 Ganlin Wu1,2
Ganlin Wu1,2 Yanli Ye
Yanli Ye
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 30 January 2025
Sec. Clinical Diabetes
Volume 15 - 2024 | https://doi.org/10.3389/fendo.2024.1431873
Purpose: To explore the influencing factors of acute kidney injury in elderly patients with diabetic nephropathy and to construct a nomogram model.
Methods: The research subjects were 680 patients with type 2 diabetic nephropathy admitted to our hospital. The patients were included from May 2018 to August 2023. Patients with acute kidney injury were used as the merge group (n=50), and patients without unmerge group (n=630) was included. The prevalence and predisposing factors of acute kidney injury in diabetic nephropathy were analyzed, multivariate logistic regression were used to analyze the influencing factors of acute kidney injury in patients, and a nomogram risk prediction model was established based on risk factors for verification.
Results: Analysis of the factors of acute kidney injury in diabetic nephropathy found that severe infection was the main trigger, accounting for 40.00%, followed by nephrotoxic antibiotics and severe heart failure. The age, urine microalbumin-to-creatinine ratio (ACR), blood urea nitrogen (BUN), uric acid(UA), and cystatin C (CysC) levels of patients in the combined acute kidney injury group were significantly higher than those in the unmerge group (P<0.05), and the left ventricular ejection fraction (LVEF) and epidermal growth factor receptor (eGFR) levels were significantly lower than those in the unmerge group (P<0.05). Age, ACR, and CysC levels are independent risk factors for acute kidney injury in diabetic nephropathy, and LVEF and eGFR are independent protective factors (P<0.05). The C-index of the nomogram risk prediction model in predicting acute kidney injury in diabetic nephropathy is 0.768 (95% CI: 0.663-0.806), and the calibration curve tends to the ideal curve; the prediction threshold is >0.18, and the nomogram risk prediction model provides a clinical net benefits, and clinical net benefits were higher than independent predictors.
Conclusion: The establishment of a nomogram model for acute kidney injury in elderly patients with diabetic nephropathy based on age, ACR, CysC, LVEF, and eGFR has a good predictive effect, which can help doctors more accurately assess the patient’s condition and provide a basis for formulating personalized treatment plans.
Diabetes is one of the chronic diseases that seriously threatens human health around the world. The kidney is one of the most commonly affected organs in diabetes. Diabetic nephropathy is a common microvascular complication of diabetes. The onset is insidious. In the early stages of kidney damage, there may be no symptoms. As the disease progresses, foamy urine, high blood pressure, and edema (swelling of feet, ankles, hands, or eyes) may gradually occur (1, 2). If it develops into end-stage renal disease, which is kidney failure, water, electrolyte, acid-base balance disorders and anemia will occur. The pathogenesis of diabetic nephropathy is complex and involves multiple factors such as hyperglycemia, hypertension, lipid metabolism disorders, and inflammatory reactions. With the increasing number of diabetic patients, diabetic nephropathy plays a vital role in promoting the occurrence of end-stage renal disease (3, 4). In our country, the prevalence of diabetic nephropathy is high, which brings a heavy burden to society and families (5). Acute kidney injury refers to a sudden decline in kidney function within a short period of time (usually 72 hours), leading to clinical manifestations such as azotemia, water and electrolyte disorders, and acid-base balance disorders. Patients with diabetic nephropathy are prone to acute kidney injury and have a poor prognosis (6). Acute kidney injury aggravates the condition of diabetic nephropathy, and patients need treatment such as dialysis or kidney transplantation, increasing the patient’s risk of death. Therefore, studying the influencing factors of acute kidney injury in elderly patients with diabetic nephropathy will help us better understand the characteristics of such patients and provide scientific basis for clinical prevention and treatment (7, 8). At the same time, by establishing a prediction model, patients can be warned of the risk of acute kidney injury in advance, providing a reference for clinicians to formulate individualized treatment plans. The nomogram model is a prediction model based on logistic regression analysis, which can predict the risk of acute kidney injury in diabetic nephropathy by integrating the relative importance of multiple influencing factors. Some studies have found (9, 10) that the nomogram model has certain accuracy in predicting acute kidney injury in diabetic nephropathy and can be used to guide clinicians in formulating preventive strategies and treatment plans. This study aims to explore the factors that influence the occurrence of acute kidney injury in elderly patients with diabetic nephropathy, which will help improve the prevention and treatment effect and reduce the mortality rate of patients.
The research subjects were 680 patients with type 2 diabetic nephropathy admitted to our hospital. The patients were included from May 2018 to August 2023. Patients with acute kidney injury were included in the merged group (n =50), unmerged group (n=630). Inclusion criteria: ① Diagnostic criteria for diabetic nephropathy are based on the chronic kidney disease assessment and clinical practice guidelines issued by KDIGO (Kidney Disease Improving Global Outcomes) in 2012. Urine microalbuminuria should be tested three times within three months, with at least two urine microalbuminurias ≥ 30 mg/24 h (11); ② Fasting blood glucose ≥7.0mmol/L (126mg/dl), and/or 2-hour blood glucose ≥11.1mmol/L (200mg/dl) in 75g OGTT), and/or HbA1c ≥ 6.5%; ③ Cognition Those with normal functions and high compliance; exclusion criteria: ① Those combined with cardiovascular disease, essential hypertension, liver damage, malignant tumors, and lupus erythematosus; ② Those combined with nephrotic syndrome, nephritis, and renal insufficiency; ③ Those combined with hyperthyroidism and thyroid dysfunction Hypoxia and other secretory diseases; ④Those who use nephrotoxic drugs; ⑤Those with communication disorders or mental illness. This study was approved by the hospital ethics committee. Signed informed consent were also obtained from all participants. According to the inclusion and exclusion criteria, 693 patients with diabetic nephropathy were screened. After excluding 13 patients who were lost to follow-up, 680 patients with diabetic nephropathy were finally obtained.The screening process is shown in Figure 1.
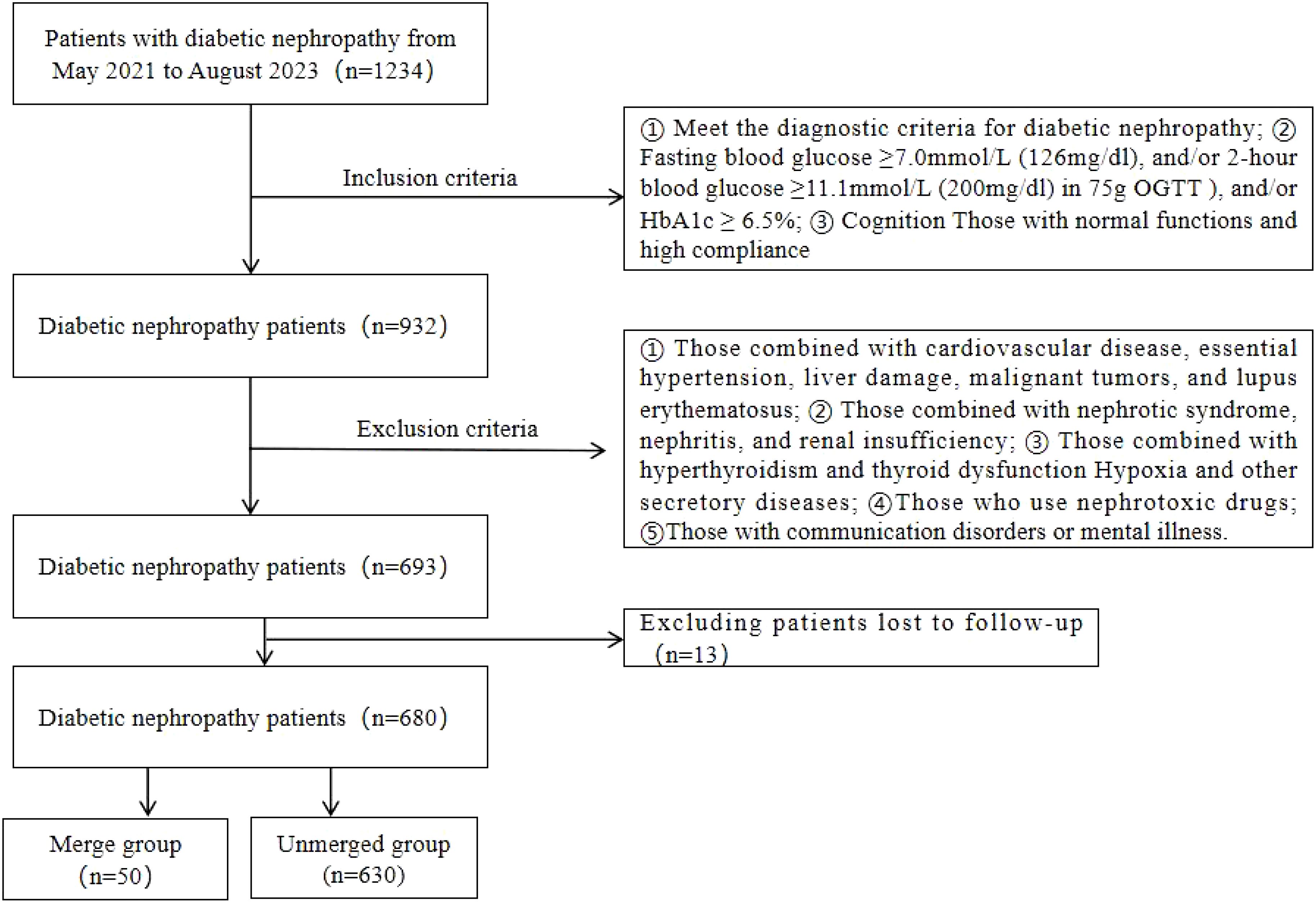
Figure 1. Literature screening flow chart.
Refer to the AKI diagnostic criteria proposed by KDIGO: serum creatinine increases by more than 1.5 times the baseline, and occurs within 7 days of the clear or inferred increase in serum creatinine level. The reference range of serum creatinine is 53-106μmol/L for adult males and 44-97μmol/L for adult females.
General information: Age, gender, systolic and diastolic blood pressure were collected for all patients.
Laboratory indicators: eGFR, glycated hemoglobin (HbAlc), serum albumin, ACR, LVEF, BUN, serum creatinine (Scr), UA, and CysC levels.
Nomogram analysis: Establish a nomogram model: Taking all patients as the research subjects, based on the results of logistic regression analysis, factors that have a significant impact on acute kidney injury in elderly patients with diabetic nephropathy are screened out and included in the nomogram model. The best model was determined through receiver operating characteristic curve (ROC) analysis.
Validate the nomogram model: Apply the established nomogram model to predict the risk of acute kidney injury. The predictive effectiveness of the model was evaluated by comparing the number of patients who actually developed acute kidney injury with the number of patients who were predicted to develop acute kidney injury. Draw a calibration chart for verification and evaluate the accuracy of the risk model.
By reviewing the patients’ medical records, the collected data were collated and statistically analysed using Excel sheets. For missing values or outliers, we used the mean to fill in or exclude to ensure the accuracy and reliability of the data. By analysing the collated data, we aimed to explore the factors affecting the occurrence of acute kidney injury in elderly patients with diabetic nephropathy, and to provide a reference basis for clinical prevention and treatment.
The enumeration data in this group of studies are expressed as [cases (%)], and the x2 test is used. The measurement data are all in the form of ( ± s) form, an independent sample t test was used between the two groups. The influencing factors of acute kidney injury in elderly patients with diabetic nephropathy were analyzed using multi-factor logistic regression, and a nomogram risk prediction model was established based on the risk factors. Bootstrap self-sampling method was used for internal testing. The predictive ability of the model was tested through the receiver operating characteristic curve (ROC curve), C-index and calibration curve are used for verification. SPSS 23.0 software was used for statistical data analysis, and P < 0.05 was considered as a statistically significant difference.
A total of 50 patients with acute kidney injury occurred among 680 patients with diabetic nephropathy, with an incidence rate of 7.35%; there were differences in the prevalence of acute kidney injury among patients with diabetic nephropathy of different ages and eGFR levels (x2 = 7.722, 18.987, P <0.05). See Table 1.
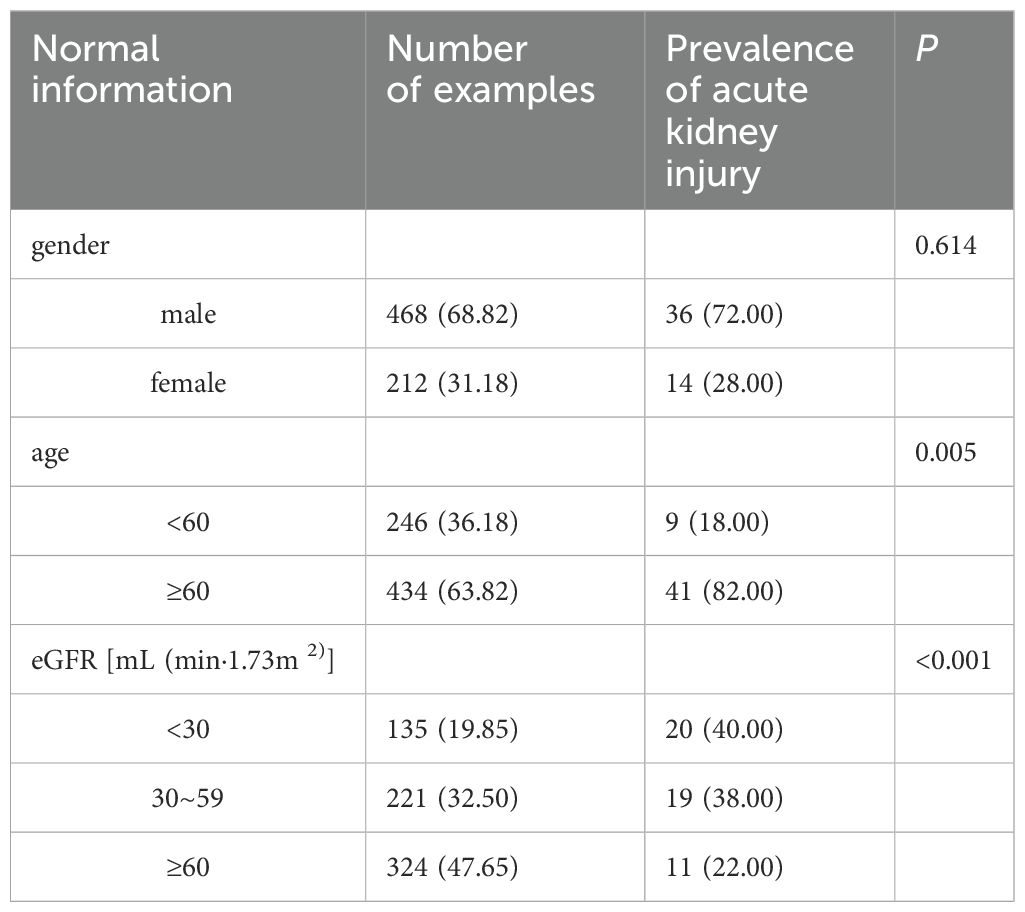
Table 1. Prevalence analysis of acute kidney injury in diabetic nephropathy.
Analysis of the influencing factors of acute kidney injury in diabetic nephropathy found that severe infection was the main trigger, accounting for 40.00%, followed by nephrotoxic antibiotics and severe heart failure. The details are shown in Table 2.
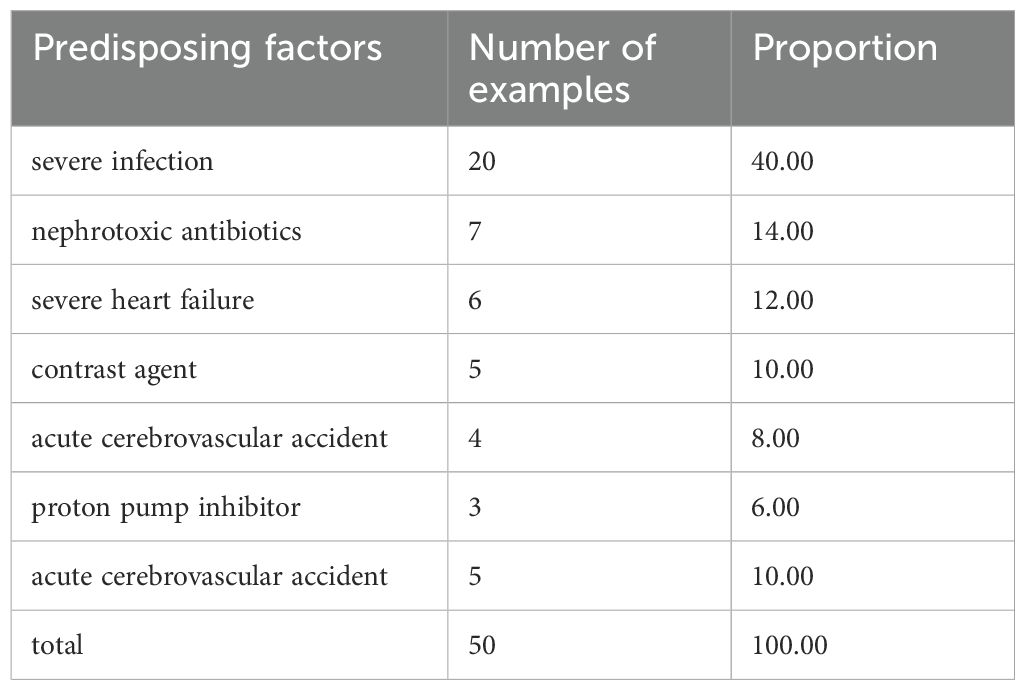
Table 2. Analysis of influencing factors of acute kidney injury in diabetic nephropathy.
CysC levels of patients in the combined acute kidney injury group were significantly higher than those in the unmerge group (P <0.05), and the LVEF and eGFR levels were significantly lower than those in the unmerge group (P <0.05), see Table 3.
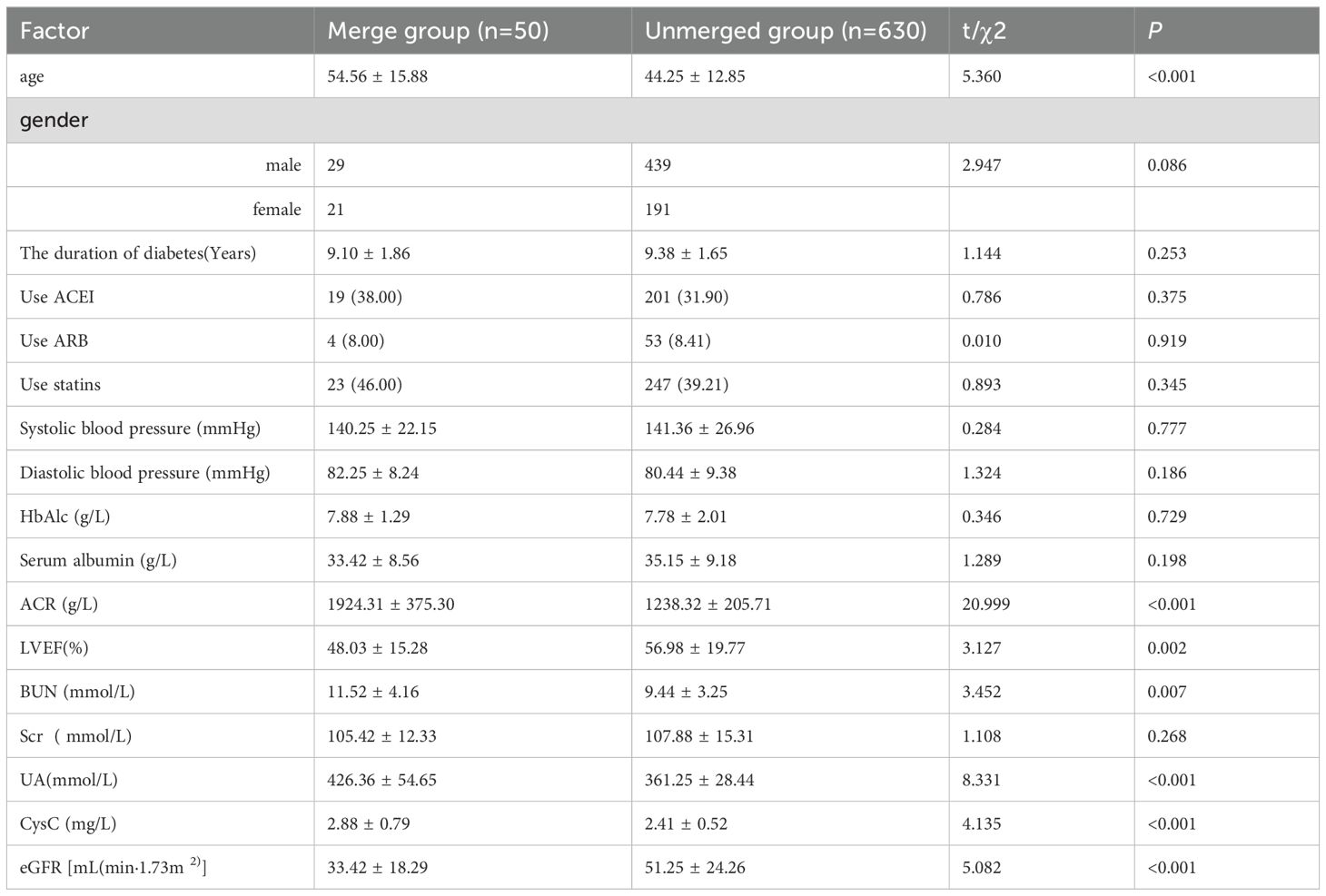
Table 3. Analysis of clinical data of the two groups.
Taking the statistically significant indicators in Table 3 as independent variables and whether acute kidney injury occurs in diabetic nephropathy as the dependent variable, the results show that age, ACR, and CysC levels are independent risk factors for acute kidney injury in diabetic nephropathy, and LVEF and eGFR are independent protective factor (P <0.05). See Supplementary Table S1.
After the multicollinearity test, the VIF range of the three variables RRI, MFI, and PVD was 1.316-2.501, indicating that there was no multicollinearity problem between them. Age, ACR, CysC, LVEF, and eGFR were used as factors to construct the nomogram risk prediction model. The nomogram risk prediction situation is shown in Figure 2.
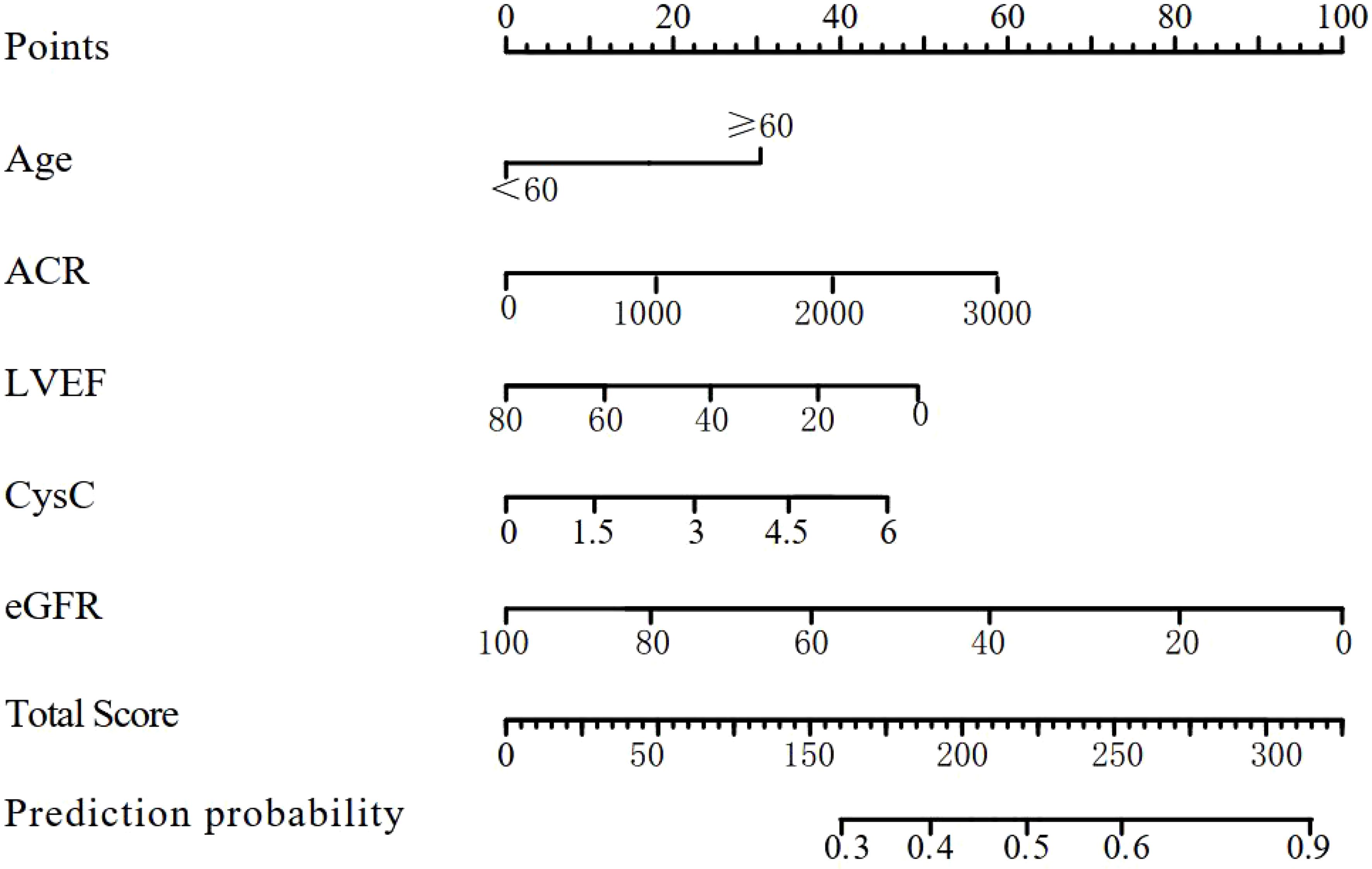
Figure 2. Nomogram risk prediction model for acute kidney injury in diabetic nephropathy.
the nomogram risk prediction model for predicting acute kidney injury in diabetic nephropathy is 0.768 (95% CI: 0.663-0.806), and the calibration curve tends to the ideal curve, see Figure 3; the prediction threshold is >0.18, and the nomogram risk prediction The model provides clinical net benefits, and the clinical net benefits are all higher than independent predictors, see Figure 4.
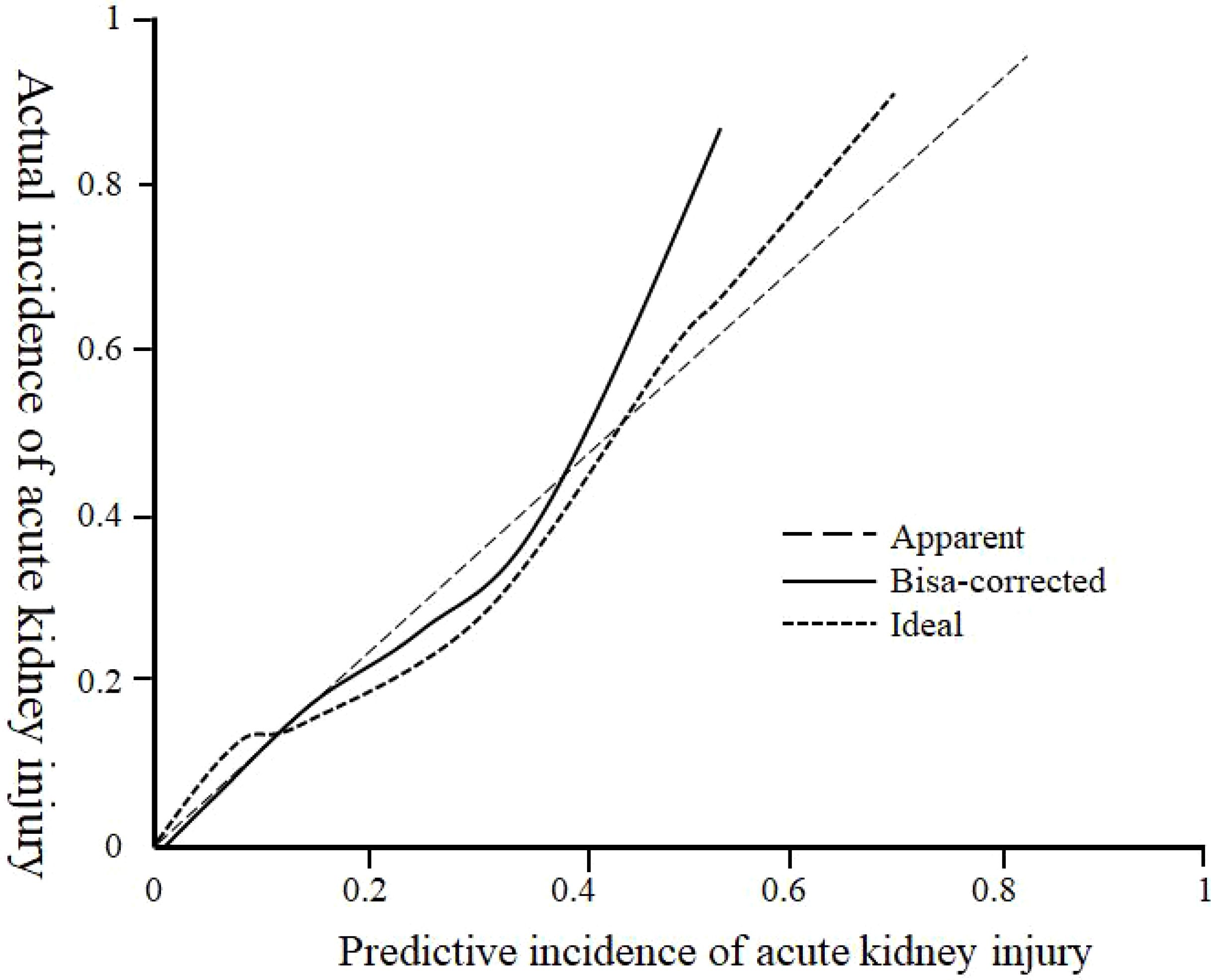
Figure 3. Calibration curve of the nomogram risk prediction model.
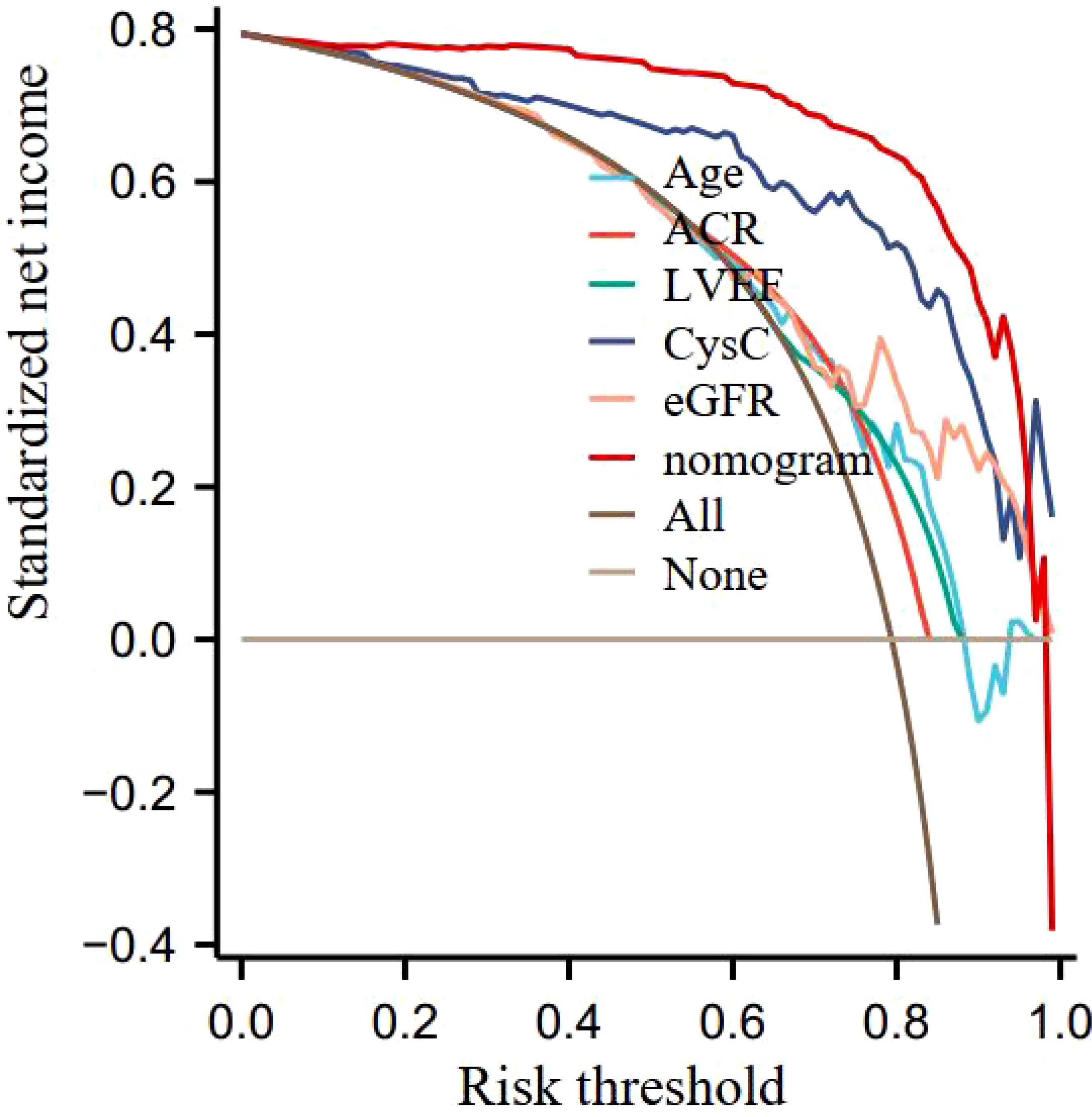
Figure 4. Nomogram risk prediction model decision curve.
Diabetic nephropathy is a complication of diabetes, which mainly manifests as decreased renal filtration function, leading to symptoms such as proteinuria and edema. As diabetes progresses, renal lesions gradually worsen and renal function gradually decreases, which may eventually lead to renal failure (12–14). Acute kidney injury is one of the important factors of exacerbation of diabetic nephropathy, seriously affecting patients’ quality of life and prognosis. Therefore, studying the influencing factors of acute kidney injury in elderly patients with diabetic nephropathy is of great significance for the prevention and treatment of diabetic nephropathy. Understanding the influencing factors of acute kidney injury in elderly patients with diabetic nephropathy will help us develop more effective prevention and treatment strategies and reduce the risk of mortality and reduced quality of life in patients.
In this study showed that age, ACR, and CysC levels are independent risk factors for acute kidney injury in diabetic nephropathy, and LVEF and eGFR are independent protective factors. The aging population of society is growing rapidly, and the elderly are also at high risk of chronic kidney disease. Due to reduced renal reserve function, various chronic diseases and comorbidities in the elderly, the elderly, especially elderly patients with chronic kidney disease, are highly susceptible to acute kidney injury, and the incidence of acute kidney injury is significantly higher than that of the general population (15–17). The risk of acute renal failure progressing to uremia or death in the elderly is also much higher than that in young adults with kidney disease. As the elderly age, the structure and function of the kidneys change, and aging changes such as glomerulosclerosis, nephron reduction, renal blood vessel wall thickening, renal blood flow and glomerular filtration rate reduction, and renal concentrating function decline gradually occur. As a result, the kidneys of the elderly are prone to acute kidney injury under emergency or injury conditions (18–20). As a clinical test indicator that has been around for many years, ACR is listed as a screening indicator for early kidney disease and a diagnostic and staging standard for chronic kidney disease. It can accurately reflect the status of renal function and improve the clinical value of test results (21). It is helpful to reduce the incidence of complications of diabetic nephropathy and reduce the risk of related diseases. Achieve early diagnosis and early treatment of diabetic nephropathy. Under normal circumstances, the concentration of CysC in serum and plasma is low. When renal function is impaired, the concentration of CysC in the blood changes with the glomerular filtration rate. In renal failure, the glomerular filtration rate decreases, and the concentration of CysC in the blood can increase more than 10 times; if the glomerular filtration rate is normal but the renal tubular function is abnormal, it will hinder the absorption of CysC in the renal tubules. And it is rapidly decomposed, increasing the concentration in urine by more than 100 times (22, 23). In order to prevent diabetes from developing into renal failure, reliable GFR must be used to evaluate the renal function status of diabetic patients. Clinically, SCr is used to evaluate GFR, which lacks sufficient sensitivity for mild renal damage, while CysC can detect mild renal damage. The damage response is sensitive, and regular detection of CysC in diabetic patients can dynamically observe the development of the disease (24, 25). Patients with diabetic nephropathy are also prone to develop cardiovascular disease. Once the ejection fraction of the heart is reduced, it will lead to relative insufficient renal perfusion. Severe infection or severe respiratory failure will further aggravate renal ischemia, leading to a rapid decline in eGFR (26, 27). In addition, drug clearance is reduced after eGFR. Once drugs that may damage the kidneys are used, such as nephrotoxic antibiotics, contrast agents, proton pump inhibitors, etc., the kidney damage will be further aggravated (28–30). Chen et al. (31) found that LVEF is a protective factor for AKI during ECMO support. For every 1% increase in LVEF, the incidence of AKI decreases by 20%. A lower LVEF value before ECMO usually indicates more severe heart failure and shock before starting ECMO support therapy. Decreased cardiac output and hypotension usually mean poor microcirculatory perfusion status. Systemic inflammation is an important mechanism driving AKI and can affect the disease progression and prognosis of patients. Systemic inflammation in elderly patients can aggravate mechanical disorders, microthrombosis, affect cell apoptosis and mitochondrial damage, and induce renal injury. In the context of diabetic nephropathy, the NF-κB signaling pathway is activated, increasing the release of downstream pro-inflammatory factors such as TNF-α, IL-6, IL-1, and IL-18, recruiting monocytes, macrophages, and lymphocytes into the renal tissue, triggering an inflammatory cascade reaction and aggravating renal damage in diabetic nephropathy.
This study established a nomogram model to predict the risk of acute kidney injury in diabetic nephropathy. The C-index of the nomogram risk prediction model in predicting acute kidney injury in diabetic nephropathy is 0.768 (95%CI: 0.663-0.806). The calibration curve tending to the ideal curve; the prediction threshold is >0.18, the nomogram risk prediction model provides clinical net benefits, and the clinical net benefits are higher than independent predictors. This model has the advantage of being easy to understand and operate, and can make individualized predictions based on the patient’s specific situation. Zou et al. (32) found that CysC and eGFR can be used as risk factors for end-stage renal disease in patients with diabetic nephropathy, and a machine learning algorithm based on sAlb, CysC, Hb, eGFR and UTP can effectively predict the incidence of end-stage renal disease.
However, the nomogram model also has certain limitations. First, the establishment of the model relies on existing research data and originates from a single medical institution. There may be differences in regions or specific populations, which makes it impossible to cover all influencing factors, resulting in limited accuracy of prediction results and affecting the external practicality of the nomogram model. Secondly, the nomogram model needs to be updated regularly to reflect the changing research progress and clinical practice. The model prediction is only for reference, and specific clinical decisions still need to be combined with the actual situation of the patient and the professional judgment of the doctor. Finally, the sample size of this study was small, which may have the risk of false negative results. Use with caution before external validation. In future studies, we will increase the sample size to improve the detection ability of different risk factors for AKI and further perform external validation of the nomogram in different populations to further confirm the practicality of this model in a wider range of clinical practice.
In summary, the influencing factors of acute kidney injury in elderly patients with diabetic nephropathy mainly include the patient’s age, ACR, CysC, LVEF, and eGFR. These factors play an important role in the occurrence and development of diabetic nephropathy and provide clinicians with information. Targeted intervention directions. By establishing a nomogram model, the risk of acute kidney injury in diabetic nephropathy was predicted. The model results show that the nomogram model has good prediction effect and has certain clinical application value for early identification of the risk of acute kidney injury in patients with diabetic nephropathy. At the same time, the nomogram model can help doctors more accurately assess the patient’s condition and provide a basis for formulating personalized treatment plans.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by The Second Affiliated Hospital of Hubei University of Science and Technology. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
GW: Writing – review & editing, Writing – original draft. YY: Writing – review & editing, Writing – original draft. MX: Writing – review & editing, Data curation. YZ: Writing – review & editing, Data curation. ZL: Writing – review & editing, Formal analysis. LH: Writing – review & editing, Formal analysis, Data curation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is funded by the Development of AI diagnostic platform based on deep learning algorithm for pathological pictures of glomerular diseases (L998/2023HX045); The Impact of Urine-Derived Stem Cell Exosomes on Diabetic Nephropathy (Hubei Province College Students' Innovation and Entrepreneurship Training Program, Project No. 202310927009).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2024.1431873/full#supplementary-material
Supplementary Table 1 | Multi-factor logistic regression analysis.
ACR, Urine microalbumin-to-creatinine ratio; BUN, Blood urea nitrogen; CysC, Cystatin C; eGFR, Epidermal growth factor receptor; HbAlc, Glycated hemoglobin; LVEF, Left ventricular ejection fraction; ROC, Receiver operating characteristic curve; Scr, Serum creatinine; UA, Uric acid.
1. Wen S, Deng F, Li L, Xu L, Li X, Fan Q. VX-765 ameliorates renal injury and fibrosis in diabetes by regulating caspase-1-mediated pyroptosis and inflammation. J Diabetes Investig. (2022) 13:22–33. doi: 10.1111/jdi.13660
2. Feng X, Wang S, Sun Z, Dong H, Yu H, Huang M, et al. Ferroptosis Enhanced Diabetic Renal Tubular Injury via HIF-1α/HO-1 Pathway in db/db Mice. Front Endocrinol (Lausanne). (2021) 12:626390. doi: 10.3389/fendo.2021.626390
3. Jiang L, Liu X, Hu X, Gao L, Zeng H, Wang X, et al. METTL3-mediated m 6 A modification of TIMP2 mRNA promotes podocyte injury in diabetic nephropathy. Mol Ther. (2022) 30:1721–40. doi: 10.1016/j.ymthe.2022.01.002
4. Wu L, Liu C, Chang DY, Zhan R, Sun J, Cui SH, et al. Annexin A1 alleviates kidney injury by promoting the resolution of inflammation in diabetic nephropathy. Kidney Int. (2021) 100:107–21. doi: 10.1016/j.kint.2021.02.025
5. Tang H, Yang M, Liu Y, Zhu X, Liu S, Liu H, et al. Melatonin alleviates renal injury by activating mitophagy in diabetic nephropathy. Front Endocrinol (Lausanne). (2022) 13:889729. doi: 10.1016/j.kint.2021.10.009
6. Wang H, Huang X, Xu P, Liu X, Zhou Z, Wang F, et al. Apolipoprotein C3 aggravates diabetic nephropathy in type 1 diabetes by activating the renal TLR2/NF- κB pathway. Metabolism. (2021) 119:154740. doi: 10.1016/j.metabol.2021.154740
7. Xu BH, Sheng J, You YK, Huang XR, Ma RCW, Wang Q, et al. Deletion of Smad3 prevents renal fibrosis and inflammation in type 2 diabetic nephropathy. Metabolism. (2020) 103:154013. doi: 10.1016/j.metabol.2019.154013
8. Yang H, Xie T, Li D, Du X, Wang T, Li C, et al. Tim-3 aggravates podocyte injury in diabetic nephropathy by promoting macrophage activation via the NF- κB/TNF-α pathway. Mol Metab. (2019) 23:24–36. doi: 10.1016/j.molmet.2019.02.007
9. Cheng Q, Pan J, Zhou ZL, Yin F, Xie HY, Chen PP, et al. Caspase-11/4 and gasdermin D-mediated pyroptosis Contributes to podocyte injury in mouse diabetic nephropathy. Acta Pharmacol Sin. (2021) 42:954–63. doi: 10.1038/s41401-020-00525-z
10. Jiang WJ, Xu CT, Du CL, Dong JH, Xu SB, Hu BF, et al. Tubular epithelial cell-to-macrophage communication forms a negative feedback loop via extracellular vesicle transfer to promote renal inflammation and apoptosis in diabetic nephropathy. Theranostics. (2022) 12:324–39. doi: 10.7150/thno.6373
11. Liu S, Zhao Y, Lu S, Zhang T, Lindenmeyer MT, Nair V, et al. Single-cell transcriptomics reveals a mechanosensitive injury signaling pathway in early diabetic nephropathy. Genome Med. (2023) 15:2. doi: 10.1186/s13073-022-01145-4
12. Zheng C, Huang L, Luo W, Yu W, Hu X, Guan X, et al. Inhibition of STAT3 in tubular epithelial cells prevents kidney fibrosis and nephropathy in STZ -induced diabetic mice. Cell Death Dis. (2019) 10:848. doi: 10.1038/s41419-019-2085-0
13. Ma R, He Y, Fang Q, Xie G, Qi M. Ferulic acid ameliorates renal injury via improving autophagy to inhibit inflammation in diabetic nephropathy mice. BioMed Pharmacother. (2022) :153:113424. doi: 10.1016/j.biopha.2022.113424
14. Han H, Chen Y, Yang H, Cheng W, Zhang S, Liu Y, et al. Identification and verification of diagnostic biomarkers for glomerular injury in diabetic nephropathy based on machine learning algorithms. Front Endocrinol (Lausanne). (2022) 13:876960. doi: 10.3389/fendo.2022.876960
15. Li Q, Liao J, Chen W, Zhang K, Li H, Ma F, et al. NAC alleviative ferroptosis in diabetic nephropathy via maintenance Mitochondria redox homeostasis through activating SIRT3-SOD2/Gpx4 pathway. Free Radic Biol Med. (2022) 187:158–70. doi: 10.1016/j.freeradbiomed.2022.05.024
16. Xiang E, Han B, Zhang Q, Rao W, Wang Z, Chang C, et al. Human umbilical cord-derived mesenchymal stem cells prevent the progression of early diabetic nephropathy through inhibiting inflammation and fibrosis. Stem Cell Res Ther. (2020) 11:336. doi: 10.1186/s13287-020-01852-y
17. Lei L, Zhao J, Liu XQ, Chen J, Qi XM, Xia LL, et al. Wogonin alleviates kidney tubular epithelial injury in diabetic nephropathy by inhibiting PI3K/akt/NF- κB signaling pathways. Drug Des Devel Ther. (2021) 15:3131–50. doi: 10.2147/DDDT.S310882
18. Li MR, Lei CT, Tang H, Yin XJ, Hao Z, Qiu Y, et al. MAD2B promotes podocyte injury through regulating Numb-dependent Notch 1 pathway in diabetic nephropathy. Int J Biol Sci. (2022) 18:1896–911. doi: 10.7150/ijbs.68977
19. Wang Z, Wu Q, Wang H, Gao Y, Nie K, Tang Y, et al. Diosgenin protects against podocyte injury in early phase of diabetic nephropathy through regulating SIRT6. Phytomedicine. (2022) :104:154276. doi: 10.7150/ijbs.68977
20. Tan SM, Ziemann M, Thallas-Bonke V, Snelson M, Kumar V, Laskowski A, et al. Complement C5a induces renal injury in diabetic kidney disease by disrupting mitochondrial metabolic agility. Diabetes. (2020) 69:83–98. doi: 10.2337/db19-0043
21. Nishio H, Ishii A, Yamada H, Mori KP, Kato Y, Ohno S, et al. Sacubitril/valsartan ameliorates renal tubulointerstitial injury through increasing renal plasma flow in a mouse model of type 2 diabetes with aldosterone excess. Nephrol Dial Transplant. (2023) 38:2517–27. doi: 10.1093/ndt/gfad098
22. Qiu M, Ding LL, Zhang M, Zhou HR. Safety of four SGLT2 inhibitors in three chronic diseases: A meta-analysis of large randomized trials of SGLT2 inhibitors. Diabetes Vasc Dis Res. (2021) 18:14791641211011016. doi: 10.1177/14791641211011016
23. Lv C, Cheng T, Zhang B, Sun K, Lu K. Triptolide protects against podocyte injury in diabetic nephropathy by activating the Nrf2/HO-1 pathway and inhibiting the NLRP3 inflammasome pathway. Ren Fail. (2023) 45:2165103. doi: 10.1080/0886022X.2023.2165103
24. Sun MY, Ye HJ, Zheng C, Jin ZJ, Yuan Y, Weng HB. Astragalin ameliorates renal injury in diabetic mice by modulating mitochondrial quality control via AMPK-dependent PGC1α pathway. Acta Pharmacol Sin. (2023) 44:1676–86. doi: 10.1038/s41401-023-01064-z
25. Zou TF, Liu ZG, Cao PC, Zheng SH, Guo WT, Wang TX, et al. Fisetin treatment alleviates kidney injury in mice with diabetes-exacerbated atherosclerosis through inhibiting CD36/fibrosis pathway. Acta Pharmacol Sin. (2023) 44:2065–74. doi: 10.1038/s41401-023-01106-6
26. Yang M, Zhang Q, Luo S, Han Y, Zhao H, Jiang N, et al. DsbA -L alleviates tubular injury in diabetic nephropathy by activating mitophagy through maintenance of MAM integrity. Clin Sci (Lond). (2023) 137:931–45. doi: 10.1042/CS20220787
27. Chung JY, Tang PM, Chan MK, Wang L, Huang XR, To KF, et al. AANG prevents smad3-dependent diabetic nephropathy by restoring pancreatic β-cell development in db/db mice. Int J Biol Sci. (2022) 18:5489–502. doi: 10.7150/ijbs.72977
28. Packer M. Role of impaired nutrient and oxygen deprivation signaling and deficient autophagic flux in diabetic CKD development: implications for understanding the effects of sodium-glucose cotransporter 2-inhibitors. J Am Soc Nephrol. (2020) 31:907–19. doi: 10.1681/ASN.2020010010
29. Bagang N, Gupta K, Singh G, Kanuri SH, Mehan S. Protease-activated receptors in kidney diseases: A comprehensive review of pathological roles, therapeutic outcomes and challenges. Chem Biol Interact. (2023) 377:110470. doi: 10.1016/j.cbi.2023.110470
30. Liu Z, Liu H, Xiao L, Liu G, Sun L, He L. STC-1 ameliorates renal injury in diabetic nephropathy by inhibiting the expression of BNIP3 through the AMPK/SIRT3 pathway. Lab Invest. (2019) 99:684–97. doi: 10.1038/s41374-018-0176-7
31. Chen W, Pei M, Chen C, Zhu R, Wang B, Shi L, et al. Independent risk factors of acute kidney injury among patients receiving extracorporeal membrane oxygenation. BMC Nephrol. (2023) 24:81. doi: 10.1186/s12882-023-03112-6
32. Zou Y, Zhao L, Zhang J, Wang Y, Wu Y, Ren H, et al. Development and internal validation of machine learning algorithms for end-stage renal disease risk prediction model of people with type 2 diabetes mellitus and diabetic kidney disease. Ren Fail. (2022) 44:562–70. doi: 10.1080/0886022X.2022.205605
Keywords: acute kidney Injury, elderly diabetic nephropathy, influencing factors, nomogram, model
Citation: Wu G, Ye Y, Xu M, Zhang Y, Lu Z and Huang L (2025) Influencing factors of acute kidney injury in elderly patients with diabetic nephropathy and establishment of nomogram model. Front. Endocrinol. 15:1431873. doi: 10.3389/fendo.2024.1431873
Received: 13 May 2024; Accepted: 19 November 2024;
Published: 30 January 2025.
Edited by:
Georgia Damoraki, National and Kapodistrian University of Athens, GreeceReviewed by:
Huaqing Zheng, The University of Utah, United StatesCopyright © 2025 Wu, Ye, Xu, Zhang, Lu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanli Ye, eWFubGl5ZWRyQHllYWgubmV0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.