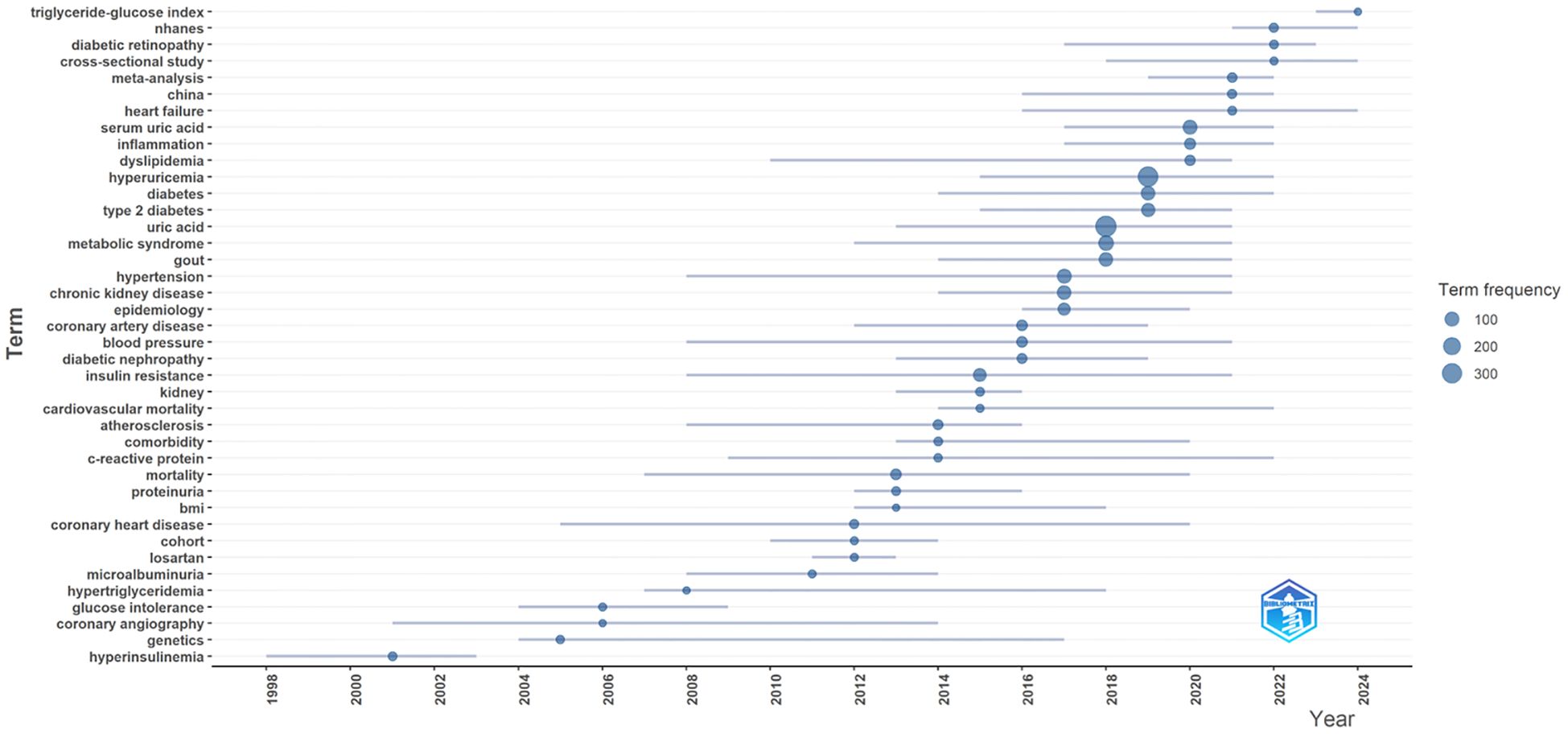
Figure 12. Trend topics diagram.
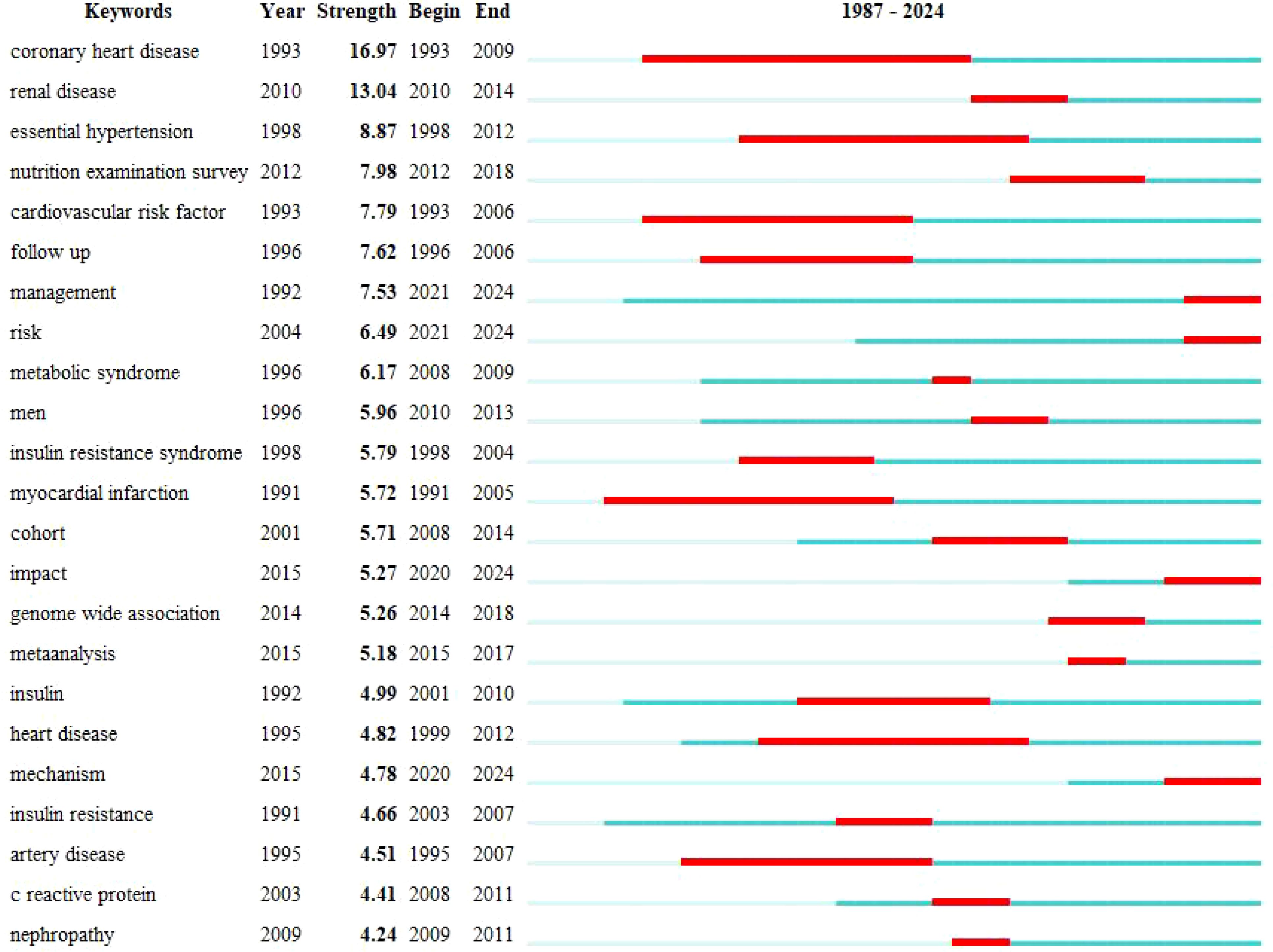
Figure 13. Top 25 keywords with the strongest citation bursts diagram.
This study represents the inaugural comprehensive scientometric analysis of HUA and diabetes. As illustrated in Figure 1, scholarly research on this subject has demonstrated a consistent annual increase since the establishment of the Web of Science Core Collection, with a marked surge in activity from 2017 to 2022, thereby attracting substantial academic interest. The collaborative network analysis revealed robust partnerships among authors, institutions, and countries, with Johnson emerging as a significant contributor. The US was at the forefront in terms of research quality and international impact. Furthermore, it is noteworthy that 70% of the research originated from Chinese universities. The journal network analysis revealed that among the top 10 journals, “Metabolism-Clinical and Experimental” possesses the highest impact factor at 13.934 (Q1), followed by “Atherosclerosis” with an impact factor of 6.842 (Q1). Although these two journals publish fewer articles than “Nutrition, Metabolism and CVDs, PLOS One, and Scientific Reports,” they are recognized for their exceptional quality and substantial impact in the field. Excluding “PLOS One,” the top 10 journals ranked by total citations were classified as Q1 and acknowledged as high-quality international publications. These journals established robust co-citation networks and significantly contributed to the recognition and advancement of research on HUA and diabetes. The journal’s dual map overlay analysis revealed that articles in Medlane, Medical, and Clinical journals are mainly cited in Molecular, Biology, Genetics, Health, Medlane, and Nursing journals. This indicates that most research on the link between HUA and diabetes is found in clinical journals, with little presence in immunology, molecular, and biological publications. This highlights the need for more fundamental research to understand the precise molecular mechanisms involved.
The findings presented in Table 3 indicate that the 10 most frequently cited articles had laid the foundational framework for research on HUA and diabetes. Chen-Xu et al. (32) reported HUA prevalence rates of 20.2% in adult males and 20.0% in females from 2007 to 2016, while Zhu et al. (38) found an average prevalence of 21.4% before 2008, linked to rising obesity. Both studies highlight an increasing trend of HUA in the US. Feig et al. (34) and Maiuolo et al. (1) studied the biological roles and metabolic syndrome caused by HUA, along with the enzymatic pathways that regulate uric acid. Their work has facilitated further research. Dehghan et al. (37) found that 10.2% of people with high serum uric acid levels were diagnosed with diabetes in a retrospective study. A meta-analysis (35) found that each 1 mg/dL increase in serum uric acid levels is linked to a 17% higher risk of type 2 diabetes, suggesting that uric acid could be a useful predictive marker for the disease and warrants further study. Takir et al. (39) discovered that allopurinol reduces uric acid, improving inflammation and insulin resistance in patients with asymptomatic HUA, but its role in preventing type 2 diabetes remains unclear. Borghi et al. (41) found that lowering serum uric acid through xanthine oxidase inhibitors, such as allopurinol and febuxostat, is the best treatment for cardiovascular and renal diseases. Goicoechea et al. (42) highlighted allopurinol’s benefits in slowing CKD and reducing cardiovascular hospitalization risk. Kuwabara et al. (35) proposed that HUA could be a useful biomarker for predicting cardiometabolic disorders, opening new research opportunities.
Figure 10 demonstrates the frequent occurrence of metabolic syndrome, hypertension, CVD, and CKD in the keyword network analysis, suggesting that diabetes with HUA may increase the risk of these conditions. We then explored the mechanisms behind this, as detailed below.
HUA is recognized as a significant element of metabolic syndrome, which is a critical risk factor for CVD and type 2 diabetes (43). Empirical evidence indicates that elevated uric acid levels in individuals with diabetes may contribute to the onset of metabolic syndrome through multiple mechanisms. Primarily, insulin resistance serves as a crucial connection between diabetes and HUA. Insulin resistance can result in dysregulated glucose metabolism, leading to hyperglycemia, which elevated uric acid levels may further aggravate through their impact on insulin signaling pathways (44). A study found (45) that high uric acid levels are significantly linked to increased body mass index, fasting blood glucose, and insulin resistance (HOMA-IR), suggesting that elevated uric acid may worsen insulin resistance in diabetic patients. Second, inflammatory responses are crucial in linking diabetes, HUA, and metabolic syndrome. Elevated uric acid levels cause chronic low-grade inflammation, closely tied to obesity, diabetes, and CVD. Uric acid acts as a pro-inflammatory agent, activating pathways that impact fat metabolism and insulin signaling (46). For example, studies indicate that high uric acid levels correlate with increased highly sensitive CRP, highlighting a link between inflammation and these diseases (47). This inflammation can negatively impact vascular health and elevate cardiovascular risk in individuals with diabetes.
Moreover, abnormal lipid metabolism links diabetes and HUA, with people with diabetes often indicating high triglycerides and low high-density lipoprotein (HDL) levels. HUA can worsen these lipid abnormalities (48). This changed lipid metabolism raises the risk of CVD and may lead to metabolic syndrome. A study on a Mediterranean population identified low HDL cholesterol (HDL-C) and high blood sugar as independent predictors of HUA (43), indicating their potential combined role in developing metabolic syndrome. Finally, genetic and environmental factors influence the link between diabetes, HUA, and metabolic syndrome. Genetic variants can increase susceptibility, while unhealthy lifestyles heighten these risks (49). Consequently, understanding the diabetes-HUA connection is crucial for preventing and managing metabolic syndrome.
In individuals with diabetes, elevated uric acid levels may influence blood pressure through various mechanisms. Initially, insulin resistance, commonly observed in this population, can result in diminished renal excretion of uric acid, thereby contributing to the development of HUA (50). HUA is an independent risk factor for hypertension, potentially raising blood pressure by causing endothelial dysfunction (51) and activating the renin-angiotensin-aldosterone system (RAAS) (52), both of which lead to blood vessel constriction and sodium retention. Moreover, diabetes-related chronic inflammation can worsen hypertension by encouraging vascular cell growth and arteriosclerosis (53). HUA, a pro-inflammatory factor, exacerbates this by triggering inflammation in vascular cells, impairing blood vessel dilation (54).
Subsequently, people with diabetes frequently experience obesity and metabolic syndrome, which worsen the link between HUA and hypertension. Obesity promotes the release of pro-inflammatory factors from adipose tissue, worsening insulin resistance and HUA (45). It also raises blood volume, contributing to higher blood pressure (55). For instance, individuals with diabetes often have elevated triglycerides and low HDL-C, both of which are closely associated with increased blood pressure. In diabetic patients, HUA may be linked to kidney ultrafiltration. Early-stage diabetes can cause renal tubule hyperfiltration, reducing the kidney’s ability to excrete uric acid and worsening HUA (56). This kidney function change can also contribute to hypertension.
The coexistence of CKD and CVD increases mortality risk and negatively affects quality of life. Research indicates that high uric acid levels are closely linked to metabolic syndrome conditions such as obesity, hypertension, and diabetes, which are independent risk factors for CKD and CVD (57). First, the inflammatory response significantly contributes to disease development. HUA is an independent risk factor for CVD and CKD, potentially worsening renal and cardiovascular damage in people with diabetes by activating the RASS, inhibiting nitric oxide synthesis, and promoting vascular lesions (58). Besides, inflammation may increase cardiovascular risk by causing endothelial dysfunction and speeding up atherosclerosis (59). In diabetic individuals, an increased inflammatory response combined with HUA significantly raises the risk of CKD. A study revealed that diabetic patients with both HUA and hypertension faced a 5.42 times higher risk of CKD compared to those with just one of these conditions (60). Inflammatory mediators such as tumor necrosis factor-alpha (TNF-α) and interleukin 6 (IL-6) are frequently elevated in diabetes and HUA, promoting inflammation and linking to insulin resistance and metabolic syndrome (61). They can also damage the heart and kidneys by triggering pro-inflammatory pathways, raising the risk of heart failure and CKD (62). Inflammation also impairs renal tubule function, causing cell apoptosis and fibrosis, which speeds up CKD progression (63).
Overall, the interplay of inflammation, uric acid, and blood pressure is crucial for cardiovascular and kidney health in people with diabetes. Second, insulin resistance can notably raise the risk of cardiovascular and CKD in diabetic and hyperuricemic patients through various mechanisms. For example, insulin resistance boosts 11β-hydroxy steroid dehydrogenase 1 in the liver, enhancing glucocorticoid activity and worsening insulin resistance. This results in increased glucose production and fat formation, aggravating metabolic disorders (64), including hyperglycemia and hyperlipidemia, and becoming a significant risk factor for CVD (65). Moreover, research indicates that insulin resistance can exacerbate HUA by boosting uric acid production and decreasing its excretion (66). It also causes endothelial dysfunction, oxidative stress, and inflammation, contributing to CVD and kidney damage (66). High uric acid levels in patients with CKD can worsen heart remodeling and fibrosis, increasing cardiovascular risk (67). Therefore, the combination of insulin resistance and HUA may significantly heighten the risk of cardiovascular and CKDs. Finally, oxidative stress plays a crucial role in increasing the risk of cardiovascular and CKDs in patients with diabetes and HUA. It triggers the release of inflammatory mediators, leading to chronic inflammation, which is closely linked to the development and progression of these diseases (68). High uric acid levels can increase oxidative stress and cause cell damage, particularly in diabetic patients (69).
Similarly, people with diabetes often have elevated inflammatory factors such as TNF-α and IL-6, which harm the vascular endothelium and promote atherosclerosis (70). In HUA, uric acid buildup causes oxidative stress in kidney cells, leading to cell death and kidney damage, which can impair kidney function and heighten CVD risk (71). Oxidative stress also encourages vascular smooth muscle cell growth and movement, contributing to vascular remodeling and atherosclerosis, especially in diabetic patients with HUA, increasing cardiovascular events (72). Oxidative stress is closely linked to metabolic syndrome, such as insulin resistance and lipid issues, which elevate the risk of cardiovascular and CKDs (58). In summary, inflammation, insulin resistance, and oxidative stress may increase the risk of cardiovascular and CKDs in diabetic patients with HUA.
Figures 11–13 illustrate that research concerning the relationship between diabetes and HUA was increasingly directed towards elucidating the underlying mechanisms and investigating pharmacological interventions. Subsequently, this study examines the pathological mechanisms that connect HUA and diabetes and evaluates effective therapeutic agents.
Numerous studies have clarified the link between uric acid and insulin resistance. Wan X et al. (73) found that uric acid activates the NOD-like receptor protein 3 (NLRP3) inflammasome, leading to liver fat accumulation and insulin resistance, while inhibiting NLRP3 reduced these effects. Yu W et al. (74) reviewed how soluble uric acid induces insulin resistance in different tissues, suggesting a new treatment target for HUA-induced insulin resistance in 2023. A recent study indicates that HOMA2 IR-CP more effectively assesses the link between insulin resistance and uric acid levels (75). Insulin resistance contributes to type 2 diabetes through oxidative stress, mitochondrial dysfunction, lipid accumulation, and inflammation, involving increased insulin receptor substrate (IRS) protein phosphorylation, IRS-1 degradation through the mammalian target of rapamycin (mTOR) pathway, reduced activation of signaling molecules such as phosphatidylinositol 3-kinase and protein kinase B (AKT), and heightened activity of phosphatases such as protein Tyrosine Phosphatases (PTPs), phosphatase and Tensin Homolog (PTEN), and protein Phosphatase 2A (PP2A). A study on mice found that high uric acid levels can speed up diabetes onset by damaging islet cells, indirectly causing the disease (76). This suggests a strong connection between diabetes and HUA due to insulin resistance impacting glucose uptake and uric acid excretion.
A 2020 study discovered that asymptomatic high uric acid levels can lead to diabetes by causing inflammation through urate crystals (77). Recent research indicates that soluble uric acid can change cell structure and pH, increasing inflammation and neutrophil activity (75). The studies suggest that soluble uric acid may contribute to inflammation in HUA and diabetes, providing insights into their mechanisms. Elevated HUA levels can trigger inflammation and impair glucose metabolism through pathways such as nuclear factor kappa B (NF-κB) and NLRP3. A mouse study indicated that high HUA levels may cause insulin resistance and decreased insulin secretion, potentially leading to type 2 diabetes (78). Uric acid’s inflammatory nature may drive this effect, as indicated by higher TNF-α levels and enzyme activation post-infusion. High uric acid levels can trigger pathways such as NF-κB and NLRP3 inflammasome, leading to inflammation and endothelial cell damage. This inflammation impacts blood vessels and insulin receptors, particularly in obese diabetic patients. Furthermore, inflammatory cells in fat tissue release cytokines, causing oxidative stress, inflammation, and increased HUA.
Oxidative stress significantly influences serum uric acid levels by affecting urate production, excretion, and reabsorption (79). High uric acid levels can induce oxidative stress by converting xanthine dehydrogenase (XDH) to xanthine oxidase (XO), activating NADPH oxidases (NOX) and hypoxia-inducible factor-1α (HIF-1α), and inhibiting antioxidant enzymes, resulting in more free radicals and immune cell activation. Additionally, HUA triggers endoplasmic reticulum stress and boosts reactive oxygen species (ROS) production, causing oxidative stress in this protein-synthesizing organelle. This sequence of events boosts free radicals and oxides, causing lipid, protein, and deoxyribonucleic acid oxidation, leading to cell death and inflammation. Indicators of oxidative stress include higher levels of malondialdehyde, peroxynitrosoides, advanced glycation end products, and lower superoxide dismutase (80), which can damage beta cells, induce insulin resistance, and speed up diabetes progression. Studies have indicated that diabetic hyperglycemia can generate oxidative stress, raising lipid peroxidation products (31). This may reduce the number or effectiveness of intracellular insulin receptors, interfere with insulin signaling, and impair the insulin pathway. Consequently, insulin signaling weakens, antioxidant capacity decreases, and ROS production rises during uric acid synthesis, leading to elevated uric acid levels. These studies indicate that people with high uric acid levels and diabetes are more susceptible to oxidative stress, suggesting new treatment approaches for managing uric acid and enhancing health and quality of life.
The kidney is crucial in HUA and diabetes development, with uric acid influencing factors that lead to kidney damage. The study found that uric acid increases growth factor production and activators while reducing nitric oxide synthesis and endothelial cell growth (81). Elevated HUA levels can induce insulin resistance impacting insulin receptors, signaling pathways, and glucose transporter protein 4 (GLUT4) expression, potentially causing kidney damage and increasing diabetes risk. Diabetic hyperglycemia worsens this by enhancing protein binding to uric acid and reducing its excretion, raising blood uric acid levels. Recent research suggests that uric acid can harm kidneys by causing inflammation, endothelial dysfunction, and overactivating the renin-angiotensin-aldosterone system (RASS), worsening HUA and diabetes (82). Patients should manage blood sugar, reduce uric acid, and address oxidative stress and inflammation to protect kidney health and prevent complications.
Research indicates a link between HUA and glycolipid metabolism issues (83), highlighting the need for careful monitoring in high-risk groups to prevent HUA. HUA influences genes related to glucose and lipid metabolism, insulin signaling, and fat cell differentiation in mouse adipocytes (84). This can cause insulin resistance, cellular damage, and the onset of HUA and diabetes. Conversely, HUA can impact liver lipid metabolism by causing hepatic steatosis and disrupting fatty acid metabolism, leading to increased fatty acid synthesis, reduced oxidation, abnormal lipid metabolism, and insulin resistance. Consequently, compromised insulin sensitivity worsens diabetes progression. Both hyperglycemia and hyperlipidemia contribute to beta cell dysfunction in newly diagnosed patients with type 2 diabetes, and either condition can independently increase insulin resistance (85). In diabetes, high blood glucose from insulin resistance or inadequate insulin can increase liver gluconeogenesis and disrupt lipid metabolism, causing oxidative stress and inflammation, which may lead to HUA. Small molecule inhibitors targeting fatty acid synthase have been indicated to enhance liver function, reduce inflammation, and lower oxidative stress in obese mice on a high-sugar diet (86). Consequently, high glucose levels can increase fatty acid production, leading to their accumulation and impacting uric acid synthesis and excretion. Diabetic patients should manage blood sugar and lipids to lower HUA risk.
Research reveals that HUA levels entering rat islet beta cells through the organic anion transporter increase oxidative stress and activate mitogen-activated protein kinase signaling, hindering cell proliferation (87). High uric acid levels can cause insulin resistance in islet beta cells by raising ROS and disrupting the IRS2/AKT pathway (88). Furthermore, the PPAR-γ-Pck1-mTOR pathway might play a role in islet cell apoptosis due to high uric acid (89). HUA can cause insulin resistance in both lab and living organisms by inhibiting insulin receptor substrate activity through retinol-binding protein 4 (90). Consequently, HUA levels may lead to islet cell death, decreasing insulin production and possibly causing diabetes.
SGLT-2 inhibitors, kidney proteins that reabsorb glucose and sodium, have been demonstrated to be effective in reducing the need for HUA and gout treatment, according to a JAMA Cardiology study on daglizin (91). The Food and Drug Administration and European Medicines Agency have approved three oral SGLT2 regimens for type 2 diabetes and CKD patients with estimated glomerular filtration rate > 30 mL/min/1.72 m², enhancing health markers (92). SGLT2 inhibitors manage diabetes by preventing glucose reabsorption in the kidneys, thus lowering blood sugar. They may also reduce uric acid levels, particularly in diabetic patients with chronic conditions (93). These inhibitors boost glucose and ketone production, increase red blood cell count, lower uric acid, and reduce heart failure and kidney issues. By inhibiting SGLT2, they raise intracavicular glucose, which competes with uric acid reabsorption u GLUT9b (94). SGLT2 inhibitors may help lower anti-inflammatory, antioxidant, and antifibrotic markers (95). They reduce blood uric acid by promoting urinary D-glucose excretion, altering renal tubule uric acid transport (96). Additionally, they improve endothelial function and decrease inflammation in the liver and fat tissue (97). Their studies indicate that SGLT-2 inhibitors can reduce inflammation, alleviate symptoms of HUA and diabetes, and lower uric acid levels by improving endothelial function and suppressing inflammation. They enhance glucose and uric acid excretion, reducing uric acid buildup in the blood. This mechanism involves an increase in glomerular filtration rate due to SGLT-2 inhibitors and reduced uric acid reabsorption in the collecting ducts through GLUT9, leading to lower blood sugar and uric acid levels by replacing glucose reabsorption (98). A meta-analysis found that SGLT-2 inhibitors promote fat oxidation and weight loss, potentially improving HUA and diabetes symptoms (99). Overall, SGLT-2 inhibitors effectively reduce blood glucose levels, decrease uric acid concentrations, lower blood pressure, and facilitate weight loss, thereby potentially contributing to a reduction in uric acid levels in patients.
GLP-1RA effectively manages HUA in diabetic patients by reducing appetite and promoting weight loss. It modulates the vagal nerve pathway to decrease food intake, leading to lower blood sugar and uric acid levels (100). Recent studies have found that AWRK6 is a new GLP-1 receptor agonist that boosts insulin secretion to control blood glucose and energy metabolism using the cAMP-calcium pathway, with minimal toxicity (101). Accordingly, AWRK6 indicates promise as a diabetes treatment. Pechenov et al. (102) revealed that combining sodium deoxycholic acid and propyl gallate in MEDI7219 tablets effectively reduces food intake, body weight, and glucose levels in obese, insulin-resistant dogs, suggesting potential for new oral peptide therapies. The study also found that short-acting GLP-1 receptor agonists such as exenatide and lixisenatide can slow gastric emptying, lower blood glucose, and reduce uric acid production (103).
Additionally, liraglutide and semaglutide cause more gastrointestinal side effects than dulaglutide. Higher doses of GLP-1RA increase this risk, regardless of drug type or formulation, possibly due to appetite center inhibition (104). GLP-1RA drugs enhance insulin sensitivity and reduce blood sugar and uric acid in diabetic patients with HUA (103). Recent studies suggest that reducing oxidative stress can improve blood glucose issues and help repair damaged blood vessels (105). GLP-1RA may lower inflammation and oxidative stress by enhancing glucose control, reducing obesity, and improving insulin resistance and metabolic function in people with diabetes and HUA. It is speculated that GLP-1RA may reduce inflammation and oxidative stress by improving glucose control and reducing obesity, as well as improving insulin resistance and metabolic function in individuals with diabetes and HUA. Overall, GLP-1RA effectively manages diabetes with HUA.
Febuxostat, a new non-purine xanthine oxidase inhibitor, has gained attention for its effectiveness in lowering serum uric acid and potentially improving diabetes-related complications in patients with hyperuricemic diabetes. Initially, febuxostat’s anti-inflammatory properties could benefit people with diabetes by reducing HUA-related inflammation, potentially improving their overall health (106). Subsequently, febuxostat might enhance cardiovascular health in diabetic patients by improving endothelial function (107). However, its limited impact on endothelial function over long-term treatment, despite effectively lowering uric acid, indicates a need for further investigation. Moreover, febuxostat’s antioxidant properties may aid in treating diabetes with HUA by reducing superoxide anion production and oxidative stress, which is linked to insulin resistance (108). This could indirectly enhance insulin sensitivity. Febuxostat may strengthen kidney function by significantly lowering uric acid levels in kidney transplant patients, offering short-term improvements (109). This is crucial for people with diabetes, as managing uric acid can help delay diabetic kidney disease progression.
In summary, there are safety concerns regarding febuxostat’s use in diabetic patients, as it may increase cardiovascular risk, necessitating careful evaluation (108, 111). Besides, febuxostat could be crucial in treating diabetes with HUA by reducing uric acid, enhancing insulin sensitivity, reducing inflammation, and protecting kidney function. However, more research is needed to verify its long-term effects and safety in diabetic patients.
This study applied scientometrics to analyze the relationship between HUA and diabetes, revealing current interests and future trends while providing a theoretical foundation for further research. However, it is limited to literature from the Web of Science Core Collection, excluding non-English studies and not addressing the relationship between HUA and different diabetes types.
Current research trends reveal that studying HUA and diabetes is a dynamic field with many opportunities. By examining their correlation, we can identify individuals at high risk for early-stage diabetes, offering a theoretical basis for interventions to prevent its progression. Consequently, comprehensive treatment plans for individuals with HUA and diabetes are crucial to manage their conditions and prevent complications. Patients with persistent HUA should be prioritized in diabetes prevention guidelines.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
LLM: Data curation, Formal analysis, Investigation, Resources, Visualization, Writing – original draft, Writing – review & editing. JW: Methodology, Writing – review & editing. LM: Conceptualization, Software, Writing – review & editing. XW: Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the National Natural Science Foundation of China (Grant No. 81960800) and the 2023 Autonomous Region Key Research and Development Task Special (No. 2023B03002-3).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1441503/full#supplementary-material
1. Maiuolo J, Oppedisano F, Gratteri S, Muscoli C, Mollace V. Regulation of uric acid metabolism and excretion. Int J Cardiol. (2016) 213:8–14. doi: 10.1016/j.ijcard.2015.08.109
2. Trifirò G, Morabito P, Cavagna L, Ferrajolo C, Pecchioli S, Simonetti M, et al. Epidemiology of gout and hyperuricaemia in Italy during the years 2005-2009: a nationwide population-based study. Ann rheumatic Dis. (2013) 72:694–700. doi: 10.1136/annrheumdis-2011-201254
3. Yang G, Zhou S, Feng Y, Lang J, Chen Y, Ren H. The prevalence of HUA and the association between HUA and age in patients with psychiatric disorders to a general hospital: A cross-section study. Int J Gen Med. (2024) 17:1467–77. doi: 10.2147/IJGM.S454670
4. Bardin T, Magnat E, Clerson P, Richette P, Rouchon B. Epidemiology of gout and HUA in New Caledonia. Joint Bone Spine. (2022) 89:105286. doi: 10.1016/j.jbspin.2021.105286
5. Wang C, Wang J, Wan R, Yuan T, Yang L, Zhang D, et al. Relationship between baseline and changed serum uric acid and the incidence of type 2 diabetes mellitus: a national cohort study. Front Public Health. (2023) 11:1170792. doi: 10.3389/fpubh.2023.1170792
6. Sun S, Chen L, Chen D, Li Y, Liu G, Ma L, et al. Prevalence and associated factors of HUA among Chinese patients with diabetes: a cross-sectional study. Ther Adv Endocrinol Metab. (2023) 14:20420188231198620. doi: 10.1177/20420188231198620
7. Jiang J, Zhang T, Liu Y, Chang Q, Zhao Y, Guo C, et al. Prevalence of diabetes in patients with HUA and gout: A systematic review and meta-analysis. Curr Diabetes Rep. (2023) 23:103–17. doi: 10.1007/s11892-023-01506-2
8. Malla P, Khanal MP, Pokhrel A, Sah B, Pathak S, Subedi A, et al. Correlation of serum uric acid and lipid profile in patients with type 2 diabetes mellitus. J Nepal Health Res Council. (2023) 21:170–4. doi: 10.33314/jnhrc.v21i1.4781
9. Zhu L, Wang X, Sun J, Qian Q, Yu J, An X. HUA predicts the progression of type 2 diabetic kidney disease in Chinese patients. Diabetes therapy: research Treat Educ Diabetes related Disord. (2023) 14:581–91. doi: 10.1007/s13300-023-01374-9
10. Dikker O, Aktaş A, Şahin M, Doğan M, Dağ H. The association of serum uric acid levels and various uric acid-related ratios with insulin resistance and obesity: A preliminary study in adolescents. Children (Basel Switzerland). (2023) 10:1493. doi: 10.3390/children10091493
11. Lu J, Hou X, Yuan X, Cui L, Liu Z, Li X, et al. Knockout of the urate oxidase gene provides a stable mouse model of HUA associated with metabolic disorders. Kidney Int. (2018) 93:69–80. doi: 10.1016/j.kint.2017.04.031
12. Zhao H, Lu J, He F, Wang M, Yan Y, Chen B, et al. HUA contributes to glucose intolerance of hepatic inflammatory macrophages and impairs the insulin signaling pathway via IRS2-proteasome degradation. Front Immunol. (2022) 13:931087. doi: 10.3389/fimmu.2022.931087
13. Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular biological and clinical understanding of the pathophysiology and treatments of HUA and its association with metabolic syndrome, cardiovascular diseases and chronic kidney disease. Int J Mol Sci. (2021) 22:9221. doi: 10.3390/ijms22179221
14. Lu J, He Y, Cui L, Xing X, Liu Z, Li X, et al. HUA predisposes to the onset of diabetes via promoting pancreatic β-cell death in uricase-deficient male mice. Diabetes. (2020) 69:1149–63. doi: 10.2337/db19-0704
15. Yu W, Chen C, Zhuang W, Wang W, Liu W, Zhao H, et al. Silencing TXNIP ameliorates high uric acid-induced insulin resistance via the IRS2/AKT and Nrf2/HO-1 pathways in macrophages. Free Radical Biol Med. (2022) 178:42–53. doi: 10.1016/j.freeradbiomed.2021.11.034
16. Huang G, Li M, Mao Y, Li Y. Development and internal validation of a risk model for HUA in diabetic kidney disease patients. Front Public Health. (2022) 10:863064. doi: 10.3389/fpubh.2022.863064
17. Lazarides MK, Lazaridou IZ, Papanas N. Bibliometric analysis: bridging informatics with science. Int J lower extremity wounds. (2023), 15347346231153538. doi: 10.1177/15347346231153538
18. Nakagawa S, Samarasinghe G, Haddaway NR, Westgate MJ, O'Dea RE, Noble DWA, et al. Research weaving: visualizing the future of research synthesis. Trends Ecol Evol. (2019) 34:224–38. doi: 10.1016/j.tree.2018.11.007
19. Chen C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. (2006) 57:359–77. doi: 10.1002/asi.20317
20. Zimmet PZ. Hyperinsulinemia–how innocent a bystander? Diabetes Care. (1993) 16 Suppl 3:56–70. doi: 10.2337/diacare.16.3.56
21. Sowers JR. Effects of calcium antagonists on insulin sensitivity and other metabolic parameters. Am J Cardiol. (1997) 79:24–48. doi: 10.1016/s0002-9149(97)89421-0
22. Reaven GM. Pathophysiology of insulin resistance in human disease. Physiol Rev. (1995) 75:473–86. doi: 10.1152/physrev.1995.75.3.473
23. Wannamethee SG, Shaper AG, Alberti KG. Physical activity, metabolic factors, and the incidence of coronary heart disease and type 2 diabetes. Arch Internal Med. (2000) 160:2108–16. doi: 10.1001/archinte.160.14.2108
24. Hsieh SD, Muto T, Tsuji H, Arase Y, Murase T. Clustering of other metabolic risk factors in subjects with metabolic syndrome. Metabolism: Clin Exp. (2010) 59:697–702. doi: 10.1016/j.metabol.2009.08.026
25. Heinig M, Johnson RJ. Role of uric acid in hypertension, renal disease, and metabolic syndrome. Cleveland Clinic J Med. (2006) 73:1059–64. doi: 10.3949/ccjm.73.12.1059
26. Hu FB, Malik VS. Sugar-sweetened beverages and risk of obesity and type 2 diabetes: epidemiologic evidence. Physiol Behav. (2010) 100:47–54. doi: 10.1016/j
27. Vázquez-Mellado J, Alvarez Hernández E, Burgos-Vargas R. Primary prevention in rheumatology: the importance of HUA. Best Pract Res Clin Rheumatol. (2004) 18:111–24. doi: 10.1016/j.berh.2004.01.001
28. Zoppini G, Targher G, Bonora E. The role of serum uric acid in cardiovascular disease in type 2 diabetic and non-diabetic subjects: a narrative review. J endocrinological Invest. (2011) 34:881–6. doi: 10.1007/BF03346733
29. Benn CL, Dua P, Gurrell R, Loudon P, Pike A, Storer RI, et al. Physiology of HUA and urate-lowering treatments. Front Med. (2018) 5:160. doi: 10.3389/fmed.2018.00160
30. Tatzber F, Rabl H, Koriska K, Erhart U, Puhl H, Waeg G, et al. Elevated serum neopterin levels in atherosclerosis. Atherosclerosis. (1991) 89:203–8. doi: 10.1016/0021-9150(91)90061-7
31. Johnson RJ, Bakris GL, Borghi C, Chonchol MB, Feldman D, Lanaspa MA, et al. HUA, acute and chronic kidney disease, hypertension, and cardiovascular disease: report of a scientific workshop organized by the national kidney foundation. Am J Kidney Dis. (2018) 71:851–65. doi: 10.1053/j.ajkd.2017.12.009
32. Chen-Xu M, Yokose C, Rai SK, Pillinger MH, Choi HK. Contemporary prevalence of gout and HUA in the United States and decadal trends: the national health and nutrition examination survey, 2007-2016. Arthritis Rheumatol (Hoboken N.J.). (2019) 71:991–9. doi: 10.1002/art.40807
33. White WB, Saag KG, Becker MA, Borer JS, Gorelick PB, Whelton A, et al. Cardiovascular safety of febuxostat or allopurinol in patients with gout. New Engl J Med. (2018) 378:1200–10. doi: 10.1056/NEJMoa1710895
34. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. New Engl J Med. (2008) 359:1811–21. doi: 10.1056/NEJMra0800885
35. Kuwabara M, Niwa K, Hisatome I, Nakagawa T, Roncal-Jimenez CA, Andres-Hernando A, et al. Asymptomatic hyperuricemia without comorbidities predicts cardiometabolic diseases: five-year Japanese cohort study. Hypertension (Dallas Tex: 1979). (2017) 69:1036–44. doi: 10.1161/HYPERTENSIONAHA.116.08998
36. Kodama S, Saito K, Yachi Y, et al. Association between serum uric acid and development of type 2 diabetes. Diabetes Care. (2009) 32:1737–42. doi: 10.2337/dc09-0288
37. Dehghan A, van Hoek M, Sijbrands EJ, Hofman A, Witteman JC. High serum uric acid as a novel risk factor for type 2 diabetes. Diabetes Care. (2008) 31:361–2. doi: 10.2337/dc07-1276
38. Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and HUA in the US general population: the National Health and Nutrition Examination Survey 2007-2008. Arthritis rheumatism. (2011) 63:3136–41. doi: 10.1002/art.30520
39. Takir M, Kostek O, Ozkok A, Elcioglu OC, Bakan A, Erek A, et al. Lowering uric acid with allopurinol improves insulin resistance and systemic inflammation in asymptomatic HUA. J Invest Med. (2015) 63:924–9. doi: 10.1097/JIM.0000000000000242
40. Zhao Y, Xu L, Tian D, et al. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. (2018) 20:458–62. doi: 10.1111/dom.13101
41. Borghi C, Rosei EA, Bardin T, Dawson J, Dominiczak A, Kielstein JT, et al. Serum uric acid and the risk of cardiovascular and renal disease. J hypertension. (2015) 33:1729–41. doi: 10.1097/HJH.0000000000000701
42. Goicoechea M, de Vinuesa SG, Verdalles U, Ruiz-Caro C, Ampuero J, Rincón A. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin J Am Soc Nephrology: CJASN. (2010) 5:1388–93. doi: 10.2215/CJN.01580210
43. Vayá A, Rivera L, Hernández-Mijares A, Bautista D, Solá E, Romagnoli M, et al. Association of metabolic syndrome and its components with hyperuricemia in a Mediterranean population. Clin hemorheology microcirculation. (2015) 60:327–34. doi: 10.3233/CH-141887
44. Verma S, Tiwari R, Verma N, Singh S, Sharma A. Anthropometry and blood biomarkers of diabetes and their possible association with obesity and metabolic syndrome. J Diabetes Metab Disord. (2023) 23:509–17. doi: 10.1007/s40200-023-01276-4
45. Singh SK, Singh R, Singh SK, Iquebal MA, Jaiswal S, Rai PK. Prevalence of obesity in newly onset diabetes mellitus and its relationship with uric acid: an Indian cross-sectional study. Int J Gen Med. (2023) 16:1217–26. doi: 10.2147/IJGM.S402683
46. Mandal AK, Leask MP, Sumpter NA, Choi HK, Merriman TR, Mount DB. Genetic and physiological effects of insulin-like growth factor-1 (IGF-1) on human urate homeostasis. J Am Soc Nephrology: JASN. (2023) 34:451–66. doi: 10.1681/ASN.0000000000000054
47. Lastra Gonzalez G, Manrique-Acevedo C. Vascular insulin resistance as a potential mechanism of increased cardiovascular risk in gestational diabetes. American journal of physiology. Heart Circulatory Physiol. (2024) 327:H828–9. doi: 10.1152/ajpheart.00572.2024
48. Kim YJ, Kim S, Seo JH, Cho SK. Prevalence and associations between metabolic syndrome components and hyperuricemia by race: findings from US population, 2011-2020. Arthritis Care Res. (2024) 76:1195–202. doi: 10.1002/acr.25338
49. Wisniewski A, DeLouize AM, Walker T, Chatterji S, Naidoo N, Kowal P, et al. Sustained metabolic dysregulation and the emergence of diabetes: associations between HbA1c and metabolic syndrome components in Tunisian diabetic and nondiabetic groups. J Physiol anthropology. (2024) 43:18. doi: 10.1186/s40101-024-00365-4
50. Hezam AAM, Shaghdar HBM, Chen L. The connection between hypertension and diabetes and their role in heart and kidney disease development. J Res Med Sci. (2024) 29:22. doi: 10.4103/jrms.jrms_470_23
51. Cho J, Kim C, Kang DR, Park JB. Hyperuricemia and uncontrolled hypertension in treated hypertensive patients: K-MetS Study. Medicine. (2016) 95:e4177. doi: 10.1097/MD.0000000000004177
52. Ferrannini E, Cushman WC. Diabetes and hypertension: the bad companions. Lancet (London England). (2012) 380:601–10. doi: 10.1016/S0140-6736(12)60987-8
53. Shahid SM, Nawab SN, Shaikh R, Mahboob T. Glycemic control, dyslipidemia and endothelial dysfunction in coexisted diabetes, hypertension and nephropathy. Pakistan J Pharm Sci. (2012) 25:123–9. doi: 10.1254/jphs.11177SC
54. Shen Y, Dai Y, Wang XQ, Zhang RY, Lu L, Ding FH, et al. Searching for optimal blood pressure targets in type 2 diabetic patients with coronary artery disease. Cardiovasc Diabetol. (2019) 18:160. doi: 10.1186/s12933-019-0959-1
55. Usui I. Common metabolic features of hypertension and type 2 diabetes. Hypertension research: Off J Japanese Soc Hypertension. (2023) 46:1227–33. doi: 10.1038/s41440-023-01233-x
56. Tonneijck L, Muskiet MH, Smits MM, van Bommel EJ, Heerspink HJ, van Raalte DH, et al. Glomerular hyperfiltration in diabetes: mechanisms, clinical significance, and treatment. J Am Soc Nephrology: JASN. (2017) 28:1023–39. doi: 10.1681/ASN.2016060666
57. Bikbov B, Perico N, Remuzzi G, & Global Burden of Disease Study Genitourinary Disease Expert Group. High serum cholesterol: a missed risk factor for chronic kidney disease mortality. Lancet Diabetes Endocrinol. (2014) 2:613–4. doi: 10.1016/S2213-8587(14)70162-7
58. Waheed Y, Yang F, Sun D. Role of asymptomatic hyperuricemia in the progression of chronic kidney disease and cardiovascular disease. Korean J Internal Med. (2021) 36:1281–93. doi: 10.3904/kjim.2020.340
59. Lai S, Mariotti A, Coppola B, Lai C, Aceto P, Dimko M, et al. Uricemia and homocysteinemia: nontraditional risk factors in the early stages of chronic kidney disease–preliminary data. Eur Rev Med Pharmacol Sci. (2014) 18:1010–7. doi: 10.1590/S1984-82502014000200023
60. Chen XY, Lu F, Zhang J, Xu CX, Du XF, Liang MB, et al. The effect of hyperuricemia and its interaction with hypertension towards chronic kidney disease in patients with type 2 diabetes: evidence from a cross- sectional study in Eastern China. Front Endocrinol. (2024) 15:1415459. doi: 10.3389/fendo.2024.1415459
61. Ribeiro M, Fanton S, Paiva BR, Baptista BG, Alvarenga L, Ribeiro-Alves M, et al. Dark chocolate (70% cocoa) attenuates the inflammatory marker TNF-α in patients on hemodialysis. Clin Nutr ESPEN. (2023) 53:189–95. doi: 10.1016/j.clnesp.2022.12.009
62. Wang C, Che H, Zhou Y, Wang R, Zhu D, Cheng L, et al. Joint association of hyperuricemia and chronic kidney disease with mortality in patients with chronic heart failure. Front Endocrinol. (2023) 14:1131566. doi: 10.3389/fendo.2023.1131566
63. Wan X, Xu C, Lin Y, Lu C, Li D, Sang J, et al. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J Hepatol. (2016) 64:925–32. doi: 10.1016/j.jhep.2015.11.022
64. Chapagain A, Caton PW, Kieswich J, Andrikopoulos P, Nayuni N, Long JH, et al. Elevated hepatic 11β-hydroxysteroid dehydrogenase type 1 induces insulin resistance in uremia. Proc Natl Acad Sci United States America. (2014) 111:3817–22. doi: 10.1073/pnas.1312436111
65. Ghorbani Z, Mirmohammadali SN, Shoaibinobarian N, Rosenkranz SK, Arami S, Hekmatdoost A, et al. Insulin resistance surrogate markers and risk of hyperuricemia among patients with and without coronary artery disease: a cross-sectional study. Front Nutr. (2023) 10:1048675. doi: 10.3389/fnut.2023.1048675
66. Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular biological and clinical understanding of the pathophysiology and treatments of hyperuricemia and its association with metabolic syndrome, cardiovascular diseases and chronic kidney disease. Int J Mol Sci. (2021) 22:9221. doi: 10.3390/ijms22179221
67. Plawecki M, Gayrard N, Jeanson L, Chauvin A, Lajoix AD, Cristol JP, et al. Cardiac remodeling associated with chronic kidney disease is enhanced in a rat model of metabolic syndrome: Preparation of mesenchymal transition. Mol Cell Biochem. (2024) 479:29–39. doi: 10.1007/s11010-023-04710-6
68. Calò LA, Naso A, D'Angelo A, Pagnin E, Zanardo M, Puato M, et al. Molecular biology-based assessment of vitamin E-coated dialyzer effects on oxidative stress, inflammation, and vascular remodeling. Artif organs. (2011) 35:E33–9. doi: 10.1111/j.1525-1594.2010.01125.x
69. Nishizawa H, Maeda N, Shimomura I. Impact of hyperuricemia on chronic kidney disease and atherosclerotic cardiovascular disease. Hypertension Res. (2022) 45:635–40. doi: 10.1038/s41440-021-00840-w
70. Jabarpour M, Rashtchizadeh N, Argani H, Ghorbanihaghjo A, Ranjbarzadhag M, Sanajou D, et al. The impact of dyslipidemia and oxidative stress on vasoactive mediators in patients with renal dysfunction. Int Urol Nephrol. (2019) 51:2235–42. doi: 10.1007/s11255-019-02319-7
71. Lee TH, Chen JJ, Wu CY, Yang CW, Yang HY. Hyperuricemia and progression of chronic kidney disease: A review from physiology and pathogenesis to the role of urate-lowering therapy. Diagnostics (Basel Switzerland). (2021) 11:1674. doi: 10.3390/diagnostics11091674
72. Honda H, Hirano T, Ueda M, Kojima S, Mashiba S, Hayase Y, et al. High-density lipoprotein subfractions and their oxidized subfraction particles in patients with chronic kidney disease. J Atheroscl Thromb. (2016) 23:81–94. doi: 10.5551/jat.30015. Mironova O. I. (2023). Terapevticheskii arkhiv, 94(12), 1426–1430. doi.org/10.26442/00403660.2022.12.201999.
73. Yu W, Xie D, Yamamoto T, Koyama H, Cheng J. Mechanistic insights of soluble uric acid-induced insulin resistance: Insulin signaling and beyond. Rev endocrine Metab Disord. (2023) 24:327–43. doi: 10.1007/s11154-023-09787-4
74. Fang F, Wang N, Liu X, et al. [Value of C-peptide-based insulin resistance index for evaluating correlation between insulin resistance and serum uric acid level in individuals undergoing health examination]. Nan Fang Yi Ke Da Xue Xue Bao. (2023) 43:1509–14. doi: 10.12122/j.issn.1673-4254.2023.09.08
75. Maahs DM, Caramori L, Cherney DZ, Galecki AT, Gao C, Jalal D, et al. Uric acid lowering to prevent kidney function loss in diabetes: the preventing early renal function loss (PERL) allopurinol study. Curr Diabetes Rep. (2013) 13:550–9. doi: 10.1007/s11892-013-0381-0
76. Joosten LAB, Crişan TO, Bjornstad P, Johnson RJ. Asymptomatic hyperuricaemia: a silent activator of the innate immune system. Nat Rev Rheumatol. (2020) 16:75–86. doi: 10.1038/s41584-019-0334-3
77. Ma Q, Immler R, Pruenster M, Sellmayr M, Li C, von Brunn A, et al. Soluble uric acid inhibits β2 integrin-mediated neutrophil recruitment in innate immunity. Blood. (2022) 139:3402–17. doi: 10.1182/blood.2021011234
78. Wu W, Dnyanmote AV, Nigam SK. Remote communication through solute carriers and ATP binding cassette drug transporter pathways: an update on the remote sensing and signaling hypothesis. Mol Pharmacol. (2011) 79:795–805. doi: 10.1124/mol.110.070607
79. Rapa SF, Di Iorio BR, Campiglia P, Heidland A, Marzocco S. Inflammation and oxidative stress in chronic kidney disease-potential therapeutic role of minerals, vitamins and plant-derived metabolites. Int J Mol Sci. (2019) 21:263. doi: 10.3390/ijms21010263
80. Ola MS. Does hyperglycemia cause oxidative stress in the diabetic rat retina? Cells. (2021) 10:794. doi: 10.3390/cells10040794
81. Gherghina ME, Peride I, Tiglis M, Neagu TP, Niculae A, Checherita IA. Uric acid and oxidative stress-relationship with cardiovascular, metabolic, and renal impairment. Int J Mol Sci. (2022) 23:3188. doi: 10.3390/ijms23063188
82. Fluck RA, Jaffe MJ. Cholinesterases from plant tissues. VI. Preliminary characterization of enzymes from Solanum melongena L. and Zea mays L. Biochim Biophys Acta. (1975) 410:130–4. doi: 10.1016/0005-2744(75)90213-2
83. Wen T. Analysis of digital gene expression profile of 3T3-L1 in mouse adipocytes affected by high uric acid and molecular mechanism of insulin resistance induction. Guangdong: Shantou University (2017).
84. Ma Y, Wang P, Zhen Q. Effects of blood pressure, body weight, glucose and lipid metabolism disorders on insulin resistance and islet beta cell function in newly diagnosed type 2 diabetes patients. National Endocrinology Conference of the Chinese Medical Association (2012).
85. Qu H. Effects of inhibition of fatty acid synthase on blood glucose level, oxidative homeostasis and metabolism in obesity induced by high fat and high sugar diets. Jiangnan University Science (2021). doi: 10.27169/,dcnki.Gwqgu.2021.000078
86. Zhang Y. Activation of AMPK and ERK signaling pathway by uric acid induces oxidative damage and proliferation inhibition of rat islet beta cells. Guangdong: Shantou Big Study (2012).
87. Hu Y. High uric acid increases ROS levels, inhibits IRS2/AKT signaling pathway, and induces INS-1 insulin resistance in islet beta cells. Shantou University (2016).
88. Qu X, Lu J, Wu X. The role of PPAR-gamma-PCK1-MTOR signaling pathway in apoptosis of islet cells induced by HUA. Qingdao Univ Stud J Med Sci. (2018) 54:5. doi: 10.11712/jms201802004
89. Liu C, Zhou XR, Ye MY, Xu XQ, Zhang YW, Liu H, et al. RBP4 is associated with insulin resistance in HUA-induced rats and patients with HUA. Front Endocrinol. (2021) 12:653819. doi: 10.3389/fendo.2021.653819
90. Butt JH, Docherty KF, Claggett BL, Desai AS, Petersson M, Langkilde AM, et al. Association of dapagliflozin use with clinical outcomes and the introduction of uric acid-lowering therapy and colchicine in patients with heart failure with and without gout: A patient-level pooled meta-analysis of DAPA-HF and DELIVER. JAMA Cardiol. (2023) 8:386–93. doi: 10.1001/jamacardio.2022.5608
91. Takata T, Isomoto H. Pleiotropic effects of sodium-glucose cotransporter-2 inhibitors: renoprotective mechanisms beyond glycemic control. Int J Mol Sci. (2021) 22:4374. doi: 10.3390/ijms22094374
92. Packer M. Critical reanalysis of the mechanisms underlying the cardiorenal benefits of SGLT2 inhibitors and reaffirmation of the nutrient deprivation signaling/autophagy hypothesis. Circulation. (2022) 146:1383–405. doi: 10.1161/CIRCULATIONAHA.122.061732
93. Bailey CJ. Uric acid and the cardio-renal effects of SGLT2 inhibitors. Diabetes Obes Metab. (2019) 21:1291–8. doi: 10.1111/dom.13670
94. Oikonen M, Wendelin-Saarenhovi M, Lyytikäinen LP, Siitonen N, Loo BM, Jula A, et al. Associations between serum uric acid and markers of subclinical atherosclerosis in young adults. Cardiovasc Risk Young Finns study Atheroscl. (2012) 223:497–503. doi: 10.1016/j.atherosclerosis.2012.05.036
95. Chino Y, Samukawa Y, Sakai S, Nakai Y, Yamaguchi J, Nakanishi T, et al. SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule by increased glycosuria. Biopharmaceutics Drug disposition. (2014) 35:391–404. doi: 10.1002/bdd.1909
96. La Grotta R, de Candia P, Olivieri F, Matacchione G, Giuliani A, Rippo MR, et al. Anti-inflammatory effect of SGLT-2 inhibitors via uric acid and insulin. Cell Mol Life sciences: CMLS. (2022) 79:273. doi: 10.1007/s00018-022-04289-z
97. Dong M, Chen H, Wen S, Yuan Y, Yang L, Xu D, et al. The mechanism of sodium-glucose cotransporter-2 inhibitors in reducing uric acid in type 2 diabetes mellitus. Diabetes Metab syndrome obesity: Targets Ther. (2023) 16:437–45. doi: 10.2147/DMSO.S399343
98. Cheong AJY, Teo YN, Teo YH, Syn NL, Ong HT, Ting AZH, et al. SGLT inhibitors on weight and body mass: A meta-analysis of 116 randomized-controlled trials. Obes (Silver Spring Md.). (2022) 30:117–28. doi: 10.1002/oby.23331
99. Wang Q, Zhao C, Jin L, Zhang H, Miao Q, Liu H, et al. AWRK6, a novel GLP-1 receptor agonist, attenuates diabetes by stimulating insulin secretion. Int J Mol Sci. (2018) 19:3053. doi: 10.3390/ijms19103053
100. Drucker DJ. GLP-1 physiology informs the pharmacotherapy of obesity. Mol Metab. (2022) 57:101351. doi: 10.1016/j.molmet.2021.101351
101. Pechenov S, Revell J, Will S, Naylor J, Tyagi P, Patel C, et al. Development of an orally delivered GLP-1 receptor agonist through peptide engineering and drug delivery to treat chronic disease. Sci Rep. (2021) 11:22521. doi: 10.1038/s41598-021-01750-0
102. Zhang Z, Zhang Q, Tan Y, Chen Y, Zhou X, Liu S, et al. GLP-1RAs caused gastrointestinal adverse reactions of drug withdrawal: a system review and network meta-analysis. Front Endocrinol. (2023) 14:1149328. doi: 10.3389/fendo.2023.1149328
103. Gentilella R, Pechtner V, Corcos A, Consoli A. Glucagon-like peptide-1 receptor agonists in type 2 diabetes treatment: are they all the same? Diabetes/metabolism Res Rev. (2019) 35:e3070. doi: 10.1002/dmrr.3070
104. Bakbak E, Terenzi DC, Trac JZ, Teoh H, Quan A, Glazer SA, et al. Lessons from bariatric surgery: Can increased GLP-1 enhance vascular repair during cardiometabolic-based chronic disease? Rev endocrine Metab Disord. (2021) 22:1171–88. doi: 10.1007/s11154-021-09669-7
105. Mukri MNA, Kong WY, Mustafar R, Shaharir SS, Shah SA, Abdul Gafor AH, et al. Role of febuxostat in retarding progression of diabetic kidney disease with asymptomatic hyperuricemia: A 6-months open-label, randomized controlled trial. EXCLI J. (2018) 17:563–75. doi: 10.17179/excli2018-1256
106. Maruhashi T, Higashi Y, Yoshida H, Tanaka A, Eguchi K, Tomiyama H, et al. Long-term effect of febuxostat on endothelial function in patients with asymptomatic hyperuricemia: A sub-analysis of the PRIZE study. Front Cardiovasc Med. (2022) 9:882821. doi: 10.3389/fcvm.2022.882821
107. Huang HH, Chen YY, Fang YW, Liou HH, Wang JT, Tsai MH. Comparative cardiovascular risks of febuxostat and allopurinol in patients with diabetes mellitus and chronic kidney disease. Med Sci monitor. (2024) 30:e944314. doi: 10.12659/MSM.944314
108. Li Y, Liu M, Zhang X, Lu Y, Meng J. Switching from allopurinol to febuxostat: efficacy and safety in the treatment of hyperuricemia in renal transplant recipients. Renal failure. (2019) 41:595–9. doi: 10.1080/0886022X.2019.1632717
Keywords: hyperuricemia, diabetes, scientometrics, VOSviewers, CiteSpace
Citation: Ma L, Wang J, Ma L and Wang XM (2025) The link between hyperuricemia and diabetes: insights from a quantitative analysis of scientific literature. Front. Endocrinol. 15:1441503. doi: 10.3389/fendo.2024.1441503
Received: 31 May 2024; Accepted: 30 December 2024;
Published: 07 February 2025.
Edited by:
Johannes Wolfgang Dietrich, Ruhr University Bochum, GermanyReviewed by:
Ai Sinan, Beijing University of Chinese Medicine, ChinaCopyright © 2025 Ma, Wang, Ma and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xian Min Wang, eGpxenl5a2pAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.